the impact of a single nucleotide polymorphism in sigmar1
TRANSCRIPT

ORIGINAL RESEARCH
The Impact of a Single Nucleotide Polymorphismin SIGMAR1 on Depressive Symptoms in MajorDepressive Disorder and Bipolar Disorder
Laura Mandelli . Sheng-Min Wang . Changsu Han . Soo-Jung Lee .
Ashwin A. Patkar . Prakash S. Masand . Chi-Un Pae .
Alessandro Serretti
Received: November 20, 2016 / Published online: January 31, 2017� Springer Healthcare 2017
ABSTRACT
Introduction: Ample evidence suggested a roleof sigma-1 receptor in affective disorders sincethe interaction of numerous antidepressantswith sigma receptors was discovered. A recentstudy on Japanese subjects found a geneticvariant within the encoding gene SIGMAR1(rs1800866A[C) associated with major depres-sive disorder (MDD). We aimed to evaluate thesame polymorphism in both MDD and bipolardisorder (BD) as well as its relationship toresponse to treatment with antidepressants andmood stabilizers.
Methods: A total of 238 MDD patients treatedfor an acute episode of depression, 132 BDpatients in treatment with mood stabilizers for amanic or mixed episode, and 324 controls weregenotyped for rs1800866. At discharge,response to treatments was evaluated in MDDand BD patients by the Hamilton Rating Scalefor Depression (HRSD) and the Young ManiaRating Score (YMRS), respectively.Results: In our Korean sample, allele frequen-cies were different from those reported in otherAsian and non-Asian populations. The CCgenotype was associated with BD and, as atrend, with MDD. No significant effect wasobserved on response to antidepressants inMDD or mood stabilizers in BD, although theCC genotype was more frequent among BDpatients experiencing a mixed episode.
Enhanced content To view enhanced content for thisarticle go to http://www.medengine.com/Redeem/8587F0601269911A.
L. Mandelli � A. SerrettiDepartment of Biomedical and NeuroMotorSciences, Institute of Psychiatry, University ofBologna, Bologna, Italy
S.-M. Wang � S.-J. Lee � C.-U. Pae (&)Department of Psychiatry, The Catholic Universityof Korea College of Medicine, Seoul,Republic of Koreae-mail: [email protected]
S.-M. WangInternational Health Care Center, Seoul St. Mary’sHospital, The Catholic University of Korea Collegeof Medicine, Seoul, Korea
C. HanDepartment of Psychiatry, Korea University, Collegeof Medicine, Seoul, Republic of Korea
A. A. Patkar � C.-U. PaeDepartment of Psychiatry and Behavioural Sciences,Duke University Medical Center, Durham, NC, USA
P. S. MasandGlobal Medical Education, New York, NY, USA
P. S. MasandAcademic Medicine Education Institute, Duke-NUSMedical School, Singapore, Singapore
Adv Ther (2017) 34:713–724
DOI 10.1007/s12325-017-0482-2

Conclusion: The present findings are the first topropose the putative role of genetic variantswithin SIGMAR1 and sigma-1 receptor in BD.Sigma-1 receptor can modulate a number ofcentral neurotransmitter systems as well assome other signaling pathways (e.g., neu-rotrophin and growth factor signaling) whichare seemingly involved in BD and other mooddisorders.
Keywords: Antidepressants; Bipolar disorder;Major depressive disorder; Mood stabilizers;Psychiatry; Sigma-1 receptor; SIGMAR1
INTRODUCTION
Sigma-1 receptors have been implicated inmany neuropsychiatric disorders including drugaddiction, schizophrenia, depression, anxietydisorders, neurodegenerative disorders, HIV-re-lated neurocognitive impairment, and paindisorders [1]. Sigma-1 receptors are located inthe specialized endoplasmatic reticulum (ER)membrane directly apposing mitochondria(mitochondria-associated ER membrane) [2, 3],but their localization can be very dynamic: theycan translocate to other areas of the cell [4, 5]where they can interact with a plethora ofmembrane targets such as voltage-gated ionchannels, glutamate and gamma-aminobutyricacid (GABA) ionotropic receptors, muscarinicand nicotinic acetylcholine receptors, dopa-mine D1 receptor, and intracellular targets[5, 6]. Sigma-1 receptors have been reported toaffect overall neuronal excitability throughinhibition of Na? and K? currents and facilita-tion or inhibition of voltage-gated Ca2? chan-nels [1]. Furthermore, sigma-1 receptors havethe potential to modulate N-methyl-D-aspartatereceptor (NMDAR, a glutamate receptor) trans-mission [7, 8] and influence the glutamatergicsystem and excitatory neurotransmission [1].
Although a precise mechanism of functionalresponse to sigma-1 receptor is still uncertain, ithas been accepted that it can modulate anumber of central neurotransmitter systemsincluding glutamate/NMDA, serotonergic,dopaminergic, noradrenergic routes, and othersignaling pathways (e.g., neurotrophin and
growth factor signaling) which are related tobrain function and involved in neuropsychi-atric disorders [9]. Upregulation of sigma-1receptor exerts a potent neuroprotective effectby ameliorating the so-called ER stress[5, 10, 11]. The ER stress is a condition charac-terized by an accumulation of unfolded proteinscaused by oxidative stress, ischemic insults,disturbances in calcium homeostasis, andenhanced expression of normal and/or fold-ing-defective proteins [12, 13]. Accumulatingevidence suggests a role of ER stress and mis-folded proteins in pathophysiology of majordepressive disorder (MDD) [5, 11], and a highlevel of ER stress proteins has been observed intemporal cortex of depressed patients [14].Upregulation of sigma-1 receptor not onlyameliorates ER stress but also results in secretionof brain-derived neurotrophic factors (BDNF) bypotentiating conversion of precursor proBDNFto mature BDNF [11, 15, 16]. Evidence alsosuggested that sigma-1 receptor greatly poten-tiates nerve-growth factor (NGF)-induced neu-rite outgrowth [17]. Sigma-1 receptor is alsostimulated by endogenous neuroactive steroids,dehydroepiandrosterone (DHEA). Moriguchiet al. [18] reported that sigma-1 receptor stim-ulation by DHEA in hippocampal dentate gyrusameliorates depressive-like behaviors in olfac-tory bulbectomized mice by enhancing neuro-genesis via activation of the protein kinase B(Akt)/glycogen synthase kinase-3 beta (GSK-3b)/b-catenin pathway.
