stroke work-up and early secondary prevention · objectives •recognize stroke symptoms....
TRANSCRIPT

Acute Ischemic Stroke Managementand
Early Secondary Prevention
Alison P. Smock, MD
Roper St Francis HealthcareNeurohospitalist
Vascular Neurologist
Medical University of South CarolinaClinical Instructor
REACH Telestroke Physician

Disclosures
• None

Objectives
• Recognize stroke symptoms.
• Identify acute stroke interventions.
• Describe the basics of stroke work-up.
• Classify stroke subtypes and etiologies.
• Apply disease-specific secondary prevention measures for stroke patients.

What is a Stroke?
• A stroke is a potentially devastating, life-threatening emergency.
• A stroke is a ‘BRAIN ATTACK’ in which the brain is suddenly deprived of blood flow and consequently, oxygen.

Definitions
• Transient ischemic attack– A transient episode of neurological dysfunction
caused by focal brain, spinal cord, or retinal ischemia, without acute infarction
– Tissue-based definition rather than time-based definition
• Stroke– Infarction of the central nervous system – May be symptomatic or silent– May not be evident by MRI
Stroke. 2009;40:2276-2293

Transient Ischemic Attack
• ABCD2 score
– Clinical score to determine the risk for stroke within the first 2 days following a TIA
Age BP Clinical Features Duration Diabetes
1 point ≥ 60 SBP ≥ 140
OR
DBP ≥ 90
Speech disturbance without unilateral
weakness
10-59 min Yes
2 points -- -- Unilateral weakness with or without speech
impairment
≥60 min --
Lancet. 2007;369:283-292.

Transient Ischemic Attack
ABCD2 score 2-day stroke risk Comment
0-3 1.0% Hospital observation may be unnecessary without another indication (ie new onset Afib)
4-5 4.1% Hospital observation justified in most situations
6-7 8.1% Hospital observationworthwhile
Lancet. 2007;369:283-292.

There are two ways a stroke may occur:
• Ischemic Stroke
• Hemorrhagic Stroke

Ischemic Stroke
http://watchlearnlive.heart.org/CVML_Player.php?moduleSelect=iscstr
In an ischemic stroke, an artery supplying the brain becomes blocked by plaque build-up or from a blood clot.

Large Vessel Stroke Syndromes
• MCA – dominant hemisphere– Contralateral hemiparesis (face/arm > leg)
– Contralateral hemisensory changes
– Head and eye deviation toward stroke
– Contralateral hemianopia
– Aphasia
– Alexia
– Agraphia
– Acalculia
– Apraxia

http://www.aphasianow.org/store/files/BrainChart

Large Vessel Stroke Syndromes
• MCA – non-dominant hemisphere– Contralateral hemiparesis (face/arm > leg)– Contralateral hemisensory changes– Neglect/extinction– Anosognosia– Loss of prosody of speech– Flat affect
• ACA– Leg paresis > arm paresis– Frontal signs (abulia)– Urinary incontinence

Large Vessel Stroke Syndromes
• Posterior Circulation
– Extra/Intracranial Vertebral Artery
Dizziness/Vertigo
Cranial nerve lesions
Cerebellar symptoms• Extremity, truncal or gait ataxia
• Nystagmus
http://radiopaedia.org/images/7513</a>

http://www.neuropenews.org/?attachment_id=2010
Large Vessel Stroke Syndromes
• Posterior Circulation
– Basilar artery
• Typically presents as ischemia in the pons
• Asymmetric but bilateral motor and reflex abnormalities
• Bulbar involvement
• Respiratory involvement
• “Tip of the Basilar” – Decreased LOC
– Oculomotor/pupillary abnormalities
– Quadriparesis/plegia

Large Vessel Stroke Syndromes
• Posterior Circulation
– Posterior Cerebral Artery
Homonymous hemianopia
Hemisensory changes (lateral thalamus)
Left PCA – alexia without agraphia
Right PCA – prosopagnosia, visual neglect
Bilateral – cortical blindness (Anton’s syndrome)
http://www.neuroradiologycases.com/2012/09/ischemic-stroke-and-vascular.html

Small Vessel Stroke Syndromes
• Pure motor– Corona radiata, posterior limb of the internal capsule,
pons, medulla
• Pure sensory– Thalamus
• Sensorimotor– Thalamus, basal ganglia
• Ataxic hemiparesis– Corona radiata, anterior limb of the internal capsule
• Dysarthria-clumsy hand syndrome– Upper pons, junction between CR and IC

Hemorrhagic Stroke
Copyright © 2012 University of Washington
A blood vessel supplying the brain bursts, causing bleeding in the brain.
Intracerebral hemorrhage (ICH) occurs in the brain tissue itself.
Subarachnoid hemorrhage (SAH) occurs on the outside of the brain.

