structured sentencing act
DESCRIPTION
NC TASC Effective Case Management for Improved Offender & System Outcomes September 30, 2004 Annapolis, Maryland. Structured Sentencing Act. Truthful & consistent sentencing that projects resource needs Established 3 forms of punishment Established statutory continuum of sanctions - PowerPoint PPT PresentationTRANSCRIPT

NC TASC Effective Case
Management for Improved Offender &
System Outcomes
September 30, 2004Annapolis, Maryland
NC TASC Effective Case
Management for Improved Offender &
System Outcomes
September 30, 2004Annapolis, Maryland

Structured Sentencing ActTruthful & consistent sentencing that
projects resource needsEstablished 3 forms of punishmentEstablished statutory continuum of sanctionsEliminated discretionary parole Established model for matching sentences &
resources
SSA-related ExpansionsLargest Expansion of probation resources in
60 year history - 900+ positionsEnhanced TASC Expansion - 1.8 mil
established 13 new programs

TypeType of Punishmentof Punishment ImposedImposedTypeType of Punishmentof Punishment ImposedImposed
35%
47%
43%
28%
22%
26%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Active Intermediate Community
Structured Sentencing*
Old Law**
35%
47%
43%
28%
22%
26%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Active Intermediate Community
Structured Sentencing*
Old Law**
* SOURCE: NC Sentencing and Policy Advisory Commission* SOURCE: NC Sentencing and Policy Advisory Commission
** SOURCE: 1993 Pre-Structured Sentencing Data** SOURCE: 1993 Pre-Structured Sentencing Data
In 1993, Average Sentence served - 16 Months
Under SSA, Average Sentence served - 34 Months
Felonies

NC Problem Statement
NC Problem Statement
• Use of criminal justice & treatment resources
• Complex clients: challenging behavioral health needs & serious consequences of failure
• Recidivism & relapse are common
• Unmanaged cases, uncharted outcomes
• Service availability & effectiveness
• Prison pop offenders entering community in increasing numbers multiple unsuccessful tx & prison admissions
• Budget shortfalls & no expansions
• Use of criminal justice & treatment resources
• Complex clients: challenging behavioral health needs & serious consequences of failure
• Recidivism & relapse are common
• Unmanaged cases, uncharted outcomes
• Service availability & effectiveness
• Prison pop offenders entering community in increasing numbers multiple unsuccessful tx & prison admissions
• Budget shortfalls & no expansions
Need options to improve access to & retention in treatment, while preserving public safety

Evolving SolutionEvolving SolutionOur Common Goal: Safely manage high-risk,
high-need offenders in the community
– Treatment System Needs:• Less reliance on institutions• Better resource utilization & management• Increased community capacity• Effective treatment, interventions & case
management
– Justice System Needs:• Effective & available care
• Regular communication • Offender & treatment accountability
Our Common Goal: Safely manage high-risk, high-need offenders in the community
– Treatment System Needs:• Less reliance on institutions• Better resource utilization & management• Increased community capacity• Effective treatment, interventions & case
management
– Justice System Needs:• Effective & available care
• Regular communication • Offender & treatment accountability

OFFENDEROFFENDER
MANAGEMENTMANAGEMENT
MODELMODEL
ONE OFFENDER - ONE CASE PLAN - ONE TEAMONE OFFENDER - ONE CASE PLAN - ONE TEAM
DOCDOC DHHSDHHS
DCCDCC TASCTASC
Balances Intervention Opportunities provided thru DMHDDSAS & Controlled Supervision provided thru DCC

NC Offender Management Model
Target Population
I Punishment, C Punishments at-risk for Revocation, Post-Releasees who completed a prison tx program
Standard TASC Screening & Assessment
Individual Case Planning
by Probation & TASC
Control, Care & Service Management
Team staffings with shared decision-making between Probation & TASC

ArrestPre-TrialHearing
Pre-SentenceHearing
Trial/Sentencing
Div of Prisons/Post-Release
Div of CommunityCorrections
North Carolina Criminal Justice Planning Flow Chart
NC Offender Management Model (OMM)
Clinical Assessment
IndividualizedCase Plan
SubstanceAbuse Svcs
Employment
Medical ServicesHousing/Food/
Clothing
Education/Voc TrainingTransportation
Continuous Case Management and Case Staffing
Mental HealthServices
EXIT MODEL
Referred to OtherServices
Figure 1. NC Criminal Justice Flow Chart
CBI