Much evidence has linked sigma receptorand mood disorders ever since the interaction ofnumerous antidepressants with sigma receptorswas first discovered. In particular, fluvoxamineis a potent agonist of sigma-1 receptor [19]. Inmice, expression of sigma-1 receptor decreasedafter chronic dexamethasone infusion, and thisdecrease was normalized after fluvoxaminetreatment [20]. In a study with a small sample of12 late-life MDD patients [21], mean plasmasigma-1 receptor concentration was increasedsignificantly following 8 weeks of antidepres-sant treatment. However, no significant corre-lation was found between changes in plasmasigma-1 receptor concentration and clinicalresponse to 8 weeks of antidepressant treat-ment. Evidence for involvement of sigma-1
714 Adv Ther (2017) 34:713–724

receptor in mood disorders also came from theobservation that sigma-1 receptor knockoutmice showed increased immobility (a depres-sive-like phenotype) in a forced swimming testand agonists of the sigma-1 receptor exertedantidepressant effects in animal models [22–26].
Genetic heterogeneity may alter expressionand functionality of sigma-1 receptor, with sig-nificant results on neuronal excitability andplasticity. The gene coding for sigma-1 receptoris located on chromosome 9 (9p13.3), and itspans about 7 kb and contains four exons [27].Two single nucleotide polymorphisms (SNPs)within sigma-1 receptor (SIGMAR1) (rs1799729and rs1800866) were reported to be possiblyfunctional [27, 28]. In particular, rs1800866 iscontained in a substitution from glutamine(CAG) to proline (CCG) that may perturbappropriate regulation of sigma-1 receptortransportation from ER to plasma membrane[28]. In humans, genome-wide associationstudies reported that there are no associationsamong genes encoding for SIGMAR1, MDD[29, 30], and clinical response to treatment withcitalopram [31, 32]. However, a recent studyperformed on an Asian population consisting ofJapanese patients with MDD treated with flu-voxamine or sertraline found that rs1800866 inSIGMAR1 is associated with pathophysiology ofMDD but not with response to fluvoxamine orsertraline [33]. In line with this result, ourreview of current literature showed that sigmareceptor-mediated events could modulateactivity of certain conventional antiepilepticdrugs and antidepressants implemented fortreatment of BD [34] and MDD [35]. However,we were not able to find any studies suggestingrelationship among SNPs and particularlybipolar disorder (BD) as well as investigationson correlation between SNPs with treatmentresponse for BD.
Even in the most recent and extensive reviewof the field of antidepressant pharmacogenetics,there is no mention of the potential role andrelevant impact of SIGMAR1 on mood disorders[36]. A number of markers in relation to thedevelopment of mood disorders and response toantidepressants have been extensively tested atmultiple levels including genetic, epigenetic,gene expression, and protein. However, only
few pharmacogenetic markers (i.e., FKBP5 insignaling transduction, SLC6A4, ABCB1, andHTR2A in neurotransmission, and CYP450isoenzymes in drug metabolism) have beenaddressed for their clinical utility in terms ofdiagnosis and treatment of mood disorders [36].In addition, pharmacogenetic tests are neitheradvised to include and combine different typesof biomarkers nor suggested to target specificsubpopulations of MDD with heterogeneousclinical features and clinical dimensions ofmood disorders [36].
Given the lack of sufficient data about role ofSIGMAR1 in MDD and BD, we investigated therole of a candidate SNP within SIGMAR1(rs1800866) in a Korean sample of subjectsaffected by MDD (n = 242) and BD (n = 132) ascompared to healthy controls (n = 324). Wealso tested the potential influence of rs1800866on antidepressant treatments in MDD patientsduring an acute depressive episode and moodstabilizers in BD patients during an acutemanic/mixed episode.
METHODS
Subjects
Patients were consecutively collected amongpatients admitted to the psychiatric unit of theDepartment of Psychiatry, Catholic Universityof Korea College of Medicine, Seoul, Korea.Inclusion criteria were represented by agebetween 18 and 80 years, current episode ofdepression for MDD patients, current episode ofmania/mixed episode for BD patients,monotherapy with venlafaxine or paroxetine inMDD patients, monotherapy with lithium, val-proate, or carbamazepine in BD patients.Exclusion criteria were represented by currentor recent substance abuse, severe or unsta-ble medical condition that may impair evalua-tions, neurological disorders, non-Asianethnicity, treatments other than those specifiedabove with the exception of antianxiety drugs,poor understanding or fluency of Korean lan-guage, mental retardation. Healthy subjectswho underwent the same assessment as psy-chiatric patients were included as a control
Adv Ther (2017) 34:713–724 715

group. The controls were aged between 18 and80 years, of Asian ethnicity with a good under-standing and fluency of Korean language, didnot have current or recent substance abuse,severe or unstable medical conditions, neuro-logical disorders, mental retardation, and theywere not receiving treatment with psychotropicdrugs with the exception of sedative/hypnoticdrugs.
Clinical and sociodemographic data werecollected by means of interviews or revision ofthe clinical charts. Diagnoses of MDD, currentdepressive episode, and BD or current manic/mixed episode were made according to theDiagnostic and Statistical Manual of mentaldisorders IV, text revised (DSM-IV-TR) criteriaby the structured clinical interview for DSM-IV(SCID-I) [37]. Symptoms severity was evaluatedby the Hamilton Rating Scale for Depression(HRSD) [38] in both MDD and BD patients, andthe Young Mania Rating Scale (YMRS) [39] inBD patients only. All the patients were evalu-ated for symptoms severity at admission anddischarge. Evaluations were performed bytrained interviewers blind to genetic data.
