static digital telepathology: a model for diagnostic and...
TRANSCRIPT

Static Digital Telepathology: A Model for Diagnostic and Educational
Support to Pathologists in the
Developing World
Aliyah R. Sohani, MDDepartment of Pathology
Massachusetts General HospitalAssistant Professor of Pathology
Harvard Medical School
HARVARD
MEDICAL SCHOOL

Pathology in the Developing World
• Limited resources
• Shortages of specialists, trained laboratory personnel
• Lack of continuing medical education programs
• Intellectual “brain drain” of medical professionals from developing to developed countries
– Retention of trained medical professionals further hampered by quality of equipment and facilities, availability of advancedtraining, and opportunities for research and career advancement
• Growing burden of non-communicable diseases
– Cancer, diabetes, heart diseases
– 70% of new cancers in next 15 years will occur in the developing world (WHO)

Pathology in Tanzania• Population: 43.7 million (2009)
• 822 physicians
– 1 per 50,000 people
– 15 pathologists
• 1520 laboratory technologists
– 1 per 25,000 people
– 2 lab technology training schools
• Pathology training programs in Kenya and South Africa; no subspecialty fellowship training programs
• No immunohistochemistry lab country-wide
– Diagnostic challenges, particularly in areas of hemepath, soft tissue path
– Lack of access to prognostic/predictive information (e.g. ER in breast cancer)
• Molecular diagnostics/cytogenetics
– Essentially non-existent

Telepathology
• Potential advantages
– Diagnostic support
– Second opinion consultations
– Ongoing training
– Opportunities for collaborative research
• Challenges
– Equipment cost
– Routine maintenance, servicing and repair
– Training
– Internet connectivity
• How does one define success?
– Relevant, Scalable, Replicable, Sustainable
• Identify best practice models in health care education and delivery in the developing world

The Aga Khan Development
Network
• Group of development agencies working to improve living conditions and opportunities in the developing world
• Mandates include health, education, environment, architecture, culture, microfinance, disaster reduction, rural development, the promotion of private sector enterprise, and the revitalization of historic cities
• AKDN agencies conduct their programs without regard to faith, origin or gender
Aga Khan Health Services (AKHS)
The Aga Khan University (AKU)
http://www.akdn.org/
Aga Khan Health Services
• One of the most comprehensive private, not-for-profit health care systems in the developing world
– Community health programs in Central and South Asia,
and Eastern Africa
– Primary health care and curative medical care in
Afghanistan, India, Kenya, Pakistan, and Tanzania
– Technical assistance to governments in the delivery of health services in Kenya, Syria and Tajikistan
– 325 health care facilities, including 9 hospitals
– Regional network of 4 hospitals in Eastern Africa
• Aga Khan University Hospital (AKUH) in Nairobi, Kenya
• Aga Khan Hospitals (AKH) in Kisumu and Mombasa, Kenya, and Dar es Salaam, Tanzania
http://www.akdn.org/akhs
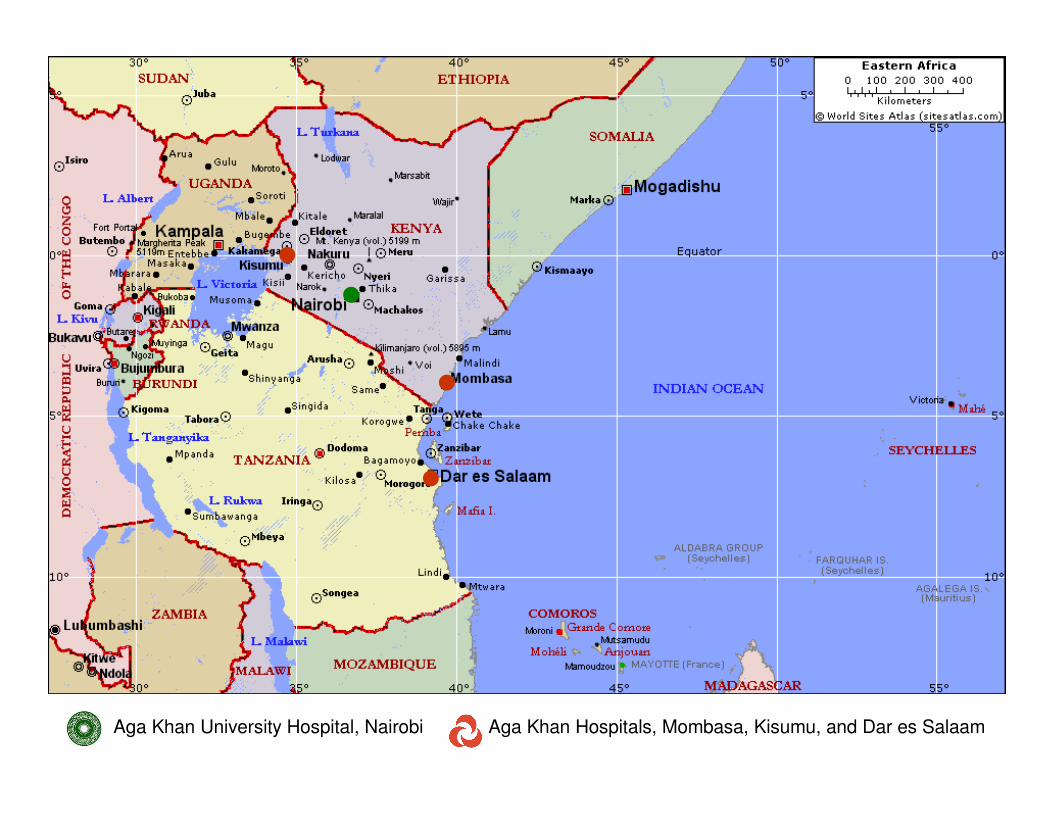
Aga Khan University Hospital, Nairobi Aga Khan Hospitals, Mombasa, Kisumu, and Dar es Salaam

