syncope - excellence.creighton.edu · 11/7/2018 1 syncope sanjay p. singh, md chairman &...
TRANSCRIPT
11/7/2018
1
SYNCOPE
Sanjay P. Singh, MD
Chairman & Professor,
Department of Neurology.
Syncope
• Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most often due to temporary and self‐terminating global cerebral hypoperfusion.
• SYNCOPE is a sudden and brief loss of consciousness associated with a loss of postural tone, from which recovery is spontaneous.
11/7/2018
2
Syncope
• This definition differentiates syncope from other nonsyncopal TLOC attacks, eg, seizures are due to a primary electrical disturbance of cerebral function and not cerebral hypoperfusion.
• Equally important is the need to distinguish syncope from apparent loss of consciousness events (so‐called syncope mimics or pseudosyncope); the latter includes cataplexy, drop attacks.
Nonsyncopal Attacks
11/7/2018
3
Causes of Syncope
• Decreased blood flow to the Brain.
• Primarily neurological problem – seizure.
Syncope ‐ Numbers
• The Framingham study reported an incidence of 6.2 per 1000 person‐years; cumulative incidence during 10 years was 6%.
• The cumulative incidence of syncope is 3 to 6 percent over 10 years, and 80 percent of patients have their first episode before 30 years of age.
•
11/7/2018
4
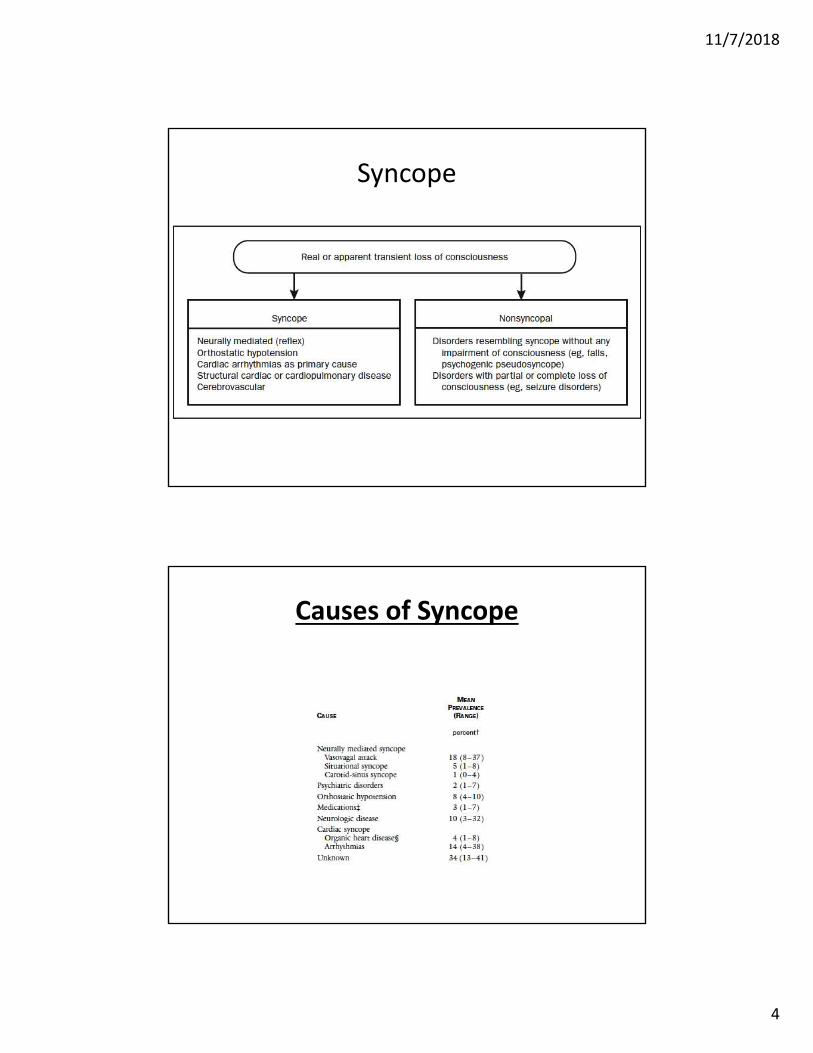
Syncope
Causes of Syncope
11/7/2018
5
Neurally Mediated Syncope
• Most common and is seen primarily in young adults . Vasovagal.
