spondyloarthropathies: using presentation to make the
TRANSCRIPT

184 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004
REVIEW
PONDYLITIS IS EASY TO MISS and is oftenjust assumed to be “back pain.” Physicians
should suspect a spondyloarthropathy in ayoung man or woman with morning stiffnesslasting more than 30 minutes; or in a patientwho has back pain and a history of uveitis, pso-riasis, or inflammatory bowel disease; or in apatient with back pain that improves dramati-cally when the patient takes prednisone or anonsteroidal anti-inflammatory drug (NSAID)for another reason.
Spondyloarthropathy is a family of arthri-tides that includes:• Ankylosing spondylitis• Reactive arthritis (including Reiter syn-
drome)• Psoriatic arthritis• Enteropathic spondyloarthropathy (ie,
spondyloarthropathy associated withinflammatory bowel disease)
• Undifferentiated spondyloarthropathy(forms that fail to meet the clinical crite-ria for the other categories).1The spondyloarthropathies are linked by
association with the class 1 human leukocyteantigen (HLA)-B27 and by a common clini-copathologic lesion—enthesitis.
There is no serologic test to aid in thediagnosis. Rather, the diagnosis is made byanalyzing a constellation of factors, such asaxial and peripheral joint and skeletal involve-ment, associated clinical features, and geneticpredisposing factors.2
Treatment has been focused on the relief ofsymptoms with drugs such as nonsteroidal anti-inflammatory drugs. The new tumor necrosisfactor inhibitors may have a role in modifyingthe course of this family of conditions, but expe-rience with these drugs is limited.
SIWAT KIRATISEAVEE, MDDepartment of Medicine, Albert EinsteinMedical Center, Philadelphia, Pa
LAWRENCE H. BRENTDepartment of Medicine, Albert EinsteinMedical Center, Philadelphia, Pa
Spondyloarthropathies: Usingpresentation to make the diagnosis■ ABSTRACT
Diagnosing the spondyloarthropathies—chronicinflammatory diseases of the spine and peripheral jointsthat share several distinctive features—is challenging anddepends on careful evaluation of the history, physicalexamination, and radiographs. The recent use of tumornecrosis factor inhibitors is exciting and may representtrue disease-modifying drugs for these conditions.
■ KEY POINTS
Common features of the spondyloathropathies areenthesitis of the axial and peripheral skeleton andvariable involvement of the peripheral joints, gut, skin,eye, or aorta.
Human leukocyte antigen B27 is strongly associated withspondyloarthropathy but is not a diagnostic test.
Serologic tests for rheumatoid factor and antinuclearantibody are usually negative in patients with aspondyloarthropathy. The erythrocyte sedimentationrate and the C-reactive protein concentration are oftenelevated, but elevations do not always correlate withdisease activity.
Tumor necrosis factor inhibitors have recently beenapproved for the treatment of spondyloarthropathy andmay have disease-modifying effects. Clinical experiencewith these drugs in patients with spondyloarthropathieshas been limited, but quite positive.
S
This paper discusses therapies that are experimental or are not approved by the US Food andDrug Administration for the use under discussion.
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004 185
Geneticimmunologic,andenvironmentalfactors appearto worktogether inspondylo-arthropathies
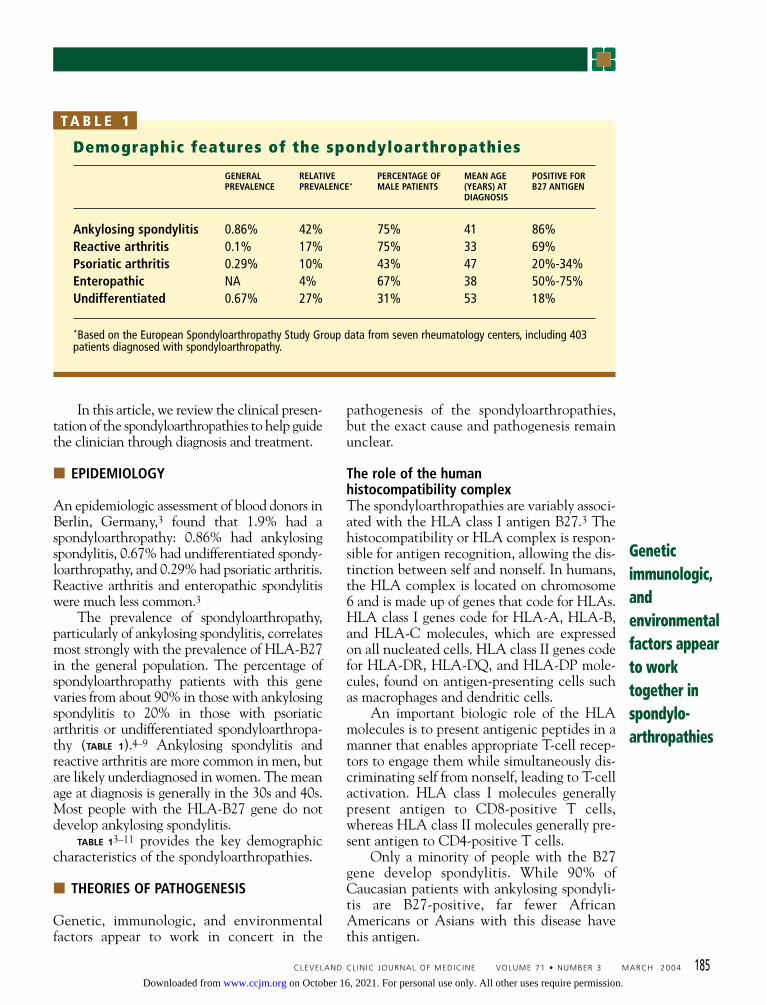
Demographic features of the spondyloarthropathies
GENERAL RELATIVE PERCENTAGE OF MEAN AGE POSITIVE FORPREVALENCE PREVALENCE* MALE PATIENTS (YEARS) AT B27 ANTIGEN
DIAGNOSIS
Ankylosing spondylitis 0.86% 42% 75% 41 86%Reactive arthritis 0.1% 17% 75% 33 69%Psoriatic arthritis 0.29% 10% 43% 47 20%-34%Enteropathic NA 4% 67% 38 50%-75%Undifferentiated 0.67% 27% 31% 53 18%
*Based on the European Spondyloarthropathy Study Group data from seven rheumatology centers, including 403patients diagnosed with spondyloarthropathy.
T A B L E 1
In this article, we review the clinical presen-tation of the spondyloarthropathies to help guidethe clinician through diagnosis and treatment.
■ EPIDEMIOLOGY
An epidemiologic assessment of blood donors inBerlin, Germany,3 found that 1.9% had aspondyloarthropathy: 0.86% had ankylosingspondylitis, 0.67% had undifferentiated spondy-loarthropathy, and 0.29% had psoriatic arthritis.Reactive arthritis and enteropathic spondylitiswere much less common.3
The prevalence of spondyloarthropathy,particularly of ankylosing spondylitis, correlatesmost strongly with the prevalence of HLA-B27in the general population. The percentage ofspondyloarthropathy patients with this genevaries from about 90% in those with ankylosingspondylitis to 20% in those with psoriaticarthritis or undifferentiated spondyloarthropa-thy (TABLE 1).4–9 Ankylosing spondylitis andreactive arthritis are more common in men, butare likely underdiagnosed in women. The meanage at diagnosis is generally in the 30s and 40s.Most people with the HLA-B27 gene do notdevelop ankylosing spondylitis.