The Aga Khan University
• Chartered in 1983
• Private, autonomous university with campuses in Afghanistan, Eastern Africa, Egypt, Pakistan, Syria and the United Kingdom
• Health-related facilities include teaching hospitals, Nursing Schools and a Medical College
• Aga Khan University Hospital, Nairobi– Regional center of new Faculty of Health Sciences
in Eastern Africa
– Heart and Cancer Center (opened July 2011)http://www.aku.edu/
http://www.akdn.org/Content/943

A Pilot Telepathology Initiative
Between MGH and AKH-Dar
• Established March 2008
• Equipment
– Olympus BH2 5-headed microscope donated by MGH Department
of Pathology
– SPOT Insight Color Digital Camera donated by an MGH pathologist
– SPOT PCI card and software
• Funding provided by Aga Khan Foundation, USA
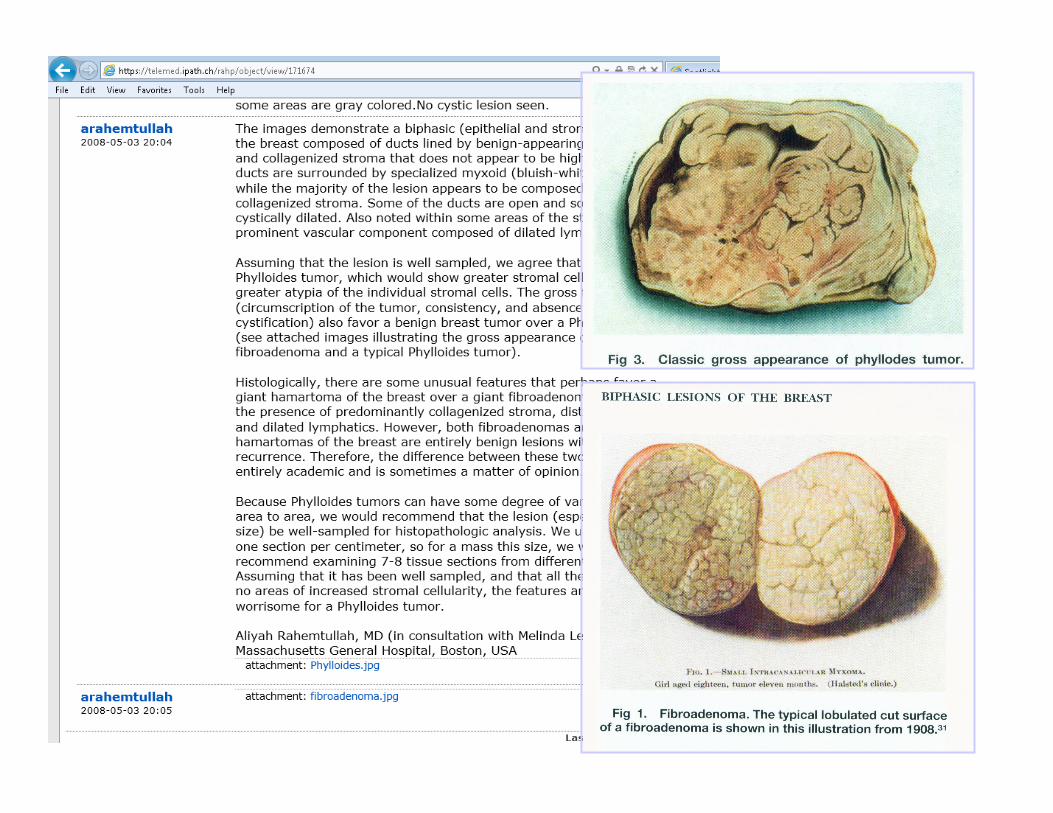
• iPath Telemed Basel telepathology server
– Open-access platform for exchange of medical knowledge, group discussions, consultations, distance learning and teaching in medicine and pathology (http://telemed.ipath.ch/rahp/)
• Site visit to train local pathologists in image capture using camera and software, image upload to iPath website, and care and maintenance of system
Sohani et al, 2009 (USCAP abstract)


