tecnologia e nuove competenze a supporto del … fimeuc 2017.pdf · tecnologia e nuove competenze a...
TRANSCRIPT

Tecnologia e nuove competenze a supporto del cambiamento
Dott Enrico MirantePronto Soccorso e Medicina drsquoUrgenzaOspedale SantrsquoEugenio Roma
ldquoIl medico drsquoEmergenza-Urgenza deve possedere conoscenze teoriche
scientifiche e professionali nei campi della metodologia clinica del primo
inquadramento diagnostico e del primo trattamento delle urgenze mediche
chirurgiche e traumatologiche [hellip]rdquo
Valutare rianimare e stabilizzare il paziente in fase intra ed extra-
ospedaliera
Inquadrare dal punto di vista diagnostico e attuare il trattamento di tutti i
pazienti inclusi i pazienti pediatrici geriatrici ed in gravidanza che
arrivano in Pronto Soccorso con diversi sintomi e bisogni in base a criteri di
prioritagrave
Arresto cardiaco
Ritmo Defibrillabile (FV)
Copyright copy2005 Canadian Medical Association or its licensors
Rivers E P et al CMAJ 20051731054-1065
Fig 5 Treatment options in sepsis
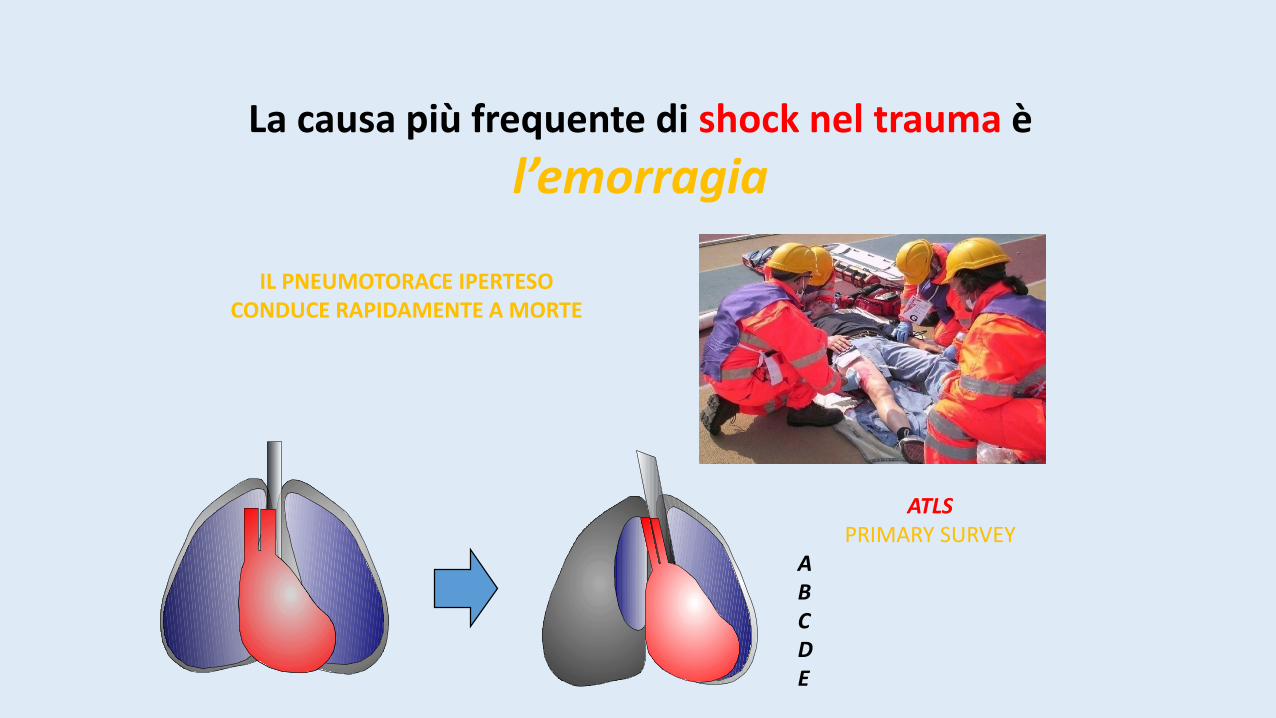
La causa piugrave frequente di shock nel trauma egrave
lrsquoemorragia
IL PNEUMOTORACE IPERTESO CONDUCE RAPIDAMENTE A MORTE
ATLSPRIMARY SURVEY
ABCDE
1
AGIRE PER PRIORITArsquo
A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