© 2009, American Heart Association. All rights reserved.
Hemorrhage Symptoms
• Hemorrhage– Focal neurological deficits as in AIS
– Headache (especially in subarachnoid hemorrhage)
– Neck pain
– Light intolerance
– Nausea, vomiting
– Decreased level of consciousness

Acute Stroke

Nursing, Council on Peripheral Vascular Disease, and Council on Clinical Cardiologyon behalf of the American Heart Association Stroke Council, Council on Cardiovascular
Howard YonasRosenfield, Phillip A. Scott, Debbie R. Summers, David Z. Wang, Max Wintermark andBart M. Demaerschalk, Pooja Khatri, Paul W. McMullan, Jr, Adnan I. Qureshi, Kenneth
Edward C. Jauch, Jeffrey L. Saver, Harold P. Adams, Jr, Askiel Bruno, J.J. (Buddy) Connors,Stroke Association
Guideline for Healthcare Professionals From the American Heart Association/American Guidelines for the Early Management of Patients With Acute Ischemic Stroke : A
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STR.0b013e318284056a
2013;44:870-947; originally published online January 31, 2013;Stroke.
http://stroke.ahajournals.org/content/44/3/870
World Wide Web at: The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2013/01/29/STR.0b013e318284056a.DC1.htmlData Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 24, 2013http://stroke.ahajournals.org/Downloaded from


Key Concept: Time is Brain!
• 1.8 Million neurons are lost per minute during a large vessel occlusion
• Ischemic brain will age 3.6 years for every hour a large vessel stroke goes untreated
• Meta-analysis: 33 studies with 1094 patients– Odds of a good outcome increase 4.5x with “successful” revascularization
Saver JL (2006). Time is brain—quantified. Stroke 37: 263–266
Rha J-H, Saver JL (2003). Recanalization as a surrogate outcome measure in thrombolytic clinical trials: a meta-analysis. Stroke 34: 347 (abstract)

FDA approved options
• (r)tPA (recombinant) tissue plasminogen activator – Gold Standard
– Approved for use within 3 hours of onset of neurologic deficits in a defined population of patients
• Aspirin 325mg
– Approved for use in patients who:
• Do not receive tPA
• Do not have any contraindications (drug allergy)
• 24 hours after receiving tPA if there is no hemorrhage on 24h post-tPA CT/MRI scan


Time to Treatment Influences Outcomes
Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004;363:768–74
NNT= 2 NNT= 4 NNT= 9 NNT is number of patients needed to treat for one to have a significantly improved outcome.

tPA
• Remains the only medication proven to affect outcomes when given in the hyper acute time frame after ischemic stroke
• Despite the well-established benefit of tPA, only an estimated 3-5% of patients are getting treated

Why Aren’t Patients Getting Treated?
• Delays in presentation
• Not recognizing stroke symptoms
• Long list of exclusions…

