the role of platelets aggregation tests in the diagnosis of clopidogril resistance rate in patients...
DESCRIPTION
eTRANSCRIPT
The Role of platelets aggregation tests in the diagnosis of clopidogril
resistance rate in patients undergoing pecutaneous coronary
intervension
Introduction:
Platelets play a key role in the pathophysiology of thrombosis after plaque
rupture (1) .Plaque rupture occurs spontaneously in patients with acute coronary
syndromes (ACS), or may be iatrogenically induced in patients undergoing
percutaneous coronary interventions (PCI).significant reduction in such vascular
events in high risk patients with coronary artery diseases or strokes has been
achieved using antiplatelet therapy (2) .
Clopidogrel is a potent antiplatelet drug that is effective in reducing the risk
of vascular events in patients with established vascular disease (3-5) .In addition, it
potentiates the effect of aspirin in reducing ischemic and vascular events in the
setting of cardiovascular diseases (6-8). However, a substantial percentage of
patients with Cardiovascular Disease (CAD) showed low or no response to
clopidogrel therapy (9-11) .
The term ‘Clopidogrel Resistance’ has been used to denote non-
responsiveness of Adenosine Di-Phophatase “ADP” induced platelet aggregation
following standard clopidogrel therapy(12). Several factors were suggested to
explain low response to clopidogrel; including genetic polymorphisms, cellular
factors “e.g. accelerated platelet turnover” and drug-drug interaction” (13) .
Platelet Aggregation:
1

Adenosine diphosphate plays an important role in platelet activation and
aggregation (14,15). Upon damaged or disrupted endothelium, circulating platelets
adhere to the vessel wall through interactions with the subendothelium constituents
(collagen, von Willebrand factor, and other adhesive proteins such as fibronectin,
laminin, and vitronectin) (15,16). After adhesion, these anchored platelets undergo
conformational changes through the action of several extrinsic activators such as
collagen, thrombin, and epinephrine.Once activated, platelets release the contents
of their dense (platelet agonists such as ADP and serotonin) and alpha-granules
(fibrinogen, von Willebrand factor, other adhesive proteins, proinflammatory
factors, and prothrombotic factors), which trigger platelet-activating intracellular
signals in surrounding platelets. Activated platelets also synthesize and release
thromboxane A2 in circulation. Activated and degranulated platelets expose
glycoprotein (GP) IIb/IIIa receptors at their surface allowing fibrinogen binding,
which forms bridges between adjacent activated platelets causing platelet
aggregation. In addition, the release of granule contents amplifies the coagulation
and inflammatory processes.
ADP and its receptor. Adenosine diphosphate binds to neighboring
platelets through two G-protein coupled receptors (P2Y1 and P2Y12) and the
cation channel-coupled P2X1 receptor (17) (Fig. 1).
The activation of P2X1 receptor mediates a rapid transient calcium ion
influx in platelets but does not play a major role in platelet aggregation (17).
Stimulation of the Gq-coupled P2Y1 receptor activates phospholipase C and
induces a transient rise in cytosolic calcium resulting in a platelet conformational
change and in weak, transient platelet aggregation (18).
2

