sterilization & disinfection allison mcgeer, msc, md, frcpc
TRANSCRIPT

Sterilization & Disinfection
Allison McGeer, MSc, MD, FRCPC
How can microorganisms be killed?
Denaturation of proteins (e.g. wet heat, ethylene oxide)
Oxidation (e.g. dry heat, hydrogen peroxide) Filtration Interruption of DNA synthesis/repair (e.g.
radiation) Interference with protein synthesis (e.g. bleach) Disruption of cell membranes (e.g. phenols)

Factors that influence efficacy of disinfection/sterilization
Contact time Physico-chemical environment (e.g. pH)
3 Presence of organic material
4 Temperature
5 Type of microorganism
6 Number of microorganisms
7 Material composition

Ideal sterilization/disinfection process
• Highly efficacious• Fast• Good penetrability• Compatible with all materials• Non-toxic• Effective despite presence of organic material• Difficult to make significant mistakes in process• Easily monitored


Spaulding Classification
Category Description Requirement Critical Enters sterile body cavity Sterile
Semi-critical Contacts mucous membranes, non-intact
skin
High level disinfection
Non-critical Contacts intact skin Low level disinfection

Types of microorganisms and levels of disinfection
Bacterial endospores Mycobacteria (tuberculosis) Non-lipid (small) viruses (polio) Fungi Vegetative bacteria (Salmonella) Lipid viruses (Herpes, HepB, HIV)
sterilization
high level disinf
low level disinf

Sterilization
• Steam
• Ethylene oxide
• Peracetic acid (.2%)
• Hydrogen peroxide gas plasma
• Vapourized hydrogen peroxide
• Ozone

Sterilization process
• Clean items• Package items• Load sterilizer• Monitor
– Physical (time/temp/pressure)
– Chemical
– Biological

Biological Monitors
• Steam: Geobacillus stearothermophilus• Dry heat: B. atrophaeus (formerly B. subtilis)• ETO: B. atropheus• Peracetic acid: G. stearothermophilus• Plasma (Sterrad): G. stearothermophilus
• Ontario guidelines: – Steam: monitor daily, every load with implantables– ETO: monitor every load
Sterilization process
• Clean items• Package items• Load sterilizer• Monitor
– Physical (time/temp/pressure)– Chemical – Biological
• Storage post-sterilization• Documentation
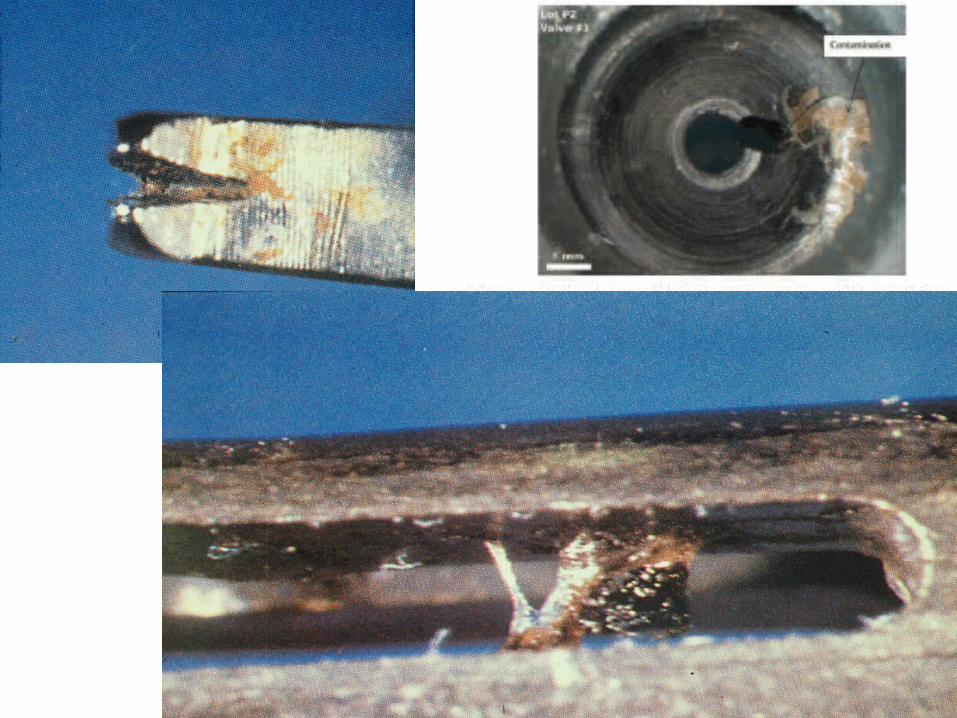

