standards for nursing · pdf filefrom the nursing services. the standards are on the same...
TRANSCRIPT
STANDARDS FOR NURSING EXCELLENCE
First Edition
October 2013
NATIONAL ACCREDITATION BOARD FOR
HOSPITALS AND HEALTHCARE
PROVIDERS

2
FOREWORD
Nursing services are an integral part of the clinical services of any health care
organization. The aim of nursing services is to provide comprehensive nursing care in
terms of health promotion, prevention of diseases and therapeutic nursing care to the
patients in a HCO as well as to the community. The objective of the nursing professional
is to provide safe, competent and ethical nursing care with compassion, comfort and
collaboration with the patients, the family, the community and the clinical care team. The
Nursing professionals are the cornerstone of any quality related programme in a health
care organization since most of the delivery and monitoring of health care is carried out
by them. The nursing professionals are the frontline staff with whom the patients, their
families and the visitors interact first hand. Their knowledge, skills, attitude,
communication and other soft skills thus make all the difference in the ultimate delivery
of health care to the patients.
Standards are pre requisite for the promotion of safe, effective, competent and ethical
nursing care. They help the individual nursing practitioner to evaluate the services being
provided by them and also act as a catalyst for self regulation and improvement.
Nursing excellence standards have been framed with a view to lay down the guidelines
for evaluating the nursing services being provided by a Health Care Organization,
thereby providing a platform for continual improvement. These standards are applicable
to all the Health care organizations irrespective of their size, role and complexity. They
will help in regulating, guiding and promoting professional nursing practice. They will
serve as guidelines to nurse administrators and supervisors for supporting and
facilitating safe, competent and ethical nursing practices within their Health Care
Organizations.
Apart from serving as a frame work for evaluation of the quality of nursing services
rendered, these standards will also provide guidelines to assist nurses in decision-
making and will support the nursing efforts by outlining the professional expectations

3
from the nursing services. The Standards are on the same framework as has been for
the NABH Standards for Health Care Organizations.
The 1st edition of nursing excellence standards is divided into 07 chapters, focusing on
various professional, administrative and governance aspects of nursing. Seven chapters
are further divided into 48 standards. Put together there are 216 objective elements
incorporated within these standards. Objective elements are required to be complied
with in order to meet the requirement of a particular standard. Similarly, standards are
required to be complied with, in order to meet the requirement of a particular chapter.
Finally all chapters are deciding factor to say whether a hospital is meeting the
requirements of the certification program. In the beginning of each chapter, intent is
given to highlight the summary of the chapter. For most of the objective elements,
interpretation is provided just to further elaborate on how that objective element can be
met.
Standards are dynamic and would be under constant review process. Comments and
suggestions for improvement are appreciated. We seek your support in keeping these
standards adequate to the need of industry.

4
TABLE OF CONTENTS
Chapter No Particulars Page No.
Chapter:1 Nursing Resource Management (NRM)
Chapter:2 Nursing Care of Patient (NCP)
Chapter:3 Management of Medication (MOM)
Chapter:4 Education, Communication and Guidance (ECG)
Chapter:5 Infection Control Practices (ICP)
Chapter:6 Empowerment and Governance (EG)
Chapter:7 Nursing Quality Indicators (NQI)
Glossary

5
CHAPTER 1
NURSING RESOURCE MANAGEMENT
Intent of the chapter:
Nursing staff is the most important resource of a hospital and healthcare system. The
goal of nursing resource management is to acquire, provide, retain and maintain
competent staff nurse in right numbers to meet the needs of the patients and community
served by the organization.
Training and development of the nursing staff must be in consonance with the expected
performance in the present and future anticipated jobs. The nursing professionals shall
be provided with opportunities for professional advancement. The organization shall lay
down the job description and procedures for credentialing and privileging of the nursing
staff.
There shall be an established procedure for addressing grievances.

6
Summary of Standard
NRM.1. The organization has a documented system of nursing resource planning.
NRM.2. The organization has structures and processes for induction and for
enhancing the transition of novices to competent nursing professionals.
NRM.3. The organization has processes in place for induction training, In-service
education and Continuous Nursing Education (CNE) programmes and for
documentation of the same in the personal files.
NRM.4.
There is a process for credentialing and privileging of nursing professionals,
permitted to provide patient care without supervision.
NRM.5. An appraisal system for evaluating the performance of nursing staff exists
as an integral part of the nursing resource management process.
NRM.6. There is a provision for acknowledging outstanding performances/
contributions of nursing professionals.
NRM.7. There is an established process in place to identify and manage problems
related to incompetent, unsafe or unprofessional conduct.
NRM.8. The organization demonstrates workplace safety for nursing professionals
and protection of their rights.
NRM.9.
The organization has a documented and established grievance handling
system.

7
Standards and Objective Elements
Standard
NRM.1. The organization has a documented system of nursing resource planning.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing resource
planning supports the
organization‟s current
and future ability to meet
the care, treatment and
service needs of the
patient.
It shall use recognised
methods for determining
levels of nursing staffing.
A yearly nursing plan is
to be documented, with
inputs from all
stakeholders including
the Nursing Head,
Medical Head, key
clinicians, HR and
Finance. This should be
in line with growth
projections, strategic
plans and budgets of the
hospital. In case higher
approvals are needed eg
in Govt sector, hospitals,
the plan approval will be
taken in advance of
implementation.
References may be
used. INC guidelines,
Acuity based norms etc.
The organization will
ensure that the plan
addresses staffing crisis
situations due to
attrition, and the hiring
plan ensures vacancies
are filled up early so that
patient care is not
compromised.
A contingency plan for
staffing in sudden high
occupancy levels is in
place. The deciding
parameters or
guidelines for nursing
manpower must be
clearly delineated.
b. The organization
maintains an adequate
number and mix of
nursing staff to meet the
The nursing staff should
be commensurate with
the workload and the
clinical requirement of
A good reference could
be the INC guidelines.

8
care, treatment and
service needs of the
patient.
the patients. Workload
on Nursing professionals
will be monitored.
c. The person heading the
nursing service has
requisite and appropriate
qualifications.
INC recognized
qualifications with
management
training/degree.
Self-explanatory.
d. The person heading the
nursing service has
requisite and appropriate
experience.
Self-explanatory As per INC guidelines /
MOHFW hospital
manual guidelines.
e. The required job
specification and job
description are defined
for each category of
nursing staff.
The content of each job
should be well defined
and the qualifications,
skills and experience
required for performing
the job should be clearly
laid down. The job
description should be
commensurate with the
qualification.
Refer to glossary for
definition of "job
description” and “job
specification". For a job
which requires the skills
of a nurse the minimum
qualification shall be a
GNM/ B.Sc Nursing.
This should be part of
nursing manual, refer
NCP 1.
Standard
NRM.2. The organization has structures and processes for induction and for
enhancing the transition of novices to competent nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)

9
a. Nursing shift plans based upon
timings of shift, day or week shall
identify and depute nursing
professionals to various areas
based on their skills and
competencies.
For eg. if the shift
for a unit is eight
hourly then the
nursing
professionals doing
the shift at night
should have skills
and competencies
that enable her to
independently
monitor and handle
emergency
situations.
Self-explanatory.
b. Training need shall be identified
on a continual basis by the senior
nursing professionals as well as
the Clinical Heads as appropriate.
Self-explanatory. Self-explanatory.
c. Required competency parameters
shall be evaluated by such senior
nursing professionals and the
clinical and support service Heads
and shall be recorded in the
training records as in NRM 2.
These are generally
bed-side nursing
care procedures
and are therefore
evaluated on a
continual basis. The
recording may be
done at suitable
periodic intervals.
Self-explanatory.
Standard
NRM.3. The organization has processes in place for induction training, In-service
education and Continuous Nursing Education (CNE) programmes and for

10
documentation of the same in the personal files.
Sr.No Objective Elements Interpretation Remark(s)
a. Every nurse entering the
organization is provided induction
training.
The organization
shall determine as
to when induction
training shall be
conducted.
However, it shall be
within 15 days of
the staff joining.
The contents of the
induction training
should be defined
and should include
issues related to
patient safety and
quality nursing care.
The contents of this
training could be
provided to every
nursing staff in the
form of a booklet.
There can be
separate induction
training at the
organizational level
and for the
respective
departments.
b. A documented training and
development policy exists for the
staff.
A training manual
incorporating the
procedure for
identification of
training needs, the
training
methodology,
documentation of
training, training
assessment, impact
of training and the
training calendar
The training shall be
for all categories of
nursing staff.
11
should be prepared.
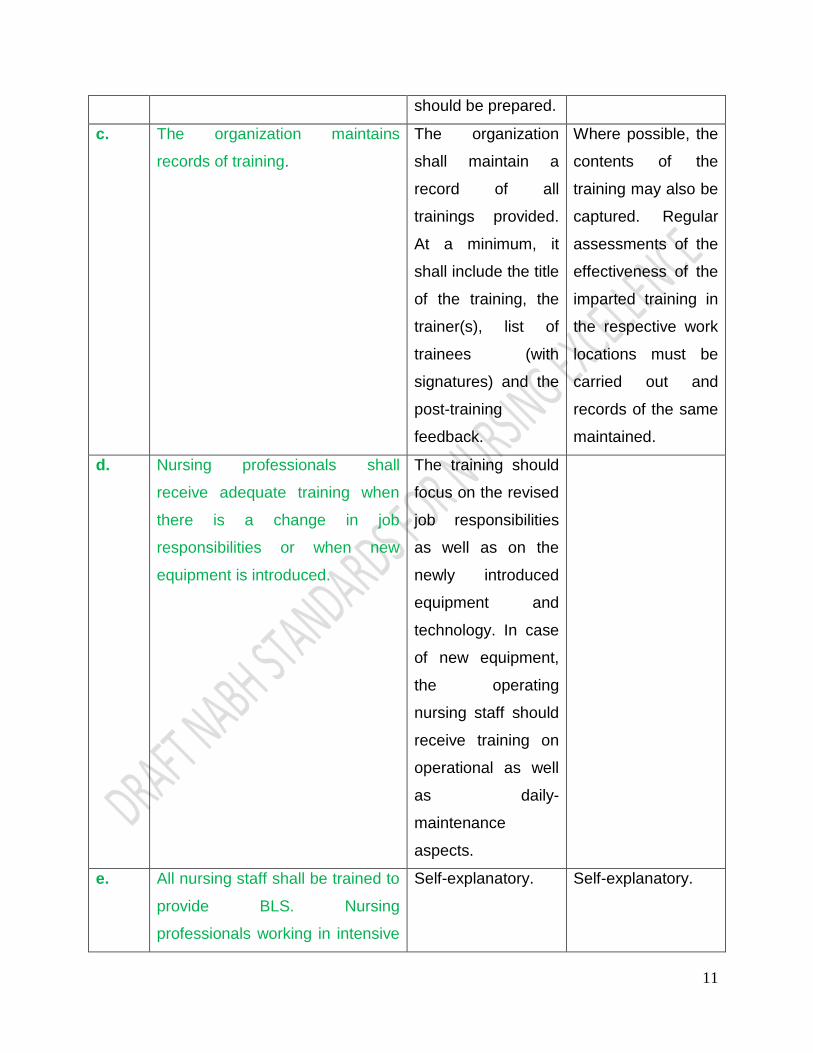
c. The organization maintains
records of training.
The organization
shall maintain a
record of all
trainings provided.
At a minimum, it
shall include the title
of the training, the
trainer(s), list of
trainees (with
signatures) and the
post-training
feedback.
Where possible, the
contents of the
training may also be
captured. Regular
assessments of the
effectiveness of the
imparted training in
the respective work
locations must be
carried out and
records of the same
maintained.
d. Nursing professionals shall
receive adequate training when
there is a change in job
responsibilities or when new
equipment is introduced.
The training should
focus on the revised
job responsibilities
as well as on the
newly introduced
equipment and
technology. In case
of new equipment,
the operating
nursing staff should
receive training on
operational as well
as daily-
maintenance
aspects.
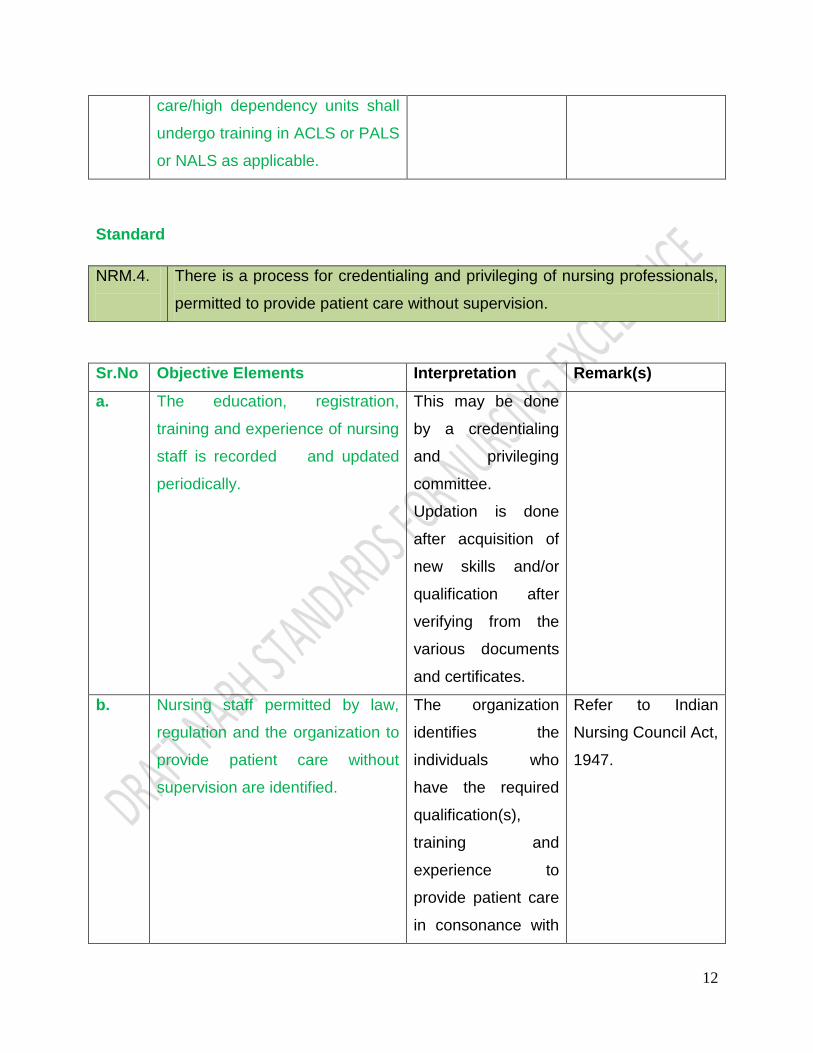
e. All nursing staff shall be trained to
provide BLS. Nursing
professionals working in intensive
Self-explanatory. Self-explanatory.
12
care/high dependency units shall
undergo training in ACLS or PALS
or NALS as applicable.
Standard
NRM.4.
There is a process for credentialing and privileging of nursing professionals,
permitted to provide patient care without supervision.
Sr.No Objective Elements Interpretation Remark(s)
a. The education, registration,
training and experience of nursing
staff is recorded and updated
periodically.
This may be done
by a credentialing
and privileging
committee.
Updation is done
after acquisition of
new skills and/or
qualification after
verifying from the
various documents
and certificates.
b. Nursing staff permitted by law,
regulation and the organization to
provide patient care without
supervision are identified.
The organization
identifies the
individuals who
have the required
qualification(s),
training and
experience to
provide patient care
in consonance with
Refer to Indian
Nursing Council Act,
1947.