SANCTIONS SUPERVISION TREATMENT TASC
NC Continuum of Sanctions, Supervision & Care
Cost & Intensity
Cost & Intensity
Cost & Intensity
Intermediate
•I Punishment
•Post-Release
•C Failures
•Sex Offenders
•Domestic Violence
•High Risk/High Need DWIs
Traditional Probation
Deferred Prosecution
Community
•C Punishment
•Unsupervised Failures
•Low Risk/Low Need DWIs
•PSIs & Targeting for Courts
Split Sentence
Community Detention
Drug Court
Enhanced Intensive
Intensive
Residential Tx
House Arrest
Day Reporting Center
Enhanced Traditional Probation
Contempt of Court (all supervision & tx levels)
No Tx
Therapeutic Community
Residential Tx
Intensive Outpatient
Tx
No Treatment
Outpatient Treatment
Education & Urinalysis
Level 1 Care Management w/
Tx Level 6 & Aftercare Services
Level 1, 2 or 3 Care Management w/ Tx Level 4 or 5
Level 1 or 2 Care Management w/ Tx Level 3
Level 1 Care Management w/ Tx Level 2
Treatment Matching
Assessment
Screening

Memorandum of Understandingbetween the
North Carolina Department of Health and Human Servicesand the
North Carolina Department of Correction
This Memorandum of Understanding (MOU) and Appendices are entered byand between the Department of Health and Human Services and theDepartment of Correction for the purpose of developing a comprehensiveoffender management model that ensures public safety while addressingthe needs of offenders. Currently, the Division of Community Corrections(DCC), the Criminal Justice Partnership Program (CJPP) and the TreatmentAlternatives to Street Crime (TASC) Network are the primary resourcesinvolved in community corrections. The Division of Alcoholism andChemical Dependency Programs (DACDP) and Division of Prisons (DOP)impact community corrections through the release of offenders who havereceived services while in custody. The purpose of a comprehensiveoffender management model is to create a seamless system built on theideals of integrated service delivery and coordination of resources thatprovide effective interventions for offenders.
With DCC, CJPP, and TASC available under the community correctionsumbrella and a structured link with DACDP and DOP for transitioningoffenders, the Offender Management Model (OMM), as described in theAppendices, presents a systemic model for screening and assessingoffenders, matching them to the appropriate intervention(s) and managingtheir case plans. Utilizing the principles of effective interventions, we canreasonably assert that the OMM will be successful in modifying offenderbehavior. The objectives of the OMM are:
To create a seamless system of care for the provision of services tooffenders;
To clarify roles in providing control and treatment; To reduce the rate of revocation for technical and drug violations; To combine efforts to guarantee the effective utilization of limited
resources and prevent duplication; To provide cognitive behavioral interventions; To develop an integrated information system; and To ensure Probation, CJPP, DACDP, DOP and TASC staff are trained to
implement the OMM.

Objectives of OMMObjectives of OMM Seamless system of care for the provision of services to
offenders, improving access to treatment for justice clients
Clarify roles & responsibilities in providing control & treatment, eliminating duplication
Target limited resources to the right clients: Combine efforts to guarantee effective utilization of limited resources
with a team approach & shared decision-making Emphasize quality over quantity
Develop coordinated information systems
Ensure staff are trained to implement the OMM
Reduce rates of revocation for technical & drug violations, while increasing accountability & community safety
Increase efficiency & improve client outcomes
Seamless system of care for the provision of services to offenders, improving access to treatment for justice clients
Clarify roles & responsibilities in providing control & treatment, eliminating duplication
Target limited resources to the right clients: Combine efforts to guarantee effective utilization of limited resources
with a team approach & shared decision-making Emphasize quality over quantity
Develop coordinated information systems
Ensure staff are trained to implement the OMM
Reduce rates of revocation for technical & drug violations, while increasing accountability & community safety
Increase efficiency & improve client outcomes

Philosophy & Principles
Processes & Policies & Protocols
Programs
Philosophy & Principles
Processes & Policies & Protocols
Programs
Developing & Maintaining an Integrated Approach

ELEMENTS OF SUCCESSFUL COLLABORATION
•Convergence of needs
•Commitment - mutual respect, understanding & trust
•Vision - shared mission; shared objectives & strategies
•Willingness to re-think policies/procedures
•Communication - communicate w/ & involve staff
•Resources - commitment of financial & human
•Regular meetings w/ diverse participation resulting in decisions (all key systems & the right people)
•Clearly defined roles & responsibilities
•Information & a common language
•On-going oversight w/ regular feedback to an advisory group
•Formal Service Agreements - protocols & MOUs
•Formalized system for conflict resolution

