special edition 2011 the edwards transcatheter heart valve...
TRANSCRIPT

Guest Editors:
Prof. Dr. Thomas WalThEr Director, Department carDiac Surgery, KercKhoff-KliniK, BaD nauheim, germany
Prof. Dr. med. GErharD schulErherzzentrum leipzig gmBh, clinic for internal meDicine/carDiology, leipzig,germany
TAVItalkSpecial Edition 2011 The Edwards Transcatheter Heart Valve (THV) Newsletter
for uSe outSiDe the uniteD StateS only. not intenDeD for general DiStriBution.
ThIs IssuE
a landmark trial in the treatment of severe asProf. Dr. Thomas WalThEr, GuEsT EDITorDirector, Department cardiac Surgery
Kerckhoff-Klinik, Bad nauheim, germany
The recent PARTNER Trial results represent one of the landmark trials of this century,
focusing on the treatment of high-risk patients with severe aortic stenosis. New minimally inva-sive transcatheter approaches, whether delivered transfemorally (retrograde approach) or transapi-cally (antegrade approach), have proven to yield comparable results to conventional aortic valve
surgery, a procedure that has been established over five decades, in high-risk elderly patients. The teams of interventional cardiologists and cardiac surgeons have to be congratulated for obtaining excellent outcomes, especially in the short-term with very low 30-day mortality rates, and for reaching the goal of non-inferiority for the primary endpoint of 1-year mortality.
(continued on page 2)
At Edwards, our goal is to develop new technologies that will contribute to improved patient outcomes in conjunction with an
improved quality of life. However, there are many milestones on the road to developing successful new therapies. The latest results from The PARTNER Trial (Placement of AoRTic traNscathetER valves) —the world’s first randomised clinical trial of a transcatheter aortic heart valve, presented in March 2011 at the American College of Cardiology’s (ACC) 60th Annual Scientific Session in New Orleans—signify a major milestone in the continued development of aortic valve therapy.
This balloon-expandable, catheter-based aortic valve re-placement technique with a similar one-year survival represents a major advance in the treatment of patients at high risk for surgery. Nonetheless, no matter how encouraging these latest results are, The PARTNER Trial simply denotes one more step in our clinical research program.
There remains a lot to be done. Looking to the future, we have a comprehensive clinical programme in various stages of develop-ment. In 2011 alone, enrolment is on-going in no less than four clinical trials worldwide. In addition, we remain committed to our policy of publishing in peer-reviewed journals the follow-up results from previously reported trials.
This extensive R&D and clinical research programme requires dedication and commitment from all those involved. I would like to take this opportunity to thank the outstanding panel of clinical trial investigators and their respective teams for their hard work and dedication in support of the Edwards clinical trial programme.
GuEsT EDITorIal
milestones in the development of aortic valve technology
JEan-luc lEmErcIEr Vice president, thV europe edwards lifesciences
1 a lanDmark TrIal In ThE TrEaTmEnT of sEvErE as prof. Dr. thomaS Walther, gueSt eDitor
1 mIlEsTonEs In ThE DEvEloPmEnT of aorTIc valvE TEchnoloGY Jean-luc lemercier, Vp, thV, eDWarDS lifeScienceS
3 rElEcTIons on ThE ParTnEr TrIal prof. Dr. meD gerharD Schuler, gueSt eDitor
4 cosT-EffEcTIvEnEss & rElEvancE of ThE ParTnEr TrIal DaTa In EuroPE an interVieW With raymonD lauret, eDWarDS lifeScienceS
2-6 QuoTaBlEs olaf WenDler, mD, phD; frieDrich W. mohr, mD, phD; pilar tornoS maS, mD; thierry lefÈVre, mD; ottaVio alfieri, mD
7-10 sPEcIal sEcTIon: ThE ParTnEr TrIal cohorTs a & B In closE-uP
11 QuoTaBlEs eulogio garcia, mD; Joelle Keefer, mD, phD; e. murat tuzcu, mD; craig r. Smith, mD; martyn thomaS, mD; ian t. mereDith, mBBS, phD; martin leon, mD; BernarD iung, mD, phD
14 EnGInEErs’ cornEr: comparing Edwards saPIEn and saPIEn xT Thvs laKSen Sirimanne, Vp, r&D, thV, eDWarDS lifeScienceS
16 ThE ‘nauTIlus’: EDWarDs’ clInIcal hIsTorY of TavI JoDi aKin, Vp, gloBal clinical affairS, eDWarDS lifeScienceS
16 QuoTaBlE Spencer B. King iii, mD

TAVItalk sPEcIal EDITIon2
for use outside the united States only | not intended for general distribution.
TAVItalk 2
The excellent outcomes of this trial are remarkable, especially in view of the patients’ high-risk profiles. Nineteen of the 25 sites had no prior experience with TAVI procedures before starting this study. Detailed teaching protocols, specific patient screening, regular con-ference calls with detailed discussions on all specific patient-related aspects, as well as carefully proctored initial implants were clearly key factors for these successes. Guidance by the FDA in the US and study support by the sponsor contributed to these favourable outcomes. Thus, thought-ful and stepwise distribution of new technology seems to be the ideal strategy to obtain meaningful and perfect results.
What can we take out of these re-sults in order to further improve out-comes in European practice? There may also be some good short-term results in Europe, but most centres that have been performing TAVI procedures for several years would not be able to obtain equivalent outcomes
given that many of the patients treated in Europe (in an all-comers situation) would have been excluded by The PARTNER Trial design. Thus, some selection bias may have influenced the over-all outcomes. As such, a comparison between The PARTNER
Trial Cohort A (n = 348) and The SOURCE Registry (n = 1,038) reveals a difference in 30-day mor-tality rates of 3.4% versus 8.5%. However, at 1 year, mortality rates are almost identical, namely 24.2% versus 23.9%, respectively.*
In summary, during the past few years, TAVI has evolved as a great procedure, using either the transfemoral or the transapical approach in treating high-risk elderly patients with aortic stenosis in a truly minimally invasive manner. In the future, we need to perform the right procedures with the right Heart Teams in order to offer our patients the best options.
THOMAS WALTHER (continued from page 1)
The PARTNER Trial Cohort A results demonstrate that, even with the first generation of the Edwards SAPIEN valve, outstanding results for transfemoral (TF) and transapical (TA) aortic valve implantation
(AVI) can be achieved. For the surgical community, it is reassuring that conventional aortic valve replace-ment (AVR) is not inferior to TAVI in terms of mortality, even in high-risk patients with aortic stenosis.
Compared to the European experience, it is impressive to see that the 30-day mortality in Cohort A (TF: 3.3%, TA: 3.8%), but also Cohort B (TF: 5%), is lower compared to The SOURCE Registry (TF: 6.3%, TA 10.3%). In fact, Cohort A 30-day mortalities are the lowest reported so far. At present, it remains to be seen if this is a result of the selection process of Cohort A, in which inoperable patients had been excluded, or if it is explained by something else. However, one wonders why this lower 30-day mortality does not translate into lower 1-year mortalities, which are very similar between Cohort A (TF: 22.2%, TA: 29%), Cohort B (30.7%), and The SOURCE Registry (TF: 19.9, TA: 27.9%).
The PARTNER Trial has answered some of the burning questions about transcatheter AVI, however, as is often the case with excellent studies, it also raises new questions. Close cooperation between Heart Teams and different regions will remain key to finding the right answers.
TAVItalk
QUOTABLE
The lowest reported 30-day mortalities so far
olaf WEnDlEr, mD, PhD, frcs clinical Director for cardiovascular Services consultant cardiothoracic Surgeon King’s college hospital, Denmark hill london, united Kingdom
Thoughtful and stepwise
distribution of new technology
seems to be the ideal
strategy to obtain meaningful and perfect results.
sPEcIal EDITIon
*percentages represent tf/ta cohorts combined

TAVItalkEuroPE 3 TAVItalkEuroPE 3
Q: What are your thoughts regarding The PARTNER Trial Cohort A data?
