targeted deprescribing in patients on hemodialysis to ... 03, 2017 · patterson et al. cochrane...
TRANSCRIPT

TargetedDeprescribinginPatientsonHemodialysistoDecrease
Polypharmacy

Presentation Objectives • Discuss Polypharmacy In HD patients• Define Deprescribing• Review results of the pilot study on
deprescribing in our HD unit• Discuss the goals of the CanSolve Study
on Deprescribing.
Background• Polypharmacymeans“manydrugs”- 5ormoredrugs
• Polypharmacyalsomeansinappropriatechoicesofmedicationsordoses
• HDptstakeanaverageof15medications/day
Pattersonetal.CochraneDatabaseSysRev2012;ManleyetalNDT2004

Deprescribing• “Theprocessoftapering,stopping,discontinuing,orwithdrawingdrugs,withthegoalofmanagingpolypharmacyandimprovingoutcomes”
• Associatedwithfewerreferralstolong-termcarefacilities,lowerdrugcosts,decreasedmortality
• Improvementsinpatient’sperceptionoftheirglobalhealth.
ThompsonandFarrellCanJHospPharm. (2013); 66(3):201–202

WhyDeprescribinginHemodialysis?• Hemodialysispatientshavehighpillburden
• Evidenceforefficacyofmanytherapiesislackinginhemodialysispopulation
• Safetyconcernsformedicationsthatareclearedbythekidneyandnotremovedbyhemodialysis
• Notoolsfordeprescribing availableforthispopulation
Chiuetal. ClinJAmSocNephrol.(2009);4(6):1089-96

Targeted Deprescribing in an Outpatient Hemodialysis Unit to
Decrease Polypharmacy:A Pilot Study

Objectives1. To develop deprescribing algorithms for target
medications that have poor evidence for efficacy and safety in the HD population
2. To determine the effectiveness of these algorithms in decreasing polypharmacy when incorporated into current practice in the HD unit
3. To monitor patient safety and satisfaction throughout this initiative

MethodsPhase1:DevelopmentofDeprescribing Tool• Literaturesearchperformed• Focusgroupswereconducted• Reviewed50chartstoassesshowcommontheselectedmedicationswereused
• Fivetargetmedicationswereselectedbasedonpoorevidenceforpatientsafetyandlackofevidenceforefficacy

FiveTargetedMedications• Diuretics• PPIs• Quinine• Alpha-blockers• Statins**
Medicationspecificalgorithmsweredeveloped

MethodsPhase2:ValidationofDeprescribing Tool• FaceandcontentvaliditywasassessedthroughthreerepetitivecycleswiththeNephrologistsandPharmacists
.

Methods
Phase3:ImplementationandEvaluationofDeprescribing Tool• ProspectiveObservationalPilotStudy• PatientsreceivingHDatTorontoGeneralHospitalbetweenMay2014andMarch2015wereincluded

Methods-Phase3ImplementationCollectBPMH,IdentifyTargetMedication,ApplyAlgorithm,InformTeam,ConsentPatient
Communicatewithpatienttheplan,monitorasperalgorithm
Followup6monthslater
BPMH-Best Possible Medication History

MethodsPhase3:EvaluationofDeprescribingAlgorithm• Primaryendpoint:
– proportionoftargetmedicationssuccessfullydeprescribed
• Secondaryendpoints:–Averagenumberofmedicationsperpatientbeforeandaftertheintervention
–Proportionofsuccessfuldeprescribingtrialsforeachtargetmedication
–Patientsafetyandsatisfaction
RESULTS
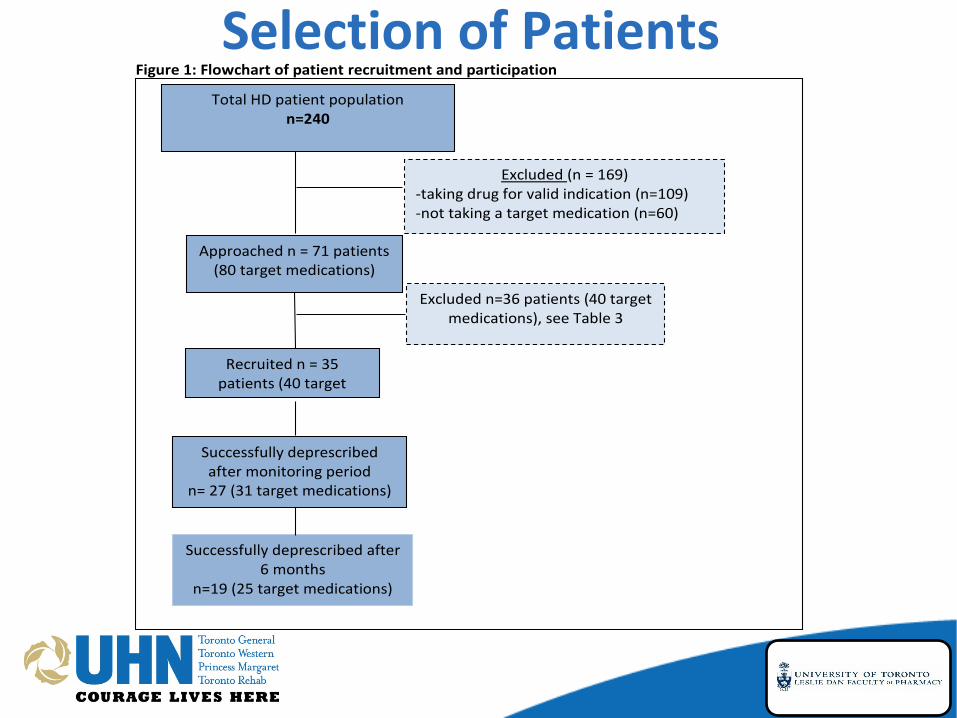
SelectionofPatientsFigure1:Flowchartofpatientrecruitmentandparticipation
TotalHDpatientpopulationn=240
Excluded(n=169)-takingdrugforvalidindication(n=109)-nottakingatargetmedication(n=60)-
Excludedn=36patients(40targetmedications),seeTable3
Approachedn=71patients(80targetmedications)
Recruitedn=35patients(40target
medications)
Successfullydeprescribedaftermonitoringperiod
n=27(31targetmedications)
Successfullydeprescribedafter6months
n=19(25targetmedications)

