table of contents - aminer · pdf filetable of contents i. brazelton touchpoints center and...
TRANSCRIPT
TABLE OF CONTENTS
I. Brazelton Touchpoints Center and Touchpoints Model Overview
II. The Touchpoints Model of Development
III. Training Modules
IV. Proposal Guidelines
As of 8/19/2004
BRAZELTON TOUCHPOINTS CENTER & TOUCHPOINTS MODEL OVERVIEW
Brazelton Touchpoints Center (BTC) is a training program located at Children’s Hospital Boston. BTC offers a training model for practitioners that emphasize the building of supportive alliances between parents and professionals around key points in the development of young children.
The Model is an outgrowth of Dr. T. Berry Brazelton’s book, Touchpoints (1992), and the long-standing research that he and his colleagues have collaborated on at the Child Development Unit, Children’s Hospital Boston. In addition, the Model stems from twenty years of experience with training on the Neonatal Behavioral Assessment Scale (NBAS - Brazelton, 1973), training which values the practitioner as a critical agent in supporting and connecting with parents. The Touchpoints Model is intended to be a form of outreach, which engages parents around important information about their baby’s development. We envision that, as a result, they will be more likely to maintain involvement with their children’s system of care.
The Touchpoints Model reflects contemporary thinking on child development as an evolution of predictable developmental bursts, regressions and pauses. Each burst in development is typically accompanied by behaviors that appear exaggerated or regressive, followed by a pause in which the new behavior is fully achieved. Through each of these developmental periods, or “touchpoints,” the family experiences a parallel cycle of disorganization and adjustment.
During these cycles, especially when the child’s behavior becomes regressive, the potential for parental anxiety increases. Such anxiety can subsequently derail the child’s development or even lead to neglect, emotional or physical abuse. These “touchpoints” are key opportunities for practitioners to connect with parents. Through understanding each of the “touchpoints” and working together to anticipate and recognize them, parents and providers can collaborate on responses that will reduce or prevent other problems in the family.
All families would benefit from the Touchpoints Model, especially families who may not otherwise return for intervention and care because they feel providers offer little that is pertinent to them. Through the Touchpoints Model of outreach and prevention, practitioners can connect with more families and work with parents to bring about healthier, brighter outcomes for children.
As of 8/19/2004
ELEMENTS OF THE MODEL A critical feature of the Touchpoints Model is its view of child development as a dynamic interplay among maturational spurts, their manifestations in the child’s behavior, and the parallel effects on the parent. Using Touchpoints as windows of opportunity for providers to communicate with parents, the Model:
• stresses prevention through developing relationships between parents and providers. The earlier the alliance between practitioner and parent is formed, the greater the opportunity to create a strong collaboration. Thus, knowledge about early child and parent development is paired with the communication skills needed to make connections with parents;
• acknowledges that developing and utilizing relationships is critical to appreciating the significance of cultural, religious and societal dynamics for families;
• encourages the practitioner to focus on strengths in individuals and families, rather than deficits;
• provides insight into the emotional experience of the developing parent; • departs from traditional medical and social service provision in its
multidisciplinary approach. By combining the knowledge and perspectives of developmental psychology, education, nursing, pediatrics, psychiatry, and social services, valuable linkages are made to support children and families.
WHO BENEFITS FROM THE MODEL? First, the practitioner gains enhanced information about early emotional and behavioral development and about strategies to establish effective, supportive relationships with parents. Second, the parent, in alliance with a practitioner, learns to anticipate frustrating but normal phases in infant and child development and to work with them, rather than against them. Third and most importantly, the child benefits from growing up in a more supportive environment.
TOUCHPOINTS TRAINING
Brazelton Touchpoints Center faculty has developed the training model and curriculum materials in conjunction with a select group of multidisciplinary professionals with expertise in relational theory, diversity, and child development.
The goals of Touchpoints training are:
• to acquaint practitioners with the Touchpoints Model; • to encourage them to focus on the importance of establishing relationships with
parents;
As of 8/19/2004
• to provide them with assessment and communication skills which will enhance their interactions with families.
With these goals in mind, the training highlights the critical first years of development. The training weaves in two threads—behavioral and relational. Practitioners receive both child development information and communication strategies around each touchpoint. Using role-play, video and live family interactions, providers learn clinical applications of the Touchpoints Model. Touchpoints training also focuses on cultivating the practitioner-parent biases on clinical practice with families.
The program offerings are flexible and designed to meet the varied needs of healthcare, child care, education and social service professionals. They include:
• one-day “overview” workshops; • multi-day programs for groups of individual practitioners; • multi-day programs for groups of individual practitioners who are joining
an existing team; • week-long “train-the-trainers” sessions to prepare for community-level
action; • programs designed for particular populations through collaboration with
non-profit and profit organizations. For more information, contact Brazelton Touchpoints Center, 1295 Boylston Street, Suite 320, Boston, MA, 02215, or call (617) 355-6947; fax (617) 730-0060; e-mail [email protected] or visit our website at www.touchpoints.org.
As of 8/19/2004
TOUCHPOINTS LEADERSHIP AND TRAINING FACULTY Terry Ann Lunt, MPA, Executive Director Ann Stadtler, MSN, CPNP, Director, Site Development and Support A nurse practitioner with experience in private practice and in specialty clinics, Ms. Stadtler has served as the assistant director of the Medical Diagnostics Programs and the Director of the Preschool Function Program, and also as the Clinical Coordinator of the Pain and Incontinence Program at Children’s Hospital, Boston. She is also Chair of the Infancy Panel for the new volume of Bright Futures in Practice Mental Health, whose focus is prevention of mental disorder and promotion of optimum mental health. T. Berry Brazelton, MD, Founder A world-renowned pediatrician and expert on child development, Dr. Brazelton has written many books for parents as well as hundreds of publications for scientific and medical communities. The Touchpoints model is based upon over 40 years of his practice and research. In recent years, Dr. Brazelton has become a leading advocate in the United States for family and child health. Three of his books are pertinent to Touchpoints: Touchpoints: the Essential Reference (1992), The Irreducible Needs of Children (2000), and Touchpoints Three to Six: Your Child’s Emotional and Behavioral Development (2001), the latter of which was co-authored with Joshua Sparrow, MD.