TABLE 13–11 provides the key demographiccharacteristics of the spondyloarthropathies.
■ THEORIES OF PATHOGENESIS
Genetic, immunologic, and environmentalfactors appear to work in concert in the
pathogenesis of the spondyloarthropathies,but the exact cause and pathogenesis remainunclear.
The role of the humanhistocompatibility complexThe spondyloarthropathies are variably associ-ated with the HLA class I antigen B27.3 Thehistocompatibility or HLA complex is respon-sible for antigen recognition, allowing the dis-tinction between self and nonself. In humans,the HLA complex is located on chromosome6 and is made up of genes that code for HLAs.HLA class I genes code for HLA-A, HLA-B,and HLA-C molecules, which are expressedon all nucleated cells. HLA class II genes codefor HLA-DR, HLA-DQ, and HLA-DP mole-cules, found on antigen-presenting cells suchas macrophages and dendritic cells.
An important biologic role of the HLAmolecules is to present antigenic peptides in amanner that enables appropriate T-cell recep-tors to engage them while simultaneously dis-criminating self from nonself, leading to T-cellactivation. HLA class I molecules generallypresent antigen to CD8-positive T cells,whereas HLA class II molecules generally pre-sent antigen to CD4-positive T cells.
Only a minority of people with the B27gene develop spondylitis. While 90% ofCaucasian patients with ankylosing spondyli-tis are B27-positive, far fewer AfricanAmericans or Asians with this disease havethis antigen.
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

Molecular mimicryand an environmental stimulusThe shared amino acid sequence between theantigen-binding region of HLA B*2705 andnitrogenase from Klebsiella pneumoniae sup-ports molecular mimicry as a possible mecha-nism for the induction of spondyloarthropathyin genetically susceptible hosts by an environ-mental stimulus, such as bacteria in the gas-trointestinal tract.12 Another possible mecha-nism is presentation of an arthritogenic pep-tide from enteric bacteria by specific HLAmolecules. Many patients with ankylosingspondylitis have subclinical gastrointestinaltract inflammation and elevated serumimmunoglobulin A antibodies directed againstKlebsiella. The bacteria may invade the gas-trointestinal tract of a genetically susceptiblehost, leading to chronic inflammation andincreased permeability. Over time, bacterialantigens containing arthritogenic peptidesenter the blood stream. Bacterial antigens arethought to play a role in the pathogenesis ofreactive arthritis.13 Further studies are neededto establish their exact role in the pathogene-sis of reactive arthritis and related arthritides.Experimental work with transgenic mice andrats transfected with human HLA-B27 andbeta-2-microglobulin has shown that certainstrains develop a multisystemic illness resem-bling spondyloarthropathy, whereas identicalanimals raised in a germ-free environmentremain healthy.14,15
■ CLASSIFICATION AND DIAGNOSIS
The system most commonly used to classifyspondyloarthropathies for diagnostic purpos-es10 is the European SpondyloarthropathyStudy Group (ESSG) criteria,10 which have asensitivity of 83.5% and a specificity of 95.2%.Diagnosis is based on the presence of one oftwo major criteria (inflammatory spinal painor synovitis) plus one or more of the following:• Positive family history of ankylosingspondylitis, psoriasis, acute uveitis, reactivearthritis, or inflammatory bowel disease (alllinked to the presence of B27 and spondylitis)• Psoriasis• Inflammatory bowel disease• Urethritis, cervicitis, or acute diarrhea
less than 1 month before arthritis
• Alternating buttock pain• Enthesitis• Sacroiliitis.
According to the Amor criteria,16 whichare less commonly used, the diagnosis is basedon a total score derived from consideration of12 weighted criteria, which include history,clinical presentation, radiologic findings,genetic background, and response to treat-ment. This method is less convenient thanthe ESSG criteria. Its rates of sensitivity(90.8%) and specificity (96.2%) are statisti-cally comparable to those of the ESSGmethod.17
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004 189
The ESSGcriteria arecommonlyused tofacilitatethe diagnosis
Common features of thespondyloarthropathies
Inflammatory back painMorning stiffness that is reducedwith activity
Peripheral arthritisTypically asymmetric, occurringpredominantly in the lower limbs
EnthesitisAchilles tendon insertionPlantar fascia insertion on calcaneusPatella, superior and inferior aspectsTibial tuberosityMetatarsal headsBase of fifth metatarsal jointIliac spine, iliac crestIschial tuberosityTarsal regionGreater trochanterLateral epicondyleDistal scapulaDistal ulna
Dactylitis
Radiographic evidence of reactiveproliferation of new bone at the siteof enthesitis
Radiographic sacroiliitis
Characteristic extra-articular features(eg, anterior uveitis)
Significant family history
Presence of human leukocyte antigen B27
T A B L E 2
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
192 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004
These general diagnostic criteria are use-ful for the diagnosis of spondyloarthropathies,including atypical, undifferentiated forms.
■ GENERAL FEATURES OF ALLSPONDYLOARTHROPATHIES
The features shared by all spondyloarthrop-athies (TABLE 2, TABLE 3) are inflammatory backpain, peripheral arthritis, enthesitis, dactylitis,and uveitis. But even though all types ofspondyloarthropathy can exhibit these fea-tures, the pattern of these features helps definethe distinct form of spondyloarthropathy.
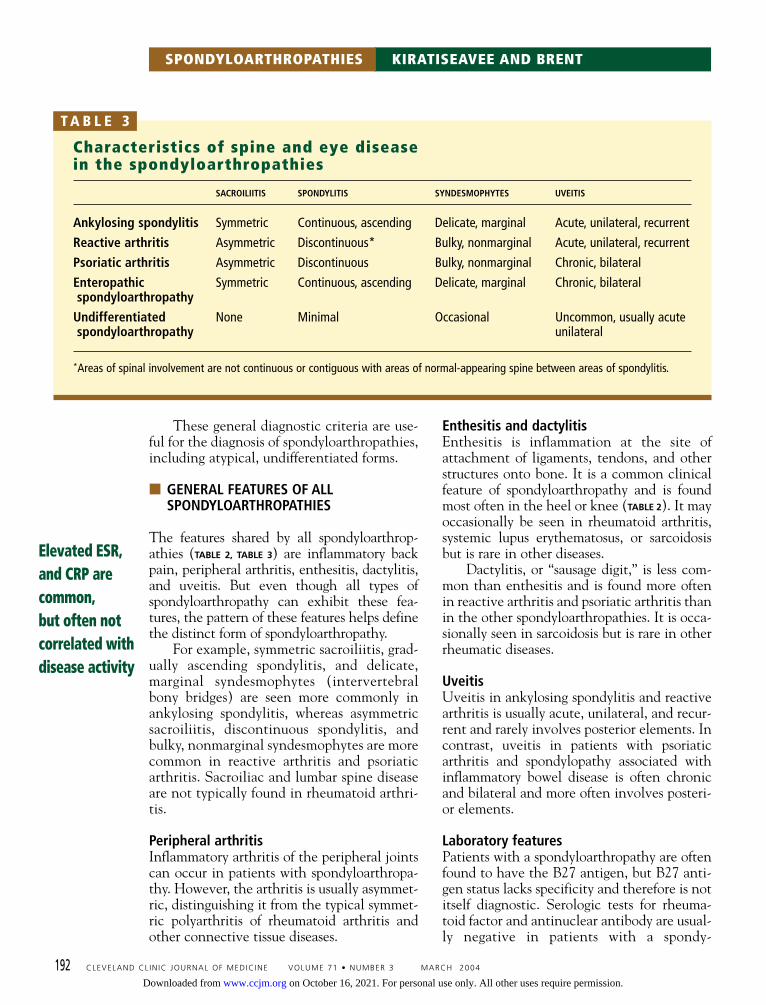
For example, symmetric sacroiliitis, grad-ually ascending spondylitis, and delicate,marginal syndesmophytes (intervertebralbony bridges) are seen more commonly inankylosing spondylitis, whereas asymmetricsacroiliitis, discontinuous spondylitis, andbulky, nonmarginal syndesmophytes are morecommon in reactive arthritis and psoriaticarthritis. Sacroiliac and lumbar spine diseaseare not typically found in rheumatoid arthri-tis.