ldquoIl medico drsquoEmergenza-Urgenza deve possedere conoscenze teoriche
scientifiche e professionali nei campi della metodologia clinica del primo
inquadramento diagnostico e del primo trattamento delle urgenze mediche
chirurgiche e traumatologiche [hellip]rdquo
Valutare rianimare e stabilizzare il paziente in fase intra ed extra-
ospedaliera
Inquadrare dal punto di vista diagnostico e attuare il trattamento di tutti i
pazienti inclusi i pazienti pediatrici geriatrici ed in gravidanza che
arrivano in Pronto Soccorso con diversi sintomi e bisogni in base a criteri di
prioritagrave
Arresto cardiaco
Ritmo Defibrillabile (FV)
Copyright copy2005 Canadian Medical Association or its licensors
Rivers E P et al CMAJ 20051731054-1065
Fig 5 Treatment options in sepsis
La causa piugrave frequente di shock nel trauma egrave
lrsquoemorragia
IL PNEUMOTORACE IPERTESO CONDUCE RAPIDAMENTE A MORTE
ATLSPRIMARY SURVEY
ABCDE
1
AGIRE PER PRIORITArsquo
A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Arresto cardiaco
Ritmo Defibrillabile (FV)
Copyright copy2005 Canadian Medical Association or its licensors
Rivers E P et al CMAJ 20051731054-1065
Fig 5 Treatment options in sepsis
La causa piugrave frequente di shock nel trauma egrave
lrsquoemorragia
IL PNEUMOTORACE IPERTESO CONDUCE RAPIDAMENTE A MORTE
ATLSPRIMARY SURVEY
ABCDE
1
AGIRE PER PRIORITArsquo
A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Copyright copy2005 Canadian Medical Association or its licensors
Rivers E P et al CMAJ 20051731054-1065
Fig 5 Treatment options in sepsis
La causa piugrave frequente di shock nel trauma egrave
lrsquoemorragia
IL PNEUMOTORACE IPERTESO CONDUCE RAPIDAMENTE A MORTE
ATLSPRIMARY SURVEY
ABCDE
1
AGIRE PER PRIORITArsquo
A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
La causa piugrave frequente di shock nel trauma egrave
lrsquoemorragia
IL PNEUMOTORACE IPERTESO CONDUCE RAPIDAMENTE A MORTE
ATLSPRIMARY SURVEY
ABCDE
1
AGIRE PER PRIORITArsquo
A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
1
AGIRE PER PRIORITArsquo
A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

A B C D E
ROSSOGIALLOVERDEBIANCO
PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

PROCEDURE SALVAVITA
Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Lrsquointubazione deve essere preceduta da pre-ossigenazione
Anche se lrsquointubazione presenta vantaggilrsquoobiettivo non egrave lrsquointubazione ma
bull il mantenimento della pervietagrave delle vie aeree
bull la ossigenazione
Non ostinarsi in ripetuti tentativi di intubazione
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
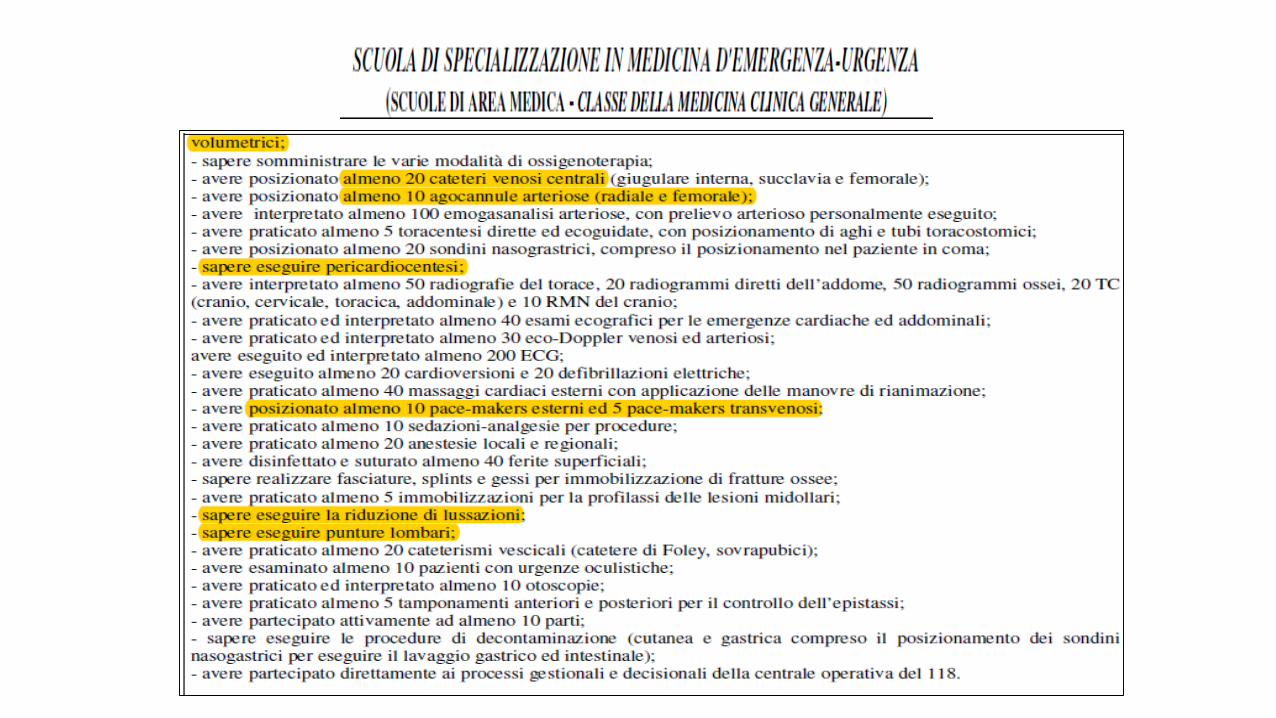
Ventilazione con pallone autoespansibile e maschera
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
Saper essere invasivihellip
bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

