timings apologies for absence and declarations of … · conference room, education centre, royal...
TRANSCRIPT
A meeting of the Council of Governors will be held on Wednesday 13 April 2016 at 08:30 in the Conference Room, Education Centre, Royal Bournemouth Hospital. If you are unable to attend on this occasion, please notify me as soon as possible on 01202 704246.
Sarah Anderson Trust Secretary
A G E N D A
TIMINGS 1. APOLOGIES FOR ABSENCE AND DECLARATIONS OF INTEREST
8.30-8.35 2. MINUTES OF THE PREVIOUS MEETING
(a) To approve the minutes of the meeting held on 3 February 2016
8.35-8.45 3. MATTERS ARISING (a) To provide updates to the Actions Log
08:45-10:15 4. PERFORMANCE (a) Quality Performance Report including
Complaints Report (Paper) Information Paula Shobbrook
(b) Performance Report (Paper) Information Richard Renaut (c) Financial Report including update from
Monitor (Paper) Information Stuart Hunter
(d) Workforce (Paper) Information Karen Allman
10:15-10:30 BREAK 10:30-11:15 5. STRATEGY
a) Trust Mortality (Presentation) Information Basil Fozard b) Vanguard Update (Verbal) Information Tony Spotswood c) CSR Update (Verbal) Information Tony Spotswood
11:15-12:15 6. GOVERNANCE (a) Changes to the Constitution (Paper) Decision Sarah Anderson (b) Governor Budget – Cost Improvement
(Paper) Information Sarah Anderson
(c) Annual Members’ Meeting (Paper) Decision Sarah Anderson
(d) Committee Work i) Membership Development Decision Chris Archibold
CoG Agenda Part 1 13 April 2016

Committee Work Programme (Paper)
ii) Membership Development
Committee Engagement Programme (Paper)
Decision Chris Archibold
iii) Membership Development
Committee Terms of Reference Update (Paper)
Decision Chris Archibold
iv) Governor Involvement with Patient
and Public Engagement Committee Update (Paper)
Information David Bellamy
v) Governor Involvement with Patient
and Public Engagement Committee Work Programme (Paper)
Decision David Bellamy
vi) Governor Involvement with Patient
and Public Engagement Terms of Reference Update (Paper)
Decision David Bellamy
vii) Governor Strategy Committee
Report (Paper) Information Eric Fisher
viii) Governor Strategy Committee
Work Programme (Paper) Decision Eric Fisher
(e) Appointment of the Lead Governor 2016-17
(Verbal) Decision Sarah Anderson
(f) Private Patients (Presentation) Information
and Discussion
Michelle Burden
(g) Draft Annual Report and Quality Accounts
(Verbal) and Schedule (Paper) Information James Donald,
Sarah Anderson and Jo Sims
12:15-12:30 7. INFORMATION (a) October – December 2015 Listening Event
feedback (Paper) Information David Bellamy
(b) Governor Concerns Log (Paper) Information Sarah Anderson
(c) Forward Planner (Paper) Information Sarah Anderson
(d) Trust Committee Governor Representative Reports (Paper)
Information Governors
CoG Agenda Part 1 13 April 2016
(e) Appointed Governors Reports (Paper)
Information Appointed
Governors (f) Staff Governors Reports (No reports
received) Information Staff Governors
(g) Additional Activity reports Information Governors
8. NEXT MEETING Thursday 21 July 2016 at 08:30 in the Conference Room, Education Centre,
Royal Bournemouth Hospital
9. COMMENTS AND QUESTIONS FROM THE PUBLIC Comments and questions from the public on items received or considered by the
Council of Governors at the meeting.
10. RESOLUTION REGARDING PRESS, PUBLIC AND OTHERS To resolve that under the provision of Section 1, Sub-Section 2, of the Public Bodies
Admission to Meetings Act 1960, representatives of the press, members of the public and others not invited to attend to the next part of the meeting be excluded on the grounds that publicity would prove prejudicial to the public interest by reason of the confidential nature of the business to be transacted.
CoG Agenda Part 1 13 April 2016

Council of Governors Meeting
THE ROYAL BOURNEMOUTH AND CHRISTCHURCH HOSPITALS NHS FOUNDATION TRUST
REGISTER OF GOVERNORS’ INTERESTS
as at 5 April 2016 The following Governors of The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust have declared interests as listed below: NAME/CONSTITUENCY
DECLARED INTEREST
ELECTED GOVERNORS Public: Bournemouth and Poole David Bellamy • The Chairman of the Patient Panel of a local GP Group Carole Deas • Partner – Roger Parsons, Public Governor Paul Higgs None Roger Parsons • Partner – Carole Deas, Public Governor Keith Mitchell • Chairman of Southbourne Tennis Club
• Chair of Governors at Victoria Education Centre Guy Rouquette • Chair of the Board of Trustees of the Steven James
Practice • Member of the Liberal Democrat Party
Alan Radley None Maureen Todd • Magistrate David Triplow None Public: Christchurch and Dorset County Chris Archibold • Wife is a member of staff employed in the Orthopaedic
Department, based at the Royal Bournemouth Hospital Paul McMillan None Derek Chaffey • Member of the Stanpit and Mudeford Residents’
Association Eric Fisher • Member of East Dorset Locality Health Network Group (in a
personal capacity) which is arranged through the Dorset CCG
• Member of the Patient and Public Engagement Group (PPEG) with Dorset CCG as part of the Clinical Services Review
• Steering Committee as the public/patient representative for the Dorset CCG supported Castleman Community Vanguard project to produce a final draft report to the Dorset CCG
Doreen Holford None Brian Young • Consultant (salaried) for Immunotec Public: New Forest, Hampshire and Salisbury David Brown None Bob Gee None Graham Swetman • Member of the Conservative Party
• Director, Family Property Investment Companies
COG/Register of Governors Interests Page 1 of 2

Council of Governors Meeting
Staff Sarah Berridge Medical and Dental
None
Ian Knox Allied Healthcare Professionals, Scientific and Technicians
Wife is a NHS Professional at Southampton General Hospital
Petrina Taylor Nursing, Midwifery and Healthcare Assistants
None
Richard Owen Hotel Services and Estates
None
Kim Waterman Administration, Clerical and Management
None
NOMINATED GOVERNORS Local Authority Governors Rae Stollard Bournemouth Borough Council
• Member of the Conservative Party • Member of Bournemouth Borough Council • Member of the Health and Adult Social Care Overview
and Scrutiny Panel, Bournemouth Borough Council Colin Jamieson Dorset County Council
• Elected member of Christchurch Borough Council • Elected member of Dorset County Council • Chairman of the Christchurch Planning Committee • Cabinet Member for Economy and Growth • Reserve Member of the Dorset Health and Wellbeing Board • Member of the Cabinet of Dorset County Council
(Economic Growth and Enterprise Portfolio) • Wife is a Constituency Agent for the Conservative Party
John Challinor Poole Borough Council
• Elected member of Poole Borough Council • Member of the Conservative Party • Friend of Derek Dundas, Non-Executive Director
Partnership Governors Philip Copson The Royal Bournemouth and Christchurch Hospitals Volunteers Group
None
Stephen Tee Bournemouth University
Wife is a nurse at St Richards Hospital, Chichester
Primary Care Trust Governors Dr Tom Knight CCG Dorset
General Practitioner Board Member of Dorset Clinical Commissioning Group (CCG)
COG/Register of Governors Interests Page 2 of 2

Minutes of a public session of the Council of Governors meeting held on Wednesday 3 February 2016 in the Education Centre, Royal Bournemouth Hospital. Present: Jane Stichbury
Chris Archibold David Bellamy Derek Chaffey Philip Copson Eric Fisher Bob Gee Doreen Holford Paul Higgs Colin Jamieson Ian Knox Paul McMillan Rae Stollard Roger Parsons Alan Radley Guy Rouquette Graham Swetman Petrina Taylor Maureen Todd David Triplow
(JS) (CA) (DB) (DC) (PC) (EF) (BG) (DH) (PH) (CJ) (IK) (PM) (RS) (RP) (AR) (GR) (GS) (PT) (MT) (DT)
Chairperson (in the Chair) Public Governor (Christchurch and Dorset County) Public Governor (Bournemouth and Poole) Public Governor (Christchurch and Dorset County) Appointed Governor (RBCH Hospital Volunteers Group) Public Governor (Christchurch and Dorset County) Public Governor (New Forest, Hampshire and Salisbury) Public Governor (Christchurch and Dorset County) Public Governor (Bournemouth and Poole) Appointed Governor (Dorset County Council) Staff Governor (Allied Health Professionals, Scientific and Technical) Public Governor (Christchurch and Dorset County) Appointed Governor (Bournemouth Borough Council) Public Governor (Bournemouth and Poole) Public Governor (Bournemouth and Poole) Public Governor (New Forest, Hampshire and Salisbury) Public Governor (Bournemouth and Poole) Staff Governor (Nursing, Midwifery & Healthcare Assistants) Public Governor (Bournemouth and Poole) Public Governor (Bournemouth and Poole)
In attendance:
Karen Allman Derek Dundas Basil Fozard Christine Hallett Stuart Hunter Ian Metcalfe Donna Parker Paula Shobbrook Tony Spotswood Bill Yardley
(KA) (DD) (BF) (CH) (SH) (IM) (DP) (PS) (TS) (BY)
Director of Human Resources Non- Executive Director/ Senior Independent Director Medical Director Non- Executive Director Director of Finance Non- Executive Director Deputy Chief Operating Officer Director of Nursing & Midwifery Chief Executive Non- Executive Director
Public in attendance
David Brown Sue Bungey Sylvia Chiswell
Member of Public Member of Public Member of Public
Apologies Sarah Berridge John Challinor Carole Deas Keith Mitchell Richard Owen Stephen Tee Brian Young
Staff Governor (Medical and Dental) Appointed Governor (Poole Borough Council) Public Governor (Bournemouth and Poole) Public Governor (Bournemouth and Poole) Staff Governor (Hotel Services and Estates) Appointed Governor (Bournemouth University) Public Governor (Christchurch and Dorset County)
Council of Governors Meeting 03.02.16 PAGE 1 OF 10
01/16 DECLARATIONS OF INTEREST Action
JS welcomed the Council of Governors and the newly appointed governors MT, AR and RS to the meeting. The Council of Governors received the declaration of interest submitted by KM highlighting his appointment as Chairman of Southbourne Tennis Club and the Chair of governors at Victoria School. RS declared her interests as a member of the Conservative Party, the Heath and Adult Social Care Overview and Scrutiny panel and as a Councillor for Bournemouth Borough Council. JS presented Dean Feegrade with a certificate, following the expiration of his term of office, recognising his valuable service as a Staff Governor.
02/16 MINUTES OF THE MEETING HELD ON 5 November 2015 (Appendix A)
The minutes of the meeting on 5 November 2015 were confirmed as an accurate record subject to the following amendments: to amend the CSR costing reference £76,000 to £76 million at 15/79.
03/16 MATTERS ARISING (ACTIONS LOG) (Appendix B)
(a) To provide updates to the action log • 15/32 (to remain amber) Exit data- further information is to be
provided once available; • 15/58- (to remain amber) the work programme of the Council of
Governors will be included as an agenda item at the next Strategy Committee.
KA SA
04/16 PERFORMANCE
(a) Performance Report (item a)
DP outlined the highlights from the report: • Significant step changes within Q3 and challenging of the targets; • Emergency Department (ED) 4 Hour target- Trust performance for
December was above target as a result of the rapid treatment model and NHS 111 service. There has been a higher rate of attendances which has increased pressures. Norovirus has also impacted upon performance;
• Cancer 62 day target- an analysis of breaches was implemented to improve pathways and the backlog of patients is clearing. It is anticipated that the Trust will be compliant for Q3;
• C-difficile - a process is in place to review cases and address compliance;
• Cancer 62 days- the Trust is working with Dorset County Hospital and the Clinical Commissioning Group (CCG) to address the backlog and waiting times. This will impact upon performance for the next quarter;
• Delayed transfers of care- packages of care are being provided and
Council of Governors Meeting 03.02.16 PAGE 2 OF 10

the Trust is working with Local Authorities and social services to ensure appropriate care is provided;
• Endoscopy- there has been a positive trend within 6 week waiting times. There has been an agreement to expedite with the CCG. Overall the Trust is in a more sustainable position.
The impact of the Junior Doctor strikes was queried. RR emphasised that the Trust had coped well as a result of the planned redirecting of some medical staff to inpatient work and the cancellation of some elective operations. Concern was raised for the provision of out of hospital community and social care. It was noted that the Trust is working with local authorities and using interim care services to support discharge and care packages to support rehabilitation out of hospital which is more beneficial to patients. Interim care beds are also utilised within the Trust. The development of assessment centres as an alternative to GP surgeries was discussed and the potential impact this would have on reducing ED attendances. Governors requested a summary of the mandated targets imposed by both the CCG and Monitor including a metric for the risks if these are not achieved.
RR
(b) Financial Performance (item b)
SH presented the key themes from the report: • The Trust’s Month 9 position is in line with the expectations of the
revised Cost Improvement Plan (CIP); • There has been an rise in pressures due to increased attendances
at the front door and this was a significant rise upon last year; • CIP- performance is ahead of plan by £0.5 million and the Quality
Investment Assurance (QIA) process is in place to reduce any loss of quality;
• Future planning- national funding from NHS England amounting to £3.8 billion will be allocated during 2016/17. £1.8 billion has been set aside to support providers of emergency care. Regulators are recognising the negative impact of the tariff system over the last three years. Around 90% of Foundation Trusts are in a deficit position;
• £30 million will be allocated for the provision of healthcare in Dorset by the Clinical Commissioning Group (CCG). Funding has been committed for Mental Health care and to support the tariff uplifts;
• It will not be sustainable for the Trust to deliver 4% as a result of the national Tariff. It is anticipated that efficiencies will be achieved through the Vanguard project. The Trust will be required to deliver an efficiency factor of 2% next year;
• Sustainability and Transformation Fund- £7.6 million will be provided to Trusts in a deficit position as a result of the Tariff. Acceptance of the funding will impose a £1.7 million control total together with performance conditions which the Trust must meet;
Council of Governors Meeting 03.02.16 PAGE 3 OF 10

• The Operational Revenue Budget and Capital Programme are currently being prepared.
It was acknowledged that the CIP savings were not recurrent and that it would be important to focus on the cash position. The Trust must deliver the non-recurrent savings for 2015/16 and this is within the current plan. There are good schemes in place and there is confidence in delivering the CIP next year. In relation to the Lord Carter review of efficiencies the Trust is operating at a higher level of efficiency than other Trusts. Care groups will be managed in terms of the efficiencies identified within the report. It was emphasised that budget setting was critical and delivering activity. Feedback from the Monitor-
• The drivers for the deficit were understood throughout the Trust; • Appropriate action is being taken eg. agency control; • Pace with the CIP was recognised; • Some inconsistency within one care group was identified although
this is being supported; • Organisational Development work is positive; • The Board meeting was well chaired; • More information should be provided from the Healthcare
Assurance Committee (HAC) to the Board; • Overall the finance position was positive.
It is anticipated that a response will be received at the end of March. The impact of the merger between Monitor and the NHS Trust Development Authority was queried. SH advised that if the Trust’s financial position remained strong it was anticipated that their role would be supportive. It was emphasised that there would be an increase in centralised control and regulation across the health sector overall.
(c) Workforce Report (item c)
KA presented the report noting the following: • Strong performance in improving appraisal compliance. The
process for the next financial year will commence soon and the Trust is developing a trajectory to ensure that performance is even better and that objectives are being cascaded throughout the organisation.
• Essential Core Skills- training has been mapped for the organisation and capacity. Departments will need to ensure there is adequate planning to map the training throughout the year;
• Sickness absence- the audit and further detail will be provided once received;
• Various health & wellbeing events to support staff are taking place throughout the Trust;
• Recruitment- events and the recent drive through social media has been positive.
Council of Governors Meeting 03.02.16 PAGE 4 OF 10

The Trust continues to maintain momentum for year 2 of the appraisal process. Individual compliance reports are being provided to managers and it is identified within rostering and staff appraisals. It was emphasised that departments need to ensure that planning is in place throughout the year to support staff who are required to complete training. Nursing Recruitment-
• EU nurses are required to have completed a level 7 English language test which is recognised by the UK;
• Non- EU nursing recruitment is a longer process as they must complete their exams and must register with the National Midwifery Council and complete the Objective Standard Clinical examination upon their arrival in the UK;
• Nurses were placed on a shortage of occupation list in 2015 and the Home Office has requested a review;
• There is a different process for the recruitment of Doctors; • The Trust’s retention rate for overseas nurses is strong. 17
European nurses have been recruited for this year; • It is difficult to retain the interest of Non- EU nurses as a result of
the longer recruitment process. KA advised that the Exit questionnaire information was being progressed and would be provided to governors once available. The staff survey results had been positive with a high response rate. The results will be provided at the next meeting.
KA
(d) Quality Performance Report (item d)
PS highlighted the following key themes from the report; • The Trust continues to focus on harm free care and there has been
some progress in the reduction of new harms; • Serious Incidents- 11 have been reported over the last three months
and these have been discussed in detail at HAC and there is a structured review process. These predominantly related to pressure damage and falls.
The progress with the Trust’s Quality Objectives was summarised: • The Trust’s aim is to maintain a high rate of serious incident
reporting as this is reflective of a healthy reporting culture. The rate is currently lower than the target set for 2014/15;
• Falls- performance is above the 2014/15 target and above trajectory;
• Medication Administration- performance is currently above trajectory for 2014/15 and 2015/16 although there are low levels of reporting and the Trust is looking to increase the reporting rate;
• Serious Incidents- performance is on trajectory to achieve the 2015/16 target. There has been an increase in reporting and a reduction in harm;
• Avoidable pressure damage- performance is on trajectory to achieve 2015/16 target;
• Staff Accidents- the number of incidents has been reduced and
Council of Governors Meeting 03.02.16 PAGE 5 OF 10
performance is on trajectory to achieve the 2015/16 target; • Friends and Family Test (FFT) - the Trust is benchmarking within
the top quartile and also within Emergency Department and the Trust is working to increase feedback in this area;
• Complaints - FFT feedback is reviewed so as to identify themes and address by department;
• Care Campaign Audit - action plans are in place to address themes identified which include the discharge process, answering call bells, pain control, noise at night, compassion and communication, nutrition, preference of clinician gender and waiting times in some areas;
• Care campaign and FFT data is collated to develop focused action plans and issues identified are fed back to each area;
• Infection Prevention and Control- ward closures took place due to the recent norovirus outbreak within the community. A structured media campaign to inform the public was put in place to address the outbreak.
• Gel hand sanitising facilities are provided at the entrance to the Hospital and each ward. Fewer bays have been closed and fewer staff have been affected and overall this has been managed very carefully.
Governors were reminded that the concerns and complaints report was available within the publically available Board papers. The report will be included in the papers for the next meeting. Feedback from the governor listening event will be submitted to GIPPE and received by the Council of Governors at the next meeting. Governors reflected that more often complaints related to patient perception rather than complaints about services or care. Governors reported that positive feedback had been received from the community about the standards of care and kindness from members of staff during busy periods.
PS DR
05/16 STRATEGY
(a) CQC Report (item a)
The Trust is in receipt of the draft report and will respond to the factual accuracy within 10 days. Three reports were received, one report for each site and an overall report for the Trust. The report will be published following the quality summit. A briefing and an annex outlining the ratings will be provided in due course.
(b) Vanguard Update (item b)
• Three acute trusts in Dorset have proposed to develop services on a unified basis to improve care, reduce variation and increase sustainability;
• Women’s health- there are plans to create a unified pathway for maternity, gynaecology and to extend to peri-natal mental health;
• Ophthalmology- services will be strengthened in the West using
Council of Governors Meeting 03.02.16 PAGE 6 OF 10
clinicians to develop a broader emergency service and integrating primary and secondary care services;
• Cancer- reconfiguration of services to address the future demand;
• Radiology - working to identify a single process for reporting out of hours;
• Cardiology- to improve preventative measures and increase access to services;
• A single approach to IT systems across the three organisations; • The project will also address efficiencies in back office functions; • The governance structure is being identified and the appointment
of an independent chair is being considered; • Competition and Markets Authority (CMA) will be required to
review the project; • A joint venture vehicle will be established in Oct 2016 with a
contractual approach.
Funding of £1.2 million will be provided by the Government and NHS England this year. The Trusts will be bidding for £8.9 million during 2017 and £3 million in 2017/18 to develop the proposals. The three trusts will remain independent and there are no plans to change the structures. Charitable money will continue to underpin services for local people. In addition there are also three community Vanguards projects and the schemes are being developed within GP localities and have different objectives. SE will provide further information on the schemes. The Clinical Services Review (CSR) forms the wider platform to preserve hospital services. The Vanguard project concerns changing the pattern and pathways to create better efficiency and quality for patients. Community services will also need to be integrated.
SE
(c) CSR Update (item c)
• Latest capital costs for developing the sites identified RBH as 40-50% less expensive to develop as the green site. The cost to develop Poole Hospital as the purple site is potentially as high as £59 million. Concern was expressed that this represented neither a credible or realistic requirement and that the cost could be constrained to substantially less;
• The assumption for the acute medical take on the purple site has been revised to 20%;
• There will not be a critical care service on the purple site due to workforce constraints;
• If RBH is identified as the green site it would be viable to continue the orthopaedic joint replacement work;
• The strategy for the provision of out of hospital care needs to be developed and the rationalisation of the inpatient provision at community hospital sites;
Council of Governors Meeting 03.02.16 PAGE 7 OF 10
• Royal College of Midwives, Obstetrics and Paediatrics have conducted a review and two options are being considered;
• The Board will need to gain assurance that the evaluation criteria used by the CCG to assess the options has been adhered to once the model has been chosen for consultation;
• The CMA are likely to perceive the CSR as a form of merger and will undertake a full review;
• The Board will continue to input into the shape of the model of care and the services at the two sites, promoting the rationale for RBH as the green site and supporting the role of external stakeholders;
• A number of issues are yet to be resolved before support can be provided for the model identified.
It was noted that the costings for the Poole purple site would include updating theatres to increase day case work and that this could be obviated by centering orthopaedic joint replacement work at RBH. It was noted that the review will include an out of hospital strategy. The main anaesthetics work will be concentrated over the three main sites. It was queried whether increases in capacity had been incorporated in to the models and the costs. The work completed by McKinsey incorporated this detail together with assumptions around 7 day working. It was emphasised that there was no provision for growth in the bed base and the out of hospital strategy will be key to ensuring the proposals were viable. The engagement with local authorities and social services is to be addressed. The anticipated timescale for implementation will be at the end of 2021 and during the interim financial challenges will need to be addressed. The workforce challenges will be significant and the fragility of the current services in the West. There will be a governor briefing on the CSR before the consultation to engage governors in the process.
SA
(d) Strategy Committee Report (item d)
The options for the audit of the quality indicator were outlined: • C-difficile- to support the Trust’s quality objective and the
challenging target set; • Patient moves- which forms part of the local CQUIN.
BG proposed that patient moves were identified as the quality indicator selected by the governors. CJ seconded the motion. The Council of Governors approved the quality indicator to be audited as patient moves.
06/16 GOVERNANCE
(a) Dissolution of the Governor Training Committee (item a)
The recommendation was outlined and it was highlighted that the mechanism for identifying training needs would be facilitated through
Council of Governors Meeting 03.02.16 PAGE 8 OF 10

the Strategy Committee with detailed focus on future training topics and the evaluation of training feedback would be remitted to the Chairs Group. It was requested that a meeting was arranged. It was also emphasised that the Trust was supportive of governor training and encouraged governor attendance at Governwell events and local networking events such as the South West Governor Engagement Network.
DR
(b) Ratification of Strategy Committee Terms of Reference (item b)
The Council of Governors approved the terms of reference. (c) Engagement Programme (item c)
The rationale for the programme was outlined and the importance of increasing engagement with patients, public across the various demographics was emphasised. Governors were advised that events would take place across each constituency and proposals would be identified at constituency meetings. Internal events will be managed by GIPPE and external events by the MDC. The programme will be linked with both Communications and the Membership Engagement Plan and governors will be briefed prior to an event. Youth representation is also being considered by the Trust and an update on the progress was requested. It was noted that a proposal for a combined membership booklet/application form across both Poole and RBCH Hospitals is being considered as a means of increasing membership. The Council of Governors approved the engagement programme.
SA SA
(d) Listening Events (item d)
Further meetings have been programmed for the remainder of the year and the feedback will be reviewed by GIPPE. The dates will be circulated and all governors were encouraged to participate. The ‘you said, we did’ feedback will be followed up after events and publicised. Staff listening events are also being planned.
DR
(e) Governor Uniform (item e)
The use of governor lanyards was supported at events and it was suggested that enamelled governor badges were considered. The Council of Governors agreed to dress smartly but not to dictate a dress code formally.
(f) FT Focus Task & Finish Group (item f)
It was proposed that for each edition of the FT Focus newsletter a task and finish group would form to compile and review the governor section
Council of Governors Meeting 03.02.16 PAGE 9 OF 10
(2 pages). The Council of Governors supported the dissolution of the FT Editorial Group and approved the recommendation to instate a task and finish group. DR to identify members.
DR
07/16 INFORMATION
(a) Forward Planner (item a)
The item was noted for information.
(b) GIPPE and MDC Committee Reports (item b)
The outpatient survey feedback has been analysed and the report will be circulated to departments within the Trust and governors. The Relatives & Carer Audit will be progressed through the volunteers office. Governors are encouraged to participate but must be registered as a volunteer and have received the required training. The questions for the survey monkey questionnaire will be agreed following the consolidation of governor feedback.
DR
(c) Trust Committee Governor Representative Reports (item c)
It was requested that the PLACE report/action plan was followed up and feedback provided to governors.
DR
(d) Appointed Governor Reports
None submitted.
(e) Staff Governor Reports
None submitted.
(f) Governor reports of additional activity - SWGEN (item f)
The item was noted for information.
08/16 DATE OF NEXT MEETING Wednesday 13 April at 08:30, Conference Room, Education Centre
There being no further business the meeting closed at 12:40. AH 03.02.16
Council of Governors Meeting 03.02.16 PAGE 10 OF 10

Council of Governors Meeting – Part 1 03 February 2016
THE ROYAL BOURNEMOUTH AND CHRISTCHURCH HOSPITALS NHS FOUNDATION TRUST
Actions carried forward from a meeting of the Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust Council of Governors Part 1 held on 03 February 2016 and previous.
Actions from Minutes of the Meeting held on 22 January 2015 DECISION
15/58 Revised Statutory and Governor Committee Terms of Reference
Provide a work programme for the next Council of Governors meeting outlining the scope of each committee
SA/ Strategy Committee agenda item
Governor Strategy Committee. Agenda item with a report to be submitted to next CoG (CoG agenda item)
Actions Log from Minutes of the Meeting held on 15 July 2015
15/77 Workforce Report Provide governors with a briefing about the processes in place for the
management of staff sickness, workforce resilience and mandatory training.
KA Information provided within the February Workforce Report. Sickness Audit currently underway and further information will be provided once available.
Actions from Minutes of the Meeting held on 03 February 2016 04/16 PERFORMANCE (a) Performance Report Provide a summary of the mandated targets imposed by both the CCG RR The CCG mandated targets are as
__________________________________________________________________________________________________________________ PAGE 1 OF 4

Council of Governors Meeting – Part 1 03 February 2016
and Monitor including a metric for the risks if these are not achieved.
set out in CoG performance report, and monthly board papers. The consequence of not meeting these in 2016/17 is loss of the £7m Stability and transformation fund (STP). The exact amount at risk for missing a target is not known at this stage.
(c) Workforce Report i) Provide an overview of the staff survey results at the next meeting.
KA/agenda item
To be included in the Workforce Report
ii) Update-Request for further information about exit data following the November Workforce report.
KA Data will be discussed at Workforce Committee after which will be shared with the Board of Directors and Council of Governors
(d) Quality Performance Report i) Include the complaints report for the next meeting. PS To be included in the Quality Report ii) Include the feedback from the governor listening event as an item on the
GIPPE agenda and submit at the report at the next Council of Governors meeting
DR/ GIPPE/CoG Agenda item
Included in agenda pack
05/16 STRATEGY
(b) Vanguard Update Provide further information on the Vanguard Community Project
schemes.
SE CCG have been requested for further details and this will be shared with Governors when it is received
(c) CSR Update
__________________________________________________________________________________________________________________ PAGE 2 OF 4
Council of Governors Meeting – Part 1 03 February 2016
Arrange a governor briefing before the CSR consultation process commences.
SA Not due until the consultant process is announced by CCG
06/16 GOVERNANCE
(a) Dissolution of the Governor Training Committee Arrange a meeting for the Chairs Group
DR Complete. Arranged for 25
February. (c) Engagement Programme
Provide an update on the progress with Youth representation at the Trust.
SA Communications are working on establishing an engagement programme with young people. CoG will be kept up to date with progress.
Develop the application form across both RBCH and Poole Hospital to increase membership.
SA All four trust secretaries were in principle happy to produce a joint form and for the data to be shared through MES (database company). We think we all collect the same data so this should be no problem. Dorset Healthcare and Dorchester have just printed a huge stack of their own forms so would be keen to use these up first.
(d) Listening Events
Circulate the dates for the proposed listening events. DR Dates are being collated. Christchurch and Dorset County are to hold an event at Christchurch
__________________________________________________________________________________________________________________ PAGE 3 OF 4

Council of Governors Meeting – Part 1 03 February 2016
Library on 12 April 10:00-15:00 (f) FT Focus Task & Finish Group Identify members for the group as and when required. DR On-going. Complete for Issue 1. 07/16 INFORMATION (b) GIPPE and MDC Committee Reports
Circulate the outpatient survey report to governors. DR Complete sent 3 February to Governors
(c) Trust Committee Governor Representative Reports
Provide governors with feedback on the PLACE report/action plan. PS Complete – sent 24 February to Governors
__________________________________________________________________________________________________________________ PAGE 4 OF 4
COUNCIL OF GOVERNORS
Meeting Date and Part: 13th April 2016 Part 1
Subject: Quality report
Section on agenda: Performance
Supplementary Reading (included in the Reading Pack)
Proposed quality objective metrics for 2016-17
Officer with overall responsibility: Paula Shobbrook, Director of Nursing and Midwifery
Author(s) of papers: Joanne Sims, Associate Director Quality & Risk Ellen Bull, Deputy Director of Nursing
Details of previous discussion and/or dissemination:
Healthcare Assurance Committee (HAC) Board of Directors
Action required: Discuss/Information
This report provides a summary of information and analysis on the key performance and quality indicators linked to the Board objectives for 15/16. The Trust level dashboard provides information on patient safety and patient experience indicators including:
• Serious Incidents • Safety Thermometer – Harm Free Care • Patient experience performance
These indicators are reviewed each month at the Healthcare Assurance Committee, attended by two governor representatives, and the Board of Directors
Executive Summary: This report provides a summary of information and analysis on the key quality performance indicators, linked to the Board objectives for 15/16, for January and February 2015. The end of year position will be provided at the meeting. 1. Serious Incidents: 3 reported 2. Safety Thermometer: Harm Free Care remains consistent. 3. 2015/16 Quality Objectives:
• Meeting quality objectives for: reducing severe harm events, SIs, serious pressure damage, staff incidents.
• Not meeting quality improvement aim for: falls, medication incidents and never events. 4. Patient experience:
• Positive feedback from our patients
Relevant CQC domain: Safe, Caring, Effective, Responsive & Well Led
Risk Profile: i. Impact on existing risk? ii. Identification of a new risk?
No

Quality and Patient Safety Performance Exception Report:
April 2016
1.0 Purpose of the report
This report accompanies the Quality/Patient Performance Dashboard and outlines the Trust’s performance exceptions against key quality indicators for patient safety and patient experience for the months of January and February 2016
2.0 Serious incidents
There have been 3Serious Incidents reported January - February 2016. All serious incidents have a structured review and root cause analysis, which is discussed at an executive led panel meeting to ensure there is appropriate action, learning and duty of candour.
3.0 Safety Thermometer
All inpatient wards collect the monthly Safety Thermometer (ST) “Harm Free Care” data. This records whether patients have had an inpatient fall within the last 72 hours, a hospital acquired category 2-4 pressure ulcer, a catheter related urinary tract infection and/or, a hospital acquired VTE. If a patient has not had any of these events they are determined to have had “harm free care”.
NHS SAFETY THERMOMETER 14/15 Trust Average
14/15 National Average
Oct 15
Nov 15 Dec 15
Jan 16
Feb 16
Safety Thermometer % Harm Free Care
90.68%
93.80% 90.3% 86.97% 90.9% 84.1% 89.5%
Safety Thermometer % Harm Free Care (New Harms only)
97.18% 97.59% 97.6% 97.7% 97.1% 96.6% 98.4%
4.0 Quality Objectives
The Trust set improvement aims which were included in the Trust’s Quality Objectives for 2015/16, following feedback from clinical staff. These were shared with the Council of Governors as part of the consultation process last year. At the time of writing, the improvement aims are being met for reducing severe harm, serious incidents reported, serious pressure damage and staff incidents. The improvement aims have not been achieved for falls, medication incidents and never events. An update will be provided to the CoG with the end of year figures. Council will also be apprised of the quality objectives and improvement metrics for 2016-17 which will be agreed by the board of directors on 1st April.
CoG April 2016
5.0 Patient Experience
5.1 Family and Friends Test The national performance benchmarking data bullet pointed below is taken from the national data provided by NHS England which is retrospectively available and therefore, represents January 2016 data.
Inpatient and day case Friends and Family Test (FFT) national performance in
January 16 ranked RBCH Trust 3rd with 25 other hospitals out of 172 placing RBCH in the second quartile as per last quarter. The response rate was sustained above the 15% national standard at 19.6%.
The Emergency Department (ED) FFT performance in January 16 ranked RBCH
Trust 6th with 9 other hospitals out of 141 placing RBCH ED department in the top quartile as per last quarter. The response rate 3.3% against the 15% national standard, a reduction on last quarter.
Outpatients FFT performance in January 16 ranked RBCH Trust 4th with 26 other
Trusts out of 234 Trusts, placing the departments in the second quartile, as per last quarter. Response rates are variable between individual outpatient departments; there is not a national response standard.
The Trust continues to receive predominantly positive feedback from patients through FFT and patient experience cards.
5.2 Patient Experience Cards There were 10,077 patient experience cards completed December - February in total which is a testament to the work of our staff and volunteers. The majority of comments are very positive. Themes for negative comments include:
waiting times, discharge lack of communication re. waiting times – particularly ED and OPD attitudes of staff lack of information regarding the patient journey food noise at night lack of compassionate care two comments regarding racism smell of smoking near ED Improvement actions are being led by Heads of Nursing and reported through HAC.
5.3 Care Audit Trend Data The care campaign audit tool has been refined following a request from the Healthcare
Assurance committee. Whilst comments from patients are predominantly positive there is feedback related to noise at night. Improvement actions are being driven by matrons and reported at the HAC.
CoG April 2016

6.0 Recommendation
The Council of Governors is requested to note this report which is provided for information
CoG April 2016

Formal Complaints 1. Introduction
This summary paper includes information on formal complaints received, acknowledged
and responded to times in month (February 2016). Complaints and clinical claims are presented by directorate in terms of incidences, response times and themes. This is measured against our own Trust Policy and reviewed in detail at the Healthcare Assurance Committee.
2. Number of complaints and concerns
• 28 formal complaints were received in February 2016.
3. Acknowledgement and response times
Acknowledgements to the patient/carer/relative may be by telephone/letter and email within the timeframes to acknowledge the complaint. This remains largely consistent meeting the 100% Trust target.
Responses to complaints should be within 25 working days (quality strategy standard of 75%), which is monitored monthly at the Healthcare Assurance Committee. For February on aggregate the response times was 44% (12 out of 27 complaint responses due were within 25 working days)
The graphs below show the performance for first responses due in February 2016 by Care Group. All Care Groups need to improve consistency in response times with Care Group B needing significant improvement.
Directorates requiring the most focus and support to close complaints within the 25
working day deadline are medicine and older people’s medicine, with surgery, anaesthetics and orthopaedics all having overdue complaints at February end. Responses are being chased. Response time improvement remains a strong focus. Directorate leads
0%
20%
40%
60%
80%
100%
Perf
orm
ance
Mar-15 Apr-15 May-
15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16
CGRPA 22% 56% 67% 64% 91% 71% 67% 60% 60% 60% 50% 57%CGRPB 73% 43% 67% 55% 40% 20% 17% 27% 36% 50% 25% 29%CGRPC 75% 100% 33% 67% 75% 83% 100% 50% 100% 67% 100% 60%
Formal Complaints with 1st Response within 25 Working Days of Receipt (by month 1st Response Due)
are requested to monitor and support closing their overdue and pending complaints to improve the overall position. A request has been made of the Heads of Nursing to discuss with directorates 16/17 improvement trajectories, which it is proposed will be by quarter.
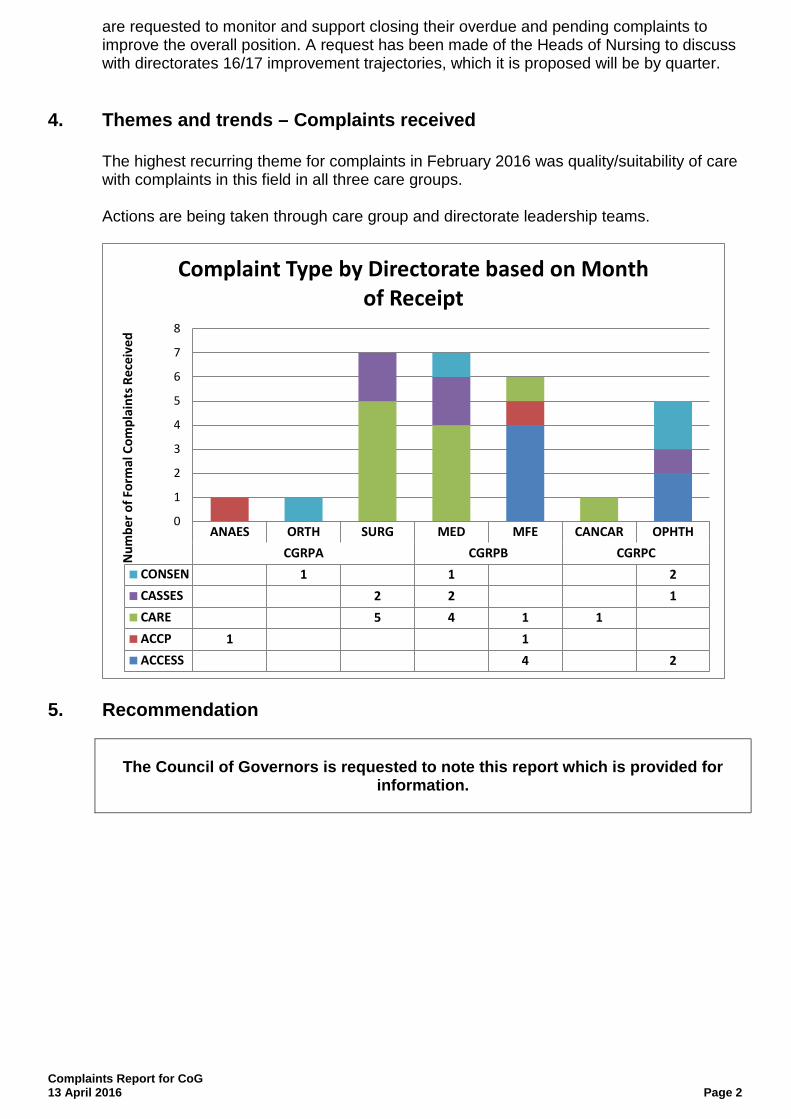
4. Themes and trends – Complaints received
The highest recurring theme for complaints in February 2016 was quality/suitability of care
with complaints in this field in all three care groups. Actions are being taken through care group and directorate leadership teams.
5. Recommendation
The Council of Governors is requested to note this report which is provided for information.
ANAES ORTH SURG MED MFE CANCAR OPHTHCGRPA CGRPB CGRPC
CONSEN 1 1 2CASSES 2 2 1CARE 5 4 1 1ACCP 1 1ACCESS 4 2
0
1
2
3
4
5
6
7
8
Num
ber o
f For
mal
Com
plai
nts R
ecei
ved
Complaint Type by Directorate based on Month of Receipt
Complaints Report for CoG 13 April 2016 Page 2