Activation of the Gi-coupled P2Y12 receptor by ADP liberates the Gi
protein subunits αGi and βγ, which couple to independent signaling events and
lead to a sustained platelet aggregation (19).
The subunit αGi decreases the platelet cyclic adenosine monophosphate
(cAMP) level through the inhibition of adenylyl cyclase. This decrease in cAMP
production leads, in turn, to a reduction in the activation of specific protein
kinases,which can no longer phosphorylate the vasodilator stimulated
phosphoprotein (VASP); VASP phosphorylation is crucial for GP IIb/IIIa receptor
inhibition (19).
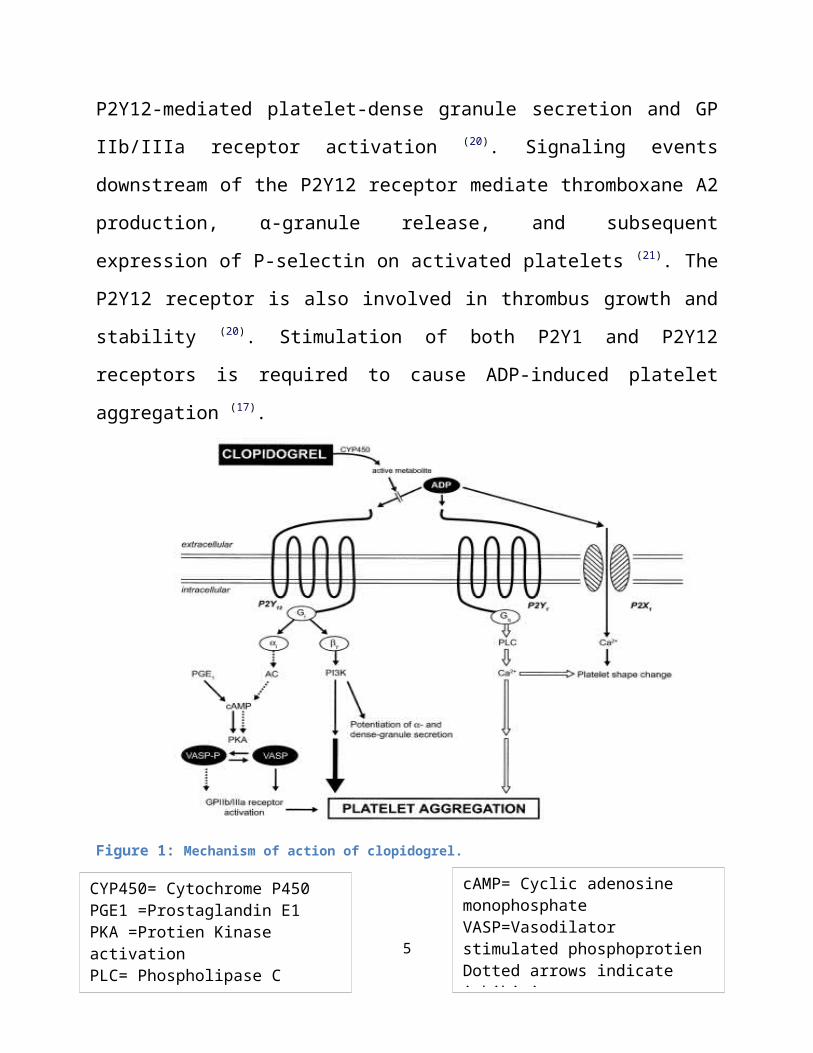
The subunit βγ activates the phosphatidylinositol 3-kinase, which is an
important signaling molecule for P2Y12-mediated platelet-dense granule secretion
and GP IIb/IIIa receptor activation (20). Signaling events downstream of the P2Y12
receptor mediate thromboxane A2 production, α-granule release, and subsequent
expression of P-selectin on activated platelets (21). The P2Y12 receptor is also
involved in thrombus growth and stability (20). Stimulation of both P2Y1 and
P2Y12 receptors is required to cause ADP-induced platelet aggregation (17).
3

Figure 1: Mechanism of action of clopidogrel.
Platelets in the pathogenesis of atherothrombosis:
The complicated pathophysiological procedure underlying acute thrombotic
episodes includes interactions between platelets, plaque components and
coagulation factors (22,23) Figure 2.
The rupture of the intima of acoronary artery, following a plaque rupture or
a iatrogenic injury during PCI, exposes the sub-endothelial elements, such as von
Willebrand factor and collagen,to the bloodstream. Specific receptors on the
4
cAMP= Cyclic adenosine monophosphateVASP=Vasodilator stimulated phosphoprotienDotted arrows indicate inhibitionSolid arrows represent activation
CYP450= Cytochrome P450PGE1 =Prostaglandin E1PKA =Protien Kinase activationPLC= Phospholipase CPI3K= Phosphatidylinositol 3-KinaseAc= adenylyl cyclase
surface of the platelets (GPIa/IIa, GPIb/V/IX, GPVI, etc.) bind the former
molecules, causing the platelet to adhere to the site of the endothelial injury (23,24).
Platelet adhesion leads to activation of the cell through intracellular
metabolic cascades. As a result,platelets aggregate through fibrinogen bridges,
which bind to the activated platelet receptor-integrin αIIbβ3 (GPIIb/IIIa). Activated
platelets release biologically active substances, stored inside the cell or newly
synthesised,among them adenosine diphosphate (ADP), arachidonic acid, platelet-
activating factor (PAF) and serotonin, which induce and preserve platelet
activation and aggregation through positive feedback mechanisms(24,25).
The secretion of pre-coagulant factors from the platelets (e.g. Factor V) and
the interaction with the negatively charged phospholipids of the platelet membrane
maximise the reaction of thrombin synthesis,which has been initiated by the
intravascular exposure of tissue factor and is one of the most powerful platelet
activators. These mechanisms may partly explain the recurrence of thrombotic
episodes in patients already on antiplatelet medication, and justify the need for this
type of drug in cases of acute ischaemic events(26,27) .
Apart from the established importance of platelet actions in the thrombotic
procedure, they play a significant role in the formation of the atheromatous plaque.
According to recent reports, they adhere to the endothelium under mild
inflammatory conditions and attract monocytes, which penetrate the sub-
endothelium and are transformed into macrophages and foam cells.
Several adhesion molecules (P-selectin, ICAM-1) and chemokines (MCP-1,
SDF-1, IL1β, IL- 8, CD40L, RANTES, ENA-78, etc.) participate in these
intercellular interactions and enhance the inflammation in the arterial wall(28).
5

