the role of dcb in sfa subintimal tracking lesion
TRANSCRIPT

The role of DCB in SFA subintimal tracking lesion
Wei-chun Chang M.D. Wen-Lieng Lee, MD, PhD
Cardiovascular Center, Taichung Veterans General Hospital, Taiwan R.O.C
Disclosure
Speaker name:
.................................................................................
I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest

Clinical Evidence
• From literature review: IMPACT SFA 2-year outcome and LEVANT2 , DCB in FPD diastase is promising but all lesions are intra-luminal approach.
• The data about DCB effect in SFA subintimal tracking lesion is very limited.
DCB Sub-intimal Potential Performance
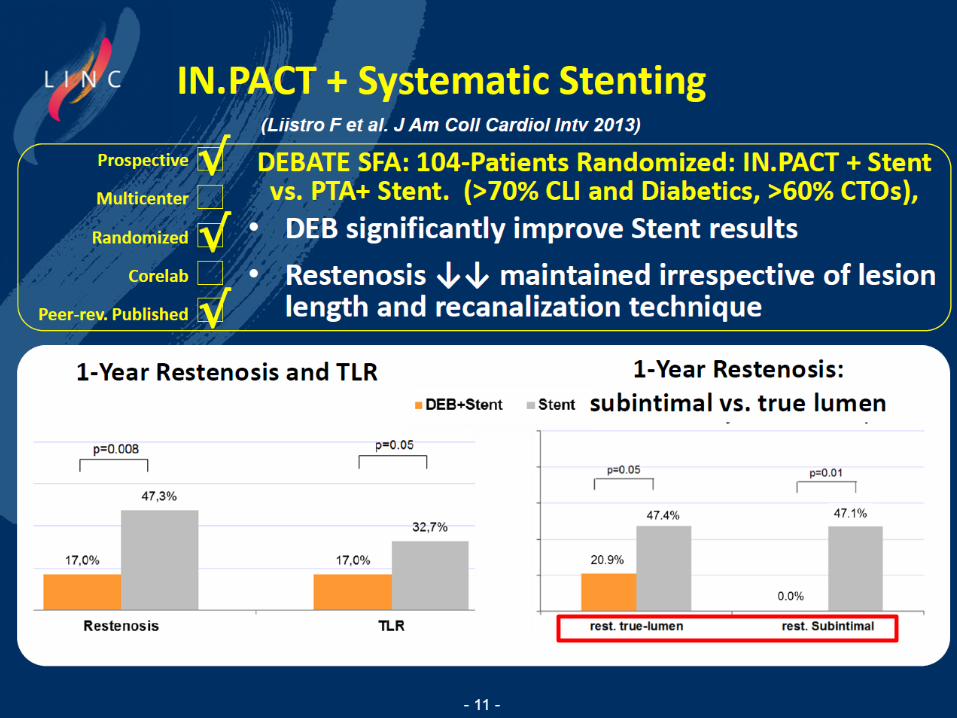
DCBATE-SFA Randomized Trial

Drug-Eluting Balloon in Peripheral Intervention for Below the Knee Angioplasty Evaluation
(DEBATE-BTK)
Francesco Liistro et al. Circulation. 2013;128:615-621
Lesson from DEBATE-BTK trial
There should be a one-to-one ratio between the DEB and the vessel. It is not worth it to oversize the balloon with respect to the vessel diameter, because on follow-up, we could see in 3% of the cases that there is an ectatic effect from the drug delivery in the vessel.

DCB in A Case of Femoropopliteal PAD with Subintimal Tracking EVT
Case Sharing • 21 y/o man with intermittent claudication of right
leg for months.
• PAD, Right leg post surgical thrombolectomy on April 14th, 2015, and popliteal pseudoaneurysm untreated.
• successful PTA to ATA (POBA, Export aspiration thrombectomy, local thrombolytic therapy) and PTA (POBA, Export aspiration thrombectomy, local thrombolytic therapy) on April 25th, 2015.
• Protein C/Protein S/Antithrombin-III deficiency with wafarin (INR: 1.6) and cilostazol