A Regional Telepathology
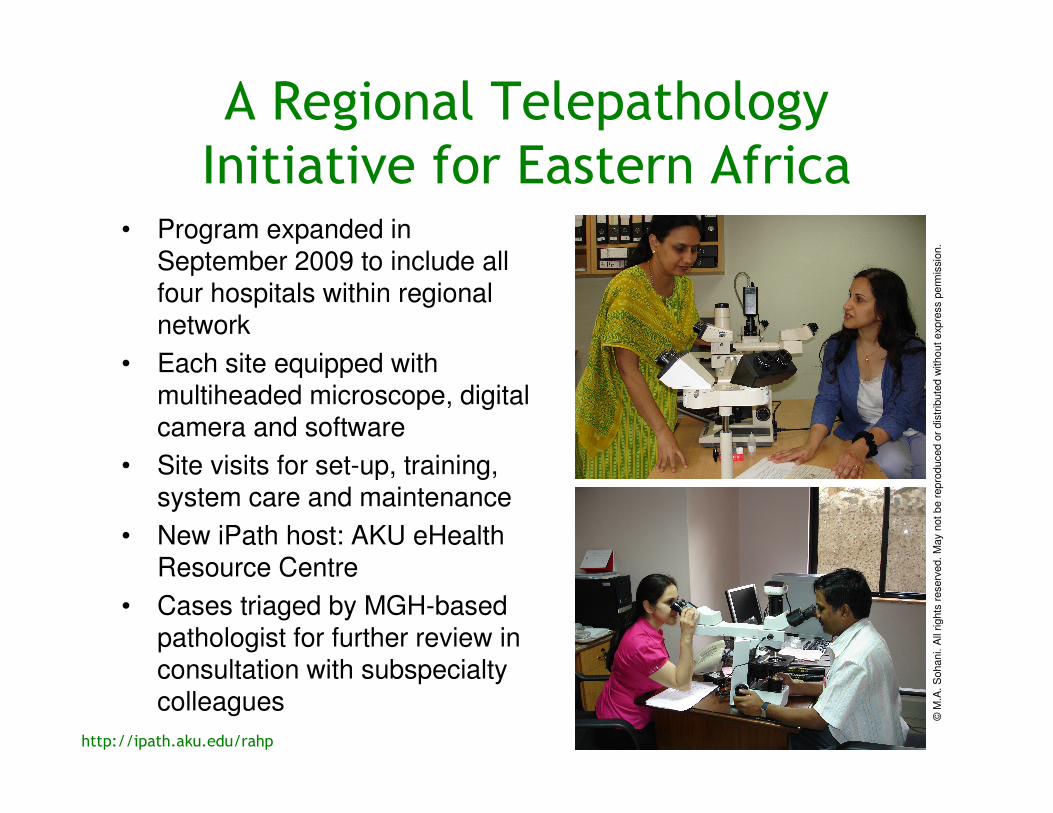
Initiative for Eastern Africa• Program expanded in
September 2009 to include all four hospitals within regional network
• Each site equipped with multiheaded microscope, digital camera and software
• Site visits for set-up, training, system care and maintenance
• New iPath host: AKU eHealth Resource Centre
• Cases triaged by MGH-based pathologist for further review in consultation with subspecialty colleagues
http://ipath.aku.edu/rahp
©M
.A.
Sohani. A
ll rights
reserv
ed.
May n
ot
be r
epro
duced o
r dis
trib
ute
d w
itho
ut
expre
ss p
erm
issio
n.
Teleconsultation Activity to Date
• 109 cases posted since March 2008
– Mean number of images per case: 11; Mean TAT: 5.6 days
• Static images have enabled a complete or partial diagnosis in 100/109 cases (91.7%)
• Responses have an educational emphasis
– Discussion of differential diagnosis, diagnostic pearls/pitfalls
– Accompanying references, links to websites, photographs
– Treatment recommendations, if applicable
• Factors precluding a definitive diagnosis
– Lack of sufficient clinical history
– Technical issues (e.g. air-drying artifact, tangential sectioning, or rarely, poor image quality)
– Absence of confirmatory immunophenotyping
• Additional testing performed at MGH in certain cases

