suicide attempts and ideation among adults in addis ababa, ethiopia
TRANSCRIPT

Suicide attempts and ideation among adults in Addis Ababa, Ethiopia
Kebede D, Alem A. Suicide attempts and ideation among adults in Addis Ababa, Ethiopia. Acta Psychiatrica Scand 1999: 100: 35-39. 0 Munksgaard 1999
Attempted suicide is one of the major risk factors for completed suicide, is associated with psychiatric disorders, and is also a potentially fatal event. We describe here a study of suicide attempts and ideation in a representative sample of 10203 adults in Addis Ababa.The study was conducted between January and March 1994. The prevalence of current suicidal ideation was 2.7%). Lifetime prevalence of suicidal attempt was 0.9'%1. Most of the attempts (66%)) occurred when subjects were under 25 years of age. Hanging was the preferred method for men and poisonings for women. There were no significant associations between suicide attempt and sex, ethnicity or religion. Current suicidal ideation was more common in men than women, odds ratio (95% confidence interval), OR (95% CI): 0.67 (0.48, 0.93). There was a statistically significant trend of decreasing risk of ideation with increasing age and educational attainment. There was a 68% decrease in the risk of ideation in the 60 years of age and above group compared to the 15-24 year group: OR (95% CI): 0.32 (0.16, 0.62). Marital status, ethnicity, and religion were not associated with suicidal ideation.
Introduction
Suicide is a major cause of mortality among adults worldwide. For youth it is ranked among the top three causes of death (1).
Attempted suicide, on the other hand, is one of the major risk factors for completed suicide, with up to one in five attempters eventually dying by suicide (2). Attempted suicide is also associated with psychiatric disorders. A diagnosis of depression, for example, is made in 35-79% of cases of attempted suicide (3). Furthermore, attempted suicide is also a potentially fatal event.
Community-based estimates of prevalence of suicide attempts are not commonly reported from Africa. Studies of outpatients in Nigeria and Egypt have reported prevalence for suicide attempts of 7.0 and 38.5 per 100000, respectively (4, 5).
Jacobson (6), based on a study of a general hospital population in rural western Ethiopia between 1966 and 1972, estimated the incidence rate of attempted suicide to be 4.5 per 100000 per year. Another study, based on a representative sample of senior high school students in Addis
D. Kebede', A. Alem2 'Department of Community Health, Faculty of Medicine, University of Addis Ababa, and 'Amanuel Psychiatric Hospital, Addis Ababa, Ethiopia
Key words suicide attempt, prevalence, Ethiopia
Derege Kebede. Department of Community Health, Faculty of Medicine, Addis Ababa University. P 0 Box 1176, Addis Ababa. Ethiopia
Ababa, reported a prevalence of 14.3'%, (7). A 6-year retrospective review of organophosphate insecticide poisoning at a teaching hospital in Addis Ababa has shown that 47 of the 50 cases of poisoning were attempted suicides (8). These studies have shown that hanging in the rural setting and poisoning in the urban setting are the preferred methods employed by attempters.
These studies are indicative of the importance of suicide attempts and the usual methods employed. However, they are of limited significance for two reasons. First, studies based on hospital utilization data in Ethiopia are of limited usefulness because of the limited access of the majority of the population to hospitals. Second, the community-based study from Addis Ababa, although based on a represen- tative sample, was limited to adolescents and was based on a relatively small sample size.
Community-based surveys based on large sam- ples are required if appropriate policies and intervention strategies are to be instituted to tackle this public health problem. We report here on a survey of over 10000 adults in Addis Ababa
35

Kebede and Alem
that measured the prevalence of suicide ideation and attempts, methods employed, and socio-demo- graphic factors associated with ideation and attempt.
Material and methods
The study was conducted in Addis Ababa between January and March 1994. We used as the source population an administrative division of the city proper that included 25 districts (woredas) and 284 sub-districts (keheles) . Using estimates and projec- tions based on an earlier census, the city had a population of 2228490 (9).
Sample selection
A questionnaire on suicide attempt was adminis- tered in conjunction with the Self Reporting Questionnaire (SRQ) for screening mental ill- nesses. The details of the methods followed have been reported elsewhere (10). Briefly, the study population of 10 203 was selected from the entire city by a cluster sampling method proportionate to size (1 1).
We employed trained and supervised interviewers to collect data. Selected households were asked for their consent to participate. The rate of non- response was less than 5% for the survey. In cases of non-participation the next household (using established municipal house numbers) was selected using the +1, +2, -1, -2 scheme, in that order. Where selected individuals were not immediately available for interview a maximum of three visits to that household was made for the interview. After three unsuccessful attempts that person was classified as a non-respondent.