Peripheral arthritisInflammatory arthritis of the peripheral jointscan occur in patients with spondyloarthropa-thy. However, the arthritis is usually asymmet-ric, distinguishing it from the typical symmet-ric polyarthritis of rheumatoid arthritis andother connective tissue diseases.
Enthesitis and dactylitisEnthesitis is inflammation at the site ofattachment of ligaments, tendons, and otherstructures onto bone. It is a common clinicalfeature of spondyloarthropathy and is foundmost often in the heel or knee (TABLE 2). It mayoccasionally be seen in rheumatoid arthritis,systemic lupus erythematosus, or sarcoidosisbut is rare in other diseases.
Dactylitis, or “sausage digit,” is less com-mon than enthesitis and is found more oftenin reactive arthritis and psoriatic arthritis thanin the other spondyloarthropathies. It is occa-sionally seen in sarcoidosis but is rare in otherrheumatic diseases.
UveitisUveitis in ankylosing spondylitis and reactivearthritis is usually acute, unilateral, and recur-rent and rarely involves posterior elements. Incontrast, uveitis in patients with psoriaticarthritis and spondylopathy associated withinflammatory bowel disease is often chronicand bilateral and more often involves posteri-or elements.
Laboratory featuresPatients with a spondyloarthropathy are oftenfound to have the B27 antigen, but B27 anti-gen status lacks specificity and therefore is notitself diagnostic. Serologic tests for rheuma-toid factor and antinuclear antibody are usual-ly negative in patients with a spondy-
SPONDYLOARTHROPATHIES KIRATISEAVEE AND BRENT
Elevated ESR,and CRP arecommon,but often notcorrelated withdisease activity
Characteristics of spine and eye diseasein the spondyloarthropathies
SACROILIITIS SPONDYLITIS SYNDESMOPHYTES UVEITIS
Ankylosing spondylitis Symmetric Continuous, ascending Delicate, marginal Acute, unilateral, recurrent
Reactive arthritis Asymmetric Discontinuous* Bulky, nonmarginal Acute, unilateral, recurrent
Psoriatic arthritis Asymmetric Discontinuous Bulky, nonmarginal Chronic, bilateral
Enteropathic Symmetric Continuous, ascending Delicate, marginal Chronic, bilateralspondyloarthropathy
Undifferentiated None Minimal Occasional Uncommon, usually acutespondyloarthropathy unilateral
*Areas of spinal involvement are not continuous or contiguous with areas of normal-appearing spine between areas of spondylitis.
T A B L E 3
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
loarthropathy. The erythrocyte sedimentationrate (ESR) and the C-reactive protein (CRP)concentration are often elevated, but eleva-tions may not correlate with disease activity.
■ ANKYLOSING SPONDYLITIS
Axial skeletal involvementBack pain is an extremely common complaintin medical practice, occurring in up to 80% ofthe general population, and the pain is mostcommonly due to a mechanical problem.
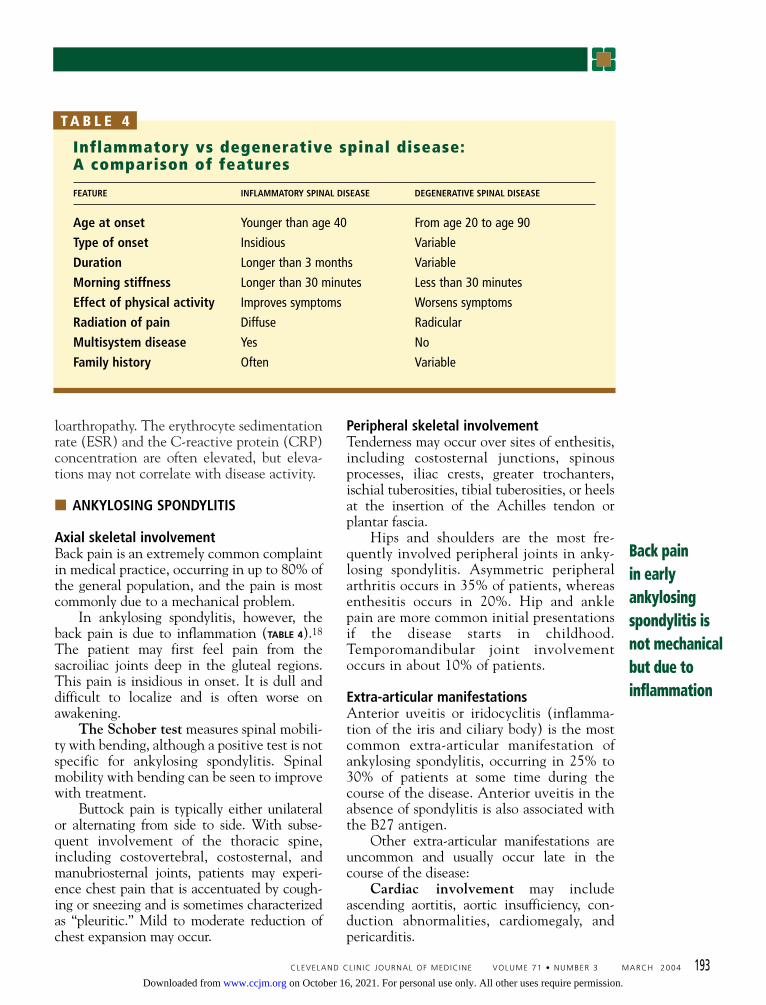
In ankylosing spondylitis, however, theback pain is due to inflammation (TABLE 4).18
The patient may first feel pain from thesacroiliac joints deep in the gluteal regions.This pain is insidious in onset. It is dull anddifficult to localize and is often worse onawakening.
The Schober test measures spinal mobili-ty with bending, although a positive test is notspecific for ankylosing spondylitis. Spinalmobility with bending can be seen to improvewith treatment.
Buttock pain is typically either unilateralor alternating from side to side. With subse-quent involvement of the thoracic spine,including costovertebral, costosternal, andmanubriosternal joints, patients may experi-ence chest pain that is accentuated by cough-ing or sneezing and is sometimes characterizedas “pleuritic.” Mild to moderate reduction ofchest expansion may occur.
Peripheral skeletal involvementTenderness may occur over sites of enthesitis,including costosternal junctions, spinousprocesses, iliac crests, greater trochanters,ischial tuberosities, tibial tuberosities, or heelsat the insertion of the Achilles tendon orplantar fascia.
Hips and shoulders are the most fre-quently involved peripheral joints in anky-losing spondylitis. Asymmetric peripheralarthritis occurs in 35% of patients, whereasenthesitis occurs in 20%. Hip and anklepain are more common initial presentationsif the disease starts in childhood.Temporomandibular joint involvementoccurs in about 10% of patients.