Joshua Sparrow, MD, Director, Special Initiatives Dr. Sparrow is a senior consultant for inpatient psychiatry services at Children’s Hospital, Boston, Instructor in Psychiatry at the Harvard School of Medicine, and Associate Professor of Psychiatry at the School of Medicine of the University of Marseille, Marseille, France. His current research interests include outcome studies in the treatment of eating disorders in adolescents, the effects of prenatal diagnostic testing on parent-infant relationships, and the application of Touchpoints model to school-age children and adolescents. Dr. Sparrow and Dr. Brazelton are the co-authors of Touchpoints Three to Six: Your Child’s Emotional and Behavioral Development (2001). Lisa Desrochers, MEd Lisa Desrochers is an early childhood educator with extensive experience working in child care and preschool environments. Her work has centered primarily on developing innovative curriculum and documentation strategies to enhance young children’s learning and form collaborative partnerships among children, parents and teachers. She currently coordinates the Touchpoints programs of the Harlem Children’s Zone and CarePlus Health Plan projects in New York City. John Hornstein, EdD A writer/trainer for the Brazelton Touchpoints Center, Dr. Hornstein is an assistant professor in early childhood education at the University of New Hampshire. He also continues his research on emotional health in early childhood with his ongoing affiliation with the Muskie School of Social

As of 8/19/2004
Policy at the University of Southern Maine. His experience includes direct service in early intervention and statewide interagency coordination. Constance H. Keefer, MD A developmental/behavioral specialist, Dr. Keefer has served as the Director of the Early Childhood Program Clinic at Children’s Hospital and Director of Newborn Nurseries at the Brigham and Women’s Hospital in Boston. She created a pediatric residency curriculum in Primary Care Neonatology, highlighting an interactive, family-centered behavioral-physical exam of the newborn. As a senior faculty of the Brazelton Institute, she has been active in the development of a clinical adaptation of the Neonatal Behavioral Assessment Scale. She brings extensive experience in pediatric practice, clinical teaching, and cross-cultural research to her Touchpoints faculty role. She is currently studying how Touchpoints can inform pediatric residency training in developmental and behavioral pediatrics. Jayne Singer, PhD Dr. Singer is a clinical psychologist with extensive experience with children and families. She has been working at Children’s Hospital, Boston since 1988 and is an Instructor in Psychology in the Department of Psychiatry at Harvard Medical School. At Children’s Hospital, she has served in inpatient psychiatry units, trauma treatment services, outpatient and community satellite programs, and intensive developmental consultation programs. She is currently the Clinical Director of the Parent- Infant Mental Health Program in the departments of Psychiatry and General Pediatrics. Dr. Singer developed towards clinical psychology from the fields of expressive arts therapy and early childhood/special education, and leads the Early Child Care and Education Initiative of the Brazelton Touchpoints Center, where she is faculty and worked clinically with Dr. Brazelton for many years in his Early Childhood Program. She has worked in numerous therapeutic milieu settings in public and private school- based programs, most intensively for many years as a Clinical Administrator at the Manville School Therapeutic Day Program of the Judge Baker Children’s Center in Boston, MA. Edward Z. Tronick, PhD A nationally-recognized researcher and teacher on infant social-emotional development, maternal depression, infant behavioral assessment (NBAS), drug exposure and parenting, cross-cultural studies, and the relation of prematurity and brain lesions to infant and child development, Dr. Tronick is an Associate Professor of Pediatrics and Chief of the Child Development Unit at Children’s Hospital.

As of 8/19/2004
THE TOUCHPOINTSTM
MODEL OF DEVELOPMENT T. BERRY BRAZELTON, M.D., AND JOSHUA SPARROW, M.D.
Copyright 2003 T.B. Brazelton and Joshua Sparrow, All rights reserved. All parents benefit from affirmation of their child’s development and the nurturing environment they have provided for their child. Our goal as caring professionals should be to join parents as allies in the systems of care for their children. Our present systems are too often crisis-driven, deficit-oriented, and unwelcoming to parents. Many families, particularly those who have a child with special needs, are often left feeling isolated and unsupported (Bowman et al., 1994; Turnbull, Turnbull, & Blue-Banning. 1994). Our focus instead should be on developing a system where providers are reaching out for stressed parents and where parents’ ethnic, religious, and lifestyle attributes are valued. For example, rather than treating a pregnant teenager overtly or covertly as a failure, which will turn her away and mitigate our opportunity for successful interaction with her, we could accept her pregnancy, point to the potential future opportunity for her baby, and offer her our acceptance, understanding, and positively framed services. When providers can offer the necessary support and modeling for parents to understand their young child’s development and to enhance it, they can play a crucial role toward the success of the family system. For the past several years, we have been working on the Touchpoints’ model (Brazelton, Touchpoints1992, Brazelton and Sparrow, Touchpoints 3 – 6, 2001). Touchpoints are periods during the first years of life during which children’s spurts in development result in disruption in the family system. (Throughout life, there are, no doubt, similar developmental crises of disorganization and reorganization that involve not solely the individual but those he or she is intimately connected with as well.) The succession of touchpoints in a child’s development is like a map of that can be identified and anticipated by both parents and providers. Thirteen touchpoints have been noted in the first three years, beginning in pregnancy. T. BERRY BRAZELTON is Professor Emeritus of Pediatrics at Harvard Medical School and founder of the Child Development Unit at Children’s Hospital, Boston. He is past president of both the Society for Research in Child Development and the National Center for Clinical Infant Programs. A practicing pediatrician for over 45 years, he introduced the concept of ‘anticipatory guidance’ for parents into pediatric training. The author of over 200 scholarly papers, Dr. Brazelton has written 35 books, both for a professional and lay audience. JOSHUA SPARROW is Assistant Professor of Psychiatry at Harvard Medical School, Supervisor for the Child Psychiatry Department at Children’s Hospital, Boston, and Director of Special Initiatives at the Brazelton Touchpoints Center. He has co-authored six books with Dr. Brazelton.