A:I was really surprised—in a positive way—to look at The PARTNER Trial data and see the successful translation of new technology into practice with a very low mortality rate. And also, I was surprised by the surgical results. I would have
guessed that, in this high-risk group, the outcome would be about 6.5% in the surgical arm, so I was really surprised to see that the transcatheter approach was even better in these early outcomes. I think that’s a very positive message, and it tells us the trial was performed in a very careful manner and that all participants, cardiologists and surgeons, tried to do their best. These are excellent data.
Q: What impact do you believe these data will have on TAVI adoption?
A:I think this is something that will cause surgeons, who did not look at this high-risk cohort until today, to now be interested in treating these patients who have previously not been operated on in many centres. We need to accept that, especially for
the high-risk patients, there is a very suitable alternative that can reduce the surgical trauma and has at least a good short-term result. In Cohort A, we are looking at data out to 12 months and, in some of the patients, we have data out to 24 months. There is no doubt that these data are valid and actually confirm our practice in Europe over the past three to four years. We have very deliberately used these catheter-based techniques in these high-risk patients.
TAVItalk
QUOTABLE
successful translation of a new technology into practice
Prof. frIEDrIch W. mohr, mD, PhD herzzentrum leipzig gmbh universitätsklinik leipzig, germany
reflections on The ParTnEr TrialProf. Dr. mED. GErharD schulEr, GuEsT EDITorherzzentrum leipzig gmbh clinic for internal medicine/cardiology leipzig,germany
As demonstrated by the commentary offered by my esteemed col-leagues that you can find throughout
this issue of TAVItalk, The PARTNER Trial results from both cohorts of this well-designed trial are impressive. Last September, the results from Cohort B demonstrated the dramatic superiority of TAVI over best medical therapy. The results from Cohort A presented last month at the Annual Scientific Session of the ACC demonstrated equivalence between TAVI and AVR in the high surgical risk patient population. I join in the comments published here and elsewhere that have commended these results, as well as all of those who took part in this exemplary trial. I also appreciate that the results from The PARTNER Trial complement the extensive data sets that we have established in the various large registries here in Europe.
I am honoured to be a guest editor of this issue of TAVItalk with Thomas Walther, who was also an early adopter of TAVI. Although he now works in Bad Nauheim, Germany, I previously had the
privilege of working with Prof. Walther when he worked with Prof. Mohr and our Heart Team in Leipzig. To the best of my knowledge, Prof. Walther has performed more trans-apical TAVI procedures than anyone else in the world, and has been instrumental in driving the transapical technology and learnings. It has been a great honour to be part of this dedicated team of cardiologists and surgeons that has propelled this therapy and built bridges between specialties.
As an early pioneer of angioplasty, it has been gratifying to be involved in the early adoption of TAVI and to see how TAVI has changed the paradigm that
was previously established in coronary care. While angioplasty once separated surgeons and cardiologists, it has been rewarding to be part of a therapy that is bringing these two specialties together to offer our patients the very best options for their treatment.
I hope that you enjoy this edition of TAVItalk and continue to share our enthusiasm for this burgeoning technology as we seek to improve the lives of our patients.
GuEsT EDITorIal
Q: In one sentence, could you describe what the cost-effectiveness results from Cohort B of The PARTNER Trial show?
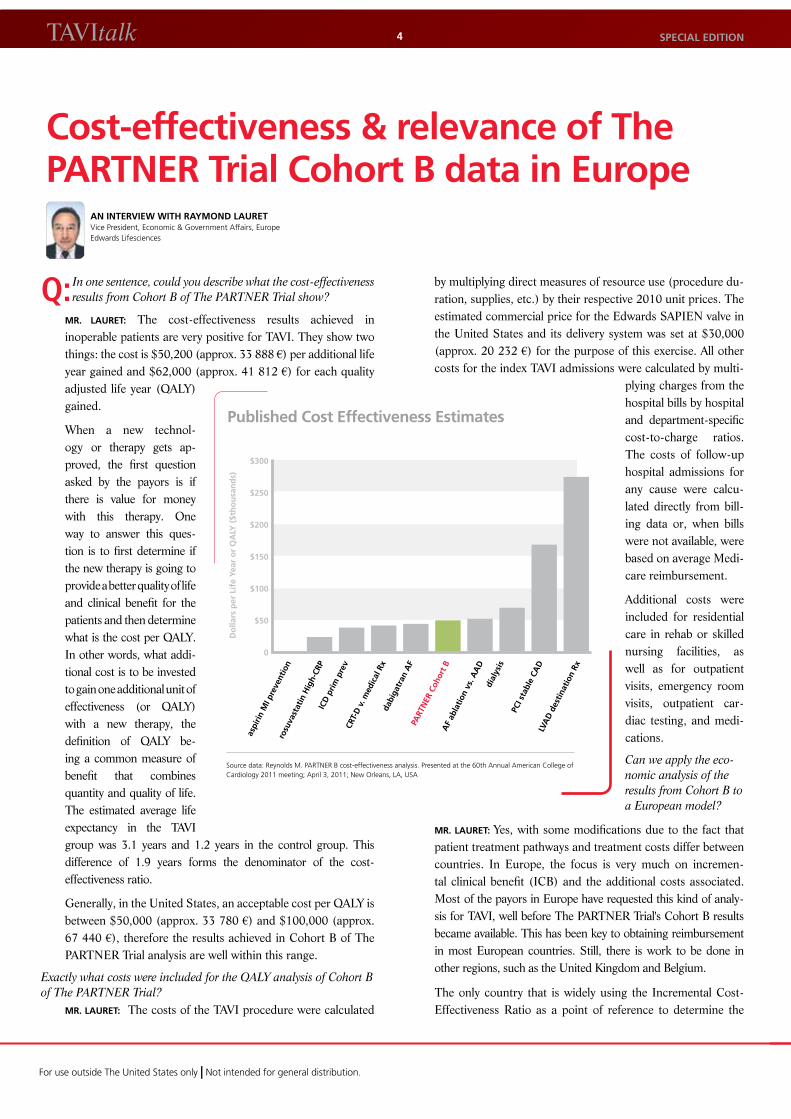
mr. laurET: The cost-effectiveness results achieved in inoperable patients are very positive for TAVI. They show two things: the cost is $50,200 (approx. 33 888 €) per additional life year gained and $62,000 (approx. 41 812 €) for each quality adjusted life year (QALY) gained.
When a new technol-ogy or therapy gets ap-proved, the first question asked by the payors is if there is value for money with this therapy. One way to answer this ques-tion is to first determine if the new therapy is going to provide a better quality of life and clinical benefit for the patients and then determine what is the cost per QALY. In other words, what addi-tional cost is to be invested to gain one additional unit of effectiveness (or QALY) with a new therapy, the definition of QALY be-ing a common measure of benefit that combines quantity and quality of life. The estimated average life expectancy in the TAVI group was 3.1 years and 1.2 years in the control group. This difference of 1.9 years forms the denominator of the cost- effectiveness ratio.
Generally, in the United States, an acceptable cost per QALY is between $50,000 (approx. 33 780 €) and $100,000 (approx. 67 440 €), therefore the results achieved in Cohort B of The PARTNER Trial analysis are well within this range.
Exactly what costs were included for the QALY analysis of Cohort B of The PARTNER Trial?
mr. laurET: The costs of the TAVI procedure were calculated
by multiplying direct measures of resource use (procedure du-ration, supplies, etc.) by their respective 2010 unit prices. The estimated commercial price for the Edwards SAPIEN valve in the United States and its delivery system was set at $30,000 (approx. 20 232 €) for the purpose of this exercise. All other costs for the index TAVI admissions were calculated by multi-
plying charges from the hospital bills by hospital and department-specific cost-to-charge ratios. The costs of follow-up hospital admissions for any cause were calcu-lated directly from bill-ing data or, when bills were not available, were based on average Medi-care reimbursement.
Additional costs were included for residential care in rehab or skilled nursing facilities, as well as for outpatient visits, emergency room visits, outpatient car-diac testing, and medi-cations.