Case Sharing • Recurrent PAD, Right leg post successful POBA +
Impact Admiral DCB x2 of R't SFA ostial to middle long CTO with bi-directional technique; successful POBA+ Impact Admiral DCB of R't SFA-D to TP trunk CTO; successful POBA of ATA-P and Peroneal-P on Nov. 27th, 2015.
• Terminal ileum ulcer with active bleeding after EVT
• Pseudo-aneurysm of left CFA (puncture site) s/p surgical repair in Jan.18th, 2016.
• Recurrent pseudo-aneurysm of SFA –M , right after surgical repair of pseudo-aneurysm of left CFA ……
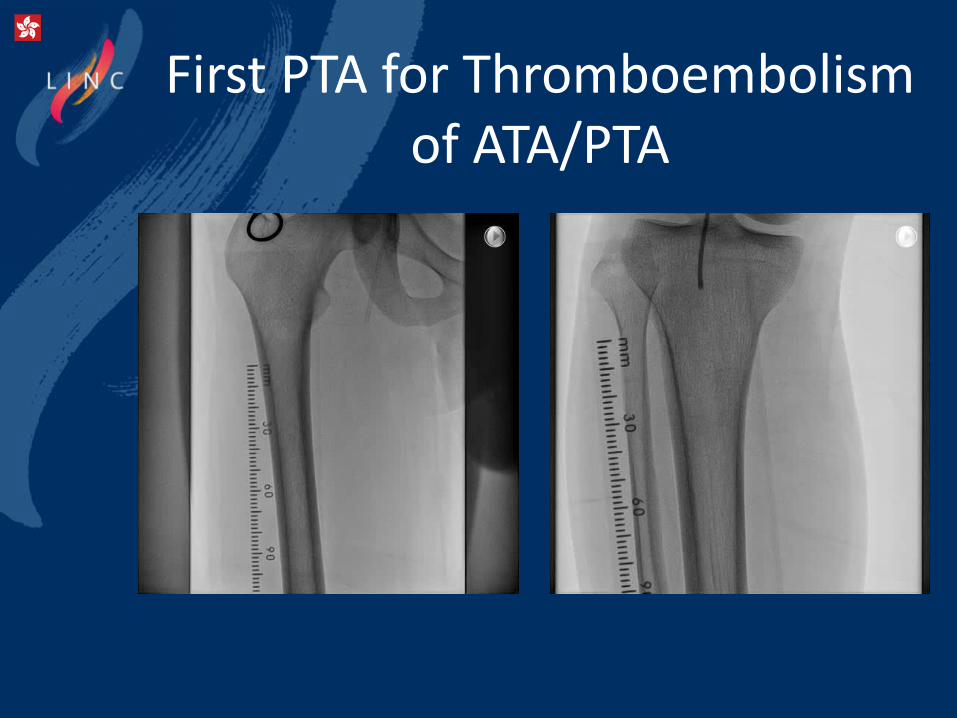
First PTA for Thromboembolism of ATA/PTA

PTA+ CDT with UK
After PTA
Before PTA

Recurrent PAD 7 months later

Cross-over EVT
Backend of control V-18 after
failed crossing with Victory 30gm Subintimal tracking with control V-18
Suppored with Pacific 4.0mmx15cm

Retrograde Puncture of D-SFA

Angio of SFA after POBA
a
BC-assisted hemostasis

Pop to TP trunk CTO
Subintimal tracking with V-18
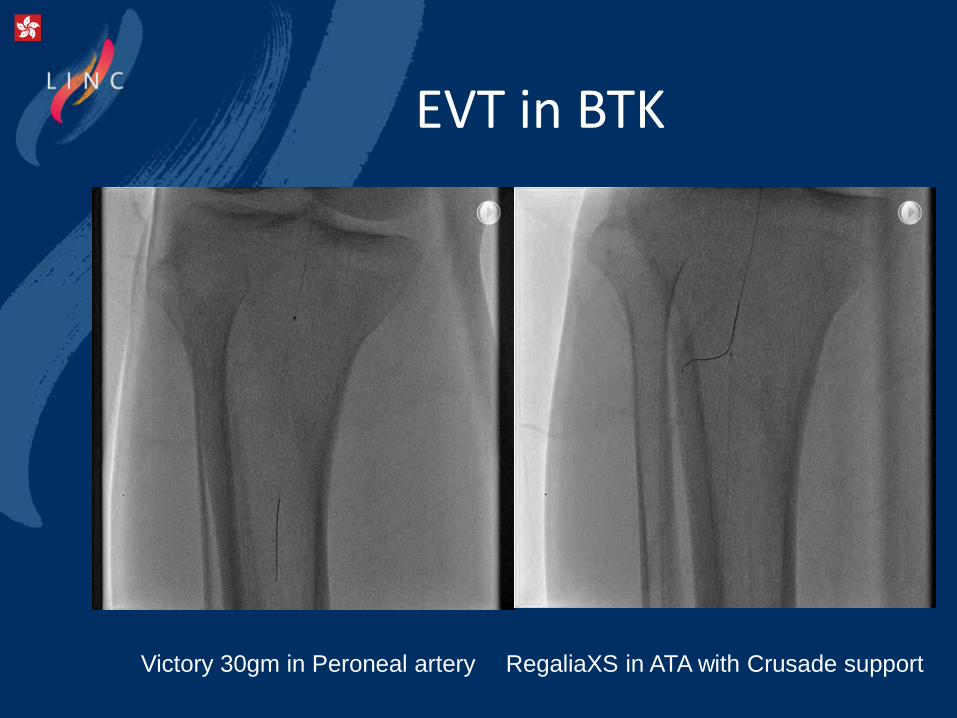
EVT in BTK
Victory 30gm in Peroneal artery RegaliaXS in ATA with Crusade support