bull PVC e ScvO2
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
Cosa serve per lrsquoinserzione di un CVC
LA STERILITArsquo
Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Ecografia
Tamponamento cardiaco
Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Emergency echocardiography
bull Subcostal or apical four chamber scan
bull The global ventricular function can be qualitatively assessed by visual ispectionalone (eye balling)
bull Evaluating whether cardiac function is normally moderately or severely impairedis sufficient in most cases
Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Rimozione di 5-10ml liquido pericardico
Aumento dello stroke volume 25-50
Tamponamento cardiaco
Rottura di atrio segni e sintomi di Tamponamento cardiaco si manifestano lentamenteECO FAST DI CONTROLLO
FAST DIAGNOSI + TRATTAMENTO (ECO + PERICARDIOCENTESI)
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
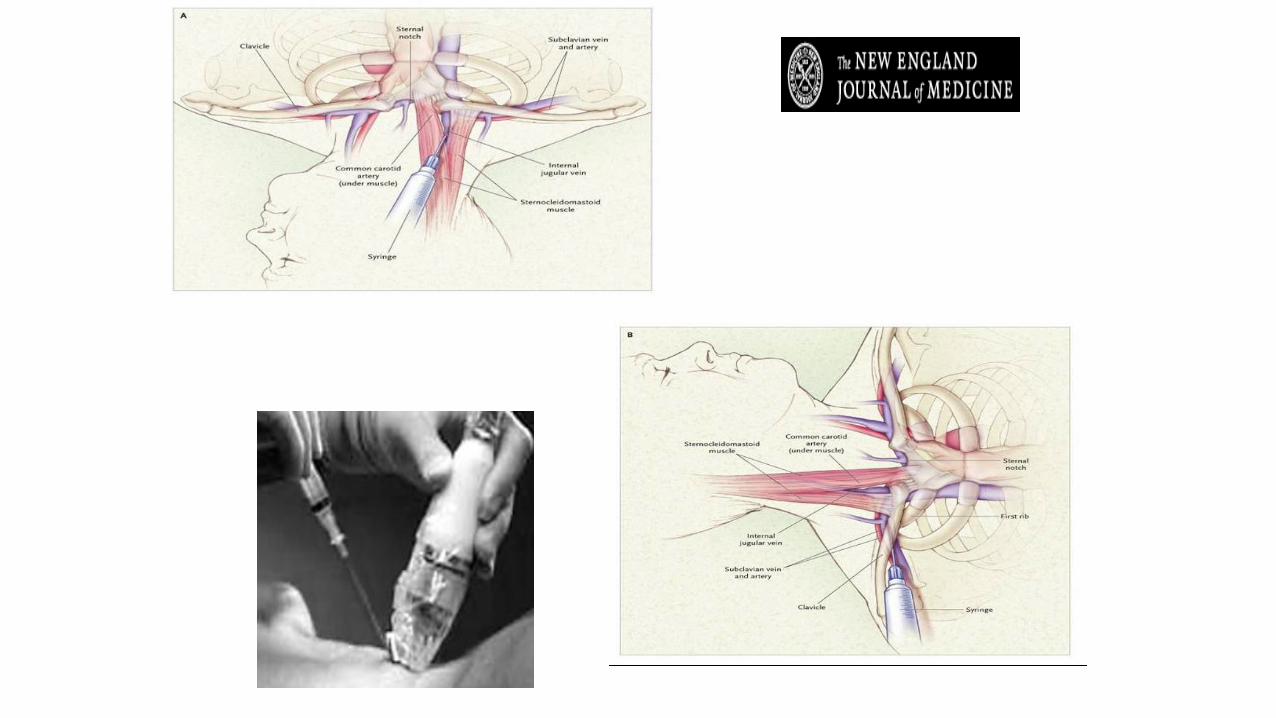
CARDIOGENICSHOCK
IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

IC = 30
Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Valvola peep
boussignac
NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

NON INVASIVE VENTILATION
Pinsp gt Pesp
Riduce il lavoro dei muscoli respiratori e puograve garantire un supporto respiratorio completo
Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Chest 2015 Jul148(1)253-61Spoletini G Alotaibi M Blasi F Hill NS
High Flow Nasal Cannula (HFNC) administer humidified and heated airoxygen mixtures at high flows (up to 60 Lmin)
Enhance patient confort and tolerance
Permit less entrainment of room air during patient inspiration
Combined with the flushing of expired air from the upper airway during expiration assuremore reliable delivery of high FiO2 levels improves ventilatory efficiency and reduces the work of breathing
HFNC also generates PEEP wich may counterbalance auto-PEEP further reducing ventilatorywork improve oxygenation and provide back pressure to enhance airway patency during
expiration
Very few high quality studies have been pubblished
EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