Can we apply the eco-nomic analysis of the results from Cohort B to a European model?
mr. laurET: Yes, with some modifications due to the fact that patient treatment pathways and treatment costs differ between countries. In Europe, the focus is very much on incremen-tal clinical benefit (ICB) and the additional costs associated. Most of the payors in Europe have requested this kind of analy-sis for TAVI, well before The PARTNER Trial's Cohort B results became available. This has been key to obtaining reimbursement in most European countries. Still, there is work to be done in other regions, such as the United Kingdom and Belgium.
The only country that is widely using the Incremental Cost-Effectiveness Ratio as a point of reference to determine the
for use outside the united States only | not intended for general distribution.
TAVItalk 4
cost-effectiveness & relevance of The ParTnEr Trial cohort B data in Europe
an InTErvIEW WITh raYmonD laurETVice president, economic & government affairs, europe edwards lifesciences
Published cost Effectiveness Estimates
Source data: reynolds m. partner B cost-effectiveness analysis. presented at the 60th annual american college of cardiology 2011 meeting; april 3, 2011; new orleans, la, uSa
$300
$250
$200
$150
$100
$50
0
aspi
rin M
I pre
vent
ion
rosu
vast
atin
Hig
h-CR
PIC
D p
rim p
rev
CRT-
D v
. med
ical
Rx
dabi
gatr
an A
FPA
RTN
ER C
ohor
t BA
F ab
latio
n vs
. AA
Ddi
alys
is
PCI s
tabl
e CA
DLV
AD
des
tinat
ion
Rx
Do
llars
per
Lif
e Ye
ar o
r Q
ALY
($t
ho
usa
nd
s)
sPEcIal EDITIon
TAVItalkEuroPE 5
willingness to pay per QALY for a new therapy is the United Kingdom. The United Kingdom has an established practice of health care economics that has been refined over several years. They assess the threshold for cost per QALY at £30,000 (approx. 33 370 € or $49,481).
Does the Cohort B economic analysis of The PARTNER Trial have any usefulness for European reimbursement decisions?
mr. laurET: When working with the European reimbursement systems, we have been careful to point out that the $62,000
(approx. 41 000 €) is not directly transferable to the European health care systems for several reasons. The cost struc-tures in the United States and Europe are very different (e.g., physicians’ salaries, cost per
intensive care unit [ICU] day, etc.). You can still take the length of time in the ICU for the TAVI patients and apply the different cost structures. As an example, the cost per ICU day in the United States is in the region of $2,500 (approx. 1 686 €); in Europe, it is in the region of 1 000 € ($1,482).
We have used the clinical data obtained from Cohort B to populate our cost-effectiveness models using the various European cost structures. With these analyses, we will be able to assess the European cost-effectiveness of TAVI compared to inoperable patients.
How are European countries measuring quality of life?mr. laurET: In most countries, when you seek to obtain re-imbursement for a new product, the first thing that you have to do is to submit a dossier to the Health Technology Assess-ment (HTA) groups. There are different tools used by the assessors, such as a detailed questionnaire measuring quality-of-life index. These questions help assess patients’ quality of life by examining factors such as fatigue, limited mobility, whether they are house-bound, their ability to stand, or if they are out of breath, etc. Inoperable patients receiving TAVI are likely to have immediate clinical benefit as a result of improved haemo-dynamics. They will be far less dependent on supplemental care, enabling greater independence and ability to enjoy life.
note: all monetary conversions are approximate, based on exchange rates valid may 3–4, 2011.
Patient screening: be careful what you are extrapolating from
Matthew Reynolds, MD, when presenting these data at the ACC, pointed out several important limitations. First, Cohort B still represents early TAVI experience with the technology, procedure, and postoperative management in the United States. The efficiency of care and outcomes for patients may improve with time. Second, the medical management of the control patients in Cohort B may have differed from the care of similar patients in community practice. Final-ly, Cohort B was a uniquely old and inoperable patient population, and therefore these results cannot be extrapolated to other patient groups.
The analysis of the Cohort A data on high-risk patients with severe symptomatic aortic stenosis comparing TAVI to conventional aortic valve replacement is currently being reviewed and will be presented at a future meeting.
When evaluating patients with severe aortic stenosis, it is extremely important to review the multitude of options available—including surgery—and to refer them to a hospital where a multidisciplinary
Heart Team will review all the information. Managing patients and family expectations is key, as many patients will be better suited to surgical valve replacement—still the gold standard for patients with lower risk profiles. It is difficult for all concerned when a patient arrives with his/her heart set on TAVI and is not a suitable candidate.
TAVItalk
QUOTABLE
managing patient expectations is key
PIlar Tornos mas, mD, fEsc hospital general universitari Vall d’hebron, Barcelona, Spain former head of the european Society of cardiology's task force for the management of valvular heart disease
Inoperable patients receiving TAVI are likely to have immediate clinical benefit as a result of improved haemodynamics.

for use outside the united States only | not intended for general distribution.
TAVItalk 6
Q:What impact do you believe these data will have on TAVI?
A: I think cardiologists and surgeons will be convinced that we can use this approach in high-risk patients. This is very important because we can now offer either TAVI or AVR to these patients, and the team can make a decision regarding the optimal
approach for a given patient.
Q:Was there anything about the Cohort A data that stood out to you?
A: If we compare the stroke rates, it is higher in the TAVI group compared to aortic valve replacement group. This was a surprise for me because it is not the experience that we have in France, nor in other countries in Europe. Looking at the SOURCE
data, for example, there is no difference in terms of strokes between TAVI and surgery. Neurologic events were really captured in this study compared to other studies in Europe where the design was less rigorous than in The PARTNER Trial. This difference in terms of neurologic events is probably related to several things. The first is the learning curve. You need to master the technique to cross the aortic arch with the delivery system, being careful not to damage the internal or external parts of the arch where there is debris that can cause embolisation in the brain. Optimal anticoagulation during the procedure is also a very important issue, as well as the profile of the device, which is clearly better with the next generation valve currently available in Europe compared to The PARTNER Trial.
TAVItalk
QUOTABLE
learning curve in mastering the technique
ThIErrY lEfèvrE, mD, fEsc, fscaI institut cardiovasculaire paris Sud hôpital privé Jacques cartier massy, france
Given the enthusiasm around the favourable results of TAVI, as documented by both cohorts in The PARTNER Trial, as well as many other non-randomised studies, what is still unknown is the long-term durability of these new valves and if they will
parallel the long-term durability proven in surgical valves.*
In addition, the risk of minor and major neurological events associated with TAVI could be reduced with the use of smaller devices. Embolic protection systems may offer another level of risk reduction, especially in patients with severe calcification of the iliofemoral vessels and aortic arch.
The various risk scores for evaluating surgical candidacy are imperfect, and the lower-than-expected rate of 30-day mortality in patients treated with surgical AVR reported in Cohort A provide further evidence that risk scores may frequently overestimate the predicted surgical risk to the patients. This finding confirms the importance of patient selection in the multidisciplinary team decision-making process and the value of an experienced team. It is also noteworthy that the surgical results in Cohort A were truly exceptional and are a testament to the skill of the surgeons participating in this study.
The non-inferior results of TAVI compared to surgical AVR should be a strong incentive for surgeons to be fully involved in transcatheter procedures, as well as to optimise surgical treatment with new techniques and technologies to offer the best range of therapeutic options for AS patients.