A 4-item questionnaire was employed to collect data on suicide attempt. The following 4 questions were included: 1. Have you ever attempted to kill yourself? 2. If yes, how many times? 3. How old were you when you attempted? 4. What methods did you use? Another question which was a component of the SRQ was also included to evaluate for suicidal ideation: Has the thought of ending your life been in your mind?
A 20-item Amharic SRQ, that was used in earlier mental health surveys in Addis Ababa (12), was used to collect data on other mental illnesses. Additional items for collecting socio-demographic data were also included in the questionnaire. The questionnaire was pretested in a community sample that was similar to, but outside of, sampled sub-districts.
Data analysis
We used the EPI-INFO version 5 program (CDC, Atlanta GA) for data entry and preliminary analysis. The Statistical Analysis System program, version 6.04 (SAS Institute, Cary NC), was used for both bivariate and multivariate analysis.
The logistic regression method was employed to adjust relative risks for potential confounding variables. In this manner, suicide attempt was included in the logistic model as a dependent variable. The following factors were included in the model as dependent variables: sex, ethnicity ( 5 levels), and religion ( 5 levels). To evaluate associa- tions with suicidal ideation the following factors were included in the model: sex, age (4 levels), education (4 levels), employment (2 levels), ethnicity ( 5 levels), and religion ( 5 levels). Test for trend was obtained from a logistic regression model with the adjusted relative risk estimates included as a continuous variable
Results
The study population consisted of 10203 indivi- duals. Of these, 45.1% were men. Adolescents (15-24 years of age) made up 44.9% of the population, 35.3% were adults, 13.1% were middle aged, and 6.6% were elderly. Most had some form of formal education (88%) although only 7.3% had post-secondary education. Only 35% were employed. The majority were from the Amhara ethnic group (52.1%), were Orthodox Christians (87.70/0), and had never been married (55.4). A positive history of mental illness in the family was given by 4.4%.
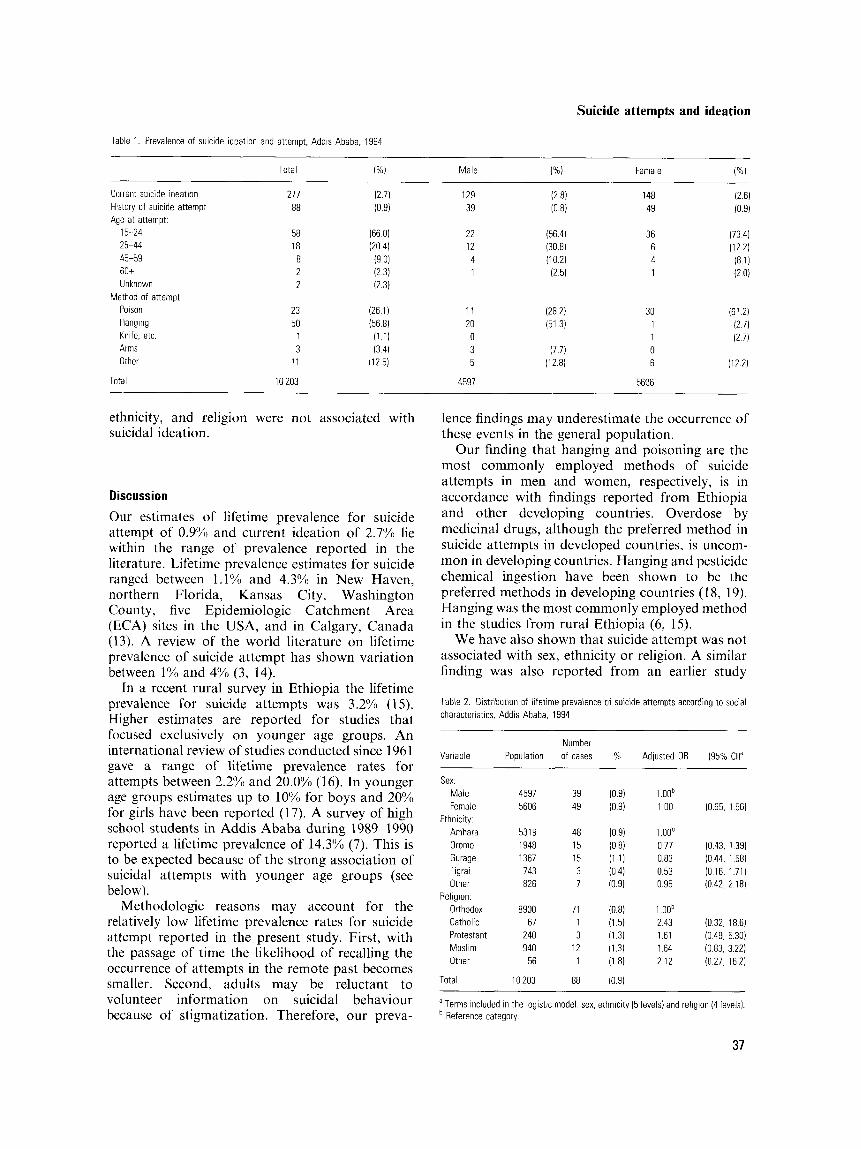
The prevalence of current suicidal ideations was similar for both sexes (Table 1). Lifetime and prevalence of suicide attempts were also similar for both sexes. Most of the attempts occurred when the subjects were under 25 years of age, and hanging was the preferred method for men and poisoning for women.