EMERGENZE PEDIATRCHE
non consideratemi un adulto in miniatura
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
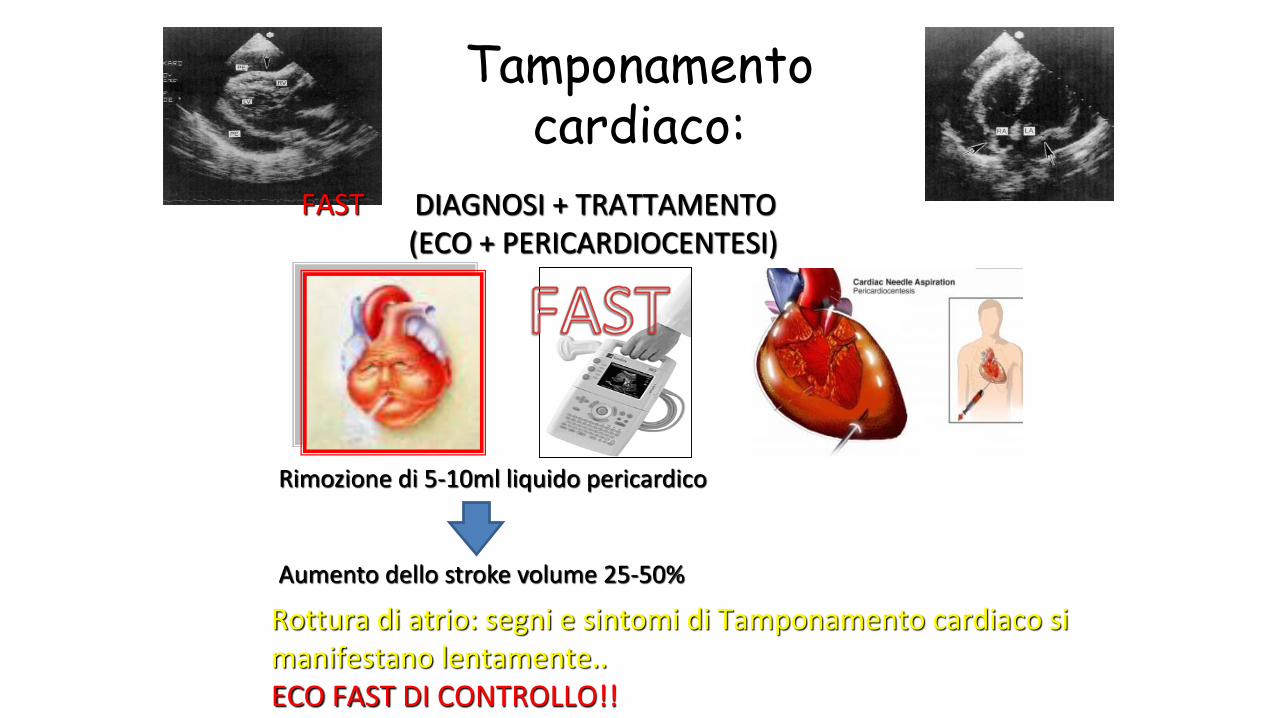
cambiano i parametri vitali normali
FCveglia FCsonno FR PA sistolica PA diastolica
Neonato 100-180 80-160 40-60 60-90 20-60
Lattante 100-160 75-160 30-60 87-105 53-66
1deg infanzia (2 anni)
80-110 60-90 24-40 95-105 53-66
2deg infanzia (5 anni)
70-100 60-90 22-34 96-110 55-69
Etagrave scolare (7 anni)
65-110 60-90 18-30 97-112 57-71
Adolescente (15 anni)
60-90 50-90 12-16 112-128 66-80
Robert M Kliegman et al editors Nelson Textbook of Pediatrics 18th edition (Philadelphia Saunders Elsevier 2007) 389 modificato
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
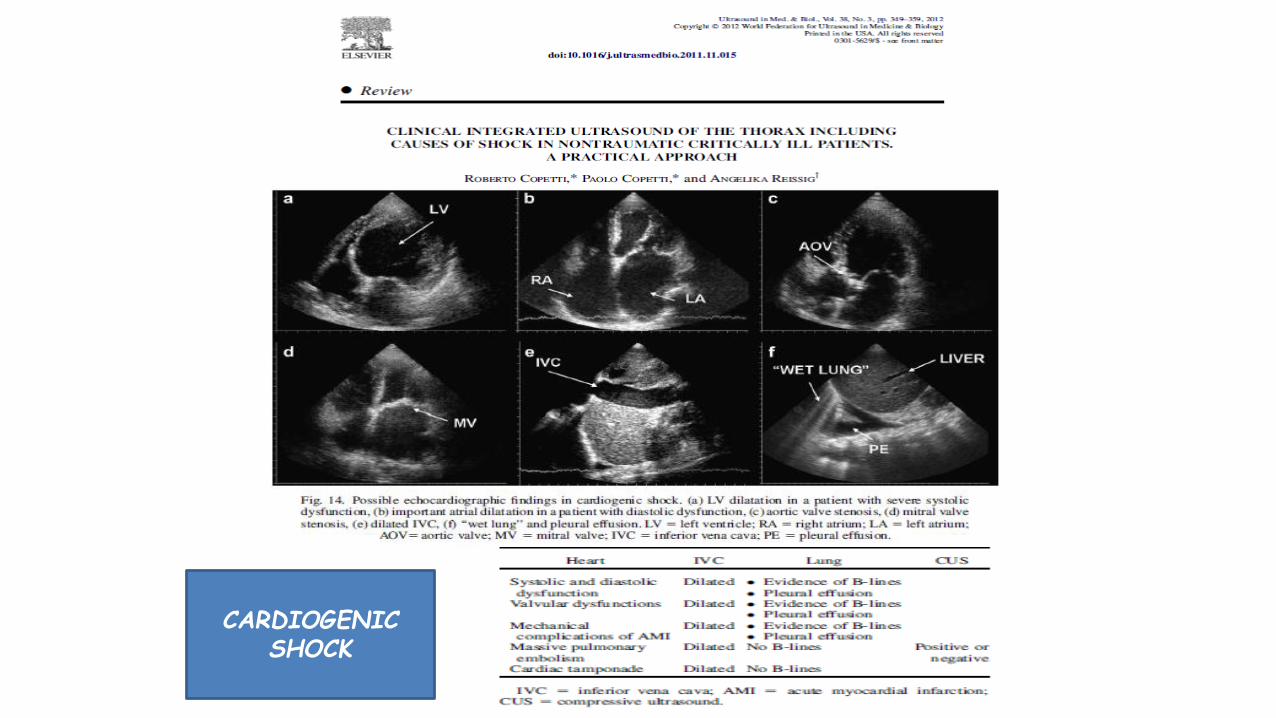
38
PRESIDI GRIGIOOK
radicROSAROSSO
OK
radicVIOLA
OK
radicGIALLO
OK
radicBIANCO
OK
radicBLU
OK
radicARANCIO
OK
radicVERDE
OK
radic
Maschera per
ventilazione0 1 2 3 3 3 3 3 3 4
Canala di
Guedel
35
mm
45 mm
45 mm 55 mm 55 mm 55 mm 70 mm 70 mm 70 90 mm
Catetere
Aspirazione8 fr 8 fr 10 fr 10 fr 10 fr 10 fr 10 fr 10 fr
Lama
laringoscopio
0 1
dritta
(curva)
1 dritta
(curva)
1 dritta
(curva)
2 dritta
(curva)
2 dritta
(curva)2 drittacurva
2
drittacurva
3
drittacurva
Tubo
endotracheal
e
25 ndash 3
35 no
cuffia
35 no cuffia
4
no
cuffia(cuffiato)
45 no
cuffia(cuffiato)
5 no
cuffia(cuffiato)
55 no
cuffia(cuffiato)6 cuffiato 65 cuffiato
Mandrino 6 fr 6 fr 6 fr 6 fr 6 fr 14 fr 14 fr 14 fr
Canula naso
faringea
12 - 14
fr14 fr 18 fr 20 fr 22 fr 24 fr 26 fr 30 fr
Maschera
Laringea LMA1 15 2 2 2 2 - 25 25 3
Sondino naso
gastrico5 - 8 fr 5 - 8 fr 8 - 10 fr 10 fr 10 fr 12 - 14 fr 14 - 18 fr 16 fr
Catetere
vescicale5 fr 8 fr 8 - 10 fr 10 fr 10 - 12 fr 10 - 12 fr 12 fr 12 fr
Tubo toracico
(trocar
Argyle)
10-12
fr10 - 12 fr 16 - 20 fr 20 - 24 fr 20 - 24 fr 24 - 32 fr 28 - 32 fr 32 - 38 fr
Ago canula22 - 24
ga22 - 24 ga 20 - 24 ga 18 - 22 ga 18 - 22 ga 18 - 20 ga 18 - 20 ga 18 - 20 ga
Butterfly22 - 24
ga23 - 25 ga 23 - 25 ga 21 - 23 ga 21 - 23 ga 21 - 23 ga 21 - 22 ga 18 - 21 ga
CHECK LIST CASSETTI BIMBI A COLORI DATAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip FIRMAhelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip
neonato tra 4 e 7 kg tra 8 ed 11 kg tra 11 e 14 kg tra 14 e 17 kg tra 18 e 22 kg tra 24 e 30 kg oltre 34 kg
sono diversi i presidi da utilizzarehellip
PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

