the microvascular disease conundrum
TRANSCRIPT
THE MICROVASCULAR DISEASE CONUNDRUM:
WHO SHOULD I REFER FOR EVALUAT ION , WHAT TESTS WILL THEY PERFORM, AND WHAT TREATMENTS MIGHT
THEY OFFER
Jennifer A Tremmel, MD, MSStanford University Medical Center

Disclosures
Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below
Abbott: Advisory Boards, Honorarium Boston Scientific: Advisory Boards, Honorarium, Research Terumo: Honorarium
Microvascular Dysfunction (MVD) Angina + normal cors ≠ MVD Angina + normal cors = several different etiologies MVD can be used as a working diagnosis and one can try
empiric treatment, but if not helping, consider testing There are different testing options for MVD
– Non-invasive and invasive MVD is evolving as a broader term for disorders of the
coronary microvasculature– Structural=plugged up, loss of density/Functional=dysregulation of vasomotion
MVD occur in obstructive/non-obstructive CAD, as well as SIHD/ACS
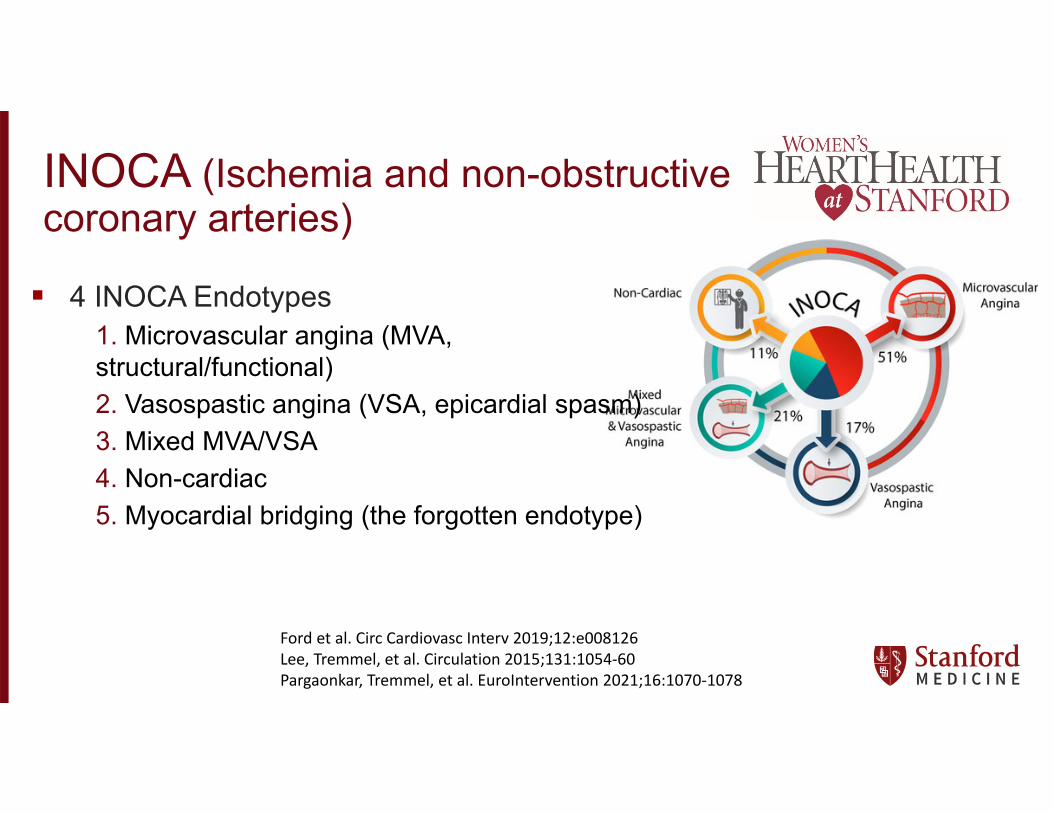
INOCA (Ischemia and non-obstructive coronary arteries)
4 INOCA Endotypes1. Microvascular angina (MVA, structural/functional)2. Vasospastic angina (VSA, epicardial spasm)3. Mixed MVA/VSA4. Non-cardiac5. Myocardial bridging (the forgotten endotype)
Ford et al. Circ Cardiovasc Interv 2019;12:e008126Lee, Tremmel, et al. Circulation 2015;131:1054‐60Pargaonkar, Tremmel, et al. EuroIntervention 2021;16:1070‐1078
Who are these patients? Usually normal people with typical (62%) or atypical (38%) angina for
>3 months (more commonly years)—more often women than men (3:1)
Don’t have other causes of angina (pulmonary hypertension, hypertrophic/other cardiomyopathy, valvular heart disease, myopericarditis, etc)