TAVItalk
QUOTABLE
cohort a: a testament to surgical skill
oTTavIo alfIErI, mD professor and chairman of the Department of cardiac Surgery San raffaele university hospital milan, italy
*Seven-year thV durability data for one of pr. cribier’s early, very compromised patients, initially treated in September 2003, are on file in rouen, france. twenty year surgical valve data are available in the clinical communiqué 20 yr results (ar002835) on file at edwards llc.
sPEcIal EDITIon
Survival rates after the onset of symptoms in severe aortic
stenosis are dismal, as low as 50% at 2 years and 20% at
5 years.1 Surgical aortic valve replacement (AVR) is the cur-
rent standard of care, but it has been estimated that between
30% and 60% of patients do not undergo AVR.2,3
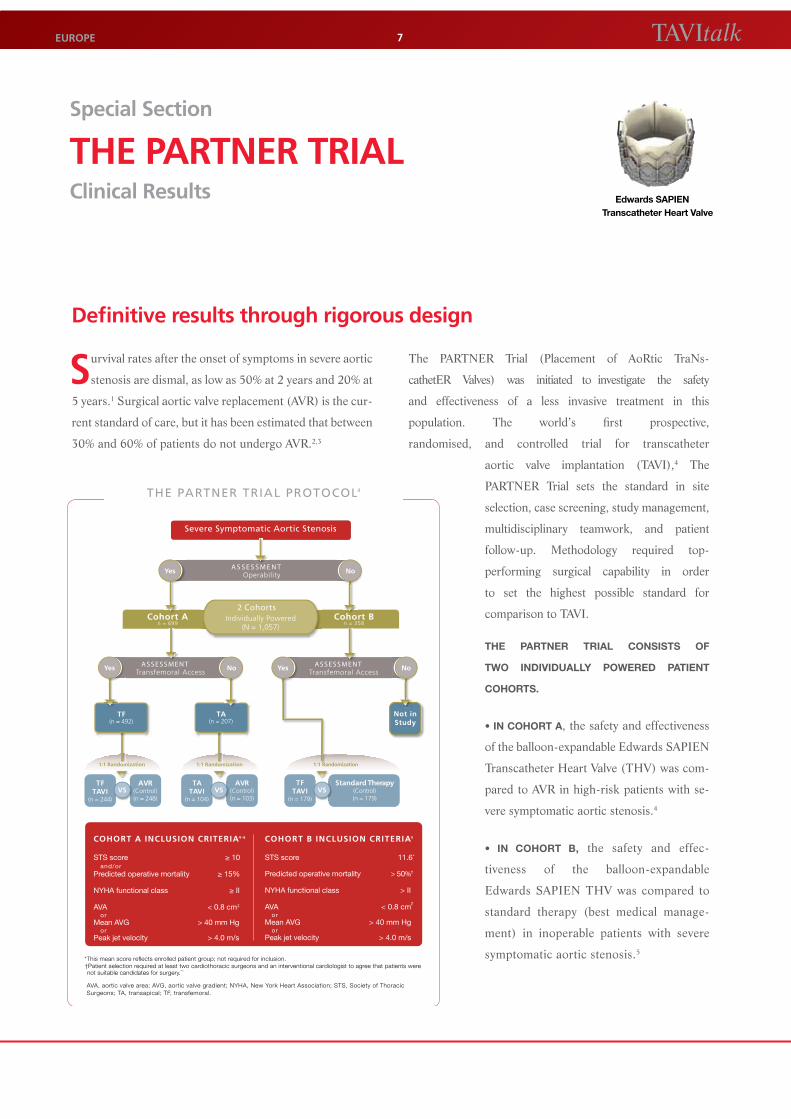
The PARTNER Trial (Placement of AoRtic TraNs-
cathetER Valves) was initiated to investigate the safety
and effectiveness of a less invasive treatment in this
population. The world’s first prospective,
randomised, and controlled trial for transcatheter
aortic valve implantation (TAVI),4 The
PARTNER Trial sets the standard in site
selection, case screening, study management,
multidisciplinary teamwork, and patient
follow-up. Methodology required top-
performing surgical capability in order
to set the highest possible standard for
comparison to TAVI.
THE PARTNER TRIAL cONSISTS Of
TWO INdIVIduALLy POWEREd PATIENT
cOHORTS.
• In Cohort A, the safety and effectiveness
of the balloon-expandable Edwards SAPIEN
Transcatheter Heart Valve (THV) was com-
pared to AVR in high-risk patients with se-
vere symptomatic aortic stenosis.4
• In Cohort B, the safety and effec-
tiveness of the balloon-expandable
Edwards SAPIEN THV was compared to
standard therapy (best medical manage-
ment) in inoperable patients with severe
symptomatic aortic stenosis.5
TAVItalkEuroPE 7
special section
ThE ParTnEr TrIalclinical results
Definitive results through rigorous design
Edwards SAPIEN Transcatheter Heart Valve
A S S E S S M E N TOperability NoYes
Severe Symptomatic Aortic Stenosis
Cohort An = 699
Cohort Bn = 358
2 Cohorts Individually Powered
(N = 1,057)
ASSESSMENTTransfemoral Access
NoYes NoYes ASSESSMENTTransfemoral Access
TF(n = 492)
TA(n = 207)
1:1 Randomization 1:1 Randomization
Not in Study
TFTAVI
(n = 244)
AVR(Control)(n = 248)
VSTF
TAVI(n = 179)
Standard Therapy (Control)(n = 179)
VSTA
TAVI(n = 104)
AVR(Control)(n = 103)
VS
1:1 Randomization
AVA, aortic valve area; AVG, aortic valve gradient; NYHA, New York Heart Association; STS, Society of Thoracic Surgeons; TA, transapical; TF, transfemoral.
THE PARTNER TRIAL PROTOCOL4
COHORT A INCLUSION CRITERIA4 - 6
STS score ≥ 10 and/orPredicted operative mortality ≥ 15%
NYHA functional class ≥ II
AVA < 0.8 cm2
orMean AVG > 40 mm Hg orPeak jet velocity > 4.0 m/s
COHORT B INCLUSION CRITERIA5
STS score 11.6*
Predicted operative mortality > 50%†
NYHA functional class > II
AVA < 0.8 cm2
orMean AVG > 40 mm Hg orPeak jet velocity > 4.0 m/s
*This mean score reflects enrolled patient group; not required for inclusion.†Patient selection required at least two cardiothoracic surgeons and an interventional cardiologist to agree that patients were
not suitable candidates for surgery.4,5
TAVItalk sPEcIal EDITIon8
for use outside the united States only | not intended for general distribution.
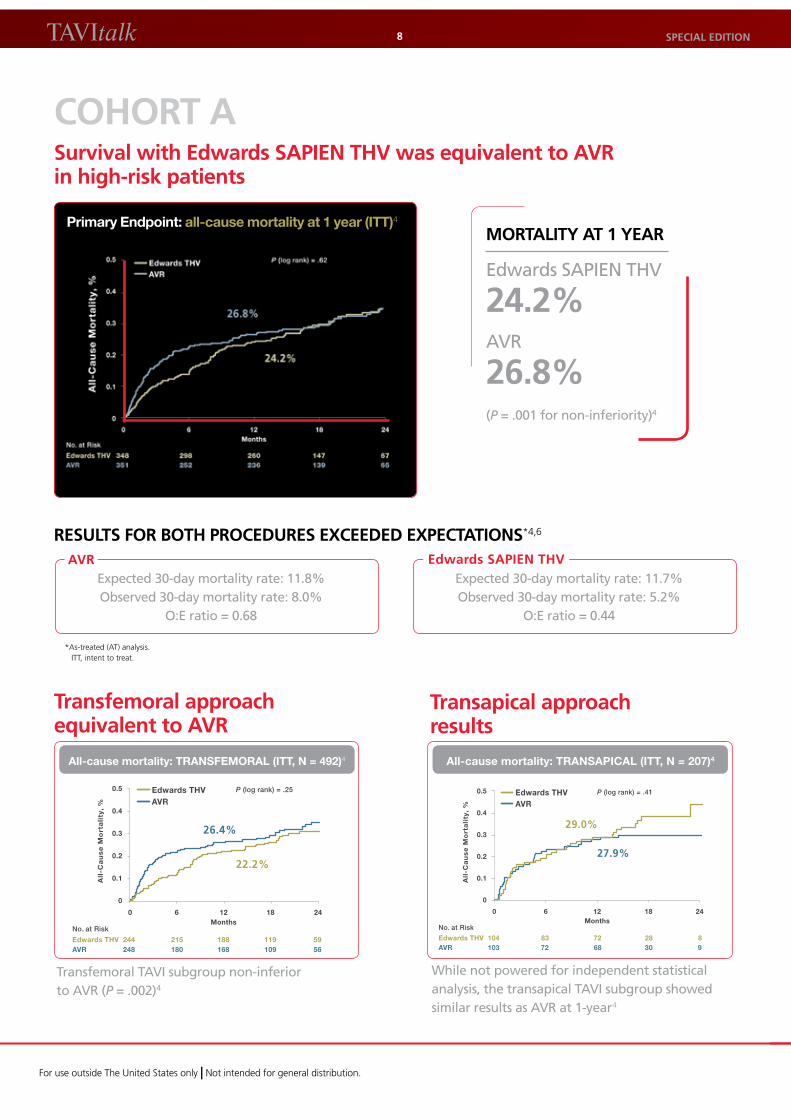
cohorT asurvival with Edwards saPIEn Thv was equivalent to avr in high-risk patients
Primary Endpoint: all-cause mortality at 1 year (ITT)4
morTalITY aT 1 YEar
Edwards SAPIEN THV
24.2%AVR
26.8%(P = .001 for non-inferiority)4
rEsulTs for BoTh ProcEDurEs ExcEEDED ExPEcTaTIons*4,6
All
-Ca
us
e M
ort
ali
ty,
%
0.5
0.4
0.3
0.2
0.1
0
No. at Risk
Edwards THV 104 83 72 28 8AVR 103 72 68 30 9
P (log rank) = .41Edwards THVAVR
29.0%
0 6 12 18 24 Months
27.9%
All-cause mortality: trAnSAPICAL (Itt, n = 207)4
All
-Ca
us
e M
ort
ali
ty,
%
0.5
0.4
0.3
0.2
0.1
0
No. at Risk
Edwards THV 244 215 188 119 59AVR 248 180 168 109 56
P (log rank) = .25Edwards THVAVR
26.4%
0 6 12 18 24 Months
22.2%
All-cause mortality: trAnSFEMorAL (Itt, n = 492)4
Transfemoral TAVI subgroup non-inferior to AVR (P = .002)4
While not powered for independent statistical analysis, the transapical TAVI subgroup showed similar results as AVR at 1-year4
*as-treated (at) analysis. itt, intent to treat.
