the patient with ahf on the icu : respiratory support
TRANSCRIPT
THE PATIENT WITH ACUTE HEART FAILURE ON THE ICU
RESPIRATORY SUPPORT Josep Masip, MD, PhD, FESC
Associate Professor of CardiologyUniversity of Barcelona
ICU DepartmentH. Sant Joan Despí Moisès Broggi
Consorci Sanitari Integral
Cardiology Department Hospital Sanitas CIMA Barcelona
HOSPITALCIMA
NO CONFLICT OF INTEREST

ALARM Trial
Follath et al. Intensive Care Med 2011
4.953 Patients 2.247 ICU 1.475 CCU 1.231 wards
75%

Esteban A, et al. JAMA 2004
INTERNATIONAL ICU SURVEY
5.183/ 15.757 33%Mechanical Ventilation
539 (10.4%) Cardiac Failure100 (1.9 %) Cardiac Arrest
12 % Cardiac reasons

Diagnosis on admission n= 6415ACS 69 %Acute Heart Failure 11 % Other* 20 %
Reasons for Invasive MV n=633 Complicated ACS 35 %AHF 25 %Cardiac Arrest 17 %Arrhythmia 11 %Other: 12 %
Reasons for NIV n=194Complicated ACS 34 %AHF 55 %Other: 11 %
Catalunya Survey on Ventilatory Support in the CICU
(*) Acute aortic syndromes, Arrhythmia-AV block, Post Cardiac Arrest; CICU: Cardiovascular Intensive Care Unit; ACS: Acute coronary syndromes; IMV: Invasive mechanical ventilation; NIV: Noninvasive mechanical ventilation; AHF: Acute heart failure
12%

Intensive Care Units• Acute respiratory failure (65%)
• Pneumonia• Sepsis • Trauma
• Surgical complications• Heart failure• ARDS
• Coma • COPD• Neuromuscular disorders• Postoperative high risk interventions
MAIN DISEASES TREATED WITH MV ACCORDING TO THE TYPE OF ICU
Masip J. Mechanical ventilation in AHF. In A. Maisel book 2013
Cardiovascular Intensive Care Unit• Cardiogenic shock (ACS or myocarditis)• Acute pulmonary edema• Cardiorespiratory arrest• Postoperative cardiac surgery
10-20%
30-40%

AHF population managed in the CICU
• Acute Pulmonary Edema
• Acute Coronary Syndrome complicated with AHF
• Cardiogenic Shock
• Cardiac Arrest
• AHF during weaning
• AHF with unstable arrhythmia
• Acute right ventricular failure
• AHF in sepsis and ARDS
• AHF Post Cardiac Surgery

IN THE ICU THESE PATIENTS
SHOULD BE TREATED WITH NONINVASIVE VENTILATION
• Continuous positive airway pressure (CPAP)
• Pressure support ventilation (NIPSV)
Bilevel (BIPAP)
ACUTE PULMONARY EDEMA

Cui-Lian Weng. Ann Intern Med. 2010;152:590-600;
CPAP
Bilevel
56% Reduction
44% Reduction
INTUBATION

Cui-Lian Weng. Ann Intern Med. 2010;152:590-600;
CPAP
Bilevel
36% Reduction
n.s.
MORTALITY

High-flow oxygen administered via nasal cannula connected to heated humidifiers
Carratala JM et al. Rev Esp Cardiol 2011
Flow : up to 60 l/min.

Patients with PaO2/FiO2 < 200mmHg
OverallPopulation
High-Flow Oxygen through Nasal Cannulain Acute HypoxemicRespiratory Failure
Frat J.P et al. NEJM 2015

High-Flow Oxygen through Nasal Cannulain Acute Hypoxemic Respiratory Failure
Frat J.P et al. NEJM 2015

Adaptative Servo-Ventilation (ASV)
Hypopnea
Pressure
Flow
Nakano S, et al. Eur Heart J Acute Cardiovasc Care 2014
58 patients APE were succesfully treated with ASV

CPAP
Oxygen Therapy in AHF
PS-PEEPInitial signs of fatigue
↑CO2 ↓pHSigns of CPAP failure
Upright positionPre-Hospital
orEmergency Room
SpO2<90%RR>25
↑ Work of breathingOrthopnea YesNo
RESPIRATORY DISTRESS (▲) ?
After blood gasesNo
Room air
After 60-90 min
Conventionaloxygen therapy
FAILURESUCCESSWeaning
(▲)
Intolerance
Yes
SIGNIFICANT HYPERCAPNIA AND ACIDOSIS
CPAP
In hospitalRESPIRATORY DISTRESS () ?
Blood gases
Conventionaloxygen therapy
Intubation
Intubation
() Same criteria than initially, although SpO2 may be >90% if FiO2 is high

Masip J. Eur Heart J: Acute Cardiovasc Care 2012
Venous blood gases in patients with APE

Masip J et al. Eur Heart J: Acute Cardiovasc Care 2012
Venous vs Arterial gas samples