Problems with sterility
• Lack of understanding of risk/process– physicians introducing new products (borrowed,
samples)– Multidose vials– What is sterile vs not
• Lack of understanding of components of process– MDs, technologists have less training than nurses
(anaesthesiology, imaging, urology)
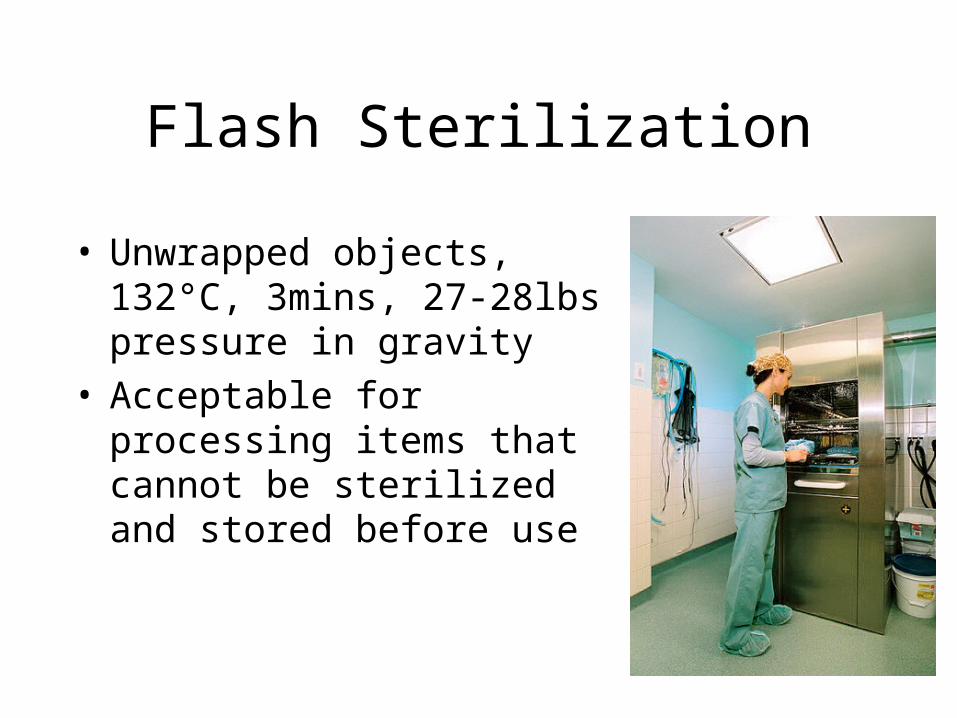
Flash Sterilization
• Unwrapped objects, 132°C, 3mins, 27-28lbs pressure in gravity
• Acceptable for processing items that cannot be sterilized and stored before use
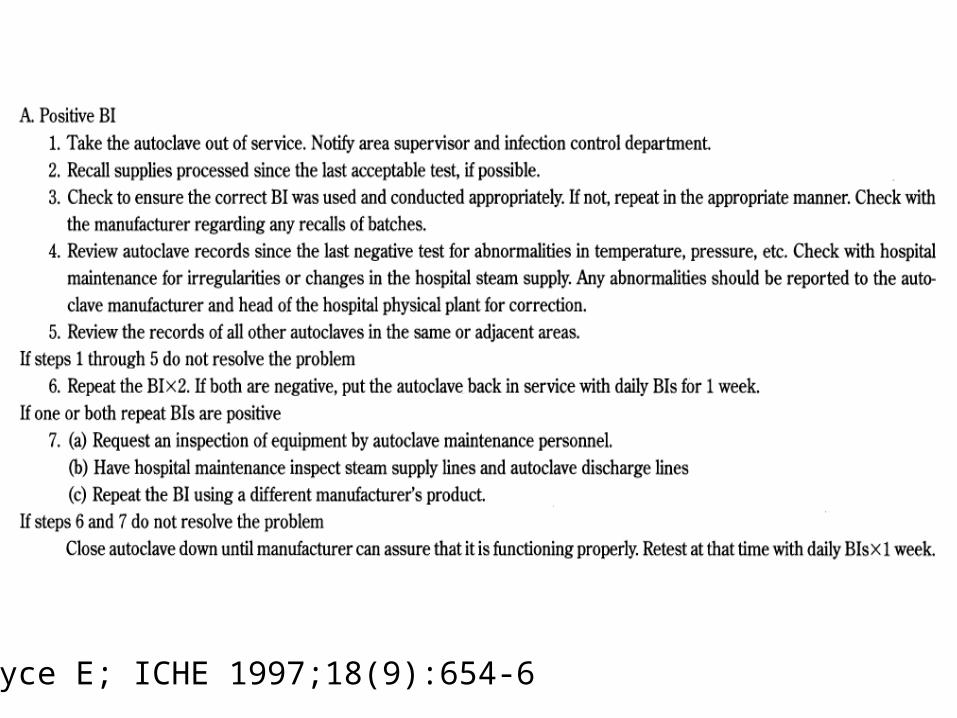
Bryce E; ICHE 1997;18(9):654-6