13
the law.
c. All such information pertaining to
the nursing staff is appropriately
verified when possible.
The organization
shall do the same
by verifying the
credentials from the
organization which
has awarded the
qualification/training.
Educational
parameters are
validated by
verifying the
qualification
certificates. Training
is validated through
training certificates
and skill verification
on the job and
experience is
validated by way of
the records
provided by the
nurse from the
previous employers.
d. Nursing staff are granted
privileges in consonance with
their qualification, training,
experience and registration.
The organization
shall lay down
parameters for
identifying as to
what each nurse is
authorised to do.
It is preferable to get
the privileging done
through a
credentialing and
privileging. To be
read in conjunction
with NRM 4b
committee based on
For example, an
Infection Control
Nurse should have
had requisite in-
house/external
training and
experience and the
aptitude and
knowledge to
perform the tasks
required of her.

14
pre existing criteria /
parameters.
e. The requisite services to be
provided by the nursing staff are
known to them as well as the
various departments/units of the
organization.
Self-explanatory. This could be done
by internal
communication.
f. Nursing professionals care for
patients as per their privileging.
Self-explanatory.
New staff members
can be under the
proctorship till
independent
privilege is being
provided for each
staff.
The organization
could evolve a
mechanism to
ensure that nursing
professionals are
providing only those
services that they
have been
privileged to offer.
Standard
NRM.5. An appraisal system for evaluating the performance of nursing staff exists
as an integral part of the nursing resource management process.
Sr.No Objective Elements Interpretation Remark(s)
a. A recorded performance
appraisal system exists in
the organization for
nursing professionals.
Self-explanatory. This shall be done for all
categories of nursing
staff starting from the
person heading the
nursing and including
nursing professionals
who are employees.

15
For definition of
“performance appraisal”
refer to glossary.
b. The nursing professionals
are made aware of the
system of appraisal at the
time of induction.
Self-explanatory.
This could be
incorporated in the
service booklet and
included in the induction
training.
c. Performance is evaluated
based on the pre-
determined criteria.
Self-explanatory.
The criteria for
assessment should be
defined and known to
the nursing
professionals. It is
preferable to have
objective criteria that
can be supplemented
by subjective remarks.
Key result areas are
identified for each
nursing staff and training
need assessment is also
done at the time of
assessment.
d. Performance appraisal is
carried out at pre-defined
intervals and is recorded.
Self-explanatory.
This shall be done at
least once a year.
Standard
NRM.6. There is a provision for acknowledging outstanding performances/
contributions of nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)

16
a. Patients, families and staff shall
be encouraged to report positive
feedback about nursing care
delivered in relevant areas.
Self-explanatory. Self-explanatory.
b. Nursing staff with managerial
responsibilities shall ensure that
soft skills in nursing, qualities of
leadership and professional
competence are duly reported to
higher authorities. This shall be
recorded (see NRM 4 c also).
Self-explanatory. Self-explanatory.
Standard
NRM.7. There is an established process in place to identify and manage problems
related to incompetent, unsafe or unprofessional conduct.
Sr.No Objective Elements Interpretation Remark(s)
a. The process shall include daily
monitoring of appearance and
ability to impart nursing care.
Appearance,
Behaviour,
Communication, and
Decorum.
Self-explanatory.
b. The process shall include analysis
of all complaints pertaining to
nursing services specifically
addressing individual nursing
staff.
Self-explanatory. The process shall
ensure that there is
no victimization and
corrective action is
focused against the
system rather than
the individual.
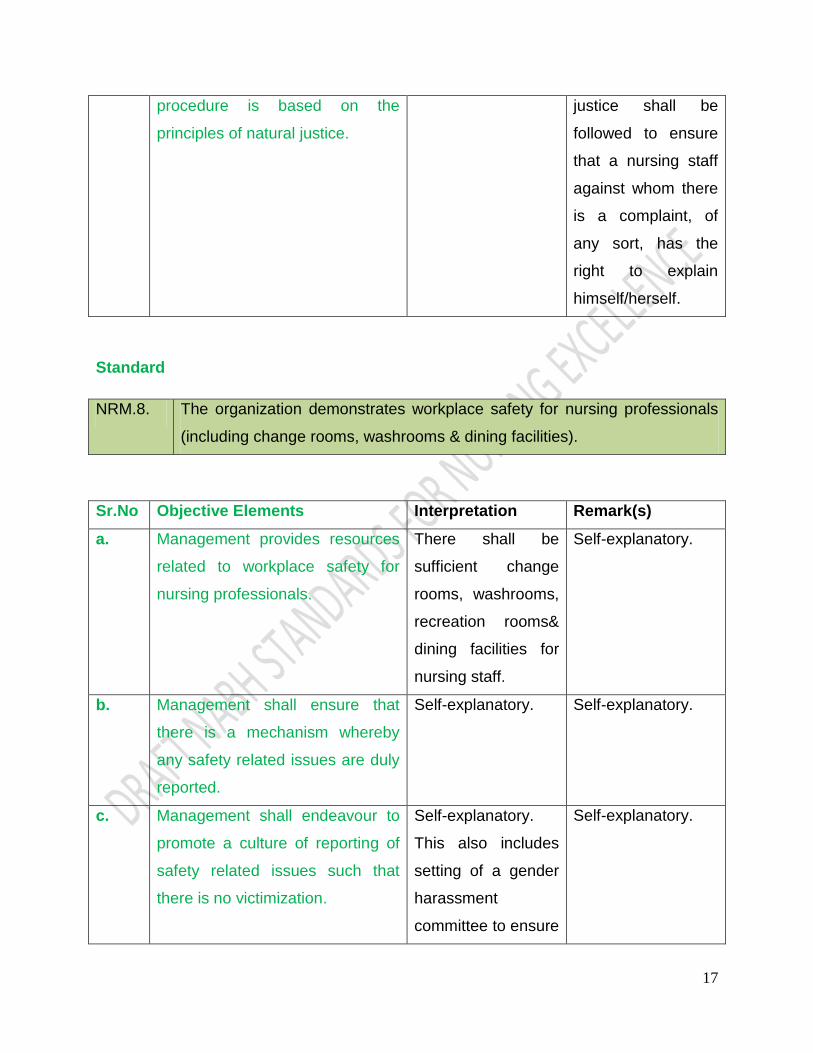
c. The disciplinary policy and Self-explanatory. Principles of natural
17
procedure is based on the
principles of natural justice.
justice shall be
followed to ensure
that a nursing staff
against whom there
is a complaint, of
any sort, has the
right to explain
himself/herself.
Standard
NRM.8. The organization demonstrates workplace safety for nursing professionals
(including change rooms, washrooms & dining facilities).
Sr.No Objective Elements Interpretation Remark(s)
a. Management provides resources
related to workplace safety for
nursing professionals.
There shall be
sufficient change
rooms, washrooms,
recreation rooms&
dining facilities for
nursing staff.
Self-explanatory.
b. Management shall ensure that
there is a mechanism whereby
any safety related issues are duly
reported.
Self-explanatory. Self-explanatory.
c. Management shall endeavour to
promote a culture of reporting of
safety related issues such that
there is no victimization.
Self-explanatory.
This also includes
setting of a gender
harassment
committee to ensure
Self-explanatory.
18
workplace safety
from sexual
harassments.
d. A record of corrective and
preventive actions shall be
maintained wherever appropriate,
with due consideration given to
anonymity.
Self-explanatory. Self-explanatory..
Standard
NRM.9.
The organization has a documented and established grievance handling
system.
Sr.No Objective Elements Interpretation Remark(s)
a. The organization has a well-
defined process for handling
nurse (s) grievances.
Self-explanatory. Self-explanatory.
b. The nursing professionals are
educated about the mechanisms
available for addressing
grievances.
Self-explanatory. Self-explanatory.
c. The head of the nursing service
protects nurse (s) rights.
Self-explanatory. Self-explanatory.
d. The nursing professionals are
educated about their rights.
Self-explanatory. Self-explanatory.

19
CHAPTER: 2
NURSING CARE OF PATIENT
Intent of the chapter:
The standard aims to guide and encourage patient safety and quality care as the
overall principle for providing nursing care to patients.
The organization supports nursing service to provide systematic method of nursing care
with specific emphasis on Assessment, Planning, Implementation and Evaluation.
Nursing care is preventive, promotive, curative and rehabilitative in nature. Patient-
centered care supports active involvement of patients and their families in the design of
new care models and in decision-making about individual options for treatment.
The registered nurse, in collaboration with the patient, family and other team members
assesses, makes decisions, plans, implements, evaluates, and documents nursing care
based on reflection, current knowledge, and best practices.
Policies and procedures in concurrence with the laws and regulation guide the nursing
services in all functional units applicable in the organization.
Patient safety and nursing professionals safety is intertwined in every aspect of the
care. Nursing professionals practice in accordance with the Code of Ethics for
Registered Nursing professionals, establishes professional therapeutic relationships
with patients and advocates for and with patients throughout their interactions with the
health system.
Nursing services promote and initiate measures to create a learning environment that
supports patient advocacy and ethical practice.
Uniform nursing care is provided to all patients in different settings that include care
provided in outpatient units, various categories of wards, intensive care units, procedure
rooms, operation theatre, etc.
20
A designated senior nursing professional controls the care of vulnerable patients
(elderly, physically and/or mentally-challenged and children), patients undergoing
moderate sedation, patients under restraints, and end of life care.
Pain management is also addressed with a view to providing comprehensive health
care.
Empowered Nursing professionals embrace the concepts of managing patient and
nursing care situations with dignity and mutual respect which produces strong and
efficient nursing leaders within the organization thereby ensuring safe and quality
nursing care.

21
Summary of Standard
NCP.1. Nursing manual shall be established and reviewed periodically as defined by
the HCO.
NCP.2. The initial assessment shall be done by the nursing professionals in
predetermined format at prescribed time and/or as per the needs of the
patients.
NCP.3. The reassessment shall be done by the nursing professionals in
predetermined format at prescribed time.
NCP.4. For provision of nursing care, appropriate number of nursing professionals
shall be maintained as per workload.
NCP.5. The nursing care planned and provided by the nursing professionals is
recorded.
NCP.6. The nursing care is individualized to address the needs of patient and family.
NCP.7. Information is exchanged and documented during each staffing shift,
between shifts, and during transfers between units/departments.
NCP.8. There shall be established policies and protocols for vascular access
devices. (VADs)
NCP.9. The nursing care of inpatients shall be supervised by senior nursing
professionals.
NCP.10. The nursing care of vulnerable patients (elderly, children, physically and/or
mentally challenged) shall be supervised by senior nursing professionals.
NCP.11. The nursing care of patients under restraints (physical and/or chemical) shall
be supervised by senior nursing professionals.
NCP.12. Appropriate pain management practices shall be supervised by senior
nursing professionals.
NCP.13. Appropriate end of life care shall be provided to patients needing the same
by the nursing professionals.