AHF in ACS
18-30% of the patients show some degree of AHF

Masip J et al. Rev Esp Cardiol 2012
SpO2 and Killip Classification

Masip J et al. Rev Esp Cardiol 2012
SpO2 and Radiology Score
RR=19RR=20
RR=21
RR=24
RR=26
SpO2 ≤ 92 %

AVOID Trial


Individual Data for CBF and CVR in Subjects During Sequential Room Air and 100% Oxygen Breathing
McNulty et al. Am J Physiol Heart Circ Physiol 2005
Hyperoxia

Pulsed Doppler Recording of LAD in Healthy Subjects and Cardiac Transplant Patients
Coronary blood flow

Wanga Ch.H et al Ressuscitation 2014
20.223 participants

SHOCK Trial
Hochman J et al. NEJM 1999
Mechanical ventilation (78 %)
Mechanical ventilation (88 %)
83%
CARDIOGENIC SHOCK

CARDIOGENICSHOCK
INOTROPIC and VENTILATORYSUPPORT
ECMO
IABP
Ventricular Assist Devices
Recovery Trasplant Destination
Revascularization

Hongisto M (1), Lassus J (2), Tarvasmäki T (3), Tolppanen H (2), Sionis A
(4), Köber L (5), Parissis J (6), Spinar J (7), Banaszewski M (8), Cardoso JS (9), Metra M (10), DiSomma S (11), Tolonen J (3), Masip J (12), Harjola V-P
(1)for the CardShock study investigators
Invasive vs. non-invasive ventilation in cardiogenic shock
(1) Helsinki University Central Hospital, Division of emergency care, Department of medicine, Helsinki, Finland; (2) Helsinki University Central Hospital, Heart and Lung Center, Division of Cardiology, Helsinki, Finland; (3) Helsinki University Central Hospital, Department of medicine, Helsinki, Finland; (4) Hospital de la Santa Creu i Sant Pau, Department of Cardiology, Barcelona, Spain; (5) Rigshospitalet - Copenhagen
University Hospital, Division of Heart Failure, Pulmonary Hypertension and Heart Transplantation, Copenhagen, Denmark; (6) Attikon University Hospital, Heart Failure Clinic and Secondary Cardiology Department, Athens, Greece; (7) University Hospital Brno, Department of Internal Medicine and
Cardiology, Brno, Czech Republic; (8) University of Porto, Department of Cardiology, São João Hospital, Porto, Portugal; (9) National Institute of Cardiology, Intensive Cardiac Therapy Clinic, Warsaw, Poland; (10) University of Brescia, Department of Experimental and Applied Medicine, Cardiology, Brescia, Italy; (11) Sapienza University of Rome, Department of Emergency Medicine, Sant'Andrea Hospital, Rome, Italy; (12) University of Barcelona, Hospital Sant Joan Despí Moisès Broggi, Critical Care Department,
Consorci Sanitari Integral, Barcelona, Spain

CLINICAL CHARACTERISTICS
220 patients included
• Those 58 (26%) treated only with oxygen mask/nasal cannulas were excluded
• 8 NIV patients were intubated (= NIV-failure) Ø3 within first 24 hours, 5 after that
* P-value NS for all

* values are mean
Clinical presentation MV NIV p-valueblood pressure (mmHg) * 78/46 82/49 NSheart rate (bpm) * 92 86 NSLVEF (%) * 32 32 NSconfusion (%) 83 36 < 0.001
Laboratory tests lactate, mmol/l * 4.9 2.9 < 0.001TroponinT, ng/l * 5081 7892 0.023NT-proBNP, pg/l * 7727 11115 0.041
Use of vasoactive drugs 0-24 h (%) Noradrenaline 85 68 0.031Adrenaline 28 0 Dobutamine 57 14 < 0.001Levosimendan 20 57 < 0.001
CLINICAL PICTURE AND BIOCHEMISTRY ON ADMISSION, VASOACTIVE TREATMENT
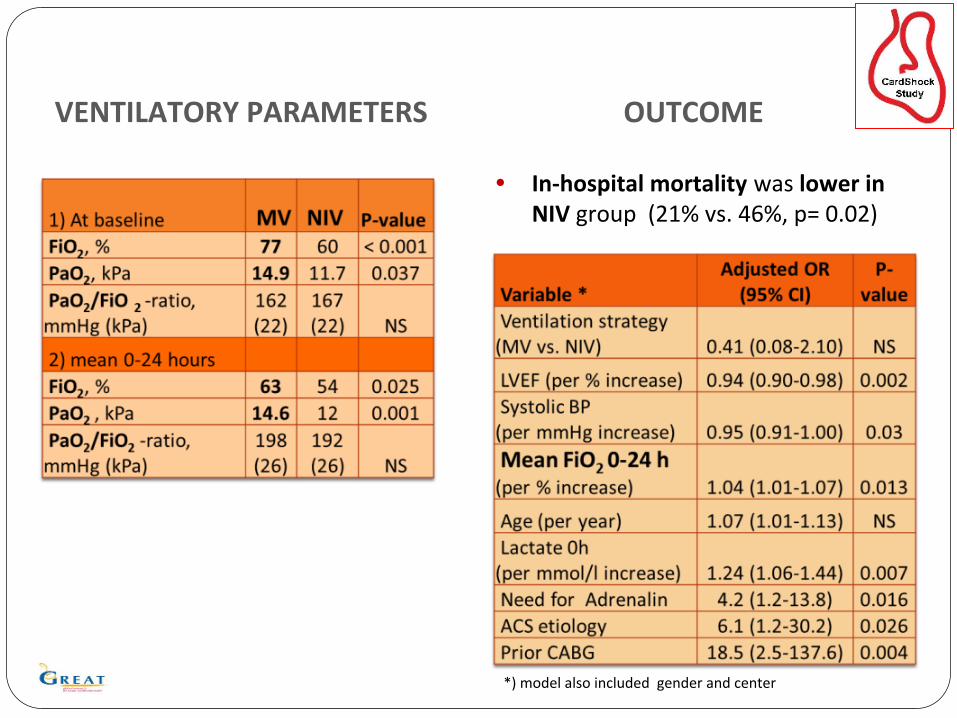
VENTILATORY PARAMETERS
• In-hospital mortality was lower in NIV group (21% vs. 46%, p= 0.02)
OUTCOME
*) model also included gender and center