• A reflex response causes vasodilation, bradycardia, and systemic hypotension leading to decreased cerebral blood flow.
• Neurally mediated syncope includes vasovagal syncope, situational syncope, and carotid sinus syndrome/hypersensitivity.
Neurally Mediated Syncope
• Autonomic sympathetic nerves that constrict blood vessels and maintain blood pressure, in reflex syncope withdraw their input, and blood pressure falls.
• The vagus nerve which directly controls heart rate, can increase activity and cause the heart rate to fall (bradycardia).
11/7/2018
6
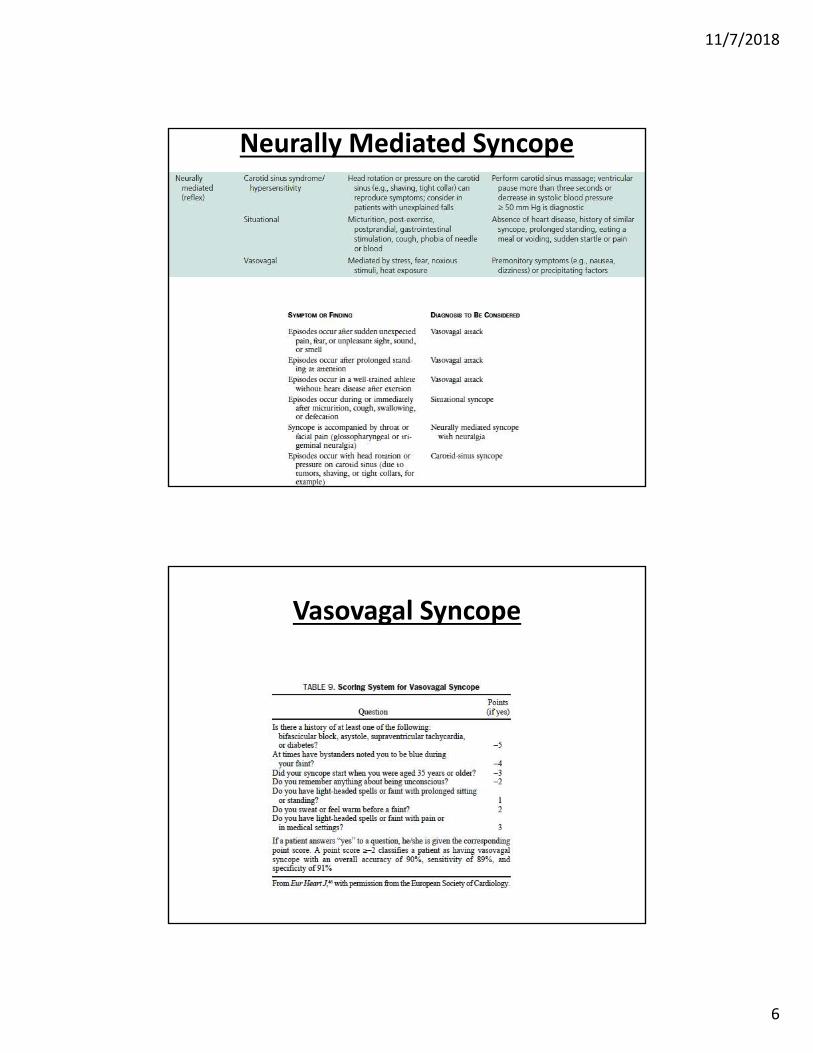
Neurally Mediated Syncope
Vasovagal Syncope
11/7/2018
7
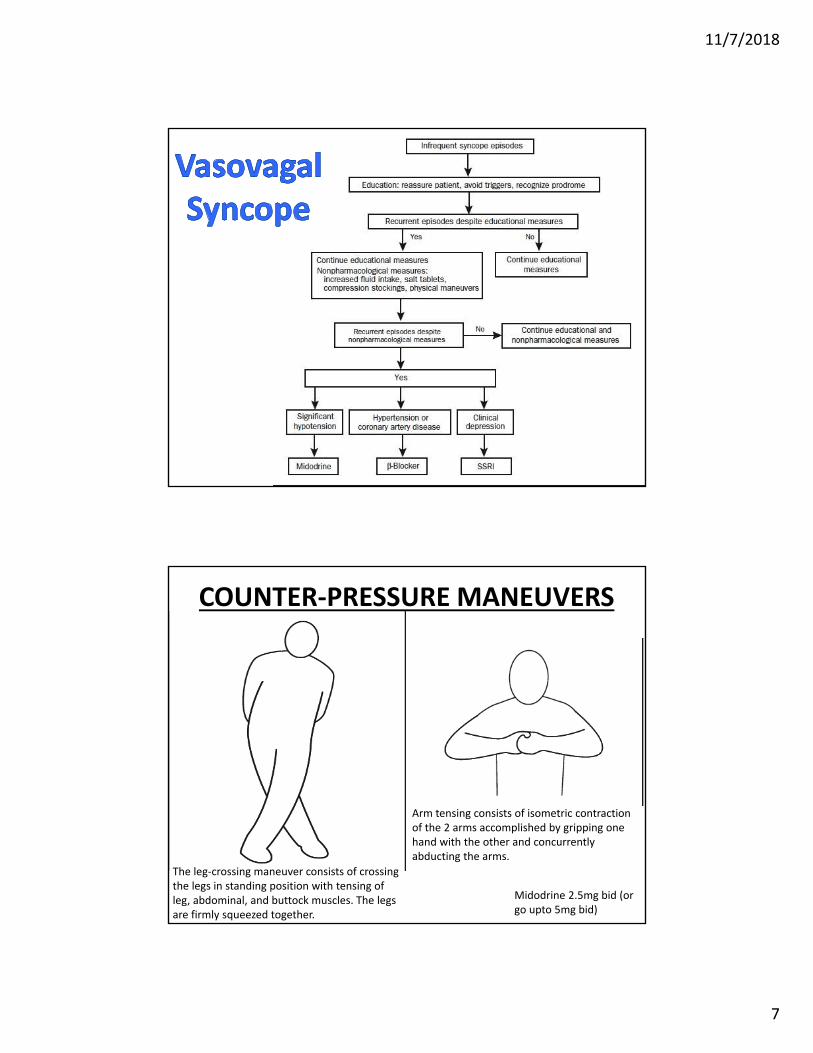
COUNTER‐PRESSURE MANEUVERS
The leg‐crossing maneuver consists of crossing the legs in standing position with tensing of leg, abdominal, and buttock muscles. The legs are firmly squeezed together.
Arm tensing consists of isometric contraction of the 2 arms accomplished by gripping one hand with the other and concurrentlyabducting the arms.