The percentage change of the HDRS andYMRS scores from baseline to discharge wascalculated by means of the formula 100 - (D/B 9 100), where D stands for discharge scoreand B for baseline score. Response was definedas a C50% symptoms reduction from baseline todischarge. Remission was defined as a YMRSscore B12 and HAMD score B7 at discharge,respectively. Drug dosage equivalents were cal-culated according to the Columbia Antidepres-sant History Form (ATHF) [40, 41]. Forantidepressants, dosage equivalents were calcu-lated as follow: (1) paroxetine\10 mg/day orvenlafaxine\75 mg/day, (2) paroxetine 10–19 mg/day or venlafaxine 75–149 mg/day, (3)paroxetine 20–39 mg/day or venlafaxine 150–224 mg/day, (4) paroxetine C40 mg/day orvenlafaxine C225 mg/day. For mood stabilizers,dosage equivalents were calculated as follow: (1)lithium or valproate \600 mg/day, or carba-mazepine\200 mg/day, (2) lithium or valproate600–899 mg/day or carbamazepine 200–399mg/day, (3) lithium or valproate C900mg/dayor carbamazepine C400 mg/day.
Compliance with Ethics Guidelines
All procedures followed were in accordancewith the ethical standards of the responsiblecommittee on human experimentation (insti-tutional and national) and with the HelsinkiDeclaration of 1964, as revised in 2013. All thepatients were informed in detail about the aimsand the procedures of the study and they signedan informed consent prior to inclusion into thestudy. The protocol and the informed consentwere approved by the local ethical committee(approval number HC10TISI0031).
Statistical Analysis
All the statistical analyses were performed bythe Statistica software [42]. Descriptive statisticswere based on calculation of mean, standarddeviation, and percentages.
For linear analyses we used the correlationanalysis, the Student t test, and the one-way orrepeated analysis of variance (ANOVA). Tocontrol for potential confounders and to testinteractive effects we employed the linear orbinary logistic regression analysis.
Although we performed a large number oftests, given the preliminary nature of the studywe chose to maintain a threshold of p\0.05 forsignificant associations, in order to detect smallbut potentially interesting effects that maydeserve attention in further studies. With thisparameter value, we had a sufficient power of0.80 to detect small effect sizes of w = 0.12 incase–control associations with three genotypes.
Genetic Analysis
Genomic DNA was extracted from blood andquantified using standard methods [43]. Ahigh-throughput genotyping method using apyrosequencer (Biotage, Uppsala, Sweden) wasused for genotyping the one rs1800866 SIG-MAR1 SNP. Polymerase chain reaction primersand sequencing primers (Bioneer, Daejeon,Korea) used for the pyrosequencing assay weredesigned using the Pyrosequencing AssayDesign Software v1 (Biotage).
716 Adv Ther (2017) 34:713–724
RESULTS
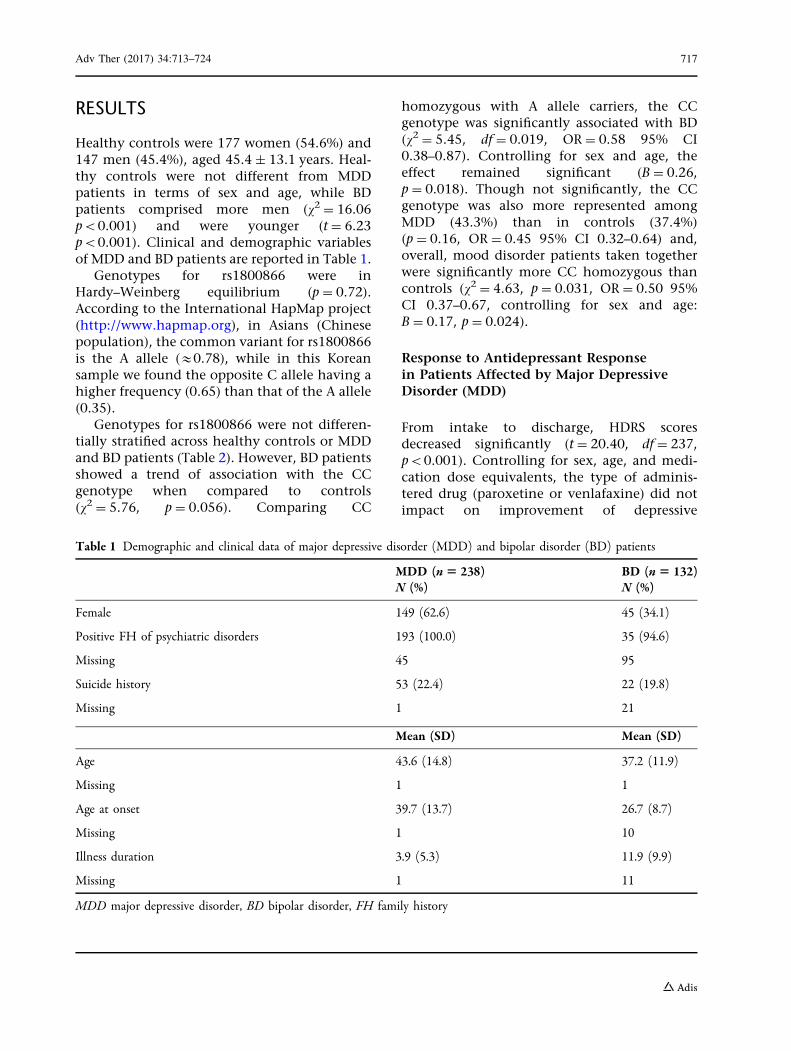
Healthy controls were 177 women (54.6%) and147 men (45.4%), aged 45.4 ± 13.1 years. Heal-thy controls were not different from MDDpatients in terms of sex and age, while BDpatients comprised more men (v2 = 16.06p\0.001) and were younger (t = 6.23p\0.001). Clinical and demographic variablesof MDD and BD patients are reported in Table 1.
Genotypes for rs1800866 were inHardy–Weinberg equilibrium (p = 0.72).According to the International HapMap project(http://www.hapmap.org), in Asians (Chinesepopulation), the common variant for rs1800866is the A allele (&0.78), while in this Koreansample we found the opposite C allele having ahigher frequency (0.65) than that of the A allele(0.35).
