surgical repair using biologic tissue matrix to facilitate ...synthes.vo.llnwd.net/o16/llnwmb8/us...
TRANSCRIPT

McMah
on P
ublis
hing
the Science Behind PoSitive Patient outcomeS
Reprinted from February 2013
Surgical Repair Using Biologic Tissue Matrix To Facilitate Tissue Healing: A Case-Based Report
IntroductionSurgeons have many prosthetic mesh options available for the rein-
forcement and repair of soft tissue. For ventral hernia repair, a common type of abdominal wall surgery, the addition of prosthetic mesh has significantly reduced recurrence rates.1 despite some favorable perfor-mance characteristics, synthetic mesh has been associated with compli-cations, particularly in complex repairs.2,3 Biologic grafts have a clinical rationale: each type is designed to serve as an extracellular matrix (ecm) scaffolding for neovascularization and eventual remodeling of tissue to resemble the native type.4 however, clinical outcomes may be greatly affected by unique characteristics and manufacturing processes that dif-ferentiate the available biologic grafts.5
Xcm Biologic tissue matrix—a sterile, non-crosslinked 3-dimensional matrix derived from porcine dermis—offers preservation of natural fibrous architecture that provides a scaffold for cell ingrowth and prolif-eration. a proprietary manufacturing process removes cells and dna for host acceptance, minimizing damage to native tissue architecture.6 Xcm has characteristics that make it advantageous for trauma surgery: it’s available in multiple sizes—2 cm × 4 cm to 20 cm × 30 cm—and comes hydrated and immediately ready for use, which eliminates the risk for contamination during soaking.6
Clinical Considerations in Mesh Selectionthe mesh material and tissue repair technique ideally are determined
after assessing patient factors, such as wound characteristics, past medi-cal history and comorbidities, anatomy, and vascularity.1
mesh-related infection—which has been reported at rates as high as 25%—is a risk factor for hernia recurrence.1 Because mesh-related infec-tion is associated with substantial morbidities like enterocutaneous fis-tulae and reoperation to remove infected mesh,7 strategies to minimize
the risk for infection are important in determining surgical approach, technique, and the choice of mesh material.
in the experience of hesham ahmed, md, assistant professor of sur-gery at umdnJ–Robert Wood Johnson medical School in new Bruns-wick, new Jersey, the strength of a mesh material is a major clinical concern because the repair must be durable. mesh strength can affect clinical performance, and a primary goal in soft tissue repair is to avoid splitting and tearing—especially in the early postoperative period.
“in abdominal wall reconstruction, you need to depend on the mesh for a few days or weeks—maybe 2 weeks in this kind of patient. the mesh is very important,” said dr. ahmed, who describes his patient pop-ulation as a mixture of acute and semi-elective cases including high-risk patients. in preclinical studies, Xcm porcine hydrated dermis mesh has been shown to sustain strengths greater than native tissue during the healing process.6,8,9,a Preclinical studies and clinical experience have shown Xcm to have high tensile strength, which, as noted by dr. ahmed, is an important mesh attribute in abdominal wall repair—one of several soft tissue repair applications for Xcm.6,8
in dr. ahmed’s practice, having a dependable mesh is paramount. “in trauma, patient selection is not an option, so the features of the mesh that is used are very important,” he said. in such a time-constrained set-ting, Xcm’s “out-of-the-package” availability for use is a clinical advan-tage. “With Xcm, there’s no hydration time, no orientation, and it’s very thick,” said dr. ahmed.