Extra-articular manifestationsAnterior uveitis or iridocyclitis (inflamma-tion of the iris and ciliary body) is the mostcommon extra-articular manifestation ofankylosing spondylitis, occurring in 25% to30% of patients at some time during thecourse of the disease. Anterior uveitis in theabsence of spondylitis is also associated withthe B27 antigen.
Other extra-articular manifestations areuncommon and usually occur late in thecourse of the disease:
Cardiac involvement may includeascending aortitis, aortic insufficiency, con-duction abnormalities, cardiomegaly, andpericarditis.
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004 193
Back painin earlyankylosingspondylitis isnot mechanicalbut due toinflammation
Inflammatory vs degenerative spinal disease:A comparison of features
FEATURE INFLAMMATORY SPINAL DISEASE DEGENERATIVE SPINAL DISEASE
Age at onset Younger than age 40 From age 20 to age 90
Type of onset Insidious Variable
Duration Longer than 3 months Variable
Morning stiffness Longer than 30 minutes Less than 30 minutes
Effect of physical activity Improves symptoms Worsens symptoms
Radiation of pain Diffuse Radicular
Multisystem disease Yes No
Family history Often Variable
T A B L E 4
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
SPONDYLOARTHROPATHIES KIRATISEAVEE AND BRENT
194 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004
Lung involvement is characterized byslowly progressive fibrosis of the upper lobesthat appears, on average, 2 decades after theonset of ankylosing spondylitis. The lesionsmay cavitate and be colonized by Aspergillusspecies.
Neurologic complications can be causedby fracture, instability, or compression of thespine. Cauda equina syndrome is a rare butserious complication of long-standing ankylos-ing spondylitis.
Diagnostic considerationsClinical manifestations of ankylosingspondylitis usually begin in late adoles-cence or early adulthood. In rare cases, they
begin after age 40 or in childhood. Two fea-tures of the history are critically important:inflammatory-pattern back pain with stiff-ness and a family history of ankylosingspondylitis.
The diagnosis is usually established byradiographic evidence of bilateral sacroili-itis,19,20 in addition to a clinical feature suchas inflammatory back pain, limitation of lum-bar spine motion, or decreased chest expan-sion. Testing for the B27 antigen has no valuein routine screening and should not be regard-ed as diagnostic or confirmatory in patientswith back pain.21
Laboratory and radiologic evaluationAn elevated ESR or CRP is seen in up to 75%of patients with ankylosing spondylitis, butthis may lack correlation with clinical disease
Key featureof ankylosingspondylitis:inflammatory-pattern backpain withstiffness anda family historyof the disease
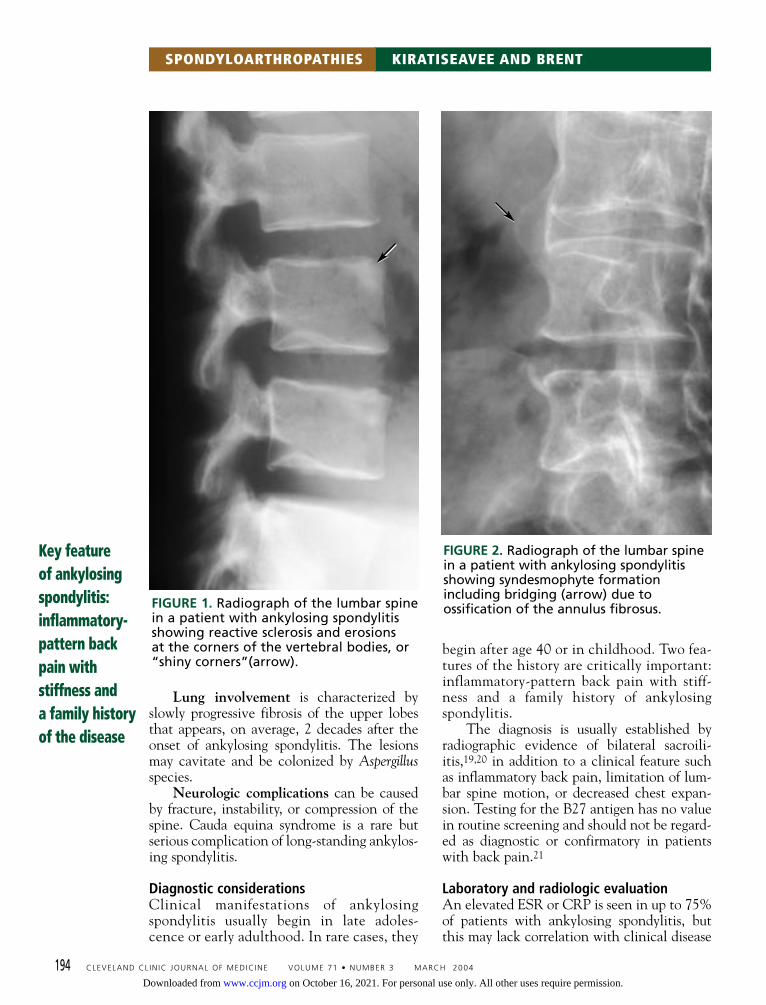
FIGURE 1. Radiograph of the lumbar spinein a patient with ankylosing spondylitisshowing reactive sclerosis and erosionsat the corners of the vertebral bodies, or“shiny corners”(arrow).
FIGURE 2. Radiograph of the lumbar spinein a patient with ankylosing spondylitisshowing syndesmophyte formationincluding bridging (arrow) due toossification of the annulus fibrosus.
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
196 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004
SPONDYLOARTHROPATHIES KIRATISEAVEE AND BRENT
activity. A mild normochromic, normocyticanemia is present in 15% of patients.
Radiographic changes of the sacroiliacjoints are usually symmetric and consist of blur-ring of the subchondral bone plate, followed byerosions and sclerosis of the adjacent bone.
Conventional plain radiography of thepelvis is a good screening tool for evaluationof sacroiliac joints in patients with inflamma-tory back pain. In the early stages of the evo-lution of syndesmophytes, there is inflamma-tion of the superficial layers of the annulusfibrosus with subsequent reactive sclerosis anderosion of the adjacent corners of the verte-bral bodies (called “shiny corners”) (FIGURE 1).This combination of destructive osteitis andrepair leads to “squaring” of the vertebral bod-ies. The inflammatory process is associated
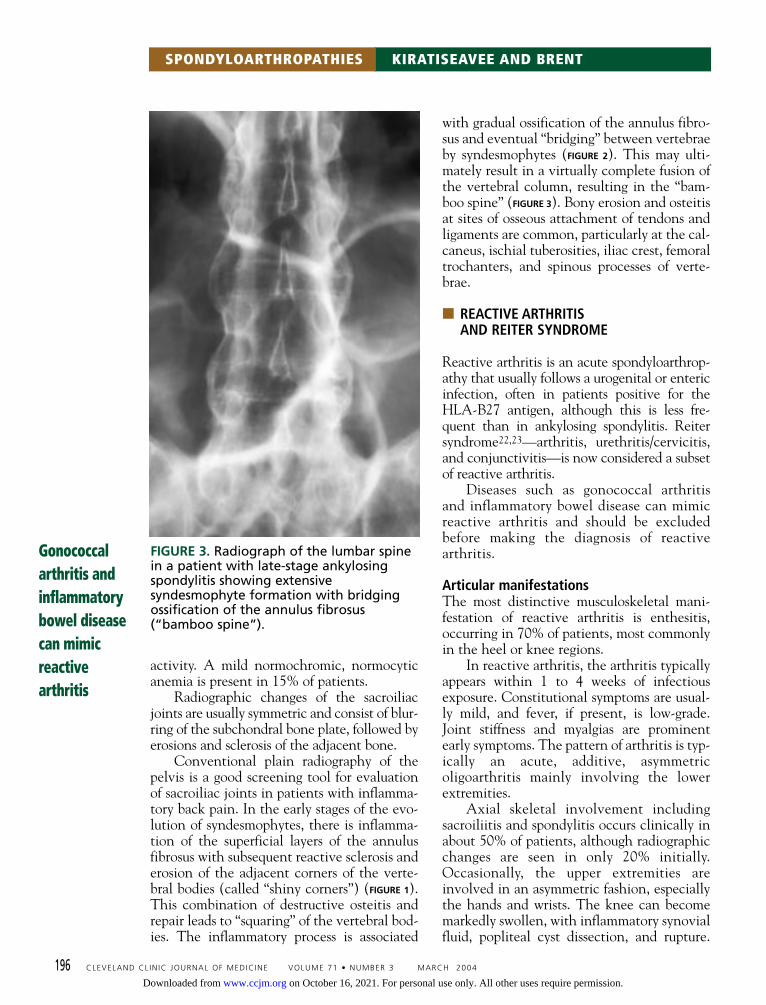
with gradual ossification of the annulus fibro-sus and eventual “bridging” between vertebraeby syndesmophytes (FIGURE 2). This may ulti-mately result in a virtually complete fusion ofthe vertebral column, resulting in the “bam-boo spine” (FIGURE 3). Bony erosion and osteitisat sites of osseous attachment of tendons andligaments are common, particularly at the cal-caneus, ischial tuberosities, iliac crest, femoraltrochanters, and spinous processes of verte-brae.