Genotypes for rs1800866 were not differen-tially stratified across healthy controls or MDDand BD patients (Table 2). However, BD patientsshowed a trend of association with the CCgenotype when compared to controls(v2 = 5.76, p = 0.056). Comparing CC
homozygous with A allele carriers, the CCgenotype was significantly associated with BD(v2 = 5.45, df = 0.019, OR = 0.58 95% CI0.38–0.87). Controlling for sex and age, theeffect remained significant (B = 0.26,p = 0.018). Though not significantly, the CCgenotype was also more represented amongMDD (43.3%) than in controls (37.4%)(p = 0.16, OR = 0.45 95% CI 0.32–0.64) and,overall, mood disorder patients taken togetherwere significantly more CC homozygous thancontrols (v2 = 4.63, p = 0.031, OR = 0.50 95%CI 0.37–0.67, controlling for sex and age:B = 0.17, p = 0.024).
Response to Antidepressant Responsein Patients Affected by Major DepressiveDisorder (MDD)
From intake to discharge, HDRS scoresdecreased significantly (t = 20.40, df = 237,p\0.001). Controlling for sex, age, and medi-cation dose equivalents, the type of adminis-tered drug (paroxetine or venlafaxine) did notimpact on improvement of depressive
Table 1 Demographic and clinical data of major depressive disorder (MDD) and bipolar disorder (BD) patients
MDD (n5 238)N (%)
BD (n5 132)N (%)
Female 149 (62.6) 45 (34.1)
Positive FH of psychiatric disorders 193 (100.0) 35 (94.6)
Missing 45 95
Suicide history 53 (22.4) 22 (19.8)
Missing 1 21
Mean (SD) Mean (SD)
Age 43.6 (14.8) 37.2 (11.9)
Missing 1 1
Age at onset 39.7 (13.7) 26.7 (8.7)
Missing 1 10
Illness duration 3.9 (5.3) 11.9 (9.9)
Missing 1 11
MDD major depressive disorder, BD bipolar disorder, FH family history
Adv Ther (2017) 34:713–724 717
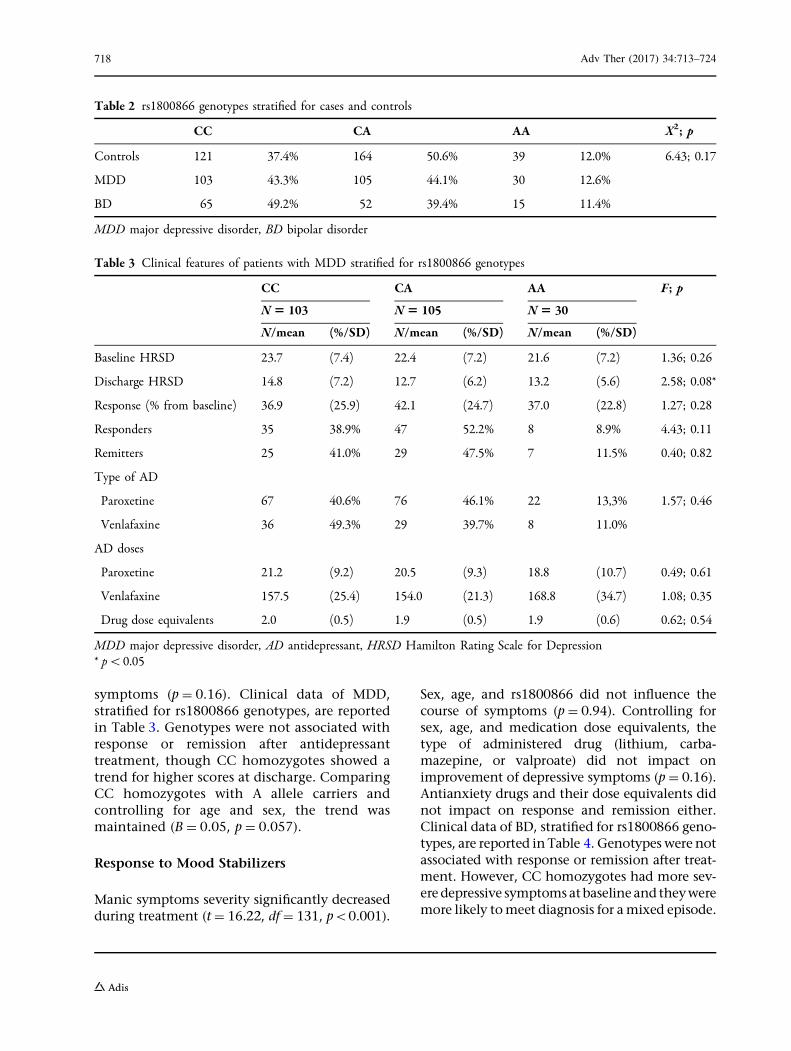
symptoms (p = 0.16). Clinical data of MDD,stratified for rs1800866 genotypes, are reportedin Table 3. Genotypes were not associated withresponse or remission after antidepressanttreatment, though CC homozygotes showed atrend for higher scores at discharge. ComparingCC homozygotes with A allele carriers andcontrolling for age and sex, the trend wasmaintained (B = 0.05, p = 0.057).
Response to Mood Stabilizers
Manic symptoms severity significantly decreasedduring treatment (t = 16.22, df = 131, p\0.001).
Sex, age, and rs1800866 did not influence thecourse of symptoms (p = 0.94). Controlling forsex, age, and medication dose equivalents, thetype of administered drug (lithium, carba-mazepine, or valproate) did not impact onimprovement of depressive symptoms (p = 0.16).Antianxiety drugs and their dose equivalents didnot impact on response and remission either.Clinical data of BD, stratified for rs1800866 geno-types, are reported in Table 4. Genotypes were notassociated with response or remission after treat-ment. However, CC homozygotes had more sev-eredepressive symptomsatbaseline and theyweremore likely tomeet diagnosis for amixed episode.