CHALLENGES TO SUCCESSFUL
COLLABORATION
CHALLENGES TO SUCCESSFUL
COLLABORATION• Separate Systems with Seemingly Disparate Goals
• Competitive Markets
• Lack of/Limited Communication
• Duplicative Services
• Revolving Door Treatment & Correctional Systems
• Inadequate Funding
• Limited Number of Service Providers
• Limited Service Capacity, including Limited Effective Services in practice
• Restricted Availability of certain Levels of Care & over abundance of other Levels of Care
• Limited Specialized Services
• Insufficient Aftercare & Transition Services
• Separate Systems with Seemingly Disparate Goals
• Competitive Markets
• Lack of/Limited Communication
• Duplicative Services
• Revolving Door Treatment & Correctional Systems
• Inadequate Funding
• Limited Number of Service Providers
• Limited Service Capacity, including Limited Effective Services in practice
• Restricted Availability of certain Levels of Care & over abundance of other Levels of Care
• Limited Specialized Services
• Insufficient Aftercare & Transition Services

The Bottom LineThe Bottom Line
• What do you want?
• What do your partners want?
• Identify resources to be shared
• Establish regular venues for communication & problem-solving
• What do you want?
• What do your partners want?
• Identify resources to be shared
• Establish regular venues for communication & problem-solving
A program model & methodology that bridges two separate systems: justice & treatment.
The justice system’s legal sanctions reflect community concerns for public safety, while treatment emphasizes therapeutic relationships as a means for changing behavior.
What is TASC?

TASC Core ServicesTASC Core Services
Screening & Clinical Assessment
Service Determination & Referral
Care Planning, Coordination & Management
Reporting to Justice System
Screening & Clinical Assessment
Service Determination & Referral
Care Planning, Coordination & Management
Reporting to Justice System

TASC Care Management ModelTASC Care Management Model
Comprehensive Clinical AssessmentComprehensive Clinical Assessment
Strategic Individualized Case PlanningStrategic Individualized Case Planning
TreatmentReferral
TreatmentReferral
OtherServices
OtherServices
OtherServices
OtherServices
MonitoringMonitoring
Reporting to Referral SourceReporting to Referral Source

TASC Person-Centered Client Flow
TASC Person-Centered Client Flow
Client Identification
TASCEligibility Determination
Service Screening
No Services NeededServices Refused
Non-TASC Services Needed
Low-Risk, Low-Need Client
Client referred out
Referral to interventionReferral to other services
TASC reporting
High-RiskHigh-Need
ClientAssessment
PersonCentered Planning
Referral toServices
TASC Care Management
Reporting,Monitoring

TASC Key ConceptsTASC Key Concepts• Facilitates communication between systems
• Based on clinical & support needs, not only medical necessity
• Develops & maintains linkages with a variety of community resources
• Incorporates justice system language & goals
• Balances control & treatment
• Active relationships - client, probation, treatment, community services
• Utilizes the influence of legal sanctions to engage & retain offenders in treatment
• Positive outcome-oriented for clients, as well as treatment & justice systems
• Facilitates communication between systems
• Based on clinical & support needs, not only medical necessity
• Develops & maintains linkages with a variety of community resources
• Incorporates justice system language & goals
• Balances control & treatment
• Active relationships - client, probation, treatment, community services
• Utilizes the influence of legal sanctions to engage & retain offenders in treatment
• Positive outcome-oriented for clients, as well as treatment & justice systems

TASC NationallyTASC Nationally
• 1962 - Robinson v. California - addiction is an illness, not a crime
• 1970s - Federal government develops model to interrupt drug-crime cycle - Treatment Alternatives to Street Crime
• 1972 - first TASC program in Wilmington, Delaware
• 2000 - Over 150 individual TASC programs in 32 states
• 1962 - Robinson v. California - addiction is an illness, not a crime
• 1970s - Federal government develops model to interrupt drug-crime cycle - Treatment Alternatives to Street Crime
• 1972 - first TASC program in Wilmington, Delaware
• 2000 - Over 150 individual TASC programs in 32 states

National TASC Critical Elements
National TASC Critical Elements
1) Process to coordinate justice, treatment & other systems
2) Procedures for providing information & cross-training to justice, treatment & other systems
1) Process to coordinate justice, treatment & other systems
2) Procedures for providing information & cross-training to justice, treatment & other systems
System Coordination Elements

