sumurr maternal and child health pilot
DESCRIPTION
In early 2011, the Ford Motor Company launched an innovative concept called Sustainable Urban Mobility with Uncompromised Rural Reach (SUMURR). To learn more, visit: http://business.gwu.edu/about-us/research/institute-for-corporate-responsibility/research-projects/TRANSCRIPT

A Report on the SUMURR Maternal and Child Health Pilot
A Partnership Between
Ford Motor Company
US Department of State and
George Washington University Institute for Corporate Responsibility
SUMURR Maternal & Child Health Pilot Final Project Review 2013

This report was prepared by the Institute for Corporate Responsibility at the George Washington University. The lead authors were Ridhima Kapur, Research Associate for University Sustainability Initiatives, Meghan Chapple-‐Brown, Director of the Office of Sustainability, Dr. John Forrer, Associate Director of the Institute for Corporate Responsibility. Research support was provided by Caitlin Curnyn, Nayantara Jacob, and Zohra Roy.
EXECUTIVE SUMMARY

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 ii
“We are also bringing the benefits of mobility and Internet cloud computing deep into the developing world. In 2012, Ford piloted the SUMURR (Sustainable Urban Mobility with Uncompromised Rural Reach) program in India, combining health applications on mobile phones and the off-‐road capabilities of a Ford Endeavour to extend the physical reach of maternal care to 3,100 people in 54 remote villages in a rural part of the country. SUMURR serves as a tangible demonstration of the synergy that can be achieved through our products, technology and partnerships to make a genuine difference in the lives of people around the globe.” -‐ William Clay Ford, Jr. Executive Chairman Ford Motor Company In early 2011, the Ford Motor Company launched an innovative concept called Sustainable Urban Mobility with Uncompromised Rural Reach (SUMURR). SUMURR seeks to examine how Ford could use its vehicles and its technology platforms to bridge the mobility gap for isolated, rural communities by providing them with sustainable access to key services such as healthcare, clean water, and education. Ford is not planning on entering any of these spaces, but rather is interested in exploring the commercial opportunities, both new and traditional that might arise from supporting these new markets.
The primary goal of SUMURR is to both gain intelligence on and shape the market by bridging the mobility gap for underserved rural populations. To achieve this goal, Ford identified three key project strategies: 1. Leverage Ford's vehicles and technology platforms by testing the technical capabilities of Ford’s innovative new OpenXC platform. 2. Engage global and local stakeholders by collaborating with partners on the implementation of the project. 3. Explore new market opportunities by conducting an analysis of local social and market needs. The Ford Motor Company, from its global headquarters, enlisted eight partner organizations globally to pilot the SUMURR concept and determine if it was viable. In 2012, the partners launched the SUMURR Maternal and Child Health Pilot project in southern India, which ran for a duration of nine months from June 2012 – February 2013.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 iii
The pilot was a test of SUMURR’s ability to enhance the accessibility of quality healthcare for pregnant women and newborns in the isolated and underserved Kalrayan Hills community by mobilizing the community health workers using a Ford Endeavor, and augmenting their ability to access government health information systems via mobile applications. At the end of the implementation period, the SUMURR pilot reached almost half the total population of this region. Hand in Hand India, a local social entrepreneur was the implementing partner. The total project costs were estimated at $36,014, and funding was the provided by the Ford Fund The SUMURR project has the potential to illustrate how, when aligned and integrated, technological innovation and social sustainability can help Ford explore new market opportunities. There is a world of social and market needs, and global and local stakeholders. Each area such as health, water or education can open up a new ecosystem of needs and partners who can play a role in the SUMURR market.

LIST OF ACRONYMS
ASHA Accredited Social Health Activists BMO Block Medical Officer CHN Community Health Nurses CSR Corporate Social Responsibility DPH Tamil Nadu Department of Health and Family Welfare EDD Expected Due Date GSP Global Solutions Partnerships GW The George Washington University ICDS Integrated Child Development Services IIT-‐M Indian Institute of Technology – Madras IVR Interactive Voice Response
mHealth Mobile Health OpenXC An open-‐source software and hardware platform
PHC Primary Health Center PICME Pregnancy and Infant Cohort Monitoring and Evaluation RCH Reproductive and Child Health RTBI Rural Technology and Business Initiative SHN Sector Health Nurses SMS Short Messaging Service/ Text Message State U.S. Department of State
SUMURR Sustainable Urban Mobility with Uncompromised Rural Reach TCOE Telecommunications Center of Excellence VHN Village Health Nurse

LIST OF FIGURES
Figure 1: SUMURR Project Framework 4 Figure 2: SUMURR Growth Strategy 5 Figure 3: SUMURR Maternal and Child Health Pilot Project Proposal 11 Figure 4: Global Partnership Map 13 Figure 5: Services Offered 14 Figure 6: How SUMURR Works in Kalrayan Hills 16 Figure 7: Beneficiaries’ Responses to SUMURR Mobile Application 18 Figure 8: Summary of SUMURR Pilot Project Indicators 20 Figure 9: Positive Outcomes from SUMURR 25 Figure 10: Potential Market Ecosystem for SUMURR 29

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 1
WHEELS ON THE GROUND, APPS IN THE CLOUD Since its founding in 1903, the Ford Motor Company (Ford) has focused on human mobility. Mobility is a basic human need, and a critical enabler of economic growth and human potential. Emerging economies require transportation systems to help their citizens access the goods and services they require. Unequal access to transportation often limits the opportunities available to those most in need. Unfortunately, there is a growing mobility gap between the rich and poor, as well as between urban and rural communities across the world.1 Over the past decade, technological advancements have helped address the issue of human mobility, but technology itself is not sufficient enough to address the global challenge of mobility gaps. In early 2011, David Berdish, Manager of Social Sustainability, and Dr. K Venkatesh Prasad, Senior Technical Leader, Open Innovation at Ford, met with each other to discuss possibilities for collaboration to help Ford go further. They were interested in exploring how to respond to the growing need for mobility in emerging markets. Mobility is a key enabler of economic growth and human potential, and unequal access to transportation often limits the opportunities available to those most in need. In particular, they used social sustainability issues as a lens for identifying future business opportunities. Berdish and Prasad decided to examine how Ford could use its vehicles and test its new technology platforms to bridge the mobility gap for isolated, rural communities by providing them with sustainable access to key services such as healthcare, clean water, and education. This conversation led to the creation of the Sustainable Urban Mobility with Uncompromised Rural Reach (SUMURR) concept, which envisioned Ford’s “wheels on the ground and apps in the cloud” empowering underserved communities. Within Ford, two key groups i.e. the Social Sustainability team and the Vehicle Design and Infotronics team played a crucial role in implementing the SUMURR project. This chapter describes how Ford’s social sustainability efforts and its technological innovations came together to define and create SUMURR, and position Ford for new market opportunities. SOCIAL SUSTAINABILITY AT FORD
In recent years, several trends have reshaped the global automobile sector including increased competition worldwide, global expansion of supply chains, changing consumer demands, and the rapid growth of sales in emerging economies. To effectively position for these changing realities, companies are integrating social sustainability priorities and resources into growth initiatives in new markets.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 2
One of the key highlights of Ford’s social sustainability strategy is its rigorous human rights code. In early 2012, Ford adopted the Code of Human Rights, Basic Working Conditions and Corporate Responsibility by revising its existing Policy Letter 24. One of the purposes of the revisions was to address human rights through the “Protect, Respect and Remedy Framework” proposed by United Nations Special Representative John Ruggie. Specifically, the code ensures respect for the rights of its employees, the communities around Ford facilities, as well as the communities around Ford’s suppliers’ facilities that might be affected by their operations.2 Not only does this code impact key operational issues, it also helps Ford maintain the trust and respect of the communities in and around which it operates. Building local trust is an important aspect of community engagement. Ford has supported community efforts since its founding more than 100 years ago. One of the primary outputs of the ONE Ford plan is to build a Better World, and so community engagement has remained a priority for the company.3 In addition, engaging local stakeholders can be a useful tool for companies to understand the needs of the communities in and around which they operate—especially in emerging economies—and integrate these considerations into their future business offerings. Ford is developing a more integrated approach to its local community engagement and human rights efforts, and linking them to the development of new products and services that meet the unique needs of the communities in emerging markets. An important stakeholder group for Ford in emerging markets can be the growing social entrepreneurship sector. By virtue of their dual motivation of profit and poverty alleviation, social entrepreneurs are well placed to facilitate a process of co-‐creating business solutions to social problems. Social entrepreneurs tend to be closer to the people to be served, to understand their needs and are better prepared to educate them, but often lack the ability to scale their ventures.4 Companies like Ford can play a critical role in helping social entrepreneurs create sustainable and affordable business models by engaging with them, learning about the market need, and providing them access to Ford’s product offerings and technology platforms.5
TECHNOLOGY PLATFORM For a number of years now, Ford has been pushing the evolution of the connected car forward. Ford believes that enhancing access to

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 3
connectivity will be the key to providing personal mobility solutions for its customers in the future. One of the teams making this vision come to life is Ford’s Vehicle Design and Infotronics team, who are responsible for research, architecture, standards, applications development and vehicle system integration of electrical, electronics and embedded software technologies. In 2007, the company launched the successful Ford SYNC system -‐ an agnostic software platform that allows users to connect their local electronic devices such as Bluetooth-‐enabled mobile phones, and digital music players, and operate them via voice commands. It opened up the demand for more available, affordable, and personalized in-‐car connectivity solutions.6 As a result, in September 2011, Ford unveiled the revolutionary OpenXC platform, together with its partner -‐ Bug Labs, an open-‐source innovation startup based in New York City. OpenXC is an open-‐source research platform that will enable developers to create custom-‐specific applications to advance in-‐car connectivity innovation.7 OpenXC transforms the car into a ‘plug-‐and-‐play’ platform where a combination of interchangeable open-‐source hardware and software modules can be quickly and easily customized to create unique applications. Applications developed for OpenXC can interact with Ford SYNC and may even extend the usefulness of the technology currently available in over three million vehicles. OpenXC technology can also send information over a 3G network, when available, which makes information accessible to others using a similarly connected device.8 Not only does OpenXC have the potential to revolutionize the customer experience in the car, it also has the potential to help Ford co-‐create new products and services directly with its stakeholders. This will enable Ford to pursue innovative business models in mature and emerging markets, where there is an exceptionally strong need for low cost, high value connectivity solutions.9
GOALS & OBJECTIVES The primary goal of SUMURR is to both gain intelligence on and shape the market by bridging the mobility gap for underserved rural populations. In other words, SUMURR will be deemed a success when sustainable access to key services such as healthcare, clean water, and education is available to isolated rural communities through the market, thereby contributing to the closure of the social equity gap by enhancing mobility.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 4
To achieve this goal, Ford identified three key project strategies and objectives: 1. Leverage Ford's vehicles and technology platforms by testing the technical capabilities of Ford’s innovative new OpenXC platform. 2. Engage global and local stakeholders by collaborating with partners on the implementation of the project. 3. Explore new market opportunities by conducting an analysis of local social and market needs.
Source: The Institute for Corporate Responsibility at the George Washington University (2013)
International public-‐private partnerships can synthesize the skills and resources needed to overcome global challenges like human mobility. This is why in 2011, Ford embarked on a partnership together with the U.S. Department of State Global Partnership Initiative (State) and the George Washington University (GW) to pilot the SUMURR concept. In 2012, the partners launched a pilot of the SUMURR concept in southern India. The pilot was designed to test the concept of a Ford vehicle delivering health services to remote areas, while connecting patients with healthcare providers and systems – their data and expertise, respectively – via the cloud through the use of applications and the OpenXC platform. The purpose of the pilot was to determine if the