Table 2 rs1800866 genotypes stratified for cases and controls
CC CA AA X2; p
Controls 121 37.4% 164 50.6% 39 12.0% 6.43; 0.17
MDD 103 43.3% 105 44.1% 30 12.6%
BD 65 49.2% 52 39.4% 15 11.4%
MDD major depressive disorder, BD bipolar disorder
Table 3 Clinical features of patients with MDD stratified for rs1800866 genotypes
CC CA AA F; p
N5 103 N5 105 N5 30
N/mean (%/SD) N/mean (%/SD) N/mean (%/SD)
Baseline HRSD 23.7 (7.4) 22.4 (7.2) 21.6 (7.2) 1.36; 0.26
Discharge HRSD 14.8 (7.2) 12.7 (6.2) 13.2 (5.6) 2.58; 0.08*
Response (% from baseline) 36.9 (25.9) 42.1 (24.7) 37.0 (22.8) 1.27; 0.28
Responders 35 38.9% 47 52.2% 8 8.9% 4.43; 0.11
Remitters 25 41.0% 29 47.5% 7 11.5% 0.40; 0.82
Type of AD
Paroxetine 67 40.6% 76 46.1% 22 13,3% 1.57; 0.46
Venlafaxine 36 49.3% 29 39.7% 8 11.0%
AD doses
Paroxetine 21.2 (9.2) 20.5 (9.3) 18.8 (10.7) 0.49; 0.61
Venlafaxine 157.5 (25.4) 154.0 (21.3) 168.8 (34.7) 1.08; 0.35
Drug dose equivalents 2.0 (0.5) 1.9 (0.5) 1.9 (0.6) 0.62; 0.54
MDD major depressive disorder, AD antidepressant, HRSD Hamilton Rating Scale for Depression* p\0.05
718 Adv Ther (2017) 34:713–724

DISCUSSION
Despite existing evidence of sigma-1 receptorbeing a target of commonly used antidepres-sants [19], its involvement in depressive-likebehaviors in animals (e.g., see [18]) and in theregulation of systems involved in the patho-physiology of depressive disorders[1, 9, 14, 16, 17], only few and inconsistenthuman studies have tested the role of SIGMAR1gene in mood disorders and its relationshipwith treatment responsiveness. As mentioned,large genome-wide association studies reportedno association among SIGMAR1, MDD [29, 30],and clinical response to treatment with citalo-pram [31, 32]. However, two recent studiesreported that antidepressant treatments areassociated with increased plasma levels ofsigma-1 receptors in MDD patients [21] and SNPrs1800866 was associated with MDD in a sampleof Japanese subjects [33], although neither of
these studies found a relationship with thera-peutic response. To the best of our knowledge,no study investigated SIGMAR1 in BD. There-fore, we aimed to (1) replicate the associationbetween rs1800866 within SIGMAR1 and MDD[33] and test the association with response toother antidepressant treatments; (2) test theassociation with BD and therapeutic response tomood stabilizers.
First, contrary to our expectation, in ourKorean population, the minor allele C forrs1800866 was more frequent than the majorallele A (minor allele frequency, MAF &64.8).According to the International HapMap project(http://hapmap.ncbi.nlm.nih.gov), MAF is ofabout 0.10 in Caucasians and 0.22 in the AsianJapanese population.
Second, the CC genotype was associatedwith BD and, to a lower extent, with MDD.While Kishi et al. reported that there is anassociation between the AA genotype and MDD
Table 4 Clinical features of patients with BD stratified for rs1800866 genotypes
CC CA AA F p
N5 65 N5 52 N5 15
Mean SD Mean SD Mean SD
Drug dose equivalents 1002.2 372.7 1107.0 309.1 1028.6 535.5 0.90 0.41
Baseline YMRS 32.9 10.1 33.6 7.9 33.9 8.9 0.12 0.89
YMRS at discharge 19.6 6.1 19.9 4.0 20.1 5.5 0.09 0.92
Baseline HRSD 8.7 4.2 7.3 3.5 4.7 3.5 7.15 0.001
HRSD at discharge 3.3 2.7 2.8 2.3 2.1 2.0 1.55 0.22
N % N % N % X2 p
Mixed episode 39 58.2 25 37.3 3 4.5 8.45 0.015
Treatment
Carbamazepine 2 50.0 1 25.0 1 25.0 1.66 0.80
Lithium 18 43.9 19 46.3 4 9.8
Valproate 25 44.6 22 39.3 9 16.1
Responders 17 51.5 13 39.4 3 9.1 0.26 0.88
Remitters 7 70.0 1 10 2 20 4.74 0.09
MDD major depressive disorder, BD bipolar disorder, AD antidepressant, HRSD Hamilton Rating Scale for Depression,YMRS Young Mania Rating Scale
Adv Ther (2017) 34:713–724 719

[33], we found an opposite relationshipbetween rs1800866 genotypes and mood disor-ders. Nevertheless, this finding may go alongwith the different frequency of the rs1800866alleles in the two populations. Genetic variantspresent different frequencies in different popu-lations and they may have opposite effects on aphenotype, probably because of different link-age disequilibrium with another causal muta-tion, the so-called flip-flop effect [44]. In oursample, MDD patients showed only a trend ofassociation with the CC genotype. However,Kishi and colleagues found an associationbetween the CC genotype with MDD small ineffect size (p = 0.02, OR = 0.56) in a largersample of 466 MDD patients and 516 controls.The sample size of our study was relativelysmall, with 238 MDD and 324 controls, whichmay have prevented us from detecting signifi-cant smaller effect size.
We found that the rs1800866 was signifi-cantly associated with BD. To the best of ourknowledge, no previous study investigatedSIGMAR1 gene in BD. Evidence showed theinvolvement of sigma-1 receptor inschizophrenia, and a recent meta-analysis of theliterature found that rs1800866 was associatedwith schizophrenia in Japanese populations[45, 46]. Since sigma-1 receptor directly orindirectly regulates signal transduction, ERstress, cellular redox, and cellular survival andsynaptogenesis, and some of their ligands exertantidepressants and neuroprotective actions[11], they may also be involved in BD. Wefound that the CC genotype was associated withmore severe depressive symptoms at baseline inBD patients having a mixed episode. Thus, theCC genotype may not only predispose devel-opment of BD but may also be involved indevelopment of more complicated illness suchas co-occurrence of manic and depressivesymptoms, which are often more resistant tomonotherapy with mood stabilizers [47].Accordingly, patients with a diagnosis of mixedepisode showed a poorer response to moodstabilizers (v2 = 4.94, p = 0.026) than those whoshowed either manic or depressive episodes. Webelieve that further investigation is needed withregard to this interesting yet still elusivefinding.