Organizational ElementsOrganizational Elements
3 & 4) Broad bases of support from justice & treatment systems, with institutionalized systems for effective communication
5) Organizational integrity
6) Policies & procedures for regular staff training
7) MIS with a program evaluation design
3 & 4) Broad bases of support from justice & treatment systems, with institutionalized systems for effective communication
5) Organizational integrity
6) Policies & procedures for regular staff training
7) MIS with a program evaluation design
Operational ElementsOperational Elements
8) Clearly defined client eligibility
9) Client-centered case management
10) Screening procedures to identify justice system candidates
11) Assessment & referral procedures
12) Policies & procedures for monitoring drug & alcohol use through testing
13) Competency with diverse populations
8) Clearly defined client eligibility
9) Client-centered case management
10) Screening procedures to identify justice system candidates
11) Assessment & referral procedures
12) Policies & procedures for monitoring drug & alcohol use through testing
13) Competency with diverse populations

For more information about TASC nationally, visit the National TASC website at
For more information about TASC nationally, visit the National TASC website at
www.nationaltasc.org

In NC, TASC is administered by the Division of Mental Health, Developmental Disabilities & Substance Abuse Services, through private NPOs & public MH Centers.
NC TASC effectively & efficiently links treatment & justice goals of reduced drug use & criminal activity through processes that increase treatment access, engagement & retention.

TASC in North CarolinaTASC in North Carolina
1978 - First TASC Programs in NC
1993 - 10 Programs in 20 Counties
1994 - Enhanced TASC (SSA)
1998 - 23 Programs in 43 Counties
2002 - TASC services available in all 100 counties
2003 - TASC Training Institute
1978 - First TASC Programs in NC
1993 - 10 Programs in 20 Counties
1994 - Enhanced TASC (SSA)
1998 - 23 Programs in 43 Counties
2002 - TASC services available in all 100 counties
2003 - TASC Training Institute

Goal for NC TASC Goal for NC TASC
Equitable statewide access to a standard of TASC
services in the most cost-effective, timely &
organizationally efficient manner, consistent with the
unified court & statewide probation systems

NC TASC TasksNC TASC Tasks
• Developed standard clinical care management procedures (TASC SOP) w/ TASC staff
• Improved current aggregate data collection & analysis
• Developed financing plan, based on I Punishment offender pop
• Proposed regional management structure & statewide expansion plan
• Issued RFA
• Developed standard clinical care management procedures (TASC SOP) w/ TASC staff
• Improved current aggregate data collection & analysis
• Developed financing plan, based on I Punishment offender pop
• Proposed regional management structure & statewide expansion plan
• Issued RFA

NC TASC TasksNC TASC Tasks• Developed performance measures:
process & outcome
• Awarded 4 grants for infrastructure development & expansion
• Identified training needs & contracted for NC TASC Training Institute
• Implemented NC-TOPPS/TASC CJM - Performance Measures project
• Developing NTASC Critical Elements audit protocols
• Developing statewide MIS
• Developed performance measures: process & outcome
• Awarded 4 grants for infrastructure development & expansion
• Identified training needs & contracted for NC TASC Training Institute
• Implemented NC-TOPPS/TASC CJM - Performance Measures project
• Developing NTASC Critical Elements audit protocols
• Developing statewide MIS
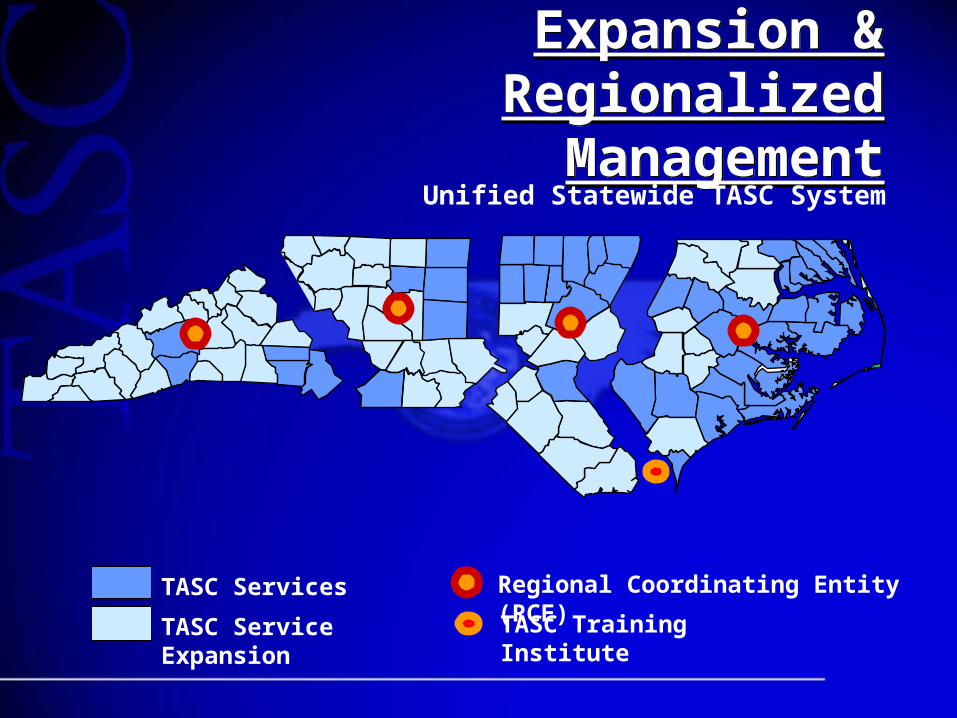
Expansion & Regionalized Management
Expansion & Regionalized Management
TASC Services Regional Coordinating Entity (RCE)
TASC Service Expansion TASC Training Institute
Unified Statewide TASC System