Teleconsultations by Hospital Location
• Nearly 80% of consultations have originated from smaller centers manned by solo pathologists
0
5
10
15
20
25
30
35
40
45
50
Dar es Salaam Kisumu Nairobi Mombasa Other
Hospital Location
Nu
mb
er
of
Cases
0
5
10
15
20
25
30
Derm
path
Hem
eC
ytol
ogy
BST G
I
GY
N
EN
T
Bre
ast
Neur
o
GU
End
ocrin
eP
ulm
onar
y
Rena
l
Pathology Subspecialty
Nu
mb
er
of
Cases
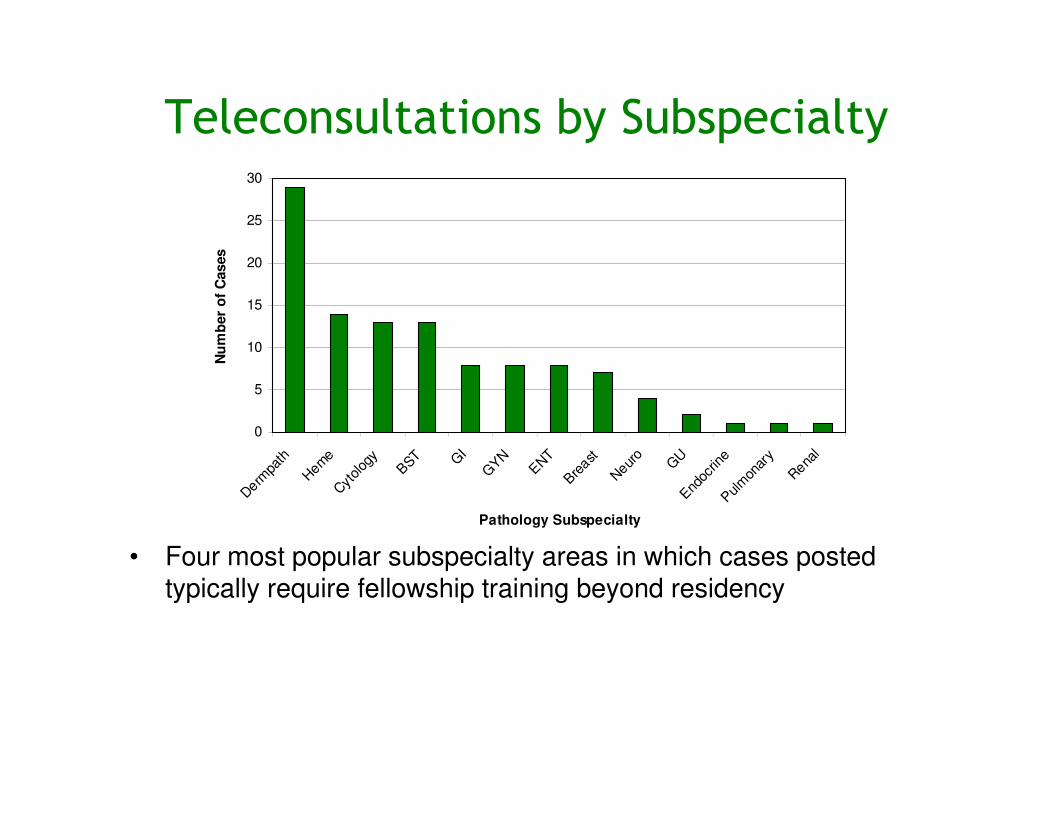
Teleconsultations by Subspecialty
• Four most popular subspecialty areas in which cases posted typically require fellowship training beyond residency
• Dermatopathology cases outweighed all others with nearly 27% of all postings
– Only 5-15% of all histology cases originating from the four
participating hospitals are skin biopsies

0
5
10
15
20
25
30
Derm
path
Hem
eC
ytol
ogy
BST G
I
GY
N
EN
T
Bre
ast
Neur
o
GU
End
ocrin
eP
ulm
onar
y
Rena
l
Pathology Subspecialty
Nu
mb
er
of
Cases
Teleconsultations by Subspecialty
• Four most popular subspecialty areas in which cases posted typically require fellowship training beyond residency
• Dermatopathology cases outweighed all others with nearly 27% of all postings
– Only 5-15% of all histology cases originating from the four
participating hospitals are skin biopsies