Transfemoral approach equivalent to avr
Transapical approach results
Expected 30-day mortality rate: 11.8%Observed 30-day mortality rate: 8.0%
O:E ratio = 0.68
Expected 30-day mortality rate: 11.7%Observed 30-day mortality rate: 5.2%
O:E ratio = 0.44
avr Edwards saPIEn Thv
TAVItalkEuroPE 9
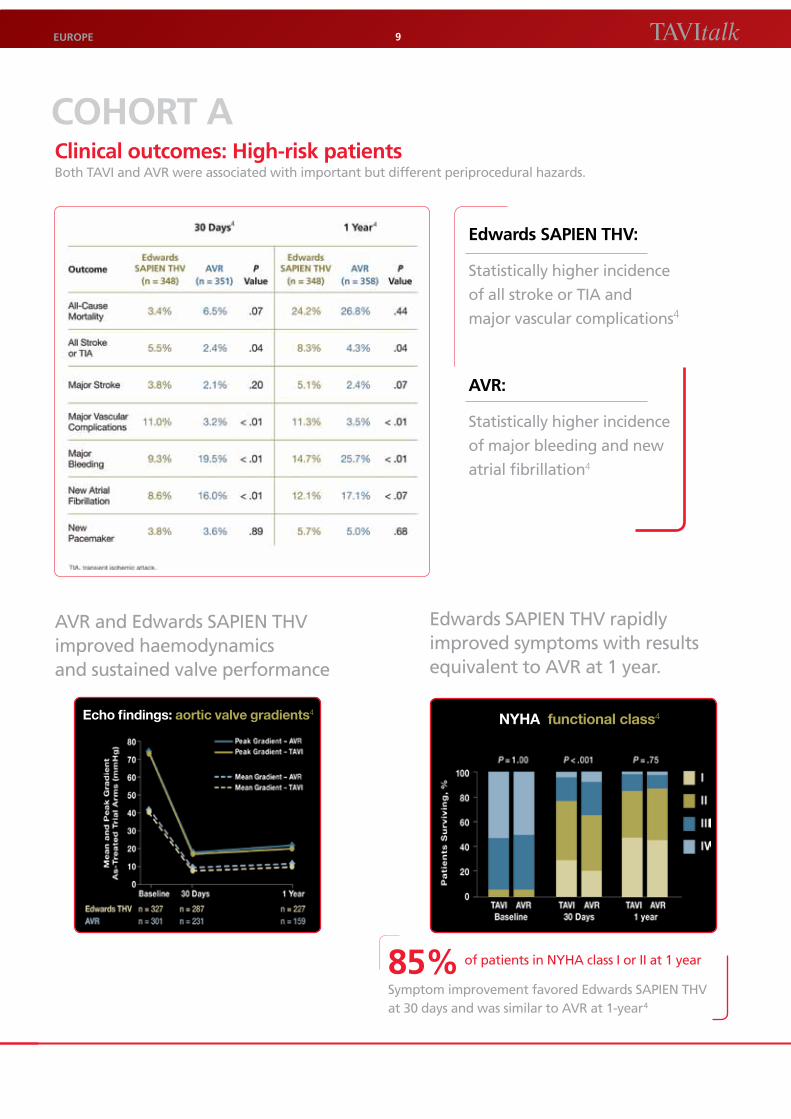
cohorT aclinical outcomes: high-risk patients Both TAVI and AVR were associated with important but different periprocedural hazards.
Edwards saPIEn Thv:
Statistically higher incidence
of all stroke or TIA and
major vascular complications4
avr:
Statistically higher incidence
of major bleeding and new
atrial fibrillation4
AVR and Edwards SAPIEN THV improved haemodynamics and sustained valve performance
Echo findings: aortic valve gradients4NyHA functional class4
Edwards SAPIEN THV rapidly improved symptoms with results equivalent to AVR at 1 year.
85% of patients in NYHA class I or II at 1 year
Symptom improvement favored Edwards SAPIEN THV at 30 days and was similar to AVR at 1-year4
references appear on p. 16.
for use outside the united States only | not intended for general distribution.
TAVItalk 10
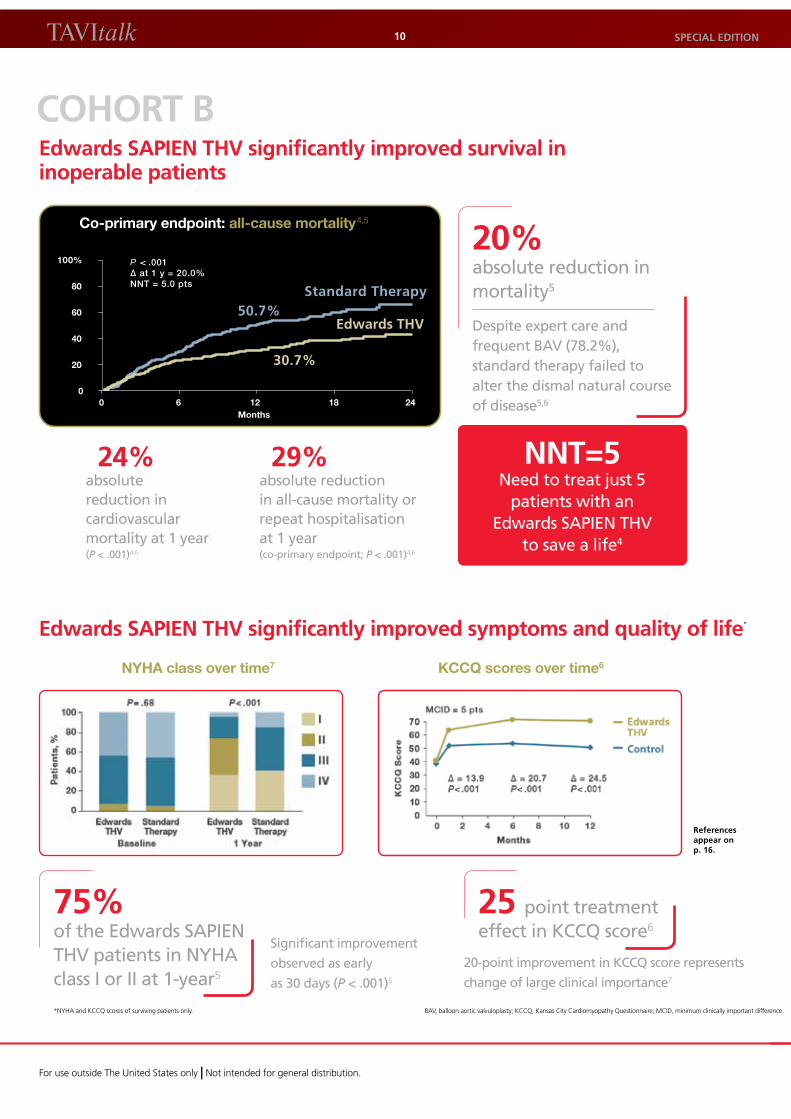
cohorT BEdwards saPIEn Thv significantly improved survival in inoperable patients
Months
100%
80
60
40
20
00 6 12 18 24
P < .001∆ at 1 y = 20.0%NNT = 5.0 pts
Standard Therapy
Edwards THV
30.7%
50.7%
co-primary endpoint: all-cause mortality4,5
20% absolute reduction in mortality5
Despite expert care and frequent BAV (78.2%), standard therapy failed to alter the dismal natural course of disease5,6
24% absolute reduction in cardiovascular mortality at 1 year (P < .001)4,6
29% absolute reduction in all-cause mortality or repeat hospitalisation at 1 year (co-primary endpoint; P < .001)4,6
nnT=5 Need to treat just 5
patients with an Edwards SAPIEN THV
to save a life4
Edwards saPIEn Thv significantly improved symptoms and quality of life*
NyHA class over time7 KccQ scores over time6
75% of the Edwards SAPIEN THV patients in NYHA class I or II at 1-year5
25 point treatment effect in KCCQ score6
Significant improvement
observed as early
as 30 days (P < .001)5
20-point improvement in KCCQ score represents
change of large clinical importance7
sPEcIal EDITIon
*nyha and KccQ scores of surviving patients only. BaV, balloon aortic valvuloplasty; KccQ, Kansas city cardiomyopathy Questionnaire; mciD, minimum clinically important difference.

