situation_concept_theories
TRANSCRIPT

พญ.ปทมา โกมทบตร
คณะแพทยศาสตรมหาวทยาลยเชยงใหม
Situation * Concepts * Theories associated with continuity
cancer care
อบรมเฉพาะทาง สาขาการพยาบาลผปวยมะเรง

นโยบาย แนวคด และทฤษฎทเกยวของ
กบการดแลผปวยมะเรงอยางตอเนอง
จนระยะสดทาย
Outline
• Part I : Situation• Part II : Concepts• Part III : Theories• Part IV : Case discussion

Part I : Situation
• ยทธศาสตรระยะทาย
• สถานการณปจจบน
• แนวโนมในอนาคต

http://www.gogood.in.th/upload/article/F_1_1.pdf


Morphine equivalent(mg/capita)
2003Thailand 4.0 Malaysia 2.0UK 101.7USA 444.1
2013Thailand 4.4 Malaysia 64.5UK 241.4USA 717.9
Medical opioid consumption :Indirect measurement of palliative medicine
The Pain & Policy Studies Group global research at the University of Wisconsinhttps://ppsg.medicine.wisc.edu/
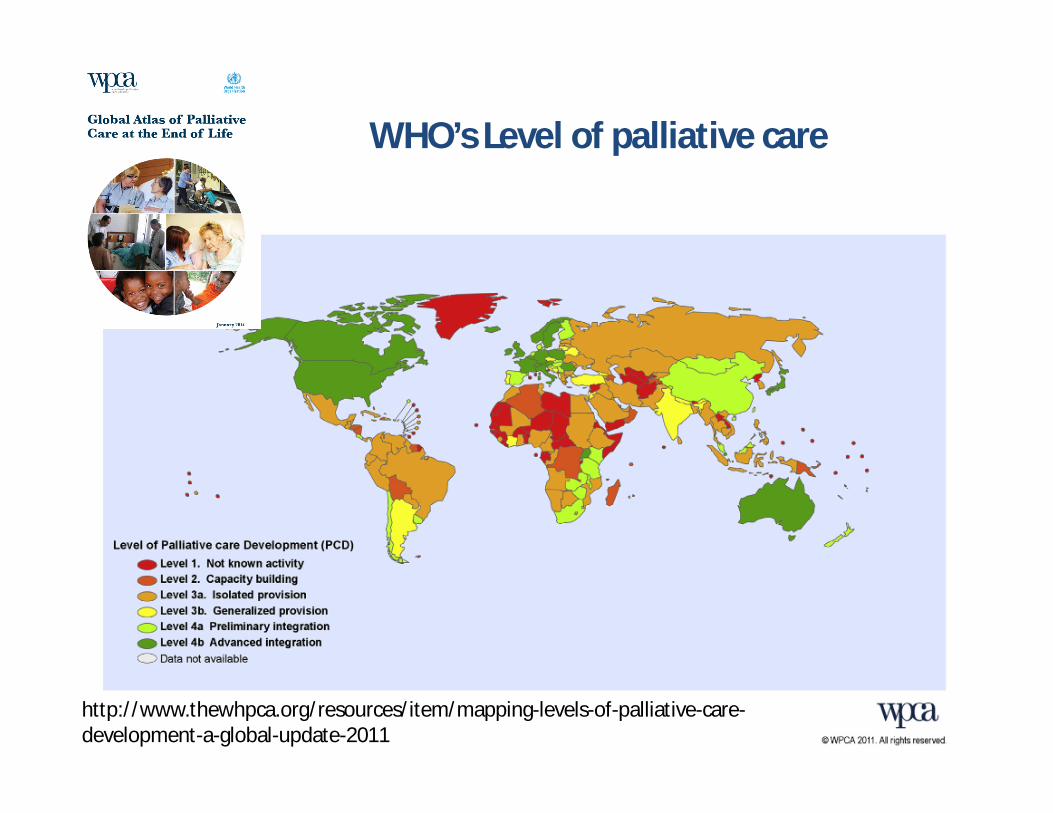
WHO’s Level of palliative care
http://www.thewhpca.org/resources/item/mapping-levels-of-palliative-care-development-a-global-update-2011