22
Standards and Objective Elements
Standard
NCP.1. A Nursing Manual shall be established and reviewed periodically as defined
by HCO
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing manual shall include
standard operating procedures
and guidelines for nursing care in
all settings.
Separate nursing
manual should be
prepared for all the
nursing areas like
ICU, OT, Dialysis,
ED, BMT,
Chemotherapy,
Endoscopy , Day-
care etc.
Self-explanatory.
b. Nursing manual shall also include
policy on nursing station
management.
Self-explanatory. This shall cover
Dressing trolleys
arrangement, Nurse
call system, record
maintenance, Crash
Cart arrangement.
c. Nursing manual shall contain a
master list of various forms and
formats used by nursing
professionals.
Self-explanatory. Self-explanatory.
d. Nursing manual shall be available
for and followed by the nursing
professionals uniformly.
Self-explanatory. Self-explanatory.
e. Nursing manual shall be reviewed Self-explanatory. Should incorporate

23
and updated regularly at least
once in annually.
changing national,
international
guidelines time to
time and GCP.
Standard
NCP.2.
The initial assessment shall be done by the nursing professionals in
predetermined format at prescribed time and/or as per the needs of the
patients.
Sr.No Objective Elements Interpretation Remark(s)
a. Initial assessment of in-patients
includes nursing assessment
done and documented at the time
of admission.
This shall identify
the nursing needs
and also help
identify any special
needs of the patient.
It shall be
completed within a
defined time frame.
This assessment
shall help in
identifying the
nursing needs of the
patient.
A checklist or
template could be
used for the same.
b. Initial assessment includes
assessment of actual and
potential needs & problems.
This include head to
foot observation,
checking of vitals,
height, weight ,
input – output charts
24
and special needs
etc.
c. The initial nursing assessment
results in a documented nursing
care plan.
This shall be
documented by the
assigned nursing
staff in the patient
record.
For definition of
“nursing care plan”
refer to glossary.
d. The care documentation must
include preventive aspects of the
care where appropriate.
The documented
nursing care plan
should cover
preventive actions
as necessary in the
case and could
include diet, drugs,
etc.
In conditions where
it is not possible to
incorporate this at
the time of
assessment (e.g.
diagnosis not made/
unclear) the same
shall be done as
soon as a definite
diagnosis is arrived
at.
This could also be
done through
booklets/patient
information leaflets
etc.
Standard
NCP.3. The reassessment shall be done by the nursing professionals in a
predetermined format at prescribed time.
25
Sr.No Objective Elements Interpretation Remark(s)
a. Patients are reassessed at
appropriate intervals.
After the initial
assessment, the
patient is
reassessed
periodically and this
is documented in
the case sheet. The
frequency may be
different for different
areas based on the
setting and the
patient‟s clinical
condition and
requirements, e.g.
patients in ICU and
ER need to be
reassessed more
frequently
compared to a
patient in the ward.
Reassessments
shall also be done
in response to
significant changes
in patient‟s
condition.
Every patient shall
be reassessed at
least once every
shift by the caring
nurse.
Reassessments
shall be done for
day care patients
(Before discharging)
or patients awaiting
admission/ bed.
b. Patients are reassessed at the
time of receiving and transferring
Self-explanatory. Self-explanatory.

26
from one unit to another.
c. Patients are also reassessed
before and after shifting for
investigations.
Self-explanatory. Self-explanatory.
d. Nursing care plan is modified
when emergency situations arise.
Self-explanatory. Self-explanatory.
e. Nursing professionals evaluate
outcomes using reassessment
and revise action plans as
needed.
Self-explanatory. Self-explanatory.
Standard
NCP.4. For provision of nursing care, appropriate number of nursing professionals
shall be maintained as per workload.
Sr.No Objective Elements Interpretation Remark(s)
a. Nurse patient ratio is planned and
provided based on the scope of
the unit.
The ratio should be
as per the
guidelines laid down
by Indian Nursing
Council.
Self-explanatory.
b. Nurse patient ratio is monitored in
every shift by the designated
senior nursing professionals.
Self-explanatory. Self-explanatory
c. Patient condition and nurse‟s
competency shall be considered
while assigning nursing
professionals to patient care in
each shift.
Self-explanatory.
Patient assignment
is followed where
ever possible.
Self-explanatory.
27
Standard
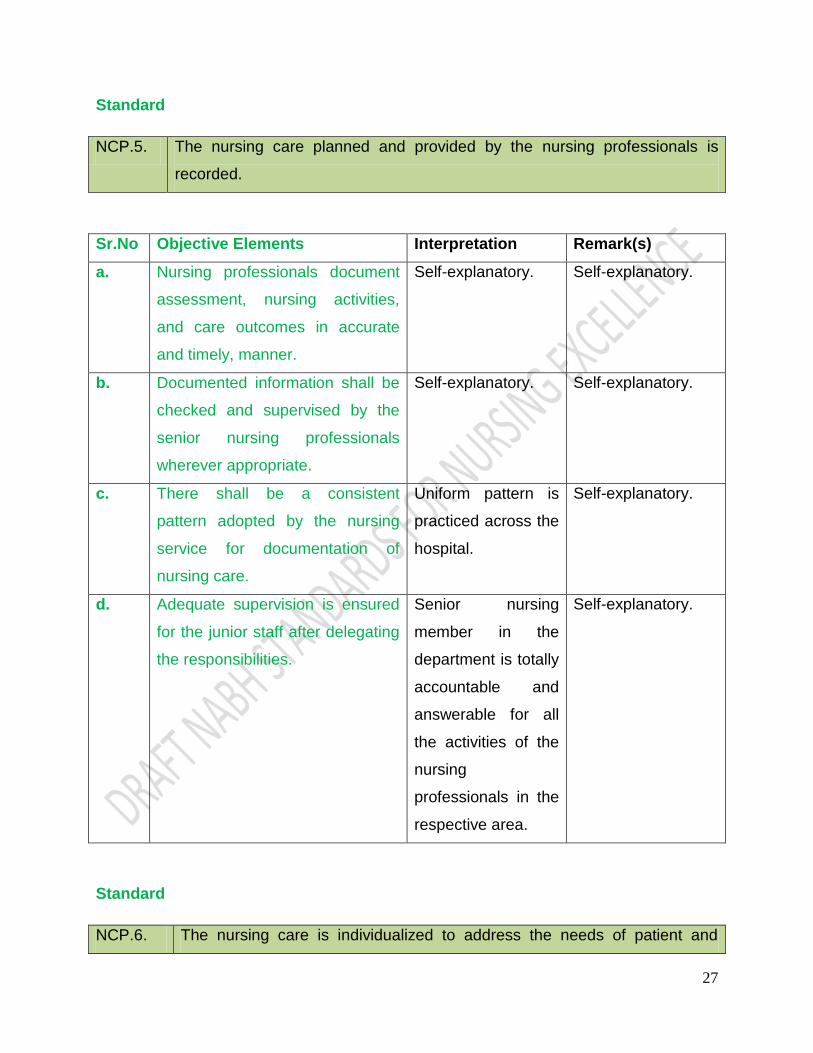
NCP.5. The nursing care planned and provided by the nursing professionals is
recorded.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing professionals document
assessment, nursing activities,
and care outcomes in accurate
and timely, manner.
Self-explanatory. Self-explanatory.
b. Documented information shall be
checked and supervised by the
senior nursing professionals
wherever appropriate.
Self-explanatory. Self-explanatory.
c. There shall be a consistent
pattern adopted by the nursing
service for documentation of
nursing care.
Uniform pattern is
practiced across the
hospital.
Self-explanatory.
d. Adequate supervision is ensured
for the junior staff after delegating
the responsibilities.
Senior nursing
member in the
department is totally
accountable and
answerable for all
the activities of the
nursing
professionals in the
respective area.
Self-explanatory.
Standard
NCP.6. The nursing care is individualized to address the needs of patient and

28
family.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing protocols are developed
by nursing professionals based on
current best practices and shall
focus on patient safety.
Self-explanatory. Self-explanatory.
b. Assignment of patients for nursing
care is based on patient needs to
maximize the outcome.
Self-explanatory. Self-explanatory.
c. Nurse use patient specific
sensitive communication and
interactive techniques to
individualize the care.
Self-explanatory Self-explanatory.
d. Care of patients is coordinated in
all care settings within the
organization.
Care of patients is
co-ordinated among
various care-
providers in a given
setting viz OPD,
emergency,IP, ICU,
etc.
The organization
shall ensure that
there is effective
communication of
patient
requirements
amongst the care-
providers in all
settings.
29
Standard
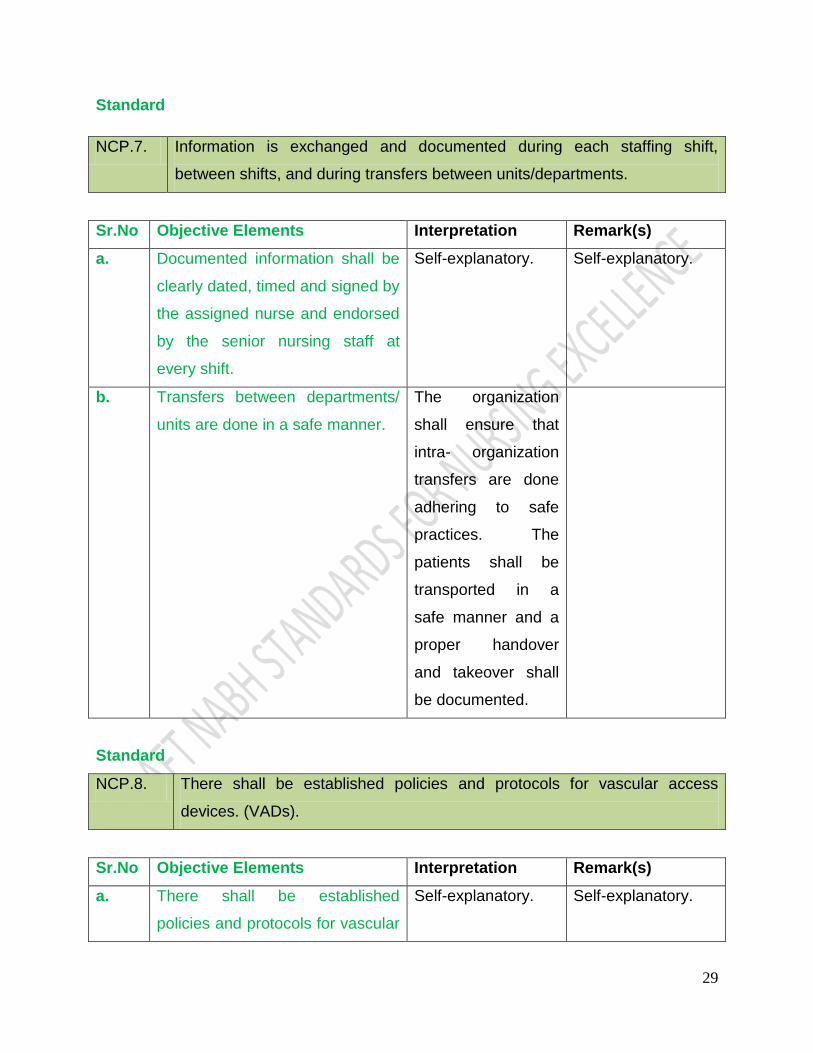
NCP.7. Information is exchanged and documented during each staffing shift,
between shifts, and during transfers between units/departments.
Sr.No Objective Elements Interpretation Remark(s)
a. Documented information shall be
clearly dated, timed and signed by
the assigned nurse and endorsed
by the senior nursing staff at
every shift.
Self-explanatory. Self-explanatory.
b. Transfers between departments/
units are done in a safe manner.
The organization
shall ensure that
intra- organization
transfers are done
adhering to safe
practices. The
patients shall be
transported in a
safe manner and a
proper handover
and takeover shall
be documented.
Standard
NCP.8. There shall be established policies and protocols for vascular access
devices. (VADs).
Sr.No Objective Elements Interpretation Remark(s)
a. There shall be established
policies and protocols for vascular
Self-explanatory. Self-explanatory.
30
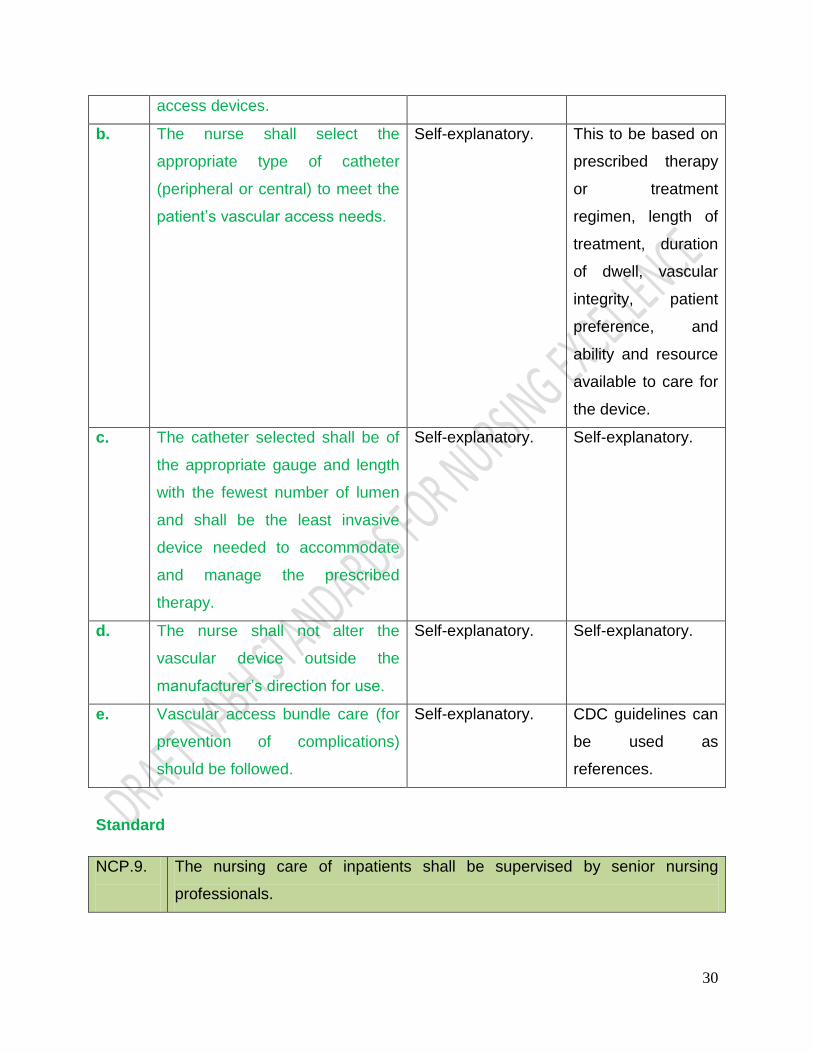
access devices.
b. The nurse shall select the
appropriate type of catheter
(peripheral or central) to meet the
patient‟s vascular access needs.
Self-explanatory. This to be based on
prescribed therapy
or treatment
regimen, length of
treatment, duration
of dwell, vascular
integrity, patient
preference, and
ability and resource
available to care for
the device.
c. The catheter selected shall be of
the appropriate gauge and length
with the fewest number of lumen
and shall be the least invasive
device needed to accommodate
and manage the prescribed
therapy.
Self-explanatory. Self-explanatory.
d. The nurse shall not alter the
vascular device outside the
manufacturer‟s direction for use.
Self-explanatory. Self-explanatory.
e. Vascular access bundle care (for
prevention of complications)
should be followed.
Self-explanatory. CDC guidelines can
be used as
references.
Standard
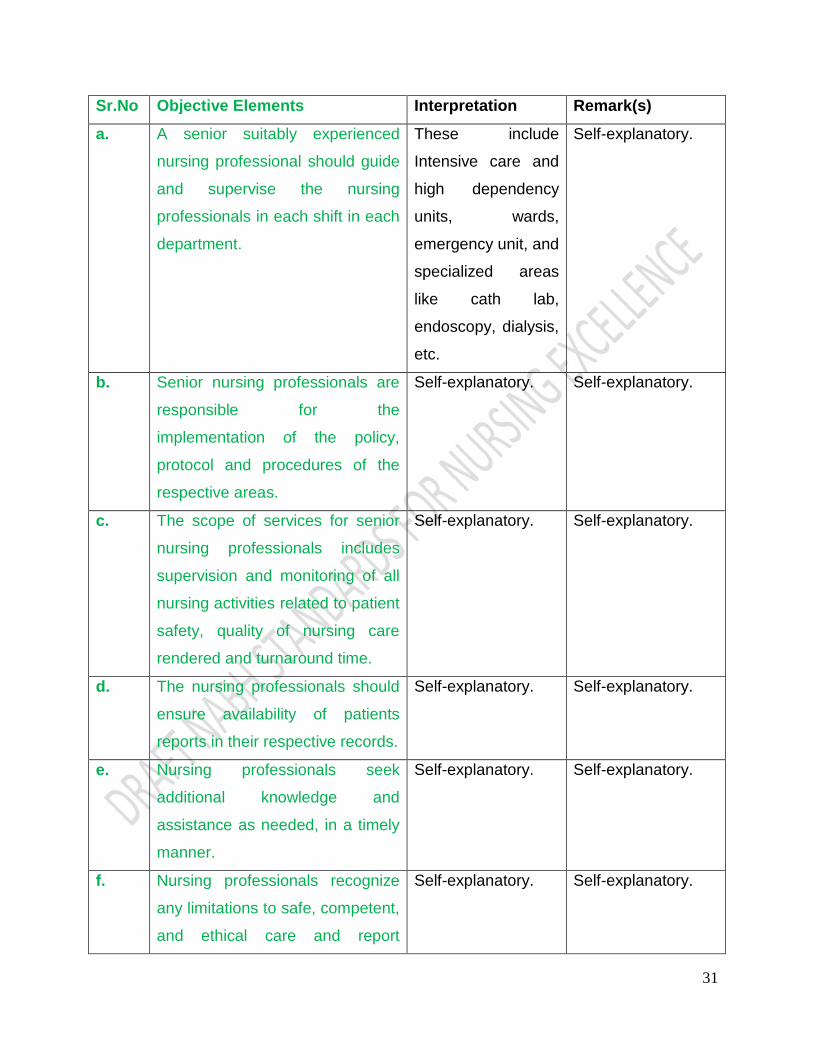
NCP.9.
The nursing care of inpatients shall be supervised by senior nursing
professionals.
31
Sr.No Objective Elements Interpretation Remark(s)
a. A senior suitably experienced
nursing professional should guide
and supervise the nursing
professionals in each shift in each
department.
These include
Intensive care and
high dependency
units, wards,
emergency unit, and
specialized areas
like cath lab,
endoscopy, dialysis,
etc.
Self-explanatory.
b. Senior nursing professionals are
responsible for the
implementation of the policy,
protocol and procedures of the
respective areas.
Self-explanatory. Self-explanatory.
c. The scope of services for senior
nursing professionals includes
supervision and monitoring of all
nursing activities related to patient
safety, quality of nursing care
rendered and turnaround time.
Self-explanatory. Self-explanatory.
d. The nursing professionals should
ensure availability of patients
reports in their respective records.
Self-explanatory. Self-explanatory.
e. Nursing professionals seek
additional knowledge and
assistance as needed, in a timely
manner.
Self-explanatory. Self-explanatory.
f. Nursing professionals recognize
any limitations to safe, competent,
and ethical care and report
Self-explanatory. Self-explanatory.