TAVItalkEuroPE 11
Cohort B of The PARTNER Trial demonstrated that TAVI, using the Edwards SAPIEN valve, achieves a 20% reduction mortality in patients with severe aortic stenosis who are inoperable. Cohort A of The PARTNER Trial demonstrated similar outcomes in
high-risk patients with severe aortic stenosis, whether they underwent conventional surgery or TAVI, but the positive quality-of-life impact was faster with TAVI.
If a patient has aortic stenosis that is considered to be inoperable and you want to increase that patient’s chance of survival in a bet-ter clinical condition, TAVI is the best choice. In addition, patients with aortic stenosis at high risk for surgery can be treated either with surgery to replace their damaged valve, or they can have a TAVI. Both treatments are excellent options for severe aortic stenosis. However, if the patient wants to be restored to a normal activity level in a shorter time, they should undergo TAVI.
TAVI increases the chance of survival if the patient is inoperable.
TAVItalk
QUOTABLE
The advantages of reduced recovery time
EuloGIo GarcIa, mD instituto cardiovascular hospital clinico San carlos madrid, Spain
Q: What are your thoughts regarding The PARTNER Trial Cohort A data?
A:These data are excellent and are of paramount importance for medical history, the history of our patients, as well as the physicians who treat aortic stenosis because this is the first randomised trial comparing a new therapeutic option (TAVI)
with the established surgical valve replacement in patients defined as being at high risk for surgery. The global results of both arms of the trial seem not simply good, but excellent. The investigators of The PARTNER Trial did a very good job in treating these high-risk patients. In the real world, patients at high risk for surgery with aortic stenosis usually are very old, very fragile, and have a lot of comorbidities. To obtain low mortality, 3% or 6%, at 30 days in these kinds of patients is exceptional.
TAVItalk
QUOTABLE
low mortality in both groups was ‘exceptional’
JoEllE kEfEr, mD, PhD Division of cardiology cliniques universitaires Saint-luc université catholique de louvain Brussels, Belgium
These extraordinary results were accomplished because of an unprecedented teamwork between a cardiologist, cardiac surgeon, and the associated caregivers.
TAVItalk
QUOTABLE
unprecedented teamwork
E. muraT Tuzcu, mD Vice chair for clinical operations Department: cardiovascular medicine cleveland clinic cleveland, oh uSa
for use outside the united States only | not intended for general distribution.
TAVItalk 12
Q: What are your thoughts regarding The PARTNER Trial Cohort A data?
A:The most remarkable thing was the performance of the multidisciplinary TAVI and surgical teams. These are the best reported results for transcatheter valve implantation. For 19 of the 26 centres to be doing their first cases within the trial
and yet still achieve a 30-day transfemoral mortality of only 3.7% is absolutely remarkable. It should be noted that both the transapical and surgical AVR mortality are remarkably low. Surgeons did brilliantly because, there is no doubt that, this was a very high-risk group of patients.
TAVItalk
QUOTABLE
a ‘remarkable’ performance in a high-risk group of patients
marTYn Thomas, mD clinical Director of cardiovascular Services guys and St. thomas’ hospital london, united Kingdom
My first take on the data is very positive. I think it’s very encouraging because we are looking at two procedures–a well-known, proven technology that has been around for more than 50 years and we are comparing it with a
technology that has had less than 10 years since first-in-man (FIM) and less than 5 years in a “real world” post-commercial setting. Essentially, we are testing, in a randomised way, a therapy that is on the steepest part of its learn-ing curve using a first-generation device, and comparing it with a very mature, sophisticated, surgical option that is probably at the plateau of its learning curve for the therapy. The results are encouraging and suggest a very bright future for the TAVI technology.
TAVItalk
QUOTABLE
Even with a steep learning curve, TavI measures up to avr
Ian T. mErEDITh, mBBs, PhD, fracP, facc, fscaI monashheart monash medical centre melbourne, australia
This is the ideal opportunity, because surgical AVR is one of the most effective operations surgeons offer, and TAVR is the most exciting new treatment for aortic stenosis in the past two to three decades. This opens up a new set of patients who may very well
benefit as much by TAVR as by the conventional gold standard surgery.
TAVItalk
QUOTABLE
Ideal opportunity to compare Tavr to the gold standard
craIG r. smITh, mD chief, Division of cardiothoracic Surgery new york-presbyterian hospital, columbia university medical center new york, ny uSa co-principal investigator of the partner trial
sPEcIal EDITIon

TAVItalkEuroPE 13
On the basis of a rate of death from any cause at 1-year that was 20 percentage points lower with TAVI than with standard therapy, balloon-expandable TAVI should be the new standard of care for patients with aortic stenosis who are not suit-
able candidates for surgery.
TAVItalk
QUOTABLE
a lower rate of death from any cause at 1-year
ThE ParTnEr TrIal InvEsTIGaTors transcatheter aortic-Valve implantation for aortic Stenosis in patients Who cannot undergo Surgery N Engl J Med. oct 2010.
We have clearly learned from The PARTNER Trial that, in our most difficult to treat aortic stenosis patients, TAVR is both the new standard-of-care for inoperable patients and an exciting alternative for carefully selected high-risk patients.
Based upon the results from the inoperable and high-risk patient cohorts in The PARTNER Trial, balloon-expandable TAVR is now an invaluable new therapy to optimally manage our most difficult aortic stenosis patients.
TAVItalk
QUOTABLE
a clear lesson for the most difficult-to-treat as patients
marTIn lEon, mD associate Director of the cardiovascular interventional therapy (ciVt) program new york-presbyterian hospital, columbia university medical center professor of medicine, columbia university college of physicians and Surgeons new york ny uSa co-principal investigator of the partner trial
The PARTNER Trial, Cohort B, is a landmark trial in the field of valvular heart disease. It is not only a major step in the evaluation of TAVI, but it is also the first study justifying—with a high level of evidence—the
treatment of severe, symptomatic aortic stenosis in high-risk elderly patients. In a paper from the Euro Heart Survey highlighting the insufficient referral of elderly patients with aortic stenosis, we concluded in 2005, “These findings underline particular difficulties regarding decision-making in the elderly, in whom current guidelines provide limited recommendations as a consequence of the low level of evidence from the literature. Randomised trials are unlikely to be conducted in this field…”
This was before TAVI gained wide application, and it illustrates how the evaluation of a new technique may con-tribute to addressing complex existing issues. There is no doubt that TAVI widens the field of effective therapies in high-risk patients with aortic stenosis. We now have proof of its usefulness in patients who were likely to be undertreated. Given new evidence from The PARTNER Trial, it can be expected that practitioners will become more interested in referring high-risk patients with aortic stenosis.
