the managers and management we need to improve...
TRANSCRIPT

1
March 26, 2015
Dial In: 877.668.4493 Code: 667 160 253
The Managers and Management We Need to Improve Care
2
Having
Audio Issues?
If you experience any disruptions or other issues with audio
during today’s WIHI, we ask that you:
• Notify WIHIAdmin through the WebEx chat
• If the problem persists, notify IHI Customer Service at
617.301.4800 or [email protected]
Download resources and slides when you log off or next day on IHI.org/WIHI
Dial In: 877.668.4493
Code: 667 160 253

Getting Started
How would you identify your role in your organization?
Choose the option that best applies:
– Frontline Staff (doctor, nurse, other clinician, clinical staff)
– Middle Manager (supervisor, care manager, coordinator, team lead)
– Senior Manager (director, executive, CMO, CNO, administrator, C-
suite)
3
If you chose Middle Manager, do you have the time and
support you need from supervisors to engage in quality
activity?
– Yes
– No

4
Madge KaplanDirector of Communications
Institute for Healthcare Improvement
For resources & slides, visit IHI.org/WIHI
Dial In: 877.668.4493
Code: 667 160 253
Madge Kaplan, IHI’s Director of Communications, is
responsible for developing new and innovative means for
IHI to communicate the stories, leading examples of
change, and policy implications emerging from the world of
quality improvement ― both in the U.S. and internationally.
Prior to joining IHI in July 2004, Ms. Kaplan spent 20 years
as a broadcast journalist for public radio – most recently
working as a health correspondent for National Public
Radio. Ms. Kaplan was the creator and Senior Editor of
Marketplace Radio's Health Desk at WGBH in Boston, and
was a 1989/99 Kaiser Media Fellow in Health. She has
produced numerous documentaries, and her reporting has
been recognized by American Women in Radio and
Television, Pew Charitable Trusts, American Academy of
Nursing and Massachusetts Broadcasters Association.

5
Dave MunchHealthcare Performance Partners
For resources & slides, visit IHI.org/WIHI
Dial In: 877.668.4493
Code: 667 160 253
Dave Munch, MD, SVP & Chief Clinical Officer, Healthcare
Performance Partners (HPP) serves as the lead of all clinical and
Lean Healthcare engagements at HPP. In addition, he is an
instructor for the Belmont College Lean Healthcare Certification
program. Dr. Munch previously served at Exempla Lutheran
Medical Center as the CMO and CQO. He was an instructor for the
University of Michigan's Lean Certification Program for four years
and has served on the Agency for Healthcare Research and
Quality's High Reliability Advisory Group. Dr. Munch has an
extensive background in hospital operations, health plan
governance, physician organization governance and clinical
practice in Internal Medicine. He is on the faculty of The Institute for
Healthcare Improvement (IHI), teaching in the areas of patient
safety, leadership, and management.
You can reach Dave at [email protected]

5 Myths about Building Quality Improvement Capability
1. Building Improvement is all about learning a quality improvement methodology
2. A strong quality department is all you need to make improvement
3. Building improvement capability is too expensive
4. The quality department should own improvement
5. Executives have the most important role in making improvement

Executive Leadership
Strategy Deployment
Developing/Coaching your Managers
Leadership Standard Work (Executive)
Org Dev. & Learning
Middle & Front Line Management
Visual Management
A3 Deployment
Developing/Coaching your Staff
Leadership Standard Work (Manager)
Front Line Staff
Standard Work
Surfacing & Solving Problems
Participate in Improvement
Continuous Improvement
and Operational Excellence
Improve Process & Performance while Developing People: “Learn by Doing”
The Interlinking Responsibilities of Continuous Improvement
The Quality ImprovementStaff act as a Catalyst for
this model

• Assessment
• Analytics
• Observation
• Interviews
• Mapping
Current State
• Create Standard Work
• Reduce Variation
• Eliminate Waste
• Improve Reliability & Quality
Process Redesign • Train & Develop
• Establish:
• Management Systems
• Operational Systems
• Governance
Deploy & Control
• Establish Deployment Teams
• Manage Tempo
• Create Reporting Structures & Data Systems
Scale and Spread