Implementing Statewide Offender Care Management
Implementing Statewide Offender Care Management
• Committed, visionary leadership & identified key staff
• Build support with community leaders, legislators & stakeholders
• Design appropriate organizational structure & financing models
• Financing plan for development, implementation & continuation
• Committed, visionary leadership & identified key staff
• Build support with community leaders, legislators & stakeholders
• Design appropriate organizational structure & financing models
• Financing plan for development, implementation & continuation

NC TASC Training InstituteNC TASC Training Institute
The mission of the TASC Training The mission of the TASC Training Institute is to improve the quality of Institute is to improve the quality of services to the offender population services to the offender population
through workforce developmentthrough workforce development
•TASC Clinical Series
•TASC Continuing Education
•On-line training
•Drug Education Schools
•Staff Certification
The mission of the TASC Training The mission of the TASC Training Institute is to improve the quality of Institute is to improve the quality of services to the offender population services to the offender population
through workforce developmentthrough workforce development
•TASC Clinical Series
•TASC Continuing Education
•On-line training
•Drug Education Schools
•Staff Certification

How is this done?How is this done?
• 4 regional training coordinators & director review requests from the field to develop annual training plan
• The Institute negotiates contracts with contractors to develop curricula, deliver TOTs, trainings, etc.
• TASC Clinical Series is provided via TASC staff who’ve become TASC trainers
• 4 regional training coordinators & director review requests from the field to develop annual training plan
• The Institute negotiates contracts with contractors to develop curricula, deliver TOTs, trainings, etc.
• TASC Clinical Series is provided via TASC staff who’ve become TASC trainers

TASC Clinical SeriesTASC Clinical Series
32 hours training for new staff:
– Understanding TASC
– Confidentiality– HIV/BRI/Infectious Disease (on-line)
– Understanding Addiction
– Criminal Justice
– Clinical Skills - Care Planning & Management
32 hours training for new staff:
– Understanding TASC
– Confidentiality– HIV/BRI/Infectious Disease (on-line)
– Understanding Addiction
– Criminal Justice
– Clinical Skills - Care Planning & Management

TASC Continuing EducationTASC Continuing Education
• American Society of Addiction Medicine
• Motivational Interviewing & Enhancement
• Mental Health Screening
• Co-Occurring Disorders
• Effective Interventions for
TASC Clients
• The TASC Journey….
An Agency’s Response to Person
Centered Services
• American Society of Addiction Medicine
• Motivational Interviewing & Enhancement
• Mental Health Screening
• Co-Occurring Disorders
• Effective Interventions for
TASC Clients
• The TASC Journey….
An Agency’s Response to Person
Centered Services
• Training.nctasc.net
• Provides on-line courses of didactic materials prior to clinical series
• Research to Practice site
• Continuous communication with users & Center’s staff
• Training.nctasc.net
• Provides on-line courses of didactic materials prior to clinical series
• Research to Practice site
• Continuous communication with users & Center’s staff

Drug Education School
• Intervention for First-time Offenders
• 15 Hours of Standard Education
• One Time Opportunity for Expungement for persons under 21 years of age
• Self Supporting $150.00 Fee
• Statutory Authority: G.S. 90-96