No evidence of involvement of sigma-1receptor in the response to either antidepres-sants or mood stabilizers agents was noted, withthe exception of a non-significant trend forslightly higher depressive symptoms in CCallele carriers at the end of follow-up. Except forthe small trend pertaining to antidepressantresponse, our data are in line with the study byKishy et al. [33] which showed that there is noassociation between CC allele carriers andtreatment response in MDD patients whoreceived fluvoxamine or sertraline. It is unclearfrom the published paper whether the authorsanalyzed clinical response in relation to thedifferent agents, but it seems that rs1800866influenced response to neither sertraline norfluvoxamine. In our study, the specific medica-tion did not have interactive effects withrs1800866 genotype either. These data are incontrast with other evidence supportingantidepressants interacting with sigma-1 recep-tor. However, antidepressants are known tohave different levels of affinity for sigma-1receptor, and some have no affinity at all. Flu-voxamine has the highest affinity for thisreceptor, followed by sertraline and fluoxetine.Citalopram and paroxetine seem to have ascarce or null affinity for sigma-1 receptor [19].Venlafaxine is also known to have a very weakaffinity for this receptor [48]. Therefore, withregard to both paroxetine and venlafaxinereserving poor affinity for sigma-1 receptor, thegenetic variability for SIGMAR1 may not influ-ence the clinical heterogeneity of therapeuticresponse to these drugs. Future studies shouldbe focused on more active ligands of sigma-1receptor, such as fluvoxamine, fluoxetine, andsertraline.
Very limited evidence has reported an inter-action between common mood stabilizers usedor treatment of BD and sigma-1 receptor activ-ity. To the best of our knowledge, sigma recep-tor-mediated events can modulate the activityof some conventional antiepileptic drugs. Asigma receptor ligand (3-PPP) has been reportedto diminish protective activity of valproate, butnot that of carbamazepine, against maximalelectroshock [34], but a direct effect ofantiepileptic drugs on sigma-1 receptor has notyet been proven. To date, there is no data
720 Adv Ther (2017) 34:713–724

supporting a role of mood stabilizers in target-ing or regulating sigma-1 receptor activity. Inour study, we found no evidence for aninvolvement of the rs1800866 variants inresponse to mood stabilizers, but further studiesboth aimed at testing the role of SIGMAR1 indisease risk and mood stabilizers efficacy arenecessarily required.
A number of limitations should be consid-ered. The overall samples size was clearly lim-ited for genetic studies, but it had a sufficientstatistical power to detect significant smalleffects. We performed a large number of testscomparing not only cases and controls but alsoanalyzing genotypes in association with remis-sion and response to antidepressants, moodstabilizers, and other clinical variables. Thus,the multiple comparisons may have increasedthe risk to detect false positive findings whichare very common in candidate gene studies. Ifwe considered a correction for multiple testing,e.g., two case–control analyses and two tests onresponse to antidepressants and to antimanicagents, we would have to consider a significancelevel of at least 0.0125 (Bonferroni correction:0.05/4 tests), leading to loss of a number ofinteresting results in the present study. To thebest of our knowledge, this the first study whichspecifically focused on a genetic variant withinSIGMAR1 in both MDD and BD as well asresponse to antidepressants and mood stabiliz-ers. Thus, we decided not to correct for multipletesting in order to maximize the possibility ofobtaining data so that the data may be furtherinvestigated in future studies pertaining to lar-ger and independent samples or different ethnicgroups. In addition, correction of multiplecomparisons may also create some caveats asproposed by a number of researchers: loss ofvaluable intriguing findings, hindering theadvance of the research, reduction of samplepower, production of publication bias, increaseof type II error; on the other hand, simpledescription of types of significance test and thereason why could be a practical and alternativeway to deal with multiple comparisons [49, 50].Further, MDD and BD share only a part of thegenetic liability.
In the present study only one SNP was con-sidered. The SIGMAR1 gene spans about 7 kband contains four exons and several polymor-phic regions which could potentially modulatethe biologic activity. However the rs1800866polymorphism is most widely investigated inthe literature, mostly in Asians (Japanese espe-cially), with evidence of it being functional[27, 28]. Since we were unable to detect studieson SIGMAR1 in the Korean population, andonly few other validated polymorphisms in thepromoter, coding exon, and 30UTR regions witha minor allele frequency (MAF) [0.05 arereported, we decided to focus specifically onthis variant only.
The BD sample was composed of patientshaving a manic or mixed episode only, as wewere specifically interested in response toantimanic agents. We did not collect informa-tion regarding previous episodes, and it may bepossible that the included BD patients repre-sent a subgroup of subjects suffering from fre-quent manic/mixed episodes. Having no suchinformation, the association between SIGMAR1and BD may not be the same as in other moreheterogeneous samples. On the other hand,the inclusion of patients with concurrentdepressive symptoms allowed us to detect anassociation between SIGMAR1 and more severedepressive symptoms in manic patients as dis-cussed above.
As previously stated, we were specificallyinterested in response to antidepressants andmood stabilizers, so we included patients onlyunder monotherapy with the exception ofantianxiety drugs. In addition, only patientsunder monotherapy with specific drugs wereincluded (i.e., venlafaxine or paroxetine inMDD and lithium or valproate or carba-mazepine in BD). On the one hand, this strictselection of drugs may represent a point ofstrength of the study (i.e., decrease bias fromvarious treatment regimens); on the otherhand, we cannot generalize the findingsobtained on response to other antidepressantsand mood stabilizers. This is especially impor-tant in the case of antidepressants, as they havedifferent affinity for sigma-1 receptors.
Adv Ther (2017) 34:713–724 721

CONCLUSION
In our Korean sample, we found a differentdistribution of alleles for rs1800866 (higherfrequency of minor allele C than major allele A)when compared to other Asian (Japanese andChinese) and Caucasian populations. In partialagreement with a previous study [33], thispolymorphism showed a trend of associationwith MDD, but the CC genotype was especiallymore frequent in BD subjects than in controls,and the same genotype was more frequentamong patients experiencing a mixed episode.To the best of our knowledge, this is the firstreport suggesting a role for sigma-1 receptor andthe encoding gene in BD. No influence of thers1800866 was observed in treatment responseeither with antidepressants in MDD or to moodstabilizers in mixed/manic BD patients. Never-theless, given previous evidence of someantidepressants as agonists of sigma-1 receptor,further studies on antidepressants with highaffinity for this receptor should be performed.The role of sigma-1 receptor in BD and potentialinteraction with mood stabilizer agents alsodeserve further investigation.