COUNCIL OF GOVERNORS Meeting Date: 13 April 2016
Subject: Performance Summary Report Q4 – 2015/16
Section on agenda: Performance
Officer with overall responsibility: Richard Renaut, Chief Operating Officer
Author(s) of papers: Donna Parker / David Mills
Details of previous discussion and/or dissemination:
Action required: Approve / Discuss / Information / Note
The Council of Governors is asked to consider the information provided in the Report and accompanying Performance Indicator Matrix.
Executive Summary:
This report provides a summary of the key performance highlights and non-compliances in Q4 2015/16. It outlines the key challenges and context of the non-compliances as well as our plans for recovery. As an overview of the key risks for our final Q4 position, these are ED 4 hour, Cancer 31 day waits, and C Difficile compliance. There is some risk related to the 62 day target. The report also references the requirements of the national Sustainability and Transformation Fund for 2016/17.
Relevant CQC domain:
Are they safe?
Are they effective?
Are they caring?
Are they responsive to people's needs?
Are they well-led?
Yes
Yes
Yes
Yes
Risk Profile:
i) Impact on existing risk?
ii) Identification of a new risk?
Council of Governors 13 April 2016
Performance Summary Report Quarter 4 - 2015/16
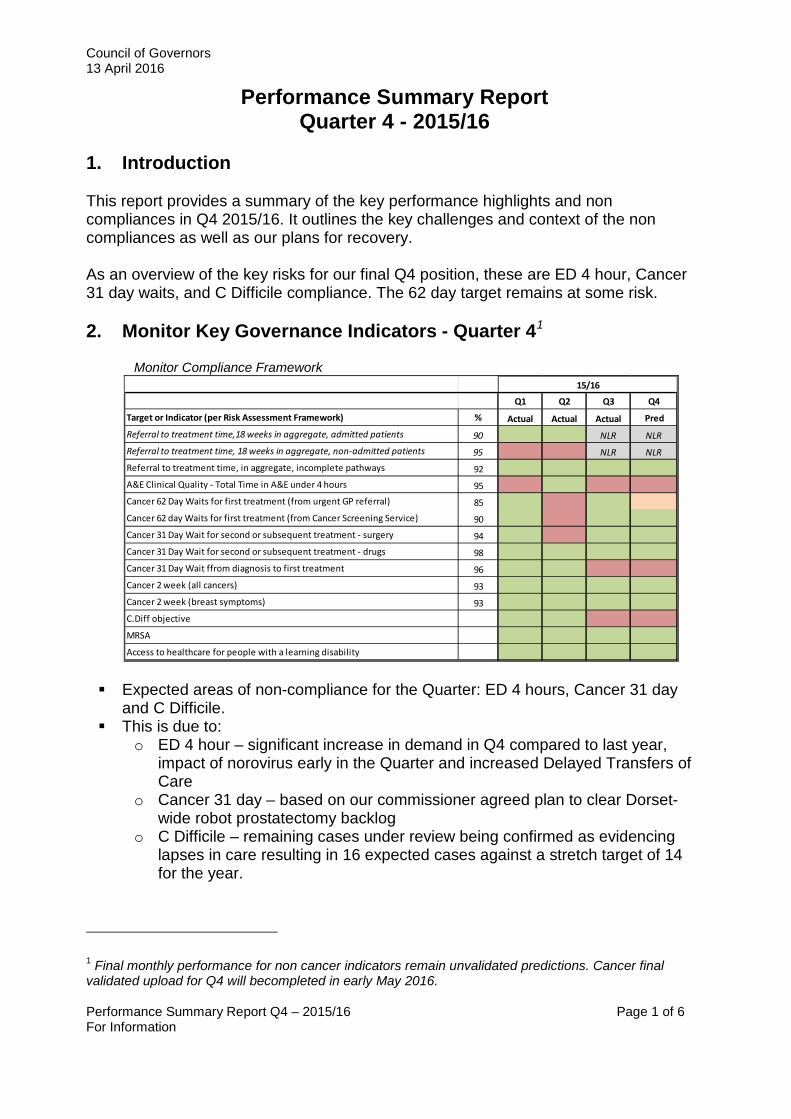
1. Introduction This report provides a summary of the key performance highlights and non compliances in Q4 2015/16. It outlines the key challenges and context of the non compliances as well as our plans for recovery. As an overview of the key risks for our final Q4 position, these are ED 4 hour, Cancer 31 day waits, and C Difficile compliance. The 62 day target remains at some risk. 2. Monitor Key Governance Indicators - Quarter 41 Monitor Compliance Framework
Q1 Q2 Q3 Q4
Target or Indicator (per Risk Assessment Framework) % Actual Actual Actual Pred
Referral to treatment time,18 weeks in aggregate, admitted patients 90 NLR NLRReferral to treatment time, 18 weeks in aggregate, non-admitted patients 95 NLR NLRReferral to treatment time, in aggregate, incomplete pathways 92A&E Clinical Quality - Total Time in A&E under 4 hours 95Cancer 62 Day Waits for first treatment (from urgent GP referral) 85Cancer 62 day Waits for first treatment (from Cancer Screening Service) 90Cancer 31 Day Wait for second or subsequent treatment - surgery 94Cancer 31 Day Wait for second or subsequent treatment - drugs 98Cancer 31 Day Wait ffrom diagnosis to first treatment 96Cancer 2 week (all cancers) 93Cancer 2 week (breast symptoms) 93C.Diff objective
MRSA
Access to healthcare for people with a learning disability
15/16
Expected areas of non-compliance for the Quarter: ED 4 hours, Cancer 31 day
and C Difficile. This is due to:
o ED 4 hour – significant increase in demand in Q4 compared to last year, impact of norovirus early in the Quarter and increased Delayed Transfers of Care
o Cancer 31 day – based on our commissioner agreed plan to clear Dorset-wide robot prostatectomy backlog
o C Difficile – remaining cases under review being confirmed as evidencing lapses in care resulting in 16 expected cases against a stretch target of 14 for the year.
1 Final monthly performance for non cancer indicators remain unvalidated predictions. Cancer final validated upload for Q4 will becompleted in early May 2016. Performance Summary Report Q4 – 2015/16 Page 1 of 6 For Information
Council of Governors 13 April 2016 The cancer 62 day target is a handful of patients either way to being compliant for
Q4. Final outturn will be dependent upon exact numbers of further treatments and cancer diagnoses confirmed.
The ED 4 hour and cancer targets performance are the subject of Contract Penalty Notices received by the Trust from our commissioners. Action plans and recovery trajectories have been agreed.
3. Contractual and Other Key Indicators - Quarter 4 Mixed sex accommodation breaches since the new protocol has further improved
in Q4 to date compared to Q3. The 6 week wait endoscopy diagnostic backlog clearance plan has remained
ahead of trajectory, achieving compliance in February (99.01%). Continued compliance is currently projected for end March. Demand and capacity pressures in Radiology and Cardiology do present some risk going forward, however, this is currently managed through additional sessions, outsourcing and locum/substantive appointments.
Although there has been an increase in cancelled operations due to winter bed pressures, unplanned Anaesthetist shortages and junior doctor strikes, there have been no 28 day rebook breaches to date in Q4.
The published Q3 Stroke Sentinel National Audit Programme results showed we retained level B. Results score was 80, just 0.1 below the threshold for a level A.
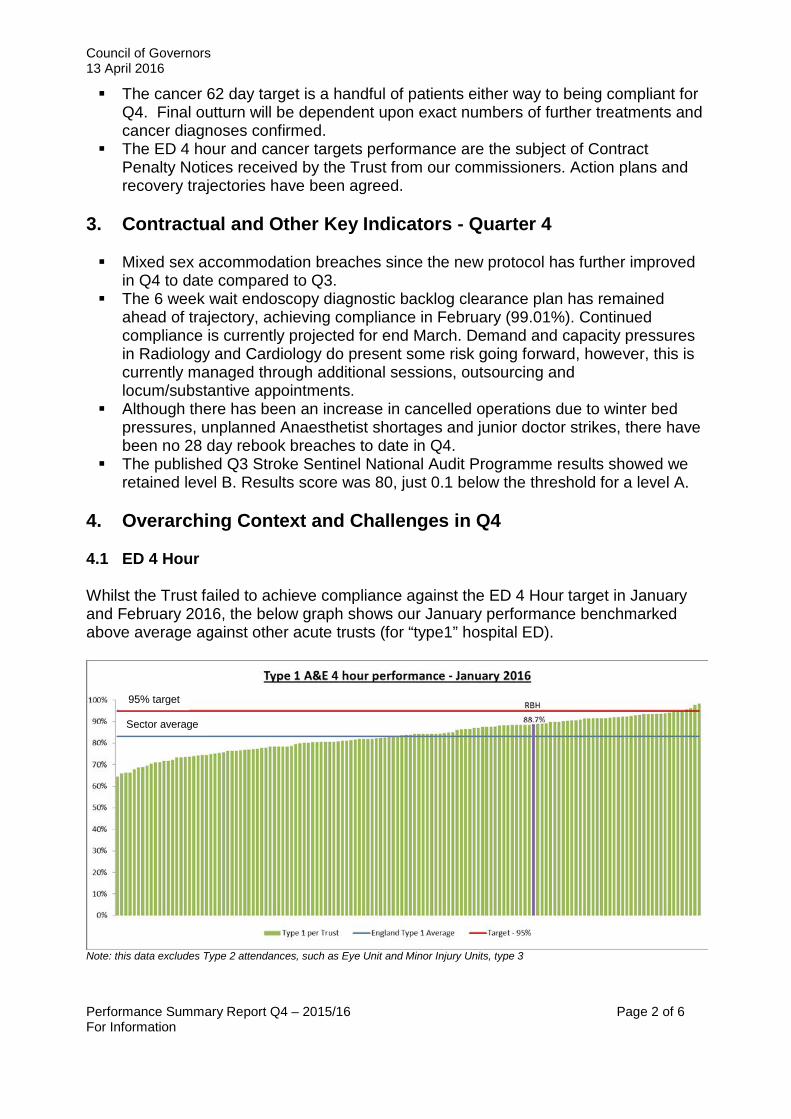
4. Overarching Context and Challenges in Q4 4.1 ED 4 Hour Whilst the Trust failed to achieve compliance against the ED 4 Hour target in January and February 2016, the below graph shows our January performance benchmarked above average against other acute trusts (for “type1” hospital ED).
Note: this data excludes Type 2 attendances, such as Eye Unit and Minor Injury Units, type 3
Sector average
95% target
Performance Summary Report Q4 – 2015/16 Page 2 of 6 For Information

Council of Governors 13 April 2016 February and March have seen pressures with a significant increase in non elective admissions compared to February last year (11.8%). This, along with a rise ED attendances (11.9% above February last year) and a high level of delayed discharges, resulted in a reduction in patient flow through the hospital. This meant that the Trust missed compliance in February with the ED 4 hour target, at 92.58% (though marginally better than February 2015 – 91.59%). March though is showing a decline, both at RBH and neighbouring Trusts.
Performance Summary Report Q4 – 2015/16 Page 3 of 6 For Information

Council of Governors 13 April 2016 4.2 Cancer Pooling the waiting lists for robotic prostatectomy patients across East and West Dorset has now commenced (February) along with the further additional sessions supported by Dorset County Hospital to reduce the backlog of patients waiting for this procedure. A significant reduction in waits has already been seen as a result of pooling the list. Monthly and quarterly compliance for the 62 day target will be finalised following final scheduling of some of the additional March capacity and as some cancer diagnoses are confirmed, but this currently remains borderline on compliance. A recovery trajectory has been agreed with Dorset CCG which clears backlog in Q1 and achieves compliance by Q2. This has also impacted on the 31 day target which remains below compliance in Q4, but in line with the trajectory agreed with our commissioners. 4.3 C Difficile By the end of January 2016, we reached the annual allowed target of C Diff cases due to lapses in care (14). In February, 1 more case was reported and a further in March. This has resulted in a total of 16 cases and thus non compliance for this indicator for this financial year. However, our rate remained low in February (see chart). 4.4 RTT The Trust continues to be compliant against the Incomplete Pathways target, though with a reduction in performance to 92.8% in February with 19,732 patients waiting less than 18 weeks. This is predominantly due to the significant increase in the waiting list for patients who require elective admission, particularly in: Urology, Orthopaedics and Ophthalmology. Some additional pressures are also being seen in Cardiology, Gynaecology, plus the visiting specialities of ENT and Allergy. Unplanned shortages in Anaesthetist capacity, prioritising capacity for cancer patients, together with increased referrals and winter bed pressures have impacted on our position this Quarter. However, we do anticipate remaining compliant overall for the Quarter.
Performance Summary Report Q4 – 2015/16 Page 4 of 6 For Information

Council of Governors 13 April 2016
5. Recovery Plans and 16/17 Two key streams of work are underway, implementing detailed action plans for the recovery of our key performance indicators: Cancer and ED 4 hour/Flow. 5.1 ED 4 hour The Trust continues to strive for full monthly and quarter performance. Our Quality Improvement work this year has continued to demonstrate a reduction in length of stay which will remain a continued focus for our work in 16/17.
Key actions going forward include: • Further development of Frailty pathways through the establishment of a Frailty
Unit, incorporating recommendations from the Frailty Network • Expansion of our Ambulatory Care pathways, particularly in Older Person’s
Medicine, Cardiology and Stroke • Bed capacity planning for 16/17, flexing to reflect in year variation • Implementation of revised ED Action Plan following positive review by the Monitor
Improvement Team, including reviewing and developing our escalation trigger and prediction tools and related protocols
• Elective care LoS programme, with a particular focus on Orthopaedics, together with Theatre efficiency QI programme
• Joint work with partner organisations to implement recommendations from an external review of delayed transfers of care.
There is considerable activity and implementation of plans underway to cope with rising demand and lower funding for social care. Furthermore, the impact of continued reduction in community/social care capacity remain significant and in addition to the potential impact of ongoing junior doctor strikes. The net effect is there remains a high risk of emergency care pressures stopping 4 hour compliance, despite innovation and improvement, and strong partnership working. Performance Summary Report Q4 – 2015/16 Page 5 of 6 For Information
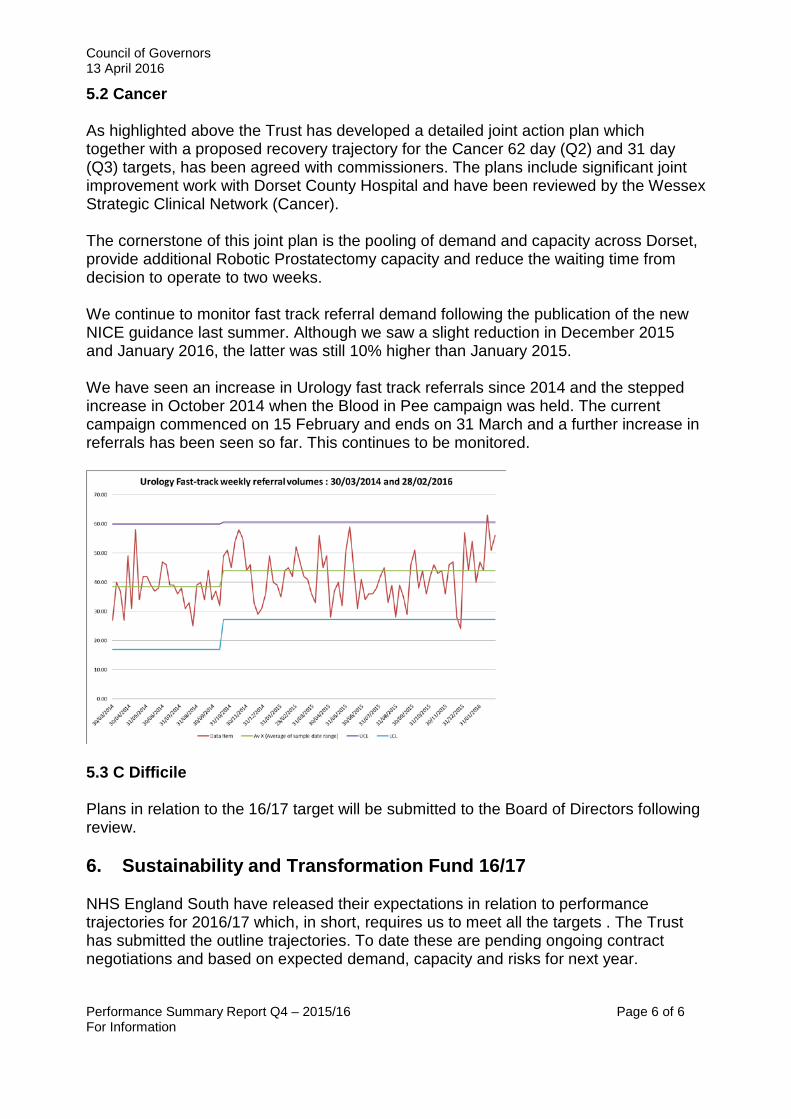
Council of Governors 13 April 2016 5.2 Cancer As highlighted above the Trust has developed a detailed joint action plan which together with a proposed recovery trajectory for the Cancer 62 day (Q2) and 31 day (Q3) targets, has been agreed with commissioners. The plans include significant joint improvement work with Dorset County Hospital and have been reviewed by the Wessex Strategic Clinical Network (Cancer). The cornerstone of this joint plan is the pooling of demand and capacity across Dorset, provide additional Robotic Prostatectomy capacity and reduce the waiting time from decision to operate to two weeks. We continue to monitor fast track referral demand following the publication of the new NICE guidance last summer. Although we saw a slight reduction in December 2015 and January 2016, the latter was still 10% higher than January 2015. We have seen an increase in Urology fast track referrals since 2014 and the stepped increase in October 2014 when the Blood in Pee campaign was held. The current campaign commenced on 15 February and ends on 31 March and a further increase in referrals has been seen so far. This continues to be monitored.
5.3 C Difficile Plans in relation to the 16/17 target will be submitted to the Board of Directors following review. 6. Sustainability and Transformation Fund 16/17 NHS England South have released their expectations in relation to performance trajectories for 2016/17 which, in short, requires us to meet all the targets . The Trust has submitted the outline trajectories. To date these are pending ongoing contract negotiations and based on expected demand, capacity and risks for next year. Performance Summary Report Q4 – 2015/16 Page 6 of 6 For Information
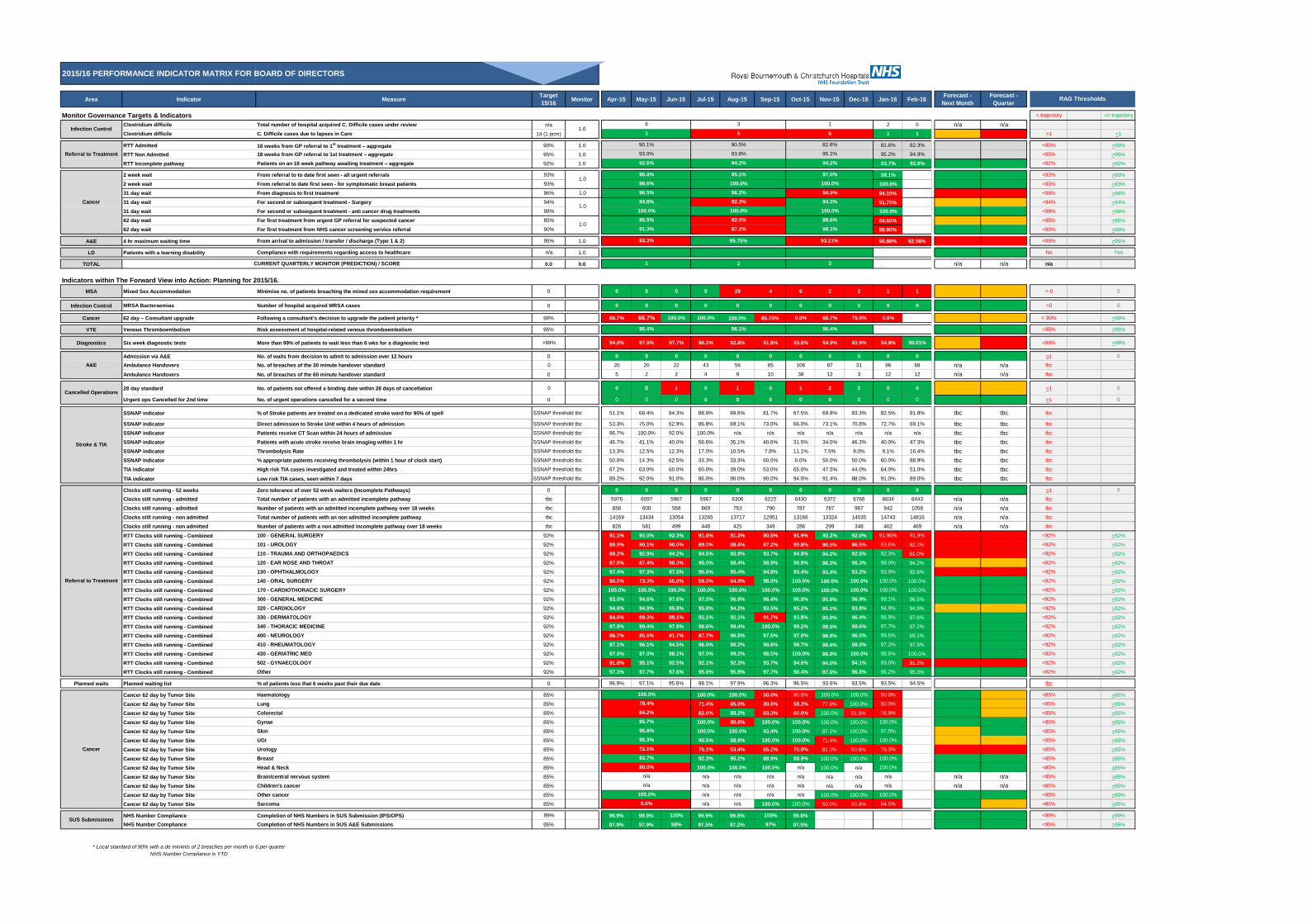
2015/16 PERFORMANCE INDICATOR MATRIX FOR BOARD OF DIRECTORS
Area Indicator Measure Target 15/16 Monitor Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Forecast -
Next MonthForecast -
Quarter
Monitor Governance Targets & Indicators > trajectory <= trajectory
Clostridium difficile Total number of hospital acquired C. Difficile cases under review n/a 2 0 n/a n/aClostridium difficile C. Difficile cases due to lapses in Care 14 (1 pcm) 1 1 >1 <1
RTT Admitted 18 weeks from GP referral to 1st treatment – aggregate 90% 1.0 81.6% 82.3% <90% >90%
RTT Non Admitted 18 weeks from GP referral to 1st treatment – aggregate 95% 1.0 95.2% 94.9% <95% >95%
RTT Incomplete pathway Patients on an 18 week pathway awaiting treatment – aggregate 92% 1.0 93.7% 92.8% <92% >92%
2 week wait From referral to to date first seen - all urgent referrals 93% 98.1% <93% >93%
2 week wait From referral to date first seen - for symptomatic breast patients 93% 100.0% <93% >93%
31 day wait From diagnosis to first treatment 96% 1.0 94.10% <96% >96%
31 day wait For second or subsequent treatment - Surgery 94% 91.70% <94% >94%
31 day wait For second or subsequent treatment - anti cancer drug treatments 98% 100.0% <98% >98%
62 day wait For first treatment from urgent GP referral for suspected cancer 85% 84.50% <85% >85%
62 day wait For first treatment from NHS cancer screening service referral 90% 88.90% <90% >90%
A&E 4 hr maximum waiting time From arrival to admission / transfer / discharge (Type 1 & 2) 95% 1.0 90.88% 92.58% <95% >95%
LD Patients with a learning disability Compliance with requirements regarding access to healthcare n/a 1.0 No Yes
TOTAL 0.0 0.0 n/a n/a n/a
Indicators within The Forward View into Action: Planning for 2015/16.MSA Mixed Sex Accommodation Minimise no. of patients breaching the mixed sex accommodation requirement 0 0 0 0 0 29 4 6 2 2 1 1 > 0 0
Infection Control MRSA Bacteraemias Number of hospital acquired MRSA cases 0 0 0 0 0 0 0 0 0 0 0 0 >0 0
Cancer 62 day – Consultant upgrade Following a consultant’s decision to upgrade the patient priority * 90% 66.7% 66.7% 100.0% 100.0% 100.0% 85.70% 0.0% 66.7% 75.0% 0.0% < 90% >90%
VTE Venous Thromboembolism Risk assessment of hospital-related venous thromboembolism 95% <95% >95%
Diagnostics Six week diagnostic tests More than 99% of patients to wait less than 6 wks for a diagnostic test >99% 94.8% 97.9% 97.7% 96.2% 92.8% 91.8% 93.8% 94.9% 93.9% 94.9% 99.01% <99% >99%
Admission via A&E No. of waits from decision to admit to admission over 12 hours 0 0 0 0 0 0 0 0 0 0 0 0 >1 0
Ambulance Handovers No. of breaches of the 30 minute handover standard 0 20 20 22 43 56 85 106 87 31 96 68 n/a n/a tbc
Ambulance Handovers No. of breaches of the 60 minute handover standard 0 5 2 2 4 9 10 38 12 3 12 12 n/a n/a tbc
28 day standard No. of patients not offered a binding date within 28 days of cancellation 0 0 0 1 0 1 0 1 2 0 0 0 >1 0
Urgent ops Cancelled for 2nd time No. of urgent operations cancelled for a second time 0 0 0 0 0 0 0 0 0 0 0 0 >1 0
SSNAP indicator % of Stroke patients are treated on a dedicated stroke ward for 90% of spell SSNAP threshold tbc 51.1% 69.4% 84.3% 88.9% 89.6% 81.7% 67.5% 69.8% 83.3% 82.5% 81.8% tbc tbc tbc
SSNAP indicator Direct admission to Stroke Unit within 4 hours of admission SSNAP threshold tbc 53.3% 75.0% 62.9% 86.8% 69.1% 73.0% 66.0% 73.1% 70.8% 72.7% 69.1% tbc tbc tbc
SSNAP indicator Patients receive CT Scan within 24 hours of admission SSNAP threshold tbc 96.7% 100.0% 92.0% 100.0% n/a n/a n/a n/a n/a n/a n/a tbc tbc tbc
SSNAP indicator Patients with acute stroke receive brain imaging within 1 hr SSNAP threshold tbc 46.7% 41.1% 40.0% 56.6% 35.1% 40.6% 31.5% 34.0% 46.3% 40.0% 47.3% tbc tbc tbc
SSNAP indicator Thrombolysis Rate SSNAP threshold tbc 13.3% 12.5% 12.3% 17.0% 10.5% 7.8% 11.1% 7.5% 9.0% 9.1% 16.4% tbc tbc tbc
SSNAP indicator % appropriate patients receiving thrombolysis (within 1 hour of clock start) SSNAP threshold tbc 50.0% 14.3% 62.5% 33.3% 33.3% 60.0% 0.0% 50.0% 50.0% 60.0% 88.9% tbc tbc tbc
TIA indicator High risk TIA cases investigated and treated within 24hrs SSNAP threshold tbc 67.2% 63.0% 60.0% 60.0% 39.0% 53.0% 65.0% 47.5% 44.0% 64.0% 51.0% tbc tbc tbc
TIA indicator Low risk TIA cases, seen within 7 days SSNAP threshold tbc 89.2% 92.0% 91.0% 86.0% 90.0% 90.0% 94.0% 91.4% 88.0% 91.0% 89.0% tbc tbc tbc
Clocks still running - 52 weeks Zero tolerance of over 52 week waiters (Incomplete Pathways) 0 0 0 0 0 0 0 0 0 0 0 0 >1 0
Clocks still running - admitted Total number of patients with an admitted incomplete pathway tbc 5976 6097 5967 5967 6306 6222 6430 6372 6766 6634 6443 n/a n/a tbc
Clocks still running - admitted Number of patients with an admitted incomplete pathway over 18 weeks tbc 656 600 568 669 753 790 787 787 967 942 1058 n/a n/a tbc
Clocks still running - non admitted Total number of patients with an non admitted incomplete pathway tbc 14169 13434 13054 13265 13717 12951 13166 13324 14035 14743 14816 n/a n/a tbc
Clocks still running - non admitted Number of patients with a non admitted incomplete pathway over 18 weeks tbc 826 581 499 448 425 349 286 299 348 402 469 n/a n/a tbc
RTT Clocks still running - Combined 100 - GENERAL SURGERY 92% 91.1% 93.0% 92.3% 91.6% 91.3% 90.5% 91.9% 92.2% 92.0% 91.96% 91.9% <92% >92%
RTT Clocks still running - Combined 101 - UROLOGY 92% 89.9% 90.1% 90.0% 89.0% 88.4% 87.2% 89.8% 90.5% 86.5% 83.6% 82.2% <92% >92%
RTT Clocks still running - Combined 110 - TRAUMA AND ORTHOPAEDICS 92% 89.2% 92.9% 94.2% 94.5% 93.9% 93.7% 94.8% 94.2% 92.5% 92.3% 91.0% <92% >92%
RTT Clocks still running - Combined 120 - EAR NOSE AND THROAT 92% 87.8% 87.4% 90.3% 95.0% 98.4% 98.9% 98.9% 98.2% 96.3% 98.0% 94.2% <92% >92%
RTT Clocks still running - Combined 130 - OPHTHALMOLOGY 92% 97.4% 97.3% 97.5% 96.6% 95.4% 94.8% 93.4% 93.4% 93.2% 93.9% 92.6% <92% >92%
RTT Clocks still running - Combined 140 - ORAL SURGERY 92% 80.5% 73.3% 65.8% 59.5% 84.9% 98.0% 100.0% 100.0% 100.0% 100.0% 100.0% <92% >92%
RTT Clocks still running - Combined 170 - CARDIOTHORACIC SURGERY 92% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% <92% >92%
RTT Clocks still running - Combined 300 - GENERAL MEDICINE 92% 93.0% 94.6% 97.6% 97.5% 96.9% 96.4% 96.9% 95.8% 96.9% 99.1% 96.5% <92% >92%
RTT Clocks still running - Combined 320 - CARDIOLOGY 92% 94.6% 94.9% 95.8% 95.8% 94.2% 93.5% 95.2% 95.1% 93.8% 94.9% 94.9% <92% >92%
RTT Clocks still running - Combined 330 - DERMATOLOGY 92% 84.6% 89.3% 89.1% 92.1% 92.1% 91.7% 93.8% 93.8% 96.4% 96.9% 97.6% <92% >92%
RTT Clocks still running - Combined 340 - THORACIC MEDICINE 92% 97.9% 99.4% 97.9% 98.6% 99.4% 100.0% 99.2% 99.5% 98.6% 97.7% 97.2% <92% >92%
RTT Clocks still running - Combined 400 - NEUROLOGY 92% 86.7% 85.6% 81.7% 87.7% 96.8% 97.5% 97.0% 98.8% 96.5% 99.5% 99.1% <92% >92%
RTT Clocks still running - Combined 410 - RHEUMATOLOGY 92% 97.1% 96.1% 94.5% 96.9% 98.2% 98.6% 98.7% 98.4% 98.0% 97.2% 97.9% <92% >92%
RTT Clocks still running - Combined 430 - GERIATRIC MED 92% 97.8% 97.0% 98.1% 97.0% 99.2% 98.5% 100.0% 98.9% 100.0% 98.6% 100.0% <92% >92%
RTT Clocks still running - Combined 502 - GYNAECOLOGY 92% 91.8% 95.1% 92.5% 92.1% 92.3% 93.7% 94.6% 94.0% 94.1% 93.0% 91.2% <92% >92%
RTT Clocks still running - Combined Other 92% 97.3% 97.7% 97.6% 95.6% 95.9% 97.7% 96.4% 97.9% 96.8% 96.2% 95.3% <92% >92%
Planned waits Planned waiting list % of patients less that 6 weeks past their due date 0 96.9% 97.1% 95.6% 98.1% 97.9% 96.3% 96.5% 93.6% 93.5% 93.5% 94.5% tbc
Cancer 62 day by Tumor Site Haematology 85% 100.0% 100.0% 50.0% 80.0% 100.0% 100.0% 50.0% <85% >85%
Cancer 62 day by Tumor Site Lung 85% 71.4% 65.0% 80.0% 58.3% 77.8% 100.0% 60.0% <85% >85%
Cancer 62 day by Tumor Site Colorectal 85% 82.6% 88.2% 83.3% 60.0% 100.0% 81.0% 76.9% <85% >85%
Cancer 62 day by Tumor Site Gynae 85% 100.0% 80.0% 100.0% 100.0% 100.0% 100.0% 100.0% <85% >85%
Cancer 62 day by Tumor Site Skin 85% 100.0% 100.0% 93.4% 100.0% 97.1% 100.0% 97.0% <85% >85%
Cancer 62 day by Tumor Site UGI 85% 90.5% 88.9% 100.0% 100.0% 71.4% 100.0% 100.0% <85% >85%
Cancer 62 day by Tumor Site Urology 85% 70.1% 53.4% 65.2% 70.0% 81.3% 83.6% 76.3% <85% >85%
Cancer 62 day by Tumor Site Breast 85% 92.3% 95.2% 88.9% 88.9% 100.0% 100.0% 100.0% <85% >85%
Cancer 62 day by Tumor Site Head & Neck 85% 100.0% 100.0% 100.0% n/a 100.0% n/a 100.0% <85% >85%
Cancer 62 day by Tumor Site Brain/central nervous system 85% n/a n/a n/a n/a n/a n/a n/a n/a n/a <85% >85%
Cancer 62 day by Tumor Site Children's cancer 85% n/a n/a n/a n/a n/a n/a n/a n/a n/a <85% >85%
Cancer 62 day by Tumor Site Other cancer 85% n/a n/a n/a n/a 100.0% 100.0% 100.0% <85% >85%
Cancer 62 day by Tumor Site Sarcoma 85% n/a n/a 100.0% 100.0% 50.0% 60.0% 84.5% <85% >85%
NHS Number Compliance Completion of NHS Numbers in SUS Submission (IPS/OPS) 99% 99.9% 99.9% 100% 99.9% 99.8% 100% 99.8% <99% >99%
NHS Number Compliance Completion of NHS Numbers in SUS A&E Submissions 95% 97.9% 97.9% 98% 97.5% 97.2% 97% 97.5% <95% >95%
* Local standard of 90% with a de minimis of 2 breaches per month or 6 per quarterNHS Number Compliance is YTD
n/a
100.0%0.0%
95.3%72.1%93.7%80.0%
n/a
1
100.0%
95.8%
RAG Thresholds
Infection Control
Referral to Treatment
Cancer
32
1.0
1.0
1.0
94.9%94.3%100.0%88.6%98.1%
93.21%
SUS Submissions
CURRENT QUARTERLY MONITOR (PREDICTION) / SCORE
A&E
Cancelled Operations
Stroke & TIA
Referral to Treatment
Cancer
1.0
6
1
90.1%
93.0%
92.6%
79.4%84.2%85.7%
92.2%96.2%100.0%95.1%
96.4%96.1%95.4%
98.6%96.5%94.8%100.0%85.5%91.3%
93.3% 95.75%
97.0%100.0%
87.2%82.6%100.0%
6
1
96.4%
3
6
94.2%
93.8%
90.5% 82.8%
95.2%
94.2%

COUNCIL OF GOVERNORS Meeting Date and Part:
13 April 2016 – Part I
Subject:
Financial Performance
Section:
Performance
Author of Paper:
Pete Papworth, Deputy Director of Finance
Details of previous discussion and/or dissemination:
Finance Committee, Trust Management Board, and Board of Directors
Key Purpose:
Patient Engagement Governance Performance Strategy
Yes Action Required by Council of Governors:
The Council of Governors is asked to note the financial performance of the Trust.
Summary:
The Trust has delivered a cumulative deficit of £11.1 million as at 29 February. This is £1.027 million better than the initial budget plan which amounts to a full year deficit of £12.9 million. As a result, the Trust is expecting to achieve a year end deficit marginally below the revised plan of £11.9 million.
Strategic Goals & Objectives:
Goal 7 – Financial Stability
Links to CQC Registration: (Outcome reference)
Outcome 26 – Financial Position
THE ROYAL BOURNEMOUTH AND CHRISTCHURCH HOSPITALS NHS FOUNDATION TRUST
Report to the Council of Governors Meeting on 13 April 2016
FINANCIAL PERFORMANCE FOR THE PERIOD TO 29 FEBRUARY 2016
INTRODUCTION This report summarises the financial performance of the Trust for the period to 29 February 2016. CURRENT FINANCIAL PERFORMANCE The Trust has delivered a cumulative deficit of £11.1 million as at 29 February. This is £1.027 million better than the initial budget plan which amounts to a full year deficit of £12.9 million. As a result, the Trust is expecting to achieve a year end deficit marginally below the revised plan of £11.9 million. Income remains broadly on plan at the end of month eleven with a moderate adverse variance of £464,000 (0.2%). Increases in non contracted activity and non patient related income are more than off-set by the significant under achievement against planned private patient income. Expenditure reports a modest under spend of £1.5 million to date equating to a variance of 0.6%. This is mainly driven by a significant pay under spend, off-set by over spends against drugs and clinical supplies budgets. Whilst the Trust remains heavily reliant upon agency staff, the premium cost has been considerably less than expected. This reflects the relentless internal focus supported by the introduction of national controls and support. By exception, to ensure patient safety, the Trust has utilised off-framework agencies and paid above cap rates. All such exceptions are subject to a rigorous executive approval process. As at 29 February the Trust has committed £13.3 million in capital spend. Key areas of spend include the Christchurch development (£4 million), the Jigsaw new build (£2.9 million), and the Trusts IT Strategy (£2.2 million). The full year forecast is for an under spend of £3.8 million, reflecting delays in the Christchurch Development and the decision not to progress the relocation of Ambulatory and Emergency Care. Under Monitor’s new risk assessment framework the Trust achieves a Financial Sustainability Rating of 2 meaning that it is within the ‘Material Risk and Potential Investigation’ category. Monitor has concluded its investigation, and the outcome is expected imminently. The Trust is keen to increase openness and transparency, and as such, further detail in relation to the Trusts financial position is included within the redesigned, public finance report to the Board of Directors which is attached. RECOMMENDATION Members are asked to note the Trust’s financial performance for the period ending 29 February 2016,

The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Pete Papworth Deputy Director of Finance
Finance Report
For the period to 29 February 2016

Finance Report As at 29 February 2016
Executive Summary The Trust has delivered a cumulative deficit of £11.1 million as at 29 February. This is £1.027 million better than the initial budget plan which amounts to a full year deficit of £12.9 million. As a result, the Trust is expecting to achieve a year end deficit marginally below the revised plan of £11.9 million.
Activity
February reported an increase in activity, being 1% above planned levels overall. Particular pressures were seen in relation to non-elective activity, which was 8% above budget. Outpatient activity also saw an increase during February, being 1% above budget. Elective activity, due to capacity issues resulting from additional emergency patients together with the Junior Doctors strike action, was below budgeted levels by 0.3%. Emergency Department attendances were consistent with budgeted levels in month.
Income
Due to the nature of the Trusts contracts with its three key commissioners, income remains broadly on plan with a moderate adverse variance of £464,000 (0.2%). Increases in non contracted activity and non patient related income are more than off-set by the significant under achievement against planned private patient income. Income reported a favourable variance of £36,000 during February.
Expenditure
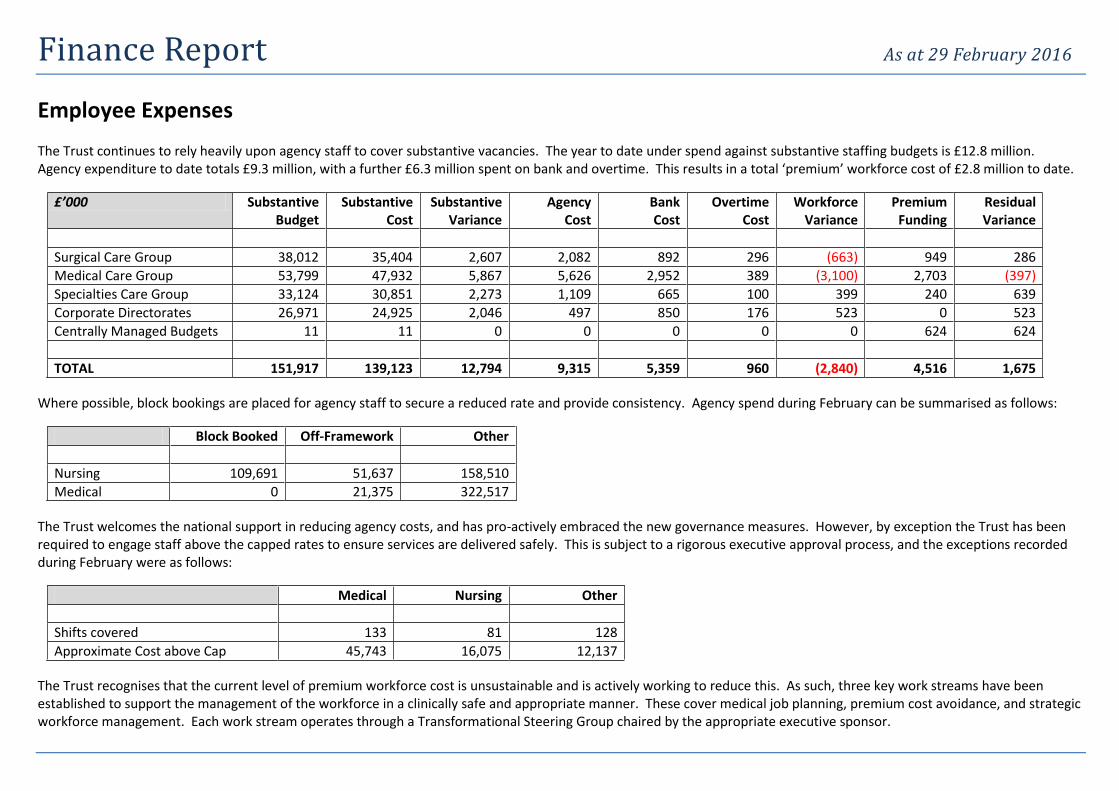
Expenditure reported an under spend of £464,000 during February resulting in a modest under spend of £1.5 million to date and equating to a variance of 0.6%. This is mainly driven by a significant pay under spend, off-set by over spends against drugs and clinical supplies budgets. Whilst the Trust remains heavily reliant upon agency staff, the premium cost has been considerably less than expected. This reflects the relentless internal focus supported by the introduction of national controls and support.
Cost Improvement Programme
To date the Trust has recorded savings of £8.2 million which is £244,000 ahead of the year to date target. The full year savings forecast reduced marginally in month and stands at £9.5 million which is £410,000 more than the target. However, the level of non-recurrent savings within this forecast remains a cause for concern.
Capital Programme
As at 29 February the Trust has committed £13.3 million in capital spend. Key areas of spend include the Christchurch development (£4 million), the Jigsaw new build (£2.9 million), and the Trusts IT Strategy (£2.2 million). The full year forecast is for an under spend of £3.8 million, reflecting delays in the Christchurch Development and the decision not to progress the relocation of Ambulatory and Emergency Care.
Statement of Financial Position
Overall the Trust’s Statement of Financial Position is on plan; however some key variances remain against individual balances. Specifically, the trust continues to report high levels of outstanding payables and receivables. The main balances are with local NHS organisations and work to resolve a number of outstanding issues has continued. This is expected to conclude shortly, for payment before 31 March.
Cash
The Trusts current cash balance includes two one-off timing benefits. After adjusting for these, the Trust currently holds £30.4 million of cash. The current forecast is that the Trust will end the year with an underlying cash balance of £26.9 million. The Trust must continue to reduce its deficit forecast in future years and proactively manage its working capital to avoid the need for external financing.
Financial Sustainability Risk Rating
Under Monitor’s new risk assessment framework the Trust achieves a Financial Sustainability Rating of 2 meaning that it is within the ‘Material Risk and Potential Investigation’ category. Monitor has concluded its investigation, and the outcome is expected imminently.

Finance Report As at 29 February 2016
Income and Expenditure To date the Trust is reporting a deficit of £11.1 million. Within this, income is below budget (adverse) by £464,000 and expenditure is below budget (favourable) by £1.491 million. This results in a net favourable variance of £1.027 million. The Trusts overall income and expenditure position is summarised below.
£’000 Budget Actual Variance
NHS Clinical Income 223,382 223,953 571
Non NHS Clinical Income 7,023 5,652 (1,371)
Non Clinical Income 19,168 19,504 336
TOTAL INCOME 249,573 249,109 (464)
Employee Expenses 156,433 154,757 1,675
Drugs 28,896 30,193 (1,298)
Clinical Supplies 33,129 33,383 (254)
Misc. other expenditure 34,564 33,175 1,391
Depreciation 8,630 8,653 (23)
TOTAL EXPENDITURE 261,652 260,161 1,491
SURPLUS/ (DEFICIT) (12,079) (11,052) 1,027
Income
NHS clinical income is above budget, mainly due to increases in the level of out of area, non contracted activity. The Trusts main contractual income remains in line with the contracted level. Non NHS clinical income remains significantly below budget due to a material reduction in private patient activity, specifically within cardiology, cancer care and radiology. The Trust is developing plans to recover this position during 2016/17. Non patient related activity is marginally ahead of plan.
Further detail at contract level is set out below.
£’000 Budget Actual Variance
NHS Dorset CCG 153,116 153,116 0
NHS England (Wessex LAT) 42,278 42,348 70
NHS West Hampshire CCG 22,762 22,789 26
Non Contracted Activity 2,469 2,758 290
Public Health Bodies 2,409 2,442 33
NHS England (Other LATs) 1,546 1,509 (37)
NHS Wiltshire CCG 680 722 42
Other NHS Patient Income 531 712 181
Private Patient Income 4,069 2,748 (1,321)
Other Non NHS Patient Income 545 462 (83)
Non Patient Related Income 19,168 19,504 336
TOTAL INCOME 249,573 249,109 (464)
Expenditure
Pay reported an over spend in month, reflecting the operational pressures faced by the Trust during February. Despite this, the Trust continues to report a significant under spend due to agency expenditure being below expected levels. This is the result of considerable efforts in relation to both substantive and bank recruitment across the Trust, together with a number of more tactical workforce initiatives. The Trust continues to report additional drugs expenditure, resulting in a significant year to date over spend. In addition, clinical supplies expenditure is above budget to date, mainly due to a significant increase in non-elective cardiac activity, off-set in part by a reduction in the level of planned orthopaedic activity undertaken to date.
Finance Report As at 29 February 2016
Employee Expenses The Trust continues to rely heavily upon agency staff to cover substantive vacancies. The year to date under spend against substantive staffing budgets is £12.8 million. Agency expenditure to date totals £9.3 million, with a further £6.3 million spent on bank and overtime. This results in a total ‘premium’ workforce cost of £2.8 million to date.
£’000 Substantive Budget
Substantive Cost
Substantive Variance
Agency Cost
Bank Cost
Overtime Cost
Workforce Variance
Premium Funding
Residual Variance
Surgical Care Group 38,012 35,404 2,607 2,082 892 296 (663) 949 286
Medical Care Group 53,799 47,932 5,867 5,626 2,952 389 (3,100) 2,703 (397)
Specialties Care Group 33,124 30,851 2,273 1,109 665 100 399 240 639
Corporate Directorates 26,971 24,925 2,046 497 850 176 523 0 523
Centrally Managed Budgets 11 11 0 0 0 0 0 624 624
TOTAL 151,917 139,123 12,794 9,315 5,359 960 (2,840) 4,516 1,675
Where possible, block bookings are placed for agency staff to secure a reduced rate and provide consistency. Agency spend during February can be summarised as follows:
Block Booked Off-Framework Other
Nursing 109,691 51,637 158,510
Medical 0 21,375 322,517
The Trust welcomes the national support in reducing agency costs, and has pro-actively embraced the new governance measures. However, by exception the Trust has been required to engage staff above the capped rates to ensure services are delivered safely. This is subject to a rigorous executive approval process, and the exceptions recorded during February were as follows:
Medical Nursing Other
Shifts covered 133 81 128
Approximate Cost above Cap 45,743 16,075 12,137
The Trust recognises that the current level of premium workforce cost is unsustainable and is actively working to reduce this. As such, three key work streams have been established to support the management of the workforce in a clinically safe and appropriate manner. These cover medical job planning, premium cost avoidance, and strategic workforce management. Each work stream operates through a Transformational Steering Group chaired by the appropriate executive sponsor.