Limitations of IV tPA
• Generalizability– 4% utilization of tPA – ~25% present within 3 hours; 29% eligible
• Big strokes are tough– Baseline NIHSS >10 and a dense MCA sign
predicted poor clinical outcome– TTATS recanalization rate of no more than 30% for
large vessel occlusion
• Sustained recanalization in only 10-20%
• Increased risk of sICH with larger strokes
(Kleindorfer Stroke 2004; 35:27-29)
(Tomsick. AJNR 1996; 17:79-85)
(Genentech, Summary basis for Activase approval. NDA. PLA96-0350)
(Alexandrov. NEJM 2004;10:1379-83)
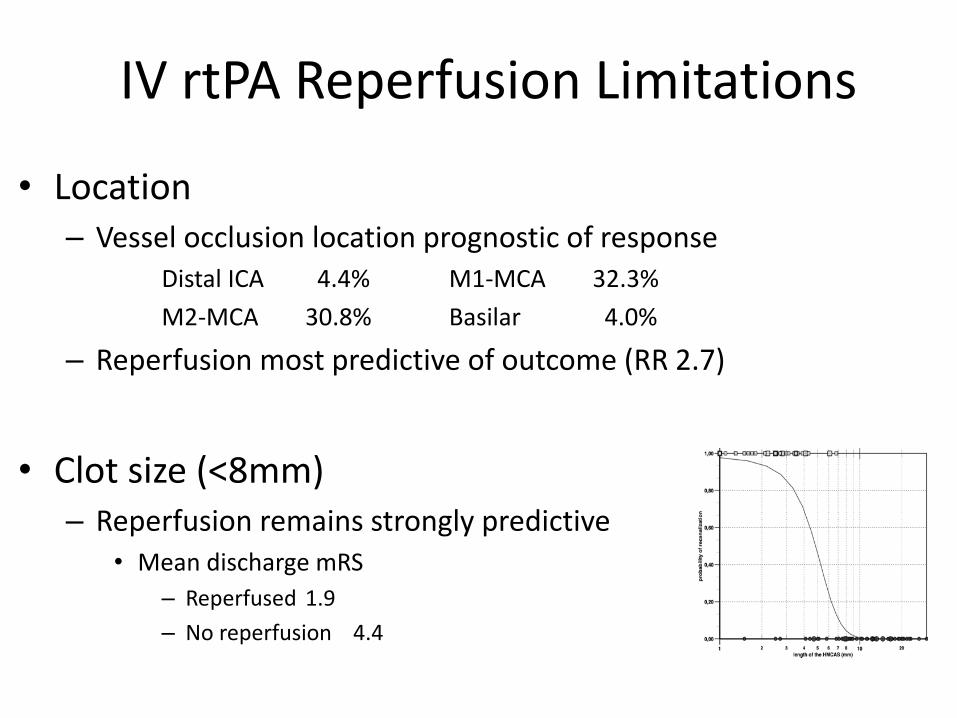
IV rtPA Reperfusion Limitations
• Location– Vessel occlusion location prognostic of response
Distal ICA 4.4% M1-MCA 32.3%
M2-MCA 30.8% Basilar 4.0%
– Reperfusion most predictive of outcome (RR 2.7)
• Clot size (<8mm)– Reperfusion remains strongly predictive
• Mean discharge mRS
– Reperfused 1.9
– No reperfusion 4.4
(Bhatia Stroke. 2010;41:2254-2258)
(Riedel, Stroke. 2011;42:1775-1777)

Potential Limitations of IV rt-PA
• Reperfusion is dependent upon available substrate and time to lyse clot
• Stimulates platelet activation (reocclusion?)
• May not be as effective with larger, older, more organized clots
• Hemorrhagic transformation concerns

What Else Can We Do?
• THROMBECTOMY
– MR CLEAN
– SWIFT PRIME
– EXTEND-IA
– ESCAPE
– REVASCATS


Large Vessel Occlusion
Patients eligible for intravenous r-tPA should receive intravenous r-tPA even if endovascular treatments are being considered (Class I; Level of Evidence A). (Unchanged from the 2013 guideline)
Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria (Class I; Level of Evidence A). (New recommendation):
(a) prestroke mRS score 0 to 1,(b) acute ischemic stroke receiving intravenous r-tPA within 4.5 hours of onset according to guidelines from professional medical societies,(c) causative occlusion of the internal carotid artery or proximal MCA (M1), (d) age ≥18 years,(e) NIHSS score of ≥6, (f) ASPECTS of ≥6, and(g) treatment can be initiated (groin puncture) within 6 hours of symptom onset
(Stroke. 2015;46:000-000.)