Contact: Brazelton Touchpoints Center, Children’s Hospital, Boston, 1295 Boylston Street, Suite 320, Boston, MA 02215

As of 8/19/2004
They are centered on caregiving themes that matter to parents (e.g. feeding, discipline), rather than traditional milestones. The child’s negotiation of these touchpoints can be seen as a source of satisfaction and encouragement for the family system. Foreknowledge of these touchpoints and strategies for dealing with them can help reduce negative interactions that might otherwise throw the child’s development off course and result in problems in the areas of sleep, feeding, toilet training, among others. Touchpoints may occur somewhat later in premature infants, but they will be even more important as opportunities for supporting their anxious parents. Atypically developing children’s touchpoints may in some instances occur at different times or have different features from those of typically developing children. It is preferable to carefully observe, understand, and respect each child’s behavior for evidence of developmental disorganization and reorganization rather than to make unhelpful comparative judgments. The guiding principles of the Touchpoints model can be found in Table 1. Professionals can use these Touchpoints as a framework for each encounter with families during the first three years of a child’s life. Several guiding assumptions about parents form the core of Touchpoints’ practice with families (see Table 2). Parents are the experts on their child’s behavior. Together, professionals and parents can discover themes that recur and strategies to negotiate upcoming challenges. For example, for four-month-olds, providers can predict that there will soon be a burst in cognitive awareness of the environment. The baby will be difficult to feed. He will stop eating to look around and to listen to every stimulus in the environment. To parents’ dismay, he will begin to awaken again at night. His awareness of his surroundings will be enhanced by a burst in visual development. Yet, when parents understand the disorganization of this period as a natural precursor to the rapid and exciting development that follows, they will not need to feel as if it represents failure. From the Touchpoints framework, the guidance or ‘scaffolding’ of this sort that professionals can give parents is supportive rather than prescriptive. Anticipatory guidance is not delivery of ‘expert advice’, but a dialogue, a shared discussion about how parents will feel and react in the face of predictable challenges to come. This is, in part, based on how they have dealt with related issues in the past. Parents find it reassuring that bursts and regressions in development are to be expected. The concept of overflow from one line of development to another is often a shift in thinking for parents, who without this concept would often misunderstand their child’s behavior as pathological and question their own caregiving efficacy. In the face of their children’s behavioral regressions, they wonder what they are doing wrong. Sharing these touchpoints preventively helps parents feel more confident in themselves and in their child. Table 1. The guiding principles of the Touchpoints model
• Value and understand the relationship between you and the parent

As of 8/19/2004
• Use the behavior of the child as your language • Value passion wherever you find it • Focus on the parent-child relationship • Look for opportunities to support mastery • Recognize the beliefs and biases that you bring to the interaction • Be willing to discuss matters that go beyond your traditional role
Table 2. Touchpoints parent assumptions
• The parent is the expert on his/her child • All parents have strengths • All parents want to do well by their child • All parents have something critical to share at each developmental stage • All parents have ambivalent feelings • Parenting is a process built on trial and error
Table 3. Touchpoints practitioner assumptions
• Each practitioner is the expert within the context of his/her practice setting • Practitioners want to be competent • Practitioners need support and respect of the kind we are asking them to give to
parents • Practitioners need to reflect on their contribution to parent-provider interactions
In order to fulfill this opportunity to use the shifts in the baby’s development and the vulnerability they stir up in parents to establish and deepen their relationships with families, a provider must make a difficult paradigm shift. (Figure 1) Figure 1. A paradigm shift
As of 8/19/2004
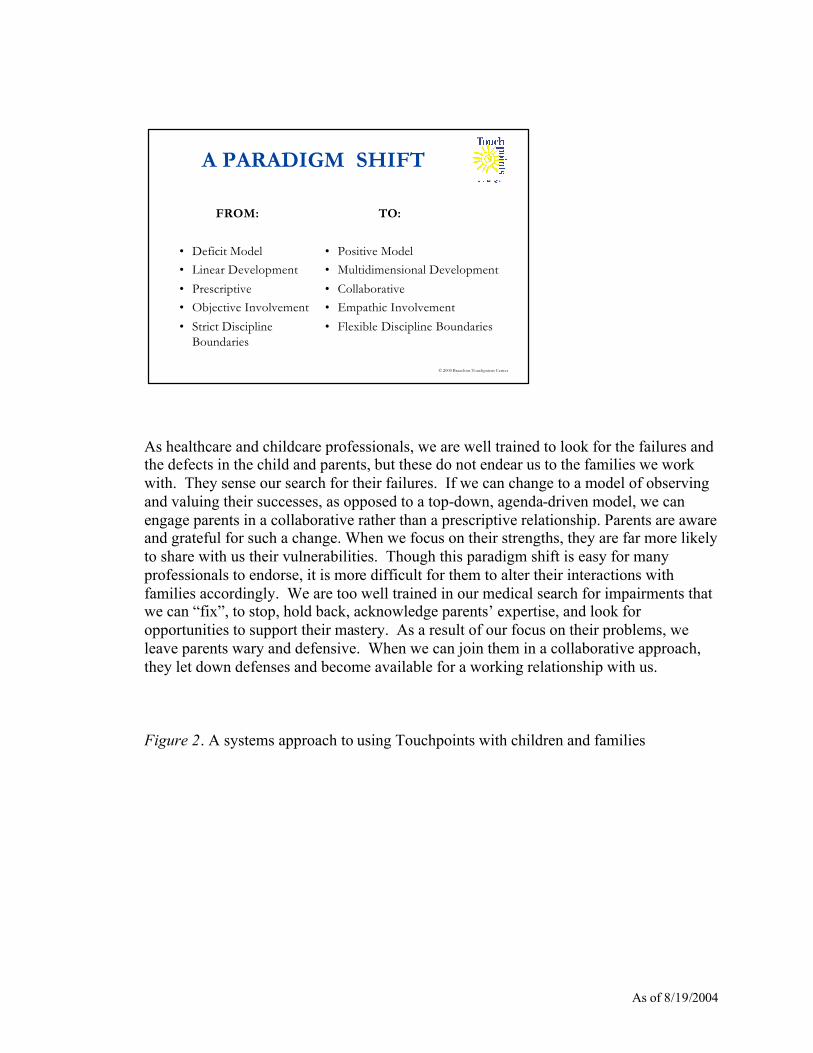
As healthcare and childcare professionals, we are well trained to look for the failures and the defects in the child and parents, but these do not endear us to the families we work with. They sense our search for their failures. If we can change to a model of observing and valuing their successes, as opposed to a top-down, agenda-driven model, we can engage parents in a collaborative rather than a prescriptive relationship. Parents are aware and grateful for such a change. When we focus on their strengths, they are far more likely to share with us their vulnerabilities. Though this paradigm shift is easy for many professionals to endorse, it is more difficult for them to alter their interactions with families accordingly. We are too well trained in our medical search for impairments that we can “fix”, to stop, hold back, acknowledge parents’ expertise, and look for opportunities to support their mastery. As a result of our focus on their problems, we leave parents wary and defensive. When we can join them in a collaborative approach, they let down defenses and become available for a working relationship with us. Figure 2. A systems approach to using Touchpoints with children and families