Staff CertificationStaff Certification
Legislation to be introduced in 2005 legislative session to create
Certified Criminal Justice Addictions Credential
Legislation to be introduced in 2005 legislative session to create
Certified Criminal Justice Addictions Credential

TASC Training Institute FY04
•Delivered 4,199 hours of training to 315 TASC & 102 partner agency staff
•Provided 100 stipends for the NTASC conference hosted in Raleigh, NC
•Addt’l 2200+ hours were received thru NTASC Conference
All hours provided at no addt’l cost to participant or participant’s employing agency

NC TASC Training Institute Web Site
www.nctasc.net
Register for Classes
Read Important Announcements
View Your Total Training Hours

TASC Quality PointsTASC Quality Points
• Statewide Availability for Equity
• Regional Management for Economies of Scale
• TASC Training Institute
• TASC in MH Reform Legislation
• MH Commission promulgated TASC Rules
• NC TASC Standard Operating Procedures
• National TASC Critical Elements
• Local Memoranda of Agreement
• TASC CJM Performance Measures
• Funding contingent on DOC-DHHS MOU compliance
• Statewide Availability for Equity
• Regional Management for Economies of Scale
• TASC Training Institute
• TASC in MH Reform Legislation
• MH Commission promulgated TASC Rules
• NC TASC Standard Operating Procedures
• National TASC Critical Elements
• Local Memoranda of Agreement
• TASC CJM Performance Measures
• Funding contingent on DOC-DHHS MOU compliance

FY04 TASC Statistics FY04 TASC Statistics
• Offenders served: 9845 (53% increase from FY99)
• 70% Less than 36 years old (43% less than 26)
• 83% Not married
• 55% Did not complete high school
• 34% Unemployed at admit (24% in FY01)
• Primary Substance Used
•Marijuana 44% •Alcohol 28% •Cocaine 19%
• Length of Stay
•0-3 months 24% •4-6 months 35%
•7-12 months 31% •More than 1 year 10%
• Offenders served: 9845 (53% increase from FY99)
• 70% Less than 36 years old (43% less than 26)
• 83% Not married
• 55% Did not complete high school
• 34% Unemployed at admit (24% in FY01)
• Primary Substance Used
•Marijuana 44% •Alcohol 28% •Cocaine 19%
• Length of Stay
•0-3 months 24% •4-6 months 35%
•7-12 months 31% •More than 1 year 10%

TASC Costs & Benefits
TASC Costs & Benefits
• $1.79 per TASC client per day
• FY96-97 sample TASC client pop*:–85.9% had at least one previous
arrests (mean # 2.6)
–61.3% were NOT re-arrested within 2 years
* NC Sentencing & Policy Advisory Commission - Submitted to the 2000 Session of the North Carolina General Assembly
• $1.79 per TASC client per day
• FY96-97 sample TASC client pop*:–85.9% had at least one previous
arrests (mean # 2.6)
–61.3% were NOT re-arrested within 2 years
* NC Sentencing & Policy Advisory Commission - Submitted to the 2000 Session of the North Carolina General Assembly

DMHDDSAS ReorganizationDMHDDSAS Reorganization
Community Policy Management Section•MH, DD & SA public policy leadership & oversight
•collaboration w/ a wide base of customers, public & private partners
Community Policy Management Section•MH, DD & SA public policy leadership & oversight
•collaboration w/ a wide base of customers, public & private partners
•Single State Agency for Substance Abuse
•Office of Employee Assistance Programs
•State Methadone Authority
•Quality Management
•Best Practice & Community Innovations
•Local Management Entity Systems Performance
•Justice System Innovations
•Prevention & Early Intervention

Justice Systems Innovations Team, Community Policy Management Section
Justice Systems Innovations Team, Community Policy Management Section
•Policy re: adults & children with mental health, developmental disabilities & substance abuse problems involved in criminal & juvenile justice systems
•Multi-system coordination with state, county & local law enforcement, institutional & community corrections
•Best practices, promising approaches & innovations related to supports, services & treatments for individuals & improved
systems performance
•Policy re: adults & children with mental health, developmental disabilities & substance abuse problems involved in criminal & juvenile justice systems
•Multi-system coordination with state, county & local law enforcement, institutional & community corrections
•Best practices, promising approaches & innovations related to supports, services & treatments for individuals & improved
systems performance