Large Vessel Occlusion
As with intravenous r-tPA, reduced time from symptom onset to reperfusion with endovascular therapies is highly associated with better clinical outcomes. To ensure benefit, reperfusion to TICI grade 2b/3 should be achieved as early as possible and within 6 hours of stroke onset (Class I; Level of Evidence B-R). (Revised from the 2013 guideline)
When treatment is initiated beyond 6 hours from symptom onset, the effectiveness of endovascular therapy is uncertain for patients with acute ischemic stroke who have causative occlusion of the internal carotid artery or proximal MCA (M1) (Class IIb; Level of Evidence C). Additional randomized trial data are needed. (New recommendation)
(Stroke. 2015;46:000-000.)


Thrombectomy Candidates
• Large vessel occlusion
• Bad patient, good scan
• They do not have to have tPA in order to get thrombectomy


Early Secondary Prevention

Stroke Work-Up
• Brain Imaging
• Pump
• Pipes
• Passengers

Keep In Mind…
• All TIA and stroke patients are fully evaluated for stroke risk factors, regardless of known medical co-morbidities

Brain Imaging
• Non-Contrasted CT Head– PROS
• Rules in/out hemorrhage
• Large territory infarcts
• Quick, accessible
• Good alternative if not able to tolerate MRI
– CONS• Does not visualize posterior fossa or brainstem
structures well
• Radiation
• “Age indeterminate infarct”

Brain Imaging
• MRI brain with and/or without contrast– PROS
• Meets criteria to define stroke vs TIA
• Visualizes smaller areas of ischemia not seen on CT
• Reveals previous injury (ie microangiopathy, multi-territory infarcts)
• Microhemorrhages
• May identify stroke mimics
– CONS• Can’t have AICD/pacemakers (not always…)
• Can’t be claustrophobic
• Have to be able to sit still for minimum 15 minutes

Cardiac Work-Up: The Pump
• EKG
• Continuous telemetry
• Transthoracic Echo (TTE)– Ejection fraction
– Evidence of wall motion abnormalities
– Vegetations
– LV thrombus
– Left atrial appendage thrombus
– PFO/ASD (in select patients)• If +PFO venous doppler of 4 extremities, pelvic vein
imaging

Cardiac Work-Up: The Pump
• Advanced cardiac imaging may be warranted:– Appearance of multiple territory infarcts
– Normal blood vessels
– Stigmata of atrial fibrillation on TTE• Atrial enlargement
• Generally leads to a cardiology consult– TEE / cardiac MRI / cardiac CT
• Implantable loop monitors versus 30 day event monitors

Vessel Imaging: The Pipes
http://www.cixip.com/index.php/page/content/id/1007 http://www.studyblue.com/notes/note/n/airway-77-93/deck/3078597


Options for Vessel Imaging
• Carotid ultrasound (CUS)
• Transcranial doppler (TCD)
• CT angiogram head & neck (CTA)
• MR angiogram head & neck (MRA)
• Digital subtraction angiography (DSA)

AJMR Am J Neuroradiol 2013;34(E117-E127)

Carotid Ultrasound
• PROS
– Plaque characterization
– Helps determine flow if question of stenosis vs occlusion
– Non-invasive
• CONS
– Does not visualize arch, vertebral arteries, or intracranial vessels
– May overcall a critical stenosis as occlusion

Transcranial Doppler
• PROS– Intracranial vessel stenosis vs occlusion
– Vasospasm in SAH
– Microemboli signal monitoring
– Non-invasive
• CONS– Blind doppler
– Does not visualize arch
– Need specially trained techs and experienced interpretation
• PROS
– Quick, reliable, accurate
– Available in most EDs and hospitals
– Non-flow dependent (like MRA)
– Less prone to motion artifact
• CONS
– Contrast load
– Radiation
CT Angiogram Head & Neck

MR Angiogram Head & Neck
• PROS
– Reliable, accurate
– Can be done without contrast
– No radiation exposure
• CONS
– AICDs or pacemakers (not always…)
– May overcall degree of stenosis or occlusion
– Susceptible to motion artifact

What Do We Gain From Head & Neck Imaging?
• Identifies proximal sources of embolism
• May identify left atrial appendage thrombus
• Identifies extra/intracranial large artery abnormalities– Plaque characteristics
– Presence of intraluminal thrombus
– Dissections
– Degree of stenosis