Finance Report As at 29 February 2016
Cost Improvement Programme The Trust has delivered financial savings amounting to £8.2 million to date, being £244,000 ahead of plan. The forecast is for total savings of £9.5 million against the full year target of £9 million. In month, the forecast has slipped overall, mainly due to a reduced forecast savings within Medical Records as part of the Electronic Document Management Project. This has been mitigated in part by improved savings forecasts within the Medical and Specialties Care Groups. Whilst further validation and challenge is taking place, currently £3.5 million continues to be reported as non recurrent. This remains a risk moving into the new financial year. The Surgical Care Group is forecasting full delivery of the full year target. Further validation of the non recurrent savings within this is taking place. The Medical Care Group position has remained broadly consistent, with a small £4,000 improvement within the ED and AMU forecast. The Specialties Care Group continues to forecast an over achievement against the full year target, with a further improvement during February. This is the result of additional drug savings. Corporate directorates continue to forecast full delivery against their targets. Some risks remain, and these are being followed up as appropriate.
DIRECTORATE TARGET ACTUAL VARIANCE TARGET ACTUAL VARIANCE
£'000 £'000 £'000 £'000 £'000 £'000
ANAESTHETICS AND THEATRES 124 0 (124) 164 164 0
MATERNITY 30 31 1 84 85 1
ORTHOPAEDICS 283 282 (2) 346 344 (2)
SURGERY 174 64 (110) 310 309 0
CARE GROUP A 611 377 (234) 903 902 (1)
CARDIOLOGY 221 153 (69) 254 174 (80)
ED AND AMU 66 16 (50) 76 17 (59)
OLDER PEOPLES MEDICINE 211 208 (2) 243 225 (18)
MEDICINE 250 509 259 251 558 307
CARE GROUP B 748 886 138 824 973 150
CANCER CARE 235 304 68 265 335 70
OPHTHALMOLOGY 233 182 (51) 258 199 (59)
PATHOLOGY 245 196 (49) 268 215 (54)
RADIOLOGY 116 188 72 131 219 88
SPECIALIST SERVICES 1,047 1,271 224 1,139 1,382 243
CARE GROUP C 1,877 2,140 264 2,061 2,350 289
NURSING, QUALITY & RISK 88 89 1 92 93 1
ESTATES 527 517 (10) 586 574 (12)
FACILITIES MANAGEMENT 296 272 (24) 354 316 (38)
FINANCE AND BUSINESS INTELLIGENCE 488 498 10 544 556 12
HR, TRAINING AND POST GRAD 173 173 0 185 185 0
INFORMATICS 682 778 96 777 824 47
OPERATIONAL SERVICES 113 113 0 122 121 (1)
OUTPATIENTS 16 12 (5) 19 14 (4)
TRUST BOARD & GOVERNORS 138 222 84 154 237 82
CORPORATE 2,521 2,673 153 2,832 2,920 87
PRODUCTIVITY 2,115 2,115 0 2,307 2,307 0
DIRECT ENGAGEMENT 77 0 (77) 115 0 (115)
CROSS DIRECTORATE 2,191 2,115 (77) 2,422 2,307 (115)
GRAND TOTAL 7,948 8,191 244 9,042 9,452 410
YEAR TO DATE FULL YEAR

Finance Report As at 29 February 2016
Care Group Performance The Trusts year to date net surplus/ (deficit) is shown by Care Group below.
£’000 Budget Actual Variance
Surgical Care Group 15,036 14,437 (599)
Medical Care Group 6,895 6,606 (289)
Specialties Care Group 5,198 4,955 (243)
Corporate Directorates (32,878) (32,302) 576
Centrally Managed Budgets (6,330) (4,748) 1,582
SURPLUS/ (DEFICIT) (12,079) (11,052) 1,027
Surgical Care Group
The Care Group reported an overall deficit in month of £124,000. This was driven by reduced elective orthopaedic income due to reduced capacity resulting from a significant increase in non-elective patients together with the impact of the junior doctors strike action. The Care Group expenditure position in month was broadly on plan, with a minor adverse variance of £6,000. The Care Group continues to forecast a balanced expenditure position overall.
Medical Care Group
The Medical Care group reported a favourable variance to budget during February of £52,000. Income reported a favourable variance of £273,000 in month reflecting the scale of additional non-elective activity reported during February, together with a planned increase in endoscopy activity.
This was off-set in part by a continued adverse variance in relation to private Cardiology activity. The volume of additional activity during February placed significant pressure on expenditure budgets, which reported an aggregate over spend of £221,000.
Specialties Care Group
Overall the Care Group reported an adverse variance in month of £76,000. This was the result of an under achievement against the income budgets together with a marginal expenditure over spend. Specific pressures were reported within Cancer Care in relation to staffing pressures and increased drug costs; and Ophthalmology to ensure continued compliance with national access standards.
Corporate Directorates
Whilst some pressures remain within a small number of directorates, overall the corporate areas continue to perform well financially, delivering a significant favourable variance to date.
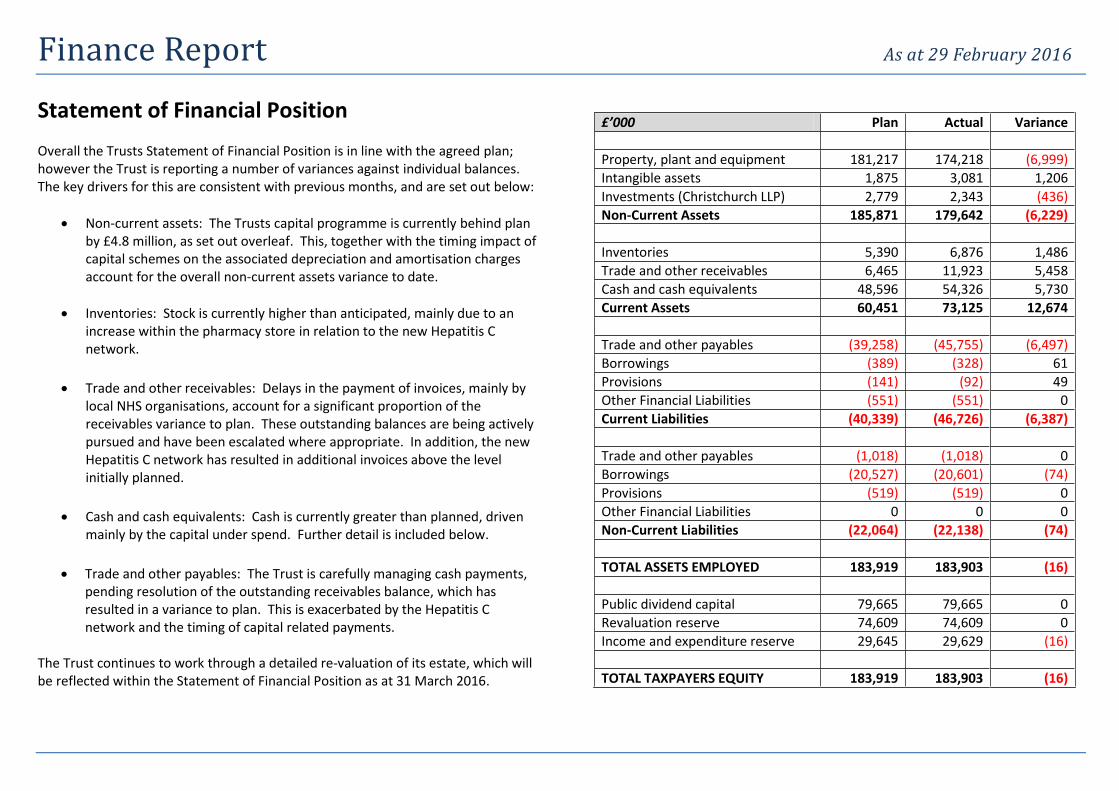
Finance Report As at 29 February 2016
Statement of Financial Position Overall the Trusts Statement of Financial Position is in line with the agreed plan; however the Trust is reporting a number of variances against individual balances. The key drivers for this are consistent with previous months, and are set out below:
Non-current assets: The Trusts capital programme is currently behind plan by £4.8 million, as set out overleaf. This, together with the timing impact of capital schemes on the associated depreciation and amortisation charges account for the overall non-current assets variance to date.
Inventories: Stock is currently higher than anticipated, mainly due to an increase within the pharmacy store in relation to the new Hepatitis C network.
Trade and other receivables: Delays in the payment of invoices, mainly by local NHS organisations, account for a significant proportion of the receivables variance to plan. These outstanding balances are being actively pursued and have been escalated where appropriate. In addition, the new Hepatitis C network has resulted in additional invoices above the level initially planned.
Cash and cash equivalents: Cash is currently greater than planned, driven mainly by the capital under spend. Further detail is included below.
Trade and other payables: The Trust is carefully managing cash payments, pending resolution of the outstanding receivables balance, which has resulted in a variance to plan. This is exacerbated by the Hepatitis C network and the timing of capital related payments.
The Trust continues to work through a detailed re-valuation of its estate, which will be reflected within the Statement of Financial Position as at 31 March 2016.
£’000 Plan Actual Variance
Property, plant and equipment 181,217 174,218 (6,999)
Intangible assets 1,875 3,081 1,206
Investments (Christchurch LLP) 2,779 2,343 (436)
Non-Current Assets 185,871 179,642 (6,229)
Inventories 5,390 6,876 1,486
Trade and other receivables 6,465 11,923 5,458
Cash and cash equivalents 48,596 54,326 5,730
Current Assets 60,451 73,125 12,674
Trade and other payables (39,258) (45,755) (6,497)
Borrowings (389) (328) 61
Provisions (141) (92) 49
Other Financial Liabilities (551) (551) 0
Current Liabilities (40,339) (46,726) (6,387)
Trade and other payables (1,018) (1,018) 0
Borrowings (20,527) (20,601) (74)
Provisions (519) (519) 0
Other Financial Liabilities 0 0 0
Non-Current Liabilities (22,064) (22,138) (74)
TOTAL ASSETS EMPLOYED 183,919 183,903 (16)
Public dividend capital 79,665 79,665 0
Revaluation reserve 74,609 74,609 0
Income and expenditure reserve 29,645 29,629 (16)
TOTAL TAXPAYERS EQUITY 183,919 183,903 (16)
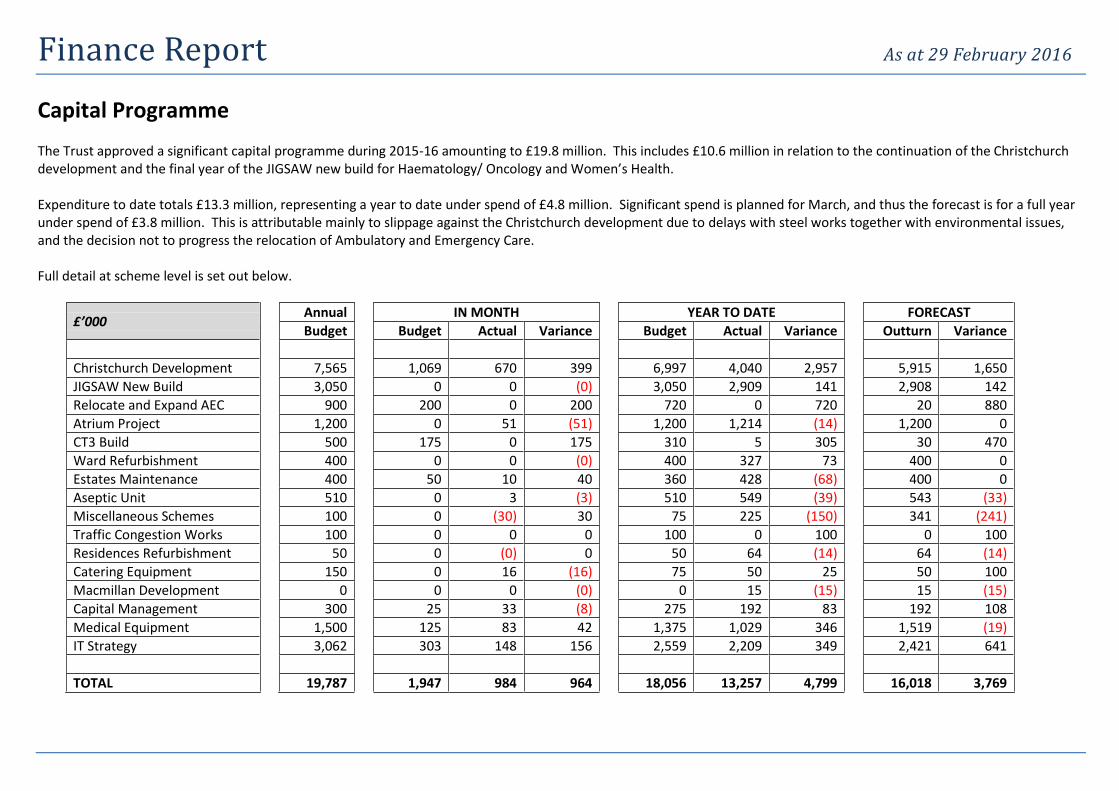
Finance Report As at 29 February 2016
Capital Programme The Trust approved a significant capital programme during 2015-16 amounting to £19.8 million. This includes £10.6 million in relation to the continuation of the Christchurch development and the final year of the JIGSAW new build for Haematology/ Oncology and Women’s Health. Expenditure to date totals £13.3 million, representing a year to date under spend of £4.8 million. Significant spend is planned for March, and thus the forecast is for a full year under spend of £3.8 million. This is attributable mainly to slippage against the Christchurch development due to delays with steel works together with environmental issues, and the decision not to progress the relocation of Ambulatory and Emergency Care. Full detail at scheme level is set out below.
£’000 Annual IN MONTH YEAR TO DATE FORECAST
Budget Budget Actual Variance Budget Actual Variance Outturn Variance
Christchurch Development 7,565 1,069 670 399 6,997 4,040 2,957 5,915 1,650
JIGSAW New Build 3,050 0 0 (0) 3,050 2,909 141 2,908 142
Relocate and Expand AEC 900 200 0 200 720 0 720 20 880
Atrium Project 1,200 0 51 (51) 1,200 1,214 (14) 1,200 0
CT3 Build 500 175 0 175 310 5 305 30 470
Ward Refurbishment 400 0 0 (0) 400 327 73 400 0
Estates Maintenance 400 50 10 40 360 428 (68) 400 0
Aseptic Unit 510 0 3 (3) 510 549 (39) 543 (33)
Miscellaneous Schemes 100 0 (30) 30 75 225 (150) 341 (241)
Traffic Congestion Works 100 0 0 0 100 0 100 0 100
Residences Refurbishment 50 0 (0) 0 50 64 (14) 64 (14)
Catering Equipment 150 0 16 (16) 75 50 25 50 100
Macmillan Development 0 0 0 (0) 0 15 (15) 15 (15)
Capital Management 300 25 33 (8) 275 192 83 192 108
Medical Equipment 1,500 125 83 42 1,375 1,029 346 1,519 (19)
IT Strategy 3,062 303 148 156 2,559 2,209 349 2,421 641
TOTAL 19,787 1,947 984 964 18,056 13,257 4,799 16,018 3,769

Finance Report As at 29 February 2016
Cash
The Trust is currently holding £54.3 million in cash reserves. However, there are two significant cash timing benefits within this figure meaning that the underlying cash position is significantly lower at £30.4 million. The first relates to the delays in the Christchurch development, which has resulted in a cash timing benefit when compared to the agreed phasing of the ITFF loan drawdown. The second relates to the contract payment schedule agreed with Dorset Clinical Commissioning Group for the year, as set against the activity and associated expenditure profile for the year. The forecast closing cash balance for the current financial year is £33.3 million. After adjusting for the residual cash timing benefits, the Trust is forecasting to end the year with £26.9 million of cash. The summarised cash forecast for the remainder of the current financial year is shown below.
Financial Sustainability Risk Rating
Monitor’s revised Risk Assessment Framework came into effect from 1 August 2015. This included a change from the previous Continuity of Services Risk Rating to the new Financial Sustainability Risk Rating. The Trusts Financial Sustainability Risk Rating as at 29 February 2016 is set out below.
Plan Metric
Actual Metric
Risk Rating
Weighted Rating
Capital Service Cover 0.24x 0.35x 1 0.25
Liquidity 19.7 28.7 4 1.00
I&E Margin (4.45) (4.88) 1 0.25
I&E Variance to Plan (1.17)% (0.43)% 3 0.75
Trust FSRR 2
Mandatory Override Yes
Final FSRR 2
This rating (after the application of mandatory overrides) of 2 places the Trust in the ‘Material Risk’ and ‘Potential Investigation’ category. Monitor’s investigation has been completed, and the Trust is awaiting final confirmation of the outcome. This is expected imminently. The Trusts draft operational plan for 2016/17 has been formally submitted to Monitor, and the medium term financial forecast has been shared as part of the investigation process. Whilst a number of key assumptions and risks remain within this plan, the Trust is forecasting a Financial Sustainability Risk Rating of 3 from August 2016. This annual plan and medium term forecast will continue to be updated as the Trust continues through the 2016/17 planning cycle.
£ million Mar-16
OPENING CASH 54.33
NHS Clinical Income 19.77
Non NHS Clinical Income 0.89
Non Patient Related Income 1.46
Working Capital (14.03)
CASH INFLOWS 8.09
Revenue Account (23.95)
Capital Account (1.50)
Christchurch Investment (0.55)
ITFF Loan Repayment (0.54)
Working Capital (2.55)
CASH OUTFLOWS (29.09)
CLOSING CASH 33.33

COUNCIL OF GOVERNORS Meeting Date and Part:
13th April 2016 – Part 1
Subject: Workforce Report
Section: Performance
Author of Paper: Karen Allman
Details of previous discussion and/or dissemination:
Workforce Committee and Board of Directors
Key Purpose:
Patient Engagement Governance Performance Strategy
X
Action Required by Council of Governors:
For Noting.
Summary:
The report shows Trust-wide figures for a range of workforce metrics and includes details of the results of the 2015 Staff Survey
Strategic Goals & Objectives: To listen to, support, motivate and develop our staff
Links to CQC Registration: (Outcome reference)
Outcomes 12, 13 & 14 - Staffing
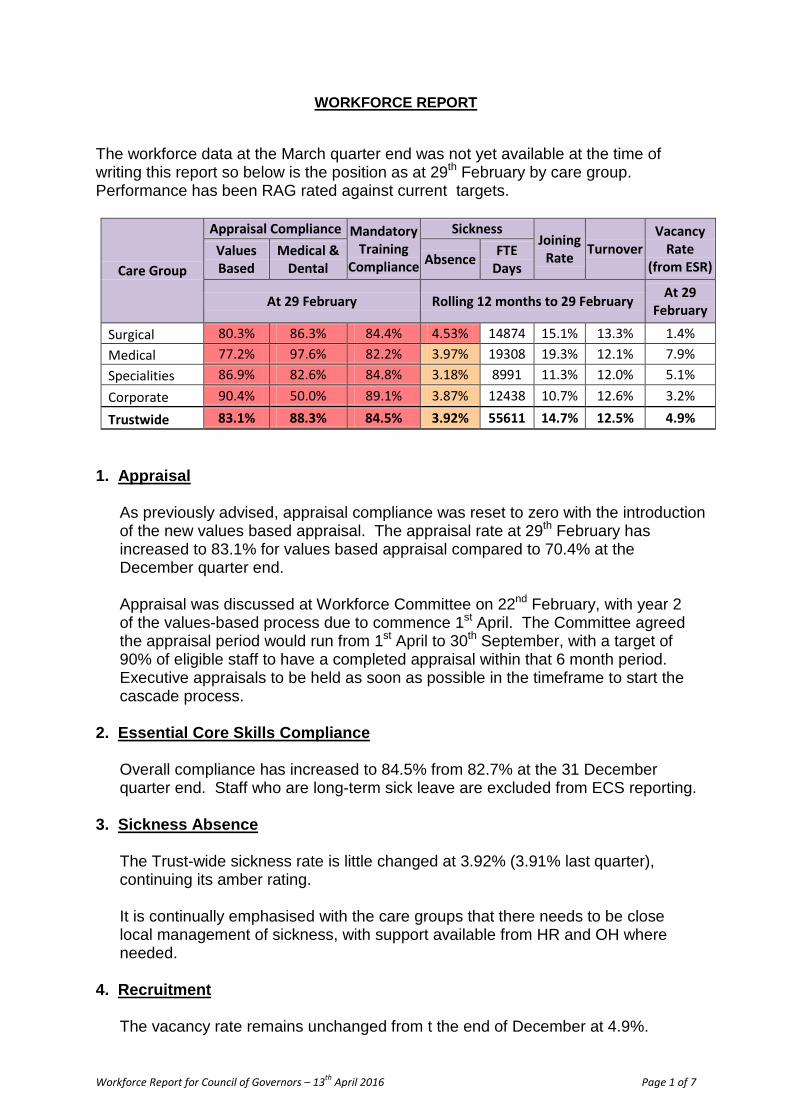
WORKFORCE REPORT The workforce data at the March quarter end was not yet available at the time of writing this report so below is the position as at 29th February by care group. Performance has been RAG rated against current targets.
Care Group
Appraisal Compliance Mandatory Training
Compliance
Sickness Joining
Rate Turnover Vacancy
Rate (from ESR)
Values Based
Medical & Dental Absence FTE
Days
At 29 February Rolling 12 months to 29 February At 29 February
Surgical 80.3% 86.3% 84.4% 4.53% 14874 15.1% 13.3% 1.4% Medical 77.2% 97.6% 82.2% 3.97% 19308 19.3% 12.1% 7.9% Specialities 86.9% 82.6% 84.8% 3.18% 8991 11.3% 12.0% 5.1% Corporate 90.4% 50.0% 89.1% 3.87% 12438 10.7% 12.6% 3.2%
Trustwide 83.1% 88.3% 84.5% 3.92% 55611 14.7% 12.5% 4.9% 1. Appraisal As previously advised, appraisal compliance was reset to zero with the introduction
of the new values based appraisal. The appraisal rate at 29th February has increased to 83.1% for values based appraisal compared to 70.4% at the December quarter end.
Appraisal was discussed at Workforce Committee on 22nd February, with year 2
of the values-based process due to commence 1st April. The Committee agreed the appraisal period would run from 1st April to 30th September, with a target of 90% of eligible staff to have a completed appraisal within that 6 month period. Executive appraisals to be held as soon as possible in the timeframe to start the cascade process.
2. Essential Core Skills Compliance
Overall compliance has increased to 84.5% from 82.7% at the 31 December quarter end. Staff who are long-term sick leave are excluded from ECS reporting.
3. Sickness Absence
The Trust-wide sickness rate is little changed at 3.92% (3.91% last quarter), continuing its amber rating.
It is continually emphasised with the care groups that there needs to be close
local management of sickness, with support available from HR and OH where needed.
4. Recruitment
The vacancy rate remains unchanged from t the end of December at 4.9%.
Workforce Report for Council of Governors – 13th April 2016 Page 1 of 7
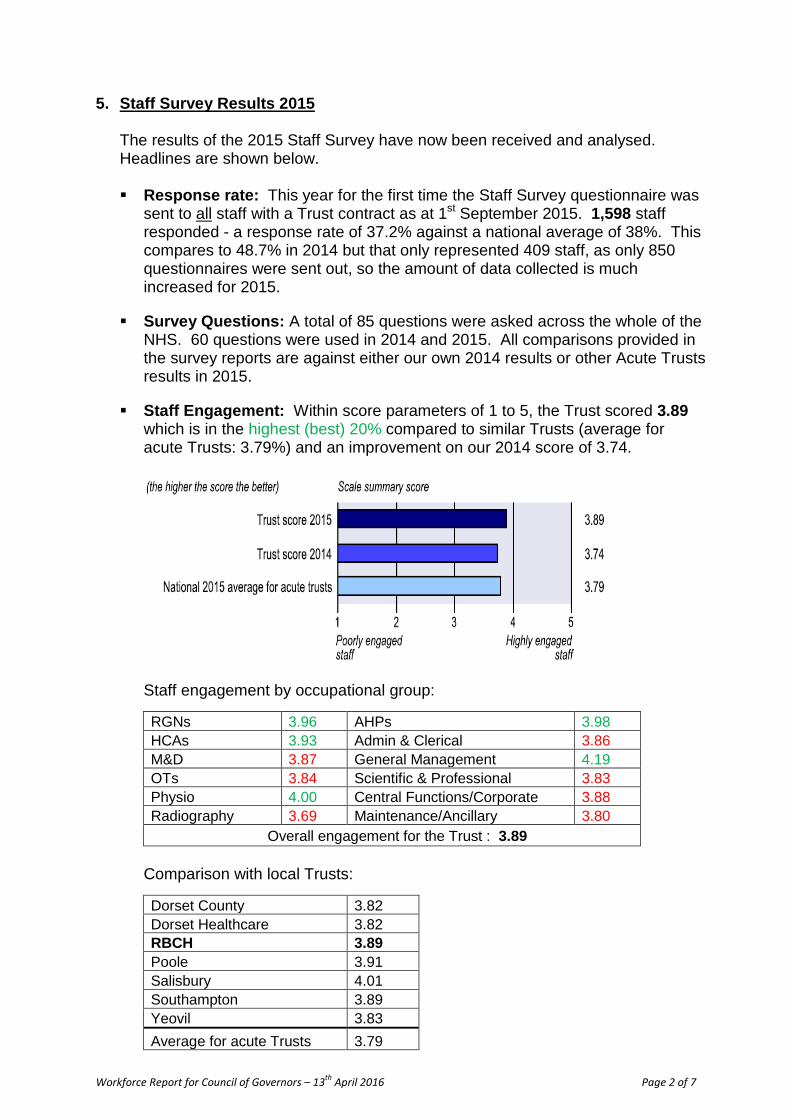
5. Staff Survey Results 2015 The results of the 2015 Staff Survey have now been received and analysed.
Headlines are shown below. Response rate: This year for the first time the Staff Survey questionnaire was
sent to all staff with a Trust contract as at 1st September 2015. 1,598 staff responded - a response rate of 37.2% against a national average of 38%. This compares to 48.7% in 2014 but that only represented 409 staff, as only 850 questionnaires were sent out, so the amount of data collected is much increased for 2015.
Survey Questions: A total of 85 questions were asked across the whole of the NHS. 60 questions were used in 2014 and 2015. All comparisons provided in the survey reports are against either our own 2014 results or other Acute Trusts results in 2015.
Staff Engagement: Within score parameters of 1 to 5, the Trust scored 3.89 which is in the highest (best) 20% compared to similar Trusts (average for acute Trusts: 3.79%) and an improvement on our 2014 score of 3.74.
Staff engagement by occupational group:
RGNs 3.96 AHPs 3.98 HCAs 3.93 Admin & Clerical 3.86 M&D 3.87 General Management 4.19 OTs 3.84 Scientific & Professional 3.83 Physio 4.00 Central Functions/Corporate 3.88 Radiography 3.69 Maintenance/Ancillary 3.80
Overall engagement for the Trust : 3.89 Comparison with local Trusts:
Dorset County 3.82 Dorset Healthcare 3.82 RBCH 3.89 Poole 3.91 Salisbury 4.01 Southampton 3.89 Yeovil 3.83 Average for acute Trusts 3.79
Workforce Report for Council of Governors – 13th April 2016 Page 2 of 7

RBCH top strengths compared to other Trusts:
RBCH top weaknesses compared to other Trusts:
Most improved (compared to other Trusts):
Workforce Report for Council of Governors – 13th April 2016 Page 3 of 7

Staff Pledges: The staff pledges were taken from the NHS constitution and first published in 2009: ~ To provide all staff with clear roles, responsibilities and rewarding jobs. ~ To provide all staff with personal development, access to appropriate
education and training for their jobs and line management support to enable them to fulfil their potential.
~ To provide support and opportunities for staff to maintain their health, wellbeing and safety.
~ To engage staff in decisions that affect them, the services they provide and empower them to put forward ways to deliver better and safer service.
Within the above pledges there are 32 key factors, of which the Trust scored in the best 20% (when compared to other Acute Trusts) for 23 key factors, average for 5 and worse than other Trusts for 4. Improvements were made in 8 key factors since 2014.
Results at a glance: Historical Trust comparisons:
Bullying & Harassment:
2013 2014 2015 Service Users 30% 31% 25% Managers 28% 25% 13% Colleagues 28% 25% 20% B&H not reported 54% 49% 61%
Significant improvements over last year: The Trust made significant
improvements in 20 measures: 2014 2015 Never/rarely look forward to going to work 15% 9% Never/rarely enthusiastic about my job 8% 4% Not able to do my job to a standard I am pleased with 11% 7% Opportunities to show initiative infrequent in my role 12% 8% Dissatisfied with recognition for good work 26% 20% Dissatisfied with support from colleagues 7% 4% Dissatisfied with extent organisation values my work 29% 23% Dissatisfied with quality of care I give 8% 4% Do not feel my role makes a difference to patients/service users 3% 1% Unable to provide the care I aspire to 14% 9%
Continued ……
Workforce Report for Council of Governors – 13th April 2016 Page 4 of 7
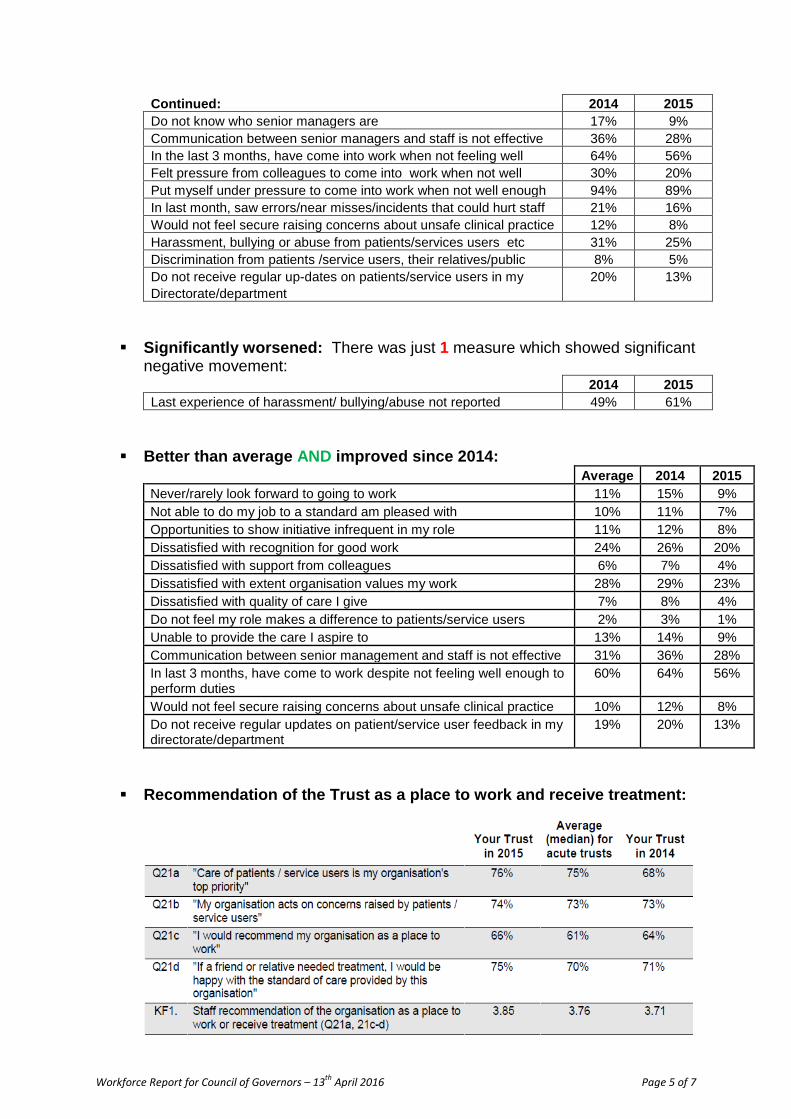
Continued: 2014 2015 Do not know who senior managers are 17% 9% Communication between senior managers and staff is not effective 36% 28% In the last 3 months, have come into work when not feeling well 64% 56% Felt pressure from colleagues to come into work when not well 30% 20% Put myself under pressure to come into work when not well enough 94% 89% In last month, saw errors/near misses/incidents that could hurt staff 21% 16% Would not feel secure raising concerns about unsafe clinical practice 12% 8% Harassment, bullying or abuse from patients/services users etc 31% 25% Discrimination from patients /service users, their relatives/public 8% 5% Do not receive regular up-dates on patients/service users in my Directorate/department
20% 13%
Significantly worsened: There was just 1 measure which showed significant
negative movement: 2014 2015 Last experience of harassment/ bullying/abuse not reported 49% 61%
Better than average AND improved since 2014:
Average 2014 2015 Never/rarely look forward to going to work 11% 15% 9% Not able to do my job to a standard am pleased with 10% 11% 7% Opportunities to show initiative infrequent in my role 11% 12% 8% Dissatisfied with recognition for good work 24% 26% 20% Dissatisfied with support from colleagues 6% 7% 4% Dissatisfied with extent organisation values my work 28% 29% 23% Dissatisfied with quality of care I give 7% 8% 4% Do not feel my role makes a difference to patients/service users 2% 3% 1% Unable to provide the care I aspire to 13% 14% 9% Communication between senior management and staff is not effective 31% 36% 28% In last 3 months, have come to work despite not feeling well enough to perform duties
60% 64% 56%
Would not feel secure raising concerns about unsafe clinical practice 10% 12% 8% Do not receive regular updates on patient/service user feedback in my directorate/department
19% 20% 13%
Recommendation of the Trust as a place to work and receive treatment:
Workforce Report for Council of Governors – 13th April 2016 Page 5 of 7

Staff recommendation of the organisation as a place to work or receive treatment by Occupational group:
RGNs 3.83 AHPs 3.90 HCAs 4.00 Admin & Clerical 3.94 M&D 3.81 General Management 3.80 OTs 3.57 Scientific & Professional 3.84 Physio 3.86 Central Functions/Corporate 3.74 Radiography 3.87 Maintenance/Ancillary 3.93
Overall Trust score 2015: 3.85 Overall Trust score 2014: 3.71 Average Acute Trusts 2015: 3.76
Comparison with local Trusts:
All Trusts
Dorset County
Dorset Healthcare
RBCH Poole Salisbury Yeovil
Key finding 1 (21a,21c,d)
Staff recommendation of the organisation as a place to work or receive treatment
3.72 3.81 3.67 3.85 3.93 4.09 3.74
Key Finding 2 (3c,6a,6c)
Staff satisfaction with the quality of work and care they are able to deliver
3.91 3.84 3.81 4.04 3.86 3.91 3.89
Key Finding 5 (5a,5f,7f)
Recognition and value of staff by managers and the organisation
3.44 3.46 3.53 3.52 3.53 3.61 3.57
Key Finding 7 (4a.b.d)
Percentage of staff able to contribute towards improvements at work
70% 70% 76% 73% 77% 78% 72%
Key Finding 9 (4h-j)
Key Finding 9. Effective team working
3.76 3.74 3.91 3.84 3.81 3.87 3.86
Key Finding 17 (9c)
Percentage of staff suffering work related stress in last 12 months
37% 33% 37% 32% 36% 29% 32%
Key Finding 26 (15b,c)
Percentage of staff experiencing harassment, bullying or abuse from staff in last 12 months
24% 26% 22% 26% 24% 23% 19%
Key priorities for improvement:
~ Monitoring of staff appraisal target and action taken if target not achieved. ~ Monitoring of mandatory training to ensure all staff are given an opportunity to
complete. ~ Encourage reporting of harassment, bullying and abuse and take action - team
meetings, focus groups, change champions. ~ Robustly address incidents of physical violence against staff by service users.
Workforce Report for Council of Governors – 13th April 2016 Page 6 of 7

Next steps: ~ Communication of results to managers and staff. ~ Results by Directorate and/or cost centre available to managers for action
planning in discussion with staff. ~ Results are communicated to staff and discussed at team meetings. ~ Care Group/Directorate action plans reported to Workforce Committee and at
Care Group reviews. ~ Results incorporated into OD and Change Champions work. ~ Quarter 4 Friends and Family Test, exploring areas of concern from national
survey. ~ Celebrate outstanding good scores within departments/directorates. ~ On-going monitoring and regular reporting of progress.
Workforce Report for Council of Governors – 13th April 2016 Page 7 of 7

COUNCIL OF GOVERNORS
Meeting Date and Part:
13 April 2016 – Part 1
Subject: Recommendations to amend the Trust Constitution April 2016
Section: Governance
Author of Paper: Sarah Anderson
Details of previous discussion and/or dissemination:
Constitution Joint Working Group (CJWG)
Key Purpose:
Patient Engagement Governance Performance Strategy
X
Action Required by Council of Governors:
For Decision
NB. The Board of Directors are also required to approve the amendments to the Constitution. This will occur on 29 April 2016.
Summary:
The report outlines the amendments agreed by the CJWG and the rationale for the revisions. The Council of Governors is asked to approve the recommendations presented by the CJWG.
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016
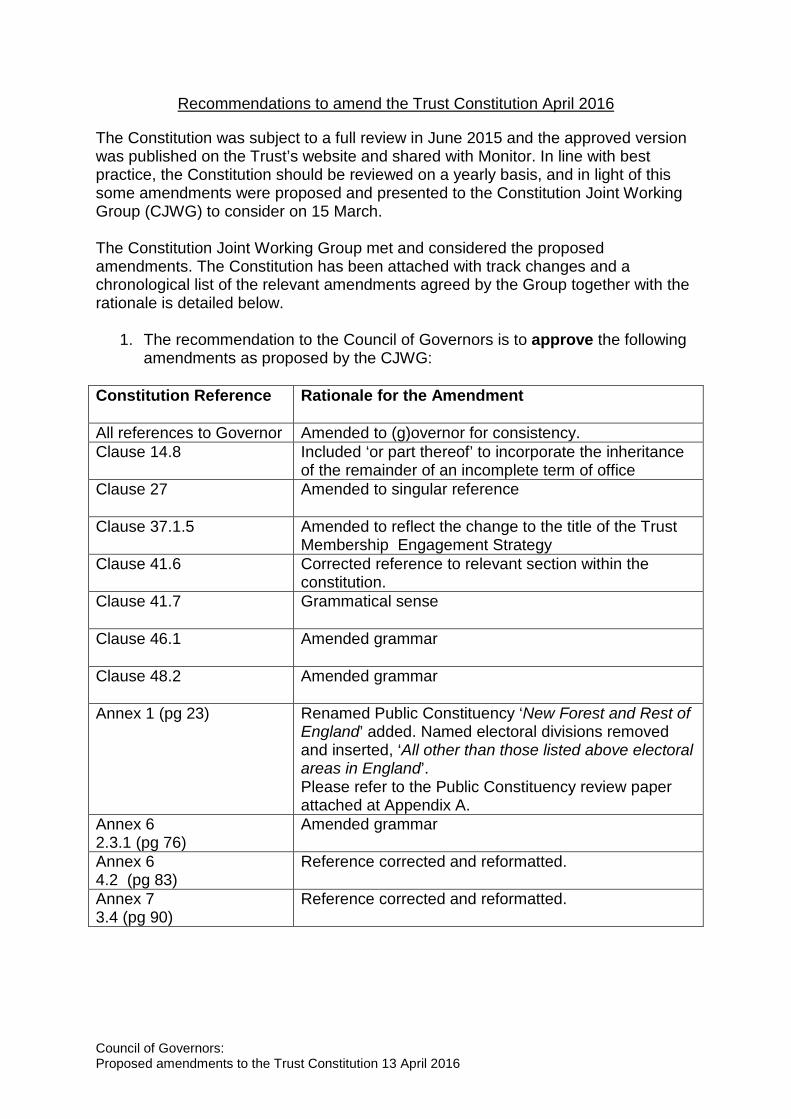
Recommendations to amend the Trust Constitution April 2016
The Constitution was subject to a full review in June 2015 and the approved version was published on the Trust’s website and shared with Monitor. In line with best practice, the Constitution should be reviewed on a yearly basis, and in light of this some amendments were proposed and presented to the Constitution Joint Working Group (CJWG) to consider on 15 March. The Constitution Joint Working Group met and considered the proposed amendments. The Constitution has been attached with track changes and a chronological list of the relevant amendments agreed by the Group together with the rationale is detailed below.
1. The recommendation to the Council of Governors is to approve the following amendments as proposed by the CJWG:
Constitution Reference Rationale for the Amendment
All references to Governor Amended to (g)overnor for consistency. Clause 14.8 Included ‘or part thereof’ to incorporate the inheritance
of the remainder of an incomplete term of office Clause 27
Amended to singular reference
Clause 37.1.5 Amended to reflect the change to the title of the Trust Membership Engagement Strategy
Clause 41.6
Corrected reference to relevant section within the constitution.
Clause 41.7
Grammatical sense
Clause 46.1
Amended grammar
Clause 48.2
Amended grammar
Annex 1 (pg 23) Renamed Public Constituency ‘New Forest and Rest of England’ added. Named electoral divisions removed and inserted, ‘All other than those listed above electoral areas in England’. Please refer to the Public Constituency review paper attached at Appendix A.
Annex 6 2.3.1 (pg 76)
Amended grammar
Annex 6 4.2 (pg 83)
Reference corrected and reformatted.
Annex 7 3.4 (pg 90)
Reference corrected and reformatted.
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016

2. The Constitution Joint Working Group requested that the following amendments were reviewed in further detail and the revised amendments presented to the Council of Governors for approval:
Constitution Reference
Rationale/ Themes considered
Revised Amendment
Page 6 Significant Transactions
• The definition should incorporate the Monitor definition but should be wider for the Trust.
• That the Trust would not strictly adhere to the definition as this was too broad in monetary terms and as such very few, if any, transactions would require CoG approval.
• The Trust wishes to bring issues less than the Monitor definition to the attention of the CoG.
• Poole Hospital’s definition was considered however is believed to be incorrect and therefore was not incorporated into the amendments.
Definition from the current Risk Assessment Framework ('rule book' for compliance with the Trust’s licence). “A major change in the Trust’s service provision or configuration which would impact on patients, the finances or reputation of the Trust. Although the Trust does not use it, Monitor defines a significant transaction as being 10% of the value of assets, income or capital.”
Clause 45.2 As above. The Constitution does not define significant transaction for the purposes of section 51A of the 2006 Act (Significant Transactions), although it notes that the Monitor definition is 10% of assets, income or capital. The Trust feels that the application of this definition would mean that the Council of Governors would very rarely be consulted on a significant transaction. By not defining significant transactions the Trust is able to ensure appropriate consultation and agreement of key
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016
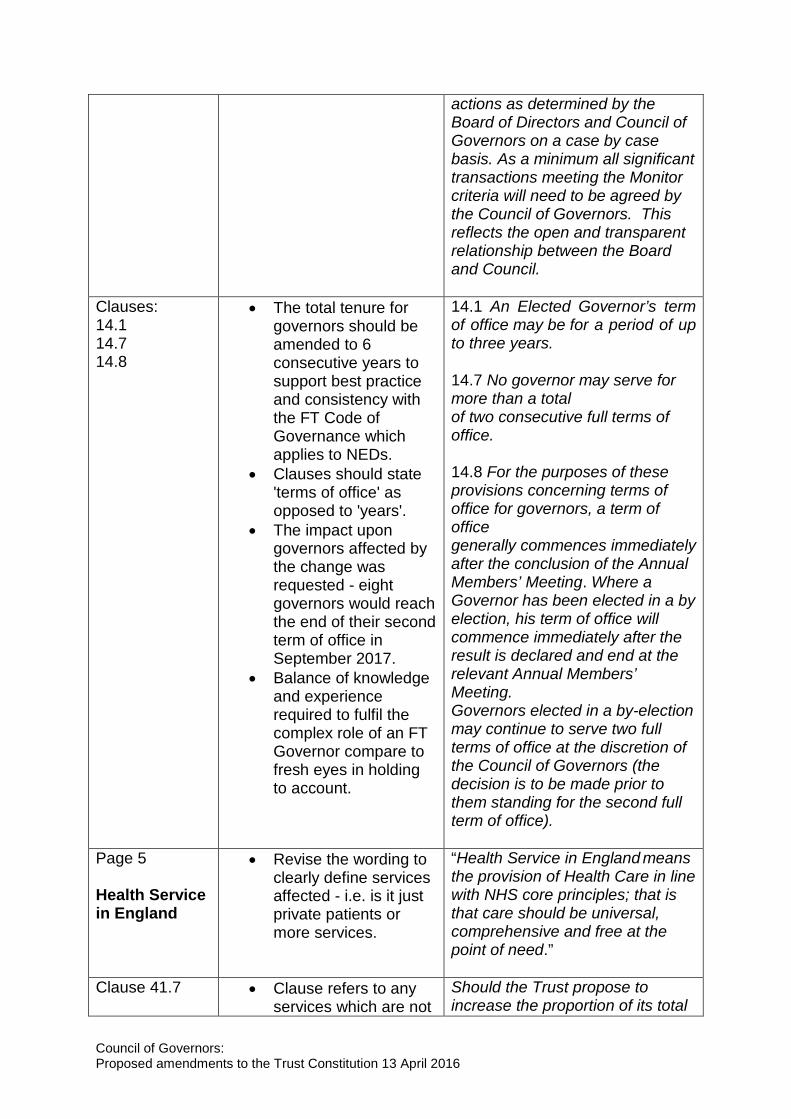
actions as determined by the Board of Directors and Council of Governors on a case by case basis. As a minimum all significant transactions meeting the Monitor criteria will need to be agreed by the Council of Governors. This reflects the open and transparent relationship between the Board and Council.
Clauses: 14.1 14.7 14.8
• The total tenure for governors should be amended to 6 consecutive years to support best practice and consistency with the FT Code of Governance which applies to NEDs.
• Clauses should state 'terms of office' as opposed to 'years'.
• The impact upon governors affected by the change was requested - eight governors would reach the end of their second term of office in September 2017.
• Balance of knowledge and experience required to fulfil the complex role of an FT Governor compare to fresh eyes in holding to account.
14.1 An Elected Governor’s term of office may be for a period of up to three years.
14.7 No governor may serve for more than a total of two consecutive full terms of office. 14.8 For the purposes of these provisions concerning terms of office for governors, a term of office generally commences immediately after the conclusion of the Annual Members’ Meeting. Where a Governor has been elected in a by election, his term of office will commence immediately after the result is declared and end at the relevant Annual Members’ Meeting. Governors elected in a by-election may continue to serve two full terms of office at the discretion of the Council of Governors (the decision is to be made prior to them standing for the second full term of office).
Page 5 Health Service in England
• Revise the wording to clearly define services affected - i.e. is it just private patients or more services.
“Health Service in England means the provision of Health Care in line with NHS core principles; that is that care should be universal, comprehensive and free at the point of need.”
Clause 41.7 • Clause refers to any services which are not
Should the Trust propose to increase the proportion of its total
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016
for the purposes of NHS health care - which may include laundry service to a private nursing home, visitor car parking, for example.
• To include a worked example of the definition.
income by 5% or more in any Financial Year that is attributable to activities other than the provision of goods and services for the purposes of the health service in England, it will require more than half of the members of the Council of Governors voting to approve its implementation e.g. if the total income is £100, £1 is Private Patient income, a change to move to £6 Private Patient income would trigger a vote, but a move to £4 would not.
The recommendations approved by the Council of Governors will be presented to the Board of Directors at the meeting on 29 April in order that a new and up to date version of the constitution can be uploaded to the website and shared with Monitor soon after.
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016
Appendix A
Review of Public Constituencies
1. Introduction
The expansion of public constituencies was recently raised by the governor led Non-Executive Directors (NED) Nomination and Remuneration Committee in consideration of future Board succession planning. It was requested that the proposal was submitted to the Council of Governors for further debate.
2. Background
There are currently three (3) public constituencies: Christchurch and Dorset County, Bournemouth and Poole, and New Forest, Hampshire and Salisbury. The Trust’s services are often used by members of public from a wider catchment area and in previous years the Council of Governors has expanded its constituency groups to incorporate surrounding areas and reflect the origin of footfall in the hospital. Preceding the current constituencies there were five groups which incorporated areas such as Salisbury, the Isle of Wight and the Rest of Hampshire and Dorset.
3. Key Points
Non- Executive Director Recruitment-
The Council of Governors is responsible for appointing the Non-Executive Directors (NEDs) including the Chairperson. This is remitted to the NED Nomination and Remuneration Committee to provide a recommendation on appointments to the Council of Governors for approval.
It is a requirement of the Trust’s Constitution that, in order to be considered for the role of Non- Executive Director, a candidate must be a member of the Trust. Therefore, to be eligible for appointment, candidates must live in one of the public constituencies. This can often be restrictive as the pool from which Non- Executive Directors can be recruited from, is fairly small. As such many Trusts address this issue by including a ‘Rest of England’ category.
Furthermore, the structure of the NHS is currently being reviewed across Dorset through the Clinical Services Review and the Vanguard project. As a result, some services will be delivered under a different model within the next three years. The Trust is also under investigation for potential breaches of its license for performance and finance.
It is apparent that a number of appointment periods for Non-Executive Directors will expire in 2016/17 and in light of these factors, together with the general uncertainty nationally; it may prove difficult to recruit Non-Executive Directors of a suitable caliber from the small pool available in the current constituency areas.
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016