ACKNOWLEDGEMENTS
This research was supported by a grant of theKorea Health Technology R&D Project throughthe Korea Health Industry Development Insti-tute (KHIDI), funded by the Ministry of Health& Welfare, Republic of Korea (Grant Number :HC15C1405).All named authors meet the International
Committee of Medical Journal Editors (ICMJE)criteria for authorship for this manuscript, takeresponsibility for the integrity of the work as awhole, and have given final approval for theversion to be published.
Disclosures. Laura Mandelli, Sheng-MinWang, Changsu Han, Soo-Jung Lee, Ashwin A.Patkar, Prakash S. Masand, Chi-Un Pae, andAlessandro Serretti declare no personal, finan-cial, commercial, or academic conflicts ofinterest.
Compliance with Ethics Guidelines. Allprocedures followed were in accordance withthe ethical standards of the responsible com-mittee on human experimentation (institu-tional and national) and with the HelsinkiDeclaration of 1964, as revised in 2013. All thepatients were informed in detail about the aimsand the procedures of the study and they signedan informed consent prior to inclusion into thestudy. The protocol and the informed consentwere approved by the local ethical committee(approval number HC10TISI0031).
Data Availability. The datasets during and/or analyzed during the current study are avail-able from the corresponding author on reason-able request. All authors presented no conflictsof interest to disclose.
REFERENCES
1. Kourrich S, Su TP, Fujimoto M, Bonci A. Thesigma-1 receptor: roles in neuronal plasticity anddisease. Trends Neurosci. 2012;35(12):762–71.
2. Fujimoto M, Hayashi T. New insights into the roleof mitochondria-associated endoplasmic reticulummembrane. Int Rev Cell Mol Biol. 2011;292:73–117.
3. Hayashi T, Rizzuto R, Hajnoczky G, Su TP. MAM:more than just a housekeeper. Trends Cell Biol.2009;19(2):81–8.
4. Hayashi T, Su TP. Intracellular dynamics of sigma-1receptors (sigma(1) binding sites) in NG108-15cells. J Pharmacol Exp Ther. 2003;306(2):726–33.
5. Su TP, Hayashi T, Maurice T, Buch S, Ruoho AE. Thesigma-1 receptor chaperone as an inter-organellesignaling modulator. Trends Pharmacol Sci.2010;31(12):557–66.
6. Maurice T, Urani A, Phan VL, Romieu P. Theinteraction between neuroactive steroids and thesigma1 receptor function: behavioral consequencesand therapeutic opportunities. Brain Res Brain ResRev. 2001;37(1–3):116–32.
7. Liang X, Wang RY. Biphasic modulatory action ofthe selective sigma receptor ligand SR 31742A onN-methyl-D-aspartate-induced neuronal responsesin the frontal cortex. Brain Res.1998;807(1–2):208–13.
722 Adv Ther (2017) 34:713–724

8. Monnet FP, Debonnel G, Junien JL, De Montigny C.N-Methyl-D-aspartate-induced neuronal activationis selectively modulated by sigma receptors. Eur JPharmacol. 1990;179(3):441–5.
9. Skuza G. Pharmacology of sigma (sigma) receptorligands from a behavioral perspective. Curr PharmDes. 2012;18(7):863–74.
10. Hayashi T, Su TP. Sigma-1 receptor chaperones atthe ER-mitochondrion interface regulate Ca(2?)signaling and cell survival. Cell.2007;131(3):596–610.
11. Hayashi T, Tsai SY, Mori T, Fujimoto M, Su TP.Targeting ligand-operated chaperone sigma-1receptors in the treatment of neuropsychiatric dis-orders. Expert Opin Ther Targets.2011;15(5):557–77.
12. Minamino T, Kitakaze M. ER stress in cardiovasculardisease. J Mol Cell Cardiol. 2010;48(6):1105–10.
13. Minamino T, Komuro I, Kitakaze M. Endoplasmicreticulum stress as a therapeutic target in cardio-vascular disease. Circ Res. 2010;107(9):1071–82.
14. Bown C, Wang JF, MacQueen G, Young LT.Increased temporal cortex ER stress proteins indepressed subjects who died by suicide. Neuropsy-chopharmacology. 2000;22(3):327–32.
15. Fujimoto M, Hayashi T, Urfer R, Mita S, Su TP.Sigma-1 receptor chaperones regulate the secretionof brain-derived neurotrophic factor. Synapse.2012;66(7):630–9.
16. Kikuchi-Utsumi K, Nakaki T. Chronic treatmentwith a selective ligand for the sigma-1 receptorchaperone, SA4503, up-regulates BDNF proteinlevels in the rat hippocampus. Neurosci Lett.2008;440(1):19–22.
17. Niitsu T, Iyo M, Hashimoto K. Sigma-1 receptoragonists as therapeutic drugs for cognitive impair-ment in neuropsychiatric diseases. Curr Pharm Des.2012;18(7):875–83.
18. Moriguchi S, Shinoda Y, Yamamoto Y, et al. Stim-ulation of the sigma-1 receptor by DHEA enhancessynaptic efficacy and neurogenesis in the hip-pocampal dentate gyrus of olfactory bulbectomizedmice. PLoS One. 2013;8(4):e60863.
19. Hashimoto K. Sigma-1 receptors and selectiveserotonin reuptake inhibitors: clinical implicationsof their relationship. Cent Nerv Syst Agents MedChem. 2009;9(3):197–204.
20. Terada K, Izumo N, Suzuki B, et al. Fluvoxaminemoderates reduced voluntary activity followingchronic dexamethasone infusion in mice via
recovery of BDNF signal cascades. Neurochem Int.2014;69:9–13.
21. Shimizu H, Takebayashi M, Tani M, et al. Sigma-1receptor concentration in plasma of patients withlate-life depression: a preliminary study. Neu-ropsychiatr Dis Treat. 2013;8:1867–72.