They’ve typically had at least one, and generally multiple stress tests, and often coronary angiography (≥1x)
They’ve generally been tried on several cardiac medications
They have been told nothing is wrong, but they continue to be limited by angina
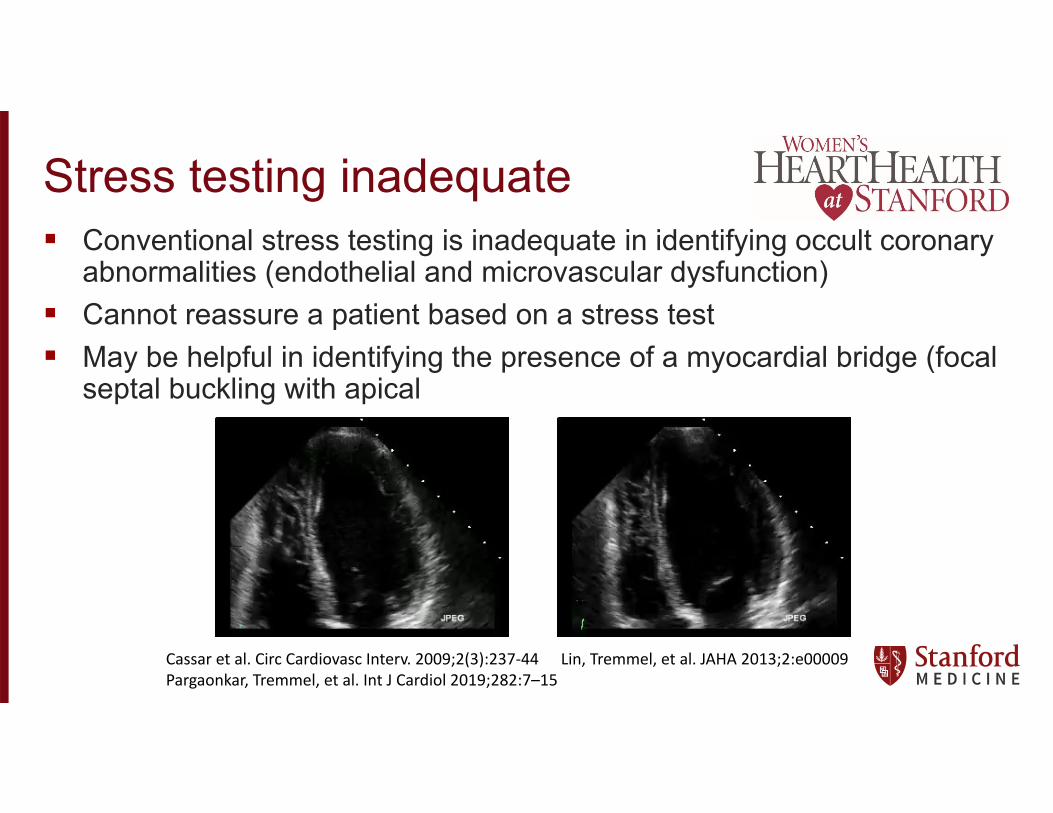
Stress testing inadequate Conventional stress testing is inadequate in identifying occult coronary
abnormalities (endothelial and microvascular dysfunction) Cannot reassure a patient based on a stress test May be helpful in identifying the presence of a myocardial bridge (focal
septal buckling with apical
Cassar et al. Circ Cardiovasc Interv. 2009;2(3):237‐44 Lin, Tremmel, et al. JAHA 2013;2:e00009Pargaonkar, Tremmel, et al. Int J Cardiol 2019;282:7–15
Case
50 yo perimenopausal woman with no significant cardiac risk factors who has had chest pain for ~3 years
