soft tissue foreign body
TRANSCRIPT
Runal Shah2nd year MEM
KDAH
Soft Tissue Foreign Body

Objectives
• Introduction• Patho-physiology• Clinical features• Diagnosis• Treatment• Disposition & Follow up

Introduction• Any object becomes a foreign body when it penetrates the
skin and lodges in the soft tissue.• Most common : Wood, metal & glass
• Inert (Nonreactive)o Bulletso Needleso Metallic itemso Glass
• Organic (Reactive)o Woodo Boneo Soilo Rubbero Thorns

Patho-physiology• Clean wound – transient inflammation• With foreign body – prolong inflammation, resistance or
minimal response to Antibiotics/ NSAIDs/ Steroids• Material which are are inert, don’t elicit abnormal tissue
response but metal with oxidized paint (Earring!!) causes moderate-severe inflammation
• Vegetative FB, such as wood, thorns, and spines, trigger the most severe inflammatory reactions.

Patho-physiology• Local toxic reaction : Blackthorns, oils-resins of cedar splinters
and redwood, sea-urchin spine, catfish spine
• Rose thorn or cactus spine : allergic response to fungi on it• Systemic toxicity and Allergic reactions are unusual but most
serious complications of FB.• FBs containing Lead can cause Lead poisoning if they are in
contact with Pleural/Peritoneal/Joint/Cerebrospinal Fluid.

Patho-physiology
• It can be as a variety from– Local inflammation– Cellulitis– Abscess formation– Lymphangitis
– Tenosynovitis– Bursitis– Septic Arthritis– Osteomyelitis
• Infections are the most common complications of retained FBs.
• Infections resolve spontaneously post foreign body removal
• Plant thorn injury : Pantoea Agglumerans (enterobacteriacae)
• Immunocompromised – fungal infections

Clinical Features• History– Mechanism of injury– Composition and shape of wounding object– Shape and location of resulting wound
• Foreign body sensation in the healed wound• Persistent pain/ infection or pressure sensation with
movement

Clinical Features• Physical examination Obtain good light and local anesthesia Before anesthetic is administered, gently run over your
gloved finger over FB suspected region for eliciting characteristic sensation
Local pressure >1min in a bleeding wound If bleeding continues, try a tourniquet for 15min,
Sphygmomanometer BP cuff inflated above SBP with limb elevation

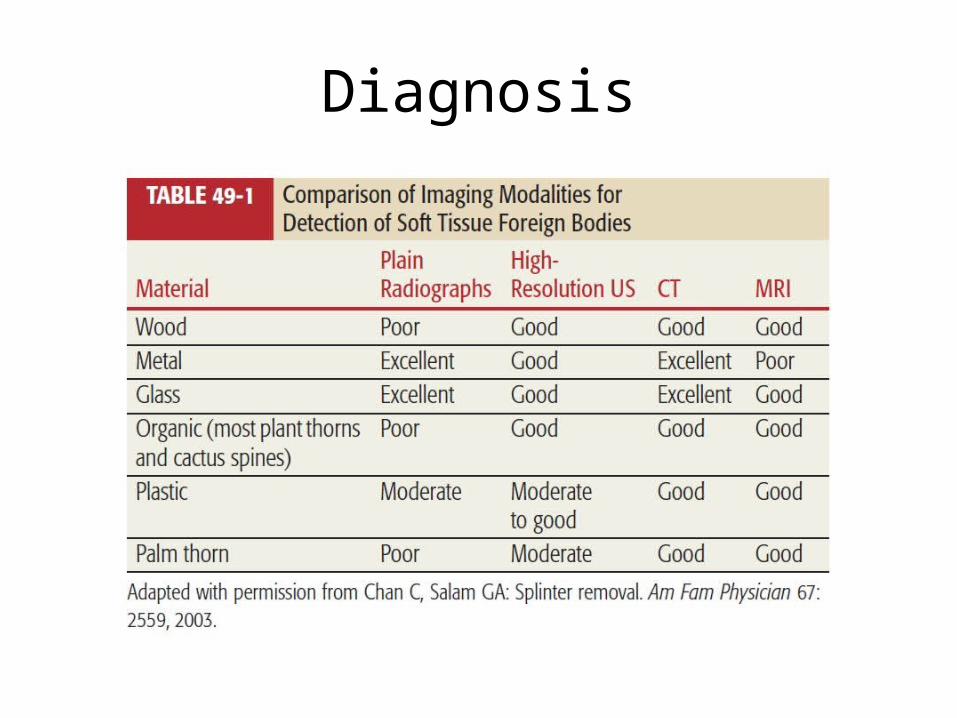
Diagnosis• Imaging1. Plain Radiography
– Most objects are readily visualized (80%)– Fragments >0.5 mm or large can be seen– Suspected sites multiple views can be taken up– Wood, thorns, chicken bones, plastics, some glass cant be seen
2. USG– Bedside tool– Prompt localization & assisted removal– Nonradiodense FB 1x2mm or larger can be detected– Operator dependent

Diagnosis• Imaging3. CT scan
– 100 times more sensitive in differentiating densities than X rays– Thorns, spines, wood splinters and toothpicks, fish bones, and plastic
foreign bodies have been identified with CT– High cost, high radiation, wood FB mimic air bubbles
4. MRI– Non-metallic FBs can be detected accurately– Gravel/ metal containing FB have ferromagnetic streaks which
obscures visualization– Exact location relating to anatomic structure can be sought
Diagnosis


http://radiopaedia.org/cases/ingested-foreign-body-fish-bone

http://radiopaedia.org/cases/foreign-body-in-oesophagus-1

http://radiopaedia.org/cases/foreign-body-in-palm-lead-tip

http://radiopaedia.org/cases/palm-frond-foreign-body

http://www.ultrasoundcases.info/Slide-View.aspx?cat=453&case=2019

Treatment
Exploration in ED• Do not explore the following wounds in ED– Stab wounds to the neck, chest, abdomen, or perineum– Compound fracture wounds requiring surgery in theatre– Wounds over suspected septic joints or infected tendon
sheaths– Most wounds with obvious neurovascular/tendon injury
needing repair– Other wounds requiring special expertise (e.g. eyelids)

Disposition & Follow up Wound care with thorough irrigation If multiple radiopaque objects removed, post procedure
imaging to be done Except clean wounds, prefer Delayed closure over Primary
closure. Tetanus immunization If a FB is near highly mobile area or joint, affected area should
be splinted before removal to prevent further injury or migration of the object.
SPECIALITY CONSULTATION [ORTHO/ GEN/PLASTIC SURGERY]

Ref :Tintinalli 7/e
Wounds and Lacerations by Alexander Trott 4/eOxford Handbook of Emergency Medicine 4/e
Medscape
THANK YOU…