Reprocessing for Prions
• High risk patient– Known/suspected CJD or other TSEs
– Rapidly progressive dementia
– Family history of CJD or other TSE
– History of dura mater transplant, cadaver-derived pituitary hormone injection
• High risk tissue– Brain, spinal cord, eyes
• High risk device– Critical or semi-critical

Inactivation of Prions
• Steam sterilization with NaOH• Alkaline cleaner (pH 2.2, 1 hr 23°C)• Copper plus peracetic acid• Vapourized hydrogen peroxide (Sterrad NX)
Yan ICHE 2004;25:280, Fichet Lancet 2004;384:251, Baier JHI 2004;57:80, Lemmer J Gen Virol 2004;85:3805; Roger-Kreuz, ICHE 2009;30(8):769-77 Lehman Hosp Infect. 2009;72(4):342-50;

Semi-critical items
• Endoscopes/bronchoscopes
• Laryngoscopes
• Respiratory therapy and anaesthesia equipment
• Tonometers
• Endocavitary probes
• Vaginal specula, diaphram fitting rings


Problems with semi-critical items
• Complex and delicate pieces of equipment
• Expensive equipment used frequently– Centralizing process difficult– Time an important factor
• Absence of regulation/guidance for design
• Narrow margin of safety





Endocavitary probes
• Prostate & vaginal ultrasounds, TEE
• Trans-rectal biopsies
• Transvaginal probes for IVF
• Infrared coagulation for hemmorhoids


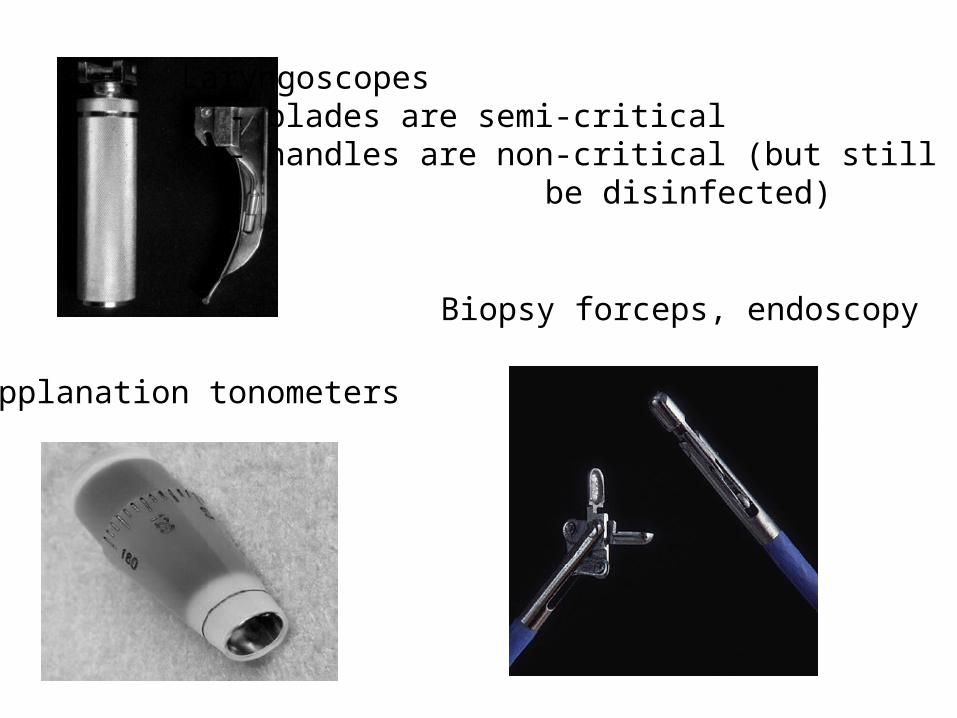
Laryngoscopes- blades are semi-critical- handles are non-critical (but still need to
be disinfected)
Applanation tonometers
Biopsy forceps, endoscopy