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 5
concept was viable. If viable, in the future the pilot could be replicated and possibly scaled to determine whether it could deliver value to a social entrepreneur, a healthcare provider, or target populations in need. Source: The Institute for Corporate Responsibility at the George Washington University (2012)
Through SUMURR, Ford has a platform on which they can convene multiple stakeholders from the private, public and non-‐profit sectors in order to co-‐create technological solutions and social interventions that will bridge the mobility gap for underserved rural communities. Additionally, by working with multiple partners, Ford will continue to learn more about the needs of the local community, develop relationships with potential partners and discover new market applications for its products and services. The SUMURR project has the potential to illustrate how, when aligned and integrated, technological innovation and social sustainability can help Ford explore new market opportunities.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 6
BUILDING THE PARTNERSHIP On June 29, 2011, Ford signed a Memorandum of Understanding with the U.S. Department of State Global Partnership Initiative (State) and the George Washington University (GW) to test the SUMURR concept. The objective of the partnership was to launch a nine month pilot in India to empower women in underserved rural communities by leveraging Ford’s new OpenXC technology platform, State’s diplomatic and policy relationships, and GW’s academic expertise on innovative public-‐private partnerships models. WHY U.S. DEPARTMENT OF STATE?
In 2009, former Secretary of State Hillary Clinton launched the Secretary’s Global Partnership Initiative to “strengthen and deepen U.S. diplomacy and development around the world through partnerships that leverage the creativity, innovation, and core business resources of partners for greater impact.”10 Furthermore, State was interested in creating partnerships focused on women’s empowerment in developing countries, as it aligned with Secretary Clinton’s strong focus on global women’s issues and sustainable development. These conditions made State an ideal partner for SUMURR. Fortunately, GW already had an established relationship with staff at the Global Partnership Initiative, and was able to facilitate introductions, and initiate a conversation between Ford and State.
WHY THE GEORGE WASHINGTON UNIVERSITY? The Institute for Corporate Responsibility (ICR) at the George Washington University is a leading resource to the business community through business associations, and the policy community through federal agencies, Congress, local and regional governments, non-‐governmental organizations, and international organizations. By leveraging its location to foster a unique business-‐university-‐government partnership—US and global, the Institute for Corporate Responsibility presents a unique knowledge creation and dissemination asset on GW’s campus, building scholarly capacity for faculty and students, and enhancing GW's prestige worldwide. Ford recognized ICR’s expertise in developing multi-‐sectoral partnerships, and invited GW to provide intellectual leadership, and help frame the issues addressed by the partnership. Professor John Forrer at the ICR developed the innovative Global Solutions Partnership (GSP) model to facilitate a sustainable and effective way for organizations in the private,

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 7
public and non-‐profit sectors to collaborate around global governance issues to achieve long-‐lasting social change. The strength of the GSP model is that it provides a framework to nurture fragile multi-‐stakeholder partnerships in the early days of their formation and to help each other leverage the positive outcomes created as a result of the partnership. For more information on how the GSP model helps create value for all the stakeholders, please see Appendix A.
WHY CHENNAI? Together with these partners, Ford identified the location, general theme and potential implementing partners for the pilot project. In terms of location, Ford focused on India, in large part because over the coming decade Ford expects its global market base to alter significantly. The company predicts that by 2020, nearly one-‐third of its sales will come from the rapidly expanding Asia Pacific and Africa region – making this an ideal testing site for the SUMURR concept.11 India is one of Ford’s key growth markets, and it has had a presence in the country since 1995. Chennai is the primary manufacturing hub for Ford in India. Ford’s Vehicle Design and Infotronics team has strong ties to the renowned Indian Institute of Technology Madras (IIT-‐M), and its affiliated research centers -‐ the Rural Technology Business Incubator (RTBI), and the Reliance IIT Center of Excellence (RITCOE). Researchers from these facilities would provide technical expertise to develop applications for the OpenXC platform.
A FOCUS ON EHEALTH In April 2011, with the help of a team of graduate students from the University of Michigan, Ford identified that the provision of healthcare services would be the most effective in testing the OpenXC platform, while providing the greatest social benefit in India. Access to basic health services can significantly impact the quality of life for women and children in developing countries. However, the widespread accessibility of mobile technology presents a unique opportunity to efficiently address the challenges of maternal health.12 Maternal Health Care Divide in India
Countless statistics shed light on the vast healthcare divide in India; it goes deep and costs many lives. While urban areas have greater access to high-‐class tertiary health services and even act as hubs of medical tourism, basic health care facilities in rural areas remain limited in terms of
In rural and underserved communities, routine pregnancy complications often become deadly due to the lack of access to quality care. Some of the factors for this include poverty, distance from health centers, gender discrimination, lack of information, inadequate services, and cultural

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 8
accessibility. Healthcare is a sizable out-‐of-‐pocket burden for the poor as public spending on health is decreasing.13 Poor women and children in rural areas have been hit the hardest by this lack of accessibility. One of the most pressing challenges for women’s health in rural India is maternal and child mortality. India has the highest rate of maternal mortality in the world, and accounted for 20 percent (56,000) of total maternal deaths worldwide in 2010. It is not on track to meet its target to improve maternal health for Millennium Development Goal 5.14 This is alarming considering that the health of women and children is the cornerstone of public health, which supports healthy societies, social harmony and successful economies. Furthermore, it is unacceptable because most maternal deaths are due to preventable complications. In 2011, the Delhi High Court passed a landmark judgment deeming maternal mortality as a human rights violation.15
practices. Sufficient monitoring during and after the pregnancy, as well as access to a health center or skilled birth attendant for delivery can drastically reduce the prevalence of maternal mortality.16 The supply aspect of spreading healthcare services far and wide conforms mostly to the lack of infrastructure and resources. Installing infrastructure to cater to the majority of the population that is spread far and wide is as a major challenge as finding qualified health care service providers who are willing and able to travel to interior villages.17 Furthermore, the field health workers who are currently the interface between the community and public health system prioritize only those components that are backed by government schemes and cash incentives. Hence, while promoting institutional delivery is high on their list, raising awareness and health education take a back seat, further exacerbating the problem.18
WHY HAND IN HAND? By August 2011, the SUMURR global partners had already begun discussions with potential partners on the ground in Chennai, India to implement the pilot. Based on the recommendations from the research report written by graduate students at the University of Michigan in 2011, Ford reached out to the management of a major Indian hospital group that was known for its work in telemedicine.19 However, after weeks of meetings and conference calls, negotiations fell through due to a misalignment of goals. This was a major setback, and in October 2011, the global partners stopped to re-‐evaluate their outcomes, clarify their criteria for local partner selection and determine their process for identifying and vetting potential local partners. In November 2011, Dr. K. Venkatesh Prasad from Ford visited India to meet with the main technology partner in Chennai – the Indian Institute of Technology – Madras (IIT-‐M).

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 9
In the meantime, David Berdish, Manager of Social Sustainability for Ford Motor Company who was leading the pilot into implementation had identified two new prospects for the local partner and healthcare provider – Hand in Hand India and Voluntary Health Services -‐ both non-‐profits with backgrounds in healthcare work in Tamil Nadu, but with different core competencies. These prospects were based on the recommendations of another graduate student team from the University of Michigan, who visited Chennai in December 2011 to meet with both organizations. The team was accompanied on these meetings by Mitul Desai, one of the Senior Partnership Advisors at State. Both local non-‐profits expressed a cautious interest in SUMURR, but wanted more information.20 In December 2011, another important discussion took place – this time between David Berdish and Michael Boneham, at that time the President and Managing Director of Ford India. Boneham enthusiastically issued his support for the SUMURR project, and offered to contribute a Ford Endeavor, a high-‐end Sports Utility Vehicle (SUV) as well as the support of local staff from the Ford India corporate office based outside of Chennai. With the momentum around SUMURR building, but no local champion to manage the pilot, the partners felt that they needed to see what was happening on the ground. In February 2012, Berdish and Prasad from Ford, along with Gloria Cabe from the US Department of State, visited Chennai and conducted a number of meetings with local NGOs, stakeholders and potential partners. They were supported by local staff from Ford India and members of the University of Michigan student research team, who also accompanied them. Their meetings with the prospective NGO partners were largely positive, and further conversations helped the SUMURR team identify which of these organizations was the best fit for the pilot. One of the key meetings was with K.S. Sudhakar, the Project Director of Health from Hand in Hand India, a local NGO dedicated to the development of disadvantaged groups, particularly rural and tribal populations in the state of Tamil Nadu. He was enthusiastic to learn about the SUMURR partnership, and invited the visitors to see some of Hand in Hand India’s work in the field. After an exchange of information and a field visit, the global partners decided to work with Hand in Hand based on the fit with their mission and their verbal commitment to the project.21 Hand in Hand’s role was to provide access to a population in need, based on its expertise, relationships and history working in remote communities.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 10
The SUMURR team also met with many other local stakeholders including public officials from the local government – the Tamil Nadu Department of Health and Family Welfare (DPH), the technology team from IIT-‐Madras, officials from the US Consulate, and local social entrepreneurs. Subsequently, several of these groups became involved in the implementation of the pilot as well, including the Tamil Nadu DPH and IIT-‐Madras. This trip was hailed as a success, because the SUMURR team was able to confirm the local implementing partners and determine the exact intervention that the pilot project would undertake in just one week.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 11
Figure 3: SUMURR Maternal and Child Health Pilot Project Proposal
Proposal: To improve the delivery of maternal and child healthcare services using mobile phone based applications.
Location: Kalrayan Hills Block, Villupuram District, Tamil Nadu, India Target Population: Pregnant women and children in 29 villages under 4 Health Sub-‐Centers
Total regional population -‐ 10,555 A detailed list of the villages identified can be found in Appendix B.
Timeline: June 2012 – February 2013 A detailed timeline can be found in Appendix C.
Technology Scope: Two types of mobile phone-‐based applications were envisioned for the SUMURR pilot: 1. Mobile Form-‐based, that enables information collection during
registration and the maintenance of day-‐to-‐day records; 2. Voice-‐based, that enables the collection of relevant health information
through interactive voice response (IVR) calls and the sending of reminders and educational messages in the local language.
eHealth Strategy: These applications serve as a front-‐end interface for the end-‐users. The data received can also be viewed on a web-‐interface, which can be integrated with the existing PICME web interface. When used in conjunction, these two applications will enable three possible mobile health (mHealth) strategies: 1. Data collection for PICME 2. Personalized awareness and education campaigns -‐ via voice and text
message 3. Applications to access and enable broader health information
management systems Using these technologies, a VHN can improve antenatal care and health service delivery by ensuring that every pregnant woman in her service area is registered on PICME—tracking the progress of her pregnancy and conducting regular follow ups. In addition, the VHN can use this technology to improve vaccination coverage for newborns and infants.
Project Budget: The total project costs were estimated at `18, 00,700 ($36,014). Funding for the project was provided by the Ford Fund via Global Giving, a global NGO.
Implementation Plan: Ford India was to provide a Ford Endeavor for the project. The team from IIT was to provide the applications and technology. Hand in Hand was to provide access to communities and expertise on public health outreach by bringing in health care providers -‐ training them, and transporting them and the technology via the vehicle. The Tamil Nadu DPH pledged support for the project by connecting project staff to PICME.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 12
SUMURR PILOT IMPLEMENTATION This section outlines the roles and responsibilities of each of the partners and describes the services that were offered to the community by the SUMURR Maternal and Child Health Pilot project. This section also describes how the pilot project distinguished itself from other eHealth interventions and its significance for the Kalrayan Hills community. Ford Motor Company, from its global headquarters, enlisted eight partner organizations globally to support the SUMURR’s visioning, launch, implementation and monitoring. A detailed listing of their responsibilities and the key individuals involved is provided in Appendix D. 1. U.S. Department of State Global Partnership Initiative was the one of the first partners to support SUMURR, and provided guidance on project design. 2. The Institute for Corporate Responsibility at the George Washington University provided expertise on multi-‐sectoral partnerships, value creation, and business models. 3. Ford India Private Limited which served as the primary project coordinator in India. 4. Tamil Nadu Department of Health and Family Welfare provided guidance on the location and scope for the project. 5. Indian Institute of Technology -‐ Madras provided guidance on the technology component of the SUMURR pilot project. 6. IIT Madras Rural Technology and Business Incubator (RTBI) developed the SUMURR mHealth application.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 13
7. Reliance IIT Center of Excellence (RITCOE) supported the development of solutions for SUMURR around the OpenXC platform. 8. Hand in Hand India was responsible for developing and rolling out the health intervention in Kalrayan Hills. Additional support for SUMURR was provided by student teams from the University of Michigan prior to the project’s launch. The local partners were responsible for implementing the SUMURR pilot. Based on its legacy of community health outreach in the region, Hand in Hand brought to the partnership both knowledge of, and access to, the community in need of health services. Using the SUMMUR vehicle, Hand in Hand provided training for health care providers, the health service to patients, and gathered health information to bring back to PICME. IIT provided the technology platform, and Ford provided the vehicle. Tamil Nadu DPH provided a connection to the PICME database. A significant challenge during the pilot was coordinating timing with each local partner, especially from Dearborn. Berdish and Prasad were in communication with local partners, but the latter did not have the ability to deliver at the same time. As a result, the vehicle was in use before the connection to the cloud