22. Ito K, Hirooka Y, Sunagawa K. Brain sigma-1receptor stimulation improves mental disorder andcardiac function in mice with myocardial infarc-tion. J Cardiovasc Pharmacol. 2013;62(2):222–8.
23. Matsuno K, Nakazawa M, Okamoto K, KawashimaY, Mita S. Binding properties of SA4503, a novel andselective sigma 1 receptor agonist. Eur J Pharmacol.1996;306(1–3):271–9.
24. Sabino V, Cottone P, Parylak SL, Steardo L, ZorrillaEP. Sigma-1 receptor knockout mice display adepressive-like phenotype. Behav Brain Res.2009;198(2):472–6.
25. Ukai M, Maeda H, Nanya Y, Kameyama T, MatsunoK. Beneficial effects of acute and repeated admin-istrations of sigma receptor agonists on behavioraldespair in mice exposed to tail suspension. Phar-macol Biochem Behav. 1998;61(3):247–52.
26. Urani A, Roman FJ, Phan VL, Su TP, Maurice T. Theantidepressant-like effect induced by sigma(1)-re-ceptor agonists and neuroactive steroids in micesubmitted to the forced swimming test. J PharmacolExp Ther. 2001;298(3):1269–79.
27. Prasad PD, Li HW, Fei YJ, et al. Exon-intron struc-ture, analysis of promoter region, and chromoso-mal localization of the human type 1 sigmareceptor gene. J Neurochem. 1998;70(2):443–51.
28. Seth P, Leibach FH, Ganapathy V. Cloning andstructural analysis of the cDNA and the geneencoding the murine type 1 sigma receptor. Bio-chem Biophys Res Commun. 1997;241(2):535–40.
29. Muglia P, Tozzi F, Galwey NW, et al. Genome-wideassociation study of recurrent major depressivedisorder in two European case-control cohorts. MolPsychiatry. 2008;15(6):589–601.
30. Sullivan PF, de Geus EJ, Willemsen G, et al. Geno-me-wide association for major depressive disorder: apossible role for the presynaptic protein piccolo.Mol Psychiatry. 2009;14(4):359–75.
31. Garriock HA, Kraft JB, Shyn SI, et al. A genomewideassociation study of citalopram response in majordepressive disorder. Biol Psychiatry.2010;67(2):133–8.
32. Laje G, Allen AS, Akula N, Manji H, John Rush A,McMahon FJ. Genome-wide association study of
Adv Ther (2017) 34:713–724 723

suicidal ideation emerging during citalopramtreatment of depressed outpatients. PharmacogenetGenomics. 2009;19(9):666–74.
33. Kishi T, Yoshimura R, Okochi T, et al. Associationanalysis of SIGMAR1 with major depressive disorderand SSRI response. Neuropharmacology.2010;58(7):1168–73.
34. Borowicz KK, Kleinrok Z, Czuczwar SJ. Influence of3-PPP, a sigma receptor ligand, on the anticonvul-sive action of conventional antiepileptic drugs.Pharmacol Res. 1999;40(6):509–16.
35. Wang Y, Guo L, Jiang HF, Zheng LT, Zhang A, ZhenXC. Allosteric modulation of sigma-1 receptorselicits rapid antidepressant activity. CNS NeurosciTher. 2016;22(5):368–77.
36. Fabbri C, Hosak L, Mossner R, et al. Consensuspaper of the WFSBP Task Force on Genetics:genetics, epigenetics and gene expression markersof major depressive disorder and antidepressantresponse. World J Biol Psychiatry. 2017;18(1):5–28.
37. First MB, Spitzer RL, Gibbon M, Williams JBW.Structured clinical interview for DSM-IV-TR axis Idisorders, research version, patient edition. (SCID-I/P). New York: Biometrics Research, New York StatePsychiatric Institute; 2002.
38. Hamilton M. A rating scale for depression. J NeurolNeurosurg Psychiatry. 1960;23:56–62.
39. Young R, Biggs J, Ziegler V, Meyer D. A rating scalefor mania: reliability, validity and sensitivity. Br JPsychiatry. 1978;133:429–35.
40. Sackeim HA. The definition and meaning of treat-ment-resistant depression. J Clin Psychiatry.2001;62(Suppl 16):10–7.
41. Dew RE, Kramer SI, McCall WV. Adequacy ofantidepressant treatment by psychiatric residents:
the antidepressant treatment history form as apossible assessment tool. Acad Psychiatry.2005;29(3):283–8.
42. StatSoft I. STATISTICA per Windows: StatSoft Italiasrl; 1995.
43. Miller SA, Dykes DD, Polesky HF. A simple saltingout procedure for extracting DNA from humannucleated acid. Nucleic Acids Res. 1988;16:1215.
44. Lin PI, Vance JM, Pericak-Vance MA, Martin ER. Nogene is an island: the flip-flop phenomenon. Am JHum Genet. 2007;80(3):531–8.
45. Ohi K, Hashimoto R, Yasuda Y, et al. The SIGMAR1gene is associated with a risk of schizophrenia andactivation of the prefrontal cortex. Prog Neuropsy-chopharmacol Biol Psychiatry. 2011;35(5):1309–15.
46. Watanabe Y, Nunokawa A, Kaneko N, Shibuya M,Egawa J, Someya T. Supportive evidence for theassociation between the Gln2Pro polymorphism inthe SIGMAR1 gene and schizophrenia in the Japa-nese population: a case-control study and anupdated meta-analysis. Schizophr Res.2012;141(2–3):279–80.
47. McIntyre RS, Yoon J. Efficacy of antimanic treat-ments in mixed states. Bipolar Disord.2012;14(Suppl 2):22–36.
48. Ishima T, Fujita Y, Hashimoto K. Interaction of newantidepressants with sigma-1 receptor chaperonesand their potentiation of neurite outgrowth inPC12 cells. Eur J Pharmacol. 2014;727:167–73.
49. Perneger TV. What’s wrong with Bonferroniadjustments. BMJ. 1998;316(7139):1236–8.
50. Nakagawa S. A farewell to Bonferroni: the problemsof low statistical power and publication bias. BehavEcol. 2004;15(6):1044–5.
724 Adv Ther (2017) 34:713–724