Teledermatopathology• Why are teleconsultations in this area so frequent?
– Lack of fellowship training programs in dermatopathology
– No board-certified dermatopathologists in the region
– Prevalence of HIV, concern for Kaposi sarcoma
– Skin biopsies are typically small, minimizing limitations of sampling bias and field selection, and can be obtained on an outpatient basis
• Focused review of 29 cases (29/109 = 26.6%)
– All biopsies of skin or subcutaneous tissue requiring MGH dermatopathologist input for diagnosis
• Glass slides available for review in 22/29 cases (76%) to measure diagnostic concordance between static-image and conventional microscopy
– Cases reviewed 5-32 months after rendering telepathologydiagnosis, blinded to original diagnoses rendered
Gimbel et al, 2011 (submitted)

0
2
4
6
8
10
12
14
Kisumu Dar es Salaam Nairobi Mombasa
Hospital Location
Nu
mb
er
of
Cases
Results• Dermatopathology cases
originated from all 4 hospitals, with >80% from locations with solo pathologists
• 28% of cases included clinical photographs in addition to H&E images
• 95% diagnostic concordance between static telepathologyand glass slide diagnosis
– Single discordant case: toxic
epidermal necrolysis
– Diagnostic field was a separate smaller fragment of
tissue on the glass slide not
included among static images
1 case (3%)Combined Inflammatory/Neoplastic
10 cases (35%)Neoplastic
18 cases (62%)Inflammatory
N=29Type of Lesion
Gimbel et al, 2011 (submitted)
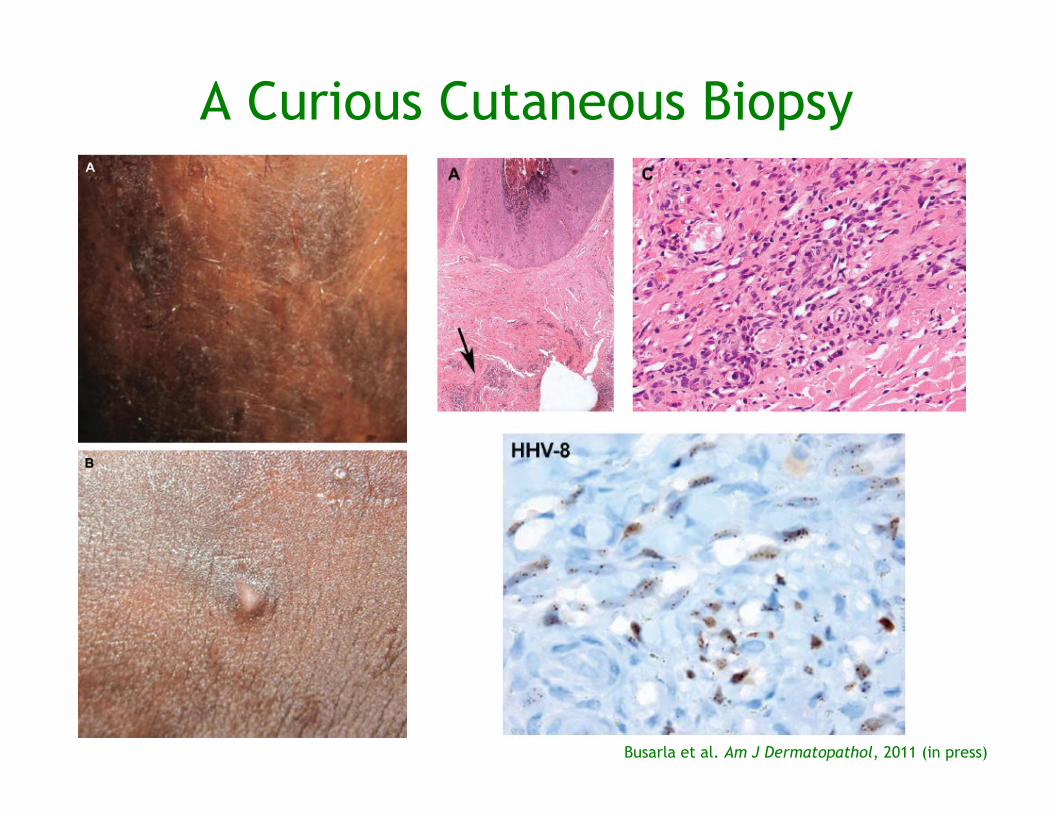
A Curious Cutaneous Biopsy
Busarla et al. Am J Dermatopathol, 2011 (in press)