• There is growing evidence to show that the presence of intracranial vessel abnormalities in TIA and non-disabling stroke patients, detected using CTA, predicts the risk of recurrent stroke and clinical outcomes at 90 days
• CTA can therefore be used as a risk stratification tool
Diagnostic Information

Labs: The Passengers
• Basic Blood Work
– CBC
– CMP
– Lipid panel
– A1c
– Urinalysis
– UDS
• Disease Specific
– B12
– Homocysteine
– RPR
– TSH
– Rheumatologic labs
– Hypercoagulable labs

Stroke Subtypes



Ischemic Stroke
Large Artery Atherosclerosis
Atherothrombotic
Atheroembolic
WatershedSmall Vessel
Disease (Lacune)
Cardioembolic
Structural
Heart failure
Valvular
Shunts
PFO
ASD
Arrhythmia
Other
Non-Athero Vasculopathy
Dissection
Moya Moya
VasculitisHypercoagulable
State
Venous Thrombosis
Hematologic Disorders
Cryptogenic
Standard Acute Secondary Prevention
• Antithrombotic therapy (antiplatelet or AC)
– By the end of day 1
• Statin therapy
– Upon admission
• Blood pressure management (after acute phase)
• Blood glucose control

Antithrombotics: Acute Management
• Antiplatelet therapy
– All stroke patients
– Aspirin, clopidogrel, dipyridamole/aspirin
– For stroke, patients only need ONE antiplatelet agent long term
– Dual antiplatelet therapy: select situations
– Choice of antiplatelet medication should be based on safety, cost, patient characteristics, patient preference
Antithrombotics: Acute Management
• Patients who present with a first or recurrent stroke are commonly already taking an antiplatelet medication
• There have been no clinical trials to indicate that switching antiplatelet agents reduces the risk for subsequent events

Antithrombotics: Acute Management
• Anticoagulation therapy– CLEAR INDICATIONS
• Atrial fibrillation
• LV thrombus
• LAA thrombus
• Identified hypercoagulable state
• Others:– PE, DVT, mechanical valve
THERE IS NO INDICATION FOR A HEPARIN DRIP IN AN ACUTE STROKE PATIENT UNLESS AN IDENTIFIED INDICATION FOR ANTICOAGULATION EXISTS
When is it Safe to Anticoagulate?
• Atrial fibrillation– Worst case scenario: large territory infarct (risk of
hemorrhagic transformation) or if patient already has HT or a hematoma
– HAEST: risk of recurrent ischemic stroke during first 14 days in patients with Afib and on aspirin only = 7.5%
Guidelines support initiating AC within 14 days of stroke onset

When is it Safe to Anticoagulate?
• Other listed conditions…
– It is a risk/benefit discussion with the patient

Statins: Acute Management
• Revised lipid guidelines November 2013
• No longer “treating to a number”
• Every stroke patient gets a statin!


Blood Pressure: Acute Management
• Permissive hypertension– Allows for collateral flow to provide adequate
perfusion to the at-risk area of ischemia– Optimal blood pressure range during acute stroke has
not been established– Most patients declare themselves with a clinical
decline when pressure dependent– May also give IVFs and place in Trendelenburg
position to improve perfusion– Within the first 24 hours, it is reasonable not to lower
blood pressure unless >220/120 or another concomitant medical condition would benefit from lowering BP

Blood Pressure: Acute Management
• After 24 hours, most patients will begin to normalize on their own– BP meds should be initiated after 24 hours
• Most will require some antihypertensive medication– This can be catered to the patient
• Goal < 140/90– Unless diabetic or with recent lacune: < 130/80
Blood Glucose: Acute Management
• Persistent in-hospital hyperglycemia during the first 24 hours after stroke is associated with worse outcomes than normoglycemia
• Treat hyperglycemia to achieve blood glucose levels in a range of 140 to 180 mg/dL
• Long term goal A1c <7%

Etiology-Specific Treatment
• Extracranial carotid stenosis– SYMPTOMATIC
• 70-99% stenosis, CEA is recommended
• 50-69% stenosis, CEA is recommended depending on patient-specific factors
• Stenosis <50%, CEA and CAS are not recommend
• It is reasonable to perform CEA within 2 weeks of TIA or stroke
– ASYMPTOMATIC• Unclear if medical therapy or intervention is best
option
• CREST 2