Example: Pareto Chart
Example: Pareto Chart
Example: Pareto Chart
Example: Pareto Chart
Example: Pareto Chart
Root Cause Analysis
Action Plan
Follow-up
Countermeasures
Future State/Target
Test/Cost/Benefit
Current Condition
Background
Issue
ExampleA3
Root Cause Analysis
Action Plan
Follow-up
Countermeasures
Future State/Target
Test/Cost/Benefit
Current Condition
Background
Issue
ExampleA3
Root Cause Analysis
Action Plan
Follow-up
Countermeasures
Future State/Target
Test/Cost/Benefit
Current Condition
Background
Issue
ExampleA3
Root Cause Analysis
Action Plan
Follow-up
Countermeasures
Future State/Target
Test/Cost/Benefit
Current Condition
Background
Issue
ExampleA3
Root Cause Analysis
Action Plan
Follow-up
Countermeasures
Future State/Target
Test/Cost/Benefit
Current Condition
Background
Issue
ExampleA3
Patient Experience
FinancialSustainability
Quality/ SafetyPeople and
PartnersCost of Care
ParetoKey Drivers of Performance
Problem Solving
Daily ManagementProcess Metric
HistoryPerformance Over Time
Example: Run Chart
Example: Run Chart
Example: Run Chart
Example: Run Chart
Example: Run Chart
x x x x
Example: Daily data
x x x x
Example: Daily data
x x x x
Example: Daily data
x x xx
Example: Daily data
x x x x
Example: Daily data
Performance Board: Tool for Situational Awareness
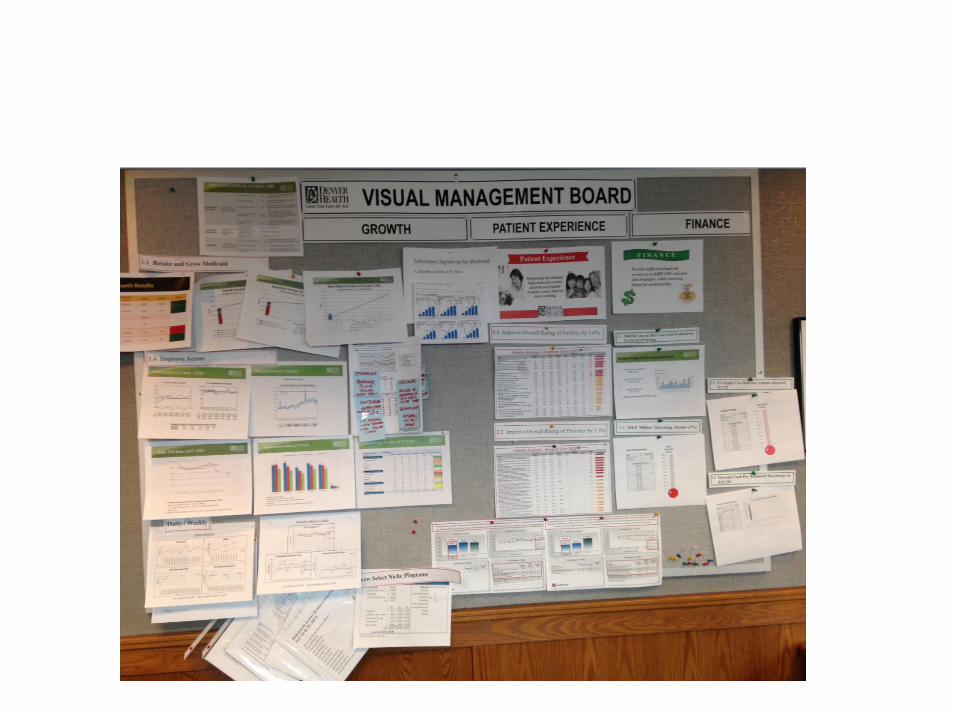
Enterprise VMB

A Story from a Middle Manager
• I work as a CN in a hyper-dynamic CVICU/Transplant unit. Just like in PICU, we are staffed with ICU nurses with very little or no CVICU experience. Due to the extreme acuity of the patients, the CN’s tend to be in “command” mode all the time. And since there is not really any time to check on delegated tasks, we tend to do everything ourselves. But I must admit, I realized very quickly that if the bedside nurses knew how to run the QC test on the ACT machine stat when they needed it in an emergency or how to operate the Defibrillator machine sufficiently during an emergency that I would not have to leave everything I am busy with to control the situation. So I started to delegate these tasks routinely to the bedside nurses to make them feel comfortable with working and touching these equipments. During this, I would sketch simple scenarios of problems that might arise and prompt them to come up with ideas of troubleshooting. This was not easy for me as I had to let go of something I was in control of. And I had to trust others to do it as well as I expect it from them. The first few times I had to let them operate the equipment was very daunting as I felt like taking over at any point but I stayed on the background and guided them verbally. Today, I can let them handle situations with this equipment in mind and not worry about it at all. This does indeed give me the extra few minutes to spend on other emergency situations