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 14
through web based applications was ready. The “wheels were on the ground” before “the apps were in the cloud”. This provided time for Hand in Hand to familiarize health care workers and villagers with the vehicle. The mobile application and technology component were only offered during a month long trial period in November 2012. SERVICES DELIVERED
Over the course of nine months from June 2012 – February 2013, the SUMURR Maternal and Child Health Pilot project provided the community in Kalrayan Hills with several services to increase the accessibility of quality care for pregnant women and newborns. It is important to note that the services related to the mobile application and technology components of SUMURR were only offered to four VHNs, 15 Accredited Social Health Activists (ASHAs) and 30 expectant mothers during a month long trial period from November to December 2012.
SERVICES FOR VILLAGE HEALTH NURSES & OTHER COMMUNITY HEALTH WORKERS
1. Mobility Services: The vehicle was used on a weekly basis by multiple community health workers – primarily the VHNs. VHNs used the vehicle to register pregnant mothers on PICME, individually counsel the pregnant women, immunize children, provide iron supplements to pregnant women, and refer women to Primary Health Centers (PHCs) and other health institutions.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 15
While it was originally intended that the Endeavour would carry basic diagnostic equipment, that plan could not be implemented as the roads were too rugged to transport lab samples without a risk of contamination. Instead, the VHNs encouraged women to come to the PHC for testing every Tuesday. The vehicle was also used by the Block Medical Officer (BMO) to monitor the service delivery, Medical Officers of the concerned PHCs for counseling pregnant women on institutional delivery, and Sector and Cluster Health Nurses for service delivery and monitoring. Usage was determined by a weekly roster shown in Appendix E. 2. Training: Community health workers were offered a series of trainings on a variety of topics including home-‐based new born care, basic computer and mobile phone skills, and use of the SUMURR mobile application for data entry and transfer with special emphasis on PICME. 3. Monitoring of Antenatal Women: Local healthcare workers and trained project staff mapped all pregnant women and children under the age of five. This information is important to ensure that these women and children are being provided with the necessary services and specialist medical care they need right at their doorstep. 4. IVR-‐based Application for Health Data Collection: RTBI developed an innovative mobile application for the VHNs to input data about each woman that uses interactive voice response (IVR) technology. VHNs call a specific number and respond to an IVR menu to register pregnant women on the system. Each pregnant woman is registered using her unique PICME identification number. The VHNs have to answer a series of 13 questions about the woman, including some basic demographic information, the name of the baby’s father, the date of her last menstruation and her expected due date. These questions were filtered down from the larger PICME survey, after consultation with the VHNs. Data is received on a web platform in real time. At present, the system merely registers mothers’ basic information and does not yet enable follow-‐up.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 16
5. Web-‐based Maternal Health Tracking Platform: RTBI developed a web interface to test the feasibility of receiving, collecting and displaying the information received from the mobile applications in real time. In order to use the mobile application, the VHNs and ASHA workers need to be registered manually on the web interface, using their phone number as a unique identification number. Once the VHNs are registered, the web interface displays all the interactions made through the system i.e. phone calls made to register women, as well as the subsequent alerts and reminders to the community health workers, and the informational voice messages that are sent directly to the beneficiaries. The interface is an important step to scale the SUMURR pilot as it will demonstrate to the Tamil Nadu DPH the enhanced impact of linking PICME directly to the mobile applications. The connectivity adds value to the health delivery system. 6. Voice Alerts and Follow-‐Up Reminders: This is a feature of the mobile application developed by RTBI. Data is received on the web interface in real time and based on the expected date of

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 17
delivery received in the system, the systems begins to dispatch alerts and reminders to the VHNs and BMOs to follow up on key dates for the woman’s pregnancy. Both VHNs and ASHA workers receive a text message every week for four weeks: two weeks before and two weeks after, the woman’s due date. At present, the application does not send out immunization reminders, but that feature is currently being developed.
SERVICES FOR PREGNANT WOMEN & MOTHERS 1. Specialist Medical Care: Hand in Hand India relies heavily on two doctors, a pediatrician and a gynecologist, who volunteer their time to conduct weekly specialist medical camps in the villages. Each doctor is accompanied by a nursing assistant, the driver, and project supervisors. In the camp, the doctor will conduct basic check-‐ups, distribute medications, and provide patients with health education and advice. As a result of this direct interface with the beneficiary community, these doctors are also well-‐placed to track overall health conditions, and provide feedback to the BMO on a regular basis. 2. Health Awareness Campaigns: To educate the local community members about various health and social issues, Hand in Hand India conducted mass health awareness programs. The objective of these campaigns was to promote positive health seeking behavior. A professional cultural unit with the help of music and local folk arts conveyed the key health and social messages. The key issues addressed were personal hygiene and sanitation, nutrition and anemia, breastfeeding, immunizations, family planning, government health schemes, discrimination against female children, early marriage, and alcoholism. During these campaigns, informational pamphlets specifically catered for pregnant women and new mothers were distributed. 3. Emergency Ambulance Services: Since the launch of the SUMURR pilot project, the Ford Endeavor has provided emergency ambulance services and shuttled pregnant women and mothers from inaccessible points to local health institutions for delivery. The mobile numbers of project staff members and the driver have been distributed throughout the community, and people sometimes call them directly for help.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 18
4. Customized Health Information via Voice Messages: This service is provided as an extension of the mobile application used by the VHNs. Once the VHNs register a pregnant woman on the web platform, the system automatically generates and starts sending the beneficiary customized health information via voice messages. The voice messages sent are based on the expected due date or the last menstrual period date entered in the system. Messages start at week 11 of the pregnancy, and continue for a few months after the baby is born. There are a total of 50 messages – each one with specific information for that specific week in the woman’s pregnancy. The content for these messages was developed specifically for the local community by Hand in Hand India. Presently, the delivery of the baby still has to be updated manually on the web interface. Once the child’s birth is registered online, the system then sends informational messages that are relevant to newborns.
TECHNOLOGY USE The mobile application and technology component were only offered during a month long trial period in November 2012. Four VHNs, 15 ASHAs and 30 mothers participated in the technology trial with mixed success. The VHNs were not confident with the IVR system initially, and so the registration of the participating women was done directly on the web interface by RTBI. During the month long trial period, a member of the RTBI team followed up with each of the participating VHNs on a weekly basis to ensure that they were regularly updating the database. However, acceptance and usage of the technology was poor – out of 120 calls sent, 54 were attended by the expectant mothers and their families. At 45 percent, this level of call attendance was below average for previous mHealth applications created by RTBI.22 Towards the end of December 2012, a member of the RTBI team began to cross validate the system data directly with the participating women, and uncovered a number of issues with the validity of data from the field. Only four women (13 percent) who

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 19
received the informational voice messages found them useful. With this feedback, RTBI ceased sending the voice messages and sought to conduct further analysis on the barriers to adoption.23 In January 2013, the RTBI team conducted a field visit and met with local stakeholders. This exercise highlighted a number of challenges moving forward:24 i. Poor connectivity in Kalrayan Hills prevents VHNs from calling in to access the application.
ii. Current software is only based on voice recognition and not recording – making it cumbersome if the system does not recognize what the VHN is saying. The system will repeat the question for a maximum of three times, before going back to the beginning of the questionnaire.
iii. For IVR-‐based technologies such as this, pronunciation and grammar are critical and local accents and slang—both Tamil and English—need to be considered.
iv. VHNs have different rate plans and mobile service providers, so calls cannot be toll-‐free. The ideal call length for application acceptance is one to two minutes.
v. VHNs perceived the application to be an additional burden that is time-‐consuming since it is not yet integrated with PICME.
vi. Some stakeholders do not realize that the effectiveness of the application hinges on the accuracy of the pregnant woman’s expected due date.
vii. Beneficiaries are unable to provide VHNs with precise information on their age or their child’s age, or the date of their last menstrual period – highlighting the need for more health education and outreach.
viii. Technology training needs to be integrated with the community health intervention to ensure application uptake. RTBI is currently in the process of conducting an in-‐depth impact analysis of the SUMURR mobile applications.
SOCIAL OUTCOMES The SUMURR pilot project has received much attention in the community since its launch in June 2012. The Ford Endeavor is now a common and welcome sight in the villages of Kalrayan Hills. The vehicle has played a vital role in fostering local trust, because it is able to navigate the terrain, and reliably bring critical services to an underserved population.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 20
Although the original scope of the project identified 29 villages for implementation, demand for its services has spread by word-‐of-‐mouth as mothers who have benefited from its services tell their stories to the broader community. As a result, the SUMURR pilot project now covers a total of 54 villages in seven sub-‐centers, which is almost half of total population in the Kalrayan Hills block. Since the project started in June 2012, the Ford Endeavour has covered 16,651 kilometers, or 10,346 miles.25 Perhaps the most significant contribution of the SUMURR pilot project has been the mobility services provided by the Ford Endeavor.
“Previously, VHNs could only walk to one village at a time. Now with the car, she can do up to three in one direction, and five in the other.”