tissue regeneration and neovascularization are sought-after per-formance criteria. dr. ahmed described a patient who, after under-going abdominal wall reconstruction with Xcm, “had significant granulation tissue covering the mesh at almost 2 weeks. it’s an advantage when granulation can happen that fast. the mesh is doing what it’s supposed to do, assimilating itself into the natural tissue of the patient.”b in another case that was particularly complex, in which he placed Xcm over exposed bowel, “granulation tissue formed very quickly. the patient did very well and fistulae were avoided.”b
Finally, elastic properties of mesh can vary significantly. human acel-lular dermal matrix, for example, has shown significant differences in the amount of stretching it offers when used in the hydrated state.10,11 Surgeons have described elasticity as a consideration when selecting a mesh graft, with excessive stretching posing a potential detriment to clinical performance and outcome. in a small prospective study of
Supported by
Hesham Ahmed, MD
Assistant Professor of SurgeryUMDNJ–Robert Wood Johnson Medical SchoolNew Brunswick, New Jersey
a Bench/animal test results may not necessarily be indicative of clinical performance.b Results from case studies are not predictive of results in other cases. Results in other cases may vary.

McMah
on P
ublis
hing
2
integration.13 in addition to good tensile and suture pullout strength, preclinical studies performed in animals have shown that Xcm exhibits cellular infiltration and is well integrated while retaining many proteins and cytokines present in native tissue.12
Case Presentationb
a 48-year-old male was involved in a car accident while wearing his seatbelt. abdominal and pelvic computed tomography (ct) scans, as part of the trauma assessment, revealed hemoperitoneum. after the scan, the patient became hemodynamically unstable and was emer-gently taken to the operating room. Because of prior exploratory lapa-rotomy, chevron incision was used to enter the abdomen. two small bowel resections and a sigmoid colon resection were required.
due to the patient’s condition, a damage control approach was used and a temporary abdominal closure was performed with the intention of returning for a mature sigmoid colostomy and closure of the abdo-men within 48 hours. this was performed as planned but post-closure, the patient continued to have a fever and elevated white blood cell count, which required a rescan. necrotizing fasciitis of the abdominal wall—especially in the left side—was diagnosed and required mul-tiple trips to the operating room for aggressive debridement of the fascia and rectus muscle on the left side of the abdominal wall. he recovered but had complications of enterocutaneous fistula (Figure 1) and wound dehiscence at the chevron incision site.
patients with large, open abdominal wounds, human acellular dermal matrix was associated with a high rate of postoperative laxity at one year.11 dr. ahmed, whose experience with a variety of mesh materials has guided his treatment strategy, considers Xcm to be a good choice because “it will not provide too much stretching.”
Mesh Matters in the Surgeon’s HandsFor abdominal wall reconstruction, dr. ahmed typically performs
component separation (cS) and places mesh using the sandwich tech-nique, which consists of an underlay and an overlay. he finds that the cS approach—which employs native tissue—is useful for avoiding the development of seroma between mesh and fascia.
one of the most important aspects of decellularized ecm mesh materials is the combination of strength and integration.12 in the event of an infection, synthetics often require removal; in contrast, dermis-based meshes that incorporate into the repair may not require removal, thus potentially preventing expensive and challenging recurrences.3,12
dr. ahmed also has observed a low incidence of seroma formation with Xcm in his cases.b his observations are consistent with a study using other biologic meshes that evaluated functional outcomes and host responses to mesh materials that were manufactured with a vari-ety of tissue processing techniques, some of which led to modified collagen matrices.13 clinically, these processed meshes may be associ-ated with scar tissue, inflammatory responses, graft pleating, and poor
Figure 1. open wound with enterocutaneous fistula and colostomy. image courtesy of hesham ahmed, md.
Figure 2. vacuum-assisted closure dressing applied to the Xcm Biologic following repair.
image courtesy of hesham ahmed, md.
McMah
on P
ublis
hing
the Science Behind PoSitive Patient outcomeS
3
after prolonged wound care management and the use of a skin graft to cover his exposed bowel and to facilitate the management of his output from the enterocutaneous fistula, the patient was dis-charged home. he then developed a large hernia, mainly on the left side of the abdomen. approximately 9 months after the initial injury, the decision was made to reverse the colostomy, take down the enterocutaneous fistula, and perform abdominal wall reconstruc-tion to repair his large incisional hernia. the patient received preop-erative bowel preparation and antibiotics. a midline surgical incision was followed by extensive lysis of adhesions, takedown of both the enterocutaneous fistula and sigmoid colostomy, and reanastomo-sis for large bowel continuity. Subsequently, a large portion of miss-ing rectus muscle and rectus sheath was observed, especially on the left side.
