sports related injuries william kesto, md. sports related injuries in the over 55 crowd over 1...
TRANSCRIPT

Sports Related InjuriesWilliam Kesto, MD

Sports Related InjuriesIn the over 55 crowdOver 1 million sports related injuries a year

Who are the Culprits
You…the athlete…just can’t stop can you?The sports you playThe body you live in

What’s this?

What?

DefinedPickle-Ball is a hybrid of Badminton, Tennis and Table-tennis, a three in one game, played with wooden paddles and a perforated plastic ball. It can be played on a normal Badminton court or on any hard surface such as driveways, parks, cul-de-sacs, playgrounds, tennis/volleyball/sepak takraw courts.

Pickleball!!!!!
Ok now I get it
See many injuries from this gameNot that the game is dangerous, just extremely popularNever knew the game existed…now I do

Golf
Now this game I knew about but…I never knew you could play so much of it…

Behind door #3

Some others
SwimmingWalkingTennisBikingTravel

Prevention
General principles– Stretch prior to activity: shouldn’t hurt– Warm up prior to activity: break a sweat– Make sure you’re in good enough shape to
participate– Ease back into activity– Don’t play through the pain

Prevention
No magic bulletIf you play…there is a chance you’ll get injured.
Injuries
ShouldersElbowsKnees

Shoulder
Bones and Ligaments

Shoulder
Anatomy: muscles and tendonsPosterior Anterior

ShoulderInjuries– Overuse: fatigued tendons and
muscles
– Subacute: fatigued tendons and muscles that now slowly begin to tear/wear out: pain is increasing
– Acute: Fell, threw too hard, swung to hard, now your shoulder hurts

ShoulderOveruse– Tendonitis:
irritation/inflammation of a tendon• Pain down the side of the
shoulder with overhead and behind the back activity
• Nighttime pain
– Tendonopathy: “sick” tendon• Similar pain complaints• Pain may have been evident for
a longer period of time

Shoulder
Treatment– Make sure that’s all it is: xrays and MRI– Non-steroidal anti-inflammatories – Ice – Physical Therapy– Corticosteroid injection

Shoulder
Subacute– Progression of an overuse injury– Had occasional pain before, now it hurts worse
and more frequently

Shoulder
Subacute– Xrays for the bones– MRI for the soft tissues– If unremarkable• Non-steroidal anti-inflammatories• Ice • Physical Therapy• +/- Corticosteroid injection

Shoulder
Acute– Xray and MRI– Treatment depends on the findings

Shoulder
In general the work up for overuse, subacute, and acute shoulder pain is the sameRadiographs are a mustMRI Indications: Drop arm sign, external rotation lag sign, dislocationI like to know what I’m dealing with before treating it

Shoulder
Concerning injuries– Pain does not improve
with conservative management
– Positive findings on xray• Fracture• Arthritis

Shoulder
Concerning injuries– Positive findings on MRI (found something wrong)• Rotator cuff tear• Labral tear• Biceps tendon tear

Shoulder
What next?– Shoulder arthroscopy– “Clean up the shoulder”– Repair torn tendons