■ REACTIVE ARTHRITISAND REITER SYNDROME
Reactive arthritis is an acute spondyloarthrop-athy that usually follows a urogenital or entericinfection, often in patients positive for theHLA-B27 antigen, although this is less fre-quent than in ankylosing spondylitis. Reitersyndrome22,23—arthritis, urethritis/cervicitis,and conjunctivitis—is now considered a subsetof reactive arthritis.
Diseases such as gonococcal arthritisand inflammatory bowel disease can mimicreactive arthritis and should be excludedbefore making the diagnosis of reactivearthritis.
Articular manifestationsThe most distinctive musculoskeletal mani-festation of reactive arthritis is enthesitis,occurring in 70% of patients, most commonlyin the heel or knee regions.
In reactive arthritis, the arthritis typicallyappears within 1 to 4 weeks of infectiousexposure. Constitutional symptoms are usual-ly mild, and fever, if present, is low-grade.Joint stiffness and myalgias are prominentearly symptoms. The pattern of arthritis is typ-ically an acute, additive, asymmetricoligoarthritis mainly involving the lowerextremities.
Axial skeletal involvement includingsacroiliitis and spondylitis occurs clinically inabout 50% of patients, although radiographicchanges are seen in only 20% initially.Occasionally, the upper extremities areinvolved in an asymmetric fashion, especiallythe hands and wrists. The knee can becomemarkedly swollen, with inflammatory synovialfluid, popliteal cyst dissection, and rupture.
Gonococcalarthritis andinflammatorybowel diseasecan mimicreactivearthritis
FIGURE 3. Radiograph of the lumbar spinein a patient with late-stage ankylosingspondylitis showing extensivesyndesmophyte formation with bridgingossification of the annulus fibrosus(“bamboo spine”).
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004 197
Exuberant calcaneal spurs may eventuallydevelop due to ossification of the tendinousinsertions. Dactylitis or sausage digits mayoccur due to flexor tenosynovitis in the fingersor toes.
Extra-articular manifestationsUrethritis may be a principal feature of reac-tive arthritis, but genitourinary manifestationscan also include cervicitis, salpingitis, vulvo-vaginitis, aseptic pyuria, and prostatitis. Asterile form of urethritis can be seen afterSalmonella and Shigella infection, as well asafter urogenital or chlamydial infection.
The precipitating episode of diarrhea isoften mild, but occasionally it may be bloodyand prolonged. Patients with Yersinia enteritisoften have mild, recurrent abdominal com-plaints.
Small, shallow, painless ulcers of the glanspenis and urethral meatus (balanitis circinata)have been described and may precede symp-toms of arthritis. In uncircumcised patients,the lesions are moist and are asymptomaticunless secondarily infected. The foreskin hasto be retracted during the physical examina-tion to detect these lesions. On the circum-cised penis, the lesions harden to a crust,which may scar and cause pain.
Keratoderma blennorrhagica is a hyper-keratotic skin lesion that is seen in 12% to14% of patients. It begins as clear vesicles onerythematous bases and progresses to macules,papules, and nodules. The lesions are oftenfound on the soles of the feet, but they mayalso be found on the toes, palms, scrotum,penis, trunk, and scalp. The lesions are indis-tinguishable clinically and microscopicallyfrom pustular psoriasis. Onycholysis mayoccur.
Superficial oral ulcers are an early andtransient feature of the disease. Erythemanodosum is a feature of Yersinia enteritis, andcan mimic inflammatory bowel disease.
Conjunctivitis is the most common ocularcomplication of reactive arthritis. It occurs inthe majority of patients with Shigella infectionsand is often the initial symptom. It also occursafter Salmonella and Campylobacter infections.About 35% of patients with postvenereal reac-tive arthritis develop conjunctivitis. Uveitismay occur as an independent, asynchronous
event due to the shared genetic susceptibilityrelated to the B27 antigen.
Cardiac complications are reported as latesequelae in 10% of patients with severe, long-standing disease including conduction abnor-malities and aortic regurgitation. Conductiondisturbances range from a prolonged PR inter-val to complete heart block.24
Laboratory evaluationThe infection triggering the reactive arthritisshould be sought and treated as warranted.Often, however, the local infection hasresolved by the time features of reactive arthri-tis have developed. Prolonged antibiotic treat-ment courses have not been shown to reliablyinfluence the course of the arthritis.