Quality of death index
http://www.economistinsights.com/healthcare/analysis/quality-death-index-2015/fullreport

UK no.1Taiwan no.6USA no.9..Thailand no.44

Trend of palliative care in Thailand
• Three main streams• Public health stream
– Community oriented – Hospice ward in hospital
• Commercial stream– Luxery long term care - hospice care
• Academic stream– Research and development model– Integrate multidisplinary experts

Part II :Concepts
• Different between– การดแลแบบบรบาลบรรเทา (Palliative care)– การดแลในระยะทาย (end of life care)– การดแลแบบบานพกระยะทาย (Hospice)
• “Why framework”– Disease management– Symptom management– Spiritual management

Palliative care คอ
• สนหวง ?• การณฆาต ?• มอรฟน ?• ถอด tube ?• ใสบาตร ?

Palliative care = Whole person care
Balfour Mount, 1975 ศลยแพทยแคนาดา ผรเรมใชคา Palliative care

WHO’s definition of palliative care

Palliative care Vs End of life careVersion 1: End of life care = Terminal care
EAPC recommendation: standard and norms for hospice and palliative care 2009 http://www.eapcnet.eu/Themes/Organisation/EAPCStandardsNorms.aspx

Version 2:End of life care = Prepare for good death
EAPC recommendation: standard and norms for hospice and palliative care 2009 http://www.eapcnet.eu/Themes/Organisation/EAPCStandardsNorms.aspx

EAPC recommendation: standard and norms for hospice and palliative care 2009 http://www.eapcnet.eu/Themes/Organisation/EAPCStandardsNorms.aspx
Graded system of Palliative care “service” (European standard)

Hospice care VS Pallaitive care
• Hospice mainly based on Art & Humanities• Palliative mainly based on Science&Medicine
‘Medical Model like a man ( Have to DO something)Hospice Model like a woman( Just BE there)’
Bart Gruzalskico-founder of Houston hospice

Definitions
• Formal definition = WHO’s• Practical definition = Depend on purpose
– National policy maker• Palliative care “service” : Health economics
– Local health care• Palliative care “approach” : Humanized

“WHY” Framework
• David C. Currow’s• Critical thinking approach for symptom
management in Palliative patient• Change form ‘ Reflex’ to ‘Reflect’ approach• Reduce Terminal sedation

คลาย อรยสจ 4
• ทกข : What is priority of concern อาการอะไรทสาคญ ‘สาหรบผ ปวย’ ทสด
• สมทย : *Any reversible cause* - อาการนนไมควรเพมขนตามความกาวหนาของโรค
- เกดขนฉบพลน
• นโรธ : What is the mutual goal - เปาหมายการบรรเทาอาการทผ ปวย(และญาต) ตองการ
• มรรค : What are acceptable means-> Solve reversible cause (Including Iatrogenic)-> Non-Med-> Med


Simplify palliative care model for FMStep objective Assess tool
(PCM)Action tools
Disease Management
Inform diagnosis and options of treatment
I = Idea Breaking bad news “SPIKES” + “NURSE”
Family support“CAREGIVER”
Family conference
Prognosisdetermination
Illness Management
Ensure optimal pain and symptom control
F = FeelingF = Function
Pain /Symptom managementguideline
Wish management **
Transform “wish/dream” to “goal”
E = Expectation AdvancedirectiveDignity therapy
Gomutbutra 2012

IFFE
• Idea: ผปวยทราบหรอไมวาตวเองเปนโรคอะไร
• Feeling: ในขณะนรสกอยางไรกบโรคทเปน มอาการอะไรทรบกวนชวตมากทสด
• Function: ใชชวตประจาวนไดหรอไม
• Expectation : “Wish” ฝนวาอยากใหเปนอยางไร -> เพราะอะไร?
“Goal” แลวจะทาอยางไร
N-U-R-S-E
• Naming
• Understand
• Respect
• Support
• Explore