© 2000 Brazelton Touchpoints Center
A PARADIGM SHIFT
FROM:
• Deficit Model
• Linear Development
• Prescriptive
• Objective Involvement
• Strict DisciplineBoundaries
TO:
• Positive Model
• Multidimensional Development
• Collaborative
• Empathic Involvement
• Flexible Discipline Boundaries

As of 8/19/2004
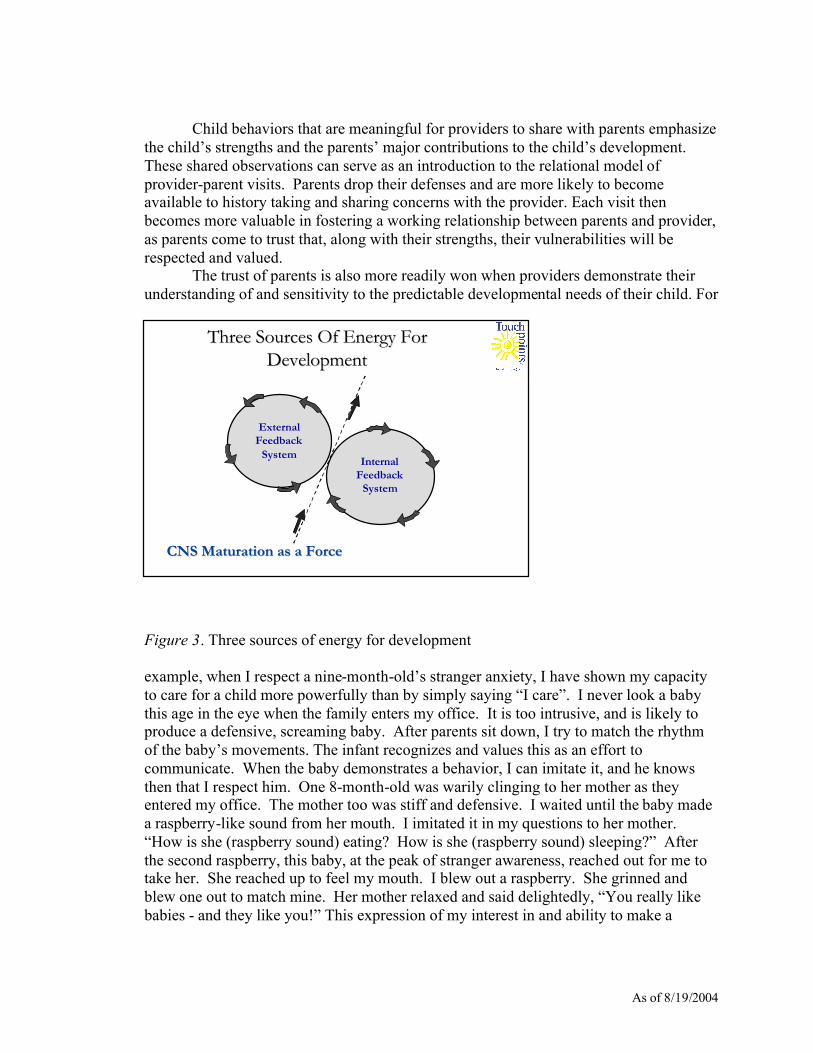
A systems model (Figure 2) is a valuable way to think of our role. Systems theory assumes that each member of the system is in balance with each other member. If there is a stress on the system, each member must adjust to the stress. As a result, stress becomes an opportunity for learning. If a provider wants the system to learn to succeed, she or he must become an equal member of the system. As a member, the professional must learn to understand and value the culture, the ethnicity, the religion, and the belief systems of the other members. Understanding a different culture is a lesson in humility, for the more we learn, the more we realize there is much that escapes us. Such a stance, which empowers the families we work with to transform us, is a far cry from the medical training of talking down to and of giving instructions to patients. In order to effect this change in our medical and childcare outreach model, we have found that we can greet a family with an initial observation of the infant or child’s behavior. Initially, the provider can observe evidence of temperament (Thomas and Chess), stage of development (Ages and Stages Social Emotional Scales), and share these behaviors with parents. Other meaningful behaviors to be shared with parents are those that offer evidence of a child’s own satisfaction in a new accomplishment. When a child strives to succeed at a developmental task, he registers his success with the behavior of, “I did it,” as the inner feedback cycle closes (Piaget). The inner feedback cycle (Figure 3), which is registered in the child’s behavior as he makes an effort to succeed, is a powerful observation to share with parents. This cycle, coupled with the parent’s efforts as represented by the external feedback cycle, fuel the expensive processes of development driven by the maturation of the Central Nervous System (CNS). Parents can be encouraged to observe these two cycles by the provider and to revel in them, if they don’t already.
© 2000 Brazelton Touchpoints Center
EXTENDED FAMILY and COMMUNITY
ClinicianMother
Father
Child
VILLAGE THAT RAISES THE CHILD
A Systems Approach to Using Touchpoints with Children and Families
As of 8/19/2004
Child behaviors that are meaningful for providers to share with parents emphasize the child’s strengths and the parents’ major contributions to the child’s development. These shared observations can serve as an introduction to the relational model of provider-parent visits. Parents drop their defenses and are more likely to become available to history taking and sharing concerns with the provider. Each visit then becomes more valuable in fostering a working relationship between parents and provider, as parents come to trust that, along with their strengths, their vulnerabilities will be respected and valued. The trust of parents is also more readily won when providers demonstrate their understanding of and sensitivity to the predictable developmental needs of their child. For
Figure 3. Three sources of energy for development example, when I respect a nine-month-old’s stranger anxiety, I have shown my capacity to care for a child more powerfully than by simply saying “I care”. I never look a baby this age in the eye when the family enters my office. It is too intrusive, and is likely to produce a defensive, screaming baby. After parents sit down, I try to match the rhythm of the baby’s movements. The infant recognizes and values this as an effort to communicate. When the baby demonstrates a behavior, I can imitate it, and he knows then that I respect him. One 8-month-old was warily clinging to her mother as they entered my office. The mother too was stiff and defensive. I waited until the baby made a raspberry-like sound from her mouth. I imitated it in my questions to her mother. “How is she (raspberry sound) eating? How is she (raspberry sound) sleeping?” After the second raspberry, this baby, at the peak of stranger awareness, reached out for me to take her. She reached up to feel my mouth. I blew out a raspberry. She grinned and blew one out to match mine. Her mother relaxed and said delightedly, “You really like babies - and they like you!” This expression of my interest in and ability to make a
CNS Maturation as a ForceCNS Maturation as a Force
Three Sources Of Energy ForThree Sources Of Energy ForDevelopmentDevelopment
ExternalFeedback
SystemInternal
FeedbackSystem
As of 8/19/2004
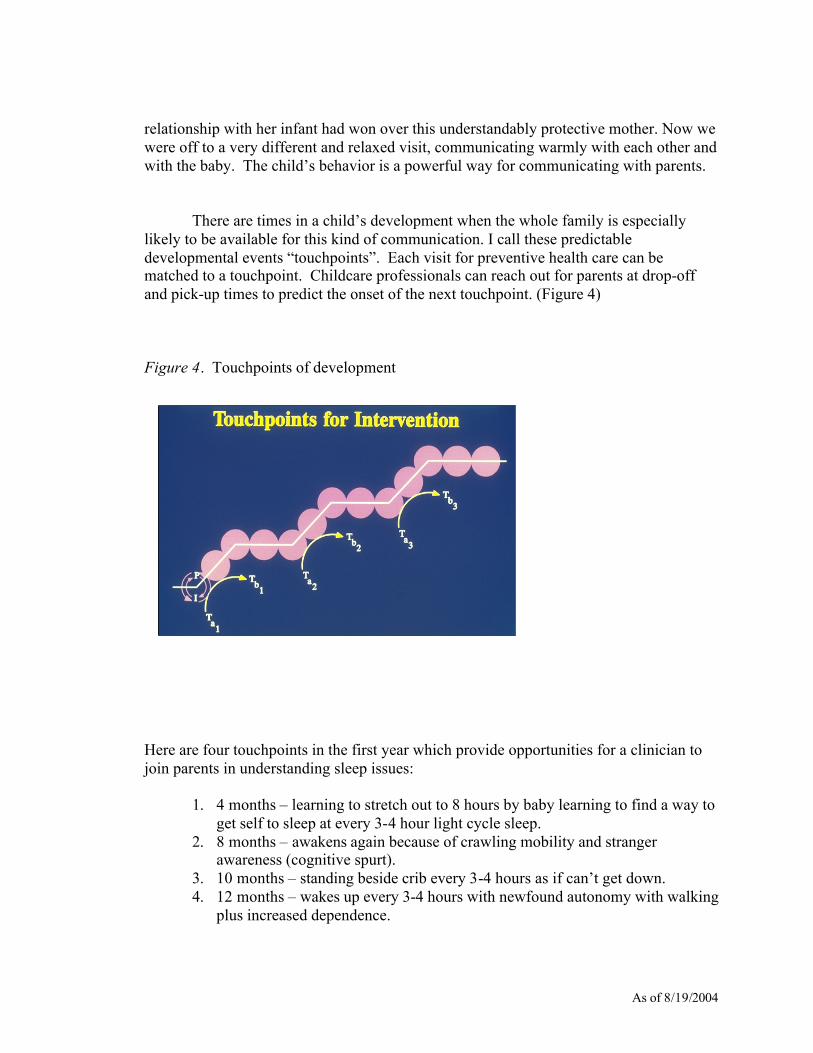