12
Stephanie CalcasolaBaystate Medical Center
For resources & slides, visit IHI.org/WIHI
Dial In: 877.668.4493
Code: 667 160 253
Stephanie Calcasola, MSN, RN-BC, is the Director of Quality and
Medical Management at Baystate Medical Center. She has held a
variety of clinical and leadership positions over the last twenty
years including cardiac staff nurse, educator, nurse manager, and
clinical nurse specialist. In her current role, she is accountable for
the strategic planning, program development and operations for
clinical quality, patient experience and patient safety programs for
Baystate Medical Center. Her work has helped to transform care at
Baystate Medical Center, a nationally recognized leader in hospital
quality. Ms. Calcasola speaks nationally on issues of healthcare
quality, and is published in peer reviewed journals.
You can reach Stephanie at

Healthcare Middle Manager like Roles
Clinical Supervisor
Lead Clinician
Manager/Assistant Manager
Employees advancing in recognition programs (high potentials)
Triage Coordinator
Care Manager/Coordinator
Leadership should be seen as a dimension of practice for all nurses, not just those in formal
leadership role (Scott & Miles, 2013)

IHI’s Leading Quality Improvement: Essentials for Managers, 2014

Baystate Medical Center Building Improvement Capacity
Improvement Expeditions/Projects
Unit Manager/Quality Mentoring Program
Manager/Medical Director Dyad Leadership Development
Easy access to improvement toolkits
Consultation Model

IHI’s Leading Quality Improvement: Essentials for Managers, 2014
17
Kedar MateInstitute for Healthcare Improvement
For resources & slides, visit IHI.org/WIHI
Dial In: 877.668.4493
Code: 667 160 253
Kedar Mate, MD, Senior Vice President, Institute for Healthcare
Improvement (IHI), oversees the development of innovative system
designs to implement high-quality health care both in the United
States and in resource-limited settings abroad. He is also IHI’s
regional lead for the Middle East and Asia-Pacific regions.
Previously, he served as Country Director for the IHI South Africa
Program and he continues to be engaged in IHI’s work in this area.
Dr. Mate is an internal medicine physician, an Assistant Professor
of Medicine at Weill Cornell Medical College, and a Research
Fellow at Harvard Medical School's Division of Global Health
Equity. He advises numerous international initiatives aiming to
strengthen health systems to improve delivery of HIV, tuberculosis,
and maternal and child health services.
You can reach Kedar at [email protected]
Identifying Roles
Which role description best matches what you do as a middle manager? – Implementer
– Synthesizer
– Influencer
– Adapter
18

What makes a MM unique?
• “The distinguishing feature of middle management is not where they sit in the organization chart. What makes them unique is their access to top management coupled with their knowledge of operations. This enables them to function as mediators between the organization’s strategy and day-to-day activities”
– Wooldridge, Schmid & Floyd, 2008, p. 1192
• Strategy to operations is the essence of being middle manager.

Key functions of a MM
DivergentIntegrative
Upward
Downward
Information Synthesizer
ChampioningAlternatives
FacilitatingAdaptation
EnsuringImplementation
Floyd, S., & Woodridge, B. (1994). Dinosaurs or dynamos? Recognizing middle management’s strategic role. Academy of management executive, 8 (4), 47-57.
Marichal, K & Segars J. Leading from the Middle 2012 Antwerp Management School


Your Quality Department doesn’t have to go it alone!
Join Passport to accelerate your efforts to improve patient care and engage staff. The benefits of a $5,000 yearlong membership include:
• Unlimited participation in Expeditions (two- to four-month, web-based programs
• Registration for Leading Quality Improvement: Essentials for Managers
• A 25% IHI Open School online course subscription discount
• A 15% IHI National Forum discount
http://www.ihi.org/Passport

Find Us at23
Thanks to everyone who makes WIHI possible!

Next up on WIHI:
April 9, 2015: All Hands on Deck to Reduce C. Difficile
April 23, 2015: Reducing Risks and Defects With Help From the Frontlines
For more information, visit IHI.org/WIHI