Justice Systems InnovationsFor Adults:
TASC develops & manages comprehensive protocols for offender management, according to DHHS-DOC MOU Implementation of OMM, in partnership with DCC &
other stakeholders Implementation of “Going Home” initiative, according to
DOC, DHHS, Department of Commerce & NC Community College System MOU
Treatment & case management for Drug Treatment Courts, in cooperation with AOC & DCC
Review & programming for DOC residential substance abuse programs & mental health services
Protocols for DWI Drug Education School (GS90-96) diversion alternative Jail-based & police partnership diversion programs
For Adults: TASC develops & manages comprehensive protocols for
offender management, according to DHHS-DOC MOU Implementation of OMM, in partnership with DCC &
other stakeholders Implementation of “Going Home” initiative, according to
DOC, DHHS, Department of Commerce & NC Community College System MOU
Treatment & case management for Drug Treatment Courts, in cooperation with AOC & DCC
Review & programming for DOC residential substance abuse programs & mental health services
Protocols for DWI Drug Education School (GS90-96) diversion alternative Jail-based & police partnership diversion programs

Justice Systems InnovationsJustice Systems Innovations
For Children and Families:
•Coordination with DJJDP for a continuum of services & care
RWJF Resources for Recovery & Co-occurring Academy projectsEvidence-based treatment in DJJDP Detention Centers & Youth Development CentersEvidence-based protocols utilized in MAJORS program for juvenile offenders with substance abuse disorders
Evidence-based protocols for treatment & case management of individuals in juvenile courts, Youth & Family Treatment Court
For Children and Families:
•Coordination with DJJDP for a continuum of services & care
RWJF Resources for Recovery & Co-occurring Academy projectsEvidence-based treatment in DJJDP Detention Centers & Youth Development CentersEvidence-based protocols utilized in MAJORS program for juvenile offenders with substance abuse disorders
Evidence-based protocols for treatment & case management of individuals in juvenile courts, Youth & Family Treatment Court

MHDDSA Reform established...
MHDDSA Reform established...
DSM criteria for a substance-related disorder; and
Services approved by a TASC care manager; and
Voluntary consent to participate; and
Status as an Intermediate Punishment offender, a Department of Correction releasee who has completed an in-prison treatment program, or a Community Punishment violator at-risk for revocation
DSM criteria for a substance-related disorder; and
Services approved by a TASC care manager; and
Voluntary consent to participate; and
Status as an Intermediate Punishment offender, a Department of Correction releasee who has completed an in-prison treatment program, or a Community Punishment violator at-risk for revocation
Adult Substance Abusing Criminal Justice Offender Target Population to ensure access to treatment for individuals with a SA diagnosis who present the greatest risk to public safety.
Eligibility includes:

COMMUNITY CORRECTIONS: SOFT ON CRIME?
ABSOLUTELY NOT!The Strategy Must:
Balance the public’s expectation for protection, control & accountability with resources necessary to control & treat high-risk/high-need offenders
Strive for a balance between Control & Treatment based on offender risk & needs
•Manage risks by supervisory control•Manage needs through treatment collaboration
Prioritize resources based on offender risk & needs
Build partnerships with law enforcement, treatment
providers, schools, victims & the public

Effectiveness & Efficiency of Community Corrections ACTIVE
44% Recidivism$63.00 Per Day21% Population
32% Recidivism $10.00 Per Day 24% Population
INTERMEDIATE PUNISHMENTS (Highest Risk Supervision)
24% Recidivism $2.00 Per Day 42% Population
COMMUNITY PUNISHMENTS(Traditional Probation/Parole Supervision)
Crime & Punishment
U.S. prison, parole population sets record One in 32 Americans in jail or on parole in 2003
The Associated PressJuly 26, 2004WASHINGTON - A record 6.9 million adults were incarcerated or on probation or parole last year, nearly 131,000 more than in 2002, according to a Justice Department study.
Put another way, about 3.2 percent of the adult U.S. population, or 1 in 32 adults, were incarcerated or on probation or parole at the end of last year.

Why is Community Corrections Vital to the Criminal Justice
System? GOOD PUBLIC POLICY
PUBLIC SAFETY
PUBLIC HEALTH
SOUND ECONOMICS
THE RIGHT THING TO DO
Regardless of sentencing practices or laws, less than 1% of all incarcerated offenders will remain there for life.
Front end control & rational planning prior to release are essential for the 99% that remain in or return to our communities.