relationship with her infant had won over this understandably protective mother. Now we were off to a very different and relaxed visit, communicating warmly with each other and with the baby. The child’s behavior is a powerful way for communicating with parents. There are times in a child’s development when the whole family is especially likely to be available for this kind of communication. I call these predictable developmental events “touchpoints”. Each visit for preventive health care can be matched to a touchpoint. Childcare professionals can reach out for parents at drop-off and pick-up times to predict the onset of the next touchpoint. (Figure 4) Figure 4. Touchpoints of development
Here are four touchpoints in the first year which provide opportunities for a clinician to join parents in understanding sleep issues:
1. 4 months – learning to stretch out to 8 hours by baby learning to find a way to get self to sleep at every 3-4 hour light cycle sleep.
2. 8 months – awakens again because of crawling mobility and stranger awareness (cognitive spurt).
3. 10 months – standing beside crib every 3-4 hours as if can’t get down. 4. 12 months – wakes up every 3-4 hours with newfound autonomy with walking
plus increased dependence.
As of 8/19/2004
Here are four touchpoints for incipient eating issues:
1. Newborn – decision about breastfeeding 2. 4 months – imminent spurt in interest in environment causes split in feeding
interest. 3. 9 months – needs to feed self with finger feeding with new pincer grasp. 4. 12 months - negativism of second year and setting up necessary diet so that
independence can be settled on child. A touchpoint is an opportunity for deepening the mutual relationship between provider (medical, child care, early interventionist) and parent. Each one is dependent on the predictable stresses of a child’s developmental surges and is matched by the parent’s passionate desire to do well by the child. As providers, we are wise to become aware of each of these stresses as opportunities. As we join the parents in their urge to foster the child’s optimal development, each contact becomes rewarding to them as well as to us as providers. Figure 5. Touchpoints
These are the predictable touchpoints (Figure 5) in the first few years. We have recently identified several of these in the years 3-6 (Brazelton and Sparrow, 2001). The Touchpoints model was originally developed for the primary health-care setting. However, our model is now being utilized by professionals from other disciplines who work in a variety of settings. For example, child care, early intervention, and school all offer such opportunities. We value practitioners’ expertise and encourage them to adapt the model to their community and practice settings. The assumptions about
© 2000 Brazelton Touchpoints Center
TO
UC
HP
OIN
TS
PregnancyNewborn1 Week3 Weeks
6-8 Weeks4 Months7 Months9 Months
12 Months15 Months18 Months
2 Years3 Years

As of 8/19/2004
professionals using this model can be found in Table 3. The essence of Touchpoints training is in preventive anticipatory guidance, in its multidisciplinary approach , and its focus is on the common interest in the child that parents and providers share. Touchpoints focuses on building relationships as an integral goal of parent and practitioner interactions in diverse settings: childbirth education classes, during office and home visits, in provider-parent encounters at child-care centers and preschools, etc. Consistent understanding and application of the Touchpoints approach across the range of health, childcare, and educational settings in a community can offer families a more coherent experience of multiple services provided. As practice settings move toward greater collaboration, a shared, explicitly articulated conceptual framework can improve coordination of care. When espoused by the organization and shared by colleagues, this framework can form the basis for professional development within the work setting and the community. Only then will we be able to move beyond the current state of fragmentation of services to more effectively join families as allies with a more caring, seamless system.
As of 8/19/2004
References Bowman, P., Grady, M., Kendrick, M., Ladew-Duncan, J., Mentzer, S., Newman, R., Pease, R., Son, K., & Spandinger, L. (1994) From the heart: Stories by mothers of children with special needs. Portland, ME: University of Southern Maine. Brazelton, T. B. (1992). Touchpoints: Emotional and behavioral development . Reading. MA: Addison-Wesley. Brazelton, T.B. (1998) Soapbox: How to help parents of young children: the Touchpoints Model. Clinical Child Psychology and Psychiatry. Sage Publications (London, Thousand Oaks, and New Delhi) Vol. 3 (3): 481-483; 004738. Brazelton, T. B., Sparrow, J. D. (2001). Touchpoints: 3-6: Cambridge, MA: Perseus. Brazelton TB, Sparrow JD. Calming Your Fussy Baby the Brazelton Way. Cambridge (MA): Perseus Books; 2003 Jan. Brazelton TB, Sparrow JD. Sleep the Brazelton Way. Perseus Books; Cambridge (MA): Perseus Books; 2003 Jan. Brazelton TB, Sparrow JD. Discipline the Brazelton Way. Perseus Books; Cambridge (MA): Perseus Books; 2003 Jan. Brazelton TB, Sparrow JD. Feeding Your Child the Brazelton Way. Perseus Books; Cambridge (MA): Perseus Books; 2004 Feb Brazelton TB, Sparrow JD. Toilet Training Your Child the Brazelton Way. Perseus Books; Cambridge (MA): Perseus Books; 2004 Feb Bricker, D., Squires, J. (1994). Ages and Stages Social Emotional Scales. Baltimore, MD: Paul H. Brookes Publishing. Piaget, J. The Origins of Intelligence in the Child. London: Routledge & Kegan Paul; New York: International Universities Press. (1936, Eng. Trans. 1953). Thomas, A., Chess, S., Brick, H. G. (1968). Temperament and behavior disorders in children, New York, NY: University Press.