Disinfection of tonometers
Rutala AAC 2006;50:1419
Recent Toronto problems• Badly designed connectors (Steris)• Inadequate manufacturer’s instructions (trans-
rectal biopsies)• Belief that a freeze thaw cycle for cryotherapy
probe will kill microbes• Both reservoirs in endoscopy washer/disinfector
filled with detergent• 2% hydrogen peroxide for high level disinfection• Vaginal ultrasound probes• Breast pump kits• Sterilizer failures

Solutions
• Centralization of disinfection & sterilization wherever possible
• Standards: PIDAC, CSA– Processes, monitoring, training
• New technology– Endoscopes that can be steam sterilized– Better sterilization technology
• Elimination of high-level disinfection

Outbreaks (1999-2007
• Failure to clean/disinfect/sterilize adequately– Manual balloons for ventilation (B. cereus)– Pasteurizer failure (x2)– Thermometers (E. cloacae, NICU) – x3– Temperature sensors for ventilators (S. maltophilia) x 2– Ophthalmology equipment (adenovirus)– Endoscopes (TB x3, P.aeruginosa x2, pseudo outbreaks x5)– OR sterilization/high-level disinfection failure– Forceps in cystoscopy (P. aeruginosa)– Rigid laryngoscopes in NICU (P. aeruginosa, M. tuberculosis)– Transrectal prostate needle biopsies (P. aeruginosa x2)– Transesophageal echocardiography probes (E. cloace)– Bite blocks (P. aeruginosa, Group A streptococci)– Laparoscopy ports (Mycobacterium chelonae)

Outbreaks (2)• Contaminated disinfectants.
• Non-antimicrobial soap x2
• Benzalkonium chloride and other quaternary ammonium compounds
• 0.5% chlorhexidine
• Chlorhexidine without alcohol
• Improperly diluted disinfectants (disinfectant spray, environmental cleaning solutions)
• Open containers with soaked cotton balls
• S. marcescens, P. aeruginosa, M. abscessus, R. picketii, A. xylosoxidans, K. oxytoca,
Outbreaks (3)
• Other– Incompetent waste drain ports on hemodialysis
machines x2– Inadequately maintained endoscopy
washer/disinfector – Incorrect hook-up for endoscopes to sterilizer– Environmental contamination with
Acinetobacter

Outbreaks (4)Adverse effects
• Anterior segment syndrome post cataract surgery due to residual glutaraldehyde
• Toxic endothelial cell destruction (TECD) syndrome after ophthalmologic surgery due to brass degradation by plasma gas sterilization
Non-critical items


Factors necessary for environmental transmission
• The organism must survive in the environment
• Environmental contamination must occur frequently
• The organism must maintain its virulence
• The organism must be transported from the environment to (new) patients

Epidemiology of streptococcal infectionsTransmission of epidemic and non-epidemic
streptococci in military barracks
0
10
20
30
40
50
60
70
Blankets harbouring streptococci Blankets not harbouring streptococci
Acqu
isiti
on o
f GAS
pe
r 100
0 m
an-w
eeks
Wannamaker, Chap 12 in McCarty, Streptococcal Infections, 1954