Reports that chest pain has been progressive over time to now daily Describes chest pain as occurring both with exertion and at rest (often
with emotional stress), and associated with dyspnea– Negative stress test– Negative angiogram– Multiple ER visits– Initially told that her symptoms were anxiety, then MVD/spasm– Tried on amlodipine, nitrate, and Coreg, with no significant change in
symptoms
What tests get done? Testing varies by:
– What is done—Epicardial spasm only, MVD only, IVUS, myocardial bridge testing
– What wires are used—Doppler wire, thermodilution wire, no wire– What drugs are used—Ach, ergonovine, adenosine, dobutamine/atropine
(and in what order)– How the drugs are given—IV, IC, through guide vs microcatheter, bolus vs
infusion– What doses are used—Ach (20mcg to 200 mcg), for example
Pargaonkar, Tremmel et al. Int J Cardiol 2019;282:7–15Pargaonkar, Tremmel et al. Circ Cardiovasc Intrv 2020;13:e008587
Femoral access, no obstructive CAD
Ach testing
The patient developed chest pain, but no EKG changes with Ach
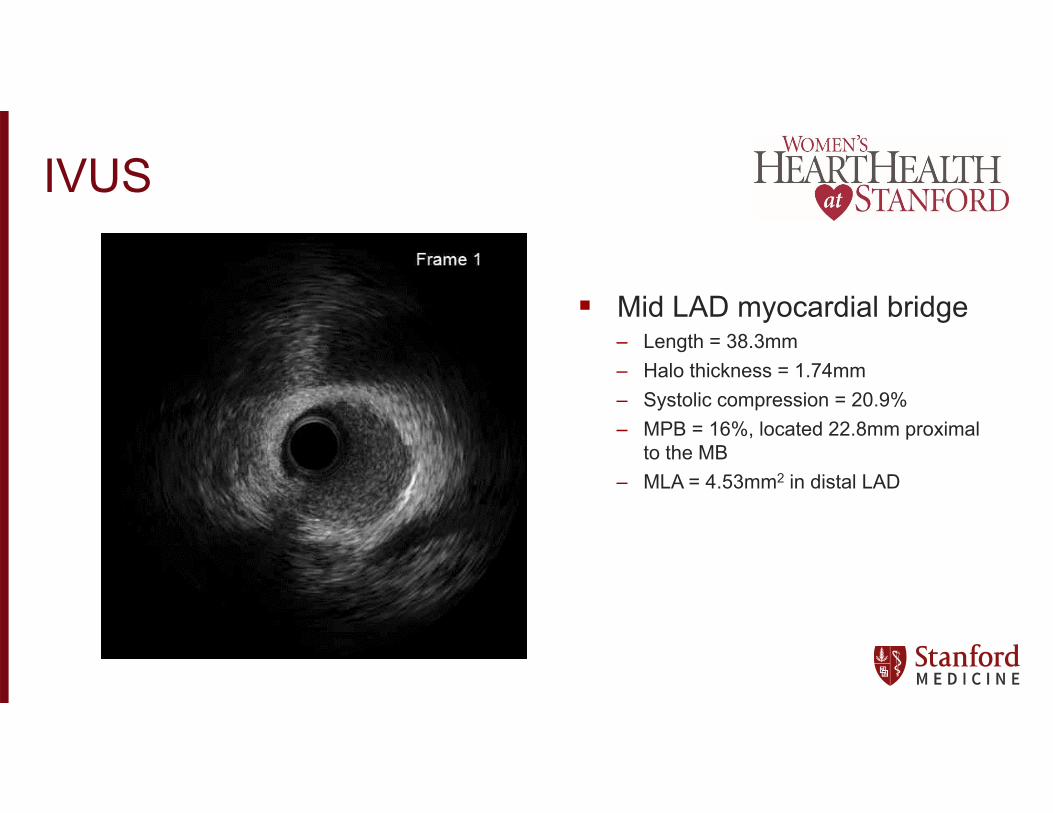
IVUS
Mid LAD myocardial bridge– Length = 38.3mm– Halo thickness = 1.74mm– Systolic compression = 20.9%– MPB = 16%, located 22.8mm proximal
to the MB– MLA = 4.53mm2 in distal LAD
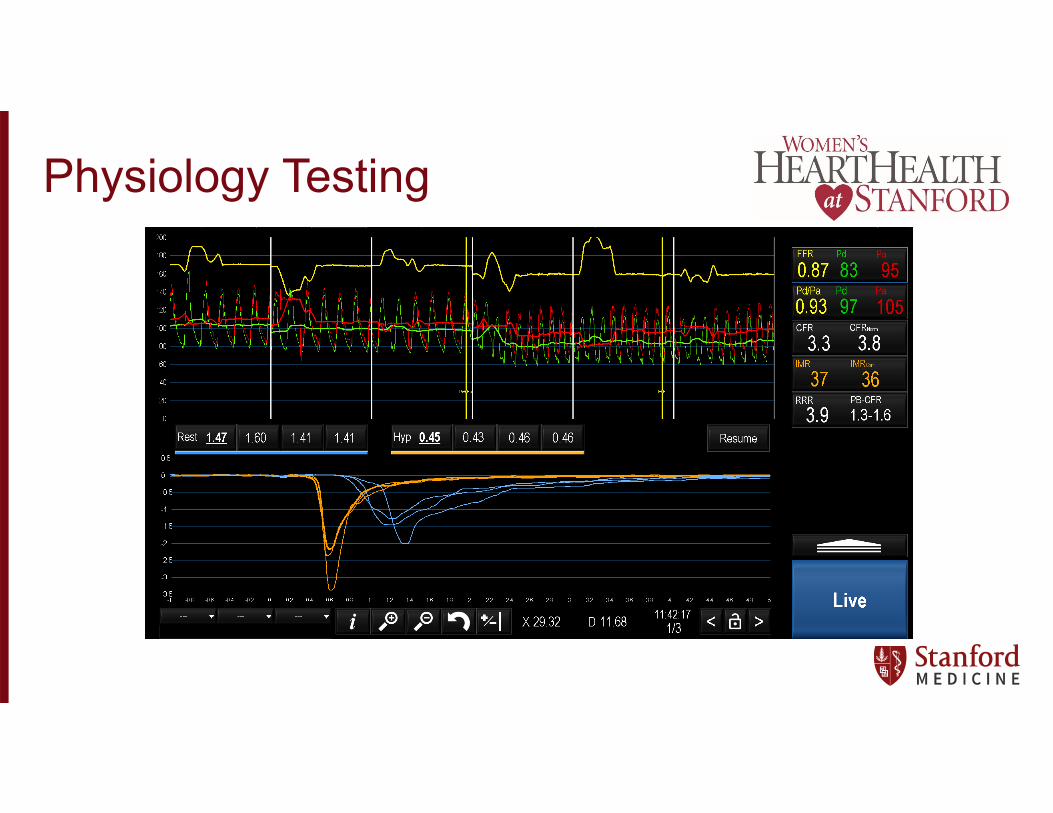
Physiology Testing
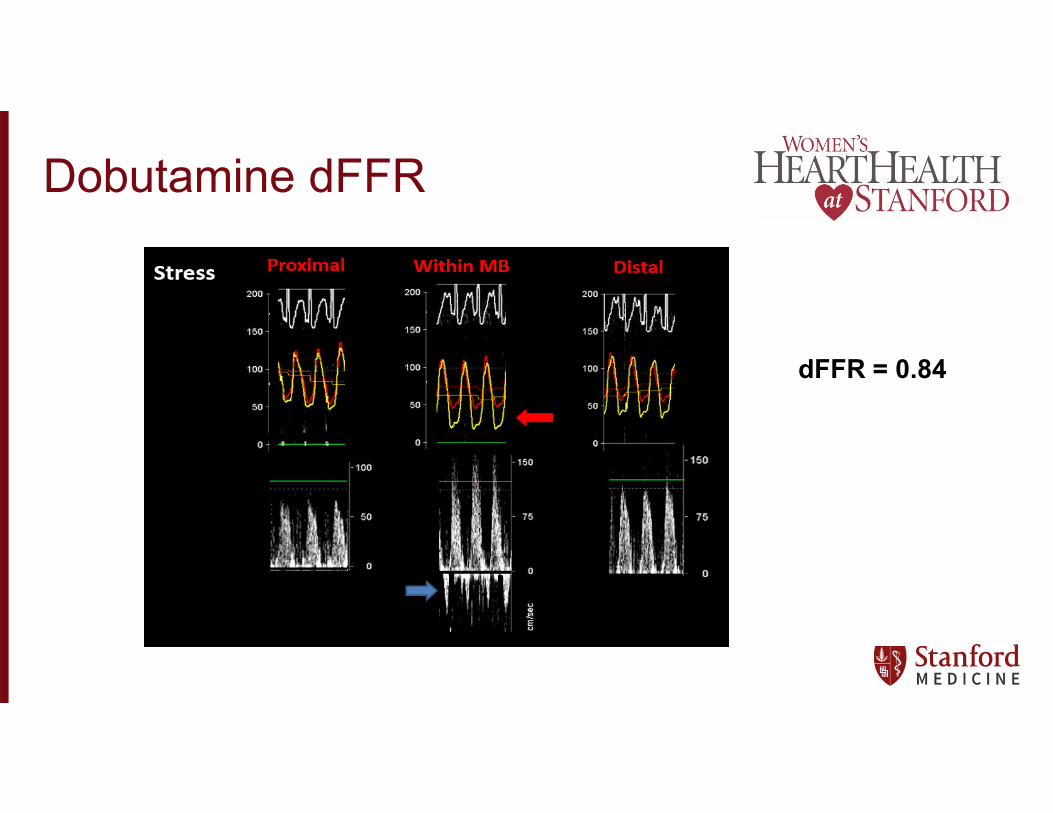
Dobutamine dFFR
dFFR = 0.84
How to treat? Testing will identify at least 1 diagnosis in ~75% of patients Treatment varies
– Microvascular dysfunction Nebivolol, ACE-inhibitors, Ranexa
– Vasospasm (epicardial or microvascular) Nitrates, CCB
– Myocardial Bridging Beta-blockers (nebivolol =/- nitrate if concomitant spasm), CCB Surgical unroofing
– Beneficial to endothelium/MB patients Statins Aspirin