Therefore by increasing the catchment area with a broader public constituency it may provide greater flexibility for recruitment and support Board Succession planning.
it should be noted that a potential ‘Rest of England’ category may have an impact upon Non-Executive Director’s expenses, as individuals travelling from outside of the county will incur greater travel costs. A limit could be considered in this respect.
Footfall of Patients-
The annual footfall of inpatients and outpatients patients (excluding Emergency Department (ED) attendances) by electoral ward is outlined below:
• NHS Dorset CCG - 112,573 • NHS West Hampshire CCG - 15,179 • NHS Wiltshire CCG - 387 (Salisbury boundary) • NHS Southampton CCG - 122
Annual footfall of inpatients and outpatients from outside of the existing constituency boundaries:
• NHS West Hampshire CCG - 84 • NHS Wiltshire CCG - 308 • NHS Southampton CCG - 4 • NHS Somerset CCG - 108 • NHS Coastal West Sussex CCG - 49 • NHS Northern, Eastern and Western Devon CCG - 54 • Wales - 56 • NHS England - 1,532 • Outside of NHS England - 2871
It is evident from the data that 2,482 (approximately 2% of our total patient base) patients, from outside of the current public constituencies, utilised Trust services over the past year.
The breakdown of the current membership by public constituency is as follows:
• Bournemouth and Poole - 8,404 • Christchurch and Dorset County - 2,035 • New Forest, Hampshire and Salisbury - 771
1 For example from Scotland, Europe, America, Asia.
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016

A ‘Rest of England’ constituency
It is fairly common practice amongst other Trusts to include a ‘Rest of England’ constituency as many services are used by members of the public from a wider catchment area. This would ensure that the Trust membership is reflective of service users. Examples of Trust’s that have included a constituency like this include Poole Hospital, Salisbury Hospital, University Hospital Southampton, Dorset Healthcare, Southern Health, Musgrove Park Hospital and Hampshire Hospitals.
In previous years the fifth constituency covering Hampshire, Wiltshire and Dorset, was removed due to a lack of interest from public members and no election to the governor vacancy.
Should the Council of Governors decide that an additional public constituency is appropriate this would require additional elected governor representation; this will increase costs for the Trust in terms of both the election process and possible travel expenses.
Alternatively one of the current public constituencies’ borders could be extended to include the ‘Rest of England’ such as the ‘New Forest and Rest of England’, which would not require additional governor representation. This could therefore potentially increase the catchment area for NED recruitment and membership.
It should be noted that governors will not be required to travel further afield to promote the Trust but to continue to improve public and patient engagement within their constituencies in the immediate area of the Trust.
4. Action Required
The Council of Governors is asked to discuss and consider the proposal outlined below in light of the information presented within the paper: 1. Consider extending the boundaries of the current public constituency of ‘New
Forest, Hampshire and Salisbury’ constituency to incorporate the ‘Rest of England’ and to rename the constituency as. ‘New Forest and Rest of England’. This will reflect the footfall of service users who come from outside of the current membership area.
Council of Governors: Proposed amendments to the Trust Constitution 13 April 2016

CONSTITUTION
THE ROYAL BOURNEMOUTH AND CHRISTCHURCH HOSPITALS NHS FOUNDATION TRUST
Approval Process Version Issue Date Review Date Document Author(s) Council of Governors; Board of Directors
V2 July 2015
July 2016 Trust Secretary
Constitution Page 1 of 107
CONTENTS
1. Interpretation and Definitions ......................................................................................4 2. Name ..........................................................................................................................6 3. Principal Purpose ........................................................................................................6 4. Powers ........................................................................................................................7 5. Membership and Constituencies .................................................................................7 6. Application for Membership .........................................................................................7 7. Public Constituency .....................................................................................................7 8. Staff Constituency .......................................................................................................7 9. Automatic Membership by Default – Staff ...................................................................8 10. Restriction on Membership .........................................................................................8 11. Annual Members' Meeting ...........................................................................................9 12. Council of Governors – Composition ...........................................................................9 13. Council of Governors – Election ..................................................................................9 14. Council of Governors - Tenure ....................................................................................9 15. Council of Governors – Disqualification and Removal .............................................. 10 16. Council of Governors – Duties .................................................................................. 11 17. Council of Governors – Meetings .............................................................................. 11 18. Council of Governors – Standing Orders .................................................................. 11 19. Council of Governors – Referral to the Panel ............................................................ 11 20. Council of Governors - Conflicts of Interest ............................................................... 12 21. Council of Governors – Travel Expenses .................................................................. 12 22. Council of Governors – further provisions ................................................................. 12 23. Board of Directors – Composition ............................................................................. 12 24. Board of Directors – General Duty ............................................................................ 13 25. Board of Directors – Qualification for Appointment as a Non-Executive Director ...... 13 26. Board of Directors – Appointment and Removal of Chairperson and Other Non-
Executive Directors ................................................................................................... 13 27. Board of Directors – Appointment of Vice-Chairperson ............................................. 13 28. Board of Directors - Appointment and Removal of the Chief Executive and Other
Executive Directors ................................................................................................... 13 29. Board of Directors – Disqualification ......................................................................... 14 30. Board of Directors – Meetings ................................................................................... 14 31. Board of Directors – Standing Orders ....................................................................... 14 32. Board of Directors - Conflicts of Interest ................................................................... 14 33. Board of Directors – Remuneration and Terms of Office .......................................... 16 34. Registers ................................................................................................................... 16 35. Admission to and removal from the registers ............................................................ 16 36. Registers – inspection and copies............................................................................. 16 37. Documents available for public inspection ................................................................ 17 38. Auditor ....................................................................................................................... 18 39. Audit committee ........................................................................................................ 18 40. Accounts ................................................................................................................... 18 41. Annual report, forward plans and non-NHS work ...................................................... 19 42. Presentation of the annual accounts and reports to the Governors and members ... 19 43. Instruments ............................................................................................................... 20 44. Amendment of the Constitution ................................................................................. 20 45. Mergers etc. and significant transactions .................................................................. 21 ANNEX 1 - THE PUBLIC CONSTITUENCY ........................................................................ 23 ANNEX 2 - THE STAFF CONSTITUENCY ......................................................................... 24 ANNEX 3 - COMPOSITION OF THE COUNCIL OF GOVERNORS ................................... 25 ANNEX 4 - MODEL ELECTION RULES .............................................................................. 27 ANNEX 5 – ADDITIONAL PROVISIONS – COUNCIL OF GOVERNORS .......................... 67
Constitution Page 2 of 107
ANNEX 6 ............................................................................................................................. 72 STANDING ORDERS - COUNCIL OF GOVERNORS ........................................................ 72 ANNEX 7 ............................................................................................................................. 85 STANDING ORDERS - BOARD OF DIRECTORS .............................................................. 85 ANNEX 8 – FURTHER PROVISIONS ............................................................................... 100 Appendix 1: Trust Core Principles ..................................................................................... 100 ANNEX 8 – FURTHER PROVISIONS ............................................................................... 101 Appendix 2: Membership ................................................................................................... 101 ANNEX 8 – FURTHER PROVISIONS ............................................................................... 103 Appendix 3: Members' Meetings ........................................................................................ 103 ANNEX 8 – FURTHER PROVISIONS ............................................................................... 106 Appendix 4: Board of Directors – Further Provisions ......................................................... 106
Constitution Page 3 of 107
1. Interpretation and Definitions
1.1 Unless otherwise stated, words or expressions contained in this Constitution shall bear the same meaning as in the National Health Service Act 2006 as amended by the Health and Social Care Act 2012.
1.2 References in this Constitution to any statute, statutory provision or subordinate legislation is a reference to it as it is in force from time to time including any amendment or re-enactment or subordinate legislation made under it.
1.3 Any phrase introduced by the terms including, include, in particular or any similar expression shall be construed as illustrative and shall not limit the sense of the words preceding those terms.
1.4 Headings in this Constitution are used for convenience only and shall not affect the construction or interpretation of this Constitution.
1.5 Words importing the masculine gender only shall include the feminine gender; words importing the singular shall import the plural and vice versa.
2006 Act means the National Health Service Act 2006. 2012 Act means the Health and Social Care Act 2012. Accounting Officer means the person who from time to time discharges the
functions specified in paragraph 25(5) of Schedule 7 to the 2006 Act.
Annual Members' Meeting is defined in paragraph 11 of the Constitution. Appointed Governors means those governors appointed by the Appointing
Organisations. Appointing Organisations means those organisations named in this Constitution
who are entitled to appoint governors. Auditor means the person appointed to audit the accounts of
the Trust who is called the auditor in the 2006 Act. Board of Directors means the Board of Directors of the Trust as constituted
in accordance with this Constitution. Chairperson means the chair of the Trust or, in relation to the
function of presiding at or chairing a meeting where another person is carrying out that role as required by the Constitution.
Constitution means this constitution and all annexes to it. Council of Governors means the Council of Governors as constituted in
accordance with this Constitution, which has the same meaning as in the 2006 Act, as amended by the 2012 Act.
Deleted: G
Deleted: G
Constitution Page 4 of 107
Director means a member of the Board of Directors. Elected Governor means each Governor elected by the Public
Constituency and the classes of the Staff Constituency. Executive Director means an executive director on the Board of Directors
of the Trust. Financial Year means each successive period of twelve months
beginning with 1 April. Governor means a member of the Council of Governors. Head Office
The Trust's head office is at the Royal Bournemouth Hospital, Castle Lane East, Bournemouth BH7 7DW.
Health Service in England means the provision of Health Care in line with NHS core principles; that is that care should be universal, comprehensive and free at the point of need.
Lead Governor means one (1) Governor appointed by the Council of Governors to lead the Council of Governors and to communicate directly with Monitor in certain circumstances.
Local Authority Governor means a governor appointed by the local authorities listed in Annex 3 whose area includes the whole or part of the Trust.
Members' Meetings means the Annual Members' Meeting and any Special Members' Meeting.
Monitor is the body corporate known as Monitor, as provided by section 61 of the 2012 Act.
NHS Body means an NHS foundation trust, the NHS Commissioning Board, an NHS trust, a clinical commissioning group, a special health authority or a Local Health Board.
Non-Executive Director means a non-executive director on the Board of Directors of the Trust.
Panel is defined in paragraph 19 of this Constitution. Partner means, in relation to another person, a member of the
same household living together as a family unit. Partnership Governor means a Governor appointed by a Partnership
Organisation. Partnership Organisation means those organisations specified in Annex 3 of this
Constitution as Partnership Organisations, which are specified organisations for the purposes of sub-paragraph 9(7) of Schedule 7 of the 2006 Act, as amended by the 2012 Act.
Public Constituency means that part of the Trust's membership consisting of members living in the area of the Trust specified in
Deleted: G
Constitution Page 5 of 107

Annex 1. Public Governor means a governor elected by the Public Constituency. Secretary means the person appointed as the Secretary to the
Trust or any other person appointed to perform the duties of secretary to the Trust, including a joint, assistant or deputy secretary, hereinafter to be referred to as the Secretary.
Senior Independent Director
means the non-executive Director appointed by the Board of Directors in accordance with paragraph 29.3 of this Constitution.
Significant Transaction A major change in the Trust’s service provision or configuration which would impact on patients, the finances or reputation of the Trust. Although the Trust does not use it, Monitor defines a significant transaction as being 10% of the value of assets, income or capital.
Special Members' Meeting shall have the meaning set out in Annex 8, Appendix 3, paragraph 1.2.
Staff Classes means the classes of the Staff Constituency as specified in Annex 2.
Staff Constituency means that that part of the Trust's membership consisting of the staff of the Trust and other person as described in paragraph 8 of this Constitution and which is divided into the Staff Classes.
Staff Governor means a governor elected by the members of one of the classes of Staff Constituency.
Trust means The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust.
Vice Chairperson means the non-executive director appointed by the Council of Governors in accordance with paragraph 27.1 of this Constitution.
2. Name 2.1 The name of the Trust is The Royal Bournemouth and Christchurch
Hospitals NHS Foundation Trust.
3. Principal Purpose
3.1 The principal purpose of the Trust is the provision of goods and services for the purposes of the health service in England.
3.2 The Trust does not fulfil its principal purpose unless, in each Financial Year, its total income from the provision of goods and services for the purposes of the health service in England is greater than its total income from the provision of goods and services for any other purposes.
3.3 The Trust may provide goods and services for any purposes related to:
Deleted: G
Deleted: This could include adding or removing services from the Trust’s portfolio, selling or acquiring land or assets.
Deleted: G
Constitution Page 6 of 107
3.3.1 the provision of services provided to individuals for or in connection with the prevention, diagnosis or treatment of illness, and
3.3.2 the promotion and protection of public health.
3.4 The Trust may also carry on activities other than those mentioned in paragraph 3.3 for the purpose of making additional income available in order better to carry on its principal purpose.
4. Powers
4.1 The powers of the Trust are set out in the 2006 Act.
4.2 All the powers of the Trust shall be exercised by the Board of Directors on behalf of the Trust.
4.3 Any of these powers may be delegated to a committee of Directors or to an Executive Director.
5. Membership and Constituencies
5.1 The Trust shall have members, each of whom shall be a member of one of the following constituencies:
5.1.1 a Public Constituency; and
5.1.2 a Staff Constituency.
6. Application for Membership
6.1 An individual who is eligible to become a member of the Trust may do so on application to the Trust.
7. Public Constituency
7.1 An individual who lives in an area specified in Annex 1 as an area for a public constituency may become or continue as a member of the Trust.
7.2 Those individuals who live in an area specified for a public constituency are referred to collectively as a Public Constituency.
7.3 The minimum number of members in each Public Constituency is specified in Annex 1.
8. Staff Constituency
8.1 An individual who is employed by the Trust under a contract of employment with the Trust may become or continue as a member of the Trust provided:
8.1.1 he is employed by the Trust under a contract of employment which has no fixed term or has a fixed term
Constitution Page 7 of 107
of at least 12 months; or
8.1.2 he has been continuously employed by the Trust under a contract of employment for at least 12 months.
8.2 Individuals, who exercise functions for the purposes of the Trust, otherwise than under a contract of employment with the Trust, may become or continue as members of the Staff Constituency provided such individuals have exercised these functions continuously for a period of at least 12 months. For the avoidance of doubt this does not include individuals who assist or provide services to the Trust on a voluntary basis.
8.3 Those individuals who are eligible for membership of the Trust by reason of the previous provisions are referred to collectively as the Staff Constituency.
8.4 The Staff Constituency shall be divided into five descriptions of individuals who are eligible for membership of the Staff Constituency, each description of individuals being specified within Annex 2 and being referred to as a class within the Staff Constituency.
8.5 The Secretary shall make a final decision about the class of the Staff Constituency of which an individual is eligible for membership.
8.6 The minimum number of members in each class of the Staff Constituency is specified in Annex 2.
9. Automatic Membership by Default – Staff
9.1 An individual who is:
9.1.1 eligible to become a member of the Staff Constituency, and
9.1.2 invited by the Trust to become a member of the Staff Constituency and a member of the appropriate class within the Staff Constituency,
shall become a member of the Trust as a member of the Staff Constituency and appropriate class within the Staff Constituency without an application being made, unless he informs the Trust that he does not wish to do so.
10. Restriction on Membership
10.1 An individual, who is a member of a constituency, or of a class within a constituency, may not while membership of that constituency or class continues, be a member of any other constituency or class.
10.2 An individual who satisfies the criteria for membership of the Staff Constituency may not become or continue as a member of any
Constitution Page 8 of 107

constituency other than the Staff Constituency.
10.3 An individual must be at least 12 years old to become a member of the Trust. Members must be 16 years old or over to vote in elections for Governors.
10.4 Further provisions as to the circumstances in which an individual may not become or continue as a member of the Trust are set out in Annex 8, Appendix 2 – Further Provisions (Membership).
11. Annual Members' Meeting
11.1 The Trust shall hold an annual meeting of its members. The Annual Members’ Meeting shall be open to members of the public.
11.2 Further provisions about the Annual Members' Meeting are set out in Annex 8, Appendix 3 – Further Provisions (Members' Meetings).
12. Council of Governors – Composition
12.1 The Trust is to have a Council of Governors, which shall comprise both elected and Appointed Governors.
12.2 The composition of the Council of Governors is specified in Annex 3.
12.3 The members of the Council of Governors, other than the Appointed Governors, shall be chosen by election by their constituency or, where there are classes within a constituency, by their class within that constituency. The number of governors to be elected by each constituency, or, where appropriate, by each class of each constituency, is specified in Annex 3.
13. Council of Governors – Election
13.1 Elections for elected members of the Council of Governors shall be conducted in accordance with the Model Election Rules using the first past the post system.
13.2 The Model Election Rules as published from time to time by the Department of Health form part of this Constitution. The Model Election Rules current at the date of this Constitution are attached at Annex 4.
13.3 A subsequent variation of the Model Election Rules by the Department of Health shall not constitute a variation of the terms of this Constitution for the purposes of paragraph 44 of the Constitution (Amendment of the Constitution).
13.4 An election, if contested, shall be by secret ballot.
14. Council of Governors - Tenure
14.1 An Elected Governor’s term of office may be for a period of up to three
Deleted: G
Deleted:
Deleted: hold office
Constitution Page 9 of 107

years.
14.2 An Elected Governor shall cease to hold office if he ceases to be a member of the constituency or class by which he was elected.
14.3 Subject to paragraph 14.7, an Elected Governor shall be eligible for re-election at the end of his term.
14.4 An Appointed Governor may hold office for a period of up to three years.
14.5 An Appointed Governor shall cease to hold office if the Appointing Organisation withdraws its sponsorship of him.
14.6 Subject to paragraph 14.7, an Appointed Governor shall be eligible for re-appointment at the end of his term.
14.7 No governor may serve for more than a total of two consecutive full terms of office.
14.8 For the purposes of these provisions concerning terms of office for governors, a term of office generally commences immediately after the conclusion of the Annual Members' Meeting. Where a governor has been elected in a by-election their term of office will commence immediately after the result is declared and end at the relevant Annual Members’ Meeting. Governors elected in a by-election may continue to serve two full terms of office at the discretion of the Council of Governors (the decision is to be made prior to them standing for the second full term of office).
15. Council of Governors – Disqualification and Removal
15.1 The following may not become or continue as a member of the Council of Governors:
15.1.1 a person under 18 years of age;
15.1.2 a person who has been adjudged bankrupt or whose estate has been sequestrated and (in either case) has not been discharged;
15.1.3 a person who has made a composition or arrangement with, or granted a trust deed for, his creditors and has not been discharged in respect of it;
15.1.4 a person who within the preceding five years has been convicted in the British Islands of any offence if a sentence of imprisonment (whether suspended or not) for a period of not less than three months (without the option of a fine) was imposed on him.
15.2 Further provisions as to the circumstances in which an individual may
Deleted: G
Deleted: six
Deleted: nine
Deleted: years
Deleted: G
Deleted: year means a period
Deleted: ing
Deleted: or part thereof, and ending at the conclusion of the next Annual Members' Meeting
Constitution Page 10 of 107
not become or continue, or may be removed, as a member of the Council of Governors are set out in Annex 5.
16. Council of Governors – Duties
16.1 The general duties of the Council of Governors are:
16.1.1 to hold the Non-Executive Directors individually and collectively to account for the performance of the Board of Directors; and
16.1.2 to represent the interests of the members of the Trust as a whole and the interests of the public.
16.2 The Trust must take steps to secure that the governors are equipped with the skills and knowledge they require in their capacity as such.
17. Council of Governors – Meetings
17.1 The Chairperson of the Trust (i.e. the Chairperson of the Board of Directors, appointed in accordance with the provisions of paragraph 26.1 below) or, in his absence the Vice-Chairman (appointed in accordance with the provisions of paragraph 27 below), shall preside at meetings of the Council of Governors.
17.2 Meetings of the Council of Governors shall be open to members of the public. Members of the public may be excluded from a meeting for special reasons.
17.3 For the purposes of obtaining information about the Trust’s performance of its functions or the Directors’ performance of their duties (and deciding whether to propose a vote on the Trust’s or Directors’ performance), the Council of Governors may require one or more of the Directors to attend a meeting.
18. Council of Governors – Standing Orders
18.1 The standing orders for the practice and procedure of the Council of Governors are attached at Annex 6.
19. Council of Governors – Referral to the Panel
19.1 In this paragraph, the Panel means a panel of persons appointed by Monitor to which a governor of an NHS foundation trust may refer a question as to whether the trust has failed or is failing:
19.1.1 to act in accordance with its constitution; or
19.1.2 to act in accordance with provision made by or under Chapter 5 of the 2006 Act.
Deleted: G
Constitution Page 11 of 107

19.2 A governor may refer a question to the Panel only if more than half of the members of the Council of Governors voting approve the referral.
20. Council of Governors - Conflicts of Interest
20.1 If a governor has a pecuniary, personal or family interest, whether that interest is actual or potential and whether that interest is direct or indirect, in any proposed contract or other matter which is under consideration or is to be considered by the Council of Governors, the governor shall disclose that interest to the members of the Council of Governors as soon as he becomes aware of it. The Standing Orders for the Council of Governors shall make provision for the disclosure of interests and arrangements for the exclusion of a governor declaring any interest from any discussion or consideration of the matter in respect of which an interest has been disclosed.
21. Council of Governors – Travel Expenses
21.1 The Trust may pay travelling and other expenses to members of the Council of Governors at rates determined by the Trust. These are to be disclosed in the annual report.
22. Council of Governors – further provisions
22.1 Further provisions with respect to the Council of Governors are set out in Annex 5.
23. Board of Directors – Composition
23.1 The Trust is to have a Board of Directors, which shall comprise both Executive and Non-Executive Directors.
23.2 The Board of Directors is to comprise:
23.2.1 a non-executive Chairperson;
23.2.2 six other Non-Executive Directors; and
23.2.3 seven Executive Directors.
23.3 One of the Executive Directors shall be the Chief Executive.
23.4 The Chief Executive shall be the Accounting Officer.
23.5 One of the Executive Directors shall be the finance director.
23.6 One of the Executive Directors is to be a registered medical practitioner (a fully registered person within the meaning of the Medical Act 1983) or a registered dentist (within the meaning of the Dentists Act 1984).
23.7 One of the Executive Directors is to be a registered nurse or a
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Constitution Page 12 of 107
registered midwife.
23.8 The Board of Directors shall elect one of the Non-Executive Directors, in consultation with the Council of Governors, to be the Senior Independent Director of the Board. Any Non-Executive Director so elected may at any time resign from the office of Senior Independent Director by giving notice in writing to the Chairman, and the Directors of the Trust may thereupon appoint another Non-Executive Director as Senior Independent Director in accordance with this paragraph.
23.9 The Directors shall at all times have one vote each save that where the number of votes for and against a motion is equal, the Chairperson shall be entitled to exercise a second and casting vote.
24. Board of Directors – General Duty
24.1 The general duty of the Board of Directors and of each Director individually, is to act with a view to promoting the success of the Trust so as to maximise the benefits for the members of the Trust as a whole and for the public.
25. Board of Directors – Qualification for Appointment as a Non-Executive Director
25.1 A person may be appointed as a Non-Executive Director only if:
25.1.1 he is a member of a Public Constituency, and
25.1.2 he is not disqualified by virtue of paragraph 29 below.
26. Board of Directors – Appointment and Removal of Chairperson and Other Non-Executive Directors
26.1 The Council of Governors at a general meeting of the Council of Governors shall appoint or remove the Chairperson of the Trust and the other Non-Executive Directors.
26.2 Removal of the Chairperson or another Non-Executive Director shall require the approval of three-quarters of the members of the Council of Governors.
27. Board of Directors – Appointment of Vice-Chairperson
27.1 The Council of Governors at a general meeting of the Council of Governors shall approve the appointment by the NED Nomination and Remuneration Committee of a Non-Executive Director as Vice-Chairperson. The appointed Non- Executive Director may also be the Senior Independent Director who will be appointed by the Board of Directors.
28. Board of Directors - Appointment and Removal of the Chief Executive and Other Executive Directors
Deleted: s
Constitution Page 13 of 107

28.1 A committee whose members shall be the Chairperson and at least two other Non-Executive Directors shall appoint or remove the Chief Executive.
28.2 The appointment of the Chief Executive shall require the approval of the Council of Governors.
28.3 A committee consisting of the Chairperson, the Chief Executive and at least two other Non-Executive Directors shall appoint or remove the other Executive Directors.
29. Board of Directors – Disqualification
29.1 The following may not become or continue as a member of the Board of Directors:
29.1.1 a person who has been adjudged bankrupt or whose estate has been sequestrated and (in either case) has not been discharged.
29.1.2 a person who has made a composition or arrangement with, or granted a trust deed for, his creditors and has not been discharged in respect of it.
29.1.3 a person who within the preceding five years has been convicted in the British Islands of any offence if a sentence of imprisonment (whether suspended or not) for a period of not less than three months (without the option of a fine) was imposed on him.
29.2 Further provisions as to the circumstances in which an individual may not become or continue as a Director on the Board of Directors are set out in Annex 8, Appendix 4 - Board of Directors – Further Provisions.
30. Board of Directors – Meetings
30.1 Meetings of the Board of Directors shall be open to members of the public. Members of the public may be excluded from a meeting for special reasons.
30.2 Before holding a meeting, the Board of Directors must send a copy of the agenda of the meeting to the Council of Governors. As soon as practicable after holding a meeting, the Board of Directors must send a copy of the minutes of the meeting to the Council of Governors.
31. Board of Directors – Standing Orders
31.1 The standing orders for the practice and procedure of the Board of Directors are attached at Annex 7.
32. Board of Directors - Conflicts of Interest
Constitution Page 14 of 107
32.1 The duties that a Director of the Trust has by virtue of being a Director include in particular:
32.1.1 a duty to avoid a situation in which the Director has (or can have) a direct or indirect interest that conflicts (or possibly may conflict) with the interests of the Trust.
32.1.2 a duty not to accept a benefit from a third party by reason of being a Director or doing (or not doing) anything in that capacity.
32.2 The duty referred to in sub-paragraph 32.1.1 is not infringed if:
32.2.1 the situation cannot reasonably be regarded as likely to give rise to a conflict of interest, or
32.2.2 the matter has been authorised in accordance with the Constitution.
32.3 The duty referred to in sub-paragraph 32.1.2 is not infringed if acceptance of the benefit cannot reasonably be regarded as likely to give rise to a conflict of interest.
32.4 In sub-paragraph 32.1.2, third party means a person other than:
32.4.1 the Trust, or
32.4.2 a person acting on its behalf.
32.5 If a Director of the Trust has in any way a direct or indirect interest in a proposed transaction or arrangement with the Trust, the Director must declare the nature and extent of that interest to the other Directors.
32.6 If a declaration under this paragraph proves to be, or becomes, inaccurate, incomplete, a further declaration must be made.
32.7 Any declaration required by this paragraph must be made before the Trust enters into the transaction or arrangement.
32.8 This paragraph does not require a declaration of an interest of which the Director is not aware or where the Director is not aware of the transaction or arrangement in question.
32.9 A Director need not declare an interest:
32.9.1 if it cannot reasonably be regarded as likely to give rise to a conflict of interest;
32.9.2 if, or to the extent that, the Directors are already aware of it;
32.9.3 if, or to the extent that, it concerns terms of the Director’s appointment that have been or are to be considered –
Constitution Page 15 of 107

32.9.3.1 by a meeting of the Board of Directors, or
32.9.3.2 by a committee of the Directors appointed for the purpose under the Constitution.
33. Board of Directors – Remuneration and Terms of Office
33.1 The Council of Governors at a general meeting of the Council of Governors shall decide the remuneration and allowances, and the other terms and conditions of office, of the Chairperson and the other Non-Executive Directors.
33.2 The Trust shall establish a committee of Non-Executive Directors to decide the remuneration and allowances, and the other terms and conditions of office, of the Chief Executive and other Executive Directors.
34. Registers
34.1 The Trust shall have:
34.1.1 a register of members showing, in respect of each member, the constituency to which he belongs and, where there are classes within it, the class to which he belongs;
34.1.2 a register of members of the Council of Governors;
34.1.3 a register of interests of governors;
34.1.4 a register of Directors; and
34.1.5 a register of interests of the Directors.
35. Admission to and removal from the registers
35.1 The members of the Trust are those individuals whose names are entered in the register of members.
35.2 The Secretary shall remove from the register of members the name of
any member who ceases to be entitled to be a member under the provisions of this Constitution.
35.3. The Secretary is to send to Monitor a list of persons who are elected or
appointed as governors or Directors.
36. Registers – inspection and copies
36.1 The Trust shall make the registers specified in paragraph 34 above available for inspection by members of the public, except in the circumstances set out below or as otherwise prescribed by regulations.
36.2 The Trust shall not make any part of its registers available for inspection
Deleted: G
Deleted: G
Constitution Page 16 of 107

by members of the public which shows details of any member of the Trust, if the member so requests.
36.3 So far as the registers are required to be made available:
36.3.1 they are to be available for inspection free of charge at all reasonable times; and
36.3.2 a person who requests a copy of or extract from the registers is to be provided with a copy or extract.
36.4 If the person requesting a copy or extract is not a member of the Trust, the Trust may impose a reasonable charge for doing so.
37. Documents available for public inspection
37.1 The Trust shall make the following documents available for inspection by members of the public free of charge at all reasonable times:
37.1.1 a copy of the current Constitution;
37.1.2 a copy of the latest annual accounts and of any report of the Auditor on them;
37.1.3 a copy of the latest annual report;
37.1.4 a copy of the latest information as to its forward planning;
37.1.5 a copy of the Trust's membership engagement strategy; and
37.1.6 a copy of the Trust's policy for the composition of the Council of Governors.
37.2 The Trust shall also make the following documents relating to a special administration of the Trust available for inspection by members of the public free of charge at all reasonable times:
37.2.1 a copy of any order made under section 65D (appointment of trust special administrator), 65J (power to extend time), 65KC (action following Secretary of State’s rejection of final report), 65L (trusts coming out of administration) or 65LA (trusts to be dissolved) of the 2006 Act.
37.2.2 a copy of any report laid under section 65D (appointment of trust special administrator) of the 2006 Act.
37.2.3 a copy of any information published under section 65D (appointment of trust special administrator) of the 2006 Act.
37.2.4 a copy of any draft report published under section 65F (administrator’s draft report) of the 2006 Act.
Deleted: development
Constitution Page 17 of 107

37.2.5 a copy of any statement provided under section 65F (administrator’s draft report) of the 2006 Act.
37.2.6 a copy of any notice published under section 65F (administrator’s draft report), 65G (consultation plan), 65H (consultation requirements), 65J (power to extend time), 65KA (Monitor’s decision), 65KB (Secretary of State’s response to Monitor’s decision), 65KC (action following Secretary of State’s rejection of final report) or 65KD (Secretary of State’s response to re-submitted final report) of the 2006 Act.
37.2.7 a copy of any statement published or provided under section 65G (consultation plan) of the 2006 Act.
37.2.8 a copy of any final report published under section 65I (administrator’s final report).
37.2.9 a copy of any statement published under section 65J (power to extend time) or 65KC (action following Secretary of State’s rejection of final report) of the 2006 Act.
37.2.10 a copy of any information published under section 65M (replacement of trust special administrator) of the 2006 Act.
37.3 Any person who requests a copy of or extract from any of the above documents is to be provided with a copy.
37.4 If the person requesting a copy or extract is not a member of the Trust, the Trust may impose a reasonable charge for doing so.
38. Auditor
38.1 The Trust shall have an Auditor.
38.2 The Council of Governors shall appoint or remove the Auditor at a general meeting of the Council of Governors.
39. Audit committee
39.1 The Trust shall establish a committee of Non-Executive Directors as an audit committee to perform such monitoring, reviewing and other functions as are appropriate.
40. Accounts
40.1 The Trust must keep proper accounts and proper records in relation to the accounts.
40.2 Monitor may with the approval of the Secretary of State give directions to the Trust as to the content and form of its accounts.
40.3 The accounts are to be audited by the Trust’s Auditor.
Constitution Page 18 of 107

40.4 The Trust shall prepare in respect of each Financial Year annual accounts in such form as Monitor may with the approval of the Secretary of State direct.
40.5 The functions of the Trust with respect to the preparation of the annual accounts shall be delegated to the Accounting Officer.
41. Annual report, forward plans and non-NHS work
41.1 The Trust shall prepare an Annual Report and send it to Monitor.
41.2 The Trust shall give information as to its forward planning in respect of each Financial Year to Monitor.
41.3 The document containing the information with respect to forward planning (referred to above) shall be prepared by the Directors.
41.4 In preparing the document, the Directors shall have regard to the views of the Council of Governors.
41.5 Each forward plan must include information about:
41.5.1 the activities other than the provision of goods and services for the purposes of the health service in England that the Trust proposes to carry on, and
41.5.2 the income it expects to receive from doing so.
41.6 Where a forward plan contains a proposal that the Trust carry on an activity of a kind mentioned in sub-paragraph 41.7 the Council of Governors:
41.6.1 must determine whether it is satisfied that the carrying on of the activity will not to any significant extent interfere with the fulfilment by the Trust of its principal purpose or the performance of its other functions, and
41.6.2 notify the Directors of the Trust of its determination.
41.7 Should the Trust propose to increase the proportion of its total income by 5% or more in any Financial Year that is attributable to activities other than the provision of goods and services for the purposes of the health service in England, it will require more than half of the members of the Council of Governors voting to approve its implementatione.g. if the total income is £100, £1 is Private Patient income, a change to move to £6 Private Patient income would trigger a vote, but a move to £4 would not.
42. Presentation of the annual accounts and reports to the Governors and members
Deleted: A trust which
Deleted: s
Deleted: by 5% or more
Deleted: may implement the proposal only if
Deleted: c
Deleted: g
Deleted: of the Trust
Deleted: must
Deleted:
Constitution Page 19 of 107

42.1 The following documents are to be presented to the Council of Governors at a general meeting of the Council of Governors:
42.1.1 the annual accounts;
42.1.2 any report of the Auditor on them; and
42.1.3 the annual report.
42.2 The documents shall also be presented to the members of the Trust at the Annual Members' Meeting by at least one member of the Board of Directors in attendance.
42.3 The Trust may combine a meeting of the Council of Governors convened for the purposes of sub-paragraph 42.1 with the Annual Members' Meeting.
43. Instruments
43.1 The Trust shall have a seal.
43.2 The seal shall not be affixed except under the authority of the Board of Directors.
44. Amendment of the Constitution
44.1 The Trust may make amendments of its Constitution only if:
44.1.1 more than half of the members of the Council of Governors of the Trust voting approve the amendments, and
44.1.2 more than half of the members of the Board of Directors of the Trust voting approve the amendments.
44.2 Amendments made under paragraph 44.1 take effect as soon as the conditions in that paragraph are satisfied, but the amendment has no effect in so far as the Constitution would, as a result of the amendment, not accord with schedule 7 of the 2006 Act.
44.3 Where an amendment is made to the Constitution in relation the powers or duties of the Council of Governors (or otherwise with respect to the role that the Council of Governors has as part of the Trust):
44.3.1 at least one member of the Council of Governors must attend the next Annual Members' Meeting and present the amendment, and
44.3.2 the Trust must give the members an opportunity to vote on whether they approve the amendment.
44.4 If more than half of the members voting approve the amendment, the amendment continues to have effect; otherwise, it ceases to have effect
Constitution Page 20 of 107
and the Trust must take such steps as are necessary as a result.
44.5 Amendments by the Trust of its Constitution are to be notified to Monitor. For the avoidance of doubt, Monitor’s functions do not include a power or duty to determine whether or not the Constitution, as a result of the amendments, accords with Schedule 7 of the 2006 Act.
45. Mergers etc. and significant transactions
45.1 The Trust may only apply for a merger, acquisition, separation or dissolution with the approval of more than half of the members of the Council of Governors.
45.2 The Constitution does not define significant transaction for the purposes of section 51A of the 2006 Act (Significant Transactions), although it notes that the Monitor definition is 10% of assets, income or capital. The Trust feels that the application of this definition would mean that the Council of Governors would very rarely be consulted on a significant transaction. By not defining significant transactions the Trust is able to ensure appropriate consultation and agreement of key actions as determined by the Board of Directors and Council of Governors on a case by case basis. As a minimum all significant transactions meeting the Monitor criteria will need to be agreed by the Council of Governors. This reflects the open and transparent relationship between the Board and Council.
46. Dispute Resolution Procedures
46.1 In the event of any dispute about the entitlement to membership the dispute shall be referred to the Secretary who shall make a determination on the point in issue. If a member or applicant (as the case may be) is aggrieved of the decision of the Secretary he may appeal in writing to the Council of Governors within 14 days of the Secretary's decision. The decision of the Council of Governors shall be final.
46.2 In the event of any dispute about the eligibility, disqualification and removal of a governor, the dispute shall be referred to the Council of Governors whose decision shall be final. The dispute must be notified to the Secretary within 28 days of the decision leading to the dispute.
46.3 In the event of dispute between the Council of Governors and the Board of Directors or between a governor and the Council of Governors:
46.3.1 In the first instance the Chairperson on advice of the Secretary, and such other advice as the Chairperson may see fit to obtain, shall seek to resolve the dispute;
46.3.2 If the Chairperson is unable to resolve the dispute he shall appoint a special Committee comprising equal numbers of Directors and governors to consider the circumstances and to
Deleted: contain any descriptions of the term ‘significant transaction’ for the purposes of section 51A of the 2006 Act (Significant Transactions).
Deleted: y
Deleted: G
Deleted: G
Deleted: G
Constitution Page 21 of 107

make recommendations to the Council of Governors and the Board of Directors with a view to resolving the dispute; and
46.3.3 If the recommendations (if any) of the special committee are unsuccessful in resolving the dispute, the Chairperson may refer the dispute back to the Board of Directors who shall make the final decision.
46.4 In the event of any dispute between a governor and the Council of Governors the dispute shall be referred within 28 days of it arising to the Secretary who shall make a determination on the point in issue and will reference the Chairperson and Council of Governors as necessary.
47. Indemnity
47.1 Members of the Council of Governors and the Board of Directors and the Secretary who act honestly and in good faith will not have to meet out of their personal resources any personal civil liability which is incurred in the execution or purported execution of their functions, save where they have acted recklessly. Any costs arising in this way will be met by the Trust. The Trust may purchase and maintain insurance against this liability for its own benefit and for the benefit of the Council of Governors and the Board of Directors and the Secretary.
48. Notices
48.1 Any notice required by this Constitution to be given shall be given in writing or shall be given using electronic communications to an address for the time being notified for that purpose. Address in relation to electronic communications includes any number or address used for the purposes of such communications.
48.2 Proof that an envelope containing a notice was properly addressed, prepaid and posted shall be conclusive evidence that the notice was given. A notice shall be treated as delivered 48 hours after the envelope containing it was posted or, in the case of a notice contained in an electronic communication, 48 hours after it was sent.
Constitution Page 22 of 107

ANNEX 1 - THE PUBLIC CONSTITUENCY
Name of Area Description Minimum Number of Members
Bournemouth and Poole
The electoral area covered by Bournemouth and Poole Borough Councils
4
Christchurch and Dorset County
The electoral areas covered by Christchurch Borough Council and the rest of Dorset County Council
4
New Forest and Rest of England
All other than those listed above electoral areas in England.
4
Deleted: ,
Deleted: Hampshire and Salisbury¶
Deleted: The following electoral divisions covered by New Forest Council:¶Downlands and Forest¶Fordingbridge¶Forest North West¶Ringwood North¶Ringwood South¶Ringwood East and Sopley¶Bransgore and Burley¶Bashley¶Fernhill¶Milton¶Barton¶Becton¶Milford¶Hordle¶Pennington¶Lymington town¶Buckland¶Boldre and Sway¶Brockenhurst and forest South East¶Lyndhurst¶Bramshaw, Copythorne North and Minstead¶Ashurst, Copythorne South and Netley¶Totton North¶Totton West¶Totton East¶Totton Central¶Totton South¶Marchwood¶Dibden and Hythe East¶Hythe and Langdown¶Butts Ash and Dibden Purlieu¶Furzedown and Hardley¶Holbury and North Blackfield¶Fawley, Blackfield and Langley¶¶The following electoral divisions covered¶by Wiltshire Council:¶Bemerton¶St. Mark and Stratford¶Bishopdown¶St. Paul¶Fisherton and Bemerton Village¶St. Edmund and Milford¶St. Martin and Milford¶Harnham West¶Harnham East¶Ebble¶Downton and Redlynch¶Alderbury and Whiteparish¶¶The following electoral divisions covered by Hampshire County Council:¶Blackwater¶Romsey Extra¶Chilworth, Nursling and Rownhams¶Cupernham¶Abbey¶Tadburn¶North Baddesley¶Valley Park¶Hiltingbury West¶Hiltingbury East¶Chandlers Ford West¶Chandlers Fords East¶Eastleigh North¶Eastleigh Central¶Eastleigh South¶Bishopstoke West¶Bishopstoke East¶Fair Oak and Horton Heath¶West End North¶ ...
Constitution Page 23 of 107