MRSA and environmental transmission
• 20 month retrospective study in 8 ICUs where patients were screened weekly
• Assessed odds of acquiring MRSA among patients admitted to rooms just vacated by MRSA + and + patients
• MRSA acquired by: 2.9% of those admitted to MRSA- pt room 3.9% of those admitted to MRSA + pt room
Huang SS, Arch Int Med 2006;166:1945
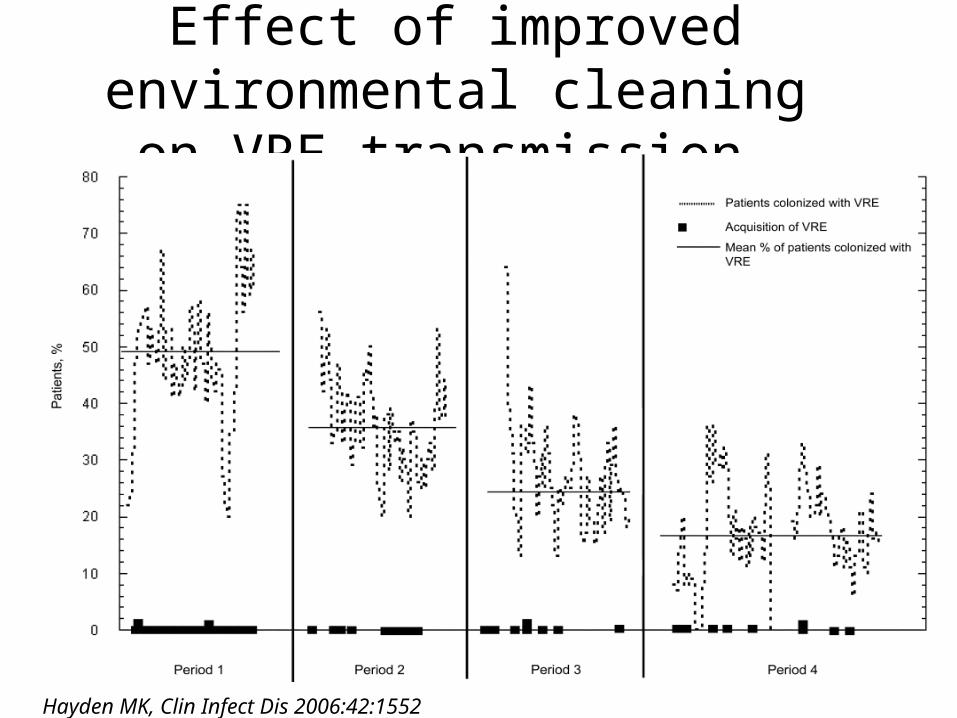
Effect of improved environmental cleaning on VRE transmission
Hayden MK, Clin Infect Dis 2006:42:1552