32
concerns and consult and/or
initiate appropriate changes as
necessary.
g. Nursing professionals evaluate,
disseminate, and support the
integration of evidence based
practice findings into practice.
Self-explanatory. Self-explanatory.
Standard
NCP.10. The nursing care of vulnerable patients (elderly, children, physically and/or
mentally challenged) shall be supervised by senior nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)
a. There are protocols governing
care of vulnerable patient.
Self-explanatory. Self-explanatory.
b. The nursing staffs are trained to
care for vulnerable patient.
Self-explanatory. Self-explanatory.
c. All vulnerable patients are
identified as per HCO policy and
then assessed and reassessed
more frequently at periodic
intervals.
Self-explanatory. Self-explanatory.
d. Nursing professionals monitor
vulnerable patients‟ closely
participating with the family
whenever required.
Self-explanatory. Self-explanatory.

33
Standard
NCP.11.
The nursing care of patients under restraints (physical and/or chemical) shall
be supervised by senior nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)
a. These include both physical and
chemical restraint measures.
Self-explanatory. Self-explanatory.
b. These patients are more
frequently monitored.
Self-explanatory. Self-explanatory.
c. Staff receives training and
periodic updating in control and
management of restraint
techniques.
Self-explanatory. Self-explanatory.
Standard
NCP.12. Appropriate pain management practices shall be supervised by senior
nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)
a. All patients screened for pain at
the time of admission and
reassessment of pain is done for
those patients who require pain
management.
Self-explanatory. Self-explanatory.
b. Nursing professionals are trained
to identify level of pain in various
categories of patients and
document the same.
Self-explanatory. Self-explanatory.
c. Nursing professionals shall Self-explanatory. Self-explanatory.

34
provide care both
pharmacological and non-
pharmacological care based on
the hospital policy.
d. The organization respects and
supports nursing management of
pain for such patients.
Self-explanatory. Self-explanatory.
e. The nursing professionals
educate the patient and their
family on various pain
management techniques
wherever appropriate.
Self-explanatory. Self-explanatory.
Standard
NCP.13. Appropriate end of life care shall be provided to patients needing the same
by the nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing professionals are aware
of end of life care policy of the
organization.
Self-explanatory. Self-explanatory.
b. Nursing professionals shall
provide care to meet the unique
end of life care needs of the
patient and family.
Social and spiritual
needs of the family
need to be
considered.
Self-explanatory.
c. Symptomatic treatment is
provided by the nursing
professionals for all end of life
care patients with special
emphasis on alleviating pain and
Self-explanatory. Self-explanatory.

35
helping them to cope
psychologically.
d. Nursing professionals are
educated and periodically trained
on end of life care.
Self-explanatory. Self-explanatory.
36
CHAPTER: 3
MEDICATION OF MANAGEMENT
Intent of the chapter:
Designated nursing personnel shall be consulted during policy formulation pertaining to
pharmacy and management of medication. The nursing staff will ensure availability,
safe storage, administration of medications and monitoring the effects of medication.
The nursing personnel should have an oversight of all medications stocked in the ward
and other clinical areas and should ensure good inventory control practices including
correct storage (as regards to temperature, look-alike, sound-alike etc.), monitoring
expiry dates and maintenance of documentation in the clinical areas.
The availability of emergency medication is stressed upon. The organization should
have a mechanism to ensure that the emergency medications are standardized
throughout the organization, readily available and replenished in a timely manner. There
should be a monitoring mechanism to ensure that the required medications are always
stocked and well within expiry dates. Appropriate nursing authorities should monitor
these parameters in all areas where drugs and consumables are stored or utilized.
Every high-risk medication order should be verified by an appropriate person so as to
ensure accuracy of the dose, frequency and route of administration. The “appropriate
person” could be another doctor, trained nurse or preferably, a clinical pharmacist. Such
a person would also look for drug-drug interactions, food-drug interactions, renal or
hepatic dosing etc. There should be a mechanism by which this person could verify the
order with prescriber in case of doubts or clarifications. The verification should occur
before the medication is administered but preferably, prior to dispensing of the
medication. There should be a protocol by way of which, in case of continued conflict,
the person can approach higher authority to ensure patient safety.
37
The process also includes monitoring of patients after administration and procedures for
reporting and analyzing medication errors. Process should include duration of
monitoring after administration of high alert medication and medication used for
managing pain.
Safe use of high-risk medication like narcotics, chemotherapeutic agents and
radioactive isotopes are guided by policies and procedures.
Patients and family members are educated about safe medication. Medications also
include blood, chemotherapy and self-administered medication.
There shall be a policy on verbal orders which would enable nursing professionals to
accurately capture all verbal orders affecting care of patients. Nursing professionals will
report and closely monitor the occurrence of adverse events including adverse drug
event.

38
Summary of standards
MOM.1. Indenting of required medication and stores will be done and supervised by
nursing staff made responsible for this function. Storage of medication in
the wards and other therapeutic areas shall be supervised by responsible
nursing professionals.
MOM.2. The dispensing, administration and accounting of medicines shall be carried
out by the concerned personnel and should be appropriately supervised by
senior nursing staff.
MOM.3. The monitoring of patients after medication administration is supervised by
responsible personnel.
MOM.4. The nursing professionals must report near misses, medication errors and
adverse drug events as per the policy of the HCO for analysis by the
appropriate staff predefined and identified by the HCO. Feedback is
provided to staff which includes the results of analysis and recommended
preventive measures for implementation by the nursing staff wherever
appropriate.
MOM.5. The organization shall ensure that it has a policy on verbal orders which will
be applicable to doctors, nursing professionals and technicians uniformly.

39
Standards and Objective Elements
Standard
MOM.1. Indenting of required medication and stores will be done and supervised by
nursing staff made responsible for this function. Storage of medication in
the wards and other therapeutic areas shall be supervised by responsible
nursing professionals.
Sr.No Objective Elements Interpretation Remark(s)
a. Medication will be indented as per
HCO policy on indenting
medicines.
Nursing
professionals
should be aware of
the reorder policy of
the HCO including
for critically low
stocks.
The senior nurse in
a ward / dept.
should monitor
appropriateness of
indents whenever
generated from the
IPD or departments.
b. Medications are stored in a clean,
safe and secure environment; and
incorporating manufacturer‟s
recommendation(s).
The organization
shall also ensure
that the storage
requirements of the
drug as specified by
the manufacturer
are adhered to. This
shall be applicable
to all areas where
medications are
stored including
wards.
Medications shall be
protected from loss
Vaccines could
preferably be kept in
vaccine refrigerators
(Ice Lined
Refrigerator).
Where appropriate,
temperature
monitoring of the
storage
area/refrigerator
shall be done at
least once a day. In
case of areas which
are not open all

40
or theft. The overall
ventilation,
cleanliness of the
storage area shall
be maintained.
days, it shall be
done on all working
days.
To check for loss or
theft the
organization could
conduct audits at
regular intervals (as
defined by the
organization) to
detect such
instances.
c. Sound inventory control practices
guide storage of the medications.
Organization shall
follow or
demonstrate ABC,
VED, FSN, FIFO-
led time analysis,
etc. The medicines
shall be stored in
alphabetical or
company‟s name.
First expiry and first
Out policy should be
adhered to.
Nursing
professionals will be
trained and made
aware regarding the
need to adhere to
sound inventory
management
practices.
d. Sound-alike and look-alike
medications are identified and
stored separately.
Many drugs in
ampoules, vials or
tablets may look-
alike or sound-alike.
They should be
documented,
segregated and
The organization
can follow a method
of storing drugs by
generic name in an
alphabetical order to
address this issue.
41
stored separately at
all locations.
An effort to address
this issue should be
made while defining
the formulary and
during the
procurement of
drugs.
The list will have to
be identified at
regular intervals
depending on the
changes in the
formulary and
changes in
packaging (in case
of look-alike).
e. The list of emergency medications
is defined and is stored in a
uniform manner.
This list shall be
prepared in
consonance with
good clinical
practices and
documented. List of
drugs shall be
uniform across the
organization,
however the
quantity can differ.
A crash cart would
help the
organization to store
these medications
in a standardized
manner, i.e. the
rows and drawers
have defined
medicines.
No other drugs shall
be kept stored with
emergency
medications.
f. Emergency medications are
available all the time.
Adequate quantity
of emergency
medicines should
be stocked at all
times. Re-order
level at definite
quantity should be
clearly delineated.
Nursing staff must
know from where to
obtain emergency
medicines in the
eventuality of a
stock out during
hours when the
pharmacy / medical
stores may be