Apart from monocytes,endothelial progenitor cells (EPCs) are also recruited
by the activated platelets and have the potential to transform into either foam cells,
promoting atherogenesis, or into endothelial cells, leading to endothelial
regeneration (29).
Figure2: Central role of ADP-P2Y12 Receptor Interaction In Platelet Activation And
Aggregation.
Mechanism of action and metabolism of Clopidogrel:
Clopidogrel is a prodrug that requires hepatic conversion into an active
metabolite to exert its antiplatelet response .Most of absorbed clopidogrel (85% to
90%) is hydrolyzed by carboxylase to an inactive carboxylic acid
metabolite,SR26334, whereas the remaining 10% to 15% is rapidly metabolized by
hepatic cytochrome (CYP) P450 isoenzymes in a 2-step process ( Fig. 3).
6

In the first step, the thiophene ring of clopidogrel is oxidized to 2-oxo-
clopidogrel, which is then hydrolyzed to a highly labile active metabolite, R-
130964, which has both carboxylic acid and thiol groups (30-32).
Recent studies indicate that CYP2C19, CYP1A2, and CYP2B6 participate in
the first metabolic step, whereas CYP2C19, CYP2C9, CYP2B6, and CYP3A are
responsible for the second step (30,31) (Fig. 3).
The highly unstable active metabolite, R-130964, covalently binds to
platelet P2Y12 receptor specifically and irreversibly during passage through the
hepatic circulation resulting in inhibition of ADP-induced platelet activation-
aggregation for the life span of the platelet (33) (Fig 1).
This metabolic activation scheme is consistent with the time-dependent
cumulative inhibition of ADP-induced platelet aggregation as observed with
repeated daily dosing of clopidogrel and is further highlighted by slow recovery of
platelet function following drug withdrawal (34-36).
Multiple lines of evidence strongly suggest that variable and insufficient
active metabolite generation are the primary explanations for clopidogrel response
variability and nonresponsiveness, respectively (37).
Variable levels of active metabolite generation following clopidogrel
administration could be explained by:
1. Variable or limited intestinal absorption, which may be affected by an ABCB1
gene polymorphism (38-40).
2. Functional variability in P450 isoenzyme activity influenced by drug-drug
interactions as well as other factors.
3. Single nucleotide polymorphisms of specific genes encoding CYP450
isoenzymes (41,42).
7

Figure 3:Clopidogrel response variability is a pharmacokinetic problem primarily influenced by the activity of cytochrome P450 isoenzymes in the generation of the active metabolite.Absorption may be affected by polymorphism of the ABCB1 gene.The activity of hepatic cytochrome isoenzymes are influenced by drug-drug interactions, single nucleotide polymorphisms, and environmental influences (smoking).
Pharmacokinetic and Pharmacodynamic properties of Clopidegrel:
Clopidogrel is a member of the thienopyridine family, along with
ticlopidyne and prasugrel, and is a powerful antiplatelet agent (43). It is a product,
which is absorbed in the gut with the aid of the ABCB1/MDR1 protein transporter.
Subsequently, it is converted to the active metabolite by several isoforms of
cytochrome P450 in the liver, mainly CYP2C19. CYP3A4, CYP3A5,CYP1A2,
CYP2B6 and CYP2C9 also participate in the procedure.
8