PALS Bradycardia Algorithm
Kleinman M E et al Circulation 2010122S876-S908
Copyright copy American Heart Association
The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

The Broselow-Luten SystemEmergency System
YELLOW
DRUGS and EQUIPMENT
GREEN
ORANGE
WHITE
YELLOW
PURPLE
RED
PINK
33mL
27 mL
17 mL
13 mL
1 mL
085 mL
065 mL
BLUE 2 mL
EPINEPHRINEConcentration
01 mgmL 110000
ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

ED overcrowding has been found tocorrelate with
1) increased patient mortality2) decreased patient satisfaction
Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Sepsis and septic shock are medical emergencies and we recommend that treatment and resuscitation begin immediatelyBest Practice Statement
Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Summary
bull Start resuscitation early with source control intravenous fluids and antibiotics
bull Frequent assessment of the patientsrsquo volume status is crucial throughout the resuscitation period
bull We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion
2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

2Diagnostica - EGA
Egrave la saturazione del sangue della vena cava o dellrsquoatrio destro
Rappresenta lrsquoossigenazione residua del sangue proveniente dai tessuti dopo lrsquoestrazione di ossigeno
Ersquo un indice della relazione tra apporto di O2 (DO2) ed estrazione di O2 (VO2)
Vn gt 70
ScvO2Saturazione venosa centrale
darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

darr DO2
Ipossia tissutale globale
ScvO2 lt 70
uarr Lattati
bull Tonometria gastrica
bull Capnografia sublinguale
bull ∆ (vc ndash a) CO2 gt 5 mmHg
uarr CO2 tissutale
World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

World Society of Abdominal
Compartment Syndrome (WSSCS)
valori normali 5-7 mmHg
pazienti obesi 7-14 mmHg
pz in posizione semiseduta (30ndash45deg) 4ndash9 mmHg
Ipertensione intra-addominale (IAH)
persistente elevazione della IAP ge 12 mmHg
I grado 12-15mmHg II grado 16-20mmHg
III grado 21-25mmHg IV grado gt25mmHg
Sindrome compartimentale addominale (ACS)
incremento della IAP gt 20 mmHg associata ad una disfunzione o insufficienza drsquoorgano di nuova insorgenza
I
A
P
APP=MAP-IAPVn gt60mmHg
Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Shock 2017 Jul 19 doi 101097SHK0000000000000949 [Epub ahead of print]
Evaluation of Non-Invasive Hemoglobin Monitoring in
Trauma Patients with Low Hemoglobin LevelsGamal M1 Abdelhamid B Zakaria D Dayem OAE Rady A Fawzy M Hasanin A
CONCLUSIONS Sp-Hb showed accurate precision in both absolute values and trend values compared to
Lab-Hb measurement in trauma patients with low hemoglobin levels
If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