Midodrine 2.5mg bid (or go upto 5mg bid)
11/7/2018
8
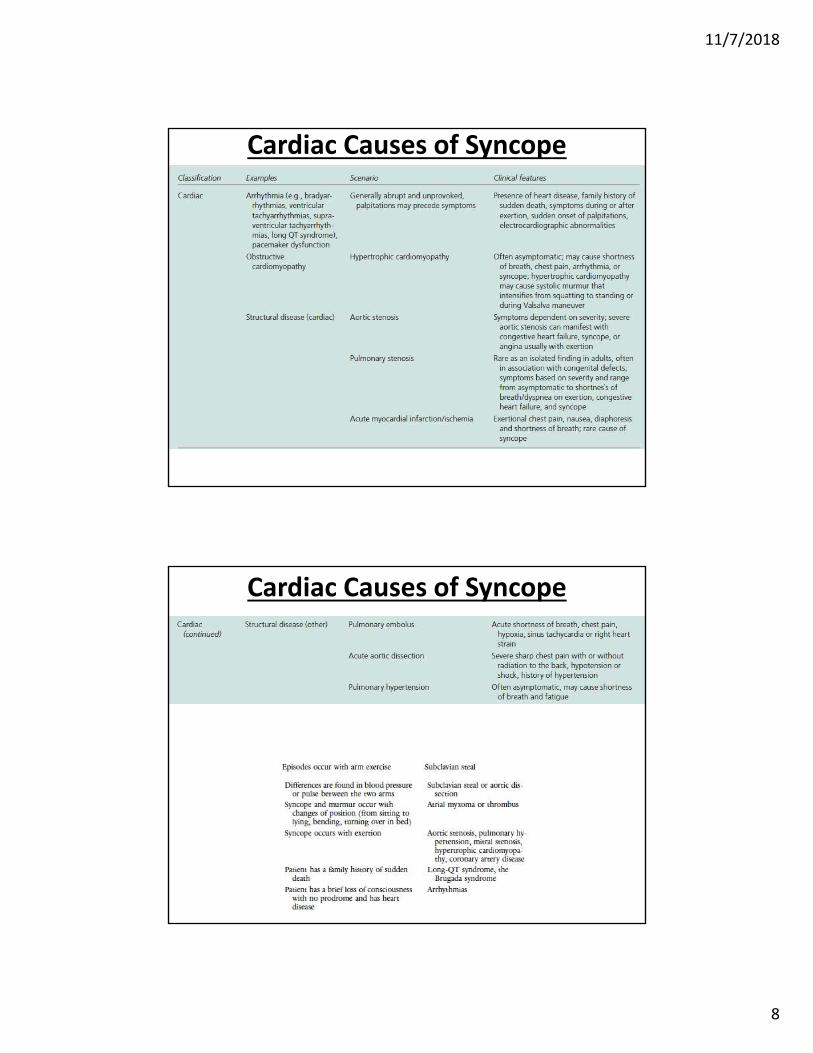
Cardiac Causes of Syncope
Cardiac Causes of Syncope
11/7/2018
9
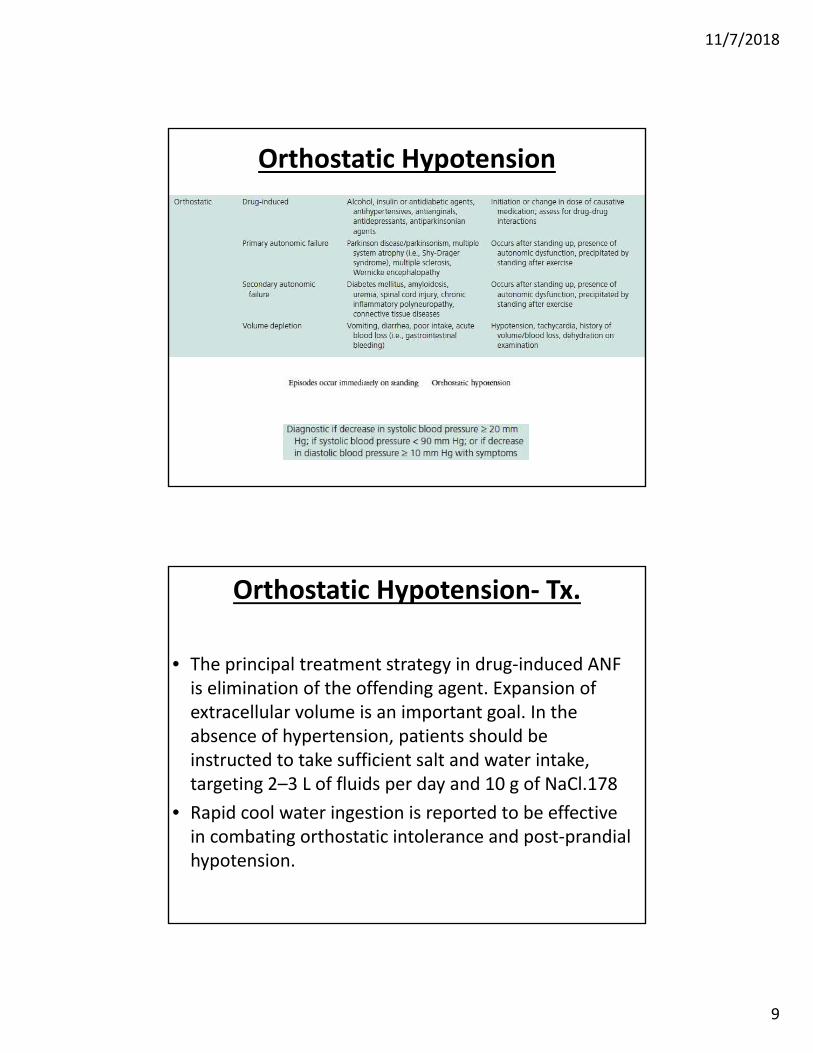
Orthostatic Hypotension
Orthostatic Hypotension‐ Tx.
• The principal treatment strategy in drug‐induced ANF is elimination of the offending agent. Expansion of extracellular volume is an important goal. In the absence of hypertension, patients should be instructed to take sufficient salt and water intake, targeting 2–3 L of fluids per day and 10 g of NaCl.178