Participant Feedback
• Technology relatively easy to use
• Fairly rapid access to expert second opinion
• Increased sense of security on difficult cases
• Increased awareness of certain diagnoses
previously unknown to the referring
pathologist
• Discussion of differential diagnosis and citing
of journal articles educational
• Discussion of treatment options allowed for a
patient-centered focus
0
5
10
15
20
25
30
Derm
path
Hem
eC
ytol
ogy
BST G
I
GY
N
EN
T
Bre
ast
Neur
o
GU
End
ocrin
eP
ulm
onar
y
Rena
l
Pathology Subspecialty
Nu
mb
er
of
Cases
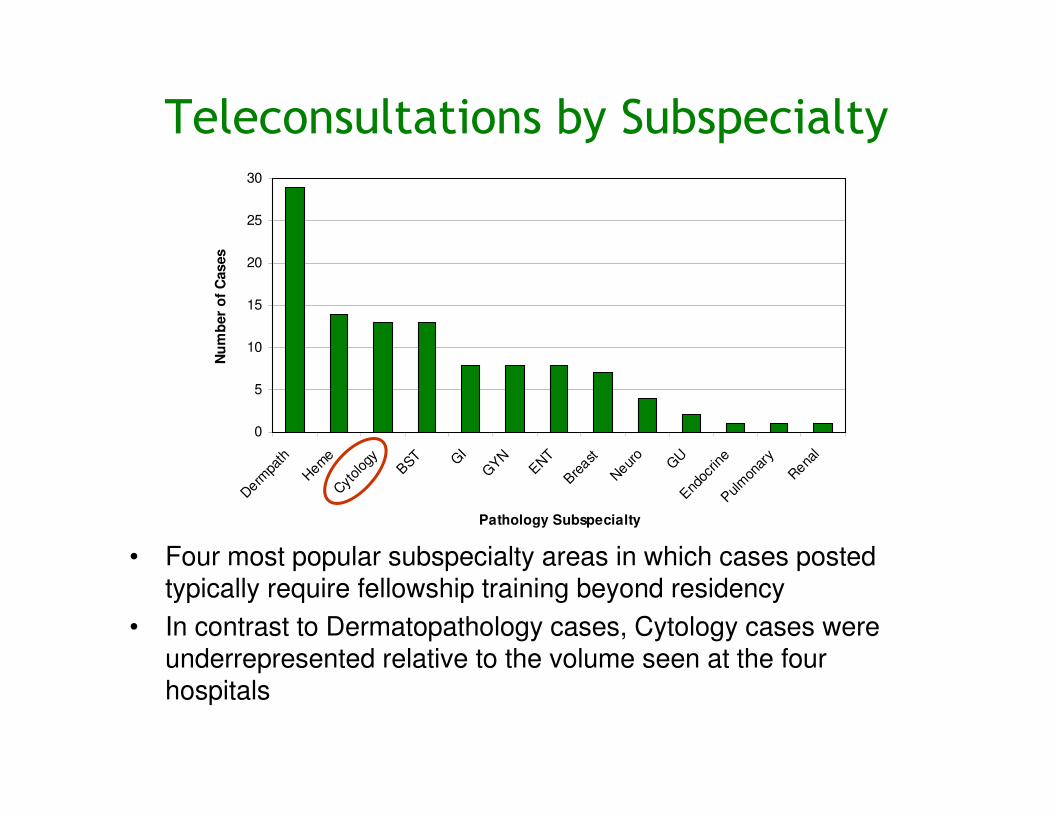
Teleconsultations by Subspecialty
• Four most popular subspecialty areas in which cases posted typically require fellowship training beyond residency
• In contrast to Dermatopathology cases, Cytology cases were underrepresented relative to the volume seen at the four hospitals
Telecytology
• Feasibility study of static imaging system for diagnosis in challenging cytology cases
• 40 consecutive cases considered difficult by referring pathologist in Kisumu, Kenya were posted
– 19 cervical smears (conventional smears; not liquid-based)
– 17 fine needle aspirations
– 4 fluids (2 urine, 1 ascites, 1 pleural fluid)
• 6 AKHS pathologists with varying levels of experience independently evaluated static images
– Telecytology diagnosis compared with consensus glass slide diagnosis in order to assess level of diagnostic concordance for each participant
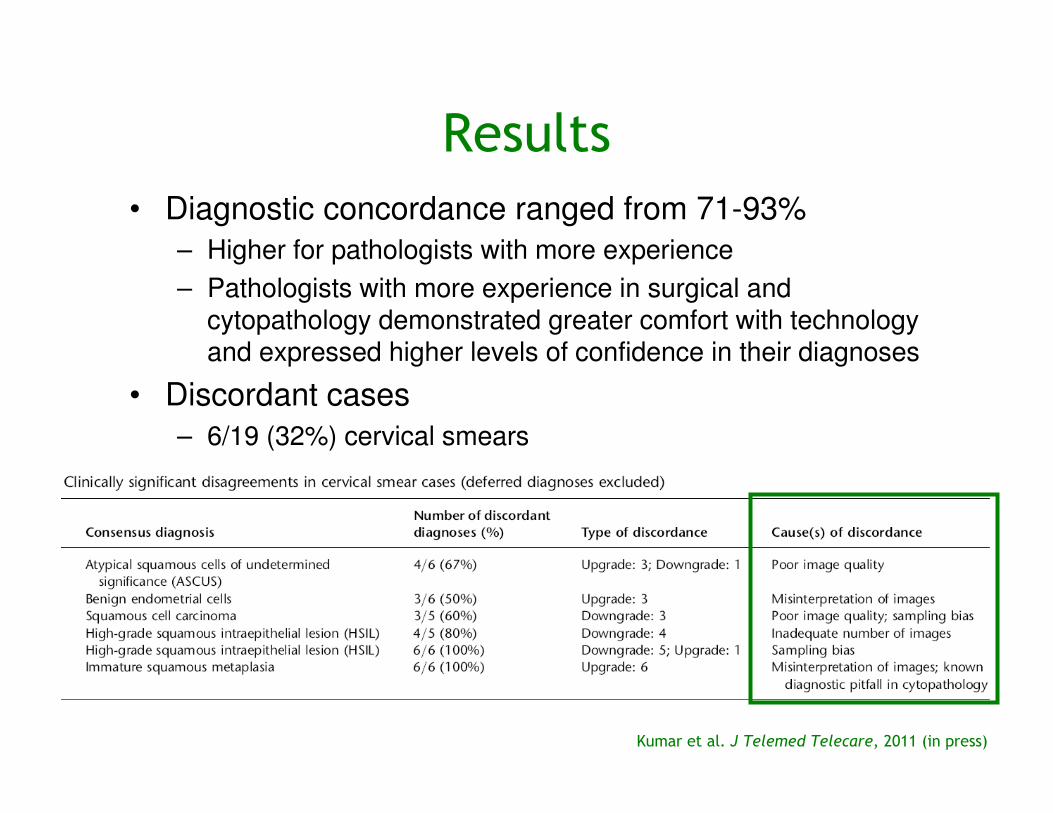
Kumar et al. J Telemed Telecare, 2011 (in press)