42
closed.
g. Emergency medications are
replenished in a timely manner
when used.
Self-explanatory.
An inventory check
shall be done at
least daily to ensure
this.
In case the
organization follows
a system of sealing
the emergency cart
then the check shall
be carried out
before re-sealing
every time.
Standard
MOM.2.
The dispensing, administration and accounting of medicines shall be carried
out by the concerned personnel and should be appropriately supervised by
senior nursing staff.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing professionals are familiar
with the medications being used
for their patients.
E.g.
dosages, route, time,
frequency of
administration
special
precautions,
dilution
requirements,
various
administration
methods and
requirement.
Self-explanatory.
b. Prepared medication is labelled
prior to preparation of a second
Self-explanatory.
Applicable
especially for

43
drug.
parenteral drugs,
anesthetic drug
preparation in
OTs, antibiotics,
chemotherapy and
high risk drugs
c. Patient is identified prior to
administration.
Self-explanatory.
Identification shall be
done by unique
identification number
(e.g. hospital
number/IP number,
etc.) and/or name.
d. Medication is verified from the
order prior to administration.
Staff administering
medications should
go through the
treatment orders
before administration
of the medication and
then only administer
them. It is preferable
that they also check
the general
appearance of the
medication (e.g.
melting, clumping
etc.) before
dispensing.
If any of the
parameters with
respect to an order
namely name,
dose, route or
frequency/time are
missing/incomplete
the medication
administration
shall be deferred.
However, to
ensure that patient
care does not
suffer a verbal
order may be got
from the treating
doctor followed by
ratification of the

44
same (refer to
MOM 4i).
In case of high risk
medication(s), the
verification shall be
done by at least
two staff (nurse-
nurse or nurse-
doctor)
independently and
documented.
e. Dosage is verified from the order
prior to administration.
Self-explanatory.
Self-explanatory.
f. Route is verified from the order
prior to administration.
Self-explanatory.
Where applicable
the site of
administration
shall also be
verified.
g. Timing is verified from the order
prior to administration.
Self-explanatory.
The organization
needs to define the
timing of
administration of
medications. For
example, o.d, b.i.d,
t.i.d, q.i.d, h.s.
h. Patient is monitored during the
administration of blood and blood
products, chemotherapy and
other invasive procedure.
IPD protocols should
identify the
parameters to be
monitored during
administration of
medications.
Nursing
professionals
should be trained
to recognize alerts
for individual
medications that

45
may be used
infrequently in their
wards /
departments.
I. Medication administration is
recorded.
The organization
shall ensure that this
is done in a uniform
location and it shall
include the name of
the medication,
dosage, route of
administration, timing
and the name and
signature of the
person who has
administered the
medication.
In case of infusions,
it shall capture the
start time, the rate of
infusion and end
time.
The records shall
reflect the actual
administration. For
example, if brand
Y was given in
place of brand X
(same generically)
the documentation
shall be of brand
Y. Similarly, if the
order was for a
tablet of 250 mg
but the
administration was
½ a tablet of 500
mg the latter shall
be documented.
Standard
MOM.3.
The monitoring of patients after medication administration is supervised by
responsible personnel.
Sr.No Objective Elements Interpretation Remark(s)
a. Monitoring of patients shall be
done after medication
Nursing
professionals
This covers drugs
including high risk
46
administration. should be familiar
with common
adverse drug
reactions of
medications.
They should know
how to recognize an
anaphylactic , any
other adverse drug
reaction and the
immediate response
required; both
therapy and
escalation.
medicines.
Senior nursing staff
should supervise
the junior nursing
professionals
involved in
monitoring critically
ill and post op
patients.
b. Monitoring of patients shall be
done after transfusion of blood
and blood products.
Self-explanatory. Self-explanatory.
c. Monitoring of patients shall be
done after chemotherapy.
Self-explanatory. Self-explanatory.
d. Monitoring of patients shall be
done in all post-operative cases
or where invasive procedures are
carried out.
Self-explanatory. Nursing
professionals must
be trained to carry
out a step wise de-
escalation of
monitoring
parameters based
on clinical
directions.

47
Standard
MOM.4. The nursing professionals must report near misses, medication errors and
adverse drug events as per the policy of the HCO for analysis by the
appropriate staff predefined and identified by the HCO. Feedback is provided
to staff which includes the results of analysis and recommended preventive
measures for implementation by the nursing staff wherever appropriate.
Sr.No Objective Elements Interpretation Remark(s)
a. A system shall exist to capture
near miss, medication error and
adverse drug reactions.
Self-explanatory. Self-explanatory.
Nursing
professionals and
paramedical staff
should be aware of
the reporting
methods, measures
and criteria being
used by the
hospital.
b. These are reported within a
specified time frame.
Self-explanatory. Self-explanatory.
c. They are collected and analysed
by appropriately trained
personnel.
Committees or
teams analysing
adverse events in
wards or related to
nursing activites
must have
representation of
senior nursing
professionals.
Self-explanatory.

48
d. Corrective and/or preventive
action(s) are taken based on the
analysis where appropriate.
A feedback
mechanism is
standardized in the
hospital.
Nursing
professionals and
paramedical staff
are aware of the
feedback
mechanism and
acknowledge the
feedback
appropriately.
Standard
MOM.5. The organization shall ensure that it has a policy on verbal orders which will
be applicable to doctors, nursing professionals and technicians uniformly.
Sr.No Objective Elements Interpretation Remark(s)
a. The organization shall have a
policy to address verbal orders.
Self-explanatory. This will be
applicable to
doctors, nursing
professionals and
technicians
uniformly.
b. The policy shall address who can
give verbal orders and how these
orders will be validated.
Self-explanatory. Self-explanatory.
c. Organization should have
approved list of drugs which can
be ordered verbally.
Self-explanatory. Nursing
professionals
should be familiar
with this list.
d. No verbal orders shall be followed
except in case of emergency, or
Self-explanatory. Self-explanatory.
49
as defined by organization.
e. Where verbal orders are given,
ratification shall be done at the
earliest and not later than 24 hrs.
Self-explanatory. Nursing
professionals
should be
empowered to seek
endorsements by
the clinicians within
the specified
timeframe.
50
CHAPTER: 4
EDUCATION, COMMUNICATION AND GUIDANCE
Intent of the chapter:
The organization shall ensure that nursing professionals are trained in communication
skills. Patients are informed of their rights and educated about their responsibilities at
the time of admission. They are informed about the disease, the possible outcomes and
are involved in decision making. The patients are educated about the mechanisms
available for addressing grievances.
Patient and families have a right to information and education about their healthcare
needs in a language and manner that is understood by them and proper timely
guidance shall be given by the nursing staff.

51
Summary of standard
ECG.1. The organization shall ensure that nursing professionals are trained in
communication skills.
ECG.2. Nursing professionals shall maintain confidentiality of all patient information.
ECG.3. Nursing professionals communicate with patient, family and relevant team
members to reflect continuity of care as and when required.
ECG.4. Patient and family are educated where essential and in case of any change
in nursing care plan.
52
Standards and Objective Elements
Standard
ECG.1. The organization shall ensure that nursing professionals are trained in
communication skills.
Sr.No Objective Elements Interpretation Remark(s)
a. There is documented evidence of
communication skills training to
nursing staff to meet the patient‟s
specific needs.
Self-explanatory. Self-explanatory.
b. The communication needs of
patients who speak different
language than the care givers is
addressed.
This shall be
identified in a timely
manner and
addressed using
resources
supported by the
management.
Self-explanatory.
c. Training is imparted to address
the patient‟s needs with impaired
communication.
Self-explanatory. Self-explanatory.
d. Communication skill shall be
improved periodically.
Self-explanatory. Self-explanatory.
Standard
ECG.2. Nursing professionals are aware of their responsibility in protecting patient
rights.
Sr.No Objective Elements Interpretation Remark(s)

53
a. The nursing professionals are
aware of patient rights.
The nursing
professionals are
made aware of
patient and family
rights at the time of
induction.
Self – explanatory.
b. Nursing professionals maintain
the confidentiality of patients
information.
Self-explanatory. Self-explanatory.
c. Nursing professionals maintain
privacy of the patients during
care.
Self-explanatory.
Female nurse will
give care to male
patient only if
another female staff
or family member is
present. Same
holds true vice
versa for male
patient. The same
holds true when a
male nurse provides
care for a female
patient.
Self-explanatory.
d. The nursing professionals support
individual patient and family
beliefs, values and customs and
involve the patient and family in
decision making processes.
Self-explanatory. Self-explanatory.

54
Standard
ECG.3. Nursing professionals communicate as and when required with relevant
team members to achieve continuity of care.
Sr.No Objective Elements Interpretation Remark(s)
a. There is a handover mechanism
among the care team across
shifts regarding patient‟s status.
Self-explanatory. Self-explanatory.
b. Nursing professionals
communicate with staff in other
departments when required to
ensure that care plan is
implemented.
This shall include
relevant aspects of
care plan to
facilitate inter-
departmental
activities and avoid
delays.
This includes
patient transfers,
requisitioning
bedside services
etc.
c. HCO uses predetermined formats
for such communication wherever
required.
Self-explanatory. Self-explanatory.
Standard
ECG.4. Patient and family are educated where essential and in case of any change
in nursing care plan.
Sr.No Objective Elements Interpretation Remark(s)
a. Patient and family education
includes aspects of care plan.
This shall include
information on
relevant aspects of
care plan such as
This is documented
wherever essential.

55
safe and effective
use of medications,
food drug
interactions, diet
and nutrition,
immunisations, etc.
and preventive
aspects.
b. The education shall cover the
medical condition, pre and post-
operative education, special
procedures, preventing healthcare
associated infections, when to
seek urgent medical attention and
home care wherever applicable.
Self-explanatory. This could be done
through patient
education booklets /
videos/ leaflets, etc.
c. Nursing professionals explain to
patient/ family before any
procedures are performed on
patients.
Self-explanatory. Self-explanatory.
d. Nursing professionals ensure
written informed consent
wherever essential.
This should be
ensured for all
invasive
procedures, blood
and blood product
transfusions and
prior to
administration of
anaesthesia.
Self-explanatory.
e. Patient and/or family are
educated in a language and
format that they can understand.
Self-explanatory. Self-explanatory.

56
CHAPTER: 5
INFECTION CONTROL PRACTICES
Intent of the chapter:
The standards guide the provision of an effective infection control programme in the
organization. There shall be a designated Infection control nurse.
The organization provides proper facilities and adequate resources to support the
Infection Control Practices.
The practices includes an action plan to minimize hospital acquired infections, control
outbreaks, disinfection/ sterilization activities and their monitoring, biomedical waste
(BMW) management, employee health and training of nursing staff.

57
Summary of Standard
ICP.1. Infection control nurse (s)shall be designated by the organization
ICP.2. Nursing professionals shall adhere to standard precautions and hand
hygiene guidelines at all times.
ICP.3. The nursing professionals shall adhere to handling, storage and disposal of
bio medical waste as per the bio medical waste management Act, 1998.
ICP.4. The designated nursing staff shall perform surveillance activities to capture
and monitor infection control and prevention data.
ICP.5. Isolation (barrier and reverse barrier nursing) practices shall be supervised
by senior nursing professionals.
ICP.6. Infection Control Nurse maintains records of all occupational injuries and
pre- and post-exposure prophylaxis.
58
Standards and Objective Elements
Standard
ICP.1. Infection control nurse (s) shall be designated by the organization
Sr.No Objective Elements Interpretation Remark(s)
a. The criteria for designating ICN
shall be based on qualification or
training.
Self-explanatory.
Ideally there should
be at least one
Infection control
Nurse for every 200
operational beds.
Self-explanatory.
b. Infection control nurse (s) shall
have specialized training (internal
or external) in hospital infection
control.
Self-explanatory. Self-explanatory.
c. Infection control nurse (s) shall
have documented role and
responsibilities.
Self-explanatory. Role of ICN (s) is
identified and
commensurate with
the Infection Control
Program needs of
Healthcare
Organization.