If shock is not resolving quicklyhellip
bull We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (Best Practice Statement)
bull We suggest that dynamic over static variables be used to predict fluid responsiveness where available (Weak recommendation low quality of evidence)
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
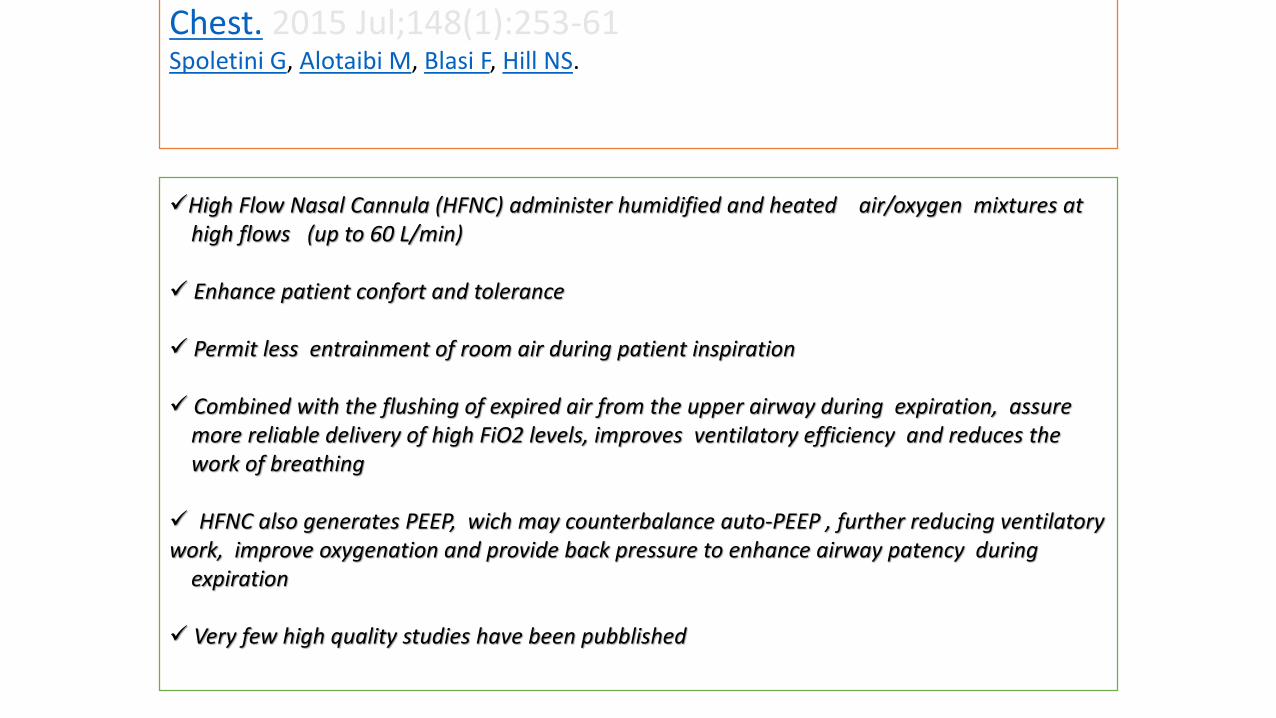
FLUID RESPONSIVE
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
Progressive volume loading
Severe tissue edema
Compromised tissueoxygenation
Further compromisedmicrovascular dysfunction
FLUID OVERLOAD ldquoPatients who have the largest cumulative fluid balance have an increased mortalityrdquo
PE Marik2011
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
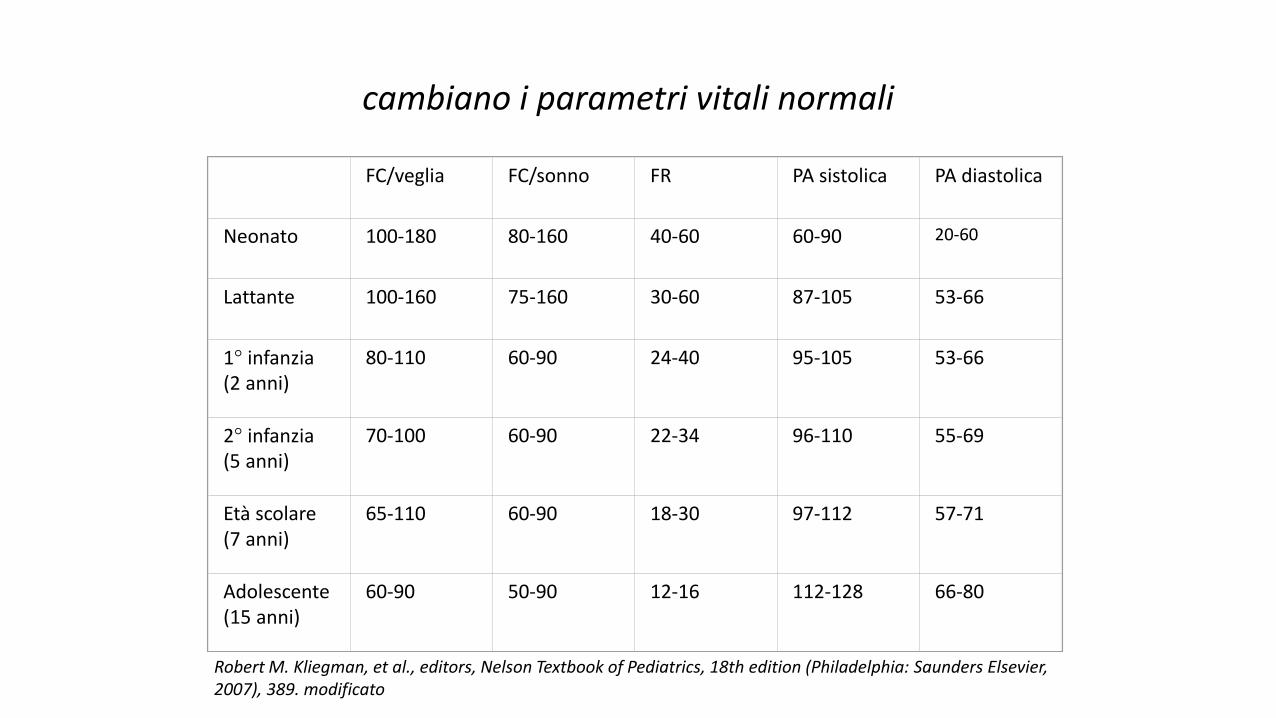
Occult Hypovolemia
bull Alto indice di sospetto
bull Monitoraggi piugrave sofisticati
Fluid Challenge Test PLG
R L Metha W C Clark M Schetz Techniques for assessing and achieving fluid balance inacute renal failure Current Opinion in Critical Care 2002 8 535-543
Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Passive leg raising
In spontaneously breathing patients Descending aorta blood flow (Esophageal Doppler)Velocity-time integral (Transthoracic echocardiography)Femoral artery flow (Arterial Doppler)Transpulmonary ThermodilutionPulse contour derived stroke volume [uncalibrated]Bioreactance
Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Pulse contour methods
Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Stroke volume
BIOIMPEDENCE AND
BIOREACTANCE
MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