As of 8/19/2004
Touchpoints Individual Level Training ***Members of site training teams will have completed either Individual Level Training, Early Child Care and Education Training, or Touchpoints training delivered by a Touchpoints site training team.
The three-day symposium is designed for individual healthcare, childcare, early education, and social service providers who want to incorporate elements of the Touchpoints Model into their practice setting. The Touchpoints Model helps professionals engage around key points in the development of young children. By helping parents identify and expect bursts and regressions in child behavior (the "touchpoints") professionals can reduce parental frustration and self-doubt while fostering parenting skills and the parents enjoyment of their child. In the process, the bond between the provider and the family is strengthened. The symposium gives participants a solid understanding of all Touchpoints elements through seminars with BTC faculty, regional site faculty, and practitioners who have been trained in the model. Participants will: • understand the theories and concepts of the Touchpoints Model, with emphasis on
the developmental and relational elements of parent-child-provider relationships, and their clinical applications;
• enhance their delivery of care to families by using relationship-building strategies and
communication tools based on the Touchpoints Model; • observe and participate in encounters that demonstrate the Touchpoints Model of
anticipatory guidance. The symposium is offered several times a year at both Brazelton Touchpoints Center, in Boston, and at Regional Training Sites across the Country. The symposium costs $1,200, and attendance is limited to 20 participants. Continuing Medical Education (CME) and Continuing Education Units (CEUs) are available. Please contact BTC for more information.
As of 8/19/2004
TOUCHPOINTS COMMUNITY LEVEL TRAINING
A five-day intensive Touchpoints training is offered to communities that want to bring Touchpoints to their family care system. Three providers from each community receive Touchpoints training in Boston and one year of ongoing mentorship that includes monthly contact, a site visit and a reunion meeting. As a team, these providers train other professionals in their community in the Touchpoints Model, with the support of BTC faculty. The Touchpoints Model helps professionals engage around key points in the development of young children. Helping parents identify and expect bursts and regressions in child behavior (the "touchpoints") can reduce parental frustration and self-doubt while fostering their parenting and enjoyment of their child. In the process, the bond between the healthcare provider and the family is strengthened. Participants will: • focus on cultivating the practitioner-parent relationship over time, and understanding
the effect of diversity and personal biases on clinical practice with families; • learn clinical applications of the Touchpoints Model by using facilitated role play,
video and live interactions; • return to their community and train other providers in the Touchpoints Model, with
mentorship from BTC faculty; • become part of a network of Touchpoints communities around the country who are
altering their paradigm of care for families. The train-the-trainer model is offered twice a year in Boston. Space is limited to five sites per training session. Continuing Medical Education (CME) and Continuing Education Units (CEUs) are available. The training fee is $25,000 and includes training costs for three people, curriculum materials, and consultation services one year following training (including a site visit and evaluation consultation). Sites should budget additional funds for travel and accommodations. Please allow approximately six months of preparation time, as the process requires submission of a proposal for BTC committee approval (see ‘Request for Proposal and Application Guidelines’ at the end of this booklet). Please contact BTC for more information.

As of 8/19/2004
TOUCHPOINTS FACULTY LEVEL TRAINING
The three-day symposium is designed for individual healthcare, child care, early education, and social service providers who are joining an existing Touchpoints training team. The training helps professionals incorporate elements of the Touchpoints Model into their setting. The Touchpoints Model helps professionals engage around key points in the development of young children. By helping parents identify and expect bursts and regressions in child behavior (the "touchpoints") professionals can reduce parental frustration and self-doubt while fostering parenting skills and the parents enjoyment of their child. In the process, the bond between the provider and the family is strengthened. The symposium gives participants a solid understanding of all Touchpoints elements through seminars with BTC faculty, regional site faculty, and practitioners who have been trained in the model. In addition, it prepares the participant to join their sponsoring training team. Participants must have attended a training in their community or and Individual Level Training (ILT) at one of the three National ILT Sites. Participation in a Faculty Level Training must be requested and supported by a training team. Participants will: • understand the theories and concepts of the Touchpoints Model, with emphasis on
the developmental and relational elements of parent-child-provider relationships, and their clinical applications;
• focus on the delivery of care to families by using relationship-building strategies and
communication tools based on the Touchpoints Model; • observe and participate in encounters that demonstrate the Touchpoints Model of
anticipatory guidance; • practice training techniques and develop implementation strategies and plans. The symposium is offered several times a year at Brazelton Touchpoints Center in Boston; the fee for training is $1,000, and attendance is limited to 20 participants. Continuing Medical Education (CME) and Continuing Education Units (CEUs) are available. Please contact BTC for more information.

As of 8/19/2004
TOUCHPOINTS COMMUNITY LEVEL TRAINING REQUEST FOR PROPOSAL & APPLICATION GUIDELINES
BRAZELTON TOUCHPOINTS CENTER CHILDREN’S HOSPITAL BOSTON
As of 8/19/2004
I. THE PROGRAM A. Site Composition We are seeking to identify sites nationwide which together will represent a breadth of practice settings and which serve families of diverse cultural, economic and life circumstances. All sites should: • focus particularly on families with children aged zero to five; • have a multidisciplinary faculty that emphasizes a team approach; • commit to a full-year involvement and collaboration with BTC and; • have some access to existing summary data on their service populations (e.g.,
demographic information, monitoring of health care visits to providers). Each site will send three or four key professionals to a week-long, intensive training session at Brazelton Touchpoints Center (“BTC”) in Boston. These professionals should be identified by the sites, in collaboration with BTC staff, according to the following criteria. The team of professionals should: • include a combination of healthcare, child care, education and social service
professionals; • have a minimum of five years experience working with diverse families of infants
and young children; • have supervisory experience with other providers; • have strong organizational and communication skills; • have training expertise. These Touchpoints professionals will implement the Model into their own practice and will train others over the course of the year. At the conclusion of the year, they will return for the Annual Networking Conference, which begins with two days of reunion activities specific to new sites. B. Training The Five-Day Seminar The primary objective of the week-long training experience in Boston will be to introduce professionals to the Touchpoints Model. In addition to furthering the knowledge base and communication skills of participants, a major goal of this week will be to engage the individual practitioner in a process of self-reflection and personal awareness. It is expected that the interdisciplinary nature of the group will provide a variety of perspectives and shared experiences.