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 21
-‐ Mrs. G. Muthulakshmi Village Health Nurse
Primary Health Center – Kariyalur
Since June 2012, the Ford Endeavor has facilitated 225 community health visits, including trips to the field by Center Health Nurses (CHNs), Sector Health Nurses (SHNs), the Block Medical Officer (BMO) and other medical officers. 97 trips were made by the VHNs alone – an average of approximately 10 trips per month, which is a significant increase from their outreach before SUMURR. The field visits are critical because that is the only way to track the health of pregnant women and children, provide basic healthcare services, and educate the community on the public health facilities available to them.26
“It is very important to have the doctor go out with the vehicle, because this is an issue of comfort. Most of the beneficiaries have never seen a doctor in their life – they need to have face-‐to-‐face contact, in order to feel comfortable.”
-‐ Mr. K. Sudhakar Project Director, Health
Hand in Hand India
The Ford Endeavor has also provided transportation for the two local specialist doctors who volunteer their time to conduct frequent expeditions to the Kalrayan Hills area, known as medical camps. Over the course of the SUMURR pilot project, Hand in Hand India has held a total of eight gynecological camps, and 21 pediatric camps. In total, these camps have provided previously unavailable healthcare services to 183 expectant mothers, and 1,520 young children.27 Through the provision of emergency ambulance services, the Ford Endeavor has become an indispensable part of the local community health infrastructure. Although each PHC has an ambulance of its own, it is unable to meet community demand on its own. Sometimes the PHC receives multiple emergency calls at the same time, and sometimes the ambulances are unable to negotiate the hilly terrain to reach the women in time – in both cases, the Ford Endeavor has successfully responded to the needs of the community. In total, the SUMURR pilot has aided 45 women in having a safe institutional delivery of their baby. 28

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 22
Apart from mobility, the SUMURR pilot project has also contributed to building the capacity of the local community health workers. Since June 2012, a total of four healthcare trainings took place with 143 local health workers participating. Participants included VHNs, SHNs, CHNs, Accredited Social Health Activists (ASHAs), Reproductive and Child Health (RCH) staff and the Integrated Child Development Services (ICDS) staff. 29
Name: Mageswari Age: 19 Husband’s Name: Elumalai Village: Kodamaathi Nearest PHC: Kariyalur (38 km)
“Whenever I heard of a delivery in my village, I was anxious to know the outcome because I am aware of deaths in the hills during pregnancy. Being pregnant, I always had this fear in me because my village is inaccessible and generally pregnant women here are carried in cots / bed sheets through the forest to the PHC in the foothill for delivery. As my expected date of delivery was fast approaching, I was getting more and more anxious. One evening when I started showing signs of labor, my husband started calling 108 and they asked us to come to the nearest accessible point Ezhuthur which is about 15 kilometers. Then my husband called the VHN who had sent us this vehicle which picked me up from my home and took me to the PHC in about an hour and half. I was admitted at around 8 pm and I delivered a healthy boy at 11 pm. We have named our son Shiva. If not for this vehicle, I might have tried to reach the PHC in a two wheeler and do not know what would have happened. I feel we should not have problems anymore. Thanks to the vehicle.”
Source: Hand in Hand India (2013)
The SUMURR pilot project also provided the broader community with health education through two mass health awareness campaigns. In total, 44 villages were covered with 3,193 villagers participating in the programs. The first program was actually extended to 15 additional villages around the project intervention areas by local request. 30 In February 2013, Hand in Hand India also held a Pregnancy Fair (Pregnancy Mela), wherein pregnant women from the intervention villages were brought to the PHCs, registered on PICME, given information on the health facilities available at the PHC and the maternal healthcare services provided by government, and provided with individual counseling.31

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 23
Apart from this, basic information regarding maternal and child health has been painted on walls in villages all across Kalrayan Hills. Pamphlets specifically designed to target pregnant women and mothers of new born were also distributed to the community members. Five pamphlets were developed including information on the SUMURR pilot, basic maternal and child health information, dengue-‐fever prevention and so on. In total, 22,000 copies of these pamphlets have been distributed within the local community. 32
RESULTS OF THE PILOT SUMURR’S PILOT PERFORMANCE
Ford’s goal with the SUMURR project is to both gain intelligence on and shape the market by bridging the mobility gap for underserved rural populations. It seeks to do this by leveraging Ford's vehicles and technology platforms, engaging global and local stakeholders and exploring new market opportunities. The goal of the pilot was to test the viability of the unique combination of the vehicle, technology, health care providers, and health care data collection. This section will examine Ford’s experience with the pilot project against the three objectives identified to determine SUMURR’s performance so far. 1. Test the technical capabilities of the OpenXC platform: As yet, Ford has been unable to test the OpenXC platform through the SUMURR pilot because of the specific connectivity challenges in Kalrayan Hills. Partners are still working to develop a solution to this problem. Some possibilities include developing store-‐and-‐forward capabilities for OpenXC, and attaching a wireless signal booster to the Ford Endeavor.33 2. Collaborate with partners on implementation: By leveraging its position as a large multinational corporation, Ford has been able to facilitate relationships with the government, universities, nonprofits and other organizations to start a dialogue. According to the local partners, Ford’s biggest contribution has been to serve as the convener. The resounding message is that “People will listen, if it's coming from Ford.”34 3. Conduct analysis of local social and market needs: Prior to the launch of the SUMURR pilot, Ford worked with its university partners to

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 24
understand the local social and market needs. Researchers at the ICR conducted extensive analysis on the opportunities for Ford in the healthcare, clean water, and education sectors, as well as alternate financing options to make SUMURR viable. In the field, Hand in Hand India conducted reconnaissance visits and a baseline assessment of the health needs in Kalrayan Hills. RTBI also visited Kalrayan Hills numerous times to understand the connectivity challenges. A number of staff from Ford India have also visited Kalrayan Hills and have a good understanding of the accessibility needs of the local population. However, more needs to be done to identify other social entrepreneurs who can help Ford unlock local business opportunities for the SUMURR pilot. Throughout the various challenges associated with the project launch and implementation, the SUMURR partnership remained agile. Key partners including Ford, State, GW, and Hand in Hand focused first on the needs identified by the local community. Ford simultaneously supported IIT in the development of the technology components based in part on feedback from the health providers deployed by Hand in Hand, the social entrepreneur in the field. As a result, Ford has been able to create a simple, but highly valuable and visible intervention that has kindled a great deal of passion and excitement amongst the project stakeholders.
OTHER OUTCOMES According to the ICR, the success of the SUMURR partnership between Ford, State and GW is grounded in an inclusive and resilient partnership. Its value emerges when one considers the positive outcomes that have resulted from the process for some of the key partners as described below:

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 25
Ford Motor Company The company’s original objective with SUMURR had been merely to test its new technology and understand its potential market applications. However, even before the completion of the SUMURR Maternal and Child Pilot, Ford had already begun to reap its benefits. Based on the connectivity challenges encountered in Kalrayan Hills, Ford’s Product Development team is already working with its partners to develop new solutions for its OpenXC platform that have promising market opportunities. One potential opportunity is emerging in New Delhi, where stakeholders want to use the OpenXC platform to develop applications for trauma care and emergency response to road accidents.35 The Ford Sustainability team has successfully engaged key stakeholders in a dialogue on the future of accessibility, and has proven Ford’s ability to create innovative partnerships to achieve its social sustainability goals. As a result, a number of internal stakeholders within Ford have already begun to notice the innovation coming out of the SUMURR project and are interested in learning how the project can be scaled to other geographic regions in order to have an even larger impact.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 26
Additionally, based on the pilot, Ford has begun to gather intelligence on market needs for women’s health in one area of India. Given global trends for increased health needs, growth of emerging markets, and persistence of poverty, Ford may be able to leverage this knowledge for future market expansion in Asia and other parts of the world. Ford has already begun to better understand that it cannot access these markets alone, but needs to develop trusted partnerships to facilitate market entry and market application. Partners such as social entrepreneurs can bridge Ford to local markets. And the government sector can connect Ford with public needs and credibility. Ford India To commemorate International Women’s Day (March 8) this year, Ford India hosted the public media launch for the SUMURR Maternal and Child Health Pilot project. Ford India promoted the SUMURR Maternal and Child Health Pilot project as one of its Better World Initiatives, and it received good coverage by domestic and international media.36 Apart from this obvious benefit of visibility, Ford India has also been able to leverage SUMURR to enhance its corporate reputation, especially with the public sector. Ford India already had earned tremendous goodwill from the Tamil Nadu DPH, because of generous donations that the Ford Foundation had made towards public health in Tamil Nadu over the past 80 years. Recipients did not make a distinction between Ford Foundation and Ford India.37 However, this ambiguity might have implications for Ford India, if it wants to leverage this goodwill to cultivate a business relationship with the Tamil Nadu DPH for fleet sales. SUMURR has reinforced Ford India’s image as a trusted private sector partner for the government. According to the local partners, rather than providing the funding for the project, Ford’s biggest contribution has been to serve as the convener and bring together the different group of stakeholders. The resounding message is, “People will listen, if it's coming from Ford.” As a result, Ford India has also developed partnerships with other various stakeholders -‐ NGOs, local universities, social entrepreneurs, and so on that can be leveraged to create scalable solutions and market opportunities. Hand in Hand India Hand in Hand India’s aim is to alleviate poverty through integrated community development. One of its five focus areas is health and hygiene promotion, where it focuses on reaching out to underserved