ANNEX 2 - THE STAFF CONSTITUENCY
Name of Class Minimum Number of Members Medical and Dental 4 Nursing, Midwifery and Healthcare Assistants 4 Estates and Ancillary Services 4 Allied Health Professions, Scientific and Technical 4 Administrative, Clerical and Management 4
Constitution Page 24 of 107

ANNEX 3 - COMPOSITION OF THE COUNCIL OF GOVERNORS 1. Public Elected Governors
There are 18 governors in the Public Constituency. Area
Number of Governors
Bournemouth and Poole 9 Christchurch and Dorset County 6 New Forest, Hampshire and Salisbury 3
2. Staff Elected Governors
There are five governors in the Staff Constituency from the following Staff Classes: Staff Class
Number of Governors
Medical and Dental 1 Nursing, Midwifery and Healthcare Assistants 1 Estates and Ancillary Services 1 Allied Health Professions, Scientific and Technical 1 Administrative, Clerical and Management 1
3. Appointed Governors
There are six Appointed Governors. Appointing Organisation
Number of Governors
Local Authority Governors Bournemouth Borough Council 1 Borough of Poole 1 Dorset County Council 1 Partnership Organisations Bournemouth University 1 NHS Dorset Clinical Commissioning Group 1 The Royal Bournemouth and Christchurch Hospitals Volunteers Group
1
4. Majority of Public Governors
4.1. The aggregate number of governors on the Council of Governors in the Public
Constituency must be more than half of the total number of members of the Council of Governors.
4.2. Where for any reason the aggregate number of governors on the Council of
Governors in the Public Constituency falls to the same number or below the number of the other governors then the Appointed Governors shall temporarily
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Constitution Page 25 of 107

stand down in the following order, until there is a majority of governors on the Council of Governors in the Public Constituency. In such circumstances, the governors that have stood down will be permitted to attend Council of Governors meetings but will not have a vote:
• firstly, the governor from NHS Dorset Clinical Commissioning Group; • secondly, the most recently appointed Local Authority Governor; and • thirdly, the most recently appointed Partnership Governor (not including the
Governor from NHS Dorset Clinical Commissioning Group).
4.3. The validity of any act of the Trust is not affected by any vacancy among the governors or by any defect in the appointment of any governor.
5. Appointment Process for Appointed Governors
Each of the Appointing Organisations listed above are entitled to appoint a governor in accordance with a process agreed with the Trust.
6. Policy on Composition of the Council of Governors 6.1. The Council of Governors, subject to the 2006 Act, shall seek to ensure that
through the composition of the Council of Governors: 6.1.1. the interest of the community served by the Trust are appropriately
represented; 6.1.2. the level of representation of the Public Constituency and the classes of the
Staff Constituency and the Appointing Organisations strikes an appropriate balance having regard to their legitimate interest in the Trust's affairs,
and to this end, the Council of Governors 6.1.3. shall at all times maintain a policy for the composition of the Council of
Governors which takes account of the membership strategy; and 6.1.4. shall from time to time and not less than every three years review the policy
for the composition of the Council of Governors; and 6.1.5. when appropriate shall propose amendments to the Constitution.
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Constitution Page 26 of 107
ANNEX 4 - MODEL ELECTION RULES PART 1: INTERPRETATION 1. Interpretation PART 2: TIMETABLE FOR ELECTION 2. Timetable 3. Computation of time PART 3: RETURNING OFFICER 4. Returning officer 5. Staff 6. Expenditure 7. Duty of co-operation PART 4: STAGES COMMON TO CONTESTED AND UNCONTESTED ELECTIONS 8. Notice of election 9. Nomination of candidates 10. Candidate’s particulars 11. Declaration of interests 12. Declaration of eligibility 13. Signature of candidate 14. Decisions as to validity of nomination forms 15. Publication of statement of nominated candidates 16. Inspection of statement of nominated candidates and nomination
forms 17. Withdrawal of candidates 18. Method of election PART 5: CONTESTED ELECTIONS 19. Poll to be taken by ballot 20. The ballot paper 21. The declaration of identity (public and patient constituencies) Action to be taken before the poll 22. List of eligible voters 23. Notice of poll 24. Issue of voting information by returning officer 25. Ballot paper envelope and covering envelope 26. E-voting systems
Constitution Page 27 of 107

The poll 27. Eligibility to vote 28. Voting by persons who require assistance 29. Spoilt ballot papers and spoilt text message votes 30. Lost voting information 31. Issue of replacement voting information 32. ID declaration form for replacement ballot papers (public and patient
constituencies) 33 Procedure for remote voting by internet 34. Procedure for remote voting by telephone 35. Procedure for remote voting by text message Procedure for receipt of envelopes, internet votes, telephone vote and text message votes 36. Receipt of voting documents 37. Validity of votes 38. Declaration of identity but no ballot (public and patient constituency) 39. De-duplication of votes 40. Sealing of packets PART 6: COUNTING THE VOTES 41. Arrangements for counting of the votes 42. The count 43. Rejected ballot papers and rejected text voting records 44. Equality of votes PART 7: FINAL PROCEEDINGS IN CONTESTED AND UNCONTESTED ELECTIONS 45. Declaration of result for contested elections 46. Declaration of result for uncontested elections PART 8: DISPOSAL OF DOCUMENTS 47. Sealing up of documents relating to the poll 48. Delivery of documents 49. Forwarding of documents received after close of the poll 50. Retention and public inspection of documents 51. Application for inspection of certain documents relating to election PART 9: DEATH OF A CANDIDATE DURING A CONTESTED ELECTION 52. Countermand or abandonment of poll on death of candidate PART 10: ELECTION EXPENSES AND PUBLICITY Expenses
Constitution Page 28 of 107

53. Election expenses 54. Expenses and payments by candidates 55. Expenses incurred by other persons Publicity 56. Publicity about election by the corporation 57. Information about candidates for inclusion with voting information 58. Meaning of “for the purposes of an election” PART 11: QUESTIONING ELECTIONS AND IRREGULARITIES 59. Application to question an election PART 12: MISCELLANEOUS 60. Secrecy 61. Prohibition of disclosure of vote 62. Disqualification 63. Delay in postal service through industrial action or unforeseen event
Constitution Page 29 of 107

PART 1: INTERPRETATION 1. Interpretation 1.1 In these rules, unless the context otherwise requires:
“2006 Act” means the National Health Service Act 2006;
“corporation” means the public benefit corporation subject to this constitution;
“council of governors” means the council of governors of the corporation;
“declaration of identity” has the meaning set out in rule 21.1;
“election” means an election by a constituency, or by a class within a constituency, to fill a vacancy among one or more posts on the council of governors;
“e-voting” means voting using either the internet, telephone or text message;
“e-voting information” has the meaning set out in rule 24.2;
“ID declaration form” has the meaning set out in Rule 21.1;
“internet voting record” has the meaning set out in rule 26.4(d);
“internet voting system” means such computer hardware and software, data other equipment and services as may be provided by the returning officer for the purpose of enabling voters to cast their votes using the internet;
“lead governor” means the governor nominated by the corporation to fulfil the role described in Appendix B to The NHS Foundation Trust Code of Governance (Monitor, December 2013) or any later version of such code.
“list of eligible voters” means the list referred to in rule 22.1, containing the information in rule 22.2;
“method of polling” means a method of casting a vote in a poll, which may be by post, internet, text message or telephone;
“Monitor” means the corporate body known as Monitor as provided by section 61 of the 2012 Act; “numerical voting code” has the meaning set out in rule 64.2(b)
“polling website” has the meaning set out in rule 26.1;
“postal voting information” has the meaning set out in rule 24.1;
“telephone short code” means a short telephone number used for
Constitution Page 30 of 107

the purposes of submitting a vote by text message;
“telephone voting facility” has the meaning set out in rule 26.2;
“telephone voting record” has the meaning set out in rule 26.5 (d);
“text message voting facility” has the meaning set out in rule 26.3;
“text voting record” has the meaning set out in rule 26.6 (d);
“the telephone voting system” means such telephone voting facility as may be provided by the returning officer for the purpose of enabling voters to cast their votes by telephone;
“the text message voting system” means such text messaging voting facility as may be provided by the returning officer for the purpose of enabling voters to cast their votes by text message;
“voter ID number” means a unique, randomly generated numeric identifier allocated to each voter by the Returning Officer for the purpose of e-voting,
“voting information” means postal voting information and/or e-voting information
1.2 Other expressions used in these rules and in Schedule 7 to the NHS Act 2006 have the same meaning in these rules as in that Schedule.
Constitution Page 31 of 107
PART 2: TIMETABLE FOR ELECTION 2. Timetable 2.1 The proceedings at an election shall be conducted in accordance
with the following timetable:
Proceeding Time
Publication of notice of election Not later than the fortieth day before the day of the close of the poll.
Final day for delivery of nomination forms to returning officer
Not later than the twenty eighth day before the day of the close of the poll.
Publication of statement of nominated candidates
Not later than the twenty seventh day before the day of the close of the poll.
Final day for delivery of notices of withdrawals by candidates from election
Not later than twenty fifth day before the day of the close of the poll.
Notice of the poll Not later than the fifteenth day before the day of the close of the poll.
Close of the poll By 5.00pm on the final day of the election.
3. Computation of time 3.1 In computing any period of time for the purposes of the timetable:
(a) a Saturday or Sunday;
(b) Christmas day, Good Friday, or a bank holiday, or
(c) a day appointed for public thanksgiving or mourning,
shall be disregarded, and any such day shall not be treated as a day for the purpose of any proceedings up to the completion of the poll, nor shall the returning officer be obliged to proceed with the counting of votes on such a day.
3.2 In this rule, “bank holiday” means a day which is a bank holiday
under the Banking and Financial Dealings Act 1971 in England and Wales.
Constitution Page 32 of 107

PART 3: RETURNING OFFICER 4. Returning Officer 4.1 Subject to rule 62, the returning officer for an election is to be
appointed by the corporation. 4.2 Where two or more elections are to be held concurrently, the
same returning officer may be appointed for all those elections. 5. Staff 5.1 Subject to rule 62, the returning officer may appoint and pay such
staff, including such technical advisers, as he or she considers necessary for the purposes of the election.
6. Expenditure 6.1 The corporation is to pay the returning officer:
(a) any expenses incurred by that officer in the exercise of his or her functions under these rules,
(b) such remuneration and other expenses as the corporation may determine.
7. Duty of co-operation 7.1 The corporation is to co-operate with the returning officer in the
exercise of his or her functions under these rules. PART 4: STAGES COMMON TO CONTESTED AND UNCONTESTED
ELECTIONS
8. Notice of election 8.1 The returning officer is to publish a notice of the election stating:
(a) the constituency, or class within a constituency, for which the election is being held,
(b) the number of members of the Council of Governors to be elected from that constituency, or class within that constituency,
(c) the details of any nomination committee that has been established by the corporation,
(d) the address and times at which nomination forms may be obtained;
Deleted: c
Deleted: g
Constitution Page 33 of 107

(e) the address for return of nomination forms (including, where the return of nomination forms in an electronic format will be permitted, the e-mail address for such return) and the date and time by which they must be received by the returning officer,
(f) the date and time by which any notice of withdrawal must be received by the returning officer
(g) the contact details of the returning officer (h) the date and time of the close of the poll in the event of a
contest. 9. Nomination of candidates 9.1 Subject to rule 9.2, each candidate must nominate themselves on
a single nomination form. 9.2 The returning officer:
(a) is to supply any member of the corporation with a nomination form, and
(b) is to prepare a nomination form for signature at the request of any member of the corporation,
but it is not necessary for a nomination to be on a form supplied by the returning officer and a nomination can, subject to rule 13, be in an electronic format.
10. Candidate’s particulars 10.1 The nomination form must state the candidate’s:
(a) full name, (b) contact address in full (which should be a postal address
although an e-mail address may also be provided for the purposes of electronic communication), and
(c) constituency, or class within a constituency, of which the candidate is a member.
11. Declaration of interests 11.1 The nomination form must state:
(a) any financial interest that the candidate has in the corporation, and
(b) whether the candidate is a member of a political party, and if so, which party,
Constitution Page 34 of 107

and if the candidate has no such interests, the paper must include a statement to that effect.
12. Declaration of eligibility 12.1 The nomination form must include a declaration made by the
candidate:
(a) that he or she is not prevented from being a member of the council of governors by paragraph 8 of Schedule 7 of the 2006 Act or by any provision of the constitution;
(b) for a member of the public or patient constituency, of the particulars of his or her qualification to vote as a member of that constituency, or class within that constituency, for which the election is being held and;
(c) they are 18 years of age or over. 13. Signature of candidate 13.1 The nomination form must be signed and dated by the candidate,
in a manner prescribed by the returning officer, indicating that:
(a) they wish to stand as a candidate, (b) their declaration of interests as required under rule 11, is
true and correct, and (c) their declaration of eligibility, as required under rule 12, is
true and correct. 13.2 Where the return of nomination forms in an electronic format is
permitted, the returning officer shall specify the particular signature formalities (if any) that will need to be complied with by the candidate.
14. Decisions as to the validity of nomination 14.1 Where a nomination form is received by the returning officer in
accordance with these rules, the candidate is deemed to stand for election unless and until the returning officer:
(a) decides that the candidate is not eligible to stand, (b) decides that the nomination form is invalid, (c) receives satisfactory proof that the candidate has died, or (d) receives a written request by the candidate of their withdrawal from
candidacy.
14.2 The returning officer is entitled to decide that a nomination form is
Constitution Page 35 of 107

invalid only on one of the following grounds:
(a) that the paper is not received on or before the final time and date for return of nomination forms, as specified in the notice of the election,
(b) that the paper does not contain the candidate’s particulars, as required by rule 10;
(c) that the paper does not contain a declaration of the interests of the candidate, as required by rule 11,
(d) that the paper does not include a declaration of eligibility as required by rule 12, or
(e) that the paper is not signed and dated by the candidate, if required by rule 13.
14.3 The returning officer is to examine each nomination form as soon
as is practicable after he or she has received it, and decide whether the candidate has been validly nominated.
14.4 Where the returning officer decides that a nomination is invalid,
the returning officer must endorse this on the nomination form, stating the reasons for their decision.
14.5 The returning officer is to send notice of the decision as to
whether a nomination is valid or invalid to the candidate at the contact address given in the candidate’s nomination form. If an e-mail address has been given in the candidate’s nomination form (in addition to the candidate’s postal address), the returning officer may send notice of the decision to that address.
15. Publication of statement of candidates 15.1 The returning officer is to prepare and publish a statement
showing the candidates who are standing for election.
15.2 The statement must show:
(a) the name, contact address (which shall be the candidate’s postal address), and constituency or class within a constituency of each candidate standing, and
(b) the declared interests of each candidate standing, as given in their nomination form.
15.3 The statement must list the candidates standing for election in
alphabetical order by surname.
15.4 The returning officer must send a copy of the statement of candidates and copies of the nomination forms to the corporation
Constitution Page 36 of 107

as soon as is practicable after publishing the statement. 16. Inspection of statement of nominated candidates and
nomination forms 16.1 The corporation is to make the statement of the candidates and
the nomination forms supplied by the returning officer under rule 15.4 available for inspection by members of the corporation free of charge at all reasonable times.
16.2 If a member of the corporation requests a copy or extract of the
statement of candidates or their nomination forms, the corporation is to provide that member with the copy or extract free of charge.
17. Withdrawal of candidates 17.1 A candidate may withdraw from election on or before the date
and time for withdrawal by candidates, by providing to the returning officer a written notice of withdrawal which is signed by the candidate and attested by a witness.
18. Method of election 18.1 If the number of candidates remaining validly nominated for an
election after any withdrawals under these rules is greater than the number of members to be elected to the council of governors, a poll is to be taken in accordance with Parts 5 and 6 of these rules.
18.2 If the number of candidates remaining validly nominated for an
election after any withdrawals under these rules is equal to the number of members to be elected to the council of governors, those candidates are to be declared elected in accordance with Part 7 of these rules.
18.3 If the number of candidates remaining validly nominated for an
election after any withdrawals under these rules is less than the number of members to be elected to be council of governors, then:
(a) the candidates who remain validly nominated are to be
declared elected in accordance with Part 7 of these rules, and
(b) the returning officer is to order a new election to fill any vacancy which remains unfilled, on a day appointed by him or her in consultation with the corporation.
Constitution Page 37 of 107

PART 5: CONTESTED ELECTIONS 19. Poll to be taken by ballot 19.1 The votes at the poll must be given by secret ballot. 19.2 The votes are to be counted and the result of the poll determined
in accordance with Part 6 of these rules.
19.3 The corporation may decide that voters within a constituency or class within a constituency, may, subject to rule 19.4, cast their votes at the poll using such different methods of polling in any combination as the corporation may determine.
19.4 The corporation may decide that voters within a constituency or
class within a constituency for whom an e-mail address is included in the list of eligible voters may only cast their votes at the poll using an e-voting method of polling.
19.5 Before the corporation decides, in accordance with rule 19.3 that
one or more e-voting methods of polling will be made available for the purposes of the poll, the corporation must satisfy itself that:
(a) if internet voting is to be a method of polling, the internet
voting system to be used for the purpose of the election is:
(i) configured in accordance with these rules; and
(ii) will create an accurate internet voting record in respect of any voter who casts his or her vote using the internet voting system;
(b) if telephone voting to be a method of polling, the telephone voting system to be used for the purpose of the election is:
(i) configured in accordance with these rules; and
(ii) will create an accurate telephone voting record in respect of any voter who casts his or her vote using the telephone voting system;
(c) if text message voting is to be a method of polling, the text message voting system to be used for the purpose of the election is:
(i) configured in accordance with these rules; and (ii) will create an accurate text voting record in respect of
any voter who casts his or her vote using the text message voting system.
Constitution Page 38 of 107
20. The ballot paper
20.1 The ballot of each voter (other than a voter who casts his or her ballot by an e-voting method of polling) is to consist of a ballot paper with the persons remaining validly nominated for an election after any withdrawals under these rules, and no others, inserted in the paper.
20.2 Every ballot paper must specify:
(a) the name of the corporation, (b) the constituency, or class within a constituency, for which
the election is being held, (c) the number of members of the council of governors to be
elected from that constituency, or class within that constituency,
(d) the names and other particulars of the candidates standing for election, with the details and order being the same as in the statement of nominated candidates,
(e) instructions on how to vote by all available methods of polling, including the relevant voter’s voter ID number if one or more e-voting methods of polling are available,
(f) if the ballot paper is to be returned by post, the address for its return and the date and time of the close of the poll, and
(g) the contact details of the returning officer. 20.3 Each ballot paper must have a unique identifier. 20.4 Each ballot paper must have features incorporated into it to
prevent it from being reproduced.
21. The declaration of identity (public and patient constituencies)
21.1 The corporation shall require each voter who participates in an
election for a public or patient constituency to make a declaration confirming:
(a) that the voter is the person:
(i) to whom the ballot paper was addressed, and/or
(ii) to whom the voter ID number contained within the e-voting information was allocated,
Constitution Page 39 of 107
(b) that he or she has not marked or returned any other voting information in the election, and
(c) the particulars of his or her qualification to vote as a
member of the constituency or class within the constituency for which the election is being held,
(“declaration of identity”)
and the corporation shall make such arrangements as it considers appropriate to facilitate the making and the return of a declaration of identity by each voter, whether by the completion of a paper form (“ID declaration form”) or the use of an electronic method.
21.2 The voter must be required to return his or her declaration of
identity with his or her ballot.
21.3 The voting information shall caution the voter that if the declaration of identity is not duly returned or is returned without having been made correctly, any vote cast by the voter may be declared invalid.
Action to be taken before the poll 22. List of eligible voters 22.1 The corporation is to provide the returning officer with a list of the
members of the constituency or class within a constituency for which the election is being held who are eligible to vote by virtue of rule 27 as soon as is reasonably practicable after the final date for the delivery of notices of withdrawals by candidates from an election.
22.2 The list is to include, for each member:
(a) a postal address; and, (b) the member’s e-mail address, if this has been provided to which his or her voting information may, subject to rule 22.3, be sent.
22.3 The corporation may decide that the e-voting information is to be
sent only by e-mail to those members in the list of eligible voters for whom an e-mail address is included in that list.
Constitution Page 40 of 107
23. Notice of poll 23.1 The returning officer is to publish a notice of the poll stating:
(a) the name of the corporation, (b) the constituency, or class within a constituency, for which
the election is being held, (c) the number of members of the council of governors to be
elected from that constituency, or class with that constituency,
(d) the names, contact addresses, and other particulars of the candidates standing for election, with the details and order being the same as in the statement of nominated candidates,
(e) that the ballot papers for the election are to be issued and returned, if appropriate, by post,
(f) the methods of polling by which votes may be cast at the election by voters in a constituency or class within a constituency, as determined by the corporation in accordance with rule 19.3,
(g) the address for return of the ballot papers, (h) the uniform resource locator (url) where, if internet voting is
a method of polling, the polling website is located; (i) the telephone number where, if telephone voting is a
method of polling, the telephone voting facility is located, (j) the telephone number or telephone short code where, if text
message voting is a method of polling, the text message voting facility is located,
(k) the date and time of the close of the poll, (l) the address and final dates for applications for replacement
voting information, and (m) the contact details of the returning officer.
24. Issue of voting information by returning officer 24.1 Subject to rule 24.3, as soon as is reasonably practicable on or
after the publication of the notice of the poll, the returning officer is to send the following information by post to each member of the corporation named in the list of eligible voters: (a) a ballot paper and ballot paper envelope,
Constitution Page 41 of 107

(b) the ID declaration form (if required), (c) information about each candidate standing for election,
pursuant to rule 61 of these rules, and (d) a covering envelope;
(“postal voting information”).
24.2 Subject to rules 24.3 and 24.4, as soon as is reasonably practicable on or after the publication of the notice of the poll, the returning officer is to send the following information by e-mail and/ or by post to each member of the corporation named in the list of eligible voters whom the corporation determines in accordance with rule 19.3 and/ or rule 19.4 may cast his or her vote by an e-voting method of polling: (a) instructions on how to vote and how to make a declaration
of identity (if required), (b) the voter’s voter ID number, (c) information about each candidate standing for election,
pursuant to rule 57 of these rules, or details of where this information is readily available on the internet or available in such other formats as the Returning Officer thinks appropriate,
(d) contact details of the returning officer,
(“e-voting information”).
24.3 The corporation may determine that any member of the corporation shall:
(a) only be sent postal voting information; or
(b) only be sent e-voting information; or
(c) be sent both postal voting information and e-voting information;
for the purposes of the poll.
24.4 If the corporation determines, in accordance with rule 22.3, that the e-voting information is to be sent only by e-mail to those members in the list of eligible voters for whom an e-mail address is included in that list, then the returning officer shall only send that information by e-mail.
24.5 The voting information is to be sent to the postal address and/ or
e-mail address for each member, as specified in the list of eligible voters.
Constitution Page 42 of 107

25. Ballot paper envelope and covering envelope 25.1 The ballot paper envelope must have clear instructions to the
voter printed on it, instructing the voter to seal the ballot paper inside the envelope once the ballot paper has been marked.
25.2 The covering envelope is to have:
(a) the address for return of the ballot paper printed on it, and (b) pre-paid postage for return to that address.
25.3 There should be clear instructions, either printed on the covering envelope or elsewhere, instructing the voter to seal the following documents inside the covering envelope and return it to the returning officer – (a) the completed ID declaration form if required, and (b) the ballot paper envelope, with the ballot paper sealed inside
it. 26. E-voting systems 26.1 If internet voting is a method of polling for the relevant election
then the returning officer must provide a website for the purpose of voting over the internet (in these rules referred to as "the polling website").
26.2 If telephone voting is a method of polling for the relevant election
then the returning officer must provide an automated telephone system for the purpose of voting by the use of a touch-tone telephone (in these rules referred to as “the telephone voting facility”).
26.3 If text message voting is a method of polling for the relevant
election then the returning officer must provide an automated text messaging system for the purpose of voting by text message (in these rules referred to as “the text message voting facility”).
26.4 The returning officer shall ensure that the polling website and
internet voting system provided will:
(a) require a voter to: (i) enter his or her voter ID number; and (ii) where the election is for a public or patient
constituency, make a declaration of identity; in order to be able to cast his or her vote;
(b) specify: (i) the name of the corporation,
Constitution Page 43 of 107

(ii) the constituency, or class within a constituency, for which the election is being held,
(iii) the number of members of the council of governors to be elected from that constituency, or class within that constituency,
(iv) the names and other particulars of the candidates standing for election, with the details and order being the same as in the statement of nominated candidates,
(v) instructions on how to vote and how to make a declaration of identity,
(vi) the date and time of the close of the poll, and
(vii) the contact details of the returning officer;
(c) prevent a voter from voting for more candidates than he or she is entitled to at the election;
(d) create a record ("internet voting record") that is stored in the internet voting system in respect of each vote cast by a voter using the internet that comprises of- (i) the voter’s voter ID number; (ii) the voter’s declaration of identity (where required); (iii) the candidate or candidates for whom the voter has
voted; and (iv) the date and time of the voter’s vote,
(e) if the voter’s vote has been duly cast and recorded, provide the voter with confirmation of this; and
(f) prevent any voter from voting after the close of poll. 26.5 The returning officer shall ensure that the telephone voting facility
and telephone voting system provided will:
(a) require a voter to: (i) enter his or her voter ID number in order to be able to
cast his or her vote; and
(ii) where the election is for a public or patient constituency, make a declaration of identity;
(b) specify: (i) the name of the corporation,
(ii) the constituency, or class within a constituency, for
Constitution Page 44 of 107

which the election is being held,
(iii) the number of members of the council of governors to be elected from that constituency, or class within that constituency,
(iv) instructions on how to vote and how to make a declaration of identity,
(v) the date and time of the close of the poll, and
(vi) the contact details of the returning officer; (c) prevent a voter from voting for more candidates than he or
she is entitled to at the election; (d) create a record ("telephone voting record") that is stored in
the telephone voting system in respect of each vote cast by a voter using the telephone that comprises of: (i) the voter’s voter ID number; (ii) the voter’s declaration of identity (where required); (iii) the candidate or candidates for whom the voter has
voted; and (iv) the date and time of the voter’s vote
(e) if the voter’s vote has been duly cast and recorded, provide
the voter with confirmation of this; (f) prevent any voter from voting after the close of poll.
26.6 The returning officer shall ensure that the text message voting
facility and text messaging voting system provided will:
(a) require a voter to: (i) provide his or her voter ID number; and
(ii) where the election is for a public or patient constituency, make a declaration of identity;
in order to be able to cast his or her vote; (b) prevent a voter from voting for more candidates than he or
she is entitled to at the election; (d) create a record ("text voting record") that is stored in the text
messaging voting system in respect of each vote cast by a voter by text message that comprises of: (i) the voter’s voter ID number;
(ii) the voter’s declaration of identity (where required);
(ii) the candidate or candidates for whom the voter has
Constitution Page 45 of 107

voted; and (iii) the date and time of the voter’s vote
(e) if the voter’s vote has been duly cast and recorded, provide the voter with confirmation of this;
(f) prevent any voter from voting after the close of poll. The poll 27. Eligibility to vote 27.1 An individual who becomes a member of the corporation on or
before the closing date for the receipt of nominations by candidates for the election is eligible to vote in that election.
28. Voting by persons who require assistance 28.1 The returning officer is to put in place arrangements to enable
requests for assistance to vote to be made.
28.2 Where the returning officer receives a request from a voter who requires assistance to vote, the returning officer is to make such arrangements as he or she considers necessary to enable that voter to vote.
29. Spoilt ballot papers and spoilt text message votes 29.1 If a voter has dealt with his or her ballot paper in such a manner
that it cannot be accepted as a ballot paper (referred to as a “spoilt ballot paper”), that voter may apply to the returning officer for a replacement ballot paper.
29.2 On receiving an application, the returning officer is to obtain the
details of the unique identifier on the spoilt ballot paper, if he or she can obtain it.
29.3 The returning officer may not issue a replacement ballot paper for
a spoilt ballot paper unless he or she:
(a) is satisfied as to the voter’s identity; and (b) has ensured that the completed ID declaration form, if
required, has not been returned.
29.4 After issuing a replacement ballot paper for a spoilt ballot paper, the returning officer shall enter in a list (“the list of spoilt ballot papers”):
(a) the name of the voter, and
Constitution Page 46 of 107

(b) the details of the unique identifier of the spoilt ballot paper (if that officer was able to obtain it), and
(c) the details of the unique identifier of the replacement ballot
paper. 29.5 If a voter has dealt with his or her text message vote in such a
manner that it cannot be accepted as a vote (referred to as a “spoilt text message vote”), that voter may apply to the returning officer for a replacement voter ID number.
29.6 On receiving an application, the returning officer is to obtain the
details of the voter ID number on the spoilt text message vote, if he or she can obtain it.
29.7 The returning officer may not issue a replacement voter ID
number in respect of a spoilt text message vote unless he or she is satisfied as to the voter’s identity.
29.8 After issuing a replacement voter ID number in respect of a spoilt
text message vote, the returning officer shall enter in a list (“the list of spoilt text message votes”):
(a) the name of the voter, and (b) the details of the voter ID number on the spoilt text message
vote (if that officer was able to obtain it), and (c) the details of the replacement voter ID number issued to the
voter. 30. Lost voting information 30.1 Where a voter has not received his or her voting information by
the tenth day before the close of the poll, that voter may apply to the returning officer for replacement voting information.
30.2 The returning officer may not issue replacement voting
information in respect of lost voting information unless he or she:
(a) is satisfied as to the voter’s identity, (b) has no reason to doubt that the voter did not receive the
original voting information, (c) has ensured that no declaration of identity, if required, has
been returned.
30.3 After issuing replacement voting information in respect of lost voting information, the returning officer shall enter in a list (“the list of lost ballot documents”):
Constitution Page 47 of 107
(a) the name of the voter (b) the details of the unique identifier of the replacement ballot
paper, if applicable, and (c) the voter ID number of the voter.
31. Issue of replacement voting information 31.1 If a person applies for replacement voting information under rule
29 or 30 and a declaration of identity has already been received by the returning officer in the name of that voter, the returning officer may not issue replacement voting information unless, in addition to the requirements imposed by rule 29.3 or 30.2, he or she is also satisfied that that person has not already voted in the election, notwithstanding the fact that a declaration of identity if required has already been received by the returning officer in the name of that voter.
31.2 After issuing replacement voting information under this rule, the
returning officer shall enter in a list (“the list of tendered voting information”):
(a) the name of the voter, (b) the unique identifier of any replacement ballot paper issued
under this rule; (c) the voter ID number of the voter.
32. ID declaration form for replacement ballot papers (public and patient constituencies)
32.1 In respect of an election for a public or patient constituency an ID
declaration form must be issued with each replacement ballot paper requiring the voter to make a declaration of identity.
Polling by internet, telephone or text 33. Procedure for remote voting by internet 33.1 To cast his or her vote using the internet, a voter will need to gain
access to the polling website by keying in the url of the polling website provided in the voting information.
33.2 When prompted to do so, the voter will need to enter his or her
voter ID number.
33.3 If the internet voting system authenticates the voter ID number, the system will give the voter access to the polling website for the election in which the voter is eligible to vote.
Constitution Page 48 of 107
33.4 To cast his or her vote, the voter will need to key in a mark on the
screen opposite the particulars of the candidate or candidates for whom he or she wishes to cast his or her vote.
33.5 The voter will not be able to access the internet voting system for
an election once his or her vote at that election has been cast. 34. Voting procedure for remote voting by telephone 34.1 To cast his or her vote by telephone, the voter will need to gain
access to the telephone voting facility by calling the designated telephone number provided in the voter information using a telephone with a touch-tone keypad.
34.2 When prompted to do so, the voter will need to enter his or her
voter ID number using the keypad.
34.3 If the telephone voting facility authenticates the voter ID number, the voter will be prompted to vote in the election.
34.4 When prompted to do so the voter may then cast his or her vote
by keying in the numerical voting code of the candidate or candidates, for whom he or she wishes to vote.
34.5 The voter will not be able to access the telephone voting facility
for an election once his or her vote at that election has been cast. 35. Voting procedure for remote voting by text message 35.1 To cast his or her vote by text message the voter will need to
gain access to the text message voting facility by sending a text message to the designated telephone number or telephone short code provided in the voter information.
35.2 The text message sent by the voter must contain his or her voter
ID number and the numerical voting code for the candidate or candidates, for whom he or she wishes to vote.
35.3 The text message sent by the voter will need to be structured
in accordance with the instructions on how to vote contained in the voter information, otherwise the vote will not be cast.
Procedure for receipt of envelopes, internet votes, telephone votes and text message votes 36. Receipt of voting documents 36.1 Where the returning officer receives:
(a) a covering envelope, or
Constitution Page 49 of 107
(b) any other envelope containing an ID declaration form if required, a ballot paper envelope, or a ballot paper,
before the close of the poll, that officer is to open it as soon as is practicable; and rules 37 and 38 are to apply.
36.2 The returning officer may open any covering envelope or any
ballot paper envelope for the purposes of rules 37 and 38, but must make arrangements to ensure that no person obtains or communicates information as to: (a) the candidate for whom a voter has voted, or (b) the unique identifier on a ballot paper.
36.3 The returning officer must make arrangements to ensure the
safety and security of the ballot papers and other documents. 37. Validity of votes 37.1 A ballot paper shall not be taken to be duly returned unless the
returning officer is satisfied that it has been received by the returning officer before the close of the poll, with an ID declaration form if required that has been correctly completed, signed and dated.
37.2 Where the returning officer is satisfied that rule 37.1 has been
fulfilled, he or she is to:
(a) put the ID declaration form if required in a separate packet, and
(b) put the ballot paper aside for counting after the close of the poll.
37.3 Where the returning officer is not satisfied that rule 37.1 has been
fulfilled, he or she is to:
(a) mark the ballot paper “disqualified”, (b) if there is an ID declaration form accompanying the ballot
paper, mark it “disqualified” and attach it to the ballot paper, (c) record the unique identifier on the ballot paper in a list of
disqualified documents (the “list of disqualified documents”); and
(d) place the document or documents in a separate packet.
37.4 An internet, telephone or text message vote shall not be taken to be duly returned unless the returning officer is satisfied that the internet voting record, telephone voting record or text voting record (as applicable) has been received by the returning officer before the close of the poll, with a declaration of identity if
Constitution Page 50 of 107

required that has been correctly made.
37.5 Where the returning officer is satisfied that rule 37.4 has been fulfilled, he or she is to put the internet voting record, telephone voting record or text voting record (as applicable) aside for counting after the close of the poll.
37.6 Where the returning officer is not satisfied that rule 37.4 has been
fulfilled, he or she is to:
(a) mark the internet voting record, telephone voting record or text voting record (as applicable) “disqualified”,
(b) record the voter ID number on the internet voting record, telephone voting record or text voting record (as applicable) in the list of disqualified documents; and
(c) place the document or documents in a separate packet.
38. Declaration of identity but no ballot paper (public and patient constituency)1
38.1 Where the returning officer receives an ID declaration form if
required but no ballot paper, the returning officer is to: (a) mark the ID declaration form “disqualified”,
(b) record the name of the voter in the list of disqualified documents, indicating that a declaration of identity was received from the voter without a ballot paper, and
(c) place the ID declaration form in a separate packet.
39. De-duplication of votes 39.1 Where different methods of polling are being used in an election,
the returning officer shall examine all votes cast to ascertain if a voter ID number has been used more than once to cast a vote in the election.
39.2 If the returning officer ascertains that a voter ID number has been
used more than once to cast a vote in the election he or she shall:
(a) only accept as duly returned the first vote received that was
cast using the relevant voter ID number; and (b) mark as “disqualified” all other votes that were cast using
the relevant voter ID number
1 It should not be possible, technically, to make a declaration of identity electronically without also submitting a vote.
Constitution Page 51 of 107

39.3 Where a ballot paper is disqualified under this rule the returning
officer shall:
(a) mark the ballot paper “disqualified”, (b) if there is an ID declaration form accompanying the ballot
paper, mark it “disqualified” and attach it to the ballot paper, (c) record the unique identifier and the voter ID number on the
ballot paper in the list of disqualified documents; (d) place the document or documents in a separate packet; and (e) disregard the ballot paper when counting the votes in
accordance with these rules. 39.4 Where an internet voting record, telephone voting record or text
voting record is disqualified under this rule the returning officer shall:
(a) mark the internet voting record, telephone voting record or
text voting record (as applicable) “disqualified”, (b) record the voter ID number on the internet voting record,
telephone voting record or text voting record (as applicable) in the list of disqualified documents;
(c) place the internet voting record, telephone voting record or text voting record (as applicable) in a separate packet, and
(d) disregard the internet voting record, telephone voting record or text voting record (as applicable) when counting the votes in accordance with these rules.
40. Sealing of packets 40.1 As soon as is possible after the close of the poll and after the
completion of the procedure under rules 37 and 38, the returning officer is to seal the packets containing:
(a) the disqualified documents, together with the list of
disqualified documents inside it, (b) the ID declaration forms, if required, (c) the list of spoilt ballot papers and the list of spoilt text
message votes, (d) the list of lost ballot documents, (e) the list of eligible voters, and (f) the list of tendered voting information and ensure that complete electronic copies of the internet voting records, telephone voting records and text voting records created
Constitution Page 52 of 107
in accordance with rule 26 are held in a device suitable for the purpose of storage.
PART 6: COUNTING THE VOTES
41. Arrangements for counting of the votes 41.1 The returning officer is to make arrangements for counting the
votes as soon as is practicable after the close of the poll.
41.2 The returning officer may make arrangements for any votes to be counted using vote counting software where:
(a) the board of directors and the Council of Governors of the
corporation have approved: (i) the use of such software for the purpose of counting
votes in the relevant election, and
(ii) a policy governing the use of such software, and
(b) the corporation and the returning officer are satisfied that the use of such software will produce an accurate result.
42. The count 42.1 The returning officer is to:
(a) count and record the number of: (iii) ballot papers that have been returned; and
(iv) the number of internet voting records, telephone voting records and/or text voting records that have been created, and
(b) count the votes according to the provisions in this Part of the rules and/or the provisions of any policy approved pursuant to rule 41.2(ii) where vote counting software is being used.
42.2 The returning officer, while counting and recording the number of
ballot papers, internet voting records, telephone voting records and/or text voting records and counting the votes, must make arrangements to ensure that no person obtains or communicates information as to the unique identifier on a ballot paper or the voter ID number on an internet voting record, telephone voting record or text voting record.
42.3 The returning officer is to proceed continuously with counting the
votes as far as is practicable.
Deleted: c
Deleted: g
Constitution Page 53 of 107
43. Rejected ballot papers and rejected text voting records 43.1 Any ballot paper:
(a) which does not bear the features that have been incorporated into the other ballot papers to prevent them from being reproduced,
(b) on which votes are given for more candidates than the voter is entitled to vote,
(c) on which anything is written or marked by which the voter can be identified except the unique identifier, or
(d) which is unmarked or rejected because of uncertainty,
shall, subject to rules 43.2 and 43.3, be rejected and not counted. 43.2 Where the voter is entitled to vote for more than one candidate, a
ballot paper is not to be rejected because of uncertainty in respect of any vote where no uncertainty arises, and that vote is to be counted.
43.3 A ballot paper on which a vote is marked:
(a) elsewhere than in the proper place, (b) otherwise than by means of a clear mark, (c) by more than one mark,
is not to be rejected for such reason (either wholly or in respect of that vote) if an intention that the vote shall be for one or other of the candidates clearly appears, and the way the paper is marked does not itself identify the voter and it is not shown that he or she can be identified by it.
43.4 The returning officer is to:
(a) endorse the word “rejected” on any ballot paper which under this rule is not to be counted, and
(b) in the case of a ballot paper on which any vote is counted under rules 43.2 and 43.3, endorse the words “rejected in part” on the ballot paper and indicate which vote or votes have been counted.
43.5 The returning officer is to draw up a statement showing the
number of rejected ballot papers under the following headings:
(a) does not bear proper features that have been incorporated into the ballot paper,
(b) voting for more candidates than the voter is entitled to,
Constitution Page 54 of 107
(c) writing or mark by which voter could be identified, and (d) unmarked or rejected because of uncertainty,
and, where applicable, each heading must record the number of ballot papers rejected in part.
43.6 Any text voting record: (a) on which votes are given for more candidates than the voter
is entitled to vote, (b) on which anything is written or marked by which the voter
can be identified except the voter ID number, or (c) which is unmarked or rejected because of uncertainty,
shall, subject to rules 43.7 and 43.8, be rejected and not counted.
43.7 Where the voter is entitled to vote for more than one candidate, a
text voting record is not to be rejected because of uncertainty in respect of any vote where no uncertainty arises, and that vote is to be counted.
43.8 A text voting record on which a vote is marked:
(a) otherwise than by means of a clear mark, (b) by more than one mark,
is not to be rejected for such reason (either wholly or in respect of that vote) if an intention that the vote shall be for one or other of the candidates clearly appears, and the way the text voting record is marked does not itself identify the voter and it is not shown that he or she can be identified by it.
43.9 The returning officer is to:
(a) endorse the word “rejected” on any text voting record which under this rule is not to be counted, and
(b) in the case of a text voting record on which any vote is counted under rules 43.7 and 43.8, endorse the words “rejected in part” on the text voting record and indicate which vote or votes have been counted.
43.10 The returning officer is to draw up a statement showing the
number of rejected text voting records under the following headings:
(a) voting for more candidates than the voter is entitled to, (b) writing or mark by which voter could be identified, and
Constitution Page 55 of 107
(c) unmarked or rejected because of uncertainty,
and, where applicable, each heading must record the number of text voting records rejected in part.
44. Equality of votes 44.1 Where, after the counting of votes is completed, an equality of
votes is found to exist between any candidates and the addition of a vote would entitle any of those candidates to be declared elected, the returning officer is to decide between those candidates by a lot, and proceed as if the candidate on whom the lot falls had received an additional vote.
PART 7: FINAL PROCEEDINGS IN CONTESTED AND UNCONTESTED
ELECTIONS 45. Declaration of result for contested elections 45.1 In a contested election, when the result of the poll has been
ascertained, the returning officer is to:
(a) declare the candidate or candidates whom more votes have been given than for the other candidates, up to the number of vacancies to be filled on the Council of Governors from the constituency, or class within a constituency, for which the election is being held to be elected,
(b) give notice of the name of each candidate who he or she has declared elected: (i) where the election is held under a proposed
constitution pursuant to powers conferred on the [insert name] NHS Trust by section 33(4) of the 2006 Act, to the Chairperson of the NHS Trust, or
(ii) in any other case, to the Chairperson of the corporation; and
(c) give public notice of the name of each candidate whom he or she has declared elected.
45.2 The returning officer is to make:
(a) the total number of votes given for each candidate (whether elected or not), and
(b) the number of rejected ballot papers under each of the headings in rule 43.5,
(c) the number of rejected text voting records under each of the headings in rule 43.10,
Deleted: c
Deleted: g
Constitution Page 56 of 107

available on request.
46. Declaration of result for uncontested elections 46.1 In an uncontested election, the returning officer is to as soon as is
practicable after final day for the delivery of notices of withdrawals by candidates from the election:
(a) declare the candidate or candidates remaining validly
nominated to be elected, (b) give notice of the name of each candidate who he or she
has declared elected to the Chairperson of the corporation, and
(c) give public notice of the name of each candidate who he or
she has declared elected. PART 8: DISPOSAL OF DOCUMENTS 47. Sealing up of documents relating to the poll
47.1 On completion of the counting at a contested election, the returning officer is to seal up the following documents in separate packets:
(a) the counted ballot papers, internet voting records, telephone
voting records and text voting records, (b) the ballot papers and text voting records endorsed with
“rejected in part”, (c) the rejected ballot papers and text voting records, and (d) the statement of rejected ballot papers and the statement of
rejected text voting records, and ensure that complete electronic copies of the internet voting records, telephone voting records and text voting records created in accordance with rule 26 are held in a device suitable for the purpose of storage.
47.2 The returning officer must not open the sealed packets of:
(a) the disqualified documents, with the list of disqualified documents inside it,
(b) the list of spoilt ballot papers and the list of spoilt text message votes,
(c) the list of lost ballot documents, and
Constitution Page 57 of 107
(d) the list of eligible voters, or access the complete electronic copies of the internet voting records, telephone voting records and text voting records created in accordance with rule 26 and held in a device suitable for the purpose of storage.
47.3 The returning officer must endorse on each packet a description
of:
(a) its contents, (b) the date of the publication of notice of the election, (c) the name of the corporation to which the election relates,
and (d) the constituency, or class within a constituency, to which the
election relates. 48. Delivery of documents 48.1 Once the documents relating to the poll have been sealed up and
endorsed pursuant to rule 49, the returning officer is to forward them to the chair of the corporation.
49. Forwarding of documents received after close of the poll 49.1 Where:
(a) any voting documents are received by the returning officer after the close of the poll, or
(b) any envelopes addressed to eligible voters are returned as undelivered too late to be resent, or
(c) any applications for replacement voting information are made too late to enable new voting information to be issued,
the returning officer is to put them in a separate packet, seal it up, and endorse and forward it to the Chairperson of the corporation.
50. Retention and public inspection of documents 50.1 The corporation is to retain the documents relating to an election
that are forwarded to the chair by the returning officer under these rules for one year, and then, unless otherwise directed by the board of directors of the corporation, cause them to be destroyed.
50.2 With the exception of the documents listed in rule 51.1, the
documents relating to an election that are held by the corporation shall be available for inspection by members of the public at all reasonable times.
Constitution Page 58 of 107
50.3 A person may request a copy or extract from the documents
relating to an election that are held by the corporation, and the corporation is to provide it, and may impose a reasonable charge for doing so.
51. Application for inspection of certain documents relating to an
election 51.1 The corporation may not allow:
(a) the inspection of, or the opening of any sealed packet containing – (i) any rejected ballot papers, including ballot papers
rejected in part,
(ii) any rejected text voting records, including text voting records rejected in part,
(iii) any disqualified documents, or the list of disqualified documents,
(iv) any counted ballot papers, internet voting records, telephone voting records or text voting records, or
(v) the list of eligible voters, or
(b) access to or the inspection of the complete electronic copies of the internet voting records, telephone voting records and text voting records created in accordance with rule 26 and held in a device suitable for the purpose of storage,
by any person without the consent of the board of directors of the corporation.
51.2 A person may apply to the board of directors of the corporation to
inspect any of the documents listed in rule 51.1, and the board of directors of the corporation may only consent to such inspection if it is satisfied that it is necessary for the purpose of questioning an election pursuant to Part 11.
51.3 The board of directors of the corporation’s consent may be on
any terms or conditions that it thinks necessary, including conditions as to –
(a) persons, (b) time, (c) place and mode of inspection, (d) production or opening,
Constitution Page 59 of 107

and the corporation must only make the documents available for inspection in accordance with those terms and conditions.
51.4 On an application to inspect any of the documents listed in rule
51.1 the board of directors of the corporation must:
(a) in giving its consent, and (b) in making the documents available for inspection ensure that the way in which the vote of any particular member has been given shall not be disclosed, until it has been established –
(i) that his or her vote was given, and (ii) that Monitor has declared that the vote was invalid.
PART 9: DEATH OF A CANDIDATE DURING A CONTESTED ELECTION 52. Countermand or abandonment of poll on death of candidate 52.1 If at a contested election, proof is given to the returning officer’s
satisfaction before the result of the election is declared that one of the persons named or to be named as a candidate has died, then the returning officer is to:
(a) countermand notice of the poll, or, if voting information has
been issued, direct that the poll be abandoned within that constituency or class, and
(b) order a new election, on a date to be appointed by him or her in consultation with the corporation, within the period of 40 days, computed in accordance with rule 3 of these rules, beginning with the day that the poll was countermanded or abandoned.
52.2 Where a new election is ordered under rule 52.1, no fresh
nomination is necessary for any candidate who was validly nominated for the election where the poll was countermanded or abandoned but further candidates shall be invited for that constituency or class.
52.3 Where a poll is abandoned under rule 52.1(a), rules 52.4 to 52.7
are to apply. 52.4 The returning officer shall not take any step or further step to
open envelopes or deal with their contents in accordance with rules 38 and 39, and is to make up separate sealed packets in accordance with rule 40.
Constitution Page 60 of 107
52.5 The returning officer is to:
(a) count and record the number of ballot papers, internet voting records, telephone voting records and text voting records that have been received,
(b) seal up the ballot papers, internet voting records, telephone voting records and text voting records into packets, along with the records of the number of ballot papers, internet voting records, telephone voting records and text voting records and
ensure that complete electronic copies of the internet voting records telephone voting records and text voting records created in accordance with rule 26 are held in a device suitable for the purpose of storage.
52.6 The returning officer is to endorse on each packet a description of:
(a) its contents, (b) the date of the publication of notice of the election, (c) the name of the corporation to which the election relates,
and (d) the constituency, or class within a constituency, to which the
election relates. 52.7 Once the documents relating to the poll have been sealed up and
endorsed pursuant to rules 52.4 to 52.6, the returning officer is to deliver them to the Chairperson of the corporation, and rules 49 and 50 are to apply.
PART 10: ELECTION EXPENSES AND PUBLICITY Election expenses 53. Election expenses 53.1 Any expenses incurred, or payments made, for the purposes of
an election which contravene this Part are an electoral irregularity, which may only be questioned in an application made to Monitor under Part 11 of these rules.
54. Expenses and payments by candidates 54.1 A candidate may not incur any expenses or make a payment (of
whatever nature) for the purposes of an election, other than expenses or payments that relate to:
Constitution Page 61 of 107

