the medical model lecture two: addiction let’s look at the mast
TRANSCRIPT

The Medical Model
LECTURE TWO: ADDICTION

Let’s Look at the MAST

Michigan Alcoholism Screening Test (MAST)
Scoring the Mast
For each yes give yourself the score indicated except for questions 1,4, and 8.
For 1,4, and 8, give yourself the score indicated if you give A NO Answer
Zero points for a Yes answer 1,4,8.
•12 or more points indicates a problem with alcoholism •5 and 10 suggestive of problem at risk

DSM IV-TR Criterion for: Alcohol Dependence - Diagnostic Code 303.90
A maladaptive pattern of alcohol use, leading to clinically significant impairment or distress, as manifested by three (or more) of the following, occurring at any time in the same 12-month period:
(1) tolerance, as defined by either of the following: (a) a need for markedly increased amounts of alcohol to achieve Intoxication or desired effect (b) markedly diminished effect with continued use of the same amount of alcohol
(2) Withdrawal, as manifested by either of the following: (a) the characteristic withdrawal syndrome for alcohol (b) alcohol (or a closely related drug such as valium) is used to relieve or avoid withdrawal symptoms
(3) alcohol is often used in larger amounts or over a longer period than was intended

DSM criteria (cont.)4) there is a persistent desire or unsuccessful efforts to cut down or control alcohol use
(5) a great deal of time is spent in activities necessary to obtain alcohol, use alcohol, or recover from its effects (6) important social, occupational, or recreational activities are given up or reduced because of alcohol use
(7) alcohol use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by alcohol

Specifiers With Physiological Dependence: evidence of tolerance or withdrawal
(i.e., either Item 1 or 2 is present)
Without Physiological Dependence: no evidence of tolerance or withdrawal (i.e., neither Item 1 nor 2 is present)
(Note--a diagnosis of Alcohol Dependence can never be changed to a diagnosis of Alcohol Abuse. A diagnosis of Alcohol Dependence is for life--it can never be removed from your medical chart not matter how much you improve.)

Why do people abuse chemicals?
The simplest answer is because it feels good!
But why then are we not all addicts?

Is it not a choice?
What do folks think?

Is it simple a choice?
Is it simple a choice?

Physical reward potential
Increased sense of pleasure
Decreased discomfort
Thus I use again and again
Pleasure center is not one a single center
Pleasure center across brain systems
Motivated to seek further stimulation

Social Learning Component
We learn how to use drugs and substances
In order to maximize their potential both physically and psychologically.
Individual Expecta
tion of
Drug/Alco
hol / Substa
nce
Individual Expecta
tion of
Drug/Alco
hol / Substa
nce

Cultural influences on chemical use patterns
People’s decision to use or not can be a result of the community, subculture, family, and social group, to which you belong.
Peele [1985] holds that “cultures where use of a substance is comfortable, familiar, and socially regulated both as to style of use and appropriate time and place for such use, addiction is less likely and maybe practically unknown”.
And yet with new emerging addictions this may not hold as true as it did 20 years ago!
What is Peele Smoking?
We also can’t forget social groups within a culture

Individual Life Goals
Present Future
Past
• It’s Important to remember that chemical abuse patterns are not fixed
• Moreover, no one sets out to become addicted

or Disease Model
MEDICAL MODEL OF ADDICTION

Basic Tenet: Medical Model / Disease Model A great deal of the individuals behavior is based
on predisposition
However, there is no universally accepted disease model that explains addiction
Instead there exists loosely related theories that addiction is (unproven) a psycho-biomedical process that can be called a disease state.

Otto Jellinek (1952) Influenced physicians
Shifted from moral disorder to medical disorder
Became recognized as formal disease in 1956 (by the AMA)
Proposed alcoholism to be a progressive / predictable disorder
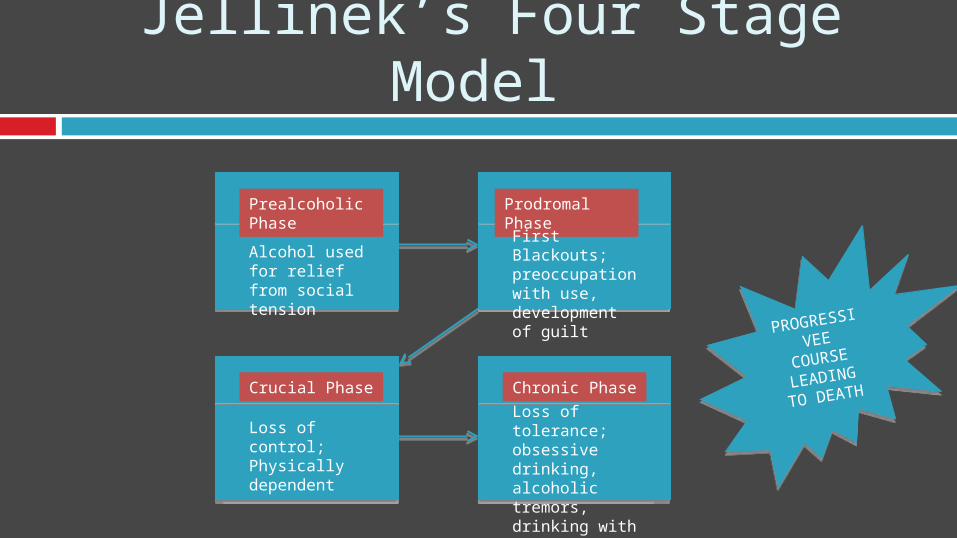
Jellinek’s Four Stage Model
Prealcoholic Phase
Prodromal Phase
Crucial Phase Chronic Phase
Alcohol used for relief from social tension
First Blackouts; preoccupation with use, development of guilt
Loss of control; Physically dependent
Loss of tolerance; obsessive drinking, alcoholic tremors, drinking with social inferiors
PROGRESSI
VEE
COURSE
LEADING
TO DEATH
PROGRESSI
VEE
COURSE
LEADING
TO DEATH

Jellinek’s Additions Later classified different types of alcoholics One hallmark of the alcoholic – they can’t
predict how much they will drink after starting
His legacy – something worth studying (brain/biology)
Removes prejudices “the immoral alcoholic” Wasn’t about will power was a “disease”

Genetic Inheritance Theories Less sensitive to alcohol
effects – (less neuronal firing)
Like / dislike certain substance(s)
Decision making (frontal cortex)
Make it harder to quit
Affect withdrawal syndrome
Different studies suggest that genes account for 20% to 58% of addiction risk
No signal gene causes addiction
Vulnerability not Destiny

Cloninger’s Type 1 and Type 2 Alcoholics 3,000 adoptees
Reared by non-alcoholic parents
Great deal of adoptees became alcoholic
Cloninger observed two distinct groups

Type 1 (larger subgroup) ¾ children had
biological parents who were alcoholic
These children drank in moderation in early adulthood
Later life developed dependence
Functioned in society as responsible adults
If raised in higher socio economic family less likely to become alcoholic

Type 2 Males
More violent than Type 1
Father’s were violent alcoholics
20% chance of becoming alcoholic regardless of SES
Later studies confirmed findings
10% of sample became alcoholics
Low Levels of MAO

Neuro-Biological Processes, Dopamine, and Drug Addiction
Addicts are biologically different from non-addicts
An addict’s brain acts differently before and after using
Addicts metabolize and bio-transform substances differently

Ego States and the Characterlogical Model of Addiction Personality and its relationship with self and
world (internal and external)
How we then deal with world
Addiction then helps to self-regulate via pharmacologic effects, attendant rituals, practices, and drug culture