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 27
communities. With the SUMURR Maternal and Child Health Pilot project, Hand in Hand India’s objective was to improve the delivery of maternal and child healthcare services by addressing accessibility gaps in Kalrayan Hills. In the process of establishing the SUMURR pilot, Hand in Hand India has begun to have an additional impact by initiating dialogue across the disparate government departments serving this neglected community. The project staff at Hand in Hand India is particularly skilled at managing relations with local government officials. Thanks to Hand in Hand India’s convening power, local stakeholders have learned of key bottlenecks in maternal and child health care, and have brought it to the attention of the local government to take action.38 Hand in Hand India is already planning to leverage its role as a convener to bring together the government departments responsible for tribal affairs to start a dialogue on the situation in Kalrayan Hills. 39 IIT-‐M’s Rural Technology Business Incubator RTBI’s mission is to design, pilot and incubate scalable business ventures with a rural focus. As an Incubator, it facilitates rural-‐inclusive technology and business innovation in India. Already, RTBI has begun to leverage the SUMURR pilot to provide opportunities for its incubated startups. For the development of the IVR technology used in the SUMURR pilot, RTBI worked with Uniphore, one of its incubated startups. For a full list of startups incubated by RTBI, see Appendix H. Moving forward, RTBI is already considering working with another one of its incubated startups, AYZH to provide community health workers in Kalrayan Hills with safe delivery kits and safe newborn kits.40

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 28
ON THE HORIZON LEVERAGING THE EHEALTH ECOSYSTEM
It is important to note that Ford is not planning on entering the eHealth space, but rather it is interested in exploring the commercial opportunities that might arise from supporting these new markets. eHealth is one example of new market space, where Ford can leverage its vehicles and technologies to create social and commercial value in this market. The business case for eHealth will likely come from two broad models. In the first scenario, participants in the eHealth value chain will need to identify unique value-‐added products and services that can generate sustained revenues.41 Partnerships between the various organizations in the eHealth space will be essential. C.K. Prahalad’s “market-‐oriented ecosystem” concept provides a useful model for a firm to leverage relationships with a wide variety of organizations from multiple sectors in order to create a pull in the market for its own products and services.42 The second model employs more of a top down approach, wherein organizations need to focus on marketing the benefits of eHealth, so as to encourage governments and other donors to invest in eHealth solutions via multi-‐sectoral partnerships together with NGOs, universities and the private sector. It is important to underscore how the firm’s products and services can integrate with existing government strategies and strengthen national health systems.43 Both models can be applied to SUMURR. Through SUMURR, Ford can help convene a group of potential partners, including non-‐profits, companies, social entrepreneurs, and government agencies -‐ to create a market-‐oriented ecosystem, and encourage governments to support this ecosystem. These organizations would provide a variety of complimentary healthcare services to its beneficiaries such as lab diagnostics, medicines, health insurance, and so on. With greater insights into the market needs and strong stakeholder relationships, Ford can leverage its core competencies to gain a competitive advantage in this new market.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 29
Using this approach and leveraging Ford’s core competencies, three possible avenues of revenue generation have been identified: 1. Fleet Sales: SUMURR-‐enabled vehicles can be modified to meet different needs such as health care, education and so on. Co-‐creation with local partners can help Ford create an appropriate vehicle to sell to the local market. The government and large institutions are the prime targets for this approach. 2. Financing: Alternative innovative financing options seek to address market challenges that prevent products or services from reaching a target market sustainably. Some examples include fee-‐for-‐service, service subsidization, and market linkage and entrepreneur support models.44 3. Data Management and Sales: SUMURR will enable Ford to collect and retain customer information about untapped markets. Previous experience in customer data sales can help Ford package and resell customers data, without infringing on customer privacy.
SCALING SUMURR GLOBALLY

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 30
The stories coming out of the SUMURR Maternal and Child Pilot project have captured the attention of senior leaders at Ford. Ford may expand the SUMURR project to China. Ford has yet to determine what intervention to provide through SUMURR, and which stakeholders to engage in China.
Ford may be able to leverage its experience with SUMURR in Chennai for future market expansion in Asia and other parts of the world. To operate in these more complex market environments, Ford must foster trusted partnerships. Such collaboration can facilitate market entry and illuminate market applications. Social entrepreneurs may be a target market as they offer a passion for solving social issues and a propensity to do it in a way that is financially viable. Social entrepreneurs and NGOs can bridge Ford to local needs. Local and regional governments can connect Ford with public needs and facilitate credibility. The SUMURR pilot has clearly addressed women’s need for mobility and connectivity during pregnancy and delivery. The next step lies in determining how the market will pay for such services. There is a great deal of opportunity for Ford to expand and scale SUMURR. The pilot in Chennai will be a worthwhile investment if only Ford will use its experience to explore how SUMURR might lead to further market opportunities. There is a world of social and market needs, and global and local stakeholders. Each area such as health, water or education can open up a new ecosystem of needs and partners who can play a role in the SUMURR market.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 31
ACKNOWLEDGEMENTS The authors would like to acknowledge the following parties for providing information and insights that contributed to the report: Mr. David Berdish, Ford Motor Company, for his tremendous passion for SUMURR, and his support and encouragement for our research. Dr. K. Venkatesh Prasad, Ford Motor Company, for connecting us with stakeholders in Chennai, and helping us understand the technological components of SUMURR. Also, thanks to Dr. Jayanthi Rao and Ms. Priya Sundaram for their assistance. Ms. Gloria Cabe, U.S. Department of State, for her strategic advice and counsel. Ms. Varsha Narasimhan, Ford India, for providing guidance and counsel, and helping to arrange meetings with the various stakeholders in Chennai. Also, thanks to the rest of the Ford India Team, including Ms. Jansi Rani, Mr. Abhishek Mahapatra, Mr. Sowmya Dev, and Mr. Prabuddha Jagadeb, for their support. The Rural Technology Business Incubator Team, including Ms. Suma Prashant, Ms. Sathyapriya Kittusami, Ms. Shanmugapriya, and Ms. Smriti, for their invaluable data and insights on the technological aspects of SUMURR, and for facilitating the various stakeholder meetings. Mr. K.S. Sudhakar, Hand in Hand India, for serving as a guide and translator in the field, and providing invaluable insights on SUMURR’s daily operations. Many thanks to the rest of Hand in Hand India team as well, including Mr. Ganesh, Mr. A. Sekar, Mr N. Babu, for arranging the meetings with stakeholders in Kalrayan Hills. Community Health Staff in Kallakurichi, including Dr. Satish Kumar and Mrs. G. Muthulakshmi, for allowing us to visit the local facilities and interact with patients and other staff. Dr. K Kulandaiswamy, Tamil Nadu Department of Health and Family Welfare, for providing insights into the local health system. Mrs. Latha Rajagopalan, Reliance IIT Center of Excellence, for her helpful explanations of the OpenXC platform. Without the time and effort of each of these individuals and entities, the completion of this report would not be possible.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 32
APPENDIX APPENDIX A: GLOBAL SOLUTIONS PARTNERSHIP MODEL
To ensure successful multi-‐stakeholder partnerships for global governance, it is important to understand the different expectations held by each individual partner and the nuances of what they are looking for in the specific partnership. The private sector needs to see the direct benefits to its business and make the business case for participating in such a partnership. To make the business case, companies need to show how the partnership will help them either manage their risks more effectively, explore new business opportunities or add value to their corporate social responsibility programs. Hence, the private sector needs a stable partnership through which they can capture value in the long-‐run. On the other hand, the public sector is driven by global rhetoric, policy and research. Priorities change with changes in leadership. There is greater emphasis on the upfront value of establishing the partnership, and lesser emphasis on the long-‐term impact. The public sector needs partners who are agile and capable of producing quick results. Meanwhile, non-‐profit organizations are strongly mission-‐driven and want stable partnerships for a substantial time period for them to show a tangible impact in their work. For this reason, non-‐profits look for partners who demonstrate a degree of flexibility, and strong commitment to the partnership, despite any initial setbacks. The Global Solutions Partnership model provides a rationale for governments and non-‐profits to engage unexpected private sector partners in innovative and resilient solutions for global governance. The primary factor that enables these creative partnerships is its unique approach to “vision the change.” Partners work together during the formation period to identify, and articulate a value creation proposition. The value creation proposition is a dynamic statement of how different stakeholders can create shared value, which can be captured individually, and furthers the individual goals and objectives of the collaborators. It serves as a catalyst in engaging stakeholders in a positive conversation around an issue. By adopting this multi-‐stakeholder and systems perspective, not only can individual actors cast the issue in a way that their stakeholders can understand and overcome a potential clash of cultures, but they can also create win-‐win-‐win scenarios for partnerships. In particular, this is very appealing to the private sector as it frames the partnership in language that is familiar to most senior managers. All businesses are founded on strong value propositions – in fact, it is the job of an entrepreneur to understand how something that is not being used can be made useful. Similarly, the value creation proposition enables businesses to think of how they can leverage their role in the partnership to create value for their own organization. Source: The Institute for Corporate Responsibility at the George Washington University (2012)

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 33
APPENDIX B: IDENTIFICATION OF TARGET AREA Before sending out the Ford Endeavour to the community, Hand in Hand India wanted to identify the most underserved villages in the Kalrayan Hills block as its intervention areas. Hand in Hand India held both informal discussions with local villagers, as well as formal stakeholder consultations with public health officials and community health workers. The following criteria were used to identify the intervention areas within the Kalrayan Hills block: • Distance from existing basic health care services • Status of basic infrastructure (i.e. roads and telecommunications) • Villages not covered frequently by the health workers • Mobile connectivity • Prevalence of myths and misconceptions • Medical issues pertaining to a local geographic area • Past occurrence of infant and maternal deaths • Observations during reconnaissance visit Source: Hand in Hand India (2012)

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 34
APPENDIX C: PROJECT TIMELINE
Source: Hand in Hand India (2012)
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
Pre-‐Planning Phase:Reconnaissance visitsInteraction with local stakeholders and expertsStakeholder ConsultationIdentification of Intervention areas Topline findings
Project Proposal & Baseline:Detailed Project ProposalBaseline report
Technology Development:Requirement ProvisionRequirement Analysis and FeedbackRequirements – Final version Framing of Use CasesApplication DevelopmentApplication testingRefinementDeployment for UATFeedback from clientsRefinement based on feedbackRelease of Version 1.0Feasibility Study
Implementation Phase:1.Training
1.1 Orientation Training for all Project staff 1.2 Training of VHNs , ASHAs & ICDS
a) Neo-‐natal care trainingb) Basic Computer Trainingc) Training on Mobile Applicationd) Refersher Trainingse) Others as per need
1.3 Training of Supervisor and Driver2. Community Education
2.1 Community Education on MCH Issues, Govt Services, Myths and Misconception3. Monitoring of Antenatal Mothers, New Born and Infants
3.1 Mapping of all antenatal mothers3.2 Screening of all antenatal mothers3.3 Mapping of all High-‐risk mothers3.4 Monthly Monitoring of High risk mothers
4. Addressing Accessibility Issues4.1 Deploying vehicle in the field4.2 Dry run4.3 First round of visits by VHN using the vehicle4.4 Monthly visit by Gynaecologist4.5 Monthly visit by Paediatrician
5. PICME Intervention6. Monitoring and Evaluation
6.1 Project Review Meetings6.2 End Line6.3 Progress Reports
7. Project Scaling and Replication7.1 Submission of pilot study findings 7.2 Discussions on scaling up / replication
January FebruaryACTIVITIES May June July August September October November December