Permanent monofilament sutures were used to approximate the sheath horizontally with some released incisions to be able to achieve approximation to reach the midline. on the right side, where most of the rectus muscle was preserved, cS was performed in the
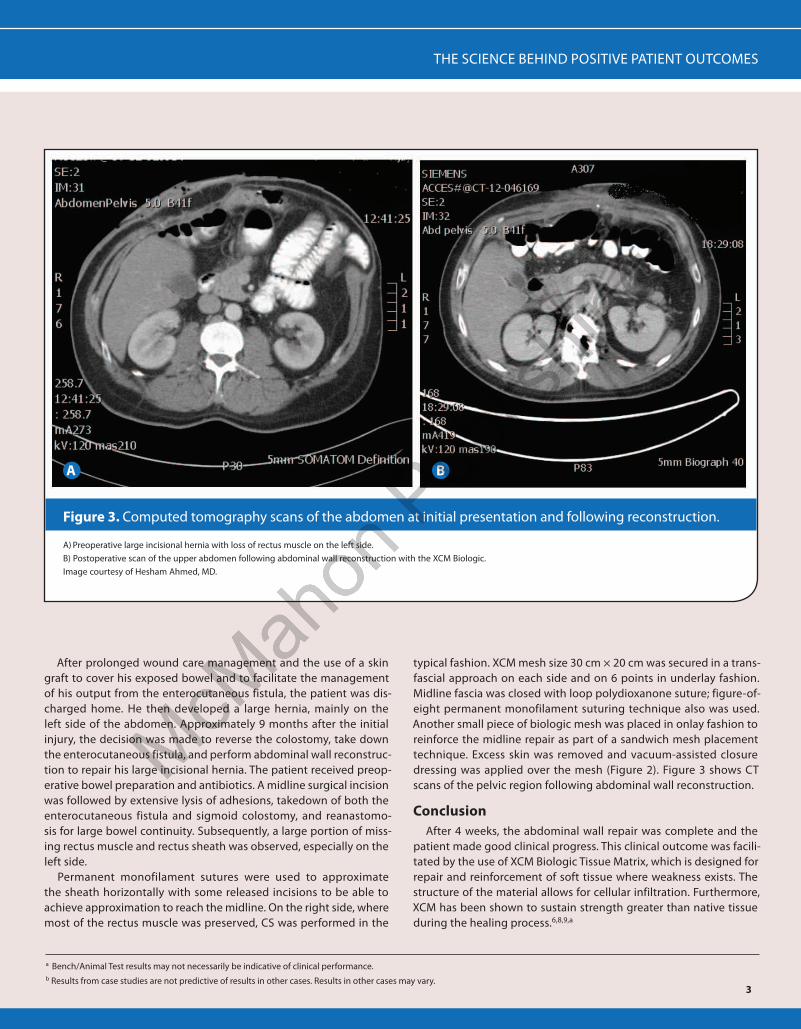
typical fashion. Xcm mesh size 30 cm × 20 cm was secured in a trans-fascial approach on each side and on 6 points in underlay fashion. midline fascia was closed with loop polydioxanone suture; figure-of-eight permanent monofilament suturing technique also was used. another small piece of biologic mesh was placed in onlay fashion to reinforce the midline repair as part of a sandwich mesh placement technique. excess skin was removed and vacuum-assisted closure dressing was applied over the mesh (Figure 2). Figure 3 shows ct scans of the pelvic region following abdominal wall reconstruction.