• Rapid cool water ingestion is reported to be effective in combating orthostatic intolerance and post‐prandial hypotension.
11/7/2018
10
Orthostatic Hypotension‐ Tx.
• Gravitational venous pooling in older patients can be treated with abdominal binders or compression stockings.
• α‐agonist, midodrine, is a useful addition to the first‐line treatment in patients with chronic ANF.
• Midodrine (5–20 mg, three times daily) has been shown to be effective in three randomized placebo‐controlled trials.
Orthostatic Hypotension‐ Tx.
• Fludrocortisone (0.1–0.3 mg once daily) is a mineralocorticoid that stimulates renal sodium retention and expands fluid volume.
• The evidence in favour of fludrocortisone is from two small observational studies.
• Sleeping with the head of the bed elevated (108) prevents nocturnal polyuria, maintains a more favourable distribution of body fluids, and ameliorates nocturnal hypertension.
11/7/2018
11
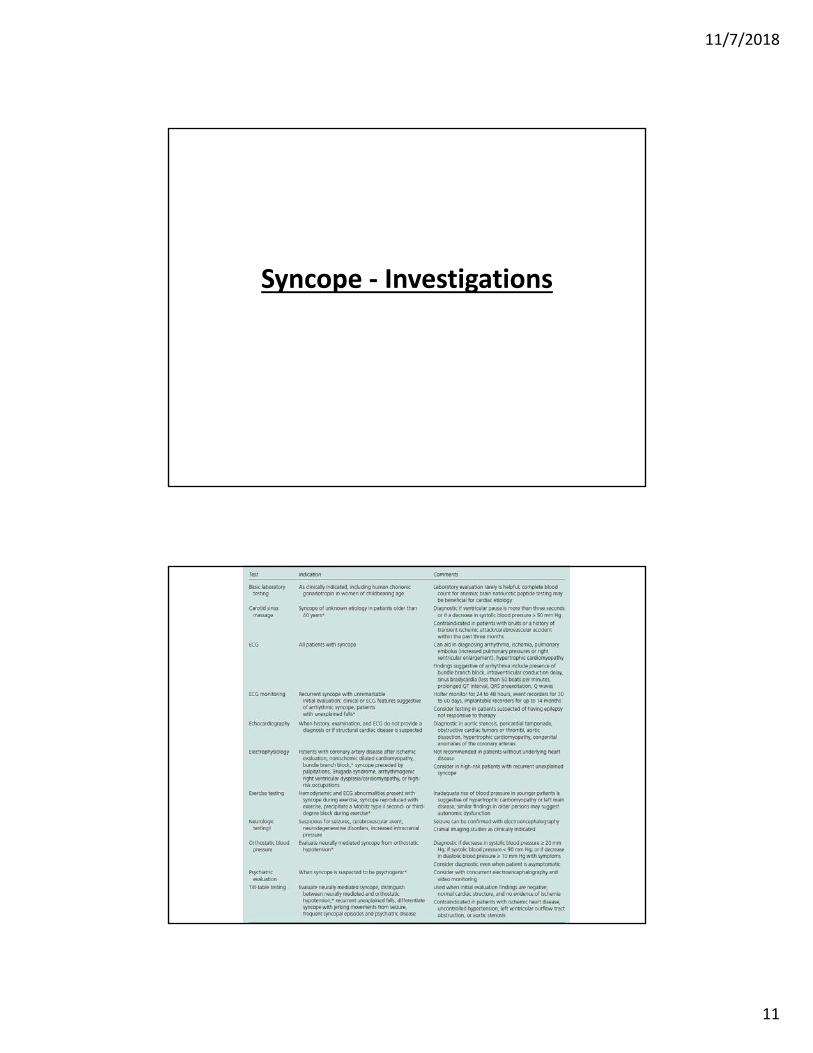
Syncope ‐ Investigations
11/7/2018
12
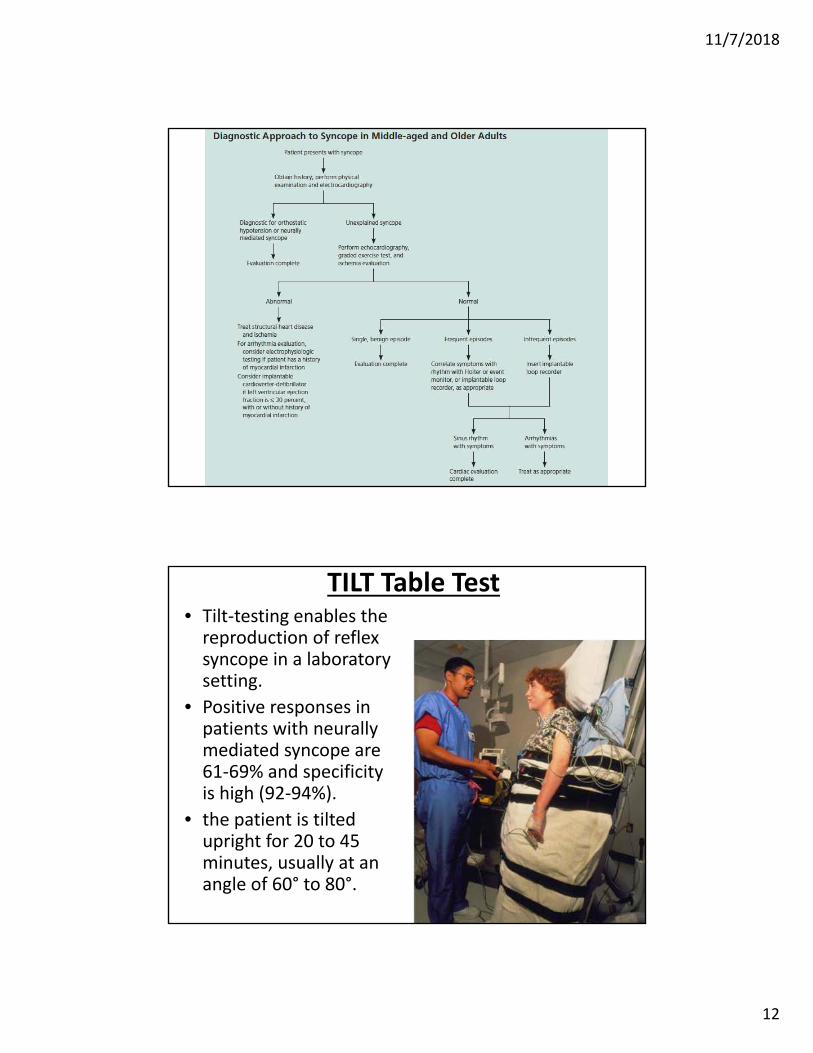