All patients should get lifestyle modification—diet, exercise, weight loss, stress reduction
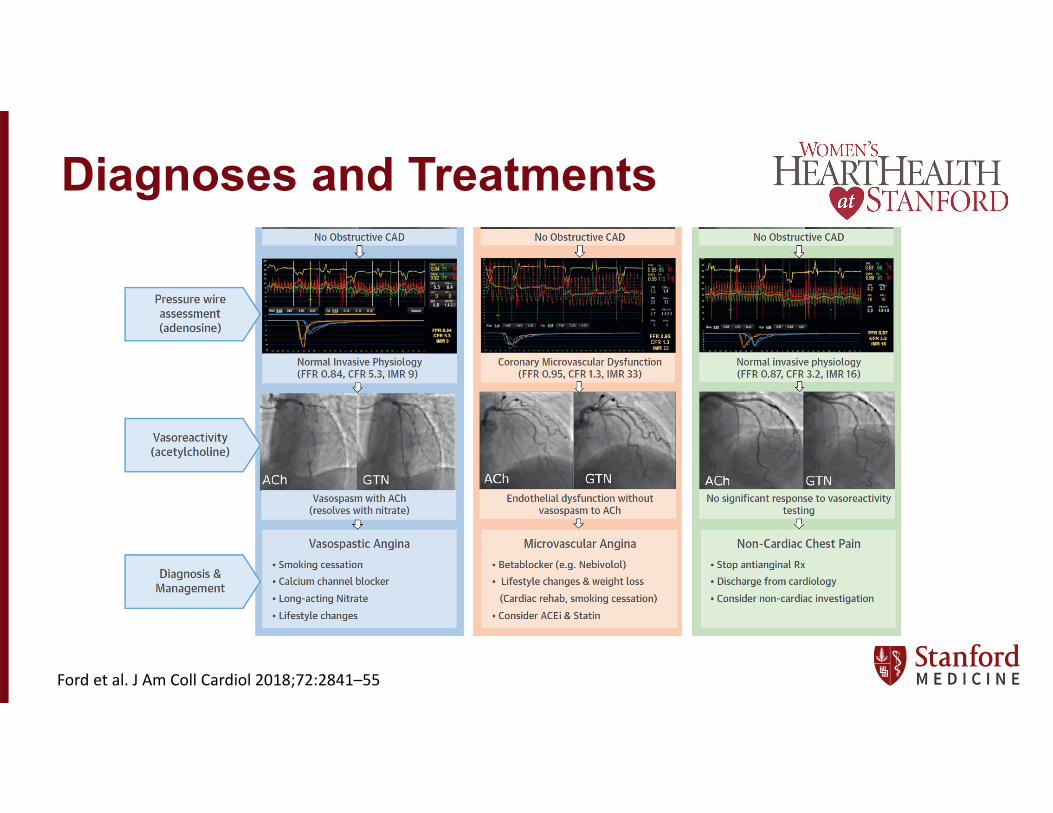
Diagnoses and Treatments
Ford et al. J Am Coll Cardiol 2018;72:2841–55
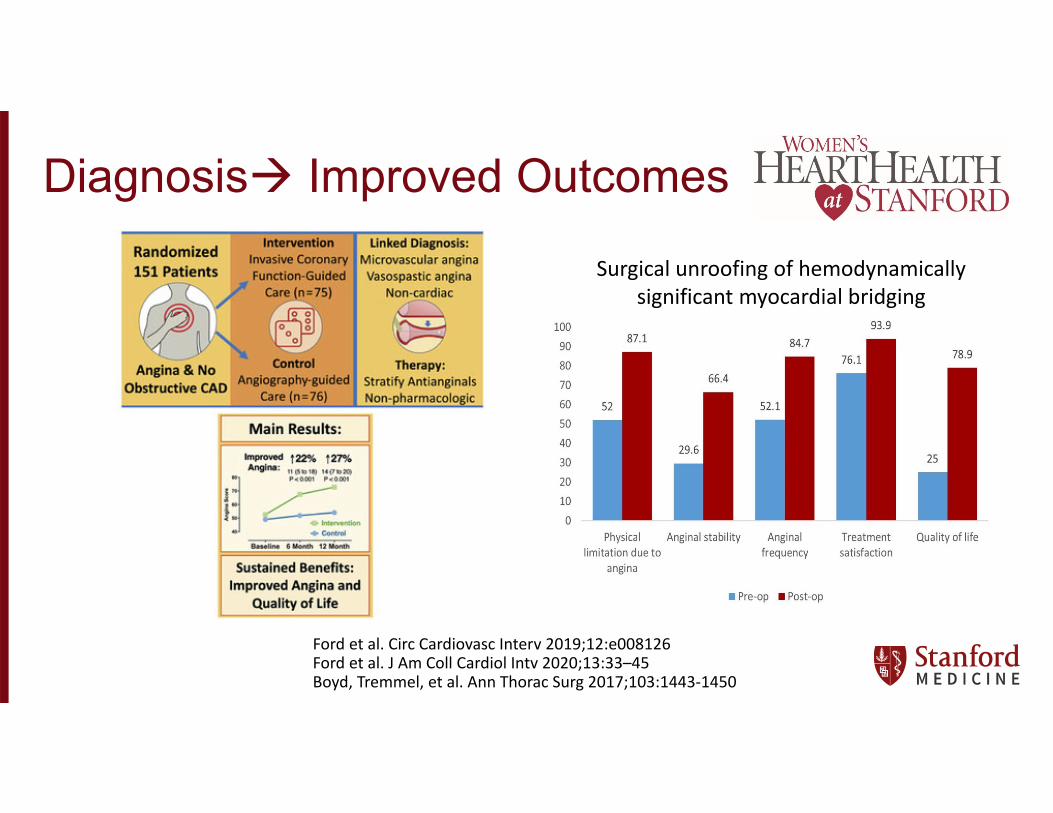
Diagnosis Improved Outcomes
Surgical unroofing of hemodynamically significant myocardial bridging
Ford et al. Circ Cardiovasc Interv 2019;12:e008126Ford et al. J Am Coll Cardiol Intv 2020;13:33–45Boyd, Tremmel, et al. Ann Thorac Surg 2017;103:1443‐1450
Conclusions Angina + normal cors ≠ MVD Angina + normal cors = INOCA (ANOCA) Symptoms sound pretty typical, stress testing may be normal There are several causes of INOCA/ANOCA
– Microvascular dysfunction (structural or functional)– Endothelial dysfunction/epicardial spasm– Myocardial bridging
Diagnosis typically requires invasive testing Getting a diagnosis guides management and improves outcomes