The maximum concentration of the active metabolite in blood is reached
within 1 hour after administration of 600 mg clopidogrel (44). interestingly, 85% of
the absorbed drug is hydrolysed by plasma and intestinal mucosa esterases to form
inactive product. The half-life of the active metabolite after a single or multiple
doses is about 8 hours (45). This active metabolite is a potent selective inhibitor of
the P2Y12ADP receptor, which exerts its action by forming disulphuric bonds with
2 serine residues (ser-17, ser-270) of the receptor molecule.
The maximum inhibitory activity of clopidogrel is reached in 24 hours after
administration of 75 mg, in six hours after 300 mg, and in two hours after 600 mg.
as the P2Y12 receptor blockade is irreversible, and 10% of platelets are renewed
daily, at 5 days after treatment cessation 50% of the circulating platelets will be
completely functional and capable of producing adequate hemostasis(46).
Clopidogrel resistance — definition
No single receptor signaling pathway mediating platelet activation is
responsible for all thrombotic complications. Therefore, a single treatment strategy
directed against a specific receptor cannot overcome all thrombotic complications.
With this in mind, it is our opinion that the optimal definition of resistance or non
responsiveness to an antiplatelet agent is the failure of the antiplatelet agent to
inhibit the target of its action. The identification of resistance would therefore
9

utilize a laboratory technique that detects residual activity of the target. Therefore,
clopidogrel resistance is best demonstrated by evidence of residual post-treatment
P2Y12 activity by measuring ADP-induced platelet aggregation before and after
treatment. Since thrombosis involves multiple signaling pathways, treatment
failure is not synonymous with drug resistance (47).
Aim of the study:
To estimate the incidence of clopidogrel resistance among Kurdish
population and to find the predictors of its resistance.
Materials and methods:
This is a prospective study, 100 patients planned to undergo
elective therapeutic percutaneous coronary intervention (PCI) admitted
in the coronary care unit (CCU) will be included in this study. All
patient will receive a loading dose of 300mg of clopidogrel "Plavix®" 12
hours before the PCI and after that will receive a maintenance dose of
75mg of clopidogrel. The patients are already on maintaining dose of
100mg of aspirin. Inform consent will be taken from indicated patients.
The first blood sample will be withdrawn for analysis of platelet
function before clopidogrel intake and the second sample will be
withdrawn 24 hours after PCI (i.e the patient received 300mg loading
dose and 75mg maintaining dose of clopidogrel) (48,49).
10

Platelet aggregation will be tested using the Multiplate analyzer®
(Verum Diagnostica GmbH, Munich, Germany) in the hematology
department in the central laboratory.
The following instruments will be required:
1. Hirudin containing test tubes.
2. Prewarmed dilute tubes.
3. Agonists reagent (adenosine diphosphate (ADP), arachidonic acid
(ASPI), thrombin receptor activating peptide (TRAP).
4. Multiplate test cell
5. Multiplate analyzer
Estimated cost: 12,500,000 ID
Procedure:
11