• 13 % were treated with NIV
• In-hospital mortality was lower in NIV group
• NIV seems to be a safe option for properly chosen cardiogenic shock patients
• Mean FiO2 0-24 h was an independent predictor
CONCLUSIONS OF NIV IN SHOCK

Crucial moments in patients with heart diseasewho require invasive mechanical ventilation:
Intubation
Weaning
Invasive ventilation

Urgent
Elective
85%
Pre-hospital
In-hospital
60%
Kouraki K et al, BEAT registry. Clin Res Cardiol 2011
N=458 MV patients
Intubation scenario in patients with AMI
2001-2002
Mortality 48%
Pre-hospitalIn-hospital
66%
Ariza et al EHJ Acute Cardiovasc Care 2013
MV IN THE PCI ERA
N= 1821 patients 106 (5.8%) required IMV
In hospital mortality: 29%
2010 - 2012

Heart failure Shock Cardiac arrest n=27 n=14 n=65
Age 68 69 58 .000Diabetes 59 43 22 .002HTA 82 86 46 .001Smoker 26 21 83 .001In hospital ETI (%) 63 54 16 .001Swan Ganz (%) 37 36 14 .024IABP (%) 56 50 15 .001Renal RT (%) 15 15 2 .030Hypothermia (%) 37Major bleeding (%) 11 29 3 .006Transfusions (%) 26 36 11 .032In H mortality (%) 22 43 33 0.4Mortality (%) 41 43 33 0.4Non-card. mortality 36 17 52 0.2
Ariza A et al Eur Heart J Acute Card Care 2013

PREVENTIVE NIV IN PRIMARY PCI

WEANING
Simple weaning: weaning to successful extubation on the first attempt
Difficult weaning Patients who fail initial weaning and require up to 3 SBT or as long as 7 days from the first SBT
Prolonged weaning Fail at least 3 weaning attempts or require >7 days of weaning after the first SBT
Spontaneous Breathing Trial (SBT)30-120 min
PROTOCOL OF WEANING

Cabello B, et al. Intensive Care Med (2010)
PCWP: 21 mmHgPCWP: 17 mmHgResp. rate:19 b/m
Resp. rate:27 b/m
Ptients with difficult weaning
Lower Tidal volumeHeart failure may be responsible for nearly 40% of SBT failures in the ICU with general population, but is higher in the CCU
Mechanisms: myocardial ischemia excessive increased LV afterload increased cardiac preload

Swan-Ganz catheterPICCO
Echocardiography
The diagnosis of HF may be confirmed by measuring the elevation of PCWP or less invasive tools: such as echocardiography, measurements of plasma protein concentration or biomarkers.
Use of diuretics, nitrates, NIV or inotropes should be considered after careful analysis of the main contributing mechanisms.

BaselineBNP > 263 ng/L NTproBNP > 1,343 ng/Lare predictive HF
An increase in :BNP 48 ng/LNTproBNP 21 ng/L are diagnostic of HF
100 patients for SBT32 failed:12 (38%) for Heart Failure
Zapata L et al ICM 2011
CARDIAC BIOMARKERS IN WEANING

Impact of negative balance in the success of weaning
Upadya A et al. Intensive Care Med 2005
Weaning Failure
Weaning Success
ml

Conclusions
Patients who require ventilatory support in the CICU are particularly different than those in the ICU
NIV should be considered in the majority of patients with AHF and ARF, even in some with cardiogenic shock
Hyperoxia should be avoided
Adequate protocols for intubation, ventilation and weaning are crucial for the success

Thank you for your attention