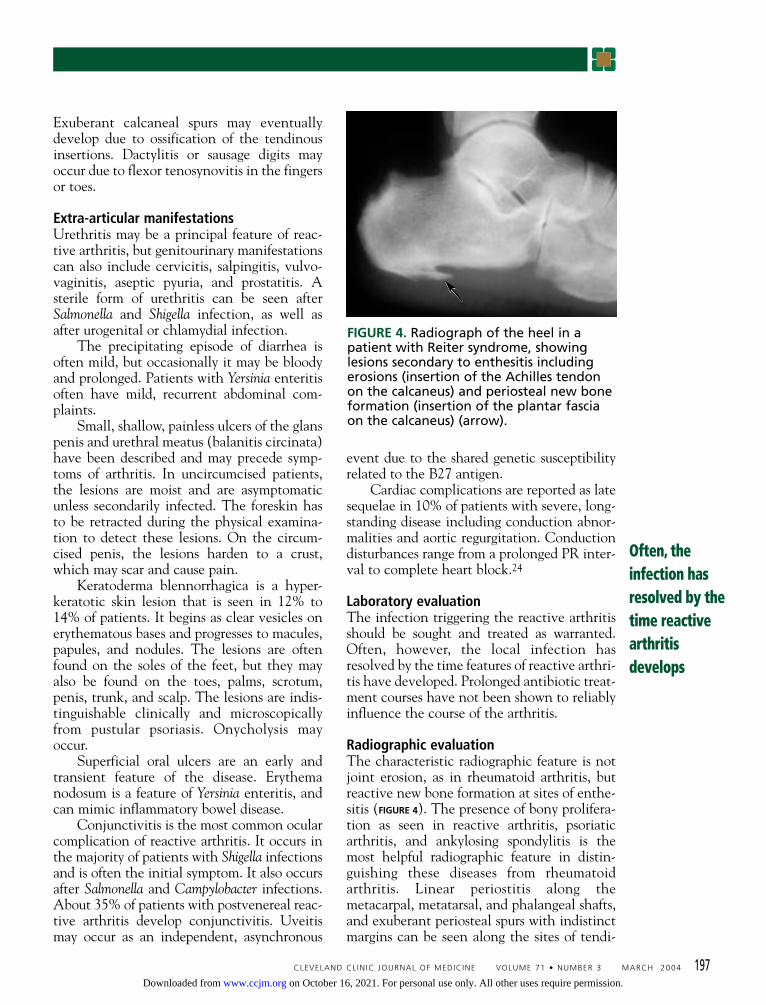
Radiographic evaluationThe characteristic radiographic feature is notjoint erosion, as in rheumatoid arthritis, butreactive new bone formation at sites of enthe-sitis (FIGURE 4). The presence of bony prolifera-tion as seen in reactive arthritis, psoriaticarthritis, and ankylosing spondylitis is themost helpful radiographic feature in distin-guishing these diseases from rheumatoidarthritis. Linear periostitis along themetacarpal, metatarsal, and phalangeal shafts,and exuberant periosteal spurs with indistinctmargins can be seen along the sites of tendi-
FIGURE 4. Radiograph of the heel in apatient with Reiter syndrome, showinglesions secondary to enthesitis includingerosions (insertion of the Achilles tendonon the calcaneus) and periosteal new boneformation (insertion of the plantar fasciaon the calcaneus) (arrow).
Often, theinfection hasresolved by thetime reactivearthritisdevelops
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

200 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004
SPONDYLOARTHROPATHIES KIRATISEAVEE AND BRENT
nous insertion onto bone.In the spine, asymmetric, paravertebral,
comma-shaped ossification is a characteristicfinding on plain radiography in reactivearthritis and psoriatic arthritis. It typicallyinvolves the lower three thoracic and upperthree lumbar vertebrae. In contrast to anky-losing spondylitis, squaring of the vertebrae isuncommon. Plain radiographs of the spine areabnormal in up to 70% of cases of chronicreactive arthritis.
■ PSORIATIC ARTHRITIS
Psoriatic arthritis is defined as inflammatoryarthritis associated with psoriasis and a nega-tive rheumatoid factor.
Articular manifestationsFive general patterns of joint involvementhave been described.25
• Asymmetric oligoarthritis: most jointsmay be involved; small joints of hands andfeet are often involved, including the distalinterphalangeal joints.• Symmetric polyarthritis indistinguishablefrom rheumatoid arthritis: similar to that seenin rheumatoid arthritis, but with a negativerheumatoid factor. Patients with psoriasis,symmetric polyarthritis, and positive rheuma-toid factor are considered to have rheumatoidarthritis and concomitant psoriasis.• Arthritis of the distal interphalangealjoints: this form is commonly associated withnail changes. Inflammation of these joints isnot seen in rheumatoid arthritis.• Destructive arthritis (arthritis mutilans):severe deforming arthritis of small joints ofthe hands and feet, with osteolysis; patientsmay have constitutional symptoms, usuallyassociated with severe skin disease andsacroiliitis.• Spondylitis: may occur alone or withother forms of psoriatic arthritis and is oftenasymptomatic; sacroiliitis is usually asymmet-ric, and syndesmophytes are usually bulky,nonmarginal, and discontinuous, as in reac-tive arthritis.
Other musculoskeletal features of psoriat-ic arthritis include dactylitis, tenosynovitis,and enthesitis. Dactylitis occurs in more than30% of patients and is characterized by a dif-
fuse swelling of the entire digit along witharthritis of the distal interphalangeal, proxi-mal interphalangeal, and metacarpopha-langeal or metatarsophalangeal joints.Dactylitis is not seen in rheumatoid arthritis.
Extra-articular manifestationsThe diagnosis of psoriatic arthritis cannot bemade with certainty in the absence of psoria-sis. A physical examination for hidden psori-atic lesions, particularly in the ears, the hair-line, the umbilical area, the gluteal crease,and the nails is mandatory. Nail changes suchas pitting, ridging, and onycholysis are oftenseen. Onset of arthritis occurs before skin dis-ease in up to 20% of patients. Uveitis has beenreported in 18% of patients.7
Laboratory and radiographic evaluationLow titers of rheumatoid factor have beendetected in 5% to 16% of patients, and anti-nuclear autoantibodies have been detectedin 2% to 16% of the patients with psoriaticarthritis.8,26,27 If high titers of rheumatoidfactor are present in the setting of symmetricpolyarthritis, the patient is considered tohave rheumatoid arthritis and concomitantpsoriasis.
Characteristic radiographic featuresinclude asymmetric distribution, involvementof distal interphalangeal joints, sacroiliitis,spondylitis, bone erosions and periosteal newbone formation, bony ankylosis, and resorp-tion of the distal phalanges. The typical latechange in the peripheral joint is the “pencil-in-cup” erosion marked by lysis of the distalend of the proximal phalanx, with remodelingof the proximal end of the more distal pha-lanx. Involvement of temporomandibular,sternoclavicular, and manubriosternal joints iscommon. The presence of periosteal reactionis also characteristic of enthesitis seen in thiscondition. Sacroiliitis tends to be asymmetric.In the spine, as in reactive arthritis, bulky,nonmarginal syndesmophytes are seen morefrequently than marginal syndesmophytes.
■ ENTEROPATHIC SPONDYLOARTHROPATHY
Articular manifestationsBetween 10% and 20% of patients withinflammatory bowel disease develop arthritis,
Acuteperipheralpsoriaticarthritis canmimic gout
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004 201
slightly more often in Crohn disease than inulcerative colitis. This enteropathic arthritis isusually nondestructive and reversible.
Enteric spondyloarthropathy can occur inone of three patterns. One is a peripheralasymmetric arthritis with fewer than fivejoints involved. Second is a peripheral sym-metric polyarthritis with five or more jointsinvolved. And the third pattern is character-ized by spinal involvement with sacroiliitisand spondylitis, sometimes with peripheraljoint involvement.28,29
The peripheral arthritis may precede thediagnosis of inflammatory bowel disease and,once established, often parallels the activity ofthe inflammatory bowel disease. Spondylitisrarely occurs prior to the diagnosis of inflam-matory bowel disease and does not correlatewith the disease activity of the underlyingbowel disease.
Extra-articular manifestationsClubbing of fingers, uveitis, erythemanodosum, and pyoderma gangrenosum are alsoobserved in inflammatory bowel disease, witha higher frequency in Crohn disease.4Subclinical inflammatory lesions in the gutare common, as observed on colonoscopicmucosal biopsy studies in patients withspondyloarthropathy but no gastrointestinalsymptoms. Follow-up studies of such patientsindicate that 6% develop inflammatory boweldisease and, of those with inflammatory gutlesions, 15% to 25% develop clinical Crohndisease.30 This suggests that patients with sub-clinical inflammatory bowel disease can pre-sent with extraintestinal manifestations, mak-ing diagnosis more challenging.