CAREGIVER
• C Care ผดแลมหนาทอะไรบาง
• A Affect รสกอยางไร
• R Rest ไดพกบางไหม
• E Empathy เขาใจความลาบาก
• G Goal อยากใหเปนอยางไร
• I Information ใหขอมลอยางงาย
• V Ventilation ใหระบายความทกข
• E Empower ปลกปลอบกาลงใจ
• R Resources หาแหลงใหความชวยเหลอ
Jaturapatporn D.2011

Part III :Theories
• ทฤษฎเกยวกบการเปลยนแปลงของรางกาย
ขณะใกลเสยชวต
เสยชวต..เมอไหร?
ก. หมดลมหายใจ
ข. หวใจหยดเตน
ค. หมดสตรบร
ง. หมดการตอบสนองตามอตโนมต

การเสยชวต ทางการแพทย
ตามประกาศแพทยสภา
• มการหยดทางานของระบบไหลเวยนโลหตและระบบการหายใจอยางไม
สามารถฟนคนสภาพได
• มภาวะสมองตาย “กานสมอง – brain stem” ตาย
- ไมอยภายใตภาวะถกกดประสาท ดวยยา เกลอแรในรางกาย หรอ สงแวดลอม
- ไมมการตอบสนองอตโนมตทางประสาท (reflex)



กระบวนการตาย (Dying process)
• Telomere

มกระบวนการตาย ระดบเซลลตลอดเวลา
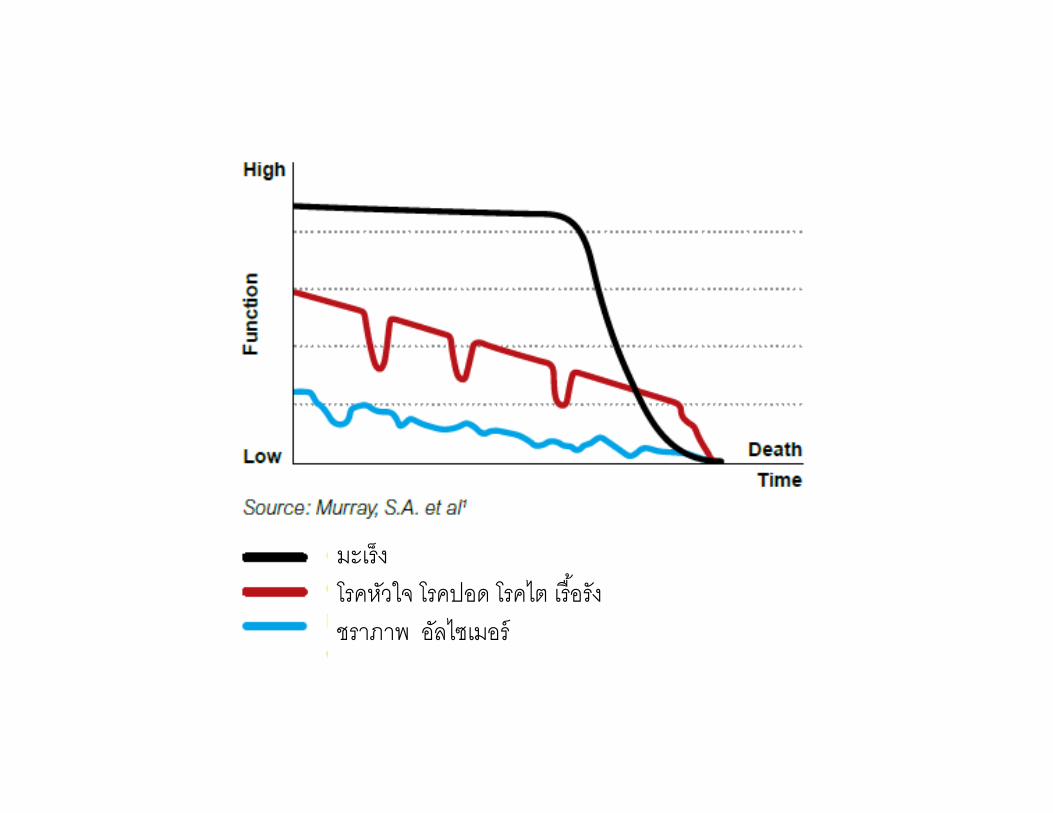
มะเรง
โรคหวใจ โรคปอด โรคไต เรอรง
ชราภาพ อลไซเมอร