MONITORAGGIO STATO VOLEMICO E FLUID RESPONSIVENESS
LA METODICA GIUSTA NEL SETTING GIUSTO
Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Grazie per lrsquoattenzione
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
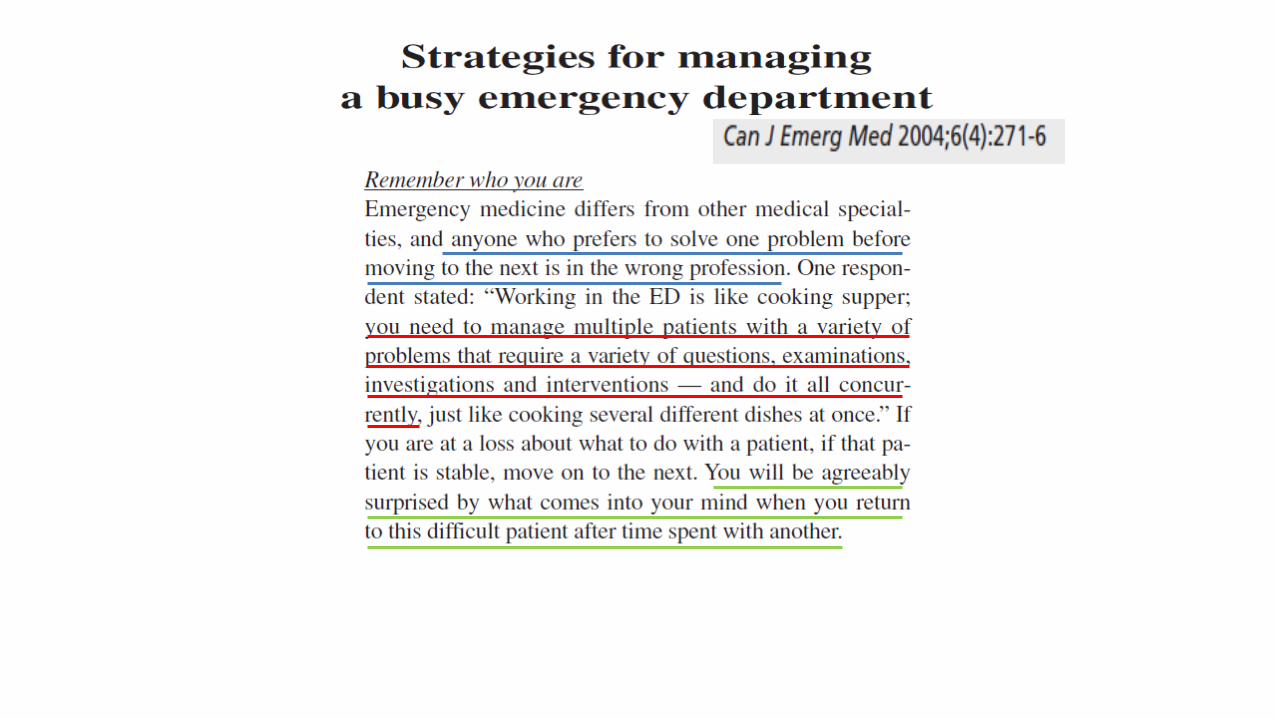
Chronic State of Emergency Department (ED) Overcrowding in North America
bull Acute care bed closures
bull Early discharge of patients who are still relatively ill
bull Patients without primary care physicians turn increasingly to Eds for this care
bull Patients with chronic illness face prolonged waits for diagnostic modalities and
specialty consultation ndash delays thet often lead to decompensation and urgent
ED treatment
bull lack of acute care beds patients held in the ED for prolonged periods interfering
with the assessment and management of arriving patient with urgent
CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