Conclusionafter 4 weeks, the abdominal wall repair was complete and the
patient made good clinical progress. this clinical outcome was facili-tated by the use of Xcm Biologic tissue matrix, which is designed for repair and reinforcement of soft tissue where weakness exists. the structure of the material allows for cellular infiltration. Furthermore, Xcm has been shown to sustain strength greater than native tissue during the healing process.6,8,9,a
Figure 3. computed tomography scans of the abdomen at initial presentation and following reconstruction.
a) Preoperative large incisional hernia with loss of rectus muscle on the left side.B) Postoperative scan of the upper abdomen following abdominal wall reconstruction with the Xcm Biologic.image courtesy of hesham ahmed, md.
A B
a Bench/animal test results may not necessarily be indicative of clinical performance.b Results from case studies are not predictive of results in other cases. Results in other cases may vary.
McMah
on P
ublis
hing
4
References1. harth Kc, Rosen mJ. Repair of ventral abdominal wall hernias. ACS Surgery: Principle
and Practice. ontario, canada: decker intellectual Properties; 2010.
2. Gaertner WB, Bonsack me, delaney JP. experimental evaluation of four biologic pros-theses for ventral hernia repair. J Gastrointest Surg. 2007;11(10):1275-1285.
3. dicocco Jm, Fabian tc, emmett KP, magnotti LJ, Goldberg SP, croce ma. components separation for abdominal wall reconstruction: the memphis modification. Surgery. 2012;151(1):118-125.
4. harth Kc, Rosen mJ. major complications associated with xenograft biologic mesh implantation in abdominal wall reconstruction. Surg Innov. 2009;16(4):324-329.
5. Gaertner WB, Bonsack me, delaney JP. visceral adhesions to hernia prostheses. Hernia. 2010;14(4):375-381.
6. Xcm biologic tissue matrix [general brochure]. West chester, Pa: Synthes, inc.; 2010.
7. Kingsnorth a. the management of incisional hernia. Ann R Coll Surg Engl. 2006;88(3): 252-260.
8. data on file. Kensey nash corporation; 2010.
9. hackett eS, harilal d, Bowley c, hawes m, turner aS, Goldman Sm. evaluation of por-cine hydrated dermis augmented repair in a fascial defect model. J Biomed Mater Res B Appl Biomater. 2010;96(1):134-138.
10. craft Ro, Rebecca am, Flahive c, casey WJ iii, dueck a, harold KL. does size matter? technical considerations of a regenerative tissue matrix for use in reconstructive sur-gery. Can J Plast Surg. 2011;19(2):51-52.
11. de moya ma, dunham m, inaba K, Bahouth h, alam hB, Sultan B, namias n. Long-term outcome of acellular dermal matrix when used for large traumatic open abdomen. J Trauma. 2008;65(2):349-353.
12. hoganson dm, o’doherty em, owens Ge, et al. the retention of extracellular matrix proteins and angiogenic and mitogenic cytokines in a decellularized porcine dermis. Biomaterial. 2010;31(26):6730-6737.
13. Sandor m, Xu h, connor J, et al. host response to implanted porcine-derived bio-logic materials in a primate model of abdominal wall repair. Tissue Eng Part A. 2008;14(12):2021-2031.
Disclosure
dr. ahmed received funding for his participation in this project.
For more information, go to www.synthes.com, or visit booth #311 and our lunch & learn symposium at the american hernia Society meeting on march 15, 2013.
disclaimer: this article is designed to be a summary of information. While it is detailed, it is not an exhaustive clinical review. mcmahon Publishing, Synthes, and the authors neither affirm nor deny the accuracy of the information contained herein. no liability will be assumed for the use of the article, and the absence of typo-graphical errors is not guaranteed. Readers are strongly urged to consult any relevant primary literature.
copyright © 2013, mcmahon Publishing, 545 West 45th Street, new York, nY 10036. Printed in the uSa. all rights reserved, including the right of reproduction, in whole or in part, in any form.
BB13
5J1
2119
-a