Whole blood impedance aggregometry will be carried out using the novel
multiplate® analyzer (Dynabyte medical, Munich, Germany) (50,51). The instrument
analyzes platelet function in whole blood at 37 °C by the attachment of platelets
onto metal electrodes, leading to a change of the electrical conductivity (or
impedance), which is continuously recorded. The Multiplate® instrument is an
improvement of impedance aggregometry using a computer-controlled 5-channel
device and disposable test cells with a dual sensor unit allowing duplicate analyses
with each test. Aggregation is recorded for 6 min. Results are expressed in
arbitrary units. Parameters are the aggregation (maximal aggregation), velocity
(steepness of the curve), and the area under curve (AUC). The application of
different activators facilitates to study, e.g., the effect of several platelet active
drugs.
In the present study, thrombin inhibitor(TI)-blood samples (3 ml withdrawn
in a hirudin “anticoagulant” containing test tube) will be used for the Multiplate®
analyses which should be carried out within 30-180 min after blood sampling in
each study participant. The TI-blood diluted with NaCl 0.9% in a 1:1 ratio, and
platelet aggregation determined thereafter in response to stimulation with thrombin
receptor activator peptide 6 with a final concentration of 32 μM (TRAP test),
adenosine- 5-diphosphate (ADP) with a final concentration of 6.4 μM (ADP
test),and arachidonic acid (ASPI test).Obtained results will be expressed as areas
under the curve (AUC).
The ADP test is used to detect copidogrel response, the ASPI test is for
detection of function of aspirin.
12
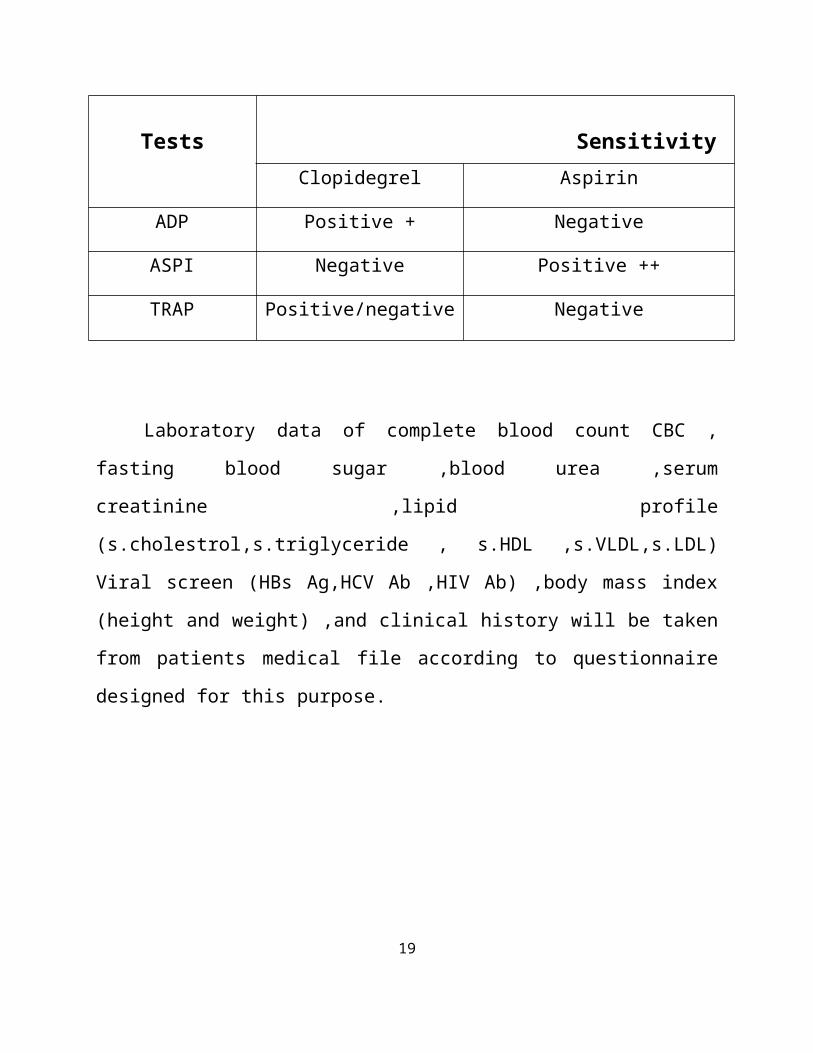
Multiplate- sensitivity to antiplatelet drugs:
Tests Sensitivity
Clopidegrel Aspirin
ADP Positive + Negative
ASPI Negative Positive ++
TRAP Positive/negative Negative
Laboratory data of complete blood count CBC , fasting blood sugar ,blood
urea ,serum creatinine ,lipid profile (s.cholestrol,s.triglyceride ,
s.HDL ,s.VLDL,s.LDL) Viral screen (HBs Ag,HCV Ab ,HIV Ab) ,body mass
index (height and weight) ,and clinical history will be taken from patients medical
file according to questionnaire designed for this purpose.
Questionnaire:
13
Date …. /…/….20 procedure:
…………………..
Mobile number: ………………….
Name: ……………… ………..…… …………..
Age: ………… years ……… Months
Sex: …………………………
Residence:
City Center: ……………
District: ………… / Town: ….…. /Sub district: …..…….. /
Village: ……
Ethnicity: Kurdish………… Arabic ………… Turkish ………..
others………….
Waist circumference …………..cm Ht……..cm Wt………..kg
Lab tests
CBC:
Hb:……. gm/dl WBC ………. Platelet count ………
Lipid profile : 14
s.cholestrol …………mg/dl
s.triglyceride…………mg/dl s.HDL…….mg/dl s.VLDL…………mg/dl
s.LDL…………..mg/dl
B.sugar ………….mg/dl Bl.urea ……..mg/dl
S.creatinine………..mg/dl
Viral screen :
HBs ……..
HCV……..
HIV………
Clinical history:
Diabetes mellitus ……….. hypertention …………. Smoking……….
cigarette/day ……… duration ………years.
Drug history :
Lipid lower agent…….
Proton pump inhibitor………
NSAID………
Reference list:
15