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 35
APPENDIX D: SUMURR PARTNERS’ ROLES & RESPONSIBILITIES
Organization Responsibilities Point of Contact Ford Motor Company Ford is the project convener, and makes all the key decisions about the project
in conjunction with its partners. • Support implementation on the ground • Provides the technology-‐enabled vehicles, and access to the OpenXC platform
• Responsible for gathering data to determine the future scalability of the project
1. David Berdish Manager of Social Sustainability
2. Dr. K. Venkatesh Prasad Senior Technical Leader, Open Innovation
3. Dr. Jayanthi Rao Research Engineer, Ford Research & Advanced Engineering
U.S. Department of State Global Partnership Initiative
Provides partnership guidance, support and facilitation. Experts from State’s Global Partnership Initiative also provide background information on corporations and NGOs that were identified as potential local partners
4. Gloria Cabe Senior Advisor Global Partnership Initiative
5. Mitul Desai Senior Advisor for Strategic Partnerships, Bureau of South and Central Asian Affairs
Institute for Corporate Responsibility at the George Washington University
Brings expertise on public-‐private partnerships models. Its activities will include: • Provide real-‐time project evaluation • Conduct research on community needs, connectivity solutions, financing frameworks and potential for scalability
6. Dr. John Forrer Associate Director Institute for Corporate Responsibility
7. Meghan Chapple-‐Brown Director Office of Sustainability
8. Ridhima Kapur Research Associate University Sustainability Initiatives
Ford India Private Limited
Responsible for providing in-‐country support, coordinating with other partners, and providing the SUMURR technology. During the implementation of the pilot, Ford will undertake the following activities:
• Provide and equip a SUMURR-‐enabled vehicle • Use its existing relationships with IITM’s RTBI and other tech organizations to ensure that appropriate, useful applications are designed for data collection
• Monitor and track effectiveness of Ford car, SUMURR technology and partnerships
9. Abhishek Mahapatra Manager for Corporate Public Relations
10. Varsha Narasimhan CSR Communications Consultant
11. Priya Sundaram General Manager, Ford Technology Services
Hand in Hand India Act as the primary lead and contact point for the pilot. Its responsibilities 12. K.S. Sudhakar

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 36
include: • Project management • Provide drivers and supervisors • Identify the target community and the nature of the healthcare intervention, under guidance from the Government of Tamil Nadu Health Department
• Provide access to targeted rural communities for improved preventative care
• Develop and conduct maternal health education sessions, tailored to local health concerns
• Identify and train VHNs and other local health workers • Conduct Baseline Assessments • Provide insight on qualitative and quantitative data to track for the pilot
Project Director, Health 13. Ganesh
Project Director 14. A. Sekar
Project Supervisor 15. N. Babu
Project Driver
Government of Tamil Nadu Department of Health & Family Welfare
Provided guidance and detailed statistics on maternal health and infant mortality and posed a challenge to Ford to pilot the program in Kalrayan Hills, a region that is remote and hard to access
16. Dr. K. Kulandaiswamy Additional Director (Primary Health Care), Dept. of Public Health & Preventive Medicine
17. Dr. K Vanaja, Joint Director (Immunizations), Dept. of Public Health & Preventive Medicine
18. Mr. Nambi Azhagappan Statistical Assistant, State Bureau of Health Intelligence, Dept. of Public Health & Preventive Medicine
Indian Institute of Technology-‐Madras
Provides guidance to RTBI and RITCOE 19. Dr. Ashok Jhunjhunwala Lead of Telecommunications and Computer Networks Group
IIT-‐Madras’ Rural Technology and Business Incubator
Provides local technology expertise, and will undertake the following activities: • Liaise with PICME team at the Health Department • Develop new apps for PICME • Provide support for and maintain existing apps for SUMURR technology
20. Suma Prashant VP for Exploratory Initiatives
21. Sathyapriya Kittusami 22. Shanmugapriya
Reliance IIT Center of Excellence (RITCOE)
Involved in developing solutions for SUMURR around OpenXC platform 23. Dr. Latha Rajagopalan
SUMURR Maternal & Child Health Pilot | Final Project Review 2013 37
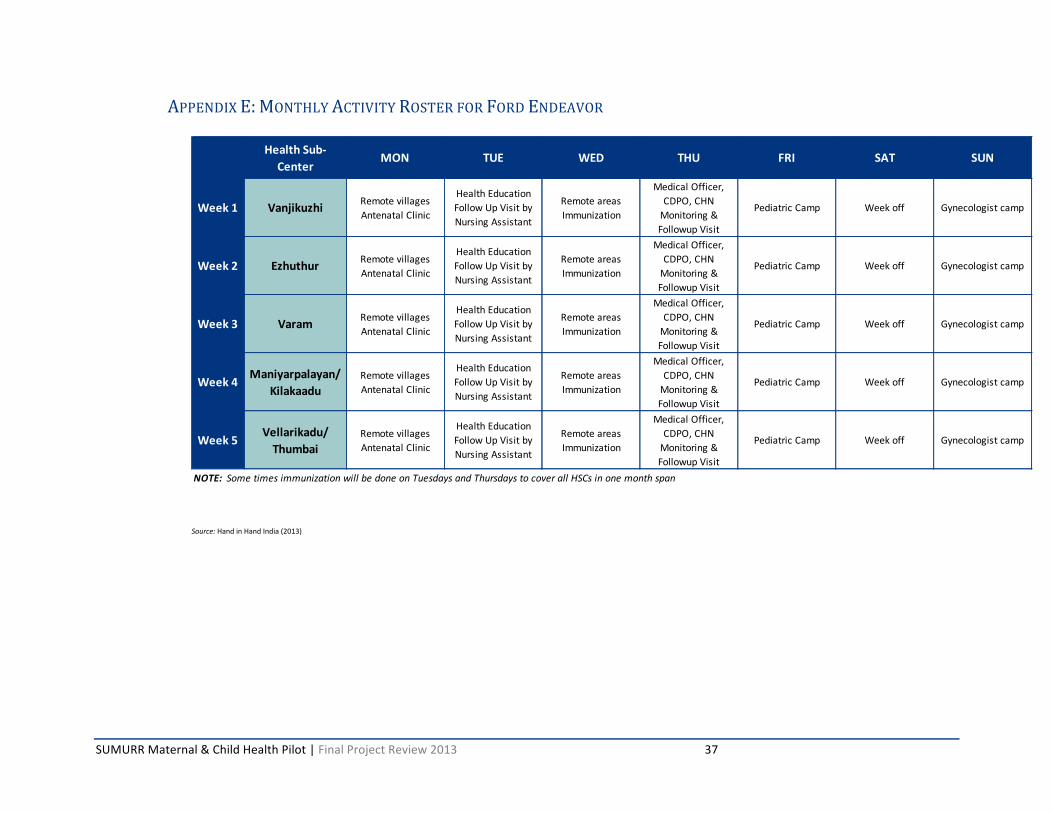
APPENDIX E: MONTHLY ACTIVITY ROSTER FOR FORD ENDEAVOR
Source: Hand in Hand India (2013)
Health Sub-‐Center
MON TUE WED THU FRI SAT SUN
Week 1 Vanjikuzhi Remote villages Antenatal Clinic
Health Education Follow Up Visit by Nursing Assistant
Remote areas Immunization
Medical Officer, CDPO, CHN Monitoring & Followup Visit
Pediatric Camp Week off Gynecologist camp
Week 2 Ezhuthur Remote villages Antenatal Clinic
Health Education Follow Up Visit by Nursing Assistant
Remote areas Immunization
Medical Officer, CDPO, CHN Monitoring & Followup Visit
Pediatric Camp Week off Gynecologist camp
Week 3 Varam Remote villages Antenatal Clinic
Health Education Follow Up Visit by Nursing Assistant
Remote areas Immunization
Medical Officer, CDPO, CHN Monitoring & Followup Visit
Pediatric Camp Week off Gynecologist camp
Week 4 Maniyarpalayan/ Kilakaadu
Remote villages Antenatal Clinic
Health Education Follow Up Visit by Nursing Assistant
Remote areas Immunization
Medical Officer, CDPO, CHN Monitoring & Followup Visit
Pediatric Camp Week off Gynecologist camp
Week 5 Vellarikadu/ Thumbai
Remote villages Antenatal Clinic
Health Education Follow Up Visit by Nursing Assistant
Remote areas Immunization
Medical Officer, CDPO, CHN Monitoring & Followup Visit
Pediatric Camp Week off Gynecologist camp
NOTE: Some times immunization will be done on Tuesdays and Thursdays to cover all HSCs in one month span

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 38
APPENDIX F: IVR TECHNOLOGIES IN MHEALTH
Name of Project: Comprehensive Rural Health Project (CRHP)45 Location: Jamkhed, India Partners: Global Health Bridge, Comprehensive Rural Health Project (CRHP) Timing: Launched in January 2012 Description: The pilot maternal health program in Jamkhed was launched by a non-‐profit in India called Global Health Bridge in partnership with the Comprehensive Rural Health Project (CRHP). This project allows Community Health Workers (CHWs) in developing countries to provide ongoing care and follow-‐up in rural communities. The cell phone-‐based health technology allows CHWs to obtain data on pregnant women and sends the CHWs and pregnant women regular reminders about essential antenatal visits in addition to helping monitor the health of high-‐risk pregnant women. The pilot has been launched in twenty-‐three villages and serves a total of 30,000 people. Name of Project: Baby Monitor: Interactive Voice Response System for Clinical Screening of Pregnant46 Location: Kenya Partners: With funding from USAID, Bill and Melinda Gates Foundation, Grand Challenges Canada, the Government of Norway, and the World Bank, InSTEDD partnered with the Population Council through their Kenya office Description: Baby Monitor was developed as a method for improved prenatal and postpartum screening of mothers and infants in resource-‐scare communities. This technology allows for clinical screening to be taken right to the women in the crucial time period prior to and after birth by using Verboice. Verboice is an interactive voice response technology (IVR) that allows for the detection of complications and allows for action to take place. Mothers receive calls at regular intervals before and after delivery where they listen to screening questions recorded in their local language and respond by pressing keys on their phone. Based on the mother’s responses, Baby Monitor will make necessary decisions and referrals that are individualized for the mother. Name of Project: Program for Accessible Health Communication and Education (PACE)47 Location: Kampala, Uganda Partners: PACE and Text to Change (TTC) Timing: Launched in 2011 Description: TTC designed a phone platform that incorporates SMS, MMS, voice and data in order to collect and spread information. Both SMS and IVR are utilized in order to reach out to women along with service providers to find out which women are utilizing family planning services. The program provides information of family planning clinic locations as well as sends reminders to women about follow-‐up appointments for the family planning services that they are seeking. The project benefits about 100,000 people.
Name of Project: Mobile Academy and Mobile Kunji48