TAVItalk
QUOTABLE
‘Widening the field of effective therapies in high-risk patients with aortic stenosis’
BErnarD IunG, mD, PhD chairman, european Society of cardiology, Working group on Valve Disease cardiology Department, Bichat hospital and paris 7 university paris, france
TAVItalk sPEcIal EDITIon14
for use outside the united States only | not intended for general distribution.
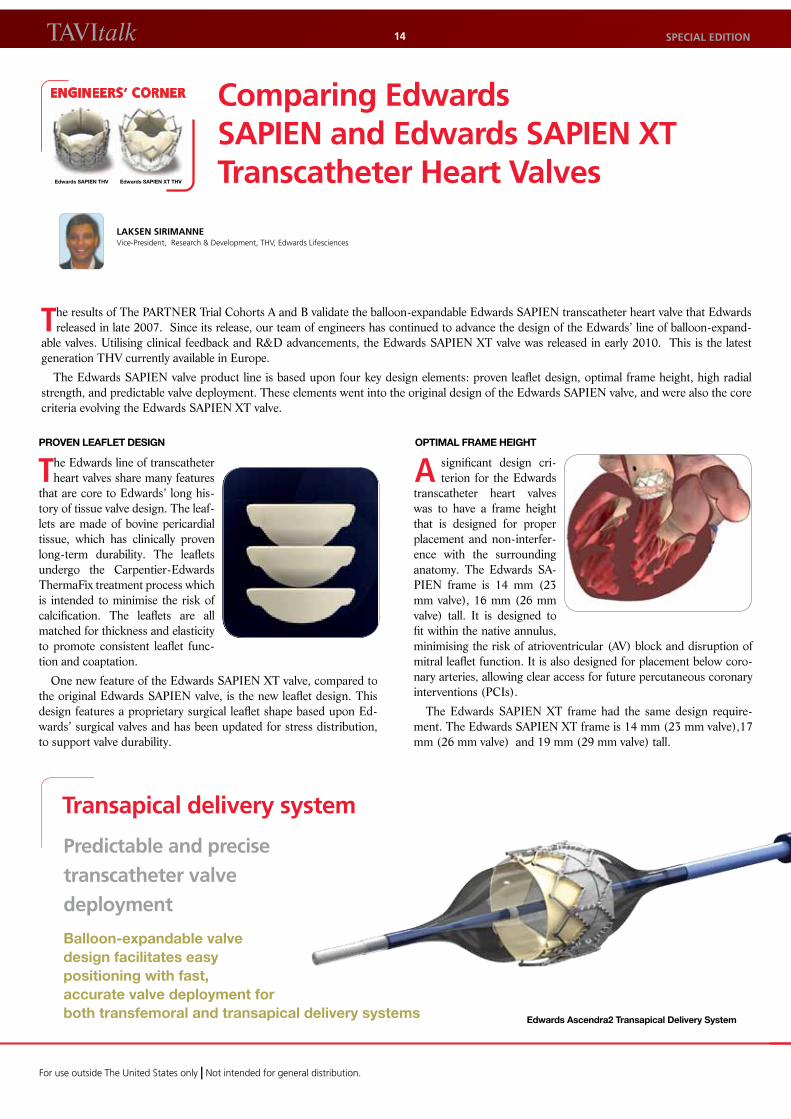
OPTIMAL fRAME HEIgHT
A significant design cri-terion for the Edwards
transcatheter heart valves was to have a frame height that is designed for proper placement and non-interfer-ence with the surrounding anatomy. The Edwards SA-PIEN frame is 14 mm (23 mm valve), 16 mm (26 mm valve) tall. It is designed to fit within the native annulus, minimising the risk of atrioventricular (AV) block and disruption of mitral leaflet function. It is also designed for placement below coro-nary arteries, allowing clear access for future percutaneous coronary interventions (PCIs).
The Edwards SAPIEN XT frame had the same design require-ment. The Edwards SAPIEN XT frame is 14 mm (23 mm valve),17 mm (26 mm valve) and 19 mm (29 mm valve) tall.
ENGINEERS’ CORNER
Edwards SAPIEN THV Edwards SAPIEN XT THV
comparing Edwards saPIEn and Edwards saPIEn xT Transcatheter heart valves
The results of The PARTNER Trial Cohorts A and B validate the balloon-expandable Edwards SAPIEN transcatheter heart valve that Edwards released in late 2007. Since its release, our team of engineers has continued to advance the design of the Edwards’ line of balloon-expand-
able valves. Utilising clinical feedback and R&D advancements, the Edwards SAPIEN XT valve was released in early 2010. This is the latest generation THV currently available in Europe.
The Edwards SAPIEN valve product line is based upon four key design elements: proven leaflet design, optimal frame height, high radial strength, and predictable valve deployment. These elements went into the original design of the Edwards SAPIEN valve, and were also the core criteria evolving the Edwards SAPIEN XT valve.
PROVEN LEAfLET dESIgN
The Edwards line of transcatheter heart valves share many features
that are core to Edwards’ long his-tory of tissue valve design. The leaf-lets are made of bovine pericardial tissue, which has clinically proven long-term durability. The leaflets undergo the Carpentier-Edwards ThermaFix treatment process which is intended to minimise the risk of calcification. The leaflets are all matched for thickness and elasticity to promote consistent leaflet func-tion and coaptation.
One new feature of the Edwards SAPIEN XT valve, compared to the original Edwards SAPIEN valve, is the new leaflet design. This design features a proprietary surgical leaflet shape based upon Ed-wards’ surgical valves and has been updated for stress distribution, to support valve durability.
laksEn sIrImannE Vice-president, research & Development, thV, edwards lifesciences
Transapical delivery system
Predictable and precise transcatheter valve deployment
Edwards Ascendra2 transapical Delivery System
Balloon-expandable valve design facilitates easy positioning with fast, accurate valve deployment for both transfemoral and transapical delivery systems
TAVItalkEuroPE 15
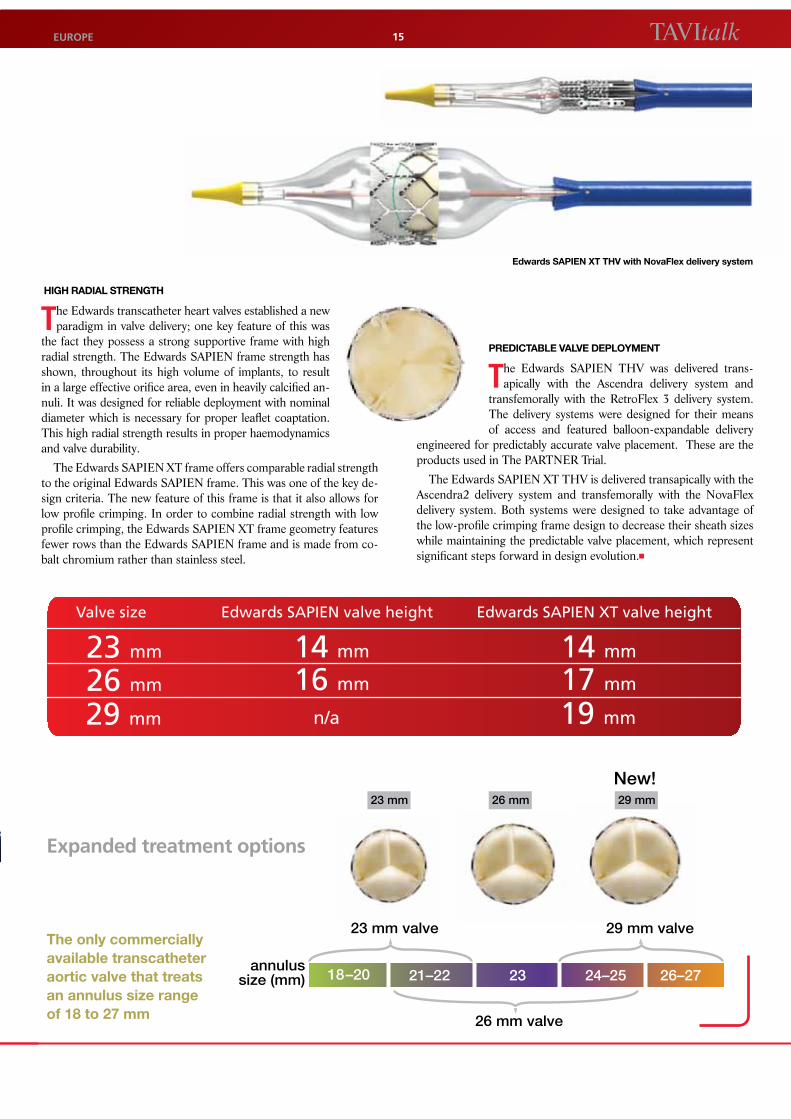
HIgH RAdIAL STRENgTH
The Edwards transcatheter heart valves established a new paradigm in valve delivery; one key feature of this was
the fact they possess a strong supportive frame with high radial strength. The Edwards SAPIEN frame strength has shown, throughout its high volume of implants, to result in a large effective orifice area, even in heavily calcified an-nuli. It was designed for reliable deployment with nominal diameter which is necessary for proper leaflet coaptation. This high radial strength results in proper haemodynamics and valve durability.