BTK Angio
KBT of ATA and TP
trunk

Final Angio
Three Impact Admiral DCB: SFA-ostium to Popliteal artery
But…. Massive GI bleeding with Terminal ileal Uncer (Hb:12>6) A Pseudo-aneurysm of left CFA

Jan. 18th, 2016
Left femoral artery repair, interposition with 8mm ringed PTFE graft 1 cm in length.

Jan. 24th, 2016

Viabahn 7mmx10cm surgical cutdown via R’t CFA
on Feb. 4th, 2016
Progressive enlargement of pseudoaneurysm (2.1cm 4.7cm)

Hospital Course
• Possible Behcet's disease with GI and vascular involvement.
• Skin biopsy of erythema nodosum of right leg: favored vasculitis
• Ileocecal ulcer: four
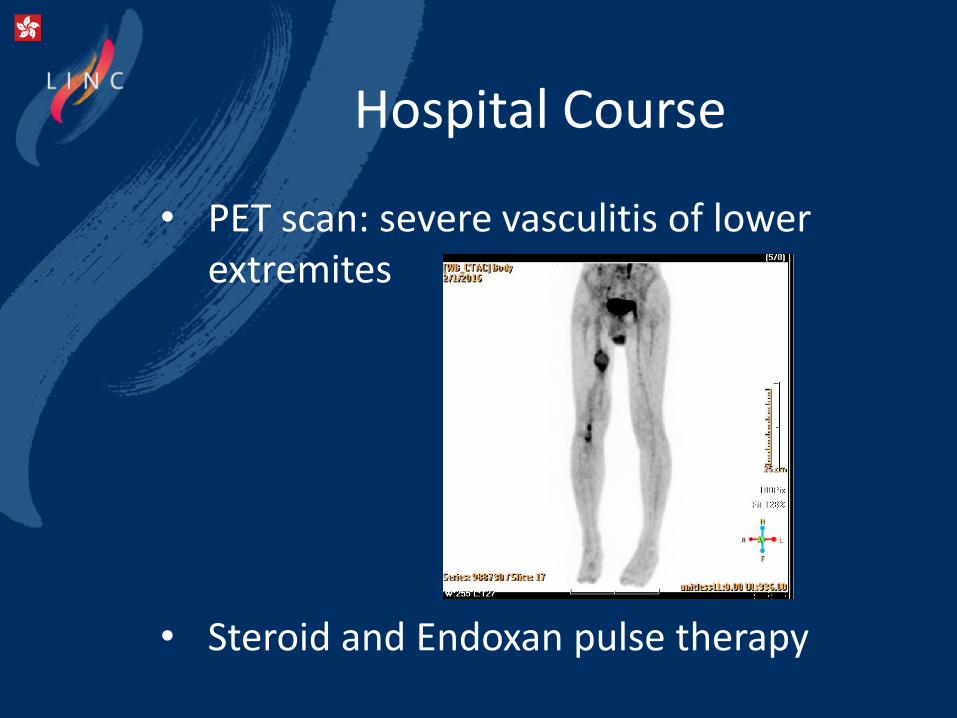
Hospital Course
• PET scan: severe vasculitis of lower extremites
• Steroid and Endoxan pulse therapy

Discussion
• From DEBATE SFA trial, DCB effect is positive irrespective of the recanalization approach (true lumen vs. subintimal) and no arterial aneurysm due to DCB was reported.
• The Global SFA Registry of LUTONIX DCB: Preliminary safety information from the 437 patients enrolled indicates that the most frequent SAEs are pseudoaneurysm (0.7%, 3/437) and Occlusion/Closure (0.7%, 3/437).

Conclusion
• We reported a rare case of young PAOD treated with subintimal approach and DCB, but multiple pseudoaneurysm developed after procedure. The location of pseudoaneurysm is not related to DCB . Finally, vascular Behcet’s disease is diagnosed and we treated the complication by hybrid procedure with surgical repair/Viabahn stenting. The main strategy of treatment is medication of immunosupressants.

Thank You for Attention!

The role of DCB in SFA subintimal tracking lesion
Wei-chun Chang M.D. Wen-Lieng Lee, MD, PhD
Cardiovascular Center, Taichung Veterans General Hospital, Taiwan R.O.C