59
Standard
ICP.2. Nursing professionals shall adhere to standard precautions and hand
hygiene guidelines at all times.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing professionals are trained
in standard precautions and hand
hygiene guidelines.
The organization
shall adhere to
international /
national guidelines
on hand hygiene.
A good reference is
the WHO guidelines
of 2009.
The organization
could display the
necessary
instructions near
every hand washing
area.
b. Nursing professionals shall be
conversant with Personal
protective equipment (PPE) and
their use.
Self-explanatory.
They should be
available at the
point of use and the
organization shall
ensure that it
maintains an
adequate inventory.
Personal protective
equipment includes:
1. Gloves
2. protective eye
wear
(goggles)
3. Mask
4. apron
5. gown
6. boots/shoe
cover, and
7. cap/ hair
cover.
c. The organization audits
compliance to standard
precautions and hand hygiene
This shall be done
at a minimum once
every month. An
A good tool for hand
hygiene monitoring
is the WHO‟s “Hand

60
practices. appropriate sample
size shall be chosen
and all categories of
staff (involved in
direct patient care)
shall be monitored.
Hygiene Observation
Form”.
Another tool that can
be utilised is use of
Infection control
assessment tool
(ICAT).
d. The nursing staff adheres to
cleaning, disinfection and
sterilization practices.
It shall be
addressed at all
levels of the
organization, e.g.
ward and OT. It is
preferable that the
organization follows
a uniform policy
across different
departments within
the organization.
Infection control
assessment tool
(ICAT) can be
utilised for
monitoring of
sterilisation and
disinfection
practices.
e. The nursing staff adheres to safe
linen management practices.
Self-explanatory. Nursing staff is
aware and use
appropriate PPE
while handling dirty
and soiled linen.
Nursing staff is
aware of safe
storage and
transport of used
linen.
f. The nursing staff adheres to the
safe injection practices.
Self-explanatory. Self-explanatory.
g. The senior nursing professionals Self-explanatory. ICAT may be used

61
along with other professionals
identified by the HCO monitor
safe linen management practices.
for such monitoring.
Standard
ICP.3.
The nursing professionals shall adhere to handling, storage and disposal of
bio medical waste as per the bio medical waste management Act, 1998.
Sr.No Objective Elements Interpretation Remark(s)
a. The organization ensures
provision for appropriate
biomedical waste management
practices.
Self-explanatory. Self-explanatory.
b. Where applicable municipal
waste (General waste) rules shall
be complied with by the nursing
personnel.
Self-explanatory. Self-explanatory.
c. Nursing professionals shall be
conversant with disposal of
Personal protective equipment
(PPE).
Self-explanatory.
Appropriate
segregation at the
point(s) of use shall
be done.
Disposal of personal
protective equipment
includes but not
limited to disposal of:
1. Gloves,
2. Protective eye
wear (goggles)
3. Mask,
4. Apron,
5. Gown,
6. Boots/shoe
cover, and

62
7. Cap/ hair cover.
Standard
ICP.4. The designated nursing staff shall perform surveillance activities to capture
and monitor infection control and prevention data.
Sr.No Objective Elements Interpretation Remark(s)
a. Surveillance activities are
appropriately directed towards the
identified high-risk areas and
procedures.
The organization
must be able to
provide evidence of
conducting periodic
surveillance
activities in its
identified high-risk
areas and
procedures.
It shall define the
frequency and
mode of
surveillance.
The surveillance
system should be
appropriate and
adhering to national
/ international
guidelines.
Surveillance
activities include
areas where
demolition,
The organization
should use a
judicious mix of
active and passive
surveillance.
The organization
could lay down the
parameters that
need to be captured
and the process for
reporting.
HCO may use ICAT
for monitoring
service areas like
surgical units,
intensive care units
and can also be
used for monitoring
isolation
precautions, care of
devices and
catheters etc.

63
construction or
repairs are
undertaken,
especially in high
risk areas.
b. Appropriate feedback regarding
HAI rates are provided on a
regular basis to appropriate
personnel.
The feedback shall
include the rates,
trends and
opportunities for
improvement. It
could also provide
specific inputs to
reduce the HAI rate.
This could be in the
form of a
bulletin/newsletter,
or periodic circulars
and meetings.
c. The surveillance activities include
monitoring of environment and
infection control indicators.
Self-explanatory.
This includes
monitoring of SSI,
VAP, CLABSI,
CAUTI.
d. The surveillance activities include
monitoring of cleaning,
sterilization and disinfection in
patient care units.
Self-explanatory.
This includes
monitoring of
terminal cleaning
procedures,
monitoring efficacy
of disinfectants in
use through
appropriate
measure.
Standard
ICP.5.
Isolation (barrier and reverse barrier nursing) practices shall be supervised
by senior nursing professionals.
64
Sr.No Objective Elements Interpretation Remark(s)
a. The organization provides
appropriate resources for isolation
practices.
The organization
shall define the
conditions where
isolation is required
and the conditions
wherein barrier
nursing or both are
required. The same
shall be carried out.
The organization
shall ensure that it
provides the
necessary
resources to carry
out the activity (e.g.
clothing, masks,
gloves, etc.).
Refer to glossary for
“isolation/barrier
nursing”.
Ideally patients
requiring isolation
(contact, droplet
and airborne)
should be placed in
isolation rooms and
droplet cases be
kept in negative
pressure rooms. An
air-conditioned
single room with an
exhaust or a well-
ventilated room is
an adequate option
for healthcare
facilities without
“negative pressure”
rooms. If an air-
conditioned single
room is not
available, a fan can
be placed in the
room to direct
airflow towards an
outside window.
The door/s to the

65
aisle or other rooms
should be kept
closed at all times.
Appropriate signage
shall be used/
displayed.
b The Nursing professionals are
familiar with the type of isolation
(barrier and reverse barrier)
facilities provided by the HCO.
Self-explanatory. Self-explanatory.
c Senior Nursing Professionals
monitor the nursing activities
provided in isolation facilities.
Self-explanatory.
This should include
monitoring of
standard
precautions,
disinfection and
sterilization of the
facility and
earmarking of
specific and trained
nursing staff for
carrying out duties
in such facilities.
Self-explanatory.
Standard
ICP.6.
Infection Control Nurse maintains records of all occupational injuries and
pre- and post-exposure prophylaxis.
Sr.No Objective Elements Interpretation Remark(s)
66
a. Hazardous materials specific to
the settings and locations that
they work in are identified by the
nursing professionals. (as
applicable).
The nursing shall
identify, list and
document the
hazardous materials
and has a
documented
procedure for their
sorting, storage,
handling,
transpirations,
disposal
mechanism, and
method for
managing spillages
and adequate
training of the
personnel for these
jobs.
The hazardous
materials include
blood, body fluids
as well as some
chemicals and
drugs like
chemotherapeutic
agents. The
hazardous materials
identified should be
specific to the work
place that they work
in and not a
generalised list of
items across the
HCO.
b. The nursing professionals
implement processes for sorting,
labeling, handling, storage,
transporting and disposal of
hazardous materials.
The organization
has ensured display
of Material Safety
Data Sheets
(MSDS) for all
hazardous materials
and has accordingly
arranged training of
personnel who
handles such
materials.
Self-explanatory.
c. The Nursing professionals are
aware of the HCOs plan for
Self-explanatory.
The organization
could have a

67
managing the spills of hazardous
materials and are able to
supervise and adequately
implement the same in their
specific locations of work.
HAZMAT kit(s) for
handling spills. The
nursing staff should
be aware of the kit
and the
methodology of use
of the kit in their
area of work.
d. Appropriate pre- and post-
exposure prophylaxis is provided
to all staff members concerned.
Self-explanatory
Infection control
Nurse maintains
documentation of all
occupational injuries
and pre- and post-
exposure
prophylaxis records.
For example,
hepatitis B
Vaccination and
immunisation status
shall be available
with designated
individuals. And
PEP (e.g. Hepatitis
B immunoglobulin,
anti-retroviral drugs
for pregnant and
non-pregnant staff)
for needle stick
injury should be
administered within
desired time frame.

68
CHAPTER: 6
EMPOWERMENT AND GOVERNANCE
Intent of the chapter:
The standards encourage the governance of the organization in a professional and
ethical manner. The responsibilities of all the Nursing professionals performing
management functions are defined.
The Nursing Service is led by qualified professionals with desired experience. Nursing
professionals are involved in decision making processes. They are encouraged to
participate in organization decision making groups and committees. There is a
commitment to support and reward nursing staff from time to time.
Nursing professionals at the bedside are empowered to take decision to meet the needs
of patients in collaboration with the care provider team. Nursing professionals at the bed
side participate in plan of treatment and discharge plan by the medical team.
Leaders ensure that patient-safety and risk-management issues are an integral part of
patient care and hospital management.
69
Summary of Standards
EG.1. The responsibilities of those responsible for nursing management are
defined.
EG.2.
The Head of the Nursing service ensures that suitable mechanisms exist to
govern the nursing Service.
EG.3. Nursing professionals are involved and participate in decision making related
to organization and nursing services.
EG.4. The Management empowers nursing staff
EG.5. The organization has an established process for proactive risk assessment
and error management.
EG.6. The infection control programme is supported by the management and
includes training of staff.

70
Standards and Objective Elements
Standard
EG.1. The responsibilities of those responsible for nursing management are
defined.
Sr.No Objective Elements Interpretation Remark(s)
a. Those responsible for nursing
management lay down the
nursing department vision.
For definition of
vision refer to
glossary.
Only a display on its
website would not
be appropriate. It is
preferable that the
same be translated
and displayed in the
local language also.
This should be part
of nursing manual,
refer NCP 1.
b. Those responsible for nursing
management lay down the
nursing department mission.
For definition of
mission refer to
glossary.
Only a display on its
website would not
be appropriate. It is
preferable that the
same be translated
and displayed in the
local language also.
This should be part
of nursing manual,
refer NCP 1.
c. Those responsible for nursing For definition of This should be part

71
management lay down the
nursing department values.
values refer to
glossary.
Only a display on its
website would not
be appropriate. It is
preferable that the
same be translated
and displayed in the
local language also.
of nursing manual,
refer NCP 1.
d. Those responsible for nursing
management establish the
nursing department organogram.
The nursing
management shall
have a well-defined
organization
structure / chart and
this shall be clearly
document the
hierarchy, line of
control, along with
the function at the
various levels.
This should be part
of nursing manual,
refer NCP 1.
Standard
EG.2.
The Head of the Nursing service ensures that suitable mechanisms exist to
govern the nursing Service.
Sr.No Objective Elements Interpretation Remark(s)
a. There is an established head of
the nursing services.
The head of the
nursing services is

72
selected based
upon identified
criteria like
qualifications,
experience and
training received.
b. The scope of Nursing services is
defined in the nursing manual.
Self-explanatory. Self-explanatory.
c. The Nursing administrative policy
and procedure is defined in the
manual and implemented.
Self-explanatory. Self-explanatory.
d. The department manual shall
govern the nursing functions and
activities within the department.
Self-explanatory. Self-explanatory.
e. Nursing administrative policy and
procedure is defined and
implemented.
Self-explanatory. Self-explanatory.
f. Structured program exists for
enhancing clinical competency
and leadership skills of nursing
professionals.
Self-explanatory. Self-explanatory.
g. The Nursing leaders are involved
in quality improvement projects
and program.
Self-explanatory. Self-explanatory.

73
Standard
EG.3. Nursing professionals are involved and participate in decision making related
to organization and nursing services.
Sr.No Objective Elements Interpretation Remark(s)
a. A Nursing Management
committee is established and it
meets periodically to oversee
Nursing related issues.
Self-explanatory.
The periodicity of
the meeting needs
to be specifically
defined by the HCO
and minutes of the
meeting are
recorded along with
the action taken
reports.
Self-explanatory.
b. Nursing professionals have
membership in various
committees as appropriate.
Self-explanatory.
Nursing
professionals shall
have representation
in Infection Control,
Grievance, Safety,
OT, Death Review
Committee, etc.
c. Nursing professionals providing
direct care are involved in action
plan development and evaluation
is based on evidence based data.
Self-explanatory. Self-explanatory.
d. The organization has a
mechanism to seek feedback
from nursing professionals and
This is reviewed
and improvement
opportunities are
Self-explanatory.
74
other staff regarding the quality of
nursing care and to for evaluating
nursing satisfaction.
identified and
implemented
accordingly.
Standard
EG.4. The Management empowers nursing staff.
Sr.No Objective Elements Interpretation Remark(s)
a. There is a policy on nursing
empowerment to ensure timely
nursing care of patients.
Self-explanatory. Self-explanatory.
b. Management empowers nursing
staff by involving them in decision
making.
Self-explanatory. Self-explanatory.
c. Management empowers nursing
staff by appraisal and Job
incentives, encouraging
innovation.
Self-explanatory. Self-explanatory.
d. Management empowers nursing
staff by supporting education.
Self-explanatory. Self-explanatory.
e. Management empowers nursing
staff by promoting interpersonal
relationships.
Self-explanatory. Self-explanatory.
Standard
EG.5. The organization has an established process for proactive risk assessment

75
and error management.
Sr.No Objective Elements Interpretation Remark(s)
a. The Nursing service has clearly
defined error prevention, error
reporting and error addressing
mechanisms and the same are
documented.
Self-explanatory. Self-explanatory.
b. The Nursing professionals are
provided with adequate resources
including materials and equipment
for providing safe and efficient
nursing services.
Self-explanatory. Self-explanatory.
c. The nursing structure and
processes support a culture of
patient safety.
Self-explanatory. Self-explanatory.
d. The Nursing professionals are
made aware of and are trained in
code blue drills, disaster
management and emergency
situations including fire and non
fire emergencies.
Self-explanatory. Self-explanatory.
e. The standards of personal health
and safety of the nursing
professionals are maintained such
that ability to practice is not
compromised.
Self-explanatory. Self-explanatory.
f. There is an escalation process for
nursing professionals when
Self-explanatory. Self-explanatory.

76
emergency and life threatening
situations arise.
Standard
EG.6. The infection control programme is supported by the management and
includes training of staff.
Sr.No Objective Elements Interpretation Remark(s)
a. The management makes
available resources required for
the infection control practices.
The organization
shall ensure that the
resources required
by the personnel
should be available
in a sustained
manner. This
includes both men
and materials.
Self-explanatory.
b. The organization conducts
induction training for all staff.
There must be a
documented
evidence of
induction training for
all categories of
staff before joining
department(s)
concerned. It should
include the policies,
procedures and
practices of the

77
infection control
programme.
c. The organization conducts
appropriate “in-service” training
sessions for all staff at least once
in a year.
Self-explanatory.
Self-explanatory.