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 39
Location: Bihar, India Partners: BBC Media Action, Bill & Melinda Gates Foundation, and Pathfinder International Timing: May 2010 Description: The project utilizes mobile phones, face-‐to-‐face training and mass media in order to reduce infant and maternal mortality in Bihar, India. A training course, named Mobile Academy, is delivered via IVR in order to broaden and refresh CHWs’ knowledge of ten life-‐saving actions and to further their communication skills. BBC Media Action has also created a multimedia service called Mobile Kunji in order to enhance CHW’s counseling of families. Mobile Kunji utilizes both an IVR-‐based mobile service and a printed deck of cards on a ring, which look like a mobile phone with pictures and key messages regarding child and maternal health. Each card has a code and when the health worker dials this number they can play the voice massage to the family via the mobile phone. Name of Project: Phones for Health49 Location: Tanzania Partners: CDC Foundation, President’s Emergency Plan for AIDS Relief (PEPFAR) Description: Phones for Health is a public-‐private partnership between mobile phone operators, handset manufacturers, technology companies, global health organizations and private donors who all want to enhance health care systems in developing countries through the widespread use of mobile phones. One project in Tanzania allows health workers to use mobile phones to collect data about infection rates for malaria, cholera, measles, typhoid and other diseases in the community. The mobile phone is connected to an IVR system, which allows health care workers to just call in and answer a few standard questions. Name of Project: The Mobile Alliance for Maternal Action (MAMA)50 Location: Primarily Bangladesh, India and South Africa Partners: Public-‐private partnership launched by the United States Agency for International Development (USAID) and Johnson and Johnson with supporting partners – the United Nations Foundation, mHealth Alliance and BabyCenter. Timing: Launched in May 2011 Description: MAMA allows expecting mothers to take health into their own hands. The program involves a global community, with over 49 countries using MAMA content as well as 111 organizations, to deliver crucial information regarding health to new and expecting mothers via mobile phones. Local programs design services based on the needs of the community. Mothers receive weekly health messages throughout the pregnancy and throughout the baby’s first year of life. Messages are continuously refined based on feedback.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 40
APPENDIX G: BUDGET PERFORMANCE REPORT
Source: Hand in Hand India (2013)
SUMURR Maternal and Child Health Pilot Project Budget Performance ReportJune 2012 -‐ March 2013
In Rs In $ In Rs In $ In Rs In $Pre-‐Planning PhaseReconnaissance visits 5,000.00 5 25,000.00 500.00$ 13,210.00 264.20$ 11,790.00 235.80$ 53%Stakeholder Consultation 20,000.00 1 20,000.00 400.00$ 9,527.00 190.54$ 10,473.00 209.46$ 48%Implementation Phase1.Training
1.1 Orientation Training for all Project staff 10,000.00 1 10,000.00 200.00$ 6,628.00 132.56$ 3,372.00 67.44$ 66%1.2 Training of VHNs, ASHAs & ICDS 80,000.00 1,600.00$ 82,673.00 1,653.46$ -‐2,673.00 -‐53.46 $ 103%1.3 Training of Supervisor and Driver 5,000.00 1 5,000.00 100.00$ -‐ -‐$ 5,000.00 100.00$ 0%
2. Community Education2.1 Community Education on MCH Issues & Govt. Services 15,000.00 30 450,000.00 9,000.00$ 383,439.00 7,668.78$ 66,561.00 1,331.22$ 85%
3. Monitoring of ANC Mothers, New Born and Infants3.2 Screening of all ANC Mothers 250.00 300 75,000.00 1,500.00$ 30,005.00 600.10$ 44,995.00 899.90$ 40%
4. Addressing Accessibility Issues4.1 Vehicle Maintenance (fuel) 10,000.00 8 80,000.00 1,600.00$ 80,000.00 1,600.00$ -‐ -‐$ 100%4.4 Monthly visit by Gynaecologist & Paediatrician 25,000.00 8 200,000.00 4,000.00$ 164,581.00 3,291.62$ 35,419.00 708.38$ 82%
6. Monitoring and Evaluation6.1 Project Review Meetings 5,000.00 8 40,000.00 800.00$ 40,000.00 800.00$ -‐ -‐$ 100%6.2 End Line 10,000.00 1 10,000.00 200.00$ 7,726.00 154.52$ 2,274.00 45.48$ 77%
Human ResourcesDriver for SUMURR Vehicle 8,000.00 9 72,000.00 1,440.00$ 44,500.00 890.00$ 27,500.00 550.00$ 62% Supervisor 10,000.00 9 90,000.00 1,800.00$ 48,623.00 972.46$ 41,377.00 827.54$ 54%Senior Project Coordinator 40,000.00 9 360,000.00 7,200.00$ 350,000.00 7,000.00$ 10,000.00 200.00$ 97%Project Director 60,000.00 2 120,000.00 2,400.00$ 120,000.00 2,400.00$ -‐ -‐$ 100%
1,637,000.00 32,740.00$ 1,380,912.00 27,618.24$ 256,088.00 5,121.76$ 84%
Administrative Costs (incl. computer, phones, etc.) 163,700.00 3,274.00$ 142,654.00 2,853.08$ 21,046.00 420.92$ 87%
1,800,700.00 36,014.00$ 1,523,566.00 30,471.32$ 277,134.00 5,542.68$ 85%
NOTE: 1) Assuming a constant exchange rate of US $ 1 = IN 50 2) Some pending advances and salaries for March 2013 still need to be booked and incorporated into the final financial overview.
PROJECT ACTIVITIES Unit Cost Units
Program Implementation Sub-‐Total
10% of Sub-‐Total
Total Costs
Total Budgeted Costs Total Actual Costs Total Unspent Amount % Budget Spent

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 41
APPENDIX H: RTBI’S INCUBATION PORTFOLIO IIT Madras’ Rural Technology and Business Incubator (RTBI) was founded in October 2006. RTBI is a registered not-‐for-‐profit society under the Tamil Nadu Societies Act. The inception funding support was from InfoDev and Department of Science and Technology, Government of India. Its mission is to design, pilot and incubate scalable business ventures with a rural focus. As an Incubator, it facilitates rural-‐inclusive technology and business innovation in India. Significantly it provides mentorship, funding, and an incubation eco-‐system suitable to entrepreneurs at any phase in their venture, including the early stage of ideation and conceptualization. Its current portfolio includes:51
Aaum -‐ Aaum Research and Analytics offers three lines of business: Advanced analytics, Competitive intelligence and Livelihood. The company is working on a first of a kind ‘credit scoring’ initiative for rural Self Help Groups supported by NABARD with pilots in Thiruvallur and Virudhunagar districts.
Arogyam Organics -‐ Arogyam Organics private limited was founded with a vision to make organic certified products available to Tier-‐2 and Tier-‐3 cities, as most of the certified organic food products are exported and availability in local market is almost negligible.
Augurtron -‐ Augurtron Systems and Solutions provides High-‐End Embedded Technology Product Engineering through research, development and productization in the Audio-‐video, Networking and Platform domains Augurtron has filed two technology patents in joint work collaborated with RTBI.
Ayzh -‐ Most maternal deaths occur in women from tribal/Dalit communities, with poor socio-‐economic status, and living in remote rural regions. Ayzh Health and Livelihood Solutions proposes to bring to market JANMA – a clean and green birth kit, for women in rural regions, with the aim to provide the “six cleans” recognized by WHO: clean hands, clean perineum, clean delivery surface, clean cord cutting and tying instruments, and clean cutting surface.
DesiCrew – DesiCrew Solutions Pvt. Ltd is a rural BPO company pioneering a new vision for stimulating inclusive growth in India. With a decentralized business model providing competitive outsourcing solutions to clients and meaningful employment opportunities, it is a technology driven, profit making social enterprise.
Edutor – Edutor Technologies e-‐learning Solutions Company focused on making Tablets an essential tool in the hands of a student. Edutor mobile learning environment and cloud based course delivery engine enables teachers/institutions deliver their courses on their new-‐age digital devices and improve their productivity.
Ét Interactive -‐ ET is a dedicated design consultancy firm working the Indian Craftsmen and Artisans. The company was established with the prime motto of uplifting rural craftsmen.
Intelizon Energy – A venture funded company designing solar based energy efficient products. They use state of the art optical, electronic and firmware technology for creating affordable energy products for the rural and semi-‐urban markets worldwide.
Invention Labs -‐ Invention Labs has developed Avaz, an augmentative and alternative communication device for the voice impaired and Cerebral Palsy affected children. This device is being used by 20 odd special schools spread throughout India.
Microspin -‐ Micro-‐spinning is a new concept in producing yarn from cotton at a scale that is hundred times smaller in scale. By establishing backward and forward linkages with other steps in the cotton value-‐chain, this technology is expected to do to the textile industry what the advent of the desktop did to the IT industry. Each such unit would sustain about 100 rural livelihoods.
MobilTrain – MobilTrain is a knowledge services company that specializes in providing mobile-‐based training to people in various sectors. After the successful teacher training pilot with rural and urban school teachers, MobilTrain approached IITM/RTBI for guidance, technology support and scaling up. RTBI would help in developing the SMS application for MobilTrain’s Teach-‐Spiration module beginning June 2011.
NewDigm -‐ Newdigm Healthcare Technologies provides healthcare solutions for resource limited settings. Their flagship product – clinical decision-‐support system (DSS) technology helps rural health-‐workers in arriving at a diagnosis, treatment and follow-‐up plan for patients. The mobile-‐phone based system guides health-‐workers in eliciting patient history, signs and symptoms and analyzes the fed data through accredited

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 42
medical protocols assisting in prompt and appropriate decisions.
POPP -‐ Phoenix Online Power Packers Pvt. Ltd. Offers a creative, professional and cost effective one stop IT solutions to fulfill business growth and varied IT needs of clients. POPP also builds a solid and respected business by specializing in Application Development, Web Development, SEO, Reputation Management, PHP, word press etc.
R.O.P.E -‐ Rural Opportunities Production Enterprise manufactures environment friendly home décor, lifestyle and packaging products from renewable natural fiber materials such as jute, bamboo, etc. ROPE empowers young women from rural families with employable artisan skills. These women are encouraged to take up suitable courses enabling them to master new crafts and production techniques, eventually becoming better professionals.
Stellapps – Stellapps Technologies provides cloud-‐based, wireless Machine-‐to Machine (M2M) solutions for the Agriculture sector. Stellapps has deployed SmartMoo™ -‐ a small-‐farm automation solution with features for efficient herd management, productivity improvement and hygienic milk production, enabling rural entrepreneurship that includes the Bottom-‐of-‐the-‐Pyramid (BoP)
Swayambhu Biologics – Swayambhu Biologics Pvt. Ltd. aims to sustain, support and promote high tech agriculture, horticulture and related economics. Swayambhu is presently imparting technology to compost sugar industry wastes and converting it into high quality manure as part of Joint Venture with Varun Phosphates and Bioorganics Pvt. Ltd.
UnClassroom – UnClassroom Learning India Pvt. Ltd. focuses on technology skills, specifically the PHP programming language and Facebook Application Development. Till date, we have created and launched three courses that are delivered via an online interactive learning platform that we have built. A provisional patent has also been filed for the above platform
Uniphore -‐ Uniphore's mission is to design and deliver mobility service applications that connect businesses with their customers and employees in real time. Uniphore's solutions elegantly integrate speech recognition and voice biometrics with smart mobile technology to deliver an efficient, end-‐to-‐end solution on the cloud.
Vastra -‐ Vastra-‐ Custom Attire (INDIA) Pvt Ltd is an initiative in distributed garment production started first in rural and urban Tamil Nadu. Vastra works with Self Help Groups who are trained for tailoring garments and customized institutional wear as per the requisite quality standard.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 43
APPENDIX I: NEW COMPANIES BILL The Indian Parliament is currently in the processing of passing the legislation known as the New Companies Bill, which is replacing the Companies Act from 1956. This bill will require companies of a certain size to spend two percent of their profits towards CSR activities. Once the bill is enacted, companies with revenue greater than ` 1000 Cr ($200M), or profits of ` 5 Cr ($1M) must spend two percent of the average of their last three years profit on CSR activity.52 In order to make this bill efficient and effective each company must establish a three-‐member CSR committee, which includes one Independent Director, to approve decisions regarding spending. There are a number of stipulations surrounding the New Companies Bill. Employee expenses may not be accounted for under CSR activity and if the proper amount of money is not spent on CSR activity the company must submit an explanation as to why and may be subject to penalization.53 The goal of this bill is to set forth money to help alleviate poverty, improve healthcare and education, and invest in social businesses in India. This bill will create approximately $5 billion in annual funds that need to be absorbed by the sector. While there is no shortage of NGOs in India, in order for the money to be invested in the most efficient way, it may be necessary for companies to prepare social enterprises for scale and sustainability.54