Etiology-Specific Treatment
• Intracranial atherosclerotic disease (ICAD)
– Symptomatic severe 70-99% stenosis
• Aspirin 325mg + Clopidogrel 75mg x 90 days: SAMMPRIS
– If indication exists for anticoagulation, warfarin is an option for ICAD: WASID

Etiology-Specific Treatment
• Large artery dissection
– Aspirin = warfarin: CADISS
• If the dissection extends intracranially, anticoagulation puts patient at risk for SAH

Etiology-Specific Treatment
• Non-disabling stroke (NIHSS < 4) or high-risk TIA (ABCD2 ≥ 4): CHANCE
– Clopidogrel load 300mg + aspirin 325mg day 1
– Clopidogrel 75mg + aspirin 325mg days 2-21
– Antiplatelet monotherapy thereafter

Etiology-Specific Treatment
• Atrial Fibrillation– CHADS2VASc
– Anticoagulation• Warfarin (with aspirin bridge)
• NOACs– Dabigatran
– Rivaroxaban
– Apixaban
– Evidence is insufficient to determine whether AF catheter ablation reduces risk of recurrent stroke• Recommended to continue AC in these patients

Etiology-Specific Treatment
• Cerebral Venous Sinus Thrombosis
– Hypercoagulable work up
– Screen for: dehydration, severe anemia, OCPs, smoking
– Anticoagulation (even in presence of hemorrhage)

Etiology-Specific Treatment
• Patent Foramen Ovale– PFO IS NOT A STROKE RISK FACTOR
• 15-25% of the population has a PFO
– Search for venous embolism• 4 extremity venous ultrasound
• Pelvic vein imaging (MRV, CTV)
• Hypercoagulable work up
• Anticoagulation if clear indication identified
– There is no data that anticoagulation is superior to antiplatelet therapy
– There is no data that closure of PFO reduces risk of stroke recurrence

Etiology-Specific Treatment
• Cryptogenic stroke
– After imaging, echo, vessels, labs are normal…
– All require a 30 day event monitor upon discharge
– Antiplatelet agents are appropriate for secondary prevention
THERE IS NO EVIDENCE TO EMPIRICALLY ANTICOAGULATE CRYPTOGENIC STROKE
PATIENTS!

Special Labs
Hypercoagulable labs
• Protein C
• Protein S
• Antithrombin III
• Factor V Leiden
• Antiphospholipid antibody panel
• Prothrombin gene mutation
• MTHFR gene mutation
• Homocysteine
• Factor 8 assay
Rheumatologic labs
• ANA
• dsDNA
• Lupus anticoagulant
• dRVVT
• Hep B
• Hep C
• ENA panel
• CRP
• ESR

Special Considerations
• Oral contraceptives/hormonal replacement
• Rx NSAIDs (meloxicam, celecoxib, etc)
• Chemotherapy medications

Summary of Stroke Don’ts
• Do not put your stroke patient on a heparin drip unless there is a clear indication
• Do not anticoagulate carotid occlusions
• Do not anticoagulate cryptogenic strokes
• Do not switch between antiplatelet medications unless there is a specific reason
• Do not close PFOs
Always have a reason for doing what you are doing!


Stroke Subtypes – Images
Left thalamic stroke: http://www.neurology.org/content/81/23/e177/F1.large.jpg
Right MCA stroke: http://frontalcortex.com/gallery/pics/jdmiles___0000000000_1361395245_i.jpg
Right ICA watershed stroke: http://www.angiologist.com/wp-content/uploads/2011/03/Watershed-infarct-DWI-protocol-MRI.jpg
Embolic stroke: http://stroke.ahajournals.org/content/31/3/688/F2.large.jpg
Venous infarct: http://www.consultant360.com/sites/default/files/images/May_figA%26B_CTscan.jpg
Moya Moya angiogram: http://images.radiopaedia.org/images/537650/6a247e2a208f320c71e9dd36f03698.png
Carotid dissection angiogram: http://images.radiopaedia.org/images/18028/4768e9c8d3059634470bada1a8d7e2.jpg