As of 8/19/2004
Trainees will engage in experiential learning. A hands-on approach to learning will emphasize role-playing, workshops, and problem-solving groups, which will highlight the interplay of early child development knowledge and relationship-building skills. Particular attention will be given to the voices of parents and professionals, and to the support that is needed (internally and externally) to promote alliances between them. Additionally, emphasis will be placed on
training others at their site in the Touchpoints Model as well as implementing the Model into their defined community.
Interdisciplinary Collaboration
A common concern of child/family professionals is a sense of isolation due to unsatisfactory collaboration with professionals in other disciplines and settings who may be serving the same families. The Touchpoints Model recognizes the validity of this issue and has designed both its training and implementation phases to address it. Not only will the participants who receive training have diverse experiences, but also the Touchpoints facilitators, the content of vignettes, and case examples in training materials will be similarly diverse.
Materials
During the training process, trainees will receive both written and audiovisual resources specifically developed for BTC as well as guidance in their optimal use. Participants will be given a Training Manual that orients them to the philosophy, goals, assumptions, and basic applications of the Touchpoints Model. The Training Manual will also contain information on child development and on communication processes to help professionals build alliances with parents of infants and toddlers around each touchpoint.
Ongoing Mentorship/Support The importance of follow-up, support and consultation cannot be overstated. The Touchpoints Model acknowledges the primacy of these needs and has structured the implementation phase accordingly. It is difficult, however, to anticipate the precise level of support needed by the site or individual provider. Thus, the consultative relationship between Touchpoints staff and site members will reflect this reality and will vary according to the unique demands of implementing the Model in such diverse settings. Monthly telephone contact with the sites, fax and electronic mail communication, a site visit from Touchpoints staff, and "on-call" availability to deal with specific questions will assure an open line of communication. All follow-up activities will be coordinated with the existing supervisory structure at each site.
As of 8/19/2004
C. Implementation This phase of the program commences upon the trainees’ return to their sites following their week at BTC in Boston. Professionals will apply to their daily practice their expanded knowledge and skills, fitting the Touchpoints Model to the needs of their particular roles and disciplines. To ensure a close working relationship with the sites, Boston staff will be in monthly contact by telephone with the site coordinator. Ongoing consultation will allow Touchpoints staff to address concerns specific to individual providers or sites. On a monthly basis, Touchpoints trainees at each site will meet to monitor their experiences implementing the Model. These meetings are a critical component of implementation from several standpoints. For professionals, they represent an opportunity to renew their connections with their colleagues involved in the Touchpoints program, to discuss how the Touchpoints Model has affected their interaction with families, and to compare and support one another’s experiences. From the perspective of Touchpoints staff, these meetings will provide feedback and thereby enable BTC to give appropriate support and consultation. Additionally, Touchpoints staff will make one site visit within the contract year. Depending on the needs of each site, the focus of this visit may emphasize support, additional training, or trouble-shooting. This visit will provide a chance for Touchpoints participants to inform Boston staff directly about their experiences implementing the Model. It will also be an opportunity for Touchpoints staff to meet with individuals instrumental to the Model's implementation. The year-long implementation phase will culminate in a final 2 day reunion meeting in conjunction with the Touchpoints Annual Meeting. These events will enable sites to review their own experiences with Touchpoints staff and one another and to receive further guidance in training others to implement the Model. D. Evaluation BTC is engaged in a comprehensive evaluation program to assess the impact of Touchpoints training on professionals as well as the families and communities they interact with. As such, each site is asked to participate in this ongoing national effort. BTC has contracted with an independent evaluator to consult with sites on the overall evaluation plan and to offer sites specific guidance relevant to their particular goals and service settings. Moreover, as part of the National Network (see “National Network” below), sites will have access to a wide variety of assessment materials already in use throughout the country.
As of 8/19/2004
E. The National Network A commitment to multidisciplinary involvement at all levels permeates the program. After training in Boston, each trained site becomes a member of the Touchpoints National Network, which consists of twenty-five trained sites nationwide. Through the quarterly newsletter, the website and the Annual National Networking Conference, sites and site-members are able to share information and resources, offer advice and support, and collaborate on the use and implementation of the Touchpoints Model.
II. SITE RESPONSIBILITIES A. Team Selection and Support In addition to identifying professionals who meet the criteria outlined on page 1, ample support must be in place in order for the professionals to meet the following obligations:
• provide baseline information via interviews/assessments; • attend the initial week-long Touchpoints training; • fulfill evaluation tasks throughout the Project, including weekly completion of
measures; • attend the monthly practitioner meetings on-site; • attend a two-day follow-up session at the end of the implementation year; • train other providers in the Touchpoints Model in their community; • provide any new materials/documents to BTC with the understanding findings
will be shared with other Touchpoints sites; • generate the necessary funds (see below). B. Funding Site costs for participation in the Touchpoints program are currently estimated at $25,000 per site, plus travel for team members (Training + Reunion = two trips per year). This fee will defray the costs of staff training; materials, including a Practitioner's Guide and Manual, audiovisual and other resources; travel for Touchpoints staff for site visits; and Touchpoints staff time devoted to ongoing site consultation, reference and referral services. Sites will be expected to cover the costs of their own travel to Boston and accommodations in Boston. Additional costs from Boston (programmatic/administrative) will be leveraged through fundraising by Touchpoints staff.