The Edwards SAPIEN XT frame offers comparable radial strength to the original Edwards SAPIEN frame. This was one of the key de-sign criteria. The new feature of this frame is that it also allows for low profile crimping. In order to combine radial strength with low profile crimping, the Edwards SAPIEN XT frame geometry features fewer rows than the Edwards SAPIEN frame and is made from co-balt chromium rather than stainless steel.
PrEDICtABLE vALvE DEPLoyMEnt
The Edwards SAPIEN THV was delivered trans-apically with the Ascendra delivery system and
transfemorally with the RetroFlex 3 delivery system. The delivery systems were designed for their means of access and featured balloon-expandable delivery
engineered for predictably accurate valve placement. These are the products used in The PARTNER Trial.
The Edwards SAPIEN XT THV is delivered transapically with the Ascendra2 delivery system and transfemorally with the NovaFlex delivery system. Both systems were designed to take advantage of the low-profile crimping frame design to decrease their sheath sizes while maintaining the predictable valve placement, which represent significant steps forward in design evolution.
Valve size Edwards SAPIEN valve height Edwards SAPIEN XT valve height
23 mm
26 mm
14 mm
16 mm
14 mm
17 mm
29 mm n/a 19 mm
annulussize (mm) 18–20 21–22 23 24–25 26–27
23 mm valve 29 mm valve
26 mm valve
23 mm 26 mm 29 mm
New!
Edwards SAPIEN XT THV with Novaflex delivery system
Expanded treatment options
The only commercially available transcatheter aortic valve that treats an annulus size range of 18 to 27 mm
Edwards lifesciences irvine, uSa i nyon, Switzerland i tokyo, Japan i Singapore, Singapore i São paulo, Brazil edwards.com
1. otto cm. timing of aortic valve surgery. Heart. 2000;84:211-218. 2. iung B, Baron g, Butchart eg, et al. a prospective survey of patients with valvular heart disease
in europe: the euro heart Survey on Valvular heart Disease. Eur Heart J. 2003;24:1231-1243.3. charlson e, legedza at, hamel mB. Decision-making and outcomes in severe symptomatic aortic
stenosis. J Heart Valve Dis. 2006;15:312-321.4. Smith, cr. transcatheter vs surgical aortic valve replacement in high risk patients with severe
aortic stenosis: results from the partner trial. presented at: 2011 american college of
cardiology annual Scientific Session; april 2, 2011; new orleans, la.5. leon mB, Smith cr, mack m, et al. transcatheter aortic-valve implantation for aortic stenosis in
patients who cannot undergo surgery. N Engl J Med. 2010;363;1597-1607.6. Data on file, edwards lifesciences.7. KccQ interpretability. cardiovascular outcomes inc. http://cvoutcomes.org/pages/3217.
accessed may 3, 2011.
references
TAVItalk sPEcIal EDITIon | EuroPE16
In an editorial titled ‘Trials, Triumphs and Tribulations,’ Dr. King gave his perspective of The PARTNER Trial Cohort B and mentioned that there were ‘no surprises’ and that ‘a positive trial was anticipated, the magnitude of which did not disappoint.’ Dr.
King went on to say that ‘these patients were so high-risk that they were turned down for surgery by some of the country’s best sur-geons’ and that ‘it is difficult to find a group of patients with any disease who have a 50% 1-year mortality rate, which was the fate of Cohort B patients randomised to medical therapy in The PARTNER Trial. There is no longer any such thing as an untreatable patient with terminal aortic stenosis…The valve, as futuristic as it may have seemed 2 to 3 years ago, is not viewed as a pipe dream but as a reality. Our European colleagues have implanted over 20,000 aortic valves with results that convinced us that the valves worked.’
TAVItalk
QUOTABLE
‘a positive trial...[that] did not disappoint.’
sPEncEr B. kInG III, mD, facc president, St. Joseph’s heart & Vascular institute, atlanta, ga uSa professor of medicine emeritus, emory university School of medicine, atlanta, ga uSa editor-in-chief, Jacc: cardiovascular interventions
from “the partner trial cohort B” JACC Vol. 3, no. 11, 2010
The Edwards SAPIEN and SAPIEN XT transcatheter heart valve and delivery systems bearing the CE conformity marking comply with the requirements of the European Medical Device Directive 93/42/EEC.
Caution: Not intended for US distribution.
Edwards is a trademark of Edwards Lifesciences Corporation. Edwards Lifesciences, the stylized E logo, The stylized Edwards logo, Edwards SAPIEN, Edwards SAPIEN XT, TRAVERCE, PARTNER, PARTNER II, PREMIER, Ascendra2, NovaFlex and RetroFlex 3 are trademarks of Edwards Lifesciences Corporation and registered in the United States Patent and Trademark Office.
Edwards Lifesciences, S.A. Route de l’Etraz 70, 1260 Nyon, Switzerland Tel: +41 22 787 4362.
Additional company information can be found at http://www.edwards.com
TAVItalk
PUBLISHER: Edwards Lifesciences, S.A., Europe EDITORIAL AND DESIGN SERVICES: SAVIpartners, Paris and New York CONTACT INfORmATION: For general information on the Edwards TAVI Programme, please contact [email protected]
E2055/05-11/THV
For professional use. For additional information, indications, contraindications, warnings, precau-tions and adverse events, please refer to the Instructions For Use provided with the products.
COmPANy AND PRODUCT INfORmATION
The ‘nautilus’: Edwards’ clinical history of TavI
The ‘Nautilus” depicts the evolution and momentum of the
Edwards Lifesciences global clinical research program for TAVI. In 2010, the results of TRAVERCE, PARTNER EU, The SOURCE Registry, and The PARTNER Trial were all published in peer-reviewed journals. Each study and manuscript reflects upon unique aspects of the TAVI experience, from feasibility through randomised controlled pivotal trials, as well as extensive postmarket surveillance of real-world practice.
Our commitment to continued leadership in clinical research is unwavering. In 2011, we initiated enrolment in four new trials (SOURCE XT,
PREMIER [pulmonic] Registry, The PARTNER II Trial, and a Valve-in-Valve
study)*, as well as continued follow-up and publication of results from all of the trials previously reported.
We wish to thank all of our investigators and scientific collaborators, including
statisticians, clinical event adjudicators, core laboratories, and thought leaders, for
their collective expertise and contributions to these important programs.
JoDI akInVice president, global clinical affairs
edwards lifesciences
* Data on file at edwards lifesciences llc