In the multivariate analysis there were no significant associations between suicide attempt and sex, ethnicity, or religion (Table 2). The risk of suicide attempt was not evaluated in terms of age, educational attainment, work, or marital status. This is because of the difficulty of ascertaining the status of these factors before the occurrence of the attempt.
On the other hand, suicidal ideation, was associated with the female sex, younger age groups, and lower educational level (Table 3). The risk of ideation decreased with increasing age and educational attainment. In both cases the trend was statistically significant. Family size, marital status,
36
Suicide attempts and ideation
Table 1 Prevalence of suicide ideation and attempt, Addis Ababa, 1994
Total
Current suicide ideation History of suicide attempt Age at attempt
15-24 25-44 45-59 60+ Unknown
Poison Hanging Knife. etc Arms Other
Method of attempt
271 88
58 18
8 2 2
23 50
1 3
11
129 39
22 12 4 1
11 20 0 3 5
148 49
36 6 4 1
30 1 1 0 6
Total 10 203 4591 5606
ethnicity, and religion were not associated with suicidal ideation.
Discussion
Our estimates of lifetime prevalence for suicide attempt of 0.9% and current ideation of 2.7% lie within the range of prevalence reported in the literature. Lifetime prevalence estimates for suicide ranged between 1.1% and 4.3Yn in New Haven, northern Florida, Kansas City, Washington County, five Epidemiologic Catchment Area (ECA) sites in the USA, and in Calgary, Canada (13). A review of the world literature on lifetime prevalence of suicide attempt has shown variation between 1% and 4% (3, 14).
In a recent rural survey in Ethiopia the lifetime prevalence for suicide attempts was 3.2% (15). Higher estimates are reported for studies that focused exclusively on younger age groups. An international review of studies conducted since 1961 gave a range of lifetime prevalence rates for attempts between 2.2% and 20.0% (1 6). In younger age groups estimates up to 10% for boys and 20% for girls have been reported (1 7). A survey of high school students in Addis Ababa during 1989-1990 reported a lifetime prevalence of 14.3% (7). This is to be expected because of the strong association of suicidal attempts with younger age groups (see below).
Methodologic reasons may account for the relatively low lifetime prevalence rates for suicide attempt reported in the present study. First, with the passage of time the likelihood of recalling the occurrence of attempts in the remote past becomes smaller. Second, adults may be reluctant to volunteer information on suicidal behaviour because of stigmatization. Therefore, our preva-
lence findings may underestimate the occurrence of these events in the general population.
Our finding that hanging and poisoning are the most commonly employed methods of suicide attempts in men and women, respectively, is in accordance with findings reported from Ethiopia and other developing countries. Overdose by medicinal drugs, although the preferred method in suicide attempts in developed countries, is uncom- mon in developing countries. Hanging and pesticide chemical ingestion have been shown to be the preferred methods in developing countries (1 8, 19). Hanging was the most commonly employed method in the studies from rural Ethiopia (6, 15).
We have also shown that suicide attempt was not associated with sex, ethnicity or religion. A similar finding was also reported from an earlier study
Table 2. Distribution of lifetime prevalence of suicide attempts according to social characteristics. Addis Ababa, 1994
Number Variable Population of cases % Adjusted OR (95% CI)”
Sex: Male 4597 39 (0.9) L O O b Female 5606 49 (0.9) 1 0 0 (0.65. 1 56)
Amhara 5319 48 (09) 1 OOb Oromo 1948 15 (0.8) 0 77 (0.43. 139) Gurage 1367 15 (1 1) 0.83 (0.44, 1 58) Tigrai 743 3 (0.4) 0.53 (0 16. 1.71) Other 826 7 (0 91 0 95 (0.42, 2 18)
Orthodox 8900 71 (0.8) 1 OOb Catholic 67 1 (1 51 2 43 (032, 186) Protestant 240 3 (1.3) 1.61 (0 49, 5.30) Muslim 940 12 (1.3) 1 64 (0.83, 3.22) Other 56 1 (1 8) 2 12 (0.27. 16 2)
Ethnicity:
Religion.