Shoulder
Recovery– Worst case scenario is cuff repair• 6 weeks: Healing phase
– Typically start therapy at 3 weeks– Full time sling 3 weeks/part time 3 weeks
• 6 weeks: Rehab• 6 weeks: Strengthening• Typically 3-4 months…start resuming previous
activities…SLOWLY
Knee
Good news about shoulder pain is we don’t walk on our handsThe knees are a different story
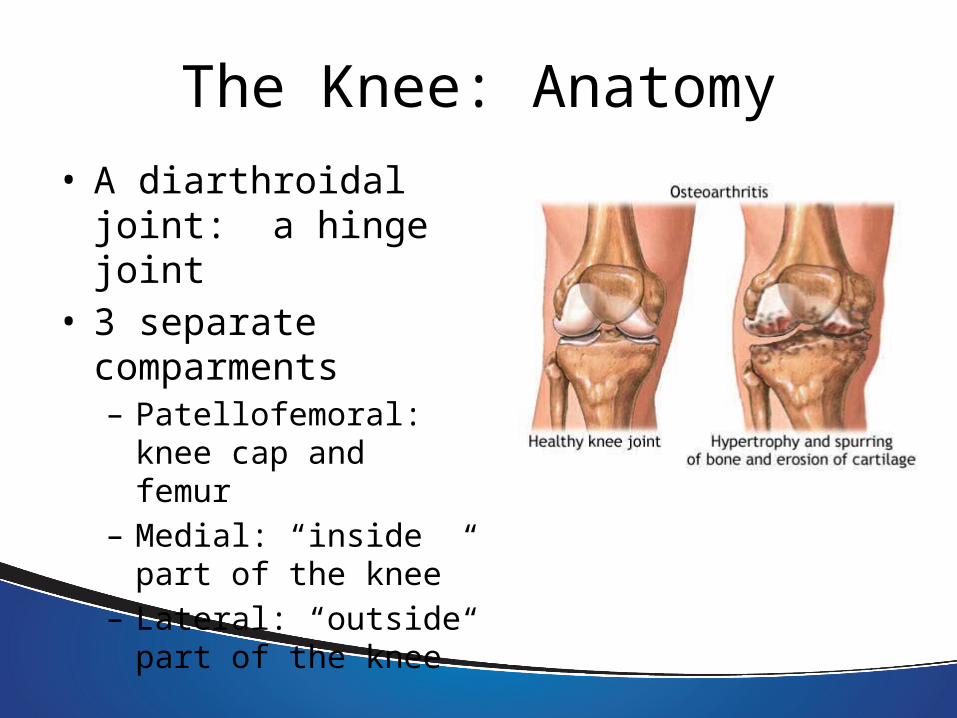
The Knee: Anatomy• A diarthroidal joint: a
hinge joint• 3 separate
comparments– Patellofemoral: knee cap
and femur– Medial: “inside part of
the knee”– Lateral: “outside part of
the knee”

The Knee
• Two main types of cartilage in the knee– Articular cartilage: a thin lining of resilient connective tissue that
serves as padding and an ultra low friction surface– Meniscal cartilage: serve to deepen the contact of the femur on the
tibia, provide stability, distribute force

The Knee
Joint reaction force in the knee is about 3 times body weight when walkingThis is absorbed by the menisci and articular cartilage

The Knee
• 4 main ligaments in the knee– Anterior Cruciate
Ligament (ACL)– Posterior Cruciate
Ligament (PCL)– Medial Collateral
Ligament (MCL)– Lateral Collateral
Ligament (LCL)

Von Mow“The human joint
functions so well… that we are totally unaware of it until there is a problem”

The Knee
Problems of the knee– “Tendonitis”– Meniscal tears– Ligament injuries– Cartilage injuries– Arthritis

Tendonitis
Tendon: strong piece of tissue that attaches a muscle to boneTendonitis: irritation/inflammation of a tendonTypically responds well to rest, ice, anti-inflammatories, and focused PT

Meniscal Tears
• Disruption of the continuity of the meniscus of the knee

Mechanism of injury
Twisting: sportsTurning: sportsDeep knee bends: sportsPivoting: sports

Meniscal Tear
Symptoms– Focal pain, typically intermittent– Swelling– Nightime pain– Pain with activity– Catching/locking

Meniscal Tears
Treatment options– Physical Therapy – Injections
– Arthroscopic surgery• remove/fix the tear• 80-90% better by 6-8 weeks

Ligament injuries
ACL– Fix in active, physical individual– NO real age restriction– Contraindicated if significant arthritis
PCL– Fix when symptomatic– Contraindicated if significant arthritis

Ligament injuries
MCL– Brace for six weeks– Weight bearing as tolerated
LCL– Brace– Fix if part of a complex of lateral injuries