Results
Kumar et al. J Telemed Telecare, 2011 (in press)
• Diagnostic concordance ranged from 71-93%
– Higher for pathologists with more experience
– Pathologists with more experience in surgical and cytopathology demonstrated greater comfort with technology and expressed higher levels of confidence in their diagnoses
• Discordant cases
– 6/19 (32%) cervical smears
– 9/21 (43%) FNA/fluids
• Challenges in static telecytology
– Greater susceptibility to technical factors and sampling bias
– Need for additional training for both referring and consulting pathologists
– Diagnostic questions of importance must be clearly outlined
Results
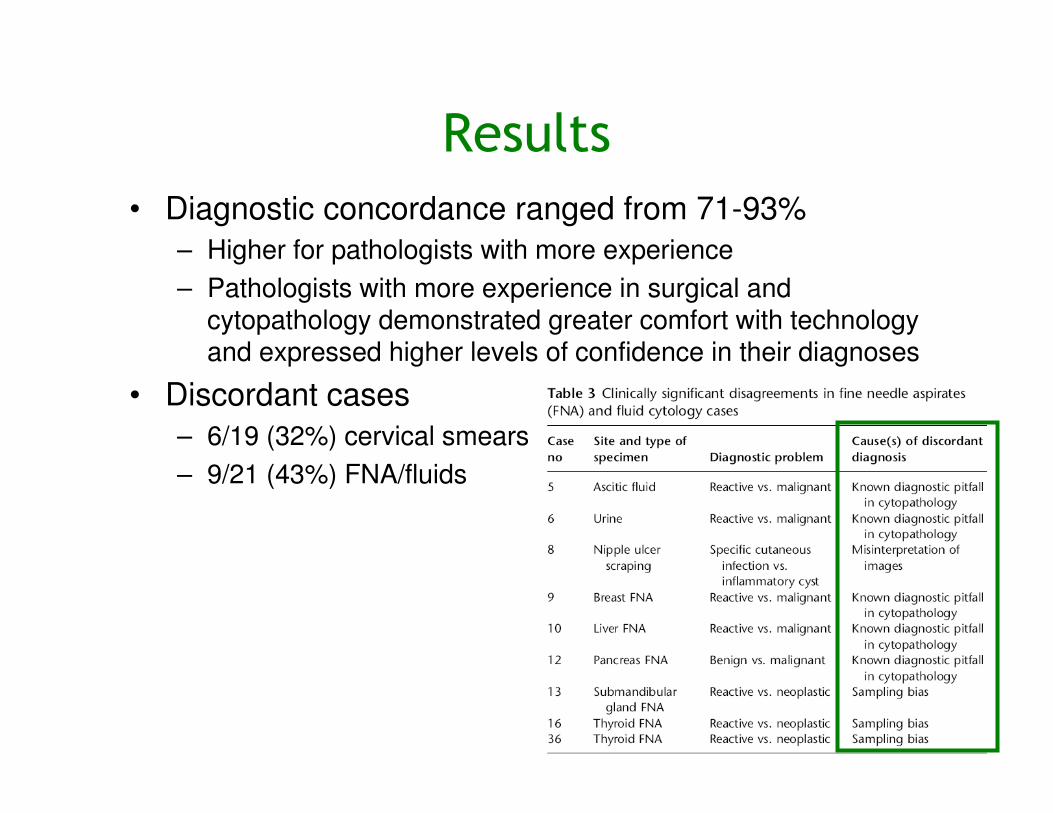
Kumar et al. J Telemed Telecare, 2011 (in press)
• Diagnostic concordance ranged from 71-93%
– Higher for pathologists with more experience
– Pathologists with more experience in surgical and cytopathology demonstrated greater comfort with technology and expressed higher levels of confidence in their diagnoses
• Discordant cases
– 6/19 (32%) cervical smears
– 9/21 (43%) FNA/fluids
• Challenges in static telecytology
– Greater susceptibility to technical factors and sampling bias
– Need for additional training for both referring and consulting pathologists
– Diagnostic questions of importance must be clearly outlined