■ UNDIFFERENTIATEDSPONDYLOARTHROPATHY
“Undifferentiated spondyloarthropathy” rep-resents a working diagnosis for patients whohave manifestations consistent with aspondyloarthropathy but who do not meetthe criteria for its well-defined forms. At pre-sent, it is unclear if these patients have anearly, incomplete form of a defined spondy-loarthropathy.
A good history and physical examinationdocumenting inflammatory back pain, enthe-
sitis, or dactylitis (FIGURE 5) should raise the sus-picion of a spondyloarthropathy. Often, thepassage of time with repeated history andexaminations will clarify the nature of anyunderlying disease.
■ TREATMENTOF SPONDYLOARTHROPATHIES
It is difficult to test treatments for thespondyloarthropathies because the disease—especially the spinal involvement—progress-es slowly. In the absence of specific treat-ments, the general goals of therapy are tocontrol symptoms of morning stiffness andpain, to slow or stop disease progression, andto help the patient maintain erect postureand functional ability.
Drug therapyNSAIDs have been the mainstay of therapy, butthey have not been shown to slow or stop dis-ease progression. Cyclooxygenase-2 inhibitorsare likely effective and have an improved gastricsafety profile compared with nonselectiveNSAIDs. Nonselective NSAIDs are oftenavoided in spondyloarthropathy associated withinflammatory bowel disease. NSAIDs are oftenvery beneficial in patients with undifferentiatedspondyloarthropathy.31,32
If patients do not response to NSAIDs,one of the following second-line therapiesshould be considered.
FIGURE 5. Dactylitis involving the leftfourth toe in a patient withundifferentiated spondyloarthropathy.
10%–20% ofpatients withinflammatorybowel diseasedeveloparthritis
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

SulfasalazineSulfasalazine has been shown to be effectivefor controlling inflammatory symptoms ofspondyloarthropathy over the short term,especially peripheral musculoskeletal involve-ment.33–35 Sulfasalazine was effective inreducing synovitis in patients with peripheralpolyarticular involvement but had no effecton axial involvement.36 Although sul-fasalazine has disease-modifying activity inrheumatoid arthritis, this has not been docu-mented for spondyloarthropathy.37
MethotrexateMethotrexate has been shown to be effectivein the treatment of the articular and skinmanifestations of psoriatic arthritis.38 In smallstudies of patients with ankylosing spondylitis,there was apparent benefit for peripheral butnot axial involvement.39–42
CorticosteroidsOral corticosteroids are occasionally used inpatients with a spondyloarthropathy whohave severe polyarticular symptoms unre-sponsive to other treatments, especiallypatients with psoriatic arthritis. Intra-articu-lar injections are used for monoarticular oroligoarticular flares. In our experience,spondyloarthropathy does not respond aswell to oral or injected corticosteroids asdoes rheumatoid arthritis. However, some
patients’ axial or peripheral arthritis mayrespond dramatically to a therapeutic courseof corticosteroids.
Tumor necrosis factor inhibitorsInfliximab has been used in the treatment ofspondyloarthropathies, including ankylosingspondylitis43,44 and psoriatic arthritis,45,46 inrelatively small studies that showed benefit.Etanercept has been shown to effectivelycontrol the articular and cutaneous manifes-tations of psoriatic arthritis47,48 and caninhibit radiographic progression as well.49 Arecent double-blind, placebo-controlled trialshowed etanercept to be effective in treatingthe musculoskeletal symptoms of ankylosingspondylitis.50 Etanercept recently wasapproved by the US Food and DrugAdministration for the treatment of activeankylosing spondylitis.
Other therapiesPhysical therapy, especially extension exer-cises for the spine, is believed to help thepatient maintain erect posture. Orthopedicsurgery—including total joint arthroplasty ofthe hips and knees and, in rare cases, correc-tive spinal surgery—may be beneficial.However, heterotopic bone formation mayoccur after total joint arthroplasty, especiallyat the hip joint, and prophylactic treatmentshould be considered.
CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004 205
■ REFERENCES1. Olivieri I, Salvarani C, Cantini F, Ciancio G, Padula A. Ankylosing
spondylitis and undifferentiated spondyloarthropathies: a clinicalreview and description of a disease subset with older age at onset.Curr Opin Rheumatol 2001; 13:280–284.
2. Zeidler H, Mau W, Khan MA. Undifferentiated spondy-loarthropathies. Rheum Dis Clin North Am 1992; 18:187–202.
3. Braun J, Bollow M, Remlinger G, et al. Prevalence of spondylo-arthropathies in HLA-B27 positive and negative blood donors.Arthritis Rheum 1998; 41:58–67.
4. de Keyser F, Elewaut D, de Vos M, et al. Bowel inflammation and thespondyloarthropathies. Rheum Dis Clin North Am 1998; 24:785–813.
5. Zeidler H. Undifferentiated arthritis and spondyloarthropathy as amajor problem of diagnosis and classification. Scand J Rheumatol1987; 65(suppl):54–62.
6. Rezaian MM, Aquino ML, Brent LH. Undifferentiated spondylo-arthropathy: comparison of clinical manifestations and outcome onHLA-B27 negative and positive patients. Ann Rheum Dis 2000;59(suppl 1):199.
7. Queiro R, Torre JC, Belzunegui J, et al. Clinical features and predic-tive factors in psoriatic arthritis-related uveitis. Semin ArthritisRheum 2002; 31:264–270.
8. Gladman DD, Farewell VT, Kopciuk KA, Cook RJ. HLA markers andprogression in psoriatic arthritis. J Rheumatol 1998; 25:730–733.
9. Marsal S, Armadans-Gil L, Martinez M, Gallardo D, Ribera A, LienceE. Clinical, radiographic and HLA association as markers for differentpatterns of psoriatic arthritis. Rheumatology 1999; 38:332–337.
10. Dougados M, van der Linden S, Juhlin R, et al. The EuropeanSpondyloarthropathy Study Group preliminary criteria for the classifi-cation of spondylarthropathy. Arthritis Rheum 1991; 34:1218–1227.
11. Boyer SG, Lanier PA, Templin WD, Bulkow L. Spondyloarthropathyand rheumatoid arthritis in Alaskan Yupik Eskimos. J Rheumatol1990; 17:489–496.
12. Sieper J, Braun J. Pathogenesis of spondylarthropathies. Persistentbacterial antigen, autoimmunity, or both? Arthritis Rheum 1995;38:1547–1554.
13. Cuchacovich R, Japa S, Huang WQ, et al. Detection of bacterial DNAin Latin American patients with reactive arthritis by polymerasechain reaction and sequencing analysis. J Rheumatol 2002;29:1426–1429.
14. Hammer RE, Maika SD, Richardson JA. Spontaneous inflammatorydisease in transgenic rats expressing HLA-B27 and human beta2microglobulin: an animal model of HLA-B27-associated human disor-ders. Cell 1990; 63:1099–1112.
15. Taurog JD, Richardson JA, Croft JT. The germ-free state preventsdevelopment of gut and joint inflammatory disease in HLA-B27transgenic rats. J Exp Med 1994; 180:2359–2364.
16. Amor B. Reiter’s syndrome. Rheum Dis Clin North Am 1998;24:677–695.
Studies of TNFinhibitors aresmall butencouraging
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

17. Collantes-Estevez E, Cisnal del Mazo A, Muñoz-Gomariz E.Assessment of 2 systems of spondyloarthropathy diagnostic and clas-sification criteria (Amor and ESSG) by a Spanish multicenter study. JRheumatol 1995; 22:246–251.
18. Calin A. Seronegative spondyloarthritides. Med Clin North Am 1986;70:323–336.
19. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnosticcriteria for ankylosing spondylitis. Arthritis Rheum 1984; 27:361–368.