Can environmental cleaning reduce MRSA transmission?
• Setting: ward with endemic MRSA, and widespread environmental contamination
• Before-after study– Cleaning time increased by 57 hours per week
– Responsibility for routine cleaning of shared equipment delineated
• In 6 months post-intervention, number of MRSA acquisitions decreased fro 30 to 3 per 6 months
Rampling A JHI 2001;49:109
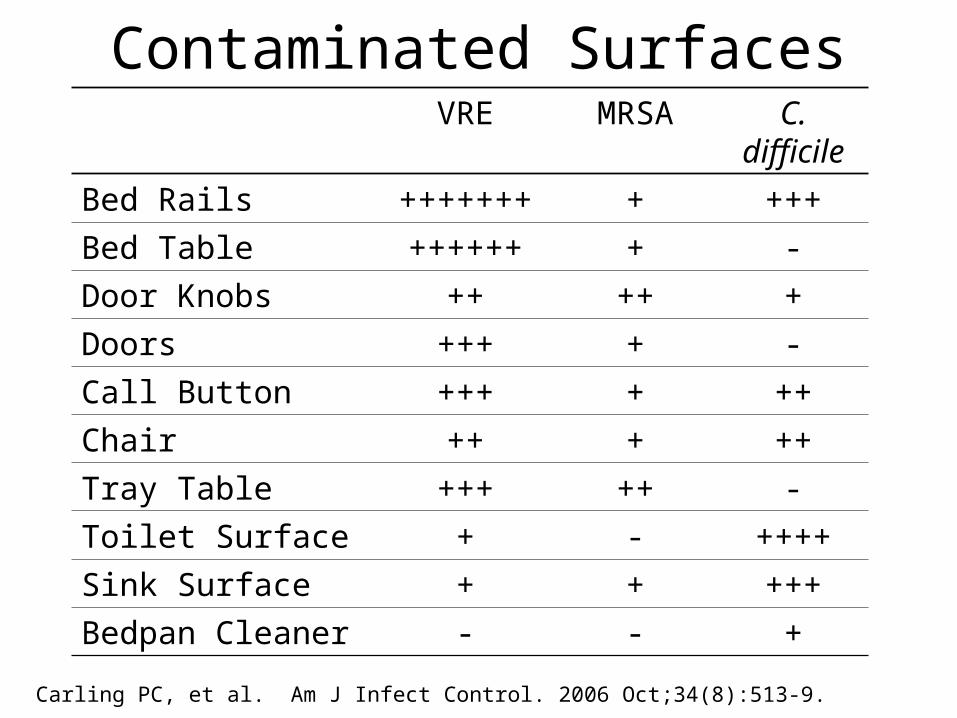
Contaminated SurfacesVRE MRSA C.
difficile
Bed Rails +++++++ + +++
Bed Table ++++++ + -
Door Knobs ++ ++ +
Doors +++ + -
Call Button +++ + ++
Chair ++ + ++
Tray Table +++ ++ -
Toilet Surface + - ++++
Sink Surface + + +++
Bedpan Cleaner - - +
Carling PC, et al. Am J Infect Control. 2006 Oct;34(8):513-9.

Contamination of objects/areas exclusively
touched by staff
• Supply cabinets, ICU telephones, keyboards
33.3% MRSA
36.6% VRE
Speck et al., Abstract, (2007) SHEA 17th Annual Scientific Meeting, Baltimore, MD

Problems
• How important is environmental transmission overall?
• What do we mean by “environment”?
• What is the right standard for “clean”?
• How do we measure adherence?