1. Fuster V, Stein B, Ambrose JA, Badimon L,Badimon JJ,ChesebroJH.
Atherosclerotic plaque rupture and thrombosis. Evolving concepts.
Circulation 1990; 82(Suppl 3):II47–59.
2. Baigent C, Sudlow C, Collins R, Peto R.. Collaborative meta-analysis of
randomised trials of antiplatelet therapy for prevention of death, myocardial
infarction, and stroke in high risk patients BMJ. 2002 January
12; 324(7329): 71–86.
3. Bhatt DL, Marso SP, Hirsch AT, Ringleb PA, Hacke W, Topol EJ.
Amplified benefit of clopidogrel versus aspirin in patients with diabetes
mellitus. Am J Cardiol. 2002; 90(6):625-628.
4. Gent M. A randomised, blinded, trial of clopidogrel versus aspirin in
patients at risk of ischaemic events (CAPRIE).Lancet.
1996;348(9038):1329-1339.
5. Mehta SR, Yusuf S, Peters RJ Bertrand ME, Lewis BS, Natarajan MK
et al. Effects of pretreatment with clopidogrel and aspirin followed by
long-term therapy in patients undergoing percutaneous coronary
intervention: the PCI-CURE study. Lancet. 2001;358(9281):527-533.
6. Chen ZM, Jiang LX, Chen YP, Xie JX,Pan HC, Peto R,Collins R et al.
Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial
infarction: randomised placebo-controlled trial. Lancet.
2005;366(9497):1607-1621.
7. Steinhubl SR, Berger PB, Mann JT, 3rd, Fry ET, DeLago A, Wilmer C,
Topol EJ. Early and sustained dual oral antiplatelet therapy following
16

percutaneous coronary intervention: a randomized controlled trial. JAMA.
2002;288(19):2411-2420.
8. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK.
Effects of clopidogrel in addition to aspirin in patients with acute coronary
syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-
502.
9. Aleil B, Ravanat C, Cazenave JP, Rochoux G, Heitz A, Gachet C. Flow
cytometric analysis of intraplatelet VASP phosphorylation for the detection
of clopidogrel resistance in patients with ischemic cardiovascular diseases. J
Thromb Haemost. 2005; 3(1):85-92.
10.Gurbel PA, Bliden KP, Hiatt BL, O'Connor CM. Clopidogrel for
coronary stenting: response variability, drug resistance, and the effect of
pretreatment platelet reactivity. Circulation. 2003;107(23):2908-2913.
11.Van der Heijden DJ, Westendorp IC, Riezebos RK, Kiemeneij F,
Slagboom T, der Weiken LR,et al. Lack of efficacy of clopidogrel pre-
treatment in the prevention of myocardial damage after elective stent
implantation. J Am Coll Cardiol. 2004;44(1): 20-24
12.Cattaneo M. Aspirin and clopidogrel: efficacy, safety, and the issue of drug
resistance. Arterioscler Thromb Vasc Biol. 2004;24(11):1980-1987.
13.Angiolillo DJ, Fernandez-Ortiz A, Bernardo E,Alfonso F, Macaya C,
Bass T, et al. Variability in individual responsiveness to clopidogrel:
clinical implications, management, and future perspectives. J Am Coll
Cardiol. 2007;49(14):1505-1516.
14.Woulfe D, Yang J, Brass L. ADP and platelets: the end of the beginning. J
Clin Invest 2001; 107:1503– 5.
17