BaselineCharacteristics
Characteristic Total(n=35)Age(y)Mean+SD(Range)
65+16.5(33-92)
Gender 21males,14femalesDialysisVintage(months)Median
40(23.2,57.2)
TotalNumberofMedicationsMean+SD(Range)
13.4+4.3
ComorbiditiesHypertension 31DiabetesMellitus 21CardioVascularDisease 21
Table1:BaselineCharacteristics

Results- Endpoints• Primaryendpoint:
– 31/40(77%)medicationsweresuccessfullydeprescribed.
• Secondaryendpoints:– Theaveragenumberofmedicationsperdaydecreasedfrom13.4± 4.3to12.7± 4.4(n=35)afterthedeprescribingtrial.
– Patientsafetyandsatisfaction

Discussion• Validateandimplementasafeandpracticaltooltodeprescribe5classesofdrugsforHDpatients
• Helpedguideclinicalpractice• Increasedawarenessofinappropriatemedicationuse
Limitations• Singlecenter• Patientmaycontinuetousemedicationathome
• Anewmedicationmaybeprescribedduringdeprescribingtrial
• Didnotfollowlongtermclinicaloutcomes

Conclusion• Feasibletoincorporatethisdeprescribingtoolinroutinepracticewithoutaddedcosts– Inroutinepractice,weperformBPMHinallpatientsandwemonitoredtheparametersthatwerepartofthedeprescribing algorithm
• Increasedpatientsafety• FutureStudies- implementasaRCTinmorecentresacrossCanada
CanSolveOverallGoal• To improve current clinical practice by
decreasing polypharmacy in the HD units across Canada.
• This will be achieved by developing deprescribing algorithms for medications that lack evidence for efficacy and safety in the HD population using a systematic national, evidence-informed consensus building process

CanSolve Objectives1.To assess and compare demographic and
medication use patterns in HD patients acrossCanada.
2.To develop new deprescribing algorithms andbuild upon current deprescribing algorithms forHD patients.
3.To establish consensus driven medicationdeprescribing algorithms that will beimplemented and evaluated in clinical practicein HD units across Canada.
CanSolve Objectives1.To assess and compare demographic and
medication use patterns in HD patients acrossCanada.
2.To develop new deprescribing algorithms andbuild upon current deprescribing algorithms forHD patients.
3.To establish consensus driven medicationdeprescribing algorithms that will beimplemented and evaluated in clinical practicein HD units across Canada.
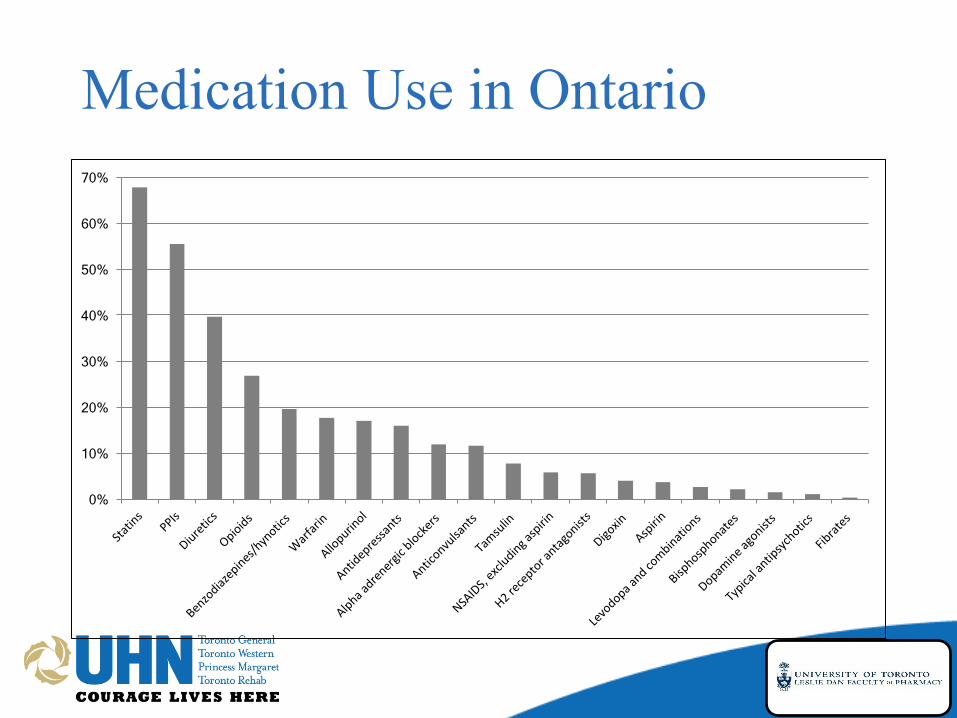
Medication Use in Ontario
0%
10%
20%
30%
40%
50%
60%
70%