(a) personal expenses, (b) travelling expenses, and expenses incurred while living
away from home, and (c) expenses for stationery, postage, telephone, internet (or any
similar means of communication) and other petty expenses, to a limit of £100.
55. Election expenses incurred by other persons 55.1 No person may:
(a) incur any expenses or make a payment (of whatever nature) for the purposes of a candidate’s election, whether on that candidate’s behalf or otherwise, or
(b) give a candidate or his or her family any money or property (whether as a gift, donation, loan, or otherwise) to meet or contribute to expenses incurred by or on behalf of the candidate for the purposes of an election.
55.2 Nothing in this rule is to prevent the corporation from incurring
such expenses, and making such payments, as it considers necessary pursuant to rules 56 and 57.
Publicity
56. Publicity about election by the corporation 56.1 The corporation may:
(a) compile and distribute such information about the candidates, and
(b) organise and hold such meetings to enable the candidates to speak and respond to questions,
as it considers necessary.
56.2 Any information provided by the corporation about the
candidates, including information compiled by the corporation under rule 57, must be:
(a) objective, balanced and fair, (b) equivalent in size and content for all candidates, (c) compiled and distributed in consultation with all of the
candidates standing for election, and (d) must not seek to promote or procure the election of a
specific candidate or candidates, at the expense of the electoral prospects of one or more other candidates.
Constitution Page 62 of 107

56.3 Where the corporation proposes to hold a meeting to enable the
candidates to speak, the corporation must ensure that all of the candidates are invited to attend, and in organising and holding such a meeting, the corporation must not seek to promote or procure the election of a specific candidate or candidates at the expense of the electoral prospects of one or more other candidates.
57. Information about candidates for inclusion with voting information 57.1 The corporation must compile information about the candidates
standing for election, to be distributed by the returning officer pursuant to rule 24 of these rules.
57.2 The information must consist of:
(a) a statement submitted by the candidate of no more than 250 words,
(b) if voting by telephone or text message is a method of polling for the election, the numerical voting code allocated by the returning officer to each candidate, for the purpose of recording votes using the telephone voting facility or the text message voting facility (“numerical voting code”), and a photograph of the candidate.
58. Meaning of “for the purposes of an election” 58.1 In this Part, the phrase “for the purposes of an election” means
with a view to, or otherwise in connection with, promoting or procuring a candidate’s election, including the prejudicing of another candidate’s electoral prospects; and the phrase “for the purposes of a candidate’s election” is to be construed accordingly.
58.2 The provision by any individual of his or her own services
voluntarily, on his or her own time, and free of charge is not to be considered an expense for the purposes of this Part.
PART 11: QUESTIONING ELECTIONS AND THE CONSEQUENCE OF
IRREGULARITIES 59. Application to question an election 59.1 An application alleging a breach of these rules, including an
electoral irregularity under Part 10, may be made to Monitor for the purpose of seeking a referral to the independent election
Constitution Page 63 of 107
arbitration panel (IEAP). 59.2 An application may only be made once the outcome of the
election has been declared by the returning officer. 59.3 An application may only be made to Monitor by:
(a) a person who voted at the election or who claimed to have had the right to vote, or
(b) a candidate, or a person claiming to have had a right to be elected at the election.
59.4 The application must:
(a) describe the alleged breach of the rules or electoral irregularity, and
(b) be in such a form as the independent panel may require. 59.5 The application must be presented in writing within 21 days of the
declaration of the result of the election. Monitor will refer the application to the independent election arbitration panel appointed by Monitor.
59.6 If the independent election arbitration panel requests further
information from the applicant, then that person must provide it as soon as is reasonably practicable.
59.7 Monitor shall delegate the determination of an application to a
person or panel of persons to be nominated for the purpose. 59.8 The determination by the IEAP shall be binding on and shall be
given effect by the corporation, the applicant and the members of the constituency (or class within a constituency) including all the candidates for the election to which the application relates.
59.9 The IEAP may prescribe rules of procedure for the determination
of an application including costs. PART 12: MISCELLANEOUS 60. Secrecy 60.1 The following persons:
(a) the returning officer, (b) the returning officer’s staff,
must maintain and aid in maintaining the secrecy of the voting
Constitution Page 64 of 107
and the counting of the votes, and must not, except for some purpose authorised by law, communicate to any person any information as to:
(i) the name of any member of the corporation who has or has
not been given voting information or who has or has not voted,
(ii) the unique identifier on any ballot paper, (iii) the voter ID number allocated to any voter, (iv) the candidate(s) for whom any member has voted.
60.2 No person may obtain or attempt to obtain information as to the
candidate(s) for whom a voter is about to vote or has voted, or communicate such information to any person at any time, including the unique identifier on a ballot paper given to a voter or the voter ID number allocated to a voter.
60.3 The returning officer is to make such arrangements as he or she
thinks fit to ensure that the individuals who are affected by this provision are aware of the duties it imposes.
61. Prohibition of disclosure of vote 61.1 No person who has voted at an election shall, in any legal or
other proceedings to question the election, be required to state for whom he or she has voted.
62. Disqualification 62.1 A person may not be appointed as a returning officer, or as staff
of the returning officer pursuant to these rules, if that person is:
(a) a member of the corporation, (b) an employee of the corporation, (c) a director of the corporation, or (d) employed by or on behalf of a person who has been
nominated for election. 63. Delay in postal service through industrial action or
unforeseen event 63.1 If industrial action, or some other unforeseen event, results in a
delay in:
(a) the delivery of the documents in rule 24, or (b) the return of the ballot papers,
Constitution Page 65 of 107

the returning officer may extend the time between the publication of the notice of the poll and the close of the poll by such period as he or she considers appropriate.
Constitution Page 66 of 107

ANNEX 5 – ADDITIONAL PROVISIONS – COUNCIL OF GOVERNORS (Paragraph 22)
1. Eligibility to be on the Council of Governors 1.1. A person may not become or continue as a governor, and if already
holding such office will immediately cease to do so if:
1.1.1. any of the grounds contained in paragraph 15 of the Constitution apply to him;
1.1.2. they are under 18 years of age;
1.1.3. they are a Director of the Trust, or a governor or director of
another NHS Body or of an independent/private sector healthcare provider. These restrictions do not apply to Appointed Governors;
1.1.4. they are the spouse, Partner, parent or child of a member of the
Board of Directors;
1.1.5. being a member of the Public Constituency, they refuse to sign a declaration in the form specified by the Secretary of particulars of their qualification to vote as a member of the Trust, and that they are not prevented from being a member of the Council of Governors;
1.1.6. they are subject to a sex offender order;
1.1.7. they are subject to an unexpired disqualification order made
under the Company Directors Disqualification Act 1986;
1.1.8. they have within the preceding two years been lawfully dismissed, otherwise than by reason of redundancy, from any paid employment with an NHS Body;
1.1.9. they are a person whose tenure of office as the Chairperson or
as a member or director of an NHS Body has been terminated on the grounds that their appointment is not in the interests of the NHS, for non-attendance at meetings, or for non-disclosure of a pecuniary interest;
1.1.10. they have had their name removed from any list maintained
by health and care professional bodies in the UK, and have not subsequently had their name included on such a list;
1.1.11. they have previously been expelled as a governor of a
foundation trust in the previous nine years.
Deleted: G
Constitution Page 67 of 107

2. Disqualification as a Governor 2.1. A person holding office as a governor shall immediately cease to do so
if: 2.1.1. they cease to fulfil the requirements of paragraph 1 above;
2.1.2. they resign by notice in writing to the Secretary;
2.1.3. they fail to attend two consecutive meetings of the Council of
Governors, unless the Council of Governors is satisfied that:
2.1.3.1. the absences were due to reasonable causes; and 2.1.3.2. they will be able to start attending meetings of the
Council of Governors again within such a periods as is considered reasonable by the Council of Governors;
2.1.4. in the case of an Elected Governor, they cease to be a member
of the constituency or class of constituency by which they were elected;
2.1.5. in the case of an Appointed Governor, the Appointing
Organisation terminates the appointment or the Appointing Organisation ceases to exist;
2.1.6. they have refused without reasonable cause to undertake any
training which the Council of Governors requires all governors to undertake;
2.1.7. they have failed to sign and deliver to the Secretary a statement
in the form required by the Secretary confirming acceptance of the code of conduct for governors;
2.1.8. they are removed from the Council of Governors pursuant to
paragraph 3 below
2.2. The process for disqualification of a governor is set out in paragraph 6.1 of the Council of Governor's Standing Orders (Annex 6).
3. Removal as a Governor
3.1. A governor may be removed from the Council of Governors by a
resolution approved by not less than three-quarters of the remaining governors present and voting at a meeting of the Council of Governors on the grounds that: 3.1.1. they have committed a serious breach of the code of conduct for
governors;
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Deleted: G
Constitution Page 68 of 107
3.1.2. they have acted in a manner detrimental to the interests of the Trust; and
3.1.3. the Council of Governors consider that it is not in the best
interests of the Trust for them to continue as a governor.
3.2. The process for removing a governor from office is set out in paragraph 6.2 of the Council of Governor's Standing Orders (Annex 6).
4. Roles and responsibilities of the Council of Governors 4.1. The roles and responsibilities of the Council of Governors, which are to
be carried out in accordance with this Constitution are to: 4.1.1. carry out in the general duties of the Council of Governors as set
out in paragraph 16 of the Constitution;
4.1.2. appoint or remove the Chairperson and the other Non-Executive Directors;
4.1.3. approve an appointment (by the Non-Executive Directors) of the
Chief Executive;
4.1.4. decide the remuneration and allowances and the other terms and conditions of office of the Non-Executive Directors;
4.1.5. appoint or remove the Trust's Auditor;
4.1.6. be presented with the annual accounts, any report of the Auditor
on them and the annual report;
4.1.7. approve the application for any merger, acquisition, separation, dissolution or the entering into of any significant transaction by the Trust;
4.1.8. approve changes to the Constitution;
4.1.9. vote on whether to approve the referral of a question to any
Panel appointed by Monitor as to whether the Trust has failed or is failing to act in accordance with this Constitution or to act in accordance with provision made by or under Chapter 5 of the 2006 Act;
4.1.10. require one or more of the Directors to attend a general
meeting of the Council of Governors for the purpose of obtaining information about the Trust's performance of its functions or the Directors' performance of their duties;
4.1.11. decide whether to propose a vote on the Trust's or Directors'
performance;
Deleted: G
Deleted: G
Constitution Page 69 of 107
4.1.12. provide their views to the Board of Directors when the Board
of Directors is preparing any document containing information about the Trust's forward planning;
4.1.13. determine whether it is satisfied that the carrying on of
activities other than the provision of goods and services for the purposes of the health service in England proposed in the forward plan will not to any significant extent interfere with the fulfilment by the Trust of its principal purpose or the performance of its other functions;
4.1.14. approve the implementation of any increase of 5% or more in
the proportion of the Trust's total income in any Financial Year attributable to activities other than the provision of goods and services for the purposes of the health service in England;
4.1.15. respond as appropriate when consulted by the Board of
Directors in accordance with this Constitution;
4.1.16. undertake such functions as the Board of Directors may from time to time request;
4.1.17. prepare and from time to time review the Trust's membership
strategy, and its policies for the composition of the Council of Governors and Non-Executive Directors, and when appropriate, to make recommendations;
4.1.18. to approve and from time to time (and at least every three
years) review the Trust's membership strategy and its policy for the composition of the Council of Governors;
4.1.19. to consider disputes as to membership referred to them; and
4.1.20. exercise such other powers and to discharge such other
duties as may be conferred on the Council of Governors under this Constitution and the 2006 Act.
5. Governors vacancies
5.1. Where a vacancy arises on the Council of Governors for any reason
other than expiry of term of office, the following provisions will apply:
5.1.1. Where the vacancy arises amongst the Appointed Governors, the Secretary shall request that the Appointing Organisation appoints a replacement to hold office for the remainder of the term of office.
5.1.2. If the term of office of an Elected Governor is terminated before
it expires, the Council of Governors shall be at liberty either:
Constitution Page 70 of 107

5.1.2.1. to call an election within three months to fill the seat for
the remainder of that term of office; or 5.1.2.2. to invite the next highest polling candidate for that seat
at the most recent election, who is willing to take office to fill the seat for any unexpired period of the term of office or;
5.1.2.3. Carry the vacancy.
6. Remuneration of Governors
6.1. Governors are not to receive remuneration.
Constitution Page 71 of 107

ANNEX 6
STANDING ORDERS - COUNCIL OF GOVERNORS
Constitution Page 72 of 107

This document provides a regulatory and business framework for the conduct of the Council of Governors.
1. INTERPRETATION AND DEFINITIONS
1.1 Save as otherwise permitted by law and subject to the Constitution, at any Council of Governors' meeting the Chairperson’s interpretation of these Standing Orders (on which he should be advised by the Chief Executive or Secretary) shall be final.
1.2 Unless a contrary intention is evident or the context otherwise requires,
the provisions relating to Interpretation and Definitions in paragraph 1 of the Constitution shall apply and the words or expressions contained in these Standing Orders shall bear the same meaning.
1.3 In these Standing Orders the following defined terms shall have the
specific meanings given to them below:
Chairperson means the Chairperson of the Trust. Lead Governor means one (1) governor appointed by the Council of
Governors to lead the Council of Governors and to communicate directly with Monitor in certain circumstances.
Officer means employee of the Trust or any other person holding a
paid appointment or office with the Trust. Secretary means the Trust Secretary or officer to whom he has
delegated this duty.
SFIs means Standing Financial Instructions. SOs means these Standing Orders of the Council of Governors.
2. MEETINGS OF THE COUNCIL OF GOVERNORS
2.1 Admission of the Public
The meetings of the Council of Governors shall be open to members of the public except when the Council of Governors decides otherwise in relation to all or part of a meeting for reasons of commercial confidentiality or on other proper grounds. The Chairperson may exclude any member of the public from a meeting of the Council of Governors if they are interfering with or preventing the proper conduct of the meeting.
Deleted: G
Constitution Page 73 of 107

2.2 Chairperson of the Meeting
At any meeting of the Council of Governors, the Chairperson, if present, shall preside. If the Chairperson is absent from the meeting or is absent temporarily on the grounds of a declared conflict of interest the Vice-Chairperson shall preside. If the Chairperson and Vice-Chairperson are absent from the meeting or absent temporarily on the grounds of a declared conflict of interest, such Non-Executive Director as the governors present shall choose shall preside. If the person presiding has a conflict of interest in relation to the business being discussed the Lead Governor will chair that part of the meeting.
2.3 Calling Meetings
2.3.1 The Council of Governors will meet at least four times in each financial year. Save in the case of emergencies or the need to conduct urgent business, the Secretary shall give at least 14 days’ written notice of the date and place of every meeting of the Council of Governors to all governors. Notice will also be published on the Trust’s website and in other locations and media as considered appropriate. Seminars, workshops or similar events involving governors are not to be treated as meetings of the Council of Governors.
2.3.2 Meetings of the Council of Governors are called by the
Secretary or by the Chairperson or by ten governors (including at least two Public or Staff Governors and two Appointed Governors) who give written notice to the Secretary specifying the business to be carried out. The Secretary shall send a written notice to all governors as soon as possible after receipt of such a request. The Secretary shall call a meeting within at least fourteen but not more than 28 days to discuss the specified business. If the Secretary fails to call such a meeting, within seven clear days, then the Chairperson or ten governors, whichever is the case, shall call such a meeting.
2.3.3 Subject to SO 2.3.4 below, lack of service of the notice of the
business of the meeting on any governor shall not affect the validity of a meeting.
2.3.4 Failure to serve such a notice on more than half of the governors
will invalidate the meeting. A notice shall be presumed to have been served at the time at which the notice would be delivered in the ordinary course of the post or, where the notice is sent by email, at the time at which the email is sent.
2.3.5 In the case of a meeting being called by ten governors in default
of the Secretary or Chairperson, the notice shall be signed by those members of the Council of Governors and no business
Deleted: G
Deleted: F
Deleted: Y
Deleted: G
Constitution Page 74 of 107
shall be transacted at the meeting other than that specified in the notice.
2.4 Agenda of Meetings and Motions on Notice
2.4.1 Agendas and supporting papers will normally be issued to arrive with governors no later than seven days in advance of the meeting. Draft minutes of the previous meeting will be circulated with these papers for approval as a specific agenda item.
2.4.2 A governor desiring a matter to be included on an agenda
including a formal proposition for discussion and voting on at a meeting shall make his request in writing to the Secretary at least 21 clear days before the meeting. The request should state whether the item of business is proposed to be transacted in the presence of the public and should include appropriate supporting information. Requests made less than 21 clear days before a meeting may be included on the agenda at the discretion of the Chairperson. Receipt of such matters via electronic means is acceptable.
2.4.3 Motions for which notice has been given will be listed on the
agenda unless the governor giving notice states, in writing, that they propose to move it to a later meeting or withdraw it.
2.4.4 Motions must be about matters for which the Council of
Governors has a responsibility or which affect the area covered by the Trust.
2.4.5 There will not be an agenda item entitled ‘Any Other Business’.
See Standing Order 2.4.2 for inclusion of agenda items. Instead, there will be an item for Questions on Notice, which is subject to Standing Order 2.7 below.
2.5 Motions without Notice
2.5.1 The following motions may be moved without notice:
(a) To change the order of business on the agenda (b) To refer a matter to an appropriate body or individual (c) To appoint a working group arising from an item on the agenda
for the meeting (d) To receive reports or adopt recommendations made by the
Board of Directors (e) To withdraw a motion (f) To amend a motion (g) To proceed to the next business (h) That the question now be put (i) To adjourn a debate
Constitution Page 75 of 107
(j) To adjourn a meeting (k) To suspend a particular Standing Order; see Standing Order 7.1
for further details. (l) To not hear further a governor, or to exclude them from the
meeting. If a governor persistently disregards the ruling of the Chairperson by behaving improperly or offensively or deliberately obstructs business, the Chairperson may move that the governor not be heard further. If seconded, the motion will be voted on without discussion. If the governor continues to behave improperly after such a motion is carried the Chairperson may move that the governor leaves the meeting room or that the meeting is adjourned for a specified period. If seconded, the motion will be voted on without discussion.
(m) To give consent of the Council where its consent is required by the Constitution.
2.6 Voting/Decision-Making
2.6.1 Save as provided otherwise in the Constitution, and/or the 2006
Act and/or the 2012 Act, and these Standing Orders, questions arising at a meeting of the Council of Governors shall be decided by a majority of votes of those present (in person) and voting.
2.6.2 Where a vote or approval of the Council of Governors is required
pursuant to sections 37 (Amendments of constitution), 39A (Panel for advising governors), 43(3D) (Authorised services), 51A (Significant transactions), 56 (Mergers), 56A (Acquisitions), 56B (Separations) or 57A (Dissolutions) of the 2006 Act, a governor entitled to attend and vote at the meeting of the Council of Governors may appoint the Chairperson, or anyone else presiding at the meeting or another governor as his proxy to attend and, on a paper ballot, to vote at the meeting on his behalf. Proxies validly appointed in accordance with these Standing Orders shall be deemed to be present at the meeting of the Council of Governors in determining the required majority on any vote in respect of which a proxy may be appointed.
2.6.3 The governor appointing a proxy may direct the proxy how to
vote at the meeting or may allow the proxy to choose how to vote. A governor appointing a proxy may revoke the proxy by delivering a notice in writing to the Secretary before the start of the meeting to which it relates or by attending the meeting in person.
2.6.4 The form for appointing a proxy shall be in writing, signed by the
governor appointing the proxy and made in such form and include such declarations as the Council of Governors may from time to time determine. Any proxy appointed not using the agreed form shall be invalid. The signed form appointing a proxy must be received by the Secretary not less than 48 hours before
Deleted: G
Constitution Page 76 of 107
the time and date of the meeting, or adjourned meeting, and shall not be treated as valid if received after this time.
2.6.5 At a meeting of the Council of Governors a vote shall be decided
on a show of hands, the result being declared by the Chairperson and recorded in the minutes. The entry in the minutes shall confirm the result without recording the number or proportion in favour or against the motion unless a request is made under Standing Order 2.6.7. Every governor shall have one vote whether voting in person or by proxy. All valid proxies received for a vote at a meeting of the Council of Governors shall be declared at the meeting and recorded in the minutes regardless of whether a vote is taken by paper ballot.
2.6.6 A paper ballot may be used if a majority of the governors present
so request. A proxy shall be deemed to have the authority to join in the request for a paper ballot on behalf of the governor(s) appointing the proxy. If a paper ballot is to be used, it shall be taken at such time and place and in such a manner as the Chairperson of the meeting shall direct and the result of the ballot shall be deemed to be the resolution of the meeting at which the ballot was demanded. The demand for a ballot shall not prevent the continuance of a meeting for the transaction of any business other than the question on which a ballot has been demanded.
2.6.7 If at least one-third of the governors present so request, the
voting on any question may be recorded to show how each governor present voted or abstained.
2.6.8 In the case of an equality of votes, whether on a show of hands
or a ballot, the Chairperson shall have a second or casting vote.
2.6.9 No resolution of the Council of Governors shall be passed if it is opposed by all of the Public Governors present.
2.6.10 All decisions taken in good faith at a meeting of the Council of
Governors shall be valid even if it is discovered subsequently that there was a defect in the calling of the meeting, or the appointment of the governors attending the meeting.
2.7 Questions from Governors
2.7.1 A governor may ask any question through the Chairperson
without notice upon a report from an Executive Director or other Officer of the Trust when that item is being received or under consideration by the Council of Governors.
2.7.2 Questions relating to matters other than those under report may
be asked with due notice. For the avoidance of confusion,
Deleted: G
Constitution Page 77 of 107

questions on notice must be given in writing (including email) to the Secretary at least 14 days in advance of the meeting. If the question is urgent and with the agreement of the person to whom the question is to be put, the content of the question may be given to the Secretary by 10.00 a.m. on the day of the meeting (if the meeting is scheduled for the afternoon) or by 2.00 p.m. on the preceding day (if the meeting is scheduled for the morning). Urgent is defined as a matter that will adversely affect the Trust in the next seven days.
2.8 Chairperson’s Ruling
Statements of members of the Council of Governors made at meetings of the Council of Governors shall be relevant to the matter under discussion at the material time and the decision of the Chairperson of the meeting on questions of order, relevancy, regularity and any other matters shall be final.
2.9 Attendance
The names of the Chairperson and governors present at the meeting shall be recorded in the minutes. Governors who are unable to attend the Council of Governors meeting should advise the Secretary in advance so that their apologies may be recorded.
2.10 Quorum
2.10.1 No business shall be transacted at a meeting unless at least
twelve governors are present in person, which must include at least four Public Governors and one Staff Governor.
2.10.2 If at any meeting there is no quorum present within 30 minutes
of the time fixed for the start of the meeting the meeting will stand adjourned for five clear days and upon reconvening those present shall constitute a quorum.
2.10.3 If the Chairperson or any governor has been disqualified from
participating in the discussion on any matter and/or from voting on any resolution by reason of the declaration of a conflict of interest he shall no longer count towards the quorum. If a quorum is then not available for the discussion and/or the passing of a resolution on any matter, that matter may not be discussed further or voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting. The meeting must then proceed to the next business.
2.11 Minutes
2.11.1 The minutes of the proceedings of a meeting shall be prepared
and submitted to be read and for agreement at the next meeting
Deleted: G
Constitution Page 78 of 107
of the Council of Governors where they will be considered to have been signed by the person presiding at it. The approved minutes will be conclusive evidence of the events of the meeting and retained in an electronic minute book held by the Trust Secretary.
2.11.2 No discussion shall take place upon the minutes, except upon
their accuracy, or where the Chairperson considers discussion appropriate. Any amendments to the minutes shall be agreed and recorded at the next meeting.
3. COMMITTEES
3.1 The Council of Governors may not delegate any of its powers to a
committee or sub-committees, but it may appoint committees to assist the Council of Governors in carrying out its functions. The Council of Governors may, through the Secretary, request that advisors assist them or any committee they appoint in carrying out its duties.
3.2 These Standing Orders, as far as they are applicable, shall apply with
appropriate alteration to meetings of any committees established by the Council of Governors.
3.2 Each committee and sub-committee shall have such terms of reference
and be subject to such conditions as the Council of Governors shall decide and shall be in accordance with any guidance issued by Monitor and any legislation or applicable guidance issued by the Secretary of State.
3.3 The Council of Governors shall establish the Non-Executive Director
Nomination and Remuneration Committee and such other committees as required to assist the Council of Governors in discharging its responsibilities.
3.4 A member of a committee shall not disclose a matter dealt with by, or
brought before, the committee without its permission until the committee shall have reported to the Council of Governors or shall otherwise have concluded on that matter.
3.5 A governor or a member of a committee shall not disclose any matter
reported to the Council of Governors or otherwise dealt with by the committee, notwithstanding that the matter has been reported or action has been concluded, if the Council of Governors or the committee shall resolve that it is confidential.
Constitution Page 79 of 107

4. DECLARATIONS OF INTERESTS AND REGISTER OF INTERESTS
4.1. Declaration of Interests
4.1.1 Any governor who has a material interest in a matter as defined below shall declare such interest to the Council of Governors via the Secretary.
4.1.2 Any governor who fails to declare any interest required to be disclosed under the preceding paragraph must permanently vacate their office if required to do so by a majority of the remaining governors.
4.1.3 Subject to the exceptions below, a material interest
is any directorship of a company;
any interest held by a governor or his spouse/partner in any firm or company or business which, in connection with the matter, is trading with the Trust, or is likely to be considered as a potential trading partner with the Trust;
any interest in an organisation providing health and social care services to the National Health Service; and
a position of authority in a charity or voluntary organisation in the field of health and social care.
4.1.4 The exceptions which shall not be treated as material interests are as follows:
shares not exceeding 2% of the total shares in issue held in any company whose shares are listed on any public exchange;
an employment contract held by Staff Governors;
a contract with their Clinical Commissioning Group held by a Partnership Governor appointed by a Clinical Commissioning Group;
an employment contract with a Local Authority held by a Local Authority Governor; and
an employment contract with a Partnership Organisation held by a Partnership Governor.
4.1.5 It is the obligation of the governor to inform the Secretary in writing within seven days of becoming aware of the existence of an interest. If a governor is in any doubt whether an interest should be disclosed, they should discuss the position with the Chairperson or Secretary
Constitution Page 80 of 107

4.1.6 A governor may not vote at a meeting of the Council of Governors unless, before attending the meeting, they have made a declaration in the form specified by the Secretary of the particulars of their qualification to vote as a member of the Trust and that they are not prevented from being a member of the Council of Governors. A governor shall be deemed to have confirmed the declaration upon attending any subsequent meeting of the Council of Governors, and every agenda for meetings of the Council of Governors will draw this to the attention of governors.
4.2 Conflict of Interest
4.2.1 During the course of a Council of Governors meeting, if a conflict of interest is disclosed the governor concerned shall withdraw from the meeting and take no further part in the matter under discussion.
4.3 Register of Interests
4.3.1 The Secretary will ensure that a register of interests is maintained to record formally the declarations of interests of governors.
4.3.2 The details on the register shall be reviewed at every meeting of
the Council of Governors.
4.3.3 The register will be available to the public on request.
4.3.4 In establishing, maintaining, updating and publicising the register, the Trust shall comply with all guidance issued from time to time by Monitor.
5. STANDARDS OF BUSINESS CONDUCT
5.1 Governors must comply with the Constitution, the Trust’s Governor Code
of Conduct, the NHS Foundation Trust Code of Governance, the requirements of the law and any guidance issued by Monitor.
5.2 Governors will confirm their agreement to adhere to the Trust’s Governor
Code of Conduct by signing a copy annually and returning it to the Secretary.
5.3 Canvassing of Directors or governors or of any members of any committee
of the Trust directly or indirectly for any appointment by the Trust shall disqualify the candidate for such appointment.
5.4 A governor shall not solicit for any person any appointment under the Trust
or recommend any person for such appointment but this Standing Order shall not preclude a governor from giving written testimonial of a candidate’s ability, experience or character for submission to the Trust.
Constitution Page 81 of 107

5.5 Informal discussions outside appointment panels or committees, whether solicited or unsolicited, should be declared to the panel or committee.
5.6 Governors will be permitted to gain access to membership data if:
5.6.1 they have explained the intended use to the Secretary;
5.6.2 the Secretary has agreed the use; and
5.6.3 they agree to keep the information secure and have regard for the Data Protection Principles.
6. SPECIAL PROVISIONS RELATING TO THE DISQUALIFICATION AND
REMOVAL OF A GOVERNOR’S TENURE
6.1 Disqualification
6.1.1 Grounds - The grounds for disqualification are as set out in paragraph 15 of the Constitution.
6.1.2 Process - Where a person has been elected or appointed to be a
governor and he becomes disqualified from office under paragraph 15 of the Constitution, he shall notify the Secretary in writing of such disqualification as soon as practicable and in any event within 14 days of first becoming aware of those matters which render him disqualified. The Secretary shall remove him from the register of the governors immediately.
6.1.3 If it comes to the notice of the Secretary that the governor is
disqualified under paragraph 15 of the Constitution, whether at the time of the governor’s appointment or later, the Secretary shall immediately declare that the individual in question is disqualified and give him notice in writing to that effect as soon as practicable and in any event within 14 days of the date of the said declaration. In the event that the governor shall dispute that he is disqualified the governor may refer the matter to the dispute resolution procedures set out in Annex 5 of this Constitution within 28 days of the date upon which the notice was given to the governor.
6.2 Removal
6.2.1 Grounds – The grounds for removal are as set out in paragraph 15 of the Constitution.
6.2.2 Process - The Chairperson shall be authorised to take such action
as may be immediately required, including but not limited to exclusion of the governor concerned so that any allegation made against a governor on any of the grounds set out in paragraph 15 of the Constitution can be investigated.
Constitution Page 82 of 107

6.2.3 Where any grounds within paragraph 15 of the Constitution are alleged, it shall be open to the Council of Governors to decide, by three-quarters of those present and voting, to lay a formal charge of non-compliance or misconduct.
6.2.4 The governor in question will be notified in writing of the
allegations. The notification will detail the specific behaviour which is considered to be detrimental to the Trust and invite him to respond. His response will be considered within a defined, appropriate and reasonable timescale.
6.2.5 The governor may be invited to address the Council of Governors
in person if the matter cannot be resolved satisfactorily through correspondence.
6.2.6 The governors, by three-quarters majority of those present and
voting can decide whether to uphold the charge of non-compliance or misconduct detrimental to the Trust. If the charge is upheld then the governor will cease to be a governor with immediate effect and the Secretary shall cause his name to be removed immediately from the register of governors.
6.2.7 The governor in question will be permitted to appeal any decision
of the Council of Governors to terminate his tenure of office made in accordance with Annex 5, Paragraph 3, in writing, within 28 days of the date upon which notice of the decision is received.
6.2.8 Any appeal of the decision of the Council of Governors to
terminate a governor’s tenure of office may be referred by the governor concerned to the dispute resolution procedures set out in Paragraph 46 of the Constitution, within 28 days of the date upon which notice in writing of the Council of Governors’ decision made in accordance with Annex 5, Paragraph 3 of the Constitution is communicated to the governor concerned.
6.2.9 A governor who has been removed in accordance with these
provisions shall not be eligible to stand for re-election to the Council of Governors for a period of nine years from the date of his removal from office or the date upon which any appeal against his removal from office is disposed of, whichever is later.
7 STANDING ORDERS
7.1 Suspension of Standing Orders
7.1.1 Except where this would contravene any statutory provision or any direction made by Monitor, any one or more of the Standing Orders may be suspended at any meeting, provided that at least two-thirds of the Council of Governors are present and that a majority of those present vote in favour of suspension.
Constitution Page 83 of 107
7.1.2 A decision to suspend Standing Orders shall be recorded in the
minutes of the meeting. 7.1.3 A separate record of matters discussed during the suspension of
Standing Orders shall be made and shall be available to the Chairperson and the members of the Council of Governors.
7.1.4 No formal business may be transacted while the Standing Orders
are suspended.
7.2 Amendment of Standing Orders
These Standing Orders may be amended only in accordance with paragraph 44 of the Constitution.
7.3 Review of Standing Orders
These Standing Orders shall be reviewed annually by the Council of Governors. The requirement for review extends to all documents having effect as if incorporated in these Standing Orders.
Constitution Page 84 of 107