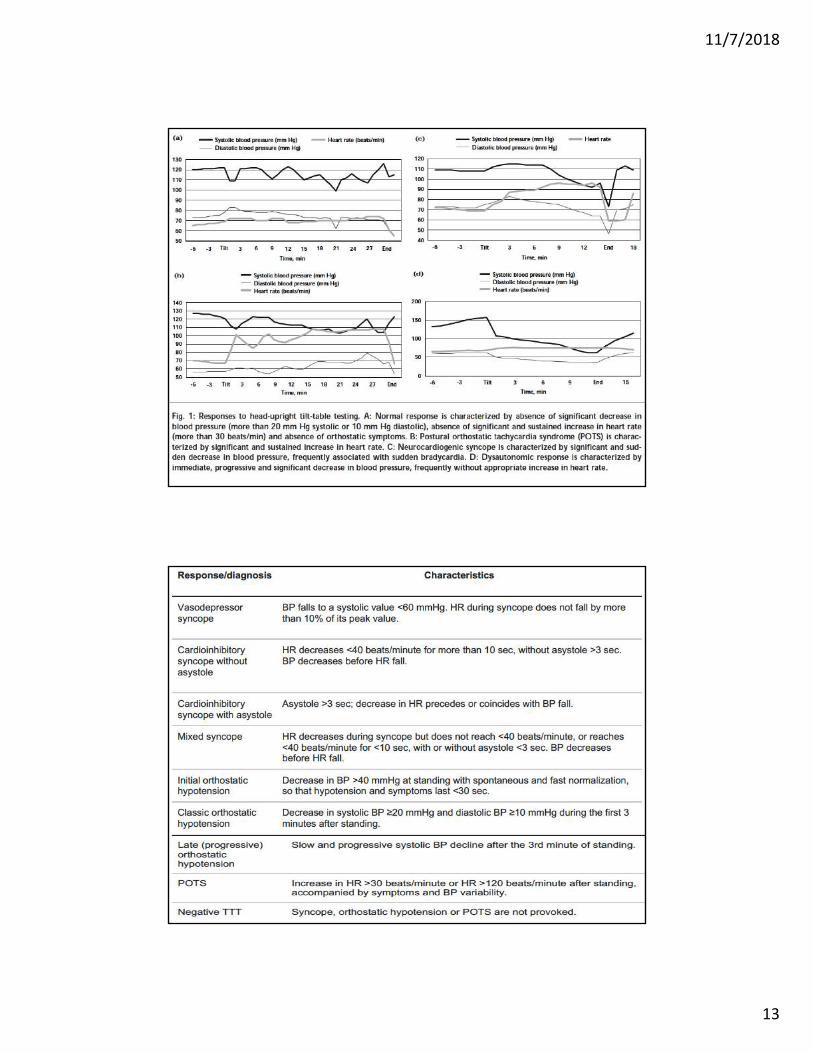
TILT Table Test• Tilt‐testing enables the reproduction of reflex syncope in a laboratory setting.
• Positive responses in patients with neurallymediated syncope are 61‐69% and specificity is high (92‐94%).
• the patient is tilted upright for 20 to 45 minutes, usually at an angle of 60° to 80°.
11/7/2018
13
11/7/2018
14
Neurological
SEIZURE
• Brain Cells
[Neurons] :
‘talk to one
another via
electrical
discharges’.
11/7/2018
15
SEIZURE
* Abnormal electrical discharges result in a
seizure.