เปลอกสมอง
สมองชนใน
กานสมอง

สงทปรากฎเมอใกลเสยชวต (Active dying)• พดนอย คดชา
• สบสน จตหลอนเปนชวงๆ ( delirium)

Delirium ผานมมมองผปวย

• ออนแรง / “ความรสก” ไมมแรง (fatigue)• ไมหวอาหาร ไมหวนา (anorexia)
- รางกายสลายไขมนและโปรตนเปน สารคโตน สารยเรย

เมอเราอดอาหารและนา• ปกตสมองใชนาตาลเปนพลงงาน
• หลง 24 ชวโมง นาตาลทสะสมในตบจะหมดไป
• รางกายเรมสลายไขมนมาเปน “สารคโตน” และ “นา”• รางกายสลายโปรตนเปนอนดบตอมา เปน “ยเรย”

• กลนไมได มเสยงครางจากนาลายทคางในปาก (death rattle)• กลไกการหายใจเรรวน ปากขยบคลายหวอากาศ ( Respiration
with mandibular movement)• หวใจใกลหยดเตน ชพจรคลาไมได มอเขยวเยน (cyanosis)

Signs of Active Dying in 100 Cancer Patients ( Morita,1998)
• Sign Mean/median hours prior to death (+ SD)• Retained respiratory secretions audible (“Death
rattle”) 57/23 hours (82)• Respirations with mandibular movement
(Jaw movement increases with breathing)7.6 /2.5hours (18)
• Cyanosis and skin mottling5.1/1.0 hours (11)
• No radial pulse2.6/1.0 hours (4.2)

Naturally,Most of dying have ‘smooth’
pathway

Part IV: Case discussion
• ผ ปวยหญงไทย อาย 63 ป ไดรบการวนจฉยเปนมะเรงปากมดลก เคยไดรบการรกษาดวยการผาตดและฉายแสง หลงจากนนมภาวะลาไสเลกอดตนจน
ตองผาตด โรคประจาตวอนคอ COPD • ผ ปวยขาดการตดตอกบแพทยเปนเวลา 2 ป เนองจากปญหาภายใน
ครอบครว จงมาพบอกครงดวยอาการปวดสะโพกราวลงกน และเหนอยงาย
• ตรวจรางกาย พบภาวะซด, ปอดขวาไดยนนอยกวาดานซาย
และขาขางขวาบวม PPS = 70%• ตรวจวนจฉยเพมเตม จงพบ CA cervix recurrent with pelvic
bone, lung metastasis และ Deep vein thrombosis

• หลงจาก Family meeting ไดขอสรป รกษาตามอาการทบาน
• ผ ปวยไดรบยาบรรเทาอาการดงน
- Morphine sustain release 300 mg/day + Morphine IR 10 mg prn pain
- Berudual prn dyspnea (ของ COPD เดม)
- Wafarin (สาหรบ DVT)- Lorazepam 1 mg hs- Folic tab
• ผ ปวยอาการคงทเปนเวลา 2 เดอน แลวเรมลกยนไมได
• 2 สปดาหตอมา นงไมไหว ทานอาหารแลวอาเจยน ลกสาวจงนามา
นอนโรงพยาบาล แพทยจงใส NG • ระหวางนอนโรงพยาบาล
- ผ ปวยบนบรเวณปวดทองนอยมากขน
- เพอ ถามไมตอบ ผดลกผดนงตอนกลางคน
- อาการเหนอยเพมขน และมเสยงหายใจดงครดคราด
- ผ ปวยมเลอดออกจากทวารหนก เปนลมเลอด
• ลกๆ ของผ ปวยแสดงเจตนารมย ตองการใหผ ปวยไปเสยชวตทบาน แต
กงวลใจวาจะทนดมารดาทรมานไมได