Total 10 203 88 (0.9)
a Terms included in the logistic model sex. ethnicity (5 levels) and religion (4 levels). Reference category
37

Kebede and Alem
Table 3 Distribution of prevalence of suicide ideation according to individual characteristics, Addis Ababa, 1994
Number P for Variable Population of cases % OR (95% Cl)a trendb
Sex Male Female
15-24 25-44 45-59 60+
Education No schooling Elementary Secondary Above
Work status Unemployed Empioyed
Marital status Married Single Divorced Separated Widowed
Ethnicity Amhara Oromo Gurage Tigrai Other
Religion Orthodox Catholic Protestant Muslim Other
Age
Total
4597 5606
4586 3603 1336 678
1216 2648 5592 747
7341 2862
3425 5654 287 253 584
531 9 1948 1367 743 826
8900 67
240 940
56
10.203
1 :'9 148
107 108 41 21
48 83
132 14
208 69
134 108
8 10 17
147 53 47 13 17
239 2 8
27 1
277
(2 8) 1 ooc (26) 067 (048 093)
(2 3) 100' 0 03 (3 0) 0 67 (045 0 99) (31) 044 (029 .065) (31) 032 ( 0 1 6 0 6 2 )
(3 9) 1 ooc 0 0006 (31) 097 ( 0 6 4 1 4 7 ) (24) 0 7 2 (045. 1 14) (1 9) 077 (0 37. 160)
(2 8) 1 00' (2 4) 0 84 (0 60. 1 191
(24) 1 00' (3 2) 084 (0 55 1 26) (2 8) 084 (038, 184) (3 9) 092 (044. 190) (29) 065 (036 .116)
(28) 1 ooc (27) 0 91 (064, 1 31) (34) 102 (068. 1 52) (1 8) 083 (044 153) (2 1 ) 0 81 (0 46, 1 45)
(2 7) 1 00' ( 3 0 ) 091 (0 16, 5 17) (3 3) 2 02 (0 88. 463) (2 9) 0 74 (045 123) (18) 070 (008 ,612)
(2 7 )
Terms included in the logistic model- sex, age (4 levels), marital status (5 levels). ethnicity (5 levels). education (4 levels). and employment (2 levels) Test for trend was obtained from a regression model with the adjusted relative risk estimates included as a continuous variable Reference category
among adolescents in Addis Ababa (7). In many other studies women were shown to have a higher risk for suicide attempt (16, 17). This female preponderance was also reported from rural Ethiopia (15). Gender roles vary across cultures and this may be an explanation for our finding and for other reports from Ethiopia.
On the other hand, our finding of similar risk between the sexes may reflect the influence of methodologic factors. Suicidal behaviour may be more stigmatizing to women than to men because of its potential effect on marital status. Therefore, women may not volunteer the information and, as a result, this may lead to a systematic underestima- tion of female rates. We have earlier reported that mood disorders occurred more frequently in women than in men in this general population (20). It is
logical to expect more suicide attempts in women because mood disorders are important predictors of suicidal behaviour (3). Therefore, our finding of similar lifetime prevalence rates for suicide attempts in men and women may be due to methodologic factors.
Ethnic and racial variations in the occurrence of suicide attempts have also been reported elsewhere (21, 22). Our results also indicate some degree of association between ethnicity and suicide attempts. However, because of the small number of cases, statistical significance was not achieved. Likewise, there seems to be some association between religion, and suicide attempts, but, again, this did not achieve statistical significance. We have not eval- uated the association with other variables because it was difficult to ascertain the presence of these variables before the occurrence of the attempt.
The prevalence for current suicidal ideation is 2.7%. This estimate is within the range reported elsewhere. One-year prevalence rates for suicidal ideation ranged from 2.3% to 3.9% in studies conducted in New Haven, northern Florida, five ECA sites, and Calgary, Canada. However, in two areas (Kansas City and Washington County), one- month prevalence estimates were 5.4% and 9.60/0, respectively (1 3).