Improving non-critical item/environment disinfection
• Audit and feedback
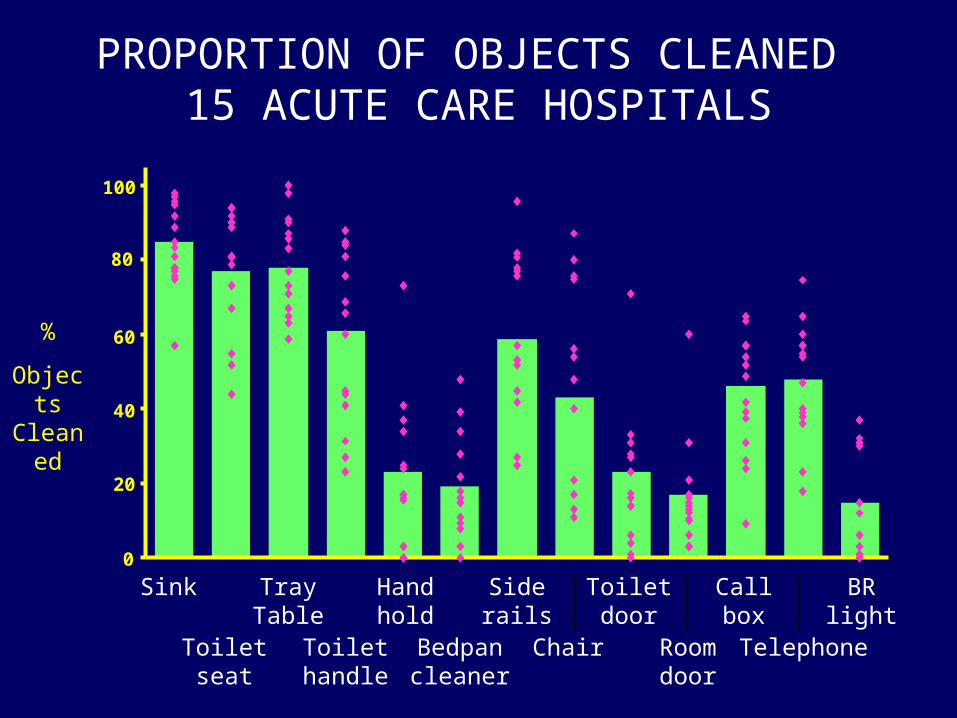
PROPORTION OF OBJECTS CLEANED 15 ACUTE CARE HOSPITALS
%
Objects Cleaned
0
20
40
60
80
100
Sink
Toiletseat
TrayTable
Toilethandle
Bedpancleaner
Chair Roomdoor
Telephone
Handhold
Siderails
Toiletdoor
Callbox
BRlight
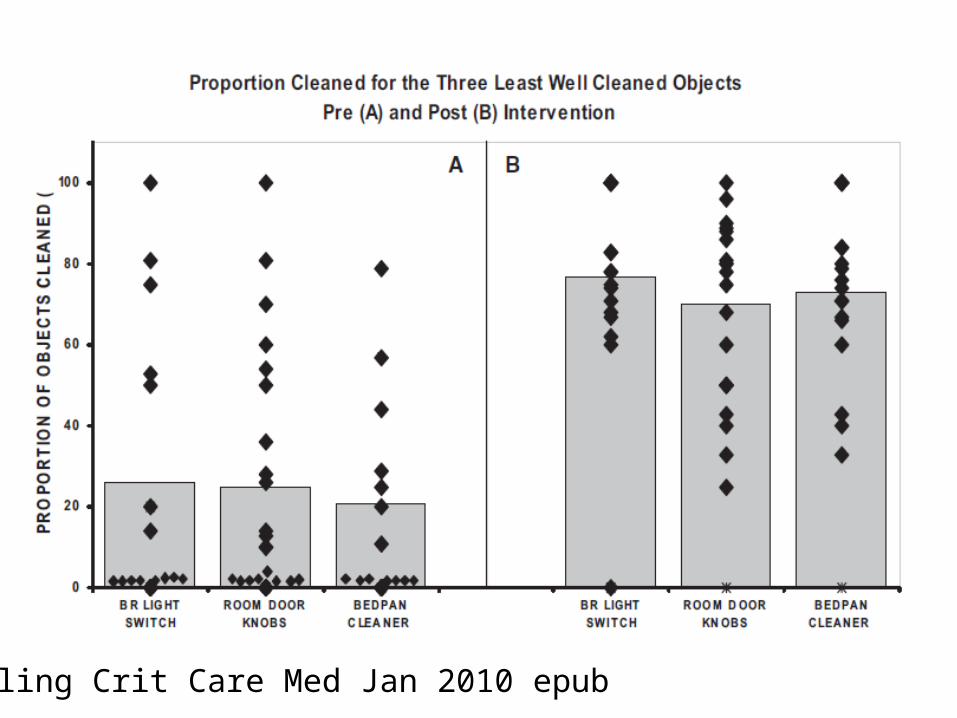
Carling Crit Care Med Jan 2010 epub
Improving non-critical item/environment disinfection
• Audit and feedback
• New technology– Hydrogen peroxide vapour/gas – UV room decontaminaion– ?antibacterial surface coatings?
Otter ICHE 2009;30(6):574-7

• Seymour S. Block: Disinfection, sterilization and preservation– Williams &Wilkins (ISBN 0812113640)
• PIDAC best practices for cleaning, sterilization and disinfection http://www.health.gov.on.ca/english/providers/program/infectious/diseases/best_prac/bp_cds_2.pdf
• PIDAC best practices for environmental cleaning
http://www.health.gov.on.ca/english/providers/program/infectious/diseases/best_prac/bp_enviro_clean.pdf
• CDC guideline for disinfection and sterilization in healthcare facilities http://www.cdc.gov/hicpac/pdf/guidelines/Disinfection_Nov_2008.pdf
• Bryce EA et al. When the biological indicator is positive: investigating autoclave failures Infect Control Hosp Epi 1997;18:654-6
• Rutala WA, Weber DJ. How to assess risk of disease transmission to patients when there is a failure to follow recommended disinfection and sterilization guidelines Infect Control Hosp Epidemiol. 2007;28(2):146-55