CanSolve Objectives1.To assess and compare demographic and
medication use patterns in HD patients acrossCanada.
2.To develop new deprescribing algorithms andbuild upon current deprescribing algorithms forHD patients.
3.To establish consensus driven medicationdeprescribing algorithms that will beimplemented and evaluated in clinical practicein HD units across Canada.

Digitalpolloftop12drugstode-prescribe1.PPI2.Allopurinol3.Quinine4.Diuretics5.Alphablockers6.Benzodiazepines/hypnnotics7.Statins8.Anticonvulsants- gabapentin/pregablin9.Prokinetics- metoclopramide/domperidone10.TCAs(antidepressants)11.Warfarin12.Opioids

Algorithm Development1.PPI2.Allopurinol3.Quinine4.Diuretics5.Alphablockers6.Benzodiazepines/hypnnotics7.Statins8.Anticonvulsants- gabapentin/pregablin9.Prokinetics- metoclopramide/domperidone
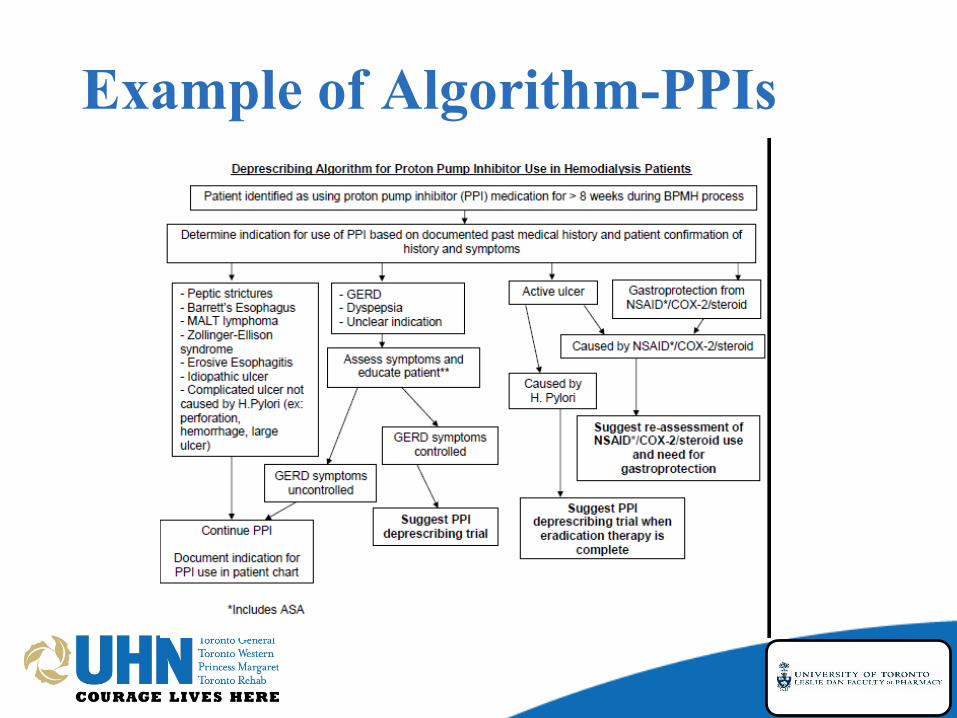
Example of Algorithm-PPIs



Objectives1.To assess and compare demographic and
medication use patterns in HD patients acrossCanada.
2.To develop new deprescribing algorithms andbuild upon current deprescribing algorithms forHD patients.
3.To establish consensus driven medicationdeprescribing algorithms that will beimplemented and evaluated in clinical practicein HD units across Canada.
Discussion/ Questions