As of 8/19/2004
C. Proposal Requirements Interested sites, which meet the selection criteria, should submit a proposal (no more than 10 double-spaced pages), which addresses all of the following categories: Goals/Need Agency Seeks to Address: Describe goals, needs or improvement in child development outcomes agency seeks to address through the integration of the Touchpoints Approach. How would the Touchpoints Approach change or enhance current service delivery, client satisfaction, employee job satisfaction, etc.? Area of Impact/Service population: Describe your client population including number served, demographics - socioeconomic status, family composition, language culture, and geographic area from which client population is drawn. Identify the predominant language spoken by these families and whether particular types of families with children age 0-6 are predominantly served (i.e., single parents, substance-abusing parents). What is the level of contact (daily, weekly, monthly) with families, and what is the rate of involvement of fathers vs. mothers vs. both parents? What kind of summary information (e.g., demographics, contact with health care system) is available on the service population, which could be accessed for the evaluation phase of the Touchpoints Program? Selection of Training Team Members: Describe how you will select members of your training team. Include roles, responsibilities and decision making authority within your organization, as well as previous training and supervisory experience. Agency/Program description: Including its goals and objectives, services rendered, which involve children, aged 0-6, and linkages/affiliations, formal and informal, with other area institutions and agencies – specifically other systems of care serving the same population of children and families served by your organization. Are there any on-site preventive or intervention programs already in place for this population? Please note if your organization’s primary focus is on the child, the parent, the family unit, or other. Staff composition: Include size of staff, disciplines represented, and range of child development background/training. Identify key stakeholders and decision makers. Note the involvement of paraprofessionals, volunteers, students or parents in delivery of services. Comment on expected level of staff turnover during a two-year period. Attach brief (one
As of 8/19/2004
paragraph) biographical outline for each potential Touchpoints training team participant, noting discipline, years of experience, and area of specialty or professional expertise. Staff training: What opportunities for professional development are offered? Describe the form and content of this training (i.e., in-service workshops, attendance at regional conferences). Location: Describe the site's geographical location – i.e., inner city, rural, suburban. Assessment information: Note whether/how service delivery is formally assessed and whether this data would be available to BTC staff. In particular, is client satisfaction with services measured? If so, how is it obtained (e.g., is it assessed on a regular, formal basis or in a more informal way)? Funding information: As evidence of financial solvency, describe funding sources for the site, with specific attention to the expected source of funding for Touchpoints involvement. Summary statement: Conclude with a brief statement on the organizations interest in becoming involved with BTC. Collaboration on any other demonstration or evaluation project should be noted. Additionally, the following points are of particular interest: • What unique contribution can this site make to the Project? • Can the site commit to both the implementation and evaluation components of the
project? Such involvement will include site members' completion of baseline and periodic survey instruments.
Proposals should be received four months prior to training. Send proposal to: Ann C. Stadtler, Director Site Development and Support Brazelton Touchpoints Center Children's Hospital Boston 1295 Boylston Street, Suite 320 Boston, MA 02215 ** Additional materials may be requested following receipt of proposals. ** We encourage you to call Ann Stadtler at the Touchpoints office at (617) 355-7601 with any questions or clarification regarding proposal
submissions.
As of 8/19/2004
FUNDING SOURCES FOR TOUCHPOINTS SITES
1996 United Way Junior League Earle Foundation
Greenville, SC
Deloitte & Touche Gasser Foundation Wine Auction Local hospital
Napa ,CA
Baby TALK Decatur, IL Peninsula Community Foundation San Mateo, CA 1997 Mid-Columbia Medical Center
The Dalles, OR
University of Texas at Austin Austin, TX Grand Haven Area Community Foundation Grand Haven Rotary Club Tri-cities Area United Fund City of Grand Haven Christ Community Church Unified Ministry Fund North Ottawa Community Hospital
Grand Haven, MI
Department of Health & Human Services U.S. Public Health Service Division of Fiscal Services Mailman Foundation
Gallup, NM
S.C. Johnson Wax Fund, Inc. Racine, WI 1998
Kellogg Foundation
Muskegon, MI
As of 8/19/2004
Muskegon Health Project Muskegon Foundation George Washington University Health Plan Washington, DC N/A Merrimack Valley, MA Procter & Gamble, Co. Baby's Milk Fund Pediatric Care
Cincinnati, OH
1999 Initiatives for Children DePelchin Children’s Center Women’s Hospital of Texas HANDS – Houston Area Network for Dependent Services
Houston, TX
The Grayce B. Kerr Fund, Inc. Easton, MD Francis Child Development Institute Junior College District of Kansas City Children’s Mercy Hospital University of Kansas Medical Center
Kansas City, MO
Ounce of Prevention Fund United Way IL Department of Human Services IL Department of Children & Family Services
Rockford, IL
N/A Haverhill, MA Brazelton Foundation Waterbury, CT 2000 SAS Corporation
Cary, NC
Sherman Hospital Provena St. Joseph’s Hospital Well-Child Center Kane County Health Department Summit School
Elgin, IL
As of 8/19/2004
State Department of Developmental Services
Los Angeles, CA
Bright Horizons Princeton, NJ NC General Assembly Wake County, NC 2001 New York State Department Office of Family and Children Services United Way Private Foundations
Port Chester, NY
California Proposition 10 Pacific Bell Telephone
Colton, CA
The Robin Hood Foundation Harlem Children’s Zone, NYC N/A United Planning Organization
Washington, DC Head Start, Early Head Start and Child Care Early Head Start Fatherhood Demonstration Project grant
Red Cliff Early Childhood Center Red Cliff, WI
National Academy for State Health Policy Commonwealth Fund
Vermont
Community Medical Center Keystone College
Scranton, PA
Butler County Early Start/Temporary Assistance to Needy Families Family and Children First Council
Butler County, OH
N/A Harlem Hospital, NYC United Way of Wyoming Valley Success By Six Luzerne County Children and Youth Services
Wilkes-Barre, PA

As of 8/19/2004
2002 MJ and Alice S. Neeley Foundation Work Advantage Board Ft. Worth Public Health Department United Way Success by Six Partnership for Children
Ft. Worth/Tarrant County, TX
F-CA/N Michigan Foster and Adoptive Parent Association
MI Family Independence Agency
Shared effort from all agencies: The Child Care Association of Brevard County, Inc. The Brevard County Department of Health Holmes Regional Medical Center Health Families United Way of Brevard The Brevard County School Board Brevard Community College Parrish Children’s Center Success By Six
CCA of Brevard County, FL
Individual donations United Way City of Rapid City, SD Pennington County SD Department of Health US Department of Health and Human Services US Department of Agriculture National Science Foundation The Bush Foundation of St. Paul (Minnesota) The John T. Vucurevich Foundation
Youth & Family Services Rapid City, SD
PCAI Ball State University Lilly Endowment Dunebrooke
Prevent Child Abuse Indiana Indianapolis, IN
Department of Human Services, Division of Child Care and Child Guidance Service Oklahoma State Department of Health
Stillwater, OK
As of 8/19/2004
2003 Head Start Grant
Puelbo of Laugna, NM Rocky Boy’s Chippewa Cree, MT
Confederated Salish & Kootenai Tribes, MT
Blackfeet Tribe, MT Port Gamble S’Kallam Tribe, WA
Prairie Band of Potawatomi Nation, KS Suquamish Tribe, WA
Grant from White Earth Tribal Council White Earth Band of Ojibwa Tribe Parents Are Teachers Too Early Head Start Program
Penquis Community Action Plan, ME
George S. and Dolores Dore Eccles Foundation In-Kind Support from University
Utah State University Hope Institute

As of 8/19/2004