* 2 Seizures – Epilepsy.
EPILEPSY
• Seizures – Abnormal electrical discharge in the brain leading to a change in behavior.
• Epilepsy – chronic disorder with spontaneous seizures.

11/7/2018
16
11/7/2018
17
Seizure ‐ Investigations
• MRI Brain.
• EEG
• Video‐EEG monitoring
Seizure ‐ Treatment
• Antiepileptic medications
• Epilepsy Surgery
• Vagal Nerve Stimulator

11/7/2018
18
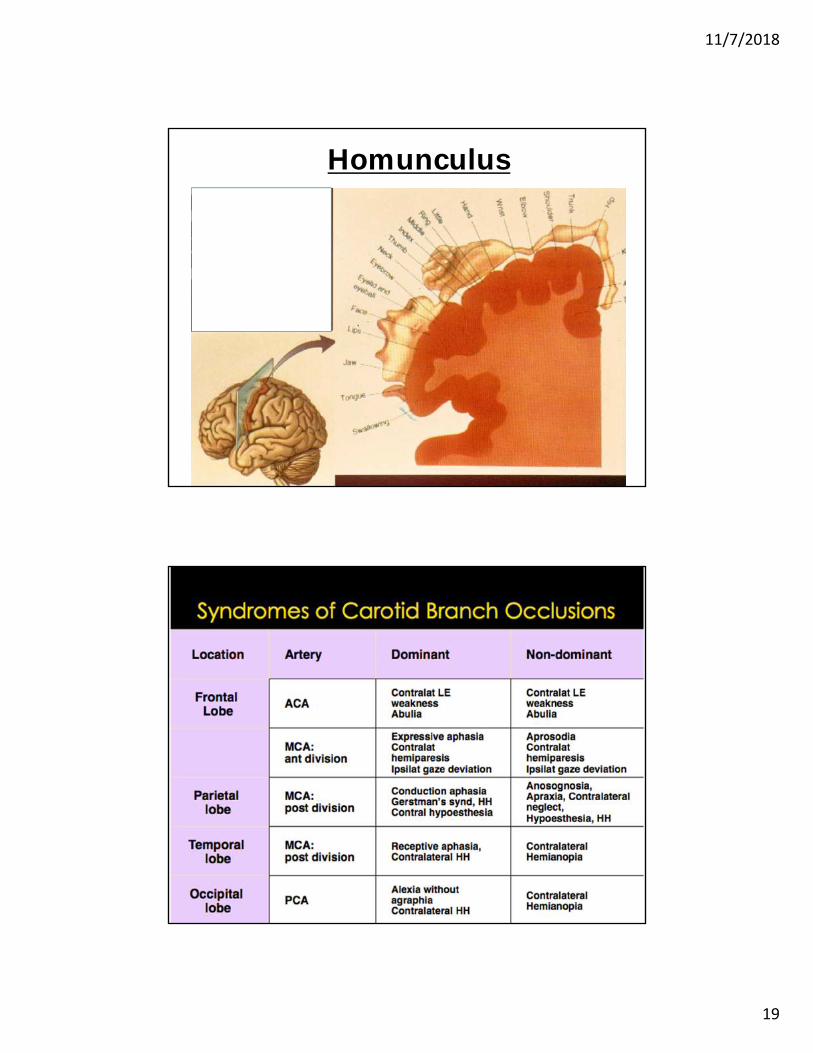
Stroke ‐ TIA
Anterior, Middle & Posterior Cerebral Artery
11/7/2018
19
Homunculus

11/7/2018
20
Vertebro-Basilar Insufficiency -Brainstem & Cerebellar signs
• Diplopia• Dysphagia• Dysarthria• Dizziness• Cranial nerve palsies
• Cerebellar – cerebellar signs.
Stroke Work up
• MRI Brain – DWI is the most senstive
• MRA Head & Neck
• Echo. – TEE vs TTE
• EKG
• Carotid Doppler