ANNEX 7
STANDING ORDERS - BOARD OF DIRECTORS
Constitution Page 85 of 107

This document provides a regulatory and business framework for the conduct of the Board of Directors. 1 INTERPRETATION AND DEFINITIONS
1.1. Save as otherwise permitted by law, and subject to the Constitution, at any Board of Directors' meeting the Chairperson's interpretation of these Standing Orders (on which he should be advised by the Chief Executive or Secretary) shall be final.
1.2. Wherever the title Chief Executive, Director or other Nominated Officer is used in these Standing Orders, it should be deemed to include such other officers who have been duly authorised to represent them in their absence.
1.3. Unless a contrary intention is evident or the context otherwise requires the provisions relating to Interpretation and Definitions in paragraph 1 of the Constitution shall apply and the words or expressions contained in these Standing Orders shall bear the same meaning.
1.4. In these Standing Orders the following defined terms shall have the specific meanings given to them below:
Chief Executive or CEO shall mean the Chief Officer of the Trust. Committee shall mean a Committee appointed by the Trust. Committee Members shall be persons formally appointed by the Trust to sit on or to chair specific Committees. Director of Finance or DOF shall mean the Chief Finance Officer of the Trust. Funds Held On Trust shall mean those funds which the Trust holds at its date of incorporation, receives on distribution by statutory instrument, or chooses subsequently to accept under powers derived under section 51 of the 2006 Act. Such funds may or may not be charitable. Motion means a formal proposition to be discussed and voted on during the course of a meeting. Nominated Officer means an officer charged with the responsibility for discharging specific tasks within SOs and SFIs. Officer means an employee of the Trust or any other person holding a paid appointment or office with the Trust. SFIs means Standing Financial Instructions. SOs means these Standing Orders of the Board of Directors.
Constitution Page 86 of 107
2 THE TRUST
2.1 All business shall be conducted in the name of the Trust.
2.2 All funds received in trust shall be in the name of the Trust as corporate trustee. In relation to Funds Held On Trust, powers exercised by the Trust as corporate trustee shall be exercised separately and distinctly from those powers exercised as a Trust.
2.3 Directors acting on behalf of the Trust as a corporate trustee are acting as quasi-trustees. Accountability for charitable Funds Held On Trust is to the Charity Commission and to Monitor. Accountability for non-charitable Funds Held On Trust is only to Monitor.
2.4 The Trust has resolved that certain powers and decisions may only be exercised or made by the Board of Directors in formal session. These powers and decisions are set out in the Reservation of Powers and Scheme of Delegation of the Board of Directors.
2.5 Powers of the Vice-Chairperson - Where the Chairperson of an NHS Foundation Trust has died or has otherwise ceased to hold office or where he has been unable to perform his duties as Chairperson owing to illness, absence from England and Wales or any other cause, references to the Chairperson in these SOs shall, so long as there is no Chairperson able to perform his duties, be taken to include references to the Vice-Chairperson.
2.6 Joint Directors - Where more than one person is appointed jointly to a post in the Trust which qualifies the holder for Executive Directorship or in relation to which an Executive Director is to be appointed, those persons shall become appointed as an Executive Director jointly, and shall count for the purpose of SO 3.8.1 as one person.
3. MEETINGS OF THE BOARD OF DIRECTORS
3.1 Admission of the Public
3.1.1 The meetings of the Board of Directors shall be open to members of the public unless the Board of Directors decides otherwise in relation to all or part of the meeting for reasons of commercial confidentiality or on other proper grounds. The Chairperson may exclude any member of the public from a meeting of the Board of Directors if they are interfering with or preventing the proper conduct of the meeting.
3.2 Chairperson of the Meeting
3.2.1 At any meeting of the Trust, the Chairperson, if present, shall preside. If the Chairperson is absent from the meeting the Vice-Chairperson shall preside. If the Chairperson and Vice-Chairperson are absent such Non-Executive Director as the Directors present shall choose shall preside.
Constitution Page 87 of 107
3.2.2 If the Chairperson is absent from a meeting temporarily on the grounds of a declared conflict of interest the Vice-Chairperson, if present, shall preside. If the Chairperson and Vice-Chairperson are absent, or are disqualified from participating, such Non-Executive Director as the Directors present shall choose shall preside.
3.3 Calling Meetings
3.3.1 Ordinary meetings of the Board of Directors shall be held at such times and places as the Board of Directors may determine.
3.3.2 Meetings of the Board of Directors are called by the Secretary, or by the Chairperson, or by four Directors who give written notice to the Secretary specifying the business to be carried out. The Secretary shall send a written notice to all Directors as soon as possible after receipt of such a request. The Secretary shall call a meeting within at least 14 but not more than 28 days to discuss the specified business. If the Secretary fails to call such a meeting within seven clear days the Chairperson or four Directors, whichever is the case, shall call such a meeting.
3.3.3 Subject to Standing Order 3.3.4 below, lack of service of the notice on any Director shall not affect the validity of a meeting.
3.3.4 Failure to serve such a notice on more than three Directors will invalidate the meeting. A notice shall be presumed to have been served 48 hours after it was posted or sent or, where the notice is sent by email, at the time when the email is sent.
3.3.5 In the case of a meeting called by Directors in default of the Chairperson, the notice shall be signed by those Directors and no business shall be transacted at the meeting other than that specified in the notice.
3.4 Agenda of Meetings and Motions on Notice
3.4.1 The Trust may determine that certain matters shall appear on every agenda for a meeting of the Trust and shall be addressed prior to any other business being conducted. (Such matters may be identified within these Standing Orders or following subsequent resolution shall be listed in an Appendix to the Standing Orders.). Before holding a meeting, a copy of the agenda shall be provided to the Council of Governors.
3.4.2 A Director desiring a matter to be included on an agenda shall make his request in writing to the Chairperson at least ten clear days before the meeting, subject to Standing Order 3.3.2. Requests made less than ten days before a meeting may be included on the agenda at the discretion of the Chairperson.
3.4.3 A Director desiring to move or amend a Motion shall send a written notice thereof at least ten clear days before the meeting to the Chairperson, who shall insert in the agenda for the meeting all Motions
Constitution Page 88 of 107
so received subject to the notice being permissible under the appropriate regulations. This paragraph shall not prevent any Motion being moved during the meeting, without notice, on any business mentioned on the agenda subject to Standing Order 3.3.5.
3.4.4 A Motion or amendment once moved and seconded may be withdrawn by the proposer with the concurrence of the seconder and the consent of the Chairperson.
3.4.5 Notice of Motion to amend or rescind any resolution (or the general substance of any resolution) which has been passed within the preceding six calendar months shall bear the signature of the Director who gives it and also the signature of four other Directors. When any such Motion has been disposed of by the Board of Directors, it shall not be competent for any Director other than the Chairperson to propose a Motion to the same effect within six months; however the Chairperson may do so if he considers it appropriate.
3.4.6 The mover of a Motion shall have a right of reply at the close of any discussion on the Motion or any amendment thereto.
3.4.7 When a Motion is under discussion, or immediately prior to discussion, it shall be open to a Director to move:
• An amendment to the Motion.
• The adjournment of the discussion or the meeting.
• That the meeting proceed to the next business.*
• The appointment of an ad hoc committee to deal with a specific item of business.
• That the Motion be now put.* In the case of sub-paragraphs denoted by * above to ensure objectivity Motions may only be put by a Director who has not previously taken part in the debate.
3.4.8 No amendment to the Motion shall be admitted if, in the opinion of the Chairperson of the meeting, the amendment negates the substance of the Motion.
3.5 Voting/Decision-Making
3.5.1 Every question at a meeting shall be determined by a majority of the votes of the Directors present and voting on the question and, in the case of any equality of votes, the person presiding shall have a second or casting vote. However, no resolution shall be passed if it is opposed by all of the Non-Executive Directors or by all of the Executive Directors present.
3.5.2 All questions put to the vote shall, at the discretion of the Chairperson of
Constitution Page 89 of 107
the meeting, be determined by oral expression or by a show of hands. A paper ballot may also be used if a majority of the Directors present so request.
3.5.3 If at least one-third of the Directors present so request, the voting (other than by paper ballot) on any question may be recorded to show how each Director present voted or abstained.
3.5.4 If a Director so requests, his vote shall be recorded by name upon any vote (other than by paper ballot).
3.5.5 In no circumstances may an absent Director vote by proxy. This does not prohibit an absent Director recording their vote with the Secretary in the election of the Vice-Chairperson and Senior Independent Director. Absence is defined as being absent at the time of the vote.
3.5.6 An Officer, who has been appointed formally by the Board of Directors to act up for an Executive Director during a period of incapacity or temporarily to fill an Executive Director vacancy, shall be entitled to exercise the voting rights of the Executive Director. An Officer attending the Board of Directors to represent an Executive Director during a period of incapacity or temporary absence without formal acting up status may not exercise the voting rights of the Executive Director. An Officer’s status when attending a meeting shall be recorded in the minutes.
3.5.7 Where a post of Executive Director is shared by more than one person:
• both persons shall be entitled to attend meetings of the Trust; • either, but not both, of those persons shall be eligible to vote in the
case of agreement between them; • in the case of disagreement between them no vote should be cast; • the presence of either or both of those persons shall count as one
person for the purposes of Standing Order 3.8.1.
3.6 Chairperson's Ruling
3.6.1 Statements of Directors made at meetings of the Trust shall be relevant to the matter under discussion at the material time and the decision of the Chairperson of the meeting on questions of order, relevancy, regularity and any other matters shall be observed at the meeting.
3.7 Attendance
3.7.1 The names of the Directors present at the meeting shall be recorded in the minutes.
3.8 Quorum
3.8.1 No business shall be transacted at a meeting of the Board of Directors unless at least six Directors are present including at least two Executive Directors, one of whom must be the Chief Executive or Deputy Chief
Constitution Page 90 of 107
Executive, and two Non-Executive Directors, one of whom must be the Chairperson or the Vice-Chairperson.
3.8.2 An Officer in attendance for an Executive Director but without formal
acting up status may not count towards the quorum. 3.8.3 If a Director has been disqualified from participating in the discussion on
any matter and/or from voting on any resolution by reason of the declaration of a conflict of interest (see SO 6 or 7) he shall no longer count towards the quorum. If a quorum is then not available for the discussion and/or the passing of a resolution on any matter, that matter may not be discussed further or voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting. The meeting must then proceed to the next business. The above requirement for at least two Executive Directors to form part of the quorum shall not apply where the Executive Directors are excluded from a meeting (for example when the Board of Directors considers the recommendations of the Remuneration Committee).
3.9 Minutes
3.9.1 The minutes of the proceedings of a meeting shall be prepared and submitted to be read and for agreement at the next ensuing meeting where they will be considered to have been signed by the person presiding at it. The approved minutes will be conclusive evidence of the events of the meeting and retained in an electronic minute book held by the Trust Secretary.
3.9.2 No discussion shall take place upon the minutes except upon their accuracy or where the Chairperson considers discussion appropriate. Any amendment to the minutes shall be agreed and recorded at the next meeting.
3.9.3 Minutes shall be circulated in accordance with Directors' wishes. A copy of the minutes of the meetings of the Board of Directors shall be sent to the Council of Governors as soon as practicable following the meeting. Where providing a record of a public meeting the minutes shall be made available to the public.
4. ARRANGEMENTS FOR THE EXERCISE OF FUNCTIONS BY DELEGATION
4.1 Subject to paragraph 4.3 of the Constitution, Standing Order 2.4 or any relevant statutory provision, the Board of Directors may make arrangements for the exercise, on behalf of the Trust, of any of its functions by a committee or sub-committee, appointed by virtue of Standing Order 5.1 or 5.2 below or by a Director or an Officer of the Trust in each case subject to such restrictions and conditions as the Board of Directors thinks fit.
4.2 Emergency Powers - The powers which the Board of Directors has retained to itself under Standing Order 2.4 may in emergency be
Constitution Page 91 of 107
exercised by the Chief Executive and the Chairperson after having consulted at least two Non-Executive Directors. The exercise of such powers by the Chief Executive and the Chairperson shall be reported to the next formal meeting of the Board of Directors for ratification.
4.3 Delegation to Committees - The Board of Directors shall agree from time to time to the delegation of executive powers to be exercised by committees or sub-committees, which it has formally constituted. The constitution and terms of reference of these committees, or sub-committees, and their specific executive powers shall be approved by the Board of Directors.
4.4 Delegation to Officers - Those functions of the Trust which have not been retained as reserved by the Board of Directors or delegated to a committee or sub-committee shall be exercised on behalf of the Board of Directors by the Chief Executive. The Chief Executive shall determine which functions he will perform personally and shall nominate officers to undertake the remaining functions for which he will still retain accountability to the Board of Directors.
4.5 The Chief Executive shall prepare a Scheme of Delegation identifying his proposals which shall be considered and approved by the Board of Directors, subject to any amendment agreed during the discussion. The Chief Executive may periodically propose amendment to the Scheme of Delegation which shall be considered and approved by the Board of Directors as indicated above.
4.6 Nothing in the Scheme of Delegation shall impair the discharge of the direct accountability to the Board of Directors of the DOF or other Executive Director to provide information and advise the Board of Directors in accordance with any statutory or Monitor requirements.
5 COMMITTEES
5.1 Subject to paragraph 4.3 of the Constitution, Standing Order 2.4 and such other guidance as may be given by Monitor, the Trust may and, if directed by Monitor, shall appoint Committees of the Trust, consisting wholly or partly of Directors of the Trust or wholly of persons who are not Directors of the Trust.
5.2 A Committee appointed under Standing Order 5.1 may, subject to such directions as may be given by Monitor or the Trust, appoint sub-committees consisting wholly or partly of members of the Committee (whether or not they include Directors of the Trust or wholly of persons who are not members of that Committee).
5.3 The Standing Orders of the Trust, as far as they are applicable, shall apply with appropriate alteration to meetings of any Committees or sub-committee established by the Trust.
Constitution Page 92 of 107
5.4 Each such Committee or sub-committee shall have such terms of reference and powers and be subject to such conditions (as to reporting back to the Board of Directors), as the Board of Directors shall decide.
5.5 Committees may not delegate their executive powers to a sub-committee unless expressly authorised by the Board of Directors.
5.6 The Board of Directors shall approve the appointments to each of the Committees which it has formally constituted. Where the Board of Directors determines that persons, who are neither Directors nor Officers, shall be appointed to a Committee, the terms of such appointment (including payment of travelling and other allowances) shall be determined by the Board of Directors.
5.7 Where the Board of Directors needs to appoint persons to a Committee and/or to undertake required statutory functions, and where such appointments are to operate independently of the Trust such appointment shall be made in accordance with any national regulations laid down.
5.8 The Committees and Sub-Committees established by the Trust are:
Audit Committee
Nomination and Remuneration Committee
and such other Committees as the Board of Directors determines are required to discharge the Board of Directors’ responsibilities in relation to quality, finance and performance.
5.9 A member of a Committee shall not disclose a matter dealt with by, or brought before, the Committee without its permission until the Committee shall have reported to the Board of Directors or shall otherwise have concluded on that matter.
5.10 A Director of the Trust or a member of a Committee shall not disclose any matter reported to the Board of Directors or otherwise dealt with by the Committee, notwithstanding that the matter has been reported or action has been concluded, if the Board of Directors or Committee shall resolve that it is confidential.
6 DECLARATION OF INTERESTS AND REGISTER OF INTERESTS
6.1 Declaration of Interests
6.1.1 The Constitution, the 2006 Act and the Code of Accountability for NHS Boards require Directors to declare interests which are relevant and material to the Board of Directors. All existing Directors should declare such interests. Any Directors appointed subsequently should do so on appointment. Any Director who fails to disclose any interest required to be disclosed under this section must permanently vacate their office if required to do so by a majority of the remaining Directors and (in the case
Constitution Page 93 of 107

of a Non-Executive Director) by the requisite majority of the Council of Governors.
6.1.2 Interests which should be regarded as relevant and material are:
a. Any directorship of a company; b. Any interest (excluding a holding of shares in a company whose
shares are listed on any public exchange where the holding is less than 2% of the total shares in issue) held by a Director in any firm or company or business which, in connection with the matter, is trading with the Trust or is likely to be considered as a potential trading partner with the Trust;
c. Any interest in an organisation providing health and social care services to the National Health Service;
d. A position of authority in a charity or voluntary organisation in the field of health and social care.
6.1.3 If Directors have any doubt about the relevance of an interest, this should be discussed with the Chairperson.
6.1.4 At the time a Directors' interests are declared, they should be recorded in the minutes. Any changes in interests should be declared at the next Board of Directors' meeting following the change occurring.
6.1.5 Directors' directorships of companies likely or possibly seeking to do business with the NHS should be published in the Trust's Annual Report. The information should be kept up to date for inclusion in succeeding Annual Reports.
6.1.6 There is no requirement for the interests of Directors' spouses or Partners to be declared, but for pecuniary interests see Standing Order 7.5.
6.1.7 A separate policy exists for the declaration of interests for all other staff.
6.2 Conflict of Interest
6.2.1 During the course of a Board of Directors’ meeting, if a conflict of interest is established, the Director concerned should withdraw from the meeting and play no part in the relevant discussion or decision and shall not vote on the issue (and if by inadvertence they do remain and vote, their vote shall not be counted).
6.3 Register of Interests
6.3.1 The Chief Executive will ensure that a Register of Interests is established to record formally declarations of interests of Directors. In particular the Register will include details of all directorships and other relevant and material interests which have been declared by both Executive and Non-Executive Directors.
6.3.2 These details will be kept up to date by means of an annual review of the Register in which any changes to interests declared during the preceding
Constitution Page 94 of 107
twelve months will be incorporated.
6.3.3 The Register will be available to the public and the Chief Executive will take reasonable steps to bring the existence of the Register to the attention of the local population and to publicise arrangements for viewing it.
7. DISABILITY OF DIRECTORS IN PROCEEDINGS ON ACCOUNT OF PECUNIARY INTEREST
7.1 Subject to the Constitution and the following provisions of this Standing Order, if any member of staff or Director of the Trust has any pecuniary interest, direct or indirect, in any contract, proposed contract or other matter and is present at a meeting of the Trust at which the contract or other matter is the subject of consideration, he shall at the meeting and as soon as practicable after its commencement disclose the fact and shall not take part in the consideration or discussion of the contract or other matter or vote on any question with respect to it.
7.2 Monitor may, subject to such conditions as it may think fit to impose, remove any disability imposed by this Standing Order in any case in which it appears to Monitor in the interests of the National Health Service that the disability should be removed.
7.3 The Trust shall exclude a Director from a meeting of the Trust while any contract, proposed contract or other matter in which he has a pecuniary interest, is under consideration.
7.4 Any remuneration, compensation or allowances payable to a Director by virtue of paragraph 18 of Schedule 7 to the 2006 Act or pursuant to the Constitution shall not be treated as a pecuniary interest for the purpose of this Standing Order.
7.5 For the purpose of this Standing Order the Chairperson or a Director shall be treated, subject to Standing Order 7.2 and Standing Order 7.6, as having indirectly a pecuniary interest in a contract, proposed contract or other matter, if:
a. he, or a nominee of his, is a director of a company or other body, not being a public body, with which the contract was made or is proposed to be made or which has a direct pecuniary interest in the other matter under consideration;
or
b. he is a partner of, or is in the employment of, a person with whom the contract was made or is proposed to be made or who has a direct pecuniary interest in the other matter under consideration;
and in the case of married persons or civil partners living together the interest of one shall, if known to the other, be deemed for the purposes of this Standing Order to be also an interest of the other.
Constitution Page 95 of 107

7.6 A Director shall not be treated as having a pecuniary interest in any contract, proposed contract or other matter by reason only:
a. of his membership of a company or other body, if he has no beneficial interest in any securities of that company or other body;
b. of an interest in any company, body or person with which he is connected as mentioned in Standing Order 7.5 above which is so remote or insignificant that it cannot reasonably be regarded as likely to influence a Director in the consideration or discussion of, or in voting on, any question with respect to that contract or matter.
7.7 Where a Director:
a. has an indirect pecuniary interest in a contract, proposed contract or other matter by reason only of a beneficial interest in securities of a company or other body; and
b. the total nominal value of those securities does not exceed £10,000 or
one-hundredth of the total nominal value of the issued share capital of the company or body, whichever is the less; and
c if the share capital is of more than one class, the total nominal value of
shares of any one class in which he has a beneficial interest does not exceed one-hundredth of the total issued share capital of that class,
this Standing Order shall not prohibit him from taking part in the
consideration or discussion of the contract or other matter or from voting on any question with respect to it without prejudice however to his duty to disclose his interest.
7.8 Standing Order 7 applies to a Committee or sub-committee of the Trust as it applies to the Trust and applies to any member of any such Committee or sub-committee (whether or not he is also a Director of the Trust) as it applies to a Director of the Trust.
8 STANDARDS OF BUSINESS CONDUCT
8.1 Policy – All staff must comply with the national guidance contained in HSG(93)5 ‘Standards of Business Conduct for NHS staff’ as amended by the Bribery Act 2010 and the ‘Code of Conduct and Accountability for all NHS Boards’. The following provisions should be read in conjunction with this document.
8.2 Interest of Officers in Contracts - If it comes to the knowledge of a Director or an Officer of the Trust that a contract in which he has any pecuniary interest not being a contract to which he is himself a party, has been, or is proposed to be, entered into by the Trust he shall, at once, give notice in writing to the Chief Executive of the fact that he is interested therein. In the case of married persons, civil partners or persons living together as partners, the interest of one partner shall, if
Constitution Page 96 of 107

known to the other, be deemed to be also the interest of that partner.
8.3 All Officers involved in contracting, tendering and procurement are required to make the appropriate declarations of actual or nil interests, hospitality or sponsorship both at the start and conclusion of each process.
8.4 An Officer must also declare to the Chief Executive any other employment or business or other relationship of his, or of a cohabiting spouse, civil partner or partner, that conflicts, or might reasonably be predicted could conflict with the interests of the Trust.
8.5 The Trust may require interests, employment or relationships so declared by staff to be entered in a Register of Interests of staff.
8.6 Canvassing of, and Recommendations by, Directors in Relation to Appointments - Canvassing of Directors of the Trust or members of any Committee of the Trust directly or indirectly for any appointment under the Trust shall disqualify the candidate for such appointment. The contents of this paragraph of the Standing Orders shall be included in application forms or otherwise brought to the attention of candidates.
8.7 A Director of the Trust shall not solicit for any person any appointment under the Trust or recommend any person for such appointment: but this paragraph of these Standing Orders shall not preclude a Director from giving written testimonial of a candidate's ability, experience or character for submission to the Trust.
8.8 Informal discussions outside appointments panels or committees, whether solicited or unsolicited, should be declared to the panel or committee.
8.9 Relatives of Directors or Officers - Candidates for any staff appointment shall when making application disclose in writing whether they are related to any Director or the holder of any office under the Trust. Failure to disclose such a relationship shall disqualify a candidate and, if appointed, render him liable to instant dismissal.
8.10 The Directors and every Officer of the Trust shall disclose to the Chief Executive any relationship with a candidate of whose candidature that Director or Officer is aware. It shall be the duty of the Chief Executive to report to the Trust any such disclosure made.
8.11 On appointment, Directors should disclose to the Trust whether they are related to any other Director or holder of any office under the Trust.
8.12 Where the relationship of an Officer or another Director to a Director of the Trust is disclosed, the Standing Order headed `Disability of Directors in Proceedings on Account of Pecuniary Interest' (Standing Order 7) shall apply.
Constitution Page 97 of 107

9. CUSTODY OF SEAL AND SEALING OF DOCUMENTS
9.1 Custody of Seal -The Common Seal of the Trust shall be kept by the Secretary in a secure place.
9.2 Sealing of Documents - The Seal of the Trust shall not be fixed to any documents unless the sealing has been authorised by a resolution of the Board of Directors or of a Committee thereof or where the Board of Directors has delegated its powers.
9.3 Before any document is sealed it must be approved and signed by the Chief Executive (or an Officer nominated by him who shall not be within the originating directorate) and authorised and countersigned by the Chairperson (or an Officer nominated by him who shall not be within the originating directorate).
9.4 Register of Sealing - An entry of every sealing shall be made and numbered consecutively in a book provided for that purpose, and shall be signed by the persons who shall have approved and authorised the document and those who attested the seal.
[Note the legal requirement to seal documents executed as a deed has beenremoved. Trusts may however, choose to continue to use the seal].
9.5 A document purporting to be duly executed under the Trust's seal or to be signed on its behalf is to be received in evidence and, unless the contrary is proved, taken to be so executed or signed.
10. SIGNATURE OF DOCUMENTS
10.1 Where the signature of any document will be a necessary step in legal proceedings involving the Trust, it shall be signed by the Chief Executive or Director of Finance, unless any enactment otherwise requires or authorises, or the Board of Directors shall have given the necessary authority to some other person for the purpose of such proceedings.
10.2 The Chief Executive or Nominated Officers shall be authorised, by resolution of the Board of Directors, to sign on behalf of the Trust any agreement or other document (not required to be executed as a deed) the subject matter of which has been approved by the Board of Directors or Committee or sub-committee to which the Board of Directors has delegated appropriate authority.
11. STANDING ORDERS
11.1 Standing Orders to be given to Directors and Officers
11.1.1 It is the duty of the Chief Executive to ensure that existing Directors and Officers and all new appointees are notified of and understand their responsibilities within Standing Orders and Standing Financial Instructions. Updated copies shall be issued to staff designated by the
Deleted:
Constitution Page 98 of 107

Chief Executive. New designated officers shall receive advice on where to find Standing Orders and Standing Financial Instructions.
11.2 Suspension of Standing Orders
11.2.1 Except where this would contravene any statutory provision or any provision in the Constitution, any one or more of the Standing Orders may be suspended at any meeting, provided that at least two-thirds of the Board of Directors are present, including one Executive Director and one Non-Executive Director, and that a majority of those present vote in favour of suspension.
11.2.2 A decision to suspend Standing Orders shall be recorded in the minutes of the meeting.
11.2.3 A separate record of matters discussed during the suspension of Standing Orders shall be made and shall be available to the Directors.
11.2.4 No formal business may be transacted while Standing Orders are suspended.
11.2.5 The Audit Committee shall review every decision to suspend Standing Orders
11.3 Amendment of Standing Orders
11.3.1 These Standing Orders may be amended only in accordance with paragraph 44 of the Constitution.
11.4 Review of Standing Orders
11.4.1 The Standing Orders shall be reviewed annually by the Trust.
Constitution Page 99 of 107
ANNEX 8 – FURTHER PROVISIONS
Appendix 1: Trust Core Principles 1. Trust Commitment
1.1 The Trust shall exercise its functions effectively, efficiently and economically. 2. Representative Membership
2.1 The Trust shall take steps to secure that taken as a whole its actual membership is representative of those eligible for membership.
To this end:
2.2 the Trust shall at all times have in place and pursue a membership strategy which shall be approved by the Council of Governors, and shall be reviewed by them from time to time, and at least every three years; and
2.3 the Council of Governors will report to the members at each Annual
Members' Meeting in accordance with the provisions in Annex 8, Appendix 3, Paragraph 1.6.2.
3 Co-operation with NHS Bodies
3.1 In exercising its functions the Trust shall co-operate with other NHS Bodies. For the purposes of this section, each of National Institute for Health and Care Excellence and the Health and Social Care Information Centre is an NHS Body.
4. Respect for rights of people
4.1 In conducting its affairs, the Trust shall respect the rights of members of the community it serves, its employees and people dealing with the Trust as set out in the Human Rights Act 1998.
5. Openness 5.1 In conducting its affairs, the Trust shall have regard to the need to provide
information to members and conduct its affairs in an open and accessible way.
6. Prohibiting distribution 6.1 The profits and surpluses of the Trust are not to be distributed either directly
or indirectly in any way at all among members of the Trust.
Constitution Page 100 of 107
ANNEX 8 – FURTHER PROVISIONS
Appendix 2: Membership
1. Disqualification from membership 1.1 A person may not become or continue as a member of the Trust if:
1.1.1 within the last five years they have shown aggressive or violent
behaviour towards Trust staff which has resulted in a Violent and Aggressive Patient Assessment being completed and/or a warning letter being sent in accordance with the Trust's Policy for Managing Violence and Aggression;
1.1.2 they have been confirmed as an unreasonable or persistent complainant in accordance with the relevant Trust policy for handling complaints; or
1.1.3 they have been removed as a member from another NHS foundation
trust.
2. Termination of membership 2.1 A member shall cease to be a member of the Trust if:
2.1.1 they resign by notice to the Secretary;
2.1.2 they die;
2.1.3 they are expelled from membership under the Constitution;
2.1.4 they are disqualified from membership under the Constitution;
2.1.5 they cease to be entitled under this Constitution to be a member of the
Public Constituency or of any of the classes of the Staff Constituency; or
2.1.6 if it appears to the Secretary that they no longer wish to be a member
of the Trust, and after enquiries made in accordance with a process approved by the Council of Governors, they fail to demonstrate that they wish to continue to be a member of the Trust.
3. Expulsion from membership
3.1 A member may be expelled by a resolution approved by not less than two-
thirds of the members of the Council of Governors present and voting at a general meeting of the Council of Governors. The following procedure is to be adopted: 3.1.1 Any member may complain to the Secretary that another member of
the Trust has acted in a way detrimental to the interests of the Trust. Constitution Page 101 of 107
3.1.2 If a complaint is made, the Council of Governors will consider the
complaint having taken such steps as it considers appropriate to ensure that each member of the Trust's point of view is heard and may:
3.1.2.1 dismiss the complaint and take no further action; or
3.1.2.2 for a period not exceeding twelve months suspend the rights of the member of the Trust complained of to attend Members' Meetings and vote under the Constitution; or
3.1.2.3 arrange for a resolution to expel the member of the Trust
complained of to be considered at the next general meeting of the Council of Governors.
3.1.3 If a resolution to expel a member of the Trust is to be considered at a
general meeting of the Council of Governors, details of the complaint must be sent to the member complained of not less than one calendar month before the meeting with an invitation to answer the complaint and attend the meeting.
3.1.4 At the meeting the Council of Governors will consider evidence in
support of the complaint and such evidence as the member complained of may wish to place before them.
3.1.5 If the member complained of fails to attend the meeting without due
cause the meeting may proceed in their absence.
3.3 A person expelled from membership will cease to be a member of the Trust upon the declaration of the Chairperson of the meeting that the resolution to expel them is carried.
3.4 No person who has been expelled from membership is to be readmitted
except by a resolution approved by not less than two-thirds of the members of the Council of Governors present and voting at a general meeting of the Council of Governors.
4. Member declaration
4.1 A member of a Public Constituency may not vote at an election for a Public
Constituency unless within 21 days before they vote they have made a declaration in the form specified by the Secretary that they are qualified to vote as a Member of the relevant Public Constituency. It is an offence to knowingly or recklessly make such a declaration which is false in a material particular.
Constitution Page 102 of 107

ANNEX 8 – FURTHER PROVISIONS
Appendix 3: Members' Meetings
1. Members' Meetings 1.1 The Trust shall hold the Annual Members' Meeting within nine months of the
end of each Financial Year. 1.2 All Members' Meetings other than Annual Members' Meetings are called
Special Members' Meetings. 1.3 Both Annual and Special Members' Meetings are open to all members of the
Trust, governors and Directors, representatives of the Auditor, and members of the public. The Council of Governors may invite representatives of the media and any experts or advisors whose attendance they consider to be in the best interests of the Trust to attend a Members' Meeting.
1.4 All Members' Meetings are to be convened by the Secretary by order of the Council of Governors.
1.5 The Council of Governors may decide where a Members' Meeting is to be
held and may also for the benefit of members:
1.5.1 arrange for the Annual Members' Meeting to be held in different venues each year; and/or
1.5.2 make provisions for an Annual or Special Members' Meeting to be held at different venues simultaneously or at different times. In making such provision the Council of Governors shall also fix an appropriate quorum for each venue, provided that the aggregate of the quorum requirements shall not be less than the quorum set out below.
1.6 At the Annual Members' Meeting:
1.6.1 the documents below shall be presented to the members with at least
one member of the Board of Directors in attendance: 1.6.1.1 the annual accounts;
1.6.1.2 any report of the Auditor on them;
1.6.1.3 the annual report; and
1.6.1.4 forward planning information for the next Financial Year;
1.6.2 the Council of Governors shall present to the members: 1.6.2.1 a report on steps taken to secure that (taken as a whole) the
actual membership of its Public Constituency and of the Constitution Page 103 of 107

classes of the Staff Constituency is representative of those eligible for such membership;
1.6.2.2 the progress of, and any changes to, the membership
strategy;
1.6.2.3 any proposed changes to the policies for the composition of the Council of Governors and of the Non-Executive Directors;
1.6.3 the results of any election or appointment of governors and the
appointment of any Non-Executive Directors in the year will be announced.
1.7 Notice of a Members' Meeting is to be given:
1.7.1 by notice to all members;
1.7.2 by notice prominently displayed at the head office and at all of the
Trust’s places of business; and
1.7.3 by notice on the Trust’s website,
at least 14 clear days before the date of the meeting. The notice must:
1.7.4 be given to the Council of Governors and the Board of Directors, and to the Auditor;
1.7.5 state whether the meeting is an Annual or Special Members' Meeting;
1.7.6 give the time, date and place of the meeting; and
1.7.7 indicate the business to be dealt with at the meeting.
1.8 Before a Members' Meeting can do business there must be a quorum present. Except where this Constitution says otherwise a quorum is three members present from any of the Trust’s constituencies.
1.9 The Trust may make arrangements for members to vote by post, or by using electronic communications.
1.10 It is the responsibility of the Council of Governors, the Chairperson of the
meeting and the Secretary to ensure that at any Members' Meeting:
1.10.1 the issues to be decided are clearly explained; and
1.10.2 sufficient information is provided to members to enable rational discussion to take place.
1.11 The Chairperson of the Trust, or in their absence the Lead Governor, or in
their absence one of the other governors from the Public Constituency shall act as Chairperson at all Members' Meetings of the Trust. If neither the Chairperson nor the Lead Governor is present, the members of the Council of
Deleted: G
Constitution Page 104 of 107

Governors present shall elect a governor from the Public Constituency to be Chairperson and if there is only one such governor present and willing to act they shall be Chairperson.
1.12 If no quorum is present within half an hour of the time fixed for the start of the meeting, the meeting shall stand adjourned to the same day in the next week at the same time and place or to such time and place as the Council of Governors determine. If a quorum is not present within half an hour of the time fixed for the start of the adjourned meeting, the number of members present during the meeting is to be a quorum.
1.13 A resolution put to the vote at a Members' Meeting shall be decided upon by a
poll. 1.14 Every member present and every member who has voted by post or using
electronic communications is to have one vote. In the case of an equality of votes the Chairperson of the meeting is to have a second or casting vote.
1.15 The result of any vote will be declared by the Chairperson and recorded in the
minutes. The minutes will be conclusive evidence of the result of the vote. 1.16 Minutes of the proceeding of a Members' Meeting shall be prepared and
submitted to be read and for agreement at the next Members' Meeting where they will be considered to have been signed by the person presiding at it. The approved minutes will be conclusive evidence of the events of the meeting and retained in an electronic minute book held by the Secretary
Constitution Page 105 of 107
ANNEX 8 – FURTHER PROVISIONS
Appendix 4: Board of Directors – Further Provisions
1. Board of Director's Disqualification 1.1 A person may not become or continue as a Director of the Trust if:
1.1.1 they are a member of the Council of Governors, or a governor or director of another NHS Body;
1.1.2 they are a member of a Patient's Forum of an NHS Body; 1.1.3 they are the spouse, Partner, parent or child of a member of the Board
of Directors; 1.1.4 they are a member of Bournemouth Borough Council's Oversight and
Scrutiny Committee covering health matters; 1.1.5 they are subject to an unexpired disqualification order made under the
Company Directors Disqualification Act 1986; 1.1.6 in the case of a Non-Executive Director, they are no longer a member
of the Public Constituency; 1.1.7 they are a person whose tenure of office as a Chairperson or as a
member or director of an NHS Body has been terminated on the grounds that their appointment is not in the interests of the health service, for non-attendance at meetings, or for non-disclosure of a pecuniary interest;
1.1.8 they have had their name removed, from any list maintained by health
and social care professional bodies in the UK and have not subsequently had their name included on such a list;
1.1.9 they have within the preceding two years been dismissed, otherwise
than by reason of redundancy, from any paid employment with an NHS Body;
1.1.10 in the case of a Non-Executive Director they have refused without
reasonable cause to fulfil any training requirement established by the Board of Directors; or
1.1.11 they have refused to sign and deliver to the Secretary a statement in
the form required by the Board of Directors confirming acceptance of the code of conduct for Directors.
2. Process for appointing Non-Executive Directors and the Chairperson
2.1 Non-Executive Directors are to be appointed by the Council of Governors
using the following procedure: Constitution Page 106 of 107

2.1.1 The Council of Governors will maintain a policy for the composition of the Non-Executive Directors which takes account of the skills and experience required for Non-Executive Directors identified by the Board of Directors, and which they shall review from time to time and not less than every three years.
2.1.2 The Board of Directors will identify the skills and experience required
for Non-Executive Directors and may work with an external organisation recognised as expert at such appointments.
2.1.3 Appropriate candidates (not more than five for each vacancy) will be
identified by a Nominations Committee through a process of open competition, which take account of the policy maintained by the Council of Governors and the skills and experience required.
2.1.4 The Nominations Committee will comprise a majority of governors.
2.1.5 Any re-appointment of a Non-Executive Director by the Council of Governors shall be subject to a satisfactory appraisal carried out in accordance with procedures which the Board of Directors has approved.
3. Process for removal of Non-Executive Directors and the Chairperson
3.1 The removal of the Chairperson or another Non-Executive Director shall be in
accordance with the following procedure: 3.1.3 Any proposal for removal must be proposed by a governor and
seconded by not less than ten Governors including at least two Elected Governors and two Appointed Governors.
3.1.4 Written reasons for the proposal shall be provided to the Non-Executive Director in question, who shall be given the opportunity to respond to such reasons.
3.1.5 In making any decision to remove a Non-Executive Director, the
Council of Governors shall take into account the annual appraisal carried out by the Chairperson.
3.1.6 If any proposal to remove a Non-Executive Director is not approved at
a meeting of the Council of Governors, no further proposal can be put forward to remove such Non-Executive Director based upon the same reasons within 12 months of the meeting.
4. Expenses
4.1 The Trust may reimburse Directors' travelling and other costs and expenses at
such rates as the remuneration committee of Non-Executive Directors decides. These are to be disclosed in the annual report.
4.2 The remuneration and allowances for Directors are to be disclosed in bands in the annual report.
Deleted: G
Deleted: G
Constitution Page 107 of 107

COUNCIL OF GOVERNORS
Meeting Date: 13 April 2016 – Part 1
Subject: Council of Governor Budget
Section on agenda: Information
Officer with overall responsibility: Sarah Anderson
Author(s) of papers: Sarah Anderson
Details of previous discussion and/or dissemination:
N/A
Action required: Approve / Discuss / Information / Note
To Note
Executive Summary:

Governor Budget The Trust Secretary holds the budget for the Governors. The total budget is £28,400. Much of this budget is committed for the elections (£10,000), membership database (£5,600), Annual Members’ Meeting (£900), membership forms (£1,000) and FT Focus (£1,000). This leaves less than half the budget which can be considered discretionary for items such as governor training, hire of premises for talks/engagement, travel and refreshments. This year the budget was subjected to a cost improvement programme target of 3%. The budget for 2016/17 is: £ Stationery 100 Printing 2,000 Travel and subsistence 4,500 Hire of premises 1,600 Elections/Membership database 15,600 Training Expenses 3,600 Refreshments 1,000 The Council of Governors is asked to note the budget. In addition, the Council of Governors is asked to be mindful of future cost improvement programme targets and the need to maintain a tight control of finance in the current year.

COUNCIL OF GOVERNORS
Meeting Date: 13 April 2016 – Part 1
Subject: 2016 Annual Members’ Meeting
Section on agenda: Decision
Officer with overall responsibility: Sarah Anderson
Author(s) of papers: Sarah Anderson
Details of previous discussion and/or dissemination:
Membership Development Committee (January 2015) and Board of Directors Meeting (April 2015)
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary:

Annual Members Meeting The Membership Development Committee of the Council of Governors proposed in January 2015 that the Trust hold an Open Day at a weekend to encourage those who work and young people to attend. This event would be bigger than the Open Days held by the Trust in recent years. The proposal included holding the Annual Members’ Meeting on the same day. This would help with the promotion of the event as we could use the Members’ networks and would give Members an opportunity to explore the Trust further whilst they were here for that meeting. It will also give a wider opportunity for the public attend the Annual Members’ Meeting and provide the Governors the potential to recruit new Trust members. In addition, it would bring a cost saving as the Annual Members’ Meeting could use the same facilities as the Open Day and governors would only need to be available for one day, not two, in September. The Open Day will include a number of departments, such as operating theatres, laboratories and some clinical areas, being open to the public so that they can gain a greater understanding of the work of the hospital. A Saturday has been chosen so that it is open to the all parts of the local community giving a greater chance for working people and children to attend. September is a good time as the weather should still be fine and it is the start of the new term – and the opening of the UCAS application window – with school/college students considering applying for a nursing degree or a career in the health service. In addition, it is hoped that the Open Day will improve recruitment and awareness of career opportunities, raise the profile for the Trust and improve connections with the community. September 2016 has been proposed as the first date for this event and that it will be an annual event thereafter. The Council of Governors is requested to support the approach of holding the Annual Members’ Meeting as part of the Open Day which can better showcase the Trust than a couple of focused talks following the formal agenda. Governors are asked to note the cost saving and benefit to the Trust that such an approach will bring. Should governors wish to continue with a separate date from the Open Day for the Annual Members’ Meeting, governors need to be mindful that the format may be restricted to the formal part of the meeting only. Staff may be unable to support a second event in such a short timeframe (i.e. no stands and no health talk). The cost of such an event would not be significantly less than in previous years due to the way that the venue and PA system are booked.

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Membership Development Committee Work Programme
Section on agenda: Decision
Officer with overall responsibility: Chris Archibold
Author(s) of papers: Chris Archibold
Details of previous discussion and/or dissemination:
Membership Development Committee
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary: The Membership Development Committee is a committee established by and responsible to the Council of Governors.
The primary aim of the Committee is to develop the Trust’s membership by increasing engagement with existing and recruiting new members. The Committee have developed the attached work programme so they can fulfil the duties remitted by the Council of Governors.

2016-17 membership Development Committee Work ProgrammeObjective Task Timing Lead of Process Task Completion Commentary
1. Membership Devlopment: Engage with Members and within the constituencies
1.1 Establish year programme for Constituency meetings in written plan. January 2016
Constituency Leads:Derek Chaffey, Bob Gee, Keith Mitchell
1.2 Each Constituency to hold one public meeting, one Understanding Health Talk and minimum of One listening Event Ongoing
Constituency Leads:Derek Chaffey, Bob Gee, Keith Mitchell
1.3 Utilise internal LCD Screens to share information Ongoing
All Governors and Trust Secretary's Office and Communications Department. Ongoing
1.4 Engage with local PPG Ongoing
All Governors and Trust Secretary's Office and Communications Department.
Liase with Eric Fisher and each Governor to investigate their local PPG.
1.5Engage with Private Patient Pathway Ongoing
All Governors and Trust Secretary's Office and Communications Department.
Dily Ruffer to liase with Michele Burden.
1.6 Engage with Education Workstream and Local Schools Ongoing
All Governors and Trust Secretary's Office and Communications Department. Dily Ruffer to liase with HR.
1.7 Engage on Corporate Initiatives in local business Ongoing
All Governors and Trust Secretary's Office and Communications Department.
CJA to contact local business working alongside Trust Secretary Office.
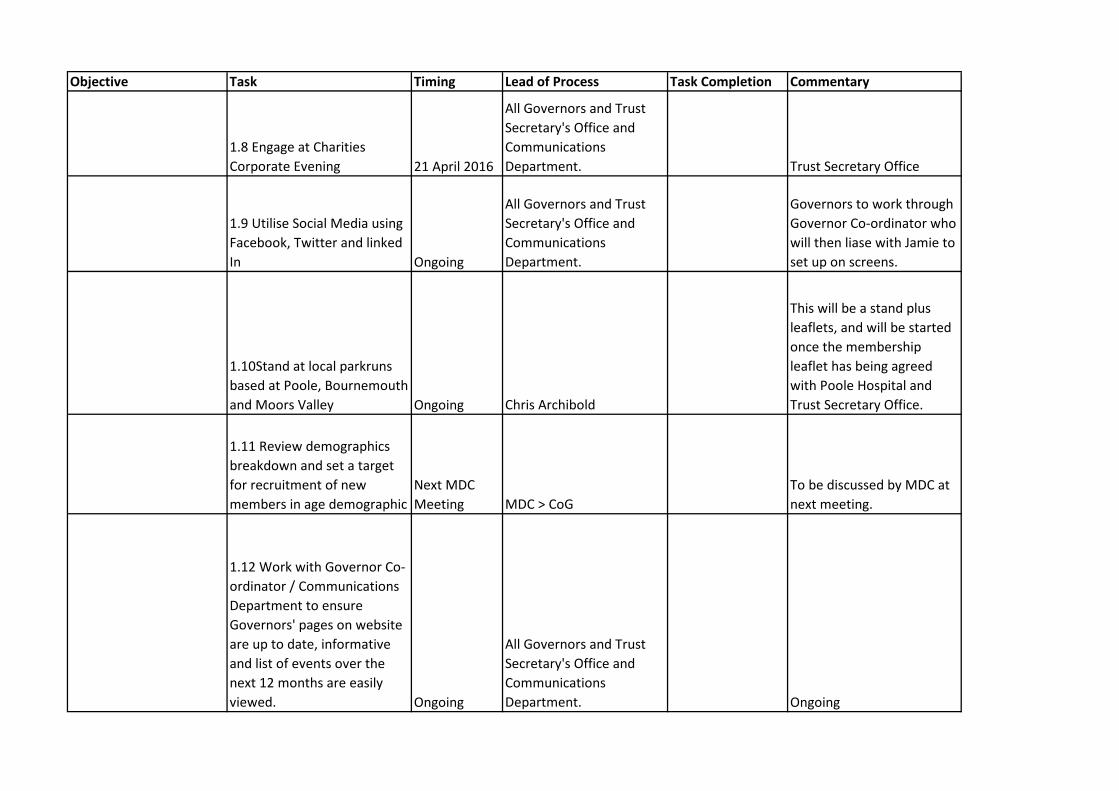
Objective Task Timing Lead of Process Task Completion Commentary
1.8 Engage at Charities Corporate Evening 21 April 2016
All Governors and Trust Secretary's Office and Communications Department. Trust Secretary Office
1.9 Utilise Social Media using Facebook, Twitter and linked In Ongoing
All Governors and Trust Secretary's Office and Communications Department.
Governors to work through Governor Co-ordinator who will then liase with Jamie to set up on screens.
1.10Stand at local parkruns based at Poole, Bournemouth and Moors Valley Ongoing Chris Archibold
This will be a stand plus leaflets, and will be started once the membership leaflet has being agreed with Poole Hospital and Trust Secretary Office.
1.11 Review demographics breakdown and set a target for recruitment of new members in age demographic
Next MDC Meeting MDC > CoG
To be discussed by MDC at next meeting.
1.12 Work with Governor Co-ordinator / Communications Department to ensure Governors' pages on website are up to date, informative and list of events over the next 12 months are easily viewed. Ongoing
All Governors and Trust Secretary's Office and Communications Department. Ongoing

Objective Task Timing Lead of Process Task Completion Commentary
1.13 Work with Poole Hospital to look at joint membership meetings and a joint membership leaflet. June 2016
CJA / Trust Secretary Office
Review with Poole Hospital once received confirmation from Trust Secretary Office on legal aspects to joint membership
1.14 Staff Governors to educate their colleagues about the benefits of membership and engagement. Ongoing Staff Governors Ongoing
1.15 Produce a Membership Benefit Statement for use on membership leaflets etc in conjunction with Poole Hospital June 2016
CJA / Trust Secretary Office/Poole Hospital
Review with Poole Hospital once received confirmation from Trust Secretary Office on legal aspects to joint membership

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Membership Development Committee Engagement Programme
Section on agenda: Decision
Officer with overall responsibility: Chris Archibold with Constituency Lead Governors
Author(s) of papers: Dily Ruffer
Details of previous discussion and/or dissemination:
Membership Development Committee
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary: Governors to approve and support the 2016-17 programme for events to be held in the community.