20. van der Linden S, van der Heijde D. Ankylosing spondylitis.In: Ruddy S, Harris J, Sledge CM, editors. Kelley’s Textbook ofRheumatology. Philadelphia: WB Saunders, 2001:1039–1053.
21. Khan MA, Khan MK. Diagnostic value of HLA-B27 testing ankylosingspondylitis and Reiter’s syndrome. Ann Intern Med 1982; 96:70–76.
22. Reiter H. Über eine bisher unerkannte Spirochateninfektion(Spirochaetosis arthritica). Dtsch Med Wochenschr 1916; 42:1535.
23. Wilkens RF, Arnett FC, Bitter T, et al. Reiter’s syndrome. Evaluation ofpreliminary criteria for definitive disease. Arthritis Rheum 1981;24:844–849.
24. Deer T, Rosencrance JG, Chillag SA. Cardiac conduction manifesta-tions of Reiter’s syndrome. South Med J 1991; 84:799–800.
25. Gladman DD, Rahman P. Psoriatic arthritis. In: Ruddy S, Harris J,Sledge CM, editors. Kelly’s Textbook of Rheumatology. Philadelphia:WB Saunders, 2001:1071–1079.
26. Torre Alonso JC, Rodriguez Perez A, Arribas Castrillo JM, BallinaGarcia J, Riestra Noriega JL, Lopez Larrea C. Psoriatic arthritis: a clini-cal, immunological and radiological study of 180 patients. Br JRheumatol 1991; 30:245–250.
27. Jones SM, Armas JB, Cohen MG, Lovell CR, Evison G, McHugh NJ.Psoriatic arthritis: outcome of disease subsets and relationship ofjoint disease to nail and skin disease. Br J Rheumatol 1994;33:834–839.
28. Orchard TR, Wordsworth P, Jewell DP. Peripheral arthropathies ininflammatory bowel disease: their articular distribution and naturalhistory. Gut 1998; 42:387–391.
29. Wollheim FA. Enteropathic arthritis. In: Ruddy S, Harris J, Sledge CM,editors. Kelly’s Textbook of Rheumatology. Philadelphia: WBSaunders, 2001:1081–1088.
30. Smale S, Natt RS, Orchard TR, Russell AS, Bjarnason I. Inflammatorybowel disease and spondyloarthropathy. Arthritis Rheum 2001;44:2728–2736.
31. Rezaian MM, Brent LH. Undifferentiated spondyloarthropathy:seven-year follow-up study of 357 patients. Arthritis Rheum 2001;44(suppl):S93.
32. Dougados M, Maetzel A, Mijiyawa M, Amor B. Evaluation of sul-phasalazine in the treatment of spondyloarthropathies. Ann RheumDis 1992; 51:955–958.
33. Clegg DO, Reda DJ, Abdellatif M. Comparison of sulfasalazine andplacebo for the treatement of axial and peripheral articular manifes-tations of the seronegative spondyloarthropathies: a Department ofVeterans Affairs cooperative study. Arthritis Rheum 1999;42:2325–2329.
34. Clegg DO, Reda DJ, Weisman MH, et al. Comparison of sulfasalazine andplacebo in the treatment of ankylosing spondylitis. A Department ofVeterans Affairs cooperative study. Arthritis Rheum 1996; 39:2004–2012.
35. Dougados M, van der Linden S, Leirisalo-Repo M, et al. Sulfasalazinein the treatment of spondyloparthropathy. A randomized, multicen-ter, double-blind, placebo-controlled study. Arthritis Rheum 1995;
38:618–627.36. Clegg DO, Reda DJ, Weisman MH, et al. Comparison of sulfasalazine
and placebo in the treatment of reactive arthritis (Reiter’s syn-drome). A Department of Veterans Affairs Cooperative Study.Arthritis Rheum 1996; 39:2021–2027.
37. Thomson GT, Thomson BR, Thomson KS, Ducharme JS. Clinical effi-cacy of mesalamine in the treatment of the spondyloarthropathies. JRheumatol 2000; 27:714–718.
38. Cuellar ML, Espinoza LR. Methotrexate use in psoriasis and psoriaticarthritis. Rheum Dis Clin North Am 1997; 23:797–809.
39. Sampiao-Barros PD, Costallat LT, Bertolo MB, Neto JF, Samara AM.Methotrexate in the treatment of ankylosing spondylitis. Scand JRheumatol 2000; 29:160–162.
40. Biasi D, Carletto A, Caramaschi P, Pacor ML, Maleknia T, BambaraLM. Efficacy of methotrexate in the treatment of ankylosingspondylitis: a three-year open study. Clin Rheumatol 2000;19:114–117.
41. Marshall RW, Kirwan JR. Methotrexate in the treatment of ankylos-ing spondylitis. Scand J Rheumatol 2001; 30:313–314.
42. Roychaudhry B, Bintley-Bagot S, Hunt J, Tunn EJ. Methotrexate insevere ankylosing spondylitis: a randomized placebo controlled, dou-ble-blind observer study [abstract]. Rheumatology 2001; 40(suppl1):43.
43. Van den Bosch F, Kruithof E, Baeten D, de Keyser F, Mielants H, VeysEM. Effects of a loading dose regimen of three infusions of chimericmonoclonal antibody to tumour necrosis factor alpha (infliximab) inspondyloarthropathy: an open pilot study. Ann Rheum Dis 2000;59:428–433.
44. Brandt J, Haibel H, Cornely D, et al. Successful treatment of activeankylosing spondylitis with the anti-tumor necrosis factor alphamonoclonal antibody infliximab. Arthritis Rheum 2000;43:1346–1352.
45. Antoni C, Kavanaugh A, Kirkham B, et al. The infliximab multina-tional psoriatic arthritis controlled trial (IMPACT) [abstract]. ArthritisRheum 2002; 46(suppl):S381.
46. Feletar MH, Brockbank JE, Schentag CT, Lapp V, Gladman DD.Treatment of recalcitrant psoriatic arthritis patients with inflix-imab—a 12-month observational study of 16 patients [abstract].ACR/ARHP Annual Scientific Meeting, New Orleans, Louisiana,2002.
47. Mease PJ, Goffe BS, Metz J, van der Stoep A, Finck B, Burge DJ.Etanercept in the treatment of psoriatic arthritis and psoriasis: a ran-domised trial. Lancet 2000; 356:385–390.
48. Mease PJ. Improvement in disease activity in patients with psoriat-ic arthritis receiving etanercept (Enbrel): results of a phase 3 mul-ticenter clinical trial [abstract]. Arthritis Rheum 2001;44(suppl):S90.
49. Ory P, Sharp JT, Salonen D, et al. Etanercept (Enbrel) inhibits radio-graphic progression in patients with psoriatic arthritis [abstract].Arthritis Rheum 2002; 46(suppl):S196.
50. Gladman DD, Sack KE, Davis JC. Treatment of ankylosing spondylitisby inhibition of tumor necrotic factor alpha. N Engl J Med 2002;346:1349–1356.
ADDRESS: Lawrence H. Brent, MD, Einstein Arthritis Center, 5501 OldYork Road, Korman 103, Philadelphia, PA 19141;e-mail [email protected].
206 CLEVELAND CL IN IC JOURNAL OF MEDICINE VOLUME 71 • NUMBER 3 MARCH 2004
SPONDYLOARTHROPATHIES KIRATISEAVEE AND BRENT
on October 16, 2021. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from