Results
• Diagnostic concordance ranged from 71-93%
– Higher for pathologists with more experience
– Pathologists with more experience in surgical and cytopathology demonstrated greater comfort with technology and expressed higher levels of confidence in their diagnoses
• Discordant cases
– 6/19 (32%) cervical smears
– 9/21 (43%) FNA/fluids
• Challenges in static telecytology
– Greater susceptibility to technical factors and sampling bias
– Need for additional training for both referring and consulting pathologists
– Diagnostic questions of importance must be clearly outlined by referring pathologist to consultant
Kumar et al. J Telemed Telecare, 2011 (in press)
Planned Projects
and Ongoing Initiatives
• Role of c-kit and pAKT signaling pathways in Kaposi sarcoma
– MGH and Aga Khan Hospital, Kisumu
• Epidemiological and pathologic differences in Hodgkin and non-Hodgkin lymphomas
– MGH and Aga Khan University Hospital, Nairobi
• Use of iPath forum in pediatric telemedicine
– MGH and Aga Khan Hospital, Dar es Salaam
Static Digital Telepathology
• A simple, cost-effective, reliable and sustainable model for diagnostic support to pathologists in resource-limited settings
• Limitation of sampling bias varies across subspecialties and may be overcome with increased awareness and additional training
• Hallmarks of successful teleconsultations
– Clear communication of diagnostic questions by referring pathologist
– Role of consultant: patient-centered and educational
• Rich source of ideas for collaborative and fruitful research endeavors
Acknowledgments
AKUH, East Africa
Zahir Moloo
Shahin Sayed
Neeta Kumar
B. Satya Vara Prasad
Veena Vyas
Shamina Jivaji
Patricia Okiro
Jesca Muthoni
Samuel Gakinya
Hasan Chande
MGH Pathology
Devon Gimbel
Rosalynn Nazarian
Martin C. Mihm
Mari Mino-Kenudson
David Louis
Rosemary Tambouret
David Wilbur
Melinda Lerwill
Eugene Mark
Peter Sadow
AKU eHealth Resource Center, Karachi, Pakistan
Aga Khan Health Board, USA
Aga Khan Foundation, USA
MGH Pathology
Robert Hasserjian
Esther Oliva
Elena Brachtel
Steve Black-Schaffer
Adriano Piris
Gregory Lauwers
Robert H. Young
G. Petur Nielsen
Andrew Rosenberg
Stephen Conley