78
CHAPTER: 7
NURSING QUALITY INDICATORS
Intent of the chapter:
Nursing care quality improvement programme should be documented and involve all
areas of the organization and all essential nursing staff members. The organization
should collect data on structures, processes and outcomes, in nursing care areas. The
collected data should be collated, analysed and used for further improvements. The
improvements should be sustained.
Excellent nursing practice is a reflection of sound ethical standards. The registered
nurse systematically enhances the quality and effectiveness of nursing practice by
demonstrating quality, by documenting the application of the nursing process in a
responsible, accountable and ethical manner and by using quality improvement
activities to initiate changes in nursing practice and health care delivery system.
A system for monitoring and measurement of nursing quality parameters shall be
established by the organization. Statistical review and analyses of trends shall be
reviewed by the Organization in order to use these as tools to aim for excellence in
nursing care delivery and satisfaction with nursing care amongst patients, thereby
contributing to overall improvement in quality of care that every patient receives.
79
Summary of Standard
NQI.1. There is a structured quality improvement and continuous monitoring
program for nursing service.
NQI.2. The organization identifies key indicators to monitor the structures,
processes and outcomes, which are used as tools for continual improvement
for nursing service.
NQI.3. The nursing quality improvement programme is supported by the
management.
NQI.4. There is an established system for nursing audit.
NQI.5. Incidents, complaints and feedback from nursing professionals are collected
and analysed to ensure continual quality improvement.
80
Standards and Objective Elements
Standard
NQI.1. There is a structured quality improvement and continuous monitoring
program for nursing service.
Sr.No Objective Elements Interpretation Remark(s)
a. The quality improvement
programme is developed,
implemented and maintained by a
committee with a representative
from nursing personnel.
There is need for a
formal controlled
documentation.
This will be aligned
with the
organizations
quality improvement
program.
At minimum, a
„nursing manual‟
shall be established.
This may refer to
SOPs where
required.
b. There is a designated individual
for coordinating and implementing
the nursing quality-improvement
programme.
Self-explanatory. This individual shall
necessarily be a
senior and
experienced nursing
professional
preferably with
exposure to NABH
and Quality
standards.
c. The quality improvement
programme shall be reviewed at
periodic intervals.
Self-explanatory. It should be
reviewed and
updated atleast
once every year.
81
Standard
NQI.2. The organization identifies key indicators to monitor the structures,
processes and outcomes, which are used as tools for continual improvement
for nursing service.
Sr.No Objective Elements Interpretation Remark(s)
a. The patient falls are monitored
and the incident of patient falls is
documented by the appropriate
nursing professionals.
The factors
responsible for
patient fall can be
classified as under:
1. Nursing related
2. Patient related-
unbalanced or
unsteady gait,
incorrect use of
equipment
3. Falls requiring
Medical
intervention
Self-explanatory.
b. The hospital acquired decubitus /
pressure ulcers in various
departments are monitored and
recorded as per laid down
protocols by the HCO.
Self-explanatory. Self-explanatory.
c. The medication errors during
provisioning of care are monitored
and recorded on occurrence by
the concerned nursing staff in
forms as laid down by the HCO.
Self-explanatory. Self-explanatory.

82
d. Monitoring of accidental delining
(if applicable).
Self-explanatory. Self-explanatory
e. All extravasations are recorded
and monitored as per the laid
down protocols.
Self-explanatory. Self-explanatory.
f. All needle stick injuries are
documented and monitored as
per the policy laid down by the
HCO that should be in
consonance with the national and
International guidelines.
Self-explanatory. Self-explanatory.
g. All restraint related incidents
including strangulation are
monitored and documented.
Self-explanatory. Self-explanatory.
h. The hand hygiene compliance is
monitored and recorded by the
nursing professionals responsible
for the same.
Self-explanatory.
The monitoring
should be as per the
criteria identified by
the WHO guidelines
on Hand Hygiene.
Self-explanatory.
i. The compliance with pain
assessment and management is
monitored by the senior nursing
professional while undertaking
their professional rounds and the
same is documented.
Self-explanatory. Self-explanatory.
j. The satisfaction of patients with
the nursing care is monitored by
the senior nursing professionals
and the same is documented.
Self-explanatory. Self-explanatory.

83
Standard
NQI.3. The nursing quality improvement programme is supported by the
management.
Sr.No Objective Elements Interpretation Remark(s)
a. The management makes
available adequate resources
required for quality improvement
programme.
This shall include
the men, material,
machine, money
and method. These
should be in steady
supply so as to
ensure that the
programme
functions smoothly.
b. The management supports and
implements use of appropriate
quality improvement, statistical
and management tools in its
quality improvement programme.
Self-explanatory. For example, Root
Cause Analysis,
FMEA, Project
Evaluation and
Review Technique
(PERT), Critical
Path Method
(CPM), Control
Charts, etc.
c. The senior nursing professionals
as delineated by the HCO also
monitor the nursing satisfaction
based on pre determined criteria
in consultation with the Human
resource department of the HCO.
Self-explanatory. Self-explanatory.

84
d. The attrition rate and frequency of
attrition of the nursing
professionals is monitored and
documented by the head of the
nursing in consultation with the
human resource department of
the HCO.
Self-explanatory. Self-explanatory.
Standard
NQI.4. There is an established system for nursing audit.
Sr.No Objective Elements Interpretation Remark(s)
a. Nursing staff participates in
the audit.
The organization shall
identify such personnel.
It shall necessarily
include senior and junior
nursing professionals
and could be a mix of
clinicians and
administrators.
These could be
members of the
core
committee/nursing
quality assurance
committee, etc.
b. The parameters to be audited
are defined by the
organization.
As these audits are
retrospective/concurrent
in nature, it is imperative
that this be done using
predefined parameters
so that there is no bias.
The parameters could be
disease based, nursing
protocol based, nursing
The audit shall
encompass all
aspects of care
including clinical
and nursing.

85
documentation based,
cost based, community
based or based on
morbidity (length of
stay).
It shall lay down the
objectives, the
parameters that are
going to be captured,
develop a checklist
where required,
sampling and data
collection guidelines and
preparation of report.
c. Patient and staff anonymity is
maintained.
This means that the
names of the patients
and the hospital staff
who may figure in the
audit documents must
not be disclosed or any
reference be made to
them in public
discussions/conferences.
This is at the stage
of report
preparation and
dissemination. The
staff participating in
the audit shall
maintain patient
and staff anonymity
and not reveal
names.
d. All audits are recorded and
reviewed.
Self-explanatory.
The organization
could use a
checklist with the
predefined
parameters and the
audit findings could
be recorded on this

86
sheet.
e. Implementation is recorded
and reviewed.
All remedial measures
as ascertained should be
documented and
implemented and
improvements thereof
recorded to complete the
audit cycle.
This should
preferably be done
based on root-
cause analysis.
Standard
NQI.5. Incidents, complaints and feedback from nursing professionals are collected
and analysed to ensure continual quality improvement.
Sr.No Objective Elements Interpretation Remark(s)
a. The organization has an incident
reporting system.
The incident
reporting system
includes:
i. identification
ii. reporting
iii. review
iv. action on
incidents.
While capturing the
organization shall
capture all incidents
without going into
the severity or
whether harm was
caused.
b. The organization has a process to
collect feedback and receive
complaints.
Self-explanatory. This shall be
communicated to
the patients using
displays or
brochures.
c. The organization has established The quality This could

87
processes for analysis of
incidents, feedbacks and
complaints.
improvement
committee (refer to
CQI 1a) shall be
responsible for this
activity.
preferably be done
by identifying the
root cause.
Where possible, it is
preferable that
patients be included
in analysing the
feedback and
complaint.
d. Corrective and preventive actions
are taken based on the findings of
such analysis.
The objective of this
is to continually
improve the quality
of patient-care
services.
All such action shall
be documented.
e. Feedback about care and service
is communicated to staff.
At a minimum,
patient satisfaction
levels shall be
communicated on a
monthly basis.
This could be done
using internal
communication.
It is equally
important that
positive feedback
about care and
service is
communicated to
staff.
88
GLOSSARY
The commonly-used terminologies in the NABH standards are briefly described and
explained herein to remove any ambiguity regarding their comprehension. The
definitions narrated have been taken from various authentic sources as stated,
wherever possible. Notwithstanding the accuracy of the explanations given, in the event
of any discrepancy with a legal requirement enshrined in the law of the land, the
provisions of the latter shall apply.
Certification
assessment
The evaluation process for assessing the compliance of an
organization with the applicable standards for determining its
accreditation status.
Advance life
support
Emergency medical care for sustaining life, including
defibrillation, airway management, and drugs and medications.
Adverse drug
event
Adverse event: Any untoward medical occurrence that may
present during treatment with a pharmaceutical product but
which does not necessarily have a causal relationship with this
treatment.
Adverse drug reaction: A response to a drug which is noxious
and unintended and which occurs at doses normally used in
man for prophylaxis, diagnosis, or therapy of disease or for the
modification of physiologic function.
Therefore ADR = adverse event with a causal link to a drug
Adverse drug event:The FDA 88abeling88e the term adverse
drug event to be a synonym for adverse event.
In the patient-safety literature, the terms adverse drug event and
adverse event usually denote a causal association betweenthe
drug and the event, but there is a wide spectrum of definitions

89
for these terms, including harm caused by a
• drug
• harm caused by drug use, and
• a medication error with or without harm
Institute of Medicine: “An injury resulting from medical
intervention related to a drug”, which has been simplified to “an
injury resulting from the use of a drug”
Adverse drug events extend beyond adverse drug reactions to
include harm from overdoses and under-doses usually related to
medication errors.
A minority of adverse drug events are medication errors, and
medication errors rarely result in adverse drug events.
Adverse event An injury related to medical management, in contrast to
complications of disease. Medical management includes all
aspects of care, including diagnosis and treatment, failure to
diagnose or treat, and the systems and equipment used to
deliver care. Adverse events may be preventable or non-
preventable. (WHO Draft Guidelines for Adverse Event
Reporting and Learning Systems).
Assessment All activities including history taking, physical examination,
laboratory investigations that contribute towards determining the
prevailing clinical status of the patient.
Barrier nursing
The nursing of patients with infectious diseases in isolation to
prevent the spread of infection.
As the name implies, the aim is to erect a barrier to the passage
of infectious pathogenic organisms between the contagious
patient and other patients and staff in the hospital, and thence to

90
the outside world. The nursing professionals wear gowns,
masks, and gloves, and they observe strict rules that labeling the
risk of passing on infectious agents.
Basic life
support
Basic life support (BLS) is the level of medical care which is used
for patients with life-threatening illnesses or injuries until the
patient can be given full medical care.
Bylaws
A rule governing the internal management of an organization. It
can supplement or complement the government law but cannot
countermand it, e.g. municipal bylaws for construction of
hospitals/nursing homes, for disposal of hazardous and/or
infectious waste.
Clinical audit A quality improvement process that seeks to improve patient
care and outcomes through systematic review of care against
explicit criteria and the implementation of change. (Principles for
Best Practice in Clinical Audit 2002, NICE/CHI).
Clinical practice
guidelines
Clinical practice guidelines are systematically developed
statements to assist practitioner and patient decisions about
appropriate health care for specific clinical circumstances. (Field
and Lohr 1990. Page 38).
Communication Communication is a two way process of exchange of thoughts,
messages, and information to the mutual understanding of all the
parties. It can be exchange by speech, gestures, and by the use
of writing. The parties in health care refer to the medical
professionals, the nursing professionals ,the paramedical staff,
the patients , the families of the patients, the visitors and other
stake holders viz suppliers, administrators etc.
Competence Demonstrated ability to apply knowledge and skills (para 3.9.2 of

91
ISO 9000: 2000).
Knowledge is the understanding of facts and procedures. Skill is
the ability to perform specific action. For example, a competent
gynaecologist knows about the patho-physiology of the female
genitalia and can conduct both normal as well as abnormal
deliveries.
Confidentiality
Restricted access to information to individuals who have a need,
a reason and permission for such access. It also includes an
individual‟s right to personal privacy as well as privacy of
information related to his/her healthcare records.
Consent
1. Willingness of a party to undergo examination/procedure/
treatment by a healthcare provider. It may be implied (e.g.
patient registering in OPD), expressed which may be written
or verbal. Informed consent is a type of consent in which the
healthcare provider has a duty to inform his/her patient about
the procedure, its potential risk and benefits, alternative
procedure with their risk and benefits so as to enable the
patient to take an informed decision of his/her health care.
2. In law, it means active acquiescence or silent compliance by
a person legally capable of consenting. In India, legal age of
consent is 18 years. It may be evidenced by words or acts or
by silence when silence implies concurrence. Actual or
implied consent is necessarily an element in every contract
and every agreement.
Credentialing The process of obtaining, verifying and assessing the
qualification of a healthcare provider.
Data Raw facts, clinical observations, or measurements collected
during an assessment activity.
92
Disciplinary
proceedings
Sequence of activities to be carried out when staff does not
conform to the laid-down norms, rules and regulations of the
healthcare organization.
Empowerment Empowerment is a dynamic process that results from mutual
interaction between personal and collective traits of nurses as
well as the culture and the structure of the organization. It means
to invest or to give authority to the nurses based upon their
demonstrated capabilities and competence the power to make
decisions for patient care under specific situations and
conditions.
End of life Period of time marked by disability or disease that is
progressively worse until death.
Ethics
Medical ethics is the discipline of evaluating the merits, risks,
and social concerns of activities in the field of
medicine.(en.wikipedia.org/wiki/Medical ethics)
Evidence-based
medicine
Evidence-based medicine is the conscientious, explicit, and
judicious use of current best evidence in making decisions about
the care of individual patients.
Family The person(s) with a significant role in the patient‟s life. It mainly
includes spouse, children and parents. It may also include a
person not legally related to the patient but can make healthcare
decisions for a patient if the patient loses decision-making ability.
Goal A broad statement describing a desired future condition or
achievement without being specific about how much and when.
(ASQ).
The term “goals” refers to a future condition or performance level
that one intends to attain. Goals can be both short- and longer-