We have also shown that suicide ideation was associated with the female sex, younger age groups, and lower educational level. These findings are in accordance with reports from other studies reviewed by Roy (3) and Diekstra and Garnefski (16).
In conclusion, our study shows suicide attempts and suicidal ideation as important public health problems. It is important that appropriate policy and strategic guidelines are worked out to address them.
Acknowledgements Financial assistance for the study was obtained from IDRC through the McGill-Ethiopia Community Health Project. Additional financial assistance was also obtained from the Swedish Medical Research Council through the Department of Psychiatry, University of UmeB. Material assistance from the Department of Community Health, Addis Ababa University is also acknowledged.
We would like to thank Professors R. Giel, L. Jacobsson and G. Kullgren, for their advice, and Drs. Barbara Singleton and Robert Kohn for their comments on an earlier draft of this manuscript.
We also thank all study workers and all those study participants who kindly agreed to be interviewed.
References I . DESJARLAIS R, EISENBERG L, GOOD B, KLEINMAN A. World
mental health: Problems and properties in low-income countries. Oxford: Oxford University Press, 1995.
38

Suicide attempts and ideation
2. BLUMENTHAL SJ. A guide to risk factors, assessment and treatment of suicidal patients. Med CIin North Am 1988: 72: 937-971.
3. ROY A. Suicide. In: KAPLAN HI, SADOCK BJ, eds. Comprehensive textbook of psychiatryNI. Baltimore: Williams and Wilkins, 1995: 1739-1752.
4. EFERAKEYA AE. Drugs and suicide attempts in Benin city, Nigeria. Br J Psychiatry 1984: 145: 70-73.
5. OKASH A, LOTAIF F. Attempted suicide: an Egyptian investigation. Acta Psychiatr Scand 1979: 60: 69-75.
6. JACOBSSON L. Suicide and attempted suicide in a general hospital in western Ethiopia. Acta Psychiatr Scand 1985: 71: 596-600.
7. KEREDE D, KETSELA T. Suicide attempts in Ethiopian high school adolescents. Ethiop Med J 1993: 31: 83-90.
8. ARERE M. Organophosphate pesticicde poisoning in 50 Ethiopian patients. Ethiop Med J 1991: 29: 109-1 18.
9. Population & Housing Census Commission. Population and Housing Census of Ethiopia 1984; Analytical report on results for Addis Ababa. Addis Ababa: 1987: 1.
10. KEREDE D, ALEM A, RASHID E. The prevalence and socio- demographic correlates of mental distress in Addis Ababa, Ethiopia. Acta Psychiatr Scand 1999: 1OO(Suppl): 5-10,
11. LEVY PS, LEMESHOW S. Sampling for health profes- sionals. Belmont: Lifetime Learning Publications, 1980: 250.
12. KORTMANN F. Problems in practising psychiatry in Ethiopia. Ethiop Med J 1988: 26: 77-83.
13. MOSCICKI EK. Epidemiologic surveys as tools for studying suicidal behaviour: a review. Suicide Life Threat Behav 1989: 19: 131-146.
14. MoscicKi EK. Epidemiology of suicidal behaviour. Suicide Life Threat Behav 1995: 25: 22-35.
15. ALEM A, KEBEDE D, KULLCREN G, JACOBSSON L, WOLDSEMAIAT G. Suicide attempts among adults in Butajira, Ethiopia. Acta Psychiatr Scand 1999: lOO(Supp1): 70-76.
16. DIEKSTRA RFW, GARNEFsKi N. On the nature, magnitude and causality of suicidal behaviours: an international perspective. Suicide Life Threat Behav 1995: 25: 36 -57.
17. MCNAMEE JE, O ~ ~ O R D DR. Prevention of suicide. Can Med Assoc J 1990: 142: 1223-1230.
18. ODEJIDE AO, WILLIAMS AO, OHAERI JU, IKUESAN BA. The epidemiology of deliberate self harm: the Ibadan experience. Br J Psychiatry 1986: 149: 734-737.
19. BERGER LR. Suicides and pesticides in Sri Lanka. Am J Public Health 1988: 78: 826-828.
20. KEREDE D, ALEM A. Major mental disorders in Addis Ababa, Ethiopia. 11. Affective disorders. Acta Psychiatr S a n d 1999: 1oo(suppl): 18-23.
21. MAUSOR SM, BEALS J, Dim RW, DUCLOS CTI. Risk factors for suicide among Indian adolescents at a boarding school. Public Health Reports 1989: 104: 609-6 14.
22. CDC. Attempted suicide among high school students - United States, 1990. MMWR CDC Surveil1 Summ 1991: 40: 633-634.
39