Why is TASC Care Management Vital to Community Corrections &
Treatment?
Why is TASC Care Management Vital to Community Corrections &
Treatment?• Maintains clear roles & responsibilities
– Probation officers focus on supervision & tx providers focus on client care
– TASC actively supports & integrates both, providing a framework & structure for managing CJ clients
• Engages clients at all points in CJ system
• Improves communication among systems re: & with client
• Advocates for & assists client in navigating multiple complex systems
• Maintains clear roles & responsibilities– Probation officers focus on supervision & tx
providers focus on client care
– TASC actively supports & integrates both, providing a framework & structure for managing CJ clients
• Engages clients at all points in CJ system
• Improves communication among systems re: & with client
• Advocates for & assists client in navigating multiple complex systems

• Appropriately manages client confidentiality rules & law
• Broadens range of sanctions available to CJ system & supports a system of graduated sanctions
• Offers tx in lieu of or in combination with punishment
• Provides added information to CJ system
• Provides basis for judicial & correctional decision-making
• Appropriately manages client confidentiality rules & law
• Broadens range of sanctions available to CJ system & supports a system of graduated sanctions
• Offers tx in lieu of or in combination with punishment
• Provides added information to CJ system
• Provides basis for judicial & correctional decision-making

• Extends power of the court to influence drug-using behaviors
• Reduces technical & drug violations
– improving probation recidivism rates & positive impact on prison pop
• Improves treatment outreach & access
• Provides independent assessments & makes appropriate referrals
• Improves treatment engagement
– orients clients to tx, reduces “no shows”, increases tx staff productivity
• Extends power of the court to influence drug-using behaviors
• Reduces technical & drug violations
– improving probation recidivism rates & positive impact on prison pop
• Improves treatment outreach & access
• Provides independent assessments & makes appropriate referrals
• Improves treatment engagement
– orients clients to tx, reduces “no shows”, increases tx staff productivity
• Improves treatment retention & supports tx compliance
– improving tx outcomes
• Provides support & continuity during CJ & tx transitions
• Facilitates access to addt’l services
• Compensates for service availability
• Utilizes resources more effectively
• Arranges goals & objectives of CJ, tx & the client
• Improves treatment retention & supports tx compliance
– improving tx outcomes
• Provides support & continuity during CJ & tx transitions
• Facilitates access to addt’l services
• Compensates for service availability
• Utilizes resources more effectively
• Arranges goals & objectives of CJ, tx & the client

TASC … a Task IndeedTASC … a Task IndeedDamn, why am I here, I know I’m not an addict, Yeah, I smoke a little weed, but it’s just a small habit;I’m not alcoholic, I drink to ease the pain, So what I popped a few pills, snorted lines of cocaine;Hell no I’m not addicted, I could stop if I want, But I don’t right now, I’m having too much fun;They say I have a disease, I only use because I choose,Drugs are harmless, what’s wrong with a blunt and a few booze;Yeah I stole from a few people, but they had enough to share,I knew that it was wrong, but drugs helped me not to care;I feel a lot more stable being clean now but I don’t like it much,I keep thinking about the past things I’ve done and people I’ve wrongly touched;On the other hand, I’m relieved I can finally love again, I can see much more clearly, I found who are my real friends;I’ve regained trust from my family, they’re no longer ashamed, Telling people I’ve changed, before they wouldn’t mention my name;Matter of fact I like being drug free, I feel like I’m really alive, And I owe all to God and Treatment Alternatives to Street Crime.
- Cumberland County, NC TASC Client
Damn, why am I here, I know I’m not an addict, Yeah, I smoke a little weed, but it’s just a small habit;I’m not alcoholic, I drink to ease the pain, So what I popped a few pills, snorted lines of cocaine;Hell no I’m not addicted, I could stop if I want, But I don’t right now, I’m having too much fun;They say I have a disease, I only use because I choose,Drugs are harmless, what’s wrong with a blunt and a few booze;Yeah I stole from a few people, but they had enough to share,I knew that it was wrong, but drugs helped me not to care;I feel a lot more stable being clean now but I don’t like it much,I keep thinking about the past things I’ve done and people I’ve wrongly touched;On the other hand, I’m relieved I can finally love again, I can see much more clearly, I found who are my real friends;I’ve regained trust from my family, they’re no longer ashamed, Telling people I’ve changed, before they wouldn’t mention my name;Matter of fact I like being drug free, I feel like I’m really alive, And I owe all to God and Treatment Alternatives to Street Crime.
- Cumberland County, NC TASC Client