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 44
APPENDIX J: REPORT METHODOLOGY Both primary and secondary data were used to prepare this report. Primary data was gathered using key informant interviews that were conducted in Chennai, India. A research associate from GW conducted the interviews on a field visit in late-‐February, 2013. During the interviews, participants identified key data points that would be illustrative of the SUMURR pilot’s experience and provided them to the research team at GW to include in this report.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 45
REFERENCES
1 Ford Motor Company. (2012). Mobility Challenges and Opportunities. Retrieved April 28, 2012, from Ford Sustainability 2011/12: http://corporate.ford.com/microsites/sustainability-‐report-‐2011-‐12/financial-‐mobility-‐challenges 2 Ford Motor Company. (2012). Policy Letter No. 24: Code of Human Rights, Basic Working Conditions and Corporate Responsibility. Retrieved March 20, 2013, from Ford Sustainability 2011/12: http://corporate.ford.com/microsites/sustainability-‐report-‐2011-‐12/blueprint-‐governance-‐sustainability-‐policy-‐code 3 Ford Motor Company. (2012). Communities. Retrieved March 20, 2013, from Ford Sustainability 2011/12: http://corporate.ford.com/microsites/sustainability-‐report-‐2011-‐12/people-‐communities 4 Guesalaga, R., Pitta, D., & Marshall, P. (2008). The quest for the fortune at the bottom of the pyramid: Potential and challenges. Journal of Consumer Marketing, 393-‐401. 5 Simanis, E., & Hart, S. (2008). The base of the pyramid: Towards next generation BOP strategy. Ithaca, New York: Centre for Sustainable Global Enterprise. 6 Ford Motor Company. (n.d.). FACT SHEET: FORD SYNC® VOICE-‐CONTROLLED COMMUNICATIONS & CONNECTIVITY SYSTEM. Retrieved March 18, 2013, from Ford Media: http://media.ford.com/article_display.cfm?article_id=33358 7 About OpenXC. (2013). Retrieved March 8, 2013, from OpenXC: http://openxcplatform.com/overview/index.html 8Terdiman, D. (2011, September 12). Ford unveils OpenXC, invites open-‐source applications. Retrieved March 18, 2013, from CNET: http://news.cnet.com/8301-‐13772_3-‐20104962-‐52/ford-‐unveils-‐openxc-‐invites-‐open-‐source-‐applications/ 9 Ramsinghani, M. (2012). Ford Bets on the Digital Car. MIT Technology Review. 10 US Department of State. (2013). Public-‐Private Partnerships. Retrieved March 10, 2013, from Global Partnership Initiative: http://www.state.gov/s/partnerships/index.htm 11 Ford Motor Company. (2012). Our Strategy. Retrieved March 20, 2013, from Ford Sustainability 2011/12: http://corporate.ford.com/microsites/sustainability-‐report-‐2011-‐12/blueprint-‐strategy 12 Chang, P., Chiang, C.-‐e., Cucco, E., Schultz, K., & Shaughnessy, I. (2011). Empowering Women through Ford Technology. Dearborn, MI: University of Michigan, Stephen M. Ross School of Business. 13 Balarajan, Y., Selvaraj, S., & Subramanian, S. (2011). Health care and equity in India. The Lancet, 505-‐515. 14 World Health Organization. (2012). Maternal Mortality Fact Sheet. Retrieved March 18, 2013, from World Health Organization: http://www.who.int/mediacentre/factsheets/fs348/en/index.html 15 World Health Organization. (2010, June 4). Groundbreaking decision on maternal mortality in India. Retrieved March 20, 2013, from Partnership for Maternal, Newborn & Child Health: http://www.who.int/pmnch/media/membernews/2010/20100604_mm_india/en/ 16 World Health Organization. (2012). Maternal Mortality Fact Sheet. Retrieved March 18, 2013, from World Health Organization: http://www.who.int/mediacentre/factsheets/fs348/en/index.html 17 Balarajan, Y., Selvaraj, S., & Subramanian, S. (2011). Health care and equity in India. The Lancet, 505-‐515. 18 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 19 Chang, P., Chiang, C.-‐e., Cucco, E., Schultz, K., & Shaughnessy, I. (2011). Empowering Women through Ford Technology. Dearborn, MI: University of Michigan, Stephen M. Ross School of Business.

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 46
20 Bossi, M., Martin, R., Ranasinghe, E., & Shaughnessy, I. (2012). Ford SUMURR. Ann Arbor: University of Michigan. 21 Bossi, M., Martin, R., Ranasinghe, E., & Shaughnessy, I. (2012). Ford SUMURR. Ann Arbor: University of Michigan. 22 Kittusami, S., & Shanmugapriya, T. (2013, February 25). GW Visit to IIT-‐M's Rural Technology Business Incubator. (R. Kapur, Interviewer) 23 Kittusami, S., & Shanmugapriya, T. (2013, February 25). GW Visit to IIT-‐M's Rural Technology Business Incubator. (R. Kapur, Interviewer) 24 Kittusami, S., & Shanmugapriya, T. (2013, February 25). GW Visit to IIT-‐M's Rural Technology Business Incubator. (R. Kapur, Interviewer) 25 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 26 Muthulakshmi, G. (2013, February 27). GW Field Visit to Kariyalur Primary Health Center. (R. Kapur, Interviewer) 27 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 28 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 29 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 30 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 31Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 32 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 33 Rajagopalan, L. (2013, February 27). GW Call with Reliance Telecom Center of Excellence. (R. Kapur, Interviewer) 34 Prashant, S., Sundaram, P., Sudhakar, K., Narasimhan, V., Kittusami, S., & Shanmugapriya, T. (2013, March 1). Joint Stakeholder Meeting for SUMURR Pilot. (R. Kapur, Interviewer) 35 Narasimhan, V., & Dev, S. (2013, February 26). GW Visit to Ford India Private Ltd. (R. Kapur, Interviewer) 36 Narasimhan, V., & Dev, S. (2013, February 26). GW Visit to Ford India Private Ltd. (R. Kapur, Interviewer) 37 Kulandaiswamy, K. (2013, March 1). How SUMURR supports the Government of Tamil Nadu Department of Health and Family Welfare. (R. Kapur, Interviewer) 38 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 39 Sudhakar, K. (2013, February 27). GW Field Visit to Kalrayan Hills. (R. Kapur, Interviewer) 40 Prashant, S., Sundaram, P., Sudhakar, K., Narasimhan, V., Kittusami, S., & Shanmugapriya, T. (2013, March 1). Joint Stakeholder Meeting for SUMURR Pilot. (R. Kapur, Interviewer) 41 Mechael, P. (2009). The Case for mHealth in Developing Countries. Innovations: Technology, Governance, Globalization, 103-‐118. 42 Prahalad, C. (2004). The Fortune at the Bottom of the Pyramid. Wharton School Publishing. 43 Mechael, P. (2009). The Case for mHealth in Developing Countries. Innovations: Technology, Governance, Globalization, 103-‐118. 44 Abdallah, A., Dillman, J., & Duncan, B. (2011). Ford SUMURR Project: Innovative Alternative Financing Concepts & Applications. Washington, D.C.: The George Washington University Institute for Corporate Responsibility. 45 Maternal Health Platform. (n.d.). Global Health Bridge. Retrieved April 8, 2013, from Global Health Bridge. http://www.globalhealthbridge.org/projects/maternal-‐health-‐platform/ 46 Baby Monitor: Interactive Voice Response System for Clinical Screening of Pregnant. (n.d.). InSTEDD. Retrieved April 8, 2013, from InSTEDD: instedd.org/baby-‐monitor/ 47 SMS & IVR to improve family planning services. (n.d.). Akvo. Retrieved April 8, 2013, from Akvo: http://www.akvo.org/rsr/project/532/ 48 Empowering community health workers in Bihar: Mobile Academy and Mobile Kunji. (n.d.). BBC. Retrieved April 8, 2013, from BBC:

SUMURR Maternal & Child Health Pilot | Final Project Review 2013 47
http://www.bbc.co.uk/mediaaction/where_we_work/asia/india/india_sdp_empowering_chw_ma_mk.html 49 PEPFAR Public-‐Private Partnerships. (n.d.). CDC Foundation. Retrieved April 8, 2013, From the CDC Foundation: http://www.cdcfoundation.org/PEPFAR 50 MAMA. (n.d.). HUB: Health Unbound. Retrieved April 9, 2013, from HUB: http://healthunbound.org/mama/ 51 RTBI. (2010). Startups Incubated at RTBI. Retrieved March 16, 2013, from IITM's Rural Technology Business Incubator: http://www.rtbi.in/startup_pf.html 52 The Hindu. (2013). New Companies Bill mandates CSR spending. Retrieved March 18, 2013, from The Hindu: http://www.thehindu.com/business/companies/new-‐companies-‐bill-‐mandates-‐csr-‐spending/article4217872.ece 53 The Hindu. (2013). New Companies Bill mandates CSR spending. Retrieved March 18, 2013, from The Hindu: http://www.thehindu.com/business/companies/new-‐companies-‐bill-‐mandates-‐csr-‐spending/article4217872.ece 54 Acumen Fund. (2013). Information in this section from: India CSR Bill Creates Ripple in Social Sector. Retrieved March 18, 2013, from Acumen Fund: http://blog.acumenfund.org/2013/03/12/new-‐bill-‐means-‐big-‐funding-‐for-‐indias-‐social-‐enterprises/