93
term. Goals are ends that guide actions. (MBNQA)
Grievance-
handling
procedures
Sequence of activities carried out to address the grievances of
patients, visitors, relatives and staff.
Guidance The act or process of guiding someone or something.
Hazardous
materials
Substances dangerous to human and other living organisms.
They include radioactive or chemical materials.
Hazardous waste Waste materials dangerous to living organisms. Such materials
require special precautions for disposal. They include biologic
waste that can transmit disease (for example, blood, tissues)
radioactive materials, and toxic chemicals. Other examples are
infectious waste such as used needles, used bandages and fluid
soaked items.
Healthcare-
associated
infection
Healthcare-associated infections (HAIs) are infections caused by
a wide variety of common and unusual bacteria, fungi, and
viruses during the course of receiving medical care. (CDC)
This was earlier referred to as Nosocomial/hospital-acquired/
hospital-associated infection(s).
Healthcare
organization
Generic term is used to describe the various types of
organization that provide healthcare services. This includes
ambulatory care centres, hospitals, laboratories, etc.
High-
dependency unit
A high-dependency unit (HDU) is an area for patients who
require more intensive observation, treatment and nursing care
than are usually provided for in a ward. It is a standard of care
between the ward and full intensive care.
In service Organised education/training usually provided in the workplace
94
education/
training
for enhancing the skills of staff members or for teaching them
new skills relevant to their jobs/tasks.
Indicator A statistical measure of the performance of functions, systems or
processes overtime. For example, hospital acquired infection
rate, mortality rate, caesarean section rate, absence rate, etc.
Information Processed data which lends meaning to the raw data.
Intent A brief explanation of the rational, meaning and significance of
the standards laid down in a particular chapter.
Inventory control The method of supervising the intake, use and disposal of
various goods in hands. It relates to supervision of the supply,
storage and accessibility of items in order to ensure adequate
supply without stock-outs/excessive storage. It is also the
process of balancing ordering costs against carrying costs of the
inventory so as to minimise total costs.
Isolation
Separation of an ill person who has a communicable disease
(e.g., measles, chickenpox, mumps, SARS) from those who are
healthy. Isolation prevents transmission of infection to others and
also allows the focused delivery of 94abeling94ed health care to
ill patients. The period of isolation varies from disease-to-
disease. Isolation facilities can also be extended to patients for
fulfilling their individual, unique needs.
Job description 1. It entails an explanation pertaining to duties, responsibilities
and conditions required to perform a job.
2. A summary of the most important features of a job, including
the general nature of the work performed (duties and
responsibilities) and level (i.e., skill, effort, responsibility and
working conditions) of the work performed. It typically
includes job specifications that include employee

95
characteristics required for competent performance of the
job. A job description should describe and focus on the job
itself and not on any specific individual who might fill the job.
Job specification 1. The qualifications/physical requirements, experience and
skills required to perform a particular job/task.
2. A statement of the minimum acceptable qualifications that
an incumbent must possess to perform a given job
successfully.
Laws
Legal document setting forth the rules of governing a particular
kind of activity, e.g. organ transplantation act, which governs the
rules for undertaking organ transplantation.
Medication error 1. A medication error is any preventable event that may cause
or lead to inappropriate medication use or harm to a patient.
(FDA)
2. A medication error is any preventable event that may cause
or lead to inappropriate medication use or patient harm while
the medication is in the control of the healthcare professional,
patient, or consumer. Such events may be related to
professional practice, healthcare products, procedures, and
systems, including prescribing, order communication, product
labeling, packaging, and nomenclature, compounding,
dispensing, distribution, administration, education,
monitoring, and use.(NCC MERP)
Mission An organization‟s purpose. (ASQ)
This refers to the overall function of an organization. The mission
answers the question, “what is this organization attempting to
accomplish?” The mission might define patients, stakeholders, or
markets served, distinctive or core competencies, or
technologies used. (MBNQA)
Monitoring The performance and analysis of routine measurements aimed
96
at identifying and detecting changes in the health status or the
environment, e.g. monitoring of growth and nutritional status, air
quality in operation theatre. It requires careful planning and use
of standardised procedures and methods of data collection.
Multi-disciplinary A generic term which includes representatives from various
disciplines, professions or service areas.
Near-miss A near-miss is an unplanned event that did not result in injury,
illness, or damage--but had the potential to do so. (Wikipedia)
Errors that did not result in patient harm, but could have, can be
categorised as near-misses.
No harm This is used synonymously with near miss. However, some
authors draw a distinction between these two phrases.
A near-miss is defined when an error is realised just in the nick
of time and abortive action is instituted to cut short its translation.
In no harm scenario, the error is not recognised and the deed is
done but fortunately for the healthcare professional, the
expected adverse event does not occur. The distinction between
the two is important and is best exemplified by reactions to
administered drugs in allergic patients. A prophylactic injection of
cephalosporin may be stopped in time because it suddenly
transpires that the patient is known to be allergic to penicillin
(near-miss). If this vital piece of information is overlooked and
the cephalosporin administered, the patient may fortunately not
develop an anaphylactic reaction (no harm event).
Nursing Audit Nursing Audit is part of the cycle of quality assurance. It
incorporates the systematic and critical analysis by nurses,
midwives and health visitors, in conjunction with other staff, of
the planning, delivery and evaluation of nursing and midwifery

97
care, in terms of their use of resources and the outcomes for
patients/clients, and introduces appropriate change in response
to that analysis (NHS ME, 1991 Framework for Audit for Nursing
Services).
It can also be defined as the process of collecting information
from nursing reports and other documented evidence about
patient care and assessing the quality of care by the use of
quality assurance programmes.
Nursing Care
Plan
A plan that identifies patient care needs, lists the strategy to
meet those needs, documents treatment goals and objectives,
outlines the criteria for ending interventions, and documents the
individual‟s progress in meeting specified goals and objectives.
The format of the plan may be guided by specific policies and
procedures, protocols, practice guidelines or a combination of
these. It includes preventive, promotive, curative and
rehabilitative aspects of care.
Objective A specific statement of a desired short-term condition or
achievement includes measurable end-results to be
accomplished by specific teams or individuals within time limits.
(ASQ)
Objective
element
It is that component of standard which can be measured
objectively on a rating scale. The acceptable compliance with
the measureable elements will determine the overall compliance
with the standard.
Occupational
health hazard
The hazards to which an individual is exposed during the course
of performance of his job. These include physical, chemical,
biological, mechanical and psychosocial hazards.
Patient-care The location where a patient is provided health care as per his

98
setting needs, e.g. ICU, speciality ward, private ward and general ward.
Patient record/
medical record/
clinical record
A document which contains the chronological sequence of
events that a patient undergoes during his stay in the healthcare
organization. It includes demographic data of the patient,
assessment findings, diagnosis, consultations, procedures
undergone, progress notes and discharge summary. (Death
certificate, where required).
Performance
appraisal
It is the process of evaluating the performance of employees
during a defined period of time with the aim of ascertaining their
suitability for the job, potential for growth as well as determining
training needs.
Policies They are the guidelines for decision-making, e.g. admission,
discharge policies, antibiotic policy, etc.
Privileging
It is the process for authorising all medical professionals to admit
and treat patients and provide other clinical services
commensurate with their qualifications and skills.
Procedure 1. A specified way to carry out an activity or a process (Para
3.4.5 of ISO 9000: 2000).
2. A series of activities for carrying out work which when
observed by all help to ensure the maximum use of
resources and efforts to achieve the desired output.
Process A set of interrelated or interacting activities which transforms
inputs into outputs (Para 3.4.1 of ISO 9000: 2000).
Programme A sequence of activities designed to implement policies and
accomplish objectives.
Project
evaluation and
Review
PERT is a method to analyze the involved tasks in completing a
given project, especially the time needed to complete each task,
and to identify the minimum time needed to complete the total

99
Technique
(PERT)
project.
PERT breaks down the project into events and activities, and
lays down their proper sequence, relationships, and duration in
the form of a network. Lines connecting the events are called
paths, and the longest path resulting from connecting all events
is called the critical path. The length (duration) of the critical path
is the duration of the project, and any delay occurring along it
delays the whole project. PERT is a scheduling tool, and does
not help in finding the best or the shortest way to complete a
project.
Protocol A plan or a set of steps to be followed in a study, an investigation
or an intervention.
Quality 1. Degree to which a set of inherent characteristics fulfil
requirements (Para 3.1.1 of ISO 9000: 2000).
Characteristics imply a distinguishing feature (Para 3.5.1 of
ISO 9000: 2000).
Requirements are a need or expectation that is stated,
generally implied or obligatory (Para 3.1.2 of ISO
9000:2000).
2. Degree of adherence to pre-established criteria or
standards.
Or
The Institute of Medicine (IOM) stated in 1990 in Medicare:
“Quality of care is the degree to which health services for
individuals and populations increase the likelihood of
desired outcomes and are consistent with current
professional knowledge” (IOM, 1990, p.21)
Quality Part of quality management focussed on providing confidence
100
assurance that quality requirements will be fulfilled (Para 3.2.11 of ISO
9000:2000).
Quality
improvement
Ongoing response to quality assessment data about a service in
ways that improve the process by which services are provided to
consumers/patients.
Re-assessment It implies continuous and ongoing assessment of the patient
which is recorded in the medical records as progress notes.
Resources It implies all inputs in terms of men, material, money, machines,
minutes (time), methods, metres (space), skills, knowledge and
information that are needed for efficient and effective functioning
of an organization.
Restraints Devices used to ensure safety by restricting and controlling a
person‟s movement. Many facilities are “restraint free” or use
alternative methods to help modify behaviour.
www.alz.org/Resources/Glossary.asp. Restraint may be physical
or chemical (by use of sedatives).
Risk assessment Risk assessment is the determination of quantitative or
qualitative value of risk related to a concrete situation and a
recognised threat (also called hazard). Risk assessment is a
step in a risk management procedure. (Wikipedia)
Risk
management
Clinical and administrative activities to identify, evaluate and
reduce the risk of injury.
Risk reduction The conceptual framework of elements considered with the
possibilities to minimise vulnerabilities and disaster risks
throughout a society to avoid (prevention) or to limit (mitigation
and preparedness) the adverse impacts of hazards, within the
broad context of sustainable development [Source:
101
http://www.preventionweb.net/english/ professional/terminology/].
It is the decrease in the risk of a healthcare facility, given activity,
and treatment process with respect to patient, staff, visitors and
community.
Root Cause
Analysis (RCA)
Root Cause Analysis (RCA) is a structured process that
uncovers the physical, human, and latent causes of any
undesirable event in the workplace. Root cause analysis (RCA)
is a method of problem solving that tries to identify the root
causes of faults or problems that cause operating events.
RCA practice tries to solve problems by attempting to identify
and correct the root causes of events, as opposed to simply
addressing their symptoms. By focusing correction on root
causes, problem recurrence can be prevented. The process
involves data collection; cause charting, root cause identification
and recommendation generation and implementation.
Safety The degree to which the risk of an intervention/procedure, in the
care environment is reduced for a patient, visitors and healthcare
providers.
Scope of
services
Range of clinical and supportive activities that are provided by a
healthcare organization.
Security Protection from loss, destruction, tampering, and unauthorised
access or use.
Senior Nursing
professional
The act or function of rendering advice or showing the correct
path on educational or vocational matters.
Staff All personnel working in the organization including employees,
“fee-for-service” medical professionals, part-time workers,

102
contractual personnel and volunteers.
Standard
precautions
1. A method of infection control in which all human blood and
other bodily fluids are considered infectious for HIV, HBV
and other blood-borne pathogens, regardless of patient
history. It encompasses a variety of practices to prevent
occupational exposure, such as the use of personal
protective equipment (PPE), disposal of sharps and safe
housekeeping
2. A set of guidelines protecting first aiders or healthcare
professionals from pathogens. The main message is: "Don't
touch or use anything that has the victim's body fluid on it
without a barrier." It also assumes that all body fluid of a
patient is infectious, and must be treated accordingly.
Standard Precautions apply to blood, all body fluids,
secretions, and excretions (except sweat) regardless of whether
or not they contain visible blood, non-intact skin and mucous
membranes.
Standards A statement of expectation that defines the structures and
process that must be substantially in place in an organization to
enhance the quality of care.
Sterilisation It is the process of killing or removing microorganisms including
their spores by thermal, chemical or irradiation means.
Surveillance The continuous scrutiny of factors that determines the
occurrence and distribution of diseases and other conditions of ill
health. It implies watching over with great attention, authority and
often with suspicion. It requires professional analysis and
sophisticated interpretation of data leading to recommendations
for control activities.
103
Transfusion
reaction
A transfusion reaction is a problem that occurs after a patient
receives a transfusion of blood.
Unstable patient A patient whose vital parameters need external assistance for
their maintenance.
Values The fundamental beliefs that drive organizational behavior and
decision making. (ASQ)
This refers to the guiding principles and behaviours that embody
how an organization and its people are expected to operate.
Values reflect and reinforce the desired culture of an
organization. (MBNQA)
Vision An overarching statement of the way, an organization wants to
be ideal state of being at a future point. (ASQ)
This refers to the desired future state of an organization. The
vision describes where the organization is headed, what it
intends to be, or how it wishes to be perceived in the future.
(MBNQA)ss
Vascular Access
Device
Catheters, tubes, or device inserted into the vascular system,
including veins, arteries, and bone marrow.
Vulnerable
patient
Those patients who are prone to injury and disease by virtue of
their age, sex, physical, mental and immunological status, e.g.
infants, elderly, physically- and mentally-challenged, those on
immunosuppressive and/or chemotherapeutic agents.

104