15.Stein B, Fuster V, Israel DH, Cohen M, Badimon L, Badimon JJ, et al.
Platelet inhibitor agents in cardiovascular disease: an update. J Am Coll
Cardiol 1989; 14:813–36.
16.Schafer AI. Antiplatelet therapy. Am J Med 1996; 101:199 –209.
17.Kunapuli SP, Dorsam RT, Kim S, Quinton TM. Platelet purinergic
receptors. Curr Opin Pharmacol 2003;3:175– 80.
18.Jin J, Daniel JL, Kunapuli SP. Molecular basis for ADP-induced platelet
activation. II.The P2Y1 receptor mediates ADP-induced intracellular
calcium mobilization and shape change in platelets. J Biol Chem 1998;
273:2030–4.
19.Geiger J, Brich J, Honig-Liedl P, Eigenthaler M, Schanzenbächer P,
Herbert J M, Walter U,et al. Specific impairment of human platelet
P2Y(AC) ADP receptor-mediated signaling by the antiplatelet drug
clopidogrel. Arterioscler Thromb Vasc Biol 1999; 19:2007–11.
20.Conley PB, Delaney SM. Scientific and therapeutic insights into the role of
the platelet P2Y12 receptor in thrombosis. Curr Opin Hematol 2003;
10:333–8.
21.Dorsam RT, Kunapuli SP. Central role of the P2Y12 receptor in platelet
activation. J Clin Invest 2004; 113:340 –5.
22.Ruggeri ZM. Platelets in atherothrombosis. Nature Med. 2002; 8: 1227-
1234.
23.Davì G, Patrono C. Platelet activation and atherothrombosis. N Engl J
Med. 2007; 357: 2482-2494.
18
24.Jennings LK. Mechanisms of platelet activation: need for new strategies to
protect against platelet-mediated atherothrombosis.Thromb Haemost. 2009;
102: 248-257.
25.Offermanns S. Activation of platelet function through G protein-coupled
receptors. Circ Res. 2006; 99: 1293-1304.
26.Mann KG. Thrombin formation. Chest. 2003; 124: 4S-10S.
27.Brummel KE, Paradis SG, Butenas S, Mann KG. Thrombin functions
during tissue factor-induced blood coagulation. Blood. 2002; 100: 148-152.
28.Lindemann S, Kramer B, Daub K, Stellos K, Gawaz M. Molecular
pathways used by platelets to initiate and accelerate atherogenesis. Curr
Opin Lipidol. 2007; 18: 566-573.
29.Stellos K, Gawaz M. Platelet interaction with progenitor cells: potential
implications for regenerative medicine. Thromb Haemost. 2007; 98: 922-
929.
30.Hagihara K, Kazui M, Kurihara A, Yoshiike M Honda K, Okazaki O,
Farid N, et al. A possible mechanism for the differences in efficiency and
variability of active metabolite formation from thienopyridine antiplatelet
agents, prasugrel and clopidogrel. Drug Metab Dispos 2009; 37:2145–52.
31. Kazui M, Nishiya Y, Ishizuka T, Hagihara K, Farid N, Okazaki O, et
al. Identification of the human cytochrome P450 enzymes involved in the
two oxidative steps in the bioactivation of clopidogrel to its
pharmacologically active metabolite. Drug Metab Dispos 2010; 38:92–9.
32.Pereillo JM, Maftouh M, Andrieu A, Pereillo JM, Maftouh M, Andrieu
A, et al. Structure and stereochemistry of the active metabolite of
clopidogrel. Drug Metab Dispos 2002; 30:1288 –95.
19