CPAP Continuous Positive Airway Pressure
- La pressione applicata durante la fase inspiratoria egrave uguale alla pressione di fine espirazione
- Inizio e fine dellrsquoinspirazione sono determinate dal paziente- Flusso e Volume sono completamente generati dai muscoli del paziente
Il suo uso egrave appropriato quando i muscoli respiratori del paziente sono in grado di generare una forza muscolare sufficiente
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
bull Ministero della Salute progressivo incremento degli accessi in Pronto Soccorso negli
ultimi anni (21274174 nel 1997 24215174 nel 2009
bull Deospedalizzazione dei processi assistenziali costante riduzione dei posti letto
ordinari (Regione Lazio riduzione del 25)
Crowding occurs when the identified need for emergency servicesexceeds available resources for patient care in the ED hospital or both
American College of Emegency Physician (ACEP) 2006
Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Spoken interactions can be especiallychallenging in Emergency Department
bull time constraintsbull interruptionsbull staff changesbull overcrowdingbull heterogeneity in the types of
patientsbull heterogeneity in the types of
medical problems
Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Insufficienza Renale AcutaValutazione Diagnostica in Urgenza
Laboratory Evaluation
bull Creatinina
bull Potassiemia
bull BUNCr
bull FENa
bull Es Urine
Eco reni e vie urinarieECG RX Torace EGA
Volume status
Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were

Surviving Sepsis Campaign International Guidelines for Management of Sepsis
and Septic Shock 2016
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were
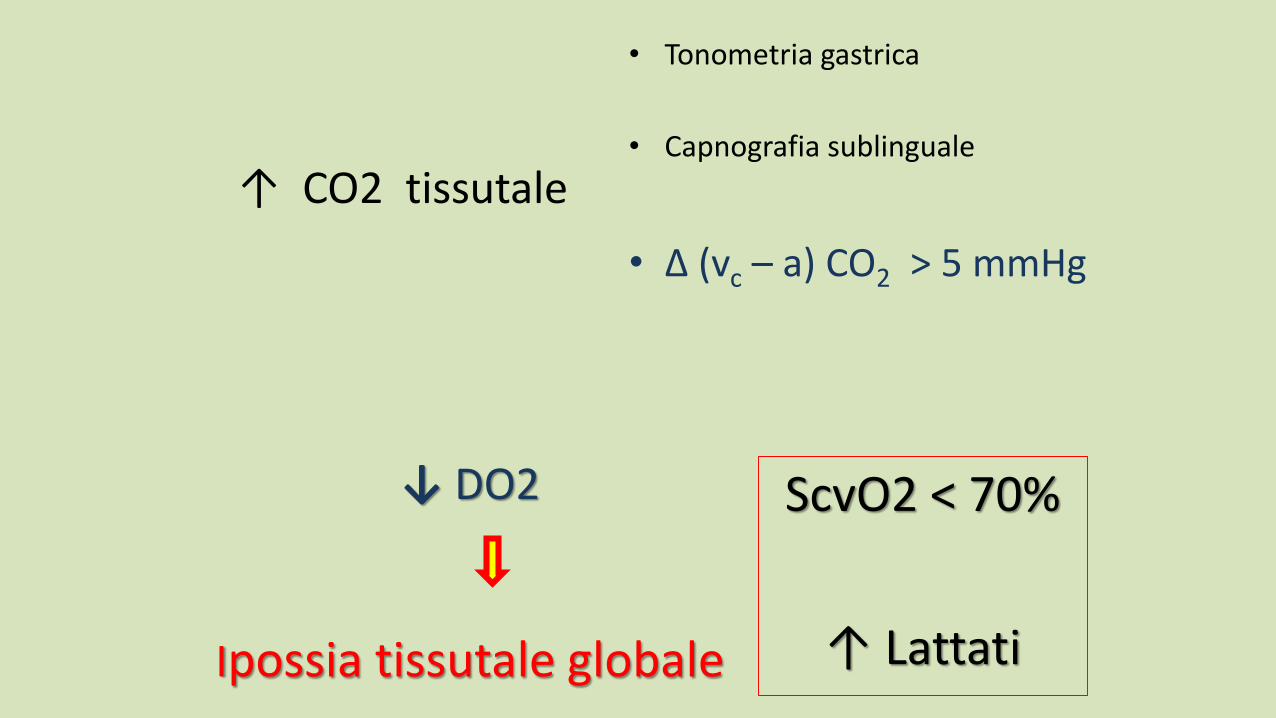
The Riverrsquos work was usefulhellip
bull As it provided us a construct on how to understand resuscitationbull Start early- (give antibiotics ndash Source control)
bull Correct hypovolaemia
bull Restore perfusion pressure
bull And in some cases a little more may be required
bull These concepts are as important today as they ever were