Cartilage injuries
• Damage to the articular cartilage of the knee

Cartilage injury

Cartilage injury
• Typically unclear severity until the time of arthroscopy
• Variety of treatments dependent on the severity– “smooth down”– Microfracture

Cartilage injury
• Cartilage transplant– Treatment for smaller,
focal cartilage defects– An attempt to prevent
the progression to osteoarthritis
Not useful in degenerative arthritis

Knee injuries
Problem
– “Just had the knee scoped. Doc told me I had a torn meniscus and he scraped some arthritis out of there”

Knee injuries
Meniscus tear with mild/mod arthritis– Rather common– Meniscus tear is the “mechanical” problem– Treatment based on 6 weeks of observation– If symptoms are improving, monitor– If not or worsening, then consider
viscosupplemenation

What is Viscosupplementation?It is a solution of hyaluronan.Hyaluronan is the lubricant and shock absorber in joints.Osteoarthritis reduces the body’s ability to produce hyaluronan.Without it, the patient experiences the pain of OA as the joint wears out.
How long will it last?It varies from patient to patient, depending on a number of factors: age, weight, stage of the disease, etc.Maximum benefits can be seen up to 12 weeks from the last injectionIn general, the beneficial effects last from 6 months to a yearNo contraindication to a repeat injection series

Elbows90% of the time it’s an overuse injury

Lateral and Medial Epicondylitis

TreatmentTreatment consists of – Rest: take some time off!– Ice – Compression– Elevation– Anti-inflammatories

Treatment
For recalcitrant cases– Consider corticosteroid injection– Platelet rich plasma injection
Most of the time these go away. Some require surgery

New Horizons in Treatment
Always working on better fixation techniquesMore anatomically correctBut what about just trying to make the body heal better?

Platelet Rich Plasma
• High concentration of functionally viable platelets and their associated growth factors
• Extracted from a small amount of patients blood: 9-18cc
• Spun through a simple centrifugation process to form a dense suturable fibrin matrix scaffold
• Delivered arthroscopically/open and placed directly into the tear site to stimulate a reparative healing response for soft tissue and bone repair

Factor Target Cell/Tissue Function
PD-EGF (epidermal growth
factor)
•Blood vessel cells, outer skin cells•Fibroblasts, and many other cell types
•Cell growth, recruitment•Differentiation, skin closure•Cytokine secretion
PDGF, A+B(platelet-derived growth
factor)
•Fibroblasts, smooth muscle cells, chondrocytes, osteoblasts, mesenchymal stem cells
•Potent cell growth, recruitment•Blood vessel growth, granulation•Growth factor secretion; matrix formation w/BMPs (collagen and bone)
TGF-ß1(transforming growth
factor beta1)
•Blood vessel tissue, outer skin cells•Fibroblasts, monocytes•TGF gene family includes the BMPs•Osteoblasts – highest levels of TGF-βr
•Blood vessel (+/-), collagen syn.•Growth inhibition, apoptosis (cell death)•Differentiation, activation
IGF-1,2(insulin-like growth
factor1,2)
•Bone, blood vessel, skin, other tissues•Fibroblasts
•Cell growth, differentiation, recruitment•Collagen synthesis w/PDGF
VEGF/ECGF(vascular endothelial GF)
•Blood vessel cells •Cell growth, migration, new blood vessel growth•Anti-apoptosis (anti-cell death)
bFGF(basic fibroblast growth
factor)
•Blood vessels, smooth muscle, skin•Fibroblasts, other cell types
•Cell growth•Cell migration, blood vessel growth
Platelet-Derived Growth Factors

ApplicationsDirect liquid form injections of concentrated platelets for the various tendonitis problemsClot form applications with extended growth factor release for cuff repairs, etc…

Conclusion
Sports and athletics are a vital part of our livesAs we continue to play, the likelihood of injury increasesThere are many treatment options available

Conclusion
My role as an orthopedic surgeon is not to tell you no but rather to “Keep your life in motion.”