33. Savi P, Zachayus JL, Delesque-Touchard N, Labouret C, Hervé C,
Uzabiaga MF, et al. The active metabolite of clopidegrel disrupts P2Y12
receptor oligomers and partitions them out of lipid rafts. Proc Natl Acad Sci
U S A2006;103:11069 –74.
34.Patrono C, Baigent C, Hirsh J, Roth G, on behalf of American College of
Chest Physicians. Antiplatelet drugs: American College of Chest Physicians
evidence-based clinical practice guidelines (8thedition). Chest 2008; 133
Suppl 6:199S–233S.
35.Price MJ, Coleman JL, Steinhubl SR, Wong GB, Cannon CP, Teirstein
PS. Onset and offset of platelet inhibition after high-dose clopidogrel
loading and standard daily therapy measured by a pointof- care assay in
healthy volunteers. Am J Cardiol 2006; 98:681– 4.
36.Gurbel PA, Bliden KP, Butler K, Udaya S. Tantry, Tania Gesheff,
Cheryl Wei, et al. Randomized double-blind assessment of the ONSET and
OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in
patients with stable coronary artery disease: the ONSET/OFFSET study.
Circulation 2009; 120:2577–85.
37.Angiolillo DJ, Ferna´ndez-Ortiz A, Bernardo E, Ramírez C, Sabaté
M, Bañuelos C, et al. High clopidegrel loading dose during coronary
stenting: effects on drug response and interindividual variability. Eur Heart
J 2004; 25:1903–10.
38.Simon T, Verstuyft C, Mary-Karuse M, Quteineh L, Drouet
E, Méneveau N, et al., on behalf of French Registry of Acute ST Elevation
and Non-ST-Elevation Myocardial Infarction (FAST-MI) Investigators.
Genetic determinants of response to clopidogrel and cardiovascular events.
N Engl J Med 2009; 360:363-75.
20

39.Hochholzer W, Trenk D, Frundi D, BlankeP; Fischer B; Andris K ,et
al. Time dependence of platelet inhibition after a 600 mg loading dose of
clopidogrel in a large, unselected cohort of candidates for percutaneous
Coronary intervention. Circulation 2005; 111:2560–4.
40.Collet JP, Silvain J, Landivier A, Tanguy M, ; Cayla G, Bellemain A,
et al. Dose effect of clopidegrel reloading in patients already on 75-mg
maintenance dose: the Reload with Clopidogrel Before Coronary
Angioplasty in Subjects Treated Long Term with Dual Antiplatelet Therapy
(RELOAD) study. Circulation 2008; 118:1225–33.
41.Gurbel PA, Antonino MJ, Tantry US. Recent developments in
clopidogrel pharmacology and their relation to clinical outcomes. Expert
Opin Drug Metab Toxicol 2009; 5:989 –1004.
42.Marı´n F, Gonza´lez-Conejero R, Capranzano P, Bass TA, Rolda´n V,
Angiolillo DJ. Pharmacogenetics in cardiovascular antithrombotic therapy.
J Am Coll Cardiol 2009; 54:1041–57.
43.Gurbel PA, Tantry US. Combination antithrombotic therapies.
Circulation. 2010; 121:569-583.
44. Montalescot G, sideris G, meulman C, Bal-dit-Sollier C, Lellouche
N, Steg PG, et al. a randomized comparsion of high clopidogrel loading
doses in patients with non-ST-segment elevation acute coronary syndromes:
the ALBION (Assessment of the best loading doses of clopidogrel) to blunt
platelet activation, inflammation and ongoing necrosis ) trial. J Am Coll
Cardiol. 2006; 48:931-938.
21

45. Lins R, Broekhuysem J, necciari J,deroubaix X. pharmakokynatic
profile of 14C-labeled clopidogrel. Semin Thromb Hemost. 1999; 25 suppl
2:29-33.
46. Tselepis A D,Gerotziafas G,Andrikopoulos G, Anninos H, Vardas
P.Mechanism of platelet activation and modification of response to
antiplatelet agents.Hellenic J Cardiol.2011;52:128-140.
47.Gurbel P A, Tantry U S. clopidogrel resistance. Thrombosis Research.
2007;120:311-321.
48.Wang L,Wang X,Chen F.clopidogrel resistance is associated with long-
term thrombotic events in patient implanted with drug-eluting stents.Drugs
RD.2010;10(4):219-24.
49.Thomas M,Benjamin D,Werner P,Andreas C,Meinhard H.Utility of
whole blood impedance aggregometry for the assesment of clopidogrel
action using the noval multiplate analyzer –comparison with two
flowcytometric methods.Thrombosis Research.2007;121(2):249-258.
50.Calatzis A, Wittwer M, Krueger B. A new approach to platelet function
analysis in whole blood—the Multiplate® analyzer. Platelets 2004; 15:479
[Abstract].
51.Calatzis A, Wittwer M, Krueger B, Spannagl M. Assessment of
cyclooxygenase, ADP receptor and GpIIb/IIIa receptor blockade by
impedance aggregometry using the Multiplate® analyzer. J Thromb
Haemost 2005; 3(Suppl 1):0962.
22