Governor Public Events – 2016
Month Date Time Event Venue Governor Lead 2016 April Tuesday 12 April
10:00 – 15:00 Listening Event Christchurch Library Derek Chaffey
May Monday 2 May 12:30 – 17:00 (set up 09:30-11:00)
Bransgore Fun Day Bransgore Recreational Ground
Bob Gee
June
July Monday 4 July Time to be confirmed
Engagement Event Boscombe Library (TBC)
Keith Mitchell (Exec: Paula Shobbrook and TBC)
August Saturday 6 August 12:00 – 17:00 (set up 09:30-11:00)
Burley Show Burley Bob Gee
September Saturday 10 September
All Day Trust Open Day and Annual Members’ Meeting
Royal Bournemouth Hospital
Communications Department and Bob Gee, as Lead Governor
As at: 06 April 2016

September Monday 26 September
18:30 – 20:00 (set up from 17:30)
Engagement Event Allendale Community Centre, Wimborne
Chris Archibold (Exec: Richard Renaut and TBC)
October 24 October or 14 November 2016 TBC
18:00-20:00 (set up 17:30)
Understanding Health in the Community Talk (Subject to be confirmed)
Greyfriars Community Centre
Bob Gee
November December 2017 January February March
Events to be arranged:
• Understanding Health Talk in the Community o to be held in:
Bournemouth and Poole Constituency Christchurch and Dorset County Constituency
• Listening Event
o To be held in: Bournemouth and Poole Constituency
• Engagement Event in the Community
o to be held in: New Forest, Hampshire and Salisbury Constituency
As at: 06 April 2016
COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Membership Development Committee Terms of Reference
Section on agenda: Decision
Officer with overall responsibility: Chris Archibold with Constituency Lead Governors
Author(s) of papers: Dily Ruffer
Details of previous discussion and/or dissemination:
Membership Development Committee
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary: Changes to membership and consistency of wording

The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
MEMBERSHIP DEVELOPMENT COMMITTEE
Terms of Reference The Membership Development Committee (the Committee) is a committee established by and responsible to the Council of Governors. The primary aim of the Committee is to develop the Trust’s membership by increasing engagement with existing members and recruiting new members.
1. Membership
1.1 The membership of the Committee will consist of the following:
• • Lead Governor of the Council of Governors • One public governor from each constituency • One staff governor • One Appointed Governor • Any two other Governors • Chairperson of Governor Involvement with Patient and Public Engagement
In addition, the following will attend the committee to provide advice as required:
• Governor Co-ordinator • Trust Secretary • Head of Communications • One Non-Executive Director
1.2 Only members of the Committee have the right to attend Committee
meetings. The Committee Chairperson may invite governors or other individuals to attend for all or part of any meeting, as and when the Committee Chairperson considers it appropriate.
1.3 The Committee Chairperson shall be a governor and will be elected
by the Committee from amongst its membership annually. 1.4 All governor appointments will be made by self-nomination and a
vote will be taken by the Council of Governors if there are more nominees than vacancies. The ballot will be organised by the Trust Secretary in accordance with a process agreed by the Council of Governors.
Deleted: Deputy Chairman
Deleted: Chairman
Deleted: Chairman
Deleted: Chairman
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
3 July 2015 April 2017 Trust Secretary
Deleted: 2
Deleted: 6
1.5 Appointments to the Committee shall be for a period of two years,
which may be extended for one further three year period. The Council of Governors may choose to make appointments for a period of not more than one year greater or less than the period specified in order to ensure some continuity of membership of the Committee when vacancies arise. However, only those governors who have served at least one year as members of the Council of Governors shall be eligible for membership of this Committee.
2. Secretary
2.1 The Trust Secretary or their representative shall act as the
Secretary of the Committee. 3. Quorum
3.1 A quorum will be four members of the Committee.
4. Frequency of meetings
4.1 Meetings are to be held quarterly and at such other times as may
be required.
5. Notice of meetings
5.1 Meetings of the Committee shall be called by the Secretary of the Committee at the request of the Committee Chairperson.
5.2 The Committee Chairperson will agree the agenda and papers to
be circulated with the Trust Secretary or their representative. 5.3 Unless otherwise agreed, notice of each meeting confirming the
venue, time and date, together with an agenda of items to be discussed, shall be forwarded to each member of the Committee and any other person required to attend, no later than five working days before the date of the meeting. Where possible, the supporting papers shall be sent to Committee members and to other attendees as appropriate, at the same time.
6. Minutes of meetings
6.1 The Secretary of the Committee shall record action notes of the proceedings of all Committee meetings. They shall also record the names of those present and in attendance.
Deleted: Chairman
Deleted: Chairman
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
3 July 2015 April 2017 Trust Secretary
Deleted: 2
Deleted: 6
6.2 Action notes of Committee meetings shall be agreed by the Committee Chairperson prior to being circulated to all members of the Committee. The Secretary of the Committee shall aim to prepare the action notes within one week of the meeting date.
7. Duties
The Committee shall: 7.1 Build and develop the membership in line with the Trust’s
Membership Development Strategy; 7.2 Increase the active participation of members so they can benefit
fully from their membership and contribute to the development of the Trust and are encouraged to stand as Governors;
7.3 Receive membership information to identify where recruitment and
engagement needs to be focused; 7.4 Identify activities and events to attend to engage with existing and
prospective members and co-ordinate governors able to support these events;
7.5 Evaluate progress on the aims and objectives for membership as
defined in the Membership Development Strategy; 7.6 Review the format and content of the Annual Members' Meeting to
ensure maximum attendance and effective engagement with members;
8. Reporting responsibilities
8.1 The Committee is a Committee of the Council of Governors and is accountable to it.
8.2 A report by the Committee Chairperson shall be submitted to the
Council of Governors at the Council of Governors’ meeting following the Committee meeting. The action notes of the Committee meetings shall be available to governors who are not members of the Committee on request to the Committee Chairperson through the Trust Secretary's Office.
8.3 The Committee shall make whatever recommendations to the
Council of Governors it deems appropriate on any area within its remit where action or improvement is needed.
Deleted: Chairman
Deleted: ¶
Deleted: Chairman
Deleted: Chairman
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
3 July 2015 April 2017 Trust Secretary
Deleted: 2
Deleted: 6

8.4 The Committee shall compile a report on its activities to be included in the Trust’s annual plan.
9. Other
9.1 The Committee shall, at least once a year, review its own performance and terms of reference to ensure it is operating at maximum effectiveness. The Committee will report on its performance and recommend any changes it considers necessary to the terms of reference to the Council of Governors for approval.
10. Authority
10.1 The Committee is authorised to assist the Council of Governors in carrying out its functions.
10.2 None of the powers of the Council of Governors are delegated to
this Committee.
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
3 July 2015 April 2017 Trust Secretary
Deleted: 2
Deleted: 6

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Involvement with Patient and Public Engagement Committee Update
Section on agenda: Information
Officer with overall responsibility: David Bellamy
Author(s) of papers: David Bellamy
Details of previous discussion and/or dissemination:
Governor Involvement with Patient and Public Engagement Committee
Action required: Approve / Discuss / Information / Note
To Note
Executive Summary:
Council of Governors Meeting Part 1 13 April 2016
GOVERNOR INVOLVEMENT with PATIENT and PUBLIC ENGAGEMENT (GIPPE) REPORTS 3 February to 13 April 2016
Chair: David Bellamy Meeting Date[s]: 29 February 2016 Key Committee Decisions/Discussions
1. The outpatient survey has received feedback from the Trust and a further follow up will be sent to the committee at the end of the year.
2. Monkey survey questions were ratified by the committee at the last meeting and will shortly be sent out to members. 3.
3.
The survey of elderly patients organised by Keith and Ellen Bull has started. Any Governor wishing to help will need a short training as a volunteer first. Sessions of meeting the public in the atrium will take place 3 monthly the next one being in April. The Trust will feed back on these sessions as quickly as possible.
Activities and Events in Previous Quarter Description Date Attendance and Outcome Monkey survey questions discussed and updated Feb 2016 Future Activities and Events Description Date Location Opportunities for Governors to be Involved New surveys on the wards are being discussed for action later in the year.
Quarter 3
The Survey Monkey questionnaire should be sent out in the next month.
April 2016 Trust membership on email
Governor Sub-Committee Meeting Reports Page 1 of 1 3 February – 13 April 2016

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Involvement with Patient and Public Engagement Committee Work Programme
Section on agenda: Decision
Officer with overall responsibility: David Bellamy
Author(s) of papers: David Bellamy
Details of previous discussion and/or dissemination:
Governor Involvement with Patient and Public Engagement Committee
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary: The Governor Involvement with Patient and Public Engagement Committee is a committee established by and responsible to the Council of Governors.
The primary aim of the Committee is to identify, and where appropriate improve, patient experience.
The Committee have developed the attached work programme so they can fulfil the duties remitted by the Council of Governors.
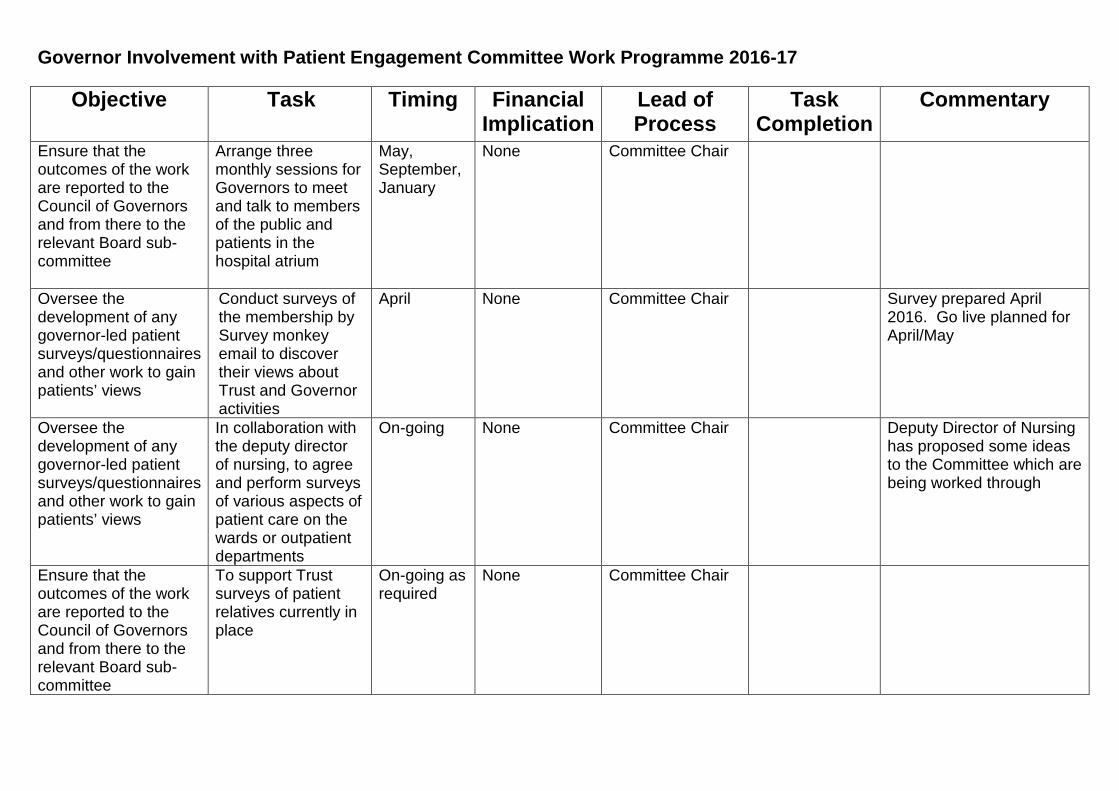
Governor Involvement with Patient Engagement Committee Work Programme 2016-17
Objective Task Timing Financial Implication
Lead of Process
Task Completion
Commentary
Ensure that the outcomes of the work are reported to the Council of Governors and from there to the relevant Board sub-committee
Arrange three monthly sessions for Governors to meet and talk to members of the public and patients in the hospital atrium
May, September, January
None Committee Chair
Oversee the development of any governor-led patient surveys/questionnaires and other work to gain patients’ views
Conduct surveys of the membership by Survey monkey email to discover their views about Trust and Governor activities
April None Committee Chair Survey prepared April 2016. Go live planned for April/May
Oversee the development of any governor-led patient surveys/questionnaires and other work to gain patients’ views
In collaboration with the deputy director of nursing, to agree and perform surveys of various aspects of patient care on the wards or outpatient departments
On-going None Committee Chair Deputy Director of Nursing has proposed some ideas to the Committee which are being worked through
Ensure that the outcomes of the work are reported to the Council of Governors and from there to the relevant Board sub-committee
To support Trust surveys of patient relatives currently in place
On-going as required
None Committee Chair
COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Involvement with Patient and Public Engagement Committee Terms of Reference
Section on agenda: Decision
Officer with overall responsibility: David Bellamy
Author(s) of papers: Sarah Anderson
Details of previous discussion and/or dissemination:
Governor Involvement with Patient and Public Engagement Committee
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary: Proposed change of committee name to recognise its primary aim to “identify, and where appropriate improve, patient experience” rather than engagement.
Change the membership.

The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
PATIENT and PUBLIC EXPERIENCE COMMITTEE (PPEC)
Terms of Reference
The Patient and Public Experience Committee (the Committee) is a committee established by and responsible to the Council of Governors. The primary aim of the Committee is to identify, and where appropriate improve, patient experience. 1. Membership
1.1 The membership of the Committee will consist of the following:
• Six governors including one staff governor • Chairperson of Membership Development Committee
In addition, the following will attend the Committee to provide advice as required: • One Non-Executive Director • Trust Secretary or their representative • Deputy Director of Nursing and Midwifery • Head of Patient Engagement • PALS Manager • Complaints Manager
1.2 Only members of the Committee have the right to attend Committee meetings. The Committee Chairman may invite other governors or any other individual to attend all or part of any meeting, as and when the Committee Chairman considers it appropriate.
1.3 The Committee Chairman shall be a governor and will be elected by
the Committee from amongst its membership annually. 1.4 All governor appointments will be made by self-nomination and a vote
will be taken by the Council of Governors if there are more nominees than vacancies. The ballot will be organised by the Trust Secretary in accordance with a process agreed by the Council of Governors.
1.5 Appointments to the Committee shall be for a period of two years,
which may be extended for one further three year period. The Council of Governors may choose to make appointments for a period of not more than one year greater or less than the period specified in order to
Deleted: GOVERNOR INVOLVEMENT with
Deleted: ENGAGEMENT
Deleted: Governor Involvement with
Deleted: Engagement
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
4 July 2015
April 2017 Trust Secretary
Deleted: 3
Deleted: 6

ensure some continuity of membership of the Committee when vacancies arise. However, only those governors who have served at least one year as members of the Council of Governors shall be eligible for membership of this Committee.
2. Secretary
2.1 The Trust Secretary or their representative shall act as the Secretary of the Committee.
3. Quorum
3.1 A quorum will be three members of the Committee.
4. Frequency of meetings
4.1 Meetings are to be held quarterly and at such other times as may be required.
5. Notice of meetings
5.1 Meetings of the Committee shall be called by the Secretary of the Committee at the request of the Committee Chairman.
5.2 The Committee Chairman will agree the agenda and papers to be
circulated with the Trust Secretary or their representative. 5.3 Unless otherwise agreed, notice of each meeting confirming the
venue, time and date, together with an agenda of items to be discussed, shall be forwarded to each member of the Committee and any other person required to attend, no later than five working days before the date of the meeting. Where possible, the supporting papers shall be sent to Committee members and to other attendees as appropriate, at the same time.
6. Minutes of meetings
6.1 The Secretary of the Committee shall record action notes of the
proceedings of all Committee meetings. They shall also record the names of those present and in attendance.
6.2 Action notes of Committee meetings shall be agreed by the
Committee Chairman prior to being circulated to all members of the Committee. The Secretary of the Committee shall aim to prepare the action notes within one week of the meeting date.
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
4 July 2015
April 2017 Trust Secretary
Deleted: 3
Deleted: 6

7. Duties The Committee shall: 7.1 Oversee the development of any governor-led patient
surveys/questionnaires and other work to gain patients’ views. This work may be undertaken within the hospital;
7.2 Work with the Clinical Audit Department to gain approval for governor
surveys/questionnaires and other work to be undertaken;
7.3 Work with the governors undertaking the survey/questionnaires and other work to ensure that the outcomes of the work are reported to the Council of Governors;
7.4 Through the chair of the Membership Development Committee
(MDC) to ensure the two committees are working together and not duplicating work;
7.5 Work with external stakeholders to understand and improve the
patient experience within the Trust.
8. Reporting responsibilities
8.1 The Committee is a Committee of the Council of Governors and is accountable to it.
8.2 A report by the Committee Chairman shall be submitted to the
Council of Governors at the Council of Governors’ meeting following the Committee meeting. The action notes of the Committee meetings shall be available to governors who are not members of the Committee on request to the Committee Chairman through the Trust Secretary's Office.
8.3 The Committee shall make whatever recommendations to the
Council of Governors it deems appropriate on any area within its remit where action or improvement is needed.
9. Other
9.1 The Committee shall, at least once a year, review its own performance and terms of reference to ensure it is operating at maximum effectiveness. The Committee will report on its performance and recommend any changes it considers necessary to the terms of reference to the Council of Governors for approval.
10. Authority
Deleted: or wider community
Deleted: and from there to the relevant Board sub-committee
Deleted: Work with the governor-led
Deleted: that recruitment and general engagement work is incorporated into the work of the Committee as required
Deleted: <#>Ensure that patient experience issues are reported to the Council of Governors and flagged to the Trust through the Trust Secretary’s office in a timely manner;¶¶
Deleted: HealthWatch and other
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
4 July 2015
April 2017 Trust Secretary
Deleted: 3
Deleted: 6

10.1 The Committee is authorised to assist the Council of Governors in
carrying out its functions. 10.2 None of the powers of the Council of Governors are delegated to
this Committee.
Approval Committee
Version Approval Date Review Date Document Author
Council of Governors
4 July 2015
April 2017 Trust Secretary
Deleted: 3
Deleted: 6
COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Strategy Committee Update
Section on agenda: Information
Officer with overall responsibility: Eric Fisher
Author(s) of papers: Eric Fisher
Details of previous discussion and/or dissemination:
Governor Strategy Committee
Action required: Approve / Discuss / Information / Note
To Note
Executive Summary:
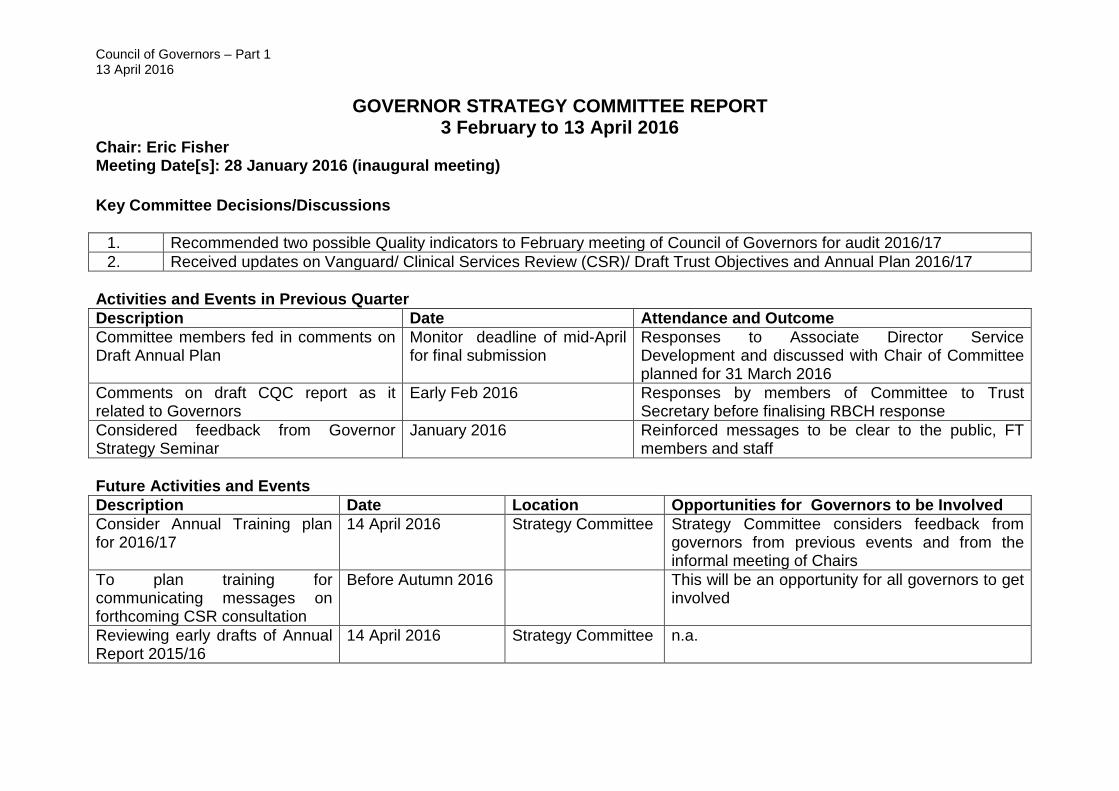
Council of Governors – Part 1 13 April 2016
GOVERNOR STRATEGY COMMITTEE REPORT 3 February to 13 April 2016
Chair: Eric Fisher Meeting Date[s]: 28 January 2016 (inaugural meeting) Key Committee Decisions/Discussions
1. Recommended two possible Quality indicators to February meeting of Council of Governors for audit 2016/17 2. Received updates on Vanguard/ Clinical Services Review (CSR)/ Draft Trust Objectives and Annual Plan 2016/17
Activities and Events in Previous Quarter Description Date Attendance and Outcome Committee members fed in comments on Draft Annual Plan
Monitor deadline of mid-April for final submission
Responses to Associate Director Service Development and discussed with Chair of Committee planned for 31 March 2016
Comments on draft CQC report as it related to Governors
Early Feb 2016 Responses by members of Committee to Trust Secretary before finalising RBCH response
Considered feedback from Governor Strategy Seminar
January 2016 Reinforced messages to be clear to the public, FT members and staff
Future Activities and Events Description Date Location Opportunities for Governors to be Involved Consider Annual Training plan for 2016/17
14 April 2016 Strategy Committee Strategy Committee considers feedback from governors from previous events and from the informal meeting of Chairs
To plan training for communicating messages on forthcoming CSR consultation
Before Autumn 2016 This will be an opportunity for all governors to get involved
Reviewing early drafts of Annual Report 2015/16
14 April 2016 Strategy Committee n.a.

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Strategy Committee Work Programme
Section on agenda: Decision
Officer with overall responsibility: Eric Fisher
Author(s) of papers: Eric Fisher
Details of previous discussion and/or dissemination:
Governor Strategy Committee
Action required: Approve / Discuss / Information / Note
To Approve
Executive Summary: The Strategy Committee is a committee established by and responsible to the Council of Governors. The primary aim of the Committee is to review the Trust’s Annual Plan (its strategic plan) and Annual Report documents on behalf of the Council of Governors. The Committee have developed the attached work programme so they can fulfil the duties remitted by the Council of Governors.

Strategy Committee Work Programme 2016/17 (draft 5 March 2016)
Objective Task timing Financial
implication
Lead of process
Task Completion
Commentary
1. Ensure public engagement views are reflected in Trust’s decisions and priorities
Input & comment on Annual Plan
Jan 16 Dec 16
n.a. Cttee 2016/17 Draft submitted 8 Feb; Considered by Strategy Committee Jan 16. Draft for final submission in April considered in March 16 Need to consider messages for 2017/18 from Dec 2016 Statutory requirement to be consulted during the preparation of the Trust forward plans
2. Ensure CoG work is accurately presented
Review an early draft of the Annual Report
March 16 n.a. Chair and one or more of Cttee members
Early draft 2015/16 Annual Report to be shared with nominated members of Strategy Committee (perhaps by an e-dialogue) Full Council of Governors’ meeting following the Annual Report having been laid before Parliament i.e. July to receive the Annual Report
3 (a) Ensure public engagement views are reflected in Trust’s decisions and priorities
Comment on the Quality Accounts
March 16 n.a. Chair and one or more of Cttee members
TS checking on when early draft is available to be shared with nominated members of Strategy Committee
3 (b) provide a formal response from CoG on Quality account
April 16 n.a. Chair To be delegated from CoG from 13 April 2016 meeting?
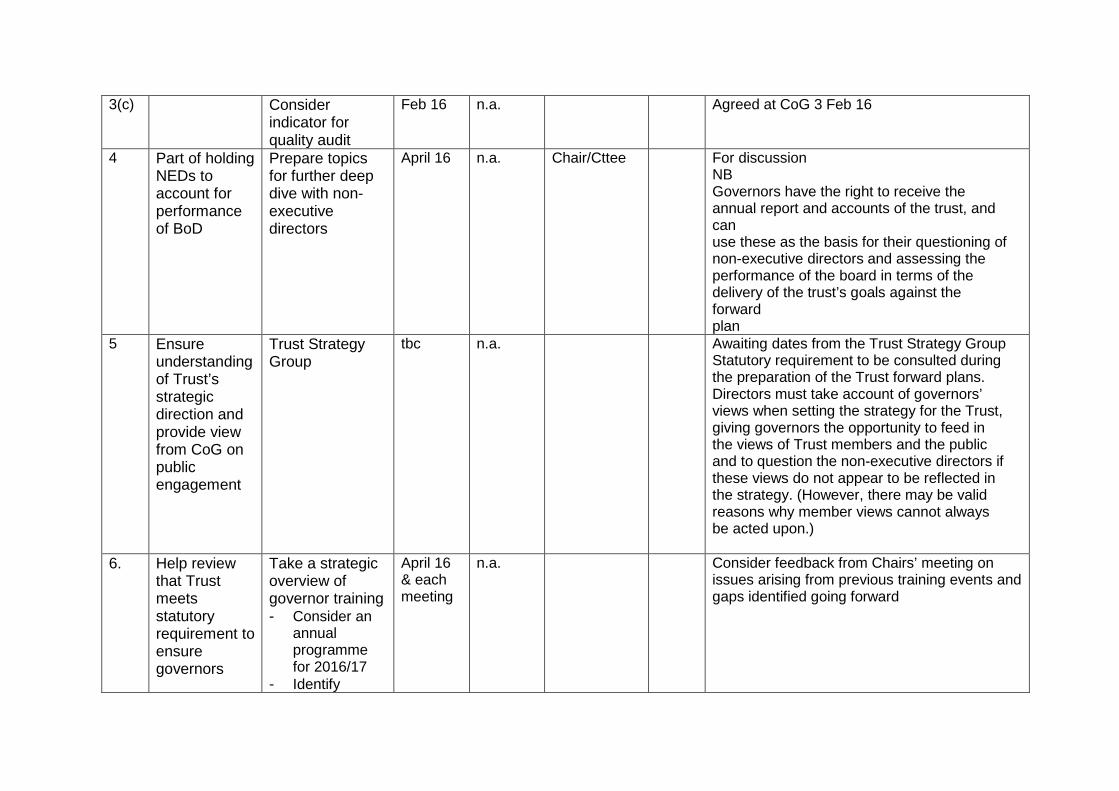
3(c) Consider indicator for quality audit
Feb 16 n.a. Agreed at CoG 3 Feb 16
4 Part of holding NEDs to account for performance of BoD
Prepare topics for further deep dive with non-executive directors
April 16 n.a. Chair/Cttee For discussion NB Governors have the right to receive the annual report and accounts of the trust, and can use these as the basis for their questioning of non-executive directors and assessing the performance of the board in terms of the delivery of the trust’s goals against the forward plan
5 Ensure understanding of Trust’s strategic direction and provide view from CoG on public engagement
Trust Strategy Group
tbc n.a. Awaiting dates from the Trust Strategy Group Statutory requirement to be consulted during the preparation of the Trust forward plans. Directors must take account of governors’ views when setting the strategy for the Trust, giving governors the opportunity to feed in the views of Trust members and the public and to question the non-executive directors if these views do not appear to be reflected in the strategy. (However, there may be valid reasons why member views cannot always be acted upon.)
6. Help review that Trust meets statutory requirement to ensure governors
Take a strategic overview of governor training - Consider an
annual programme for 2016/17
- Identify
April 16 & each meeting
n.a. Consider feedback from Chairs’ meeting on issues arising from previous training events and gaps identified going forward

receive sufficient training
mandatory as against discretionary
- Review VLE compliance re essential core skills (Mandatory) training for governors
7. Annual review of effectiveness of committees
Effectiveness of Strategy Committee
Dec 16 n.a. Chair/Cttee To use this work programme as a basis for this review
BoD – Board of Directors
CoG – Council of Governors
NED – Non Executive Director
TS – Trust Secretary
Cttee - Committee
VLE – Virtual Learning Education
tbc – to be considered
COUNCIL OF GOVERNORS
Meeting Date: 13 April 2016 – Part 1
Subject: 2015/16 Annual Report Production Schedule
Section on agenda: Information
Officer with overall responsibility: James Donald Head of Communications
Author(s) of papers: James Donald
Details of previous discussion and/or dissemination:
Action required: Approve / Discuss / Information / Note
To note
Executive Summary:

Production Schedule for AR, QR and accounts 2015/16
Below is the production timetable for the following statutory documents:
• Annual Report (lead: James Donald, Head of Communications) • Quality Report (lead: Joanne Sims, Associate Director of Clinical Governance) • Financial Accounts (lead: Mike Wilkinson, Finance)
The following versions will be produced and distributed to the following groups/committees:
• Version 1: Draft Annual Report (Word format) distributed to the CoG on training day
– 18 March • Version 2: Draft Annual Report, Quality Accounts (not designed) distributed to the
April Board (incorporating comments from the CoG) • Version 3: Final Draft Annual Report, Quality Accounts and Financial Accounts (in
design format). It is at this point that the three documents are presented as one. • Version 4: Final Annual Report, Quality Accounts and Financial Accounts to the
Audit Committee and Board of Directors for approval and sign off.
Who 1 February Requests for information for Annual Report
sent out to Directors and Heads of Department – deadline for content Friday 26 February
Head of Communications
February Internal requests sent out for Quality Report content e.g. Trust leads and governors
Joanne Sims
February Agree indicators to be audited – deadline 13 February CoG.
Joanne Sims and Sarah Anderson
March External consultation on the Quality Report content e.g. Healthwatch, governors, council. JS to create presentation.
Joanne Sims
Early April Deadline for all Quality Report content to Joanne Sims – first draft to be complete by 12 April
All directors/leads
13 April CoG to receive verbal outline of draft Annual Report
Head of Communications Sarah Anderson Jo Sims
March - June
Design work: • Annual Report – draft to be completed
by 21 April. • Quality Accounts – to be complete by ??
May and first word draft completed by 21 April
• Financial Accounts – to be completed by end of April
Head of Communications Joanne Sims Mike Wilkinson
21 April • submit Version 1 of Draft Annual Report, Quality Account to Trust Secretary for April BoD (29 April)
Head of Communications Joanne Sims
?? April Submit combined AR, QR and Accounts Mike Wilkinson
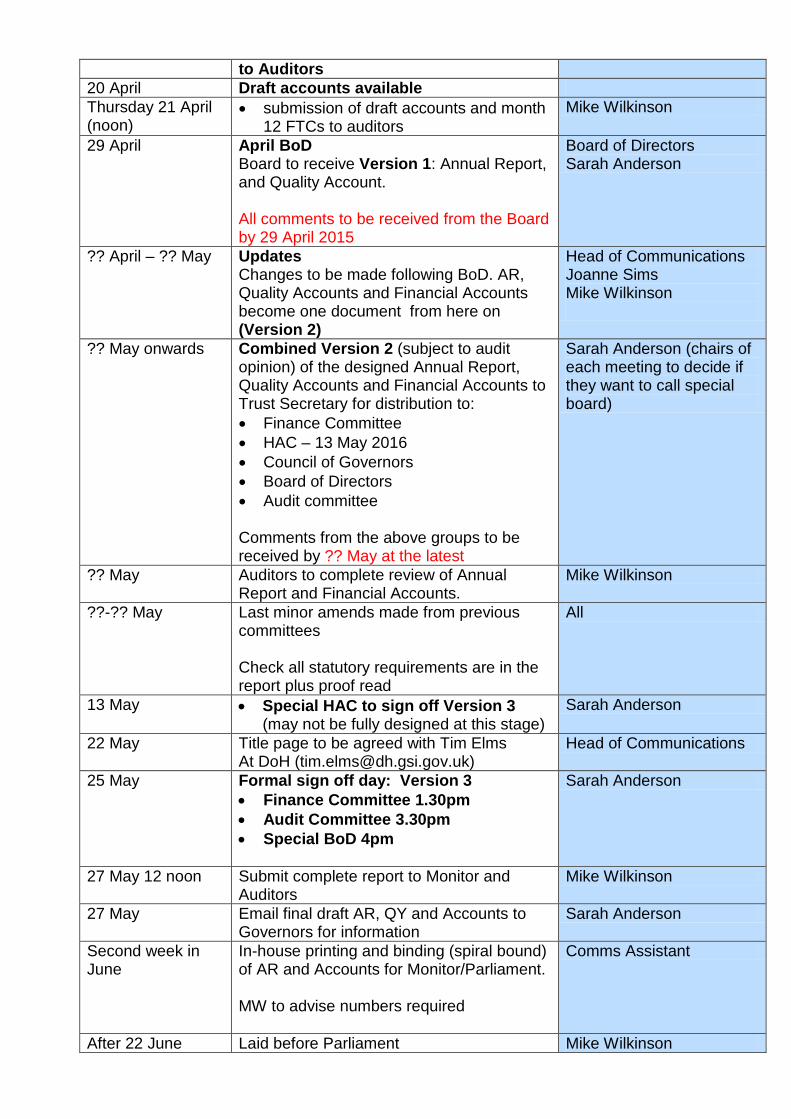
to Auditors 20 April Draft accounts available Thursday 21 April (noon)
• submission of draft accounts and month 12 FTCs to auditors
Mike Wilkinson
29 April
April BoD Board to receive Version 1: Annual Report, and Quality Account. All comments to be received from the Board by 29 April 2015
Board of Directors Sarah Anderson
?? April – ?? May Updates Changes to be made following BoD. AR, Quality Accounts and Financial Accounts become one document from here on (Version 2)
Head of Communications Joanne Sims Mike Wilkinson
?? May onwards Combined Version 2 (subject to audit opinion) of the designed Annual Report, Quality Accounts and Financial Accounts to Trust Secretary for distribution to: • Finance Committee • HAC – 13 May 2016 • Council of Governors • Board of Directors • Audit committee
Comments from the above groups to be received by ?? May at the latest
Sarah Anderson (chairs of each meeting to decide if they want to call special board)
?? May Auditors to complete review of Annual Report and Financial Accounts.
Mike Wilkinson
??-?? May Last minor amends made from previous committees Check all statutory requirements are in the report plus proof read
All
13 May • Special HAC to sign off Version 3 (may not be fully designed at this stage)
Sarah Anderson
22 May Title page to be agreed with Tim Elms At DoH ([email protected])
Head of Communications
25 May
Formal sign off day: Version 3 • Finance Committee 1.30pm • Audit Committee 3.30pm • Special BoD 4pm
Sarah Anderson
27 May 12 noon Submit complete report to Monitor and Auditors
Mike Wilkinson
27 May Email final draft AR, QY and Accounts to Governors for information
Sarah Anderson
Second week in June
In-house printing and binding (spiral bound) of AR and Accounts for Monitor/Parliament. MW to advise numbers required
Comms Assistant
After 22 June Laid before Parliament Mike Wilkinson

By 24 June at the latest
Submitted Accounts to Parliament
Mike Wilkinson
By 11 July Full annual report and accounts as laid before Parliament to be sent to Monitor
Mike Wilkinson
21 July CoG Governors to receive the AR, QR and Accounts
Trust Secretary
10 September Members’ meeting Annual Review summary required
Head of Communications (lead) Joanne Sims Mike Wilkinson Trust Secretary
*NB:
• External auditors will receive the Quality Accounts separately from the Annual Report

COUNCIL OF GOVERNORS
Meeting Date: 13 April 2016 – Part 1
Subject: October-December 2015 Governor Listening Event feedback
Section on agenda: Information
Officer with overall responsibility: Ellen Bull, Deputy Director of Nursing, Midwifery and Healthcare Assistants
Author(s) of papers: David Bellamy
Details of previous discussion and/or dissemination:
Governor Involvement with Patient and Public Engagement Committee
Action required: Approve / Discuss / Information / Note
For information
Executive Summary:

Governor Listening Events Monday 19 October, Tuesday 24 November and Monday 14
December 2015 13:00 – 17:00 Main Atrium
Concerns and Complaints
• Daughter of mother 82. Admitted with D&V - hospital said not C'diff, other daughter insisted it was C'diff! Has complained through PALS, has had two replies both with excuses 'rubbish'! Unhappy ladies.
• Carer from Totton (Southampton), patient had cardiac stent and kept in
overnight, whist in had a fall, still in RBH after two weeks. They were expecting discharge last week but told that his care package was not ready. Carer was directed to PALS.
• (I feel that this could be another example of problems of discharge over CCG county boundaries?)
• One patient had had a very poor experience in our hospital. She had been
admitted for lumber puncture treatment with steroids, which she was unfortunately allergic to. This had led to a catalogue of ill health and she requires constant nursing care by her daughter. They feel neglected by the lack of concern given by our hospital and wonder when the nightmare is going to end. I was given their telephone number if required.
• Patient had had a poor knee operation and was awaiting a revision replacement.
• Phoned AMU at night and no answer - husband had been moved to a ward
but wife had not been informed
• Some staff on wards don't have time to listen to people's needs
• Pre assessment information not always passed on to the wards
• Sharing information between hospital and external organisations not always good
• Waited 3 hours for outpatient appointment - but informed of delays You said…….
I spoke to a gentleman who was admitted to the Derwent on the 23rd of October this year for a knee operation and was on the ward for about 11 days and was in bed 6. The gentleman had a range of problems whilst on the ward but was most concerned about how he was treated by two members of the night staff. I advised him to go to PALS but he did not want to complain. I tried to explain that PALS were there to try and make improvements in the Trust when things went wrong and it needn't be seen as a complaint. It appears that the gentleman may have got an infection in his knee. It sounds as if there may have been some other difficulties Ashe also had a catheter installed. During the night of 27th October (not sure of the exact date) he got
up to go to the toilet. When he pulled on the handle it broke and he fell backward half landing on a chair and spilling his catheter bag. A male member of staff came in to see him and asked if he was ok. The gentleman answered saying 'does it look as if I am ok?' The male member of staff then said ' if that was how he was going to talk to him he was going' and left the patient where he was. The patient eventually managed to get himself up and got him self into bed. Sometime later a female member of staff come to see him and was very brisk with him. This patient has had many dealings with the hospital and has always found the standards excellent. He also said the day staff were excellent. He also has problems with his other knee but has said there is no way he will return to Bournemouth Hospital to have that looked at after his experience at the Derwent.
His wife said he is a changed man know and has lost all his confidence, he used to be such an outgoing person. He was close to tears on several occasions whilst I was talking to him. I would be grateful if you could pass this on to the appropriate person.
We did…… I’m not sure that there is much I can do without his name and without his consent, especially as he has declined speaking to PALS about his experience. The difficulty I have is that without the patient’s details I am unable to investigate fully. If we had the gentleman’s name the Trust could do a full review as it does appear that there are important learning points to review and action. Public Toilets – actioned by PS on 20 October You said…….
• There was concern re the conditions of the public toilets - this did not conform to the hygiene expected in a hospital.
• Several people this afternoon complained re the standard of hygiene in the public toilets.
We did…… Actioned by Trust as soon as the information was received. Housekeeping informed and all public toilets were inspected and cleaned. Transport
• Car parking o availability of spaces,
We are limited by the local authority in the number of spaces we can provide.
o Cost Cost reflects the need to manage the car parks and keep them in good order, cost is in line with or cheaper than other nearby Trusts
o Leaving the hospital at 4.30 needs to be improved. We are working with the council and others to provide an alternative exit from the hospital on to the Wessex Way.
o Difficult to “drop off” disabled / long term disabling medical condition passengers e.g. COPD or cardiac, near to where they need to go. long walk from disabled parking to some clinics

we have provided additional drop off points around the car parks, for Cardiac patients the closest disabled spaces are at the Rehabilitation entrance
o Difficulty parking with access to some of the departments at the back of the hospital. As above there are new set down spaces and we have improved the layout for patient parking, We are limited by how many spaces we can provide
o difficulty of parking for Community Volunteer drivers See above
o what facilities are offered to relatives visiting ITU/long term patients or patients who are receiving long term treatment e.g. oncology e.g. free car parking The Trust offers free parking for the above group and this is agreed with the department locally.
• Patient transport o Process confusing o internal bus needs to be more frequent
Respect and Dignity
• Reception areas o Privacy when booking in or discussions with reception staff
• Wards
o Privacy receiving treatment and information with only a curtain between patients. Patients become distressed being able to hear other patient’s diagnosis and treatments
• Treatment o When phoning the ward, staff unaware of husband’s condition after his
operation. Wife was informed he would call her on his mobile later. Pharmacy/Drugs
• Waiting times • Small room and perceived risk of infection for cancer patients from other
patients • Why is there a need for a retail chemist? • The length of time to receive drugs from Pharmacy when patients are
discharged • Pain relief • Long walk to pharmacy after treatment in the jigsaw building eg Bristol
Hospital has a pharmacy in the cancer unit. • Specific example of delay in providing pain relief during a procedure • Clinical advice
o Conflicting advice re medication received from two specialties
We did:

• We are working in partnership with BOOTS UK to provide an outpatient pharmacy service offering safe, high quality, and patient centred care.
• BOOTS UK is planned to open 9th March 2016 and will offer a range of services including dispensing outpatient prescriptions, advice regarding medication, a room to discuss medication in private, advice on community pharmacy services and offer a range of over the counter medicines and retail products. This will improve both the waiting times and the area in which patients will have to wait.
• Key benefits of the partnership: o A dedicated outpatient pharmacy and waiting area with a service run
by a third party pharmacy company to reduce waiting times o RBCH pharmacy staff will further improve the service to inpatient and
discharge patients allowing a faster turn around time and supporting the availability of beds
o Provide another area to gain pharmacy advice and signposting to community pharmacy services, support patient and relatives care.
o Sales of over the counter medicines to support our A&E department as appropriate.
Blood Tests
• Long wait for blood tests i.e. 2 hour wait. • Blood test area very poor – very tired
Refurbished in 2015 • not a enough seats especially when there are long waits • hard seats • Is there a possibility of an ‘appointment’ window?
Infection Control • Lack of public gelling hands on entry to the building • Staff cleaning hands between patients when taking blood pressure • No cleaner seen on a ward by patient • High cleaning not seen to be done by patient • Patient suggested that door handles should be of metal plate or copper which
is resistant to harbouring germs; the patient had read about this but also it was passed through television media., will consider these for new works in conjunction with IPCC
Suggestion for improvement • facilities for iced water or chilled water for patients
we have installed water coolers in areas where this is practical taking account of IPCC and engineering concerns
Patient Services • Appointments
o Waiting time to get an appointment o Changed at short notice – can be confusing to patients o Timing to allow access by public transport o Ability to consider related issues in clinics o Appointment letter to indicate the nearest car park to the clinic
work is underway to review wayfinding and this includes nearest car park information

o Reminder letters sent – why could these not be by text/email? o Could issue directions/map with appointment letter
information is being updated and this includes a new map. Information is available in the internet
o Eye Unit - the appointment letters are silent on the treatment(s) expected during appointment.
Environment • Atrium - explanation of improvements required
there are plans showing what is happening exhibited in the atrium, the work has created space for the RVS café and the new Chemist service
• Entrance/reception area to Jigsaw building is cold with doors keeping opening over door heater fitted and design of Jigsaw/Eye unite entrances to be undertaken
• LCD display in the Atrium would be useful • facilities for iced water or chilled water for patients
we have installed water coolers in areas where this is practical taking account of IPCC and engineering concerns
Comments made by staff included: • Morale of nursing staff • Relationship between consultants and management and nursing staff
Concerns • Phoned AMU at night and no answer - husband had been moved to a ward
but she had not been told • Some staff on wards don't have time to listen to people's needs • Pre assessment information not always passed on to the wards • Sharing information between hospital and external organisations not always
good • Waited 3 hours for outpatient appointment - but informed of delays
Attitude/Interpersonal
• Orthopaedics highlighted as a more negative experience • Patient felt asked same question time after time- “notes on the computer they
don’t read it” • “We’ve done the job, just take some pain killers” “ Consultants don’t seem
interested” ( patient subsequently went elsewhere for second knee op after having a second opinion. Reported experience elsewhere as far better, continuity of care
• Here, you do not know who you are going to see/ never the same person/ one of the team
• Communication and command of English queried
Waiting Times/Pressure of work • Seen as the only “requires improvement” element by one patient.
Understands it is pressure of work /capacity in endoscopy. Recited how initially referred in November 2014, was only seen in May 2015 due to appointments constantly being cancelled. While this patient was

understanding of the pressure on the Trust, many patients may not understand why this is happening
• Similarly within the Eye Unit similar pressures were recognised. Very long waits in the Unit (non-emergency) always 1-2 hours.
• Eye Unit described as “ completely overwhelmed/ not enough room”
Suggestions put a water fountain in waiting areas so that people can have a drink if needed see previous response
Observations
Woman who had lived in South Africa, now living in Bournemouth. Free medicine can lead to abuse as people consult their GP for minor ailments thereby delaying time when patients with more serious conditions can get an appointment. Suggested a modest contribution be required for each GP appointments to solve this problem Husband came back from pathology where he had had to wait for an hour. He did not see this as a problem. They pointed out that one hour wait is not really waiting when you have lived in a country like South Africa where the norm is more like 6 to 8 hours waiting. Managing patient expectations is key.

COUNCIL OF GOVERNORS
Meeting Date: 13 April 2016 – Part 1
Subject: Governor Concerns Log
Section on agenda: Information
Officer with overall responsibility: Sarah Anderson, Trust Secretary
Author(s) of papers: Dily Ruffer
Details of previous discussion and/or dissemination:
Staff members who deal with the items concerned and then forwarded to the individual Governors who have raised the concerns.
Action required: Approve / Discuss / Information / Note
For information
Executive Summary:

Governor Raised Concerns
DATE RAISED CONCERN / ISSUE RESOLUTION February 2016 Christchurch Hospital
How many “community beds” will there be at the new build site at Christchurch Hospital nursing home including step-up, step-down and rehab beds?
The securing Christchurch Hospital project required enabling funds. These are generated from the commercial activities of the Nursing Home and Senior Living. Without these, Christchurch Hospital would not have had the funding to continue. Both the Nursing Home and Senior Living are operated on a commercial basis. They are targeted at the top end of the market and have a commercial strategy reflecting this. If the Nursing Home decides to accept a limited number of patients at social services rates, we will access these through our interim care scheme. Our preliminary discussions are positive but it is for the Care Home management to decide. We will continue to work with all homes that meet our quality, price and patient criteria to allow interim placements. We will keep the governors updated to the opening of the Nursing Home and our discussions with the management team there.
February 2016 Christchurch Hospital - Phlebotomy Department Morning, main doors apparently are opened at 08-15 for patients. However, when they arrive at the department there are already 10 to 15 people already there. The question I was asked was 'how do these patients get ahead of the queue at the main entrance?'. Are these patients accessing via the Mac Unit? If that is so, would this constitute a security risk? Can access Phlebotomy be
Having investigated I can confirm that no patients have access to Phlebotomy until the phlebotomists arrive and unlock. When they do this however there are usually approx. 10 patients waiting in the corridor outside because at this time of day the porters open the access doors to allow patient access to various parts of the Christchurch site and patients for requiring phlebotomy may enter by any of these and find their way to the corridor outside of phlebotomy.
Updated 06 April 2016 Page 1
accessed without going through the main entrance?
March 2016 Christchurch Hospital - Phlebotomy Department I attempted to visit your Blood Test department at 15.00 hours yesterday and found it had closed early due to an inability to deal with the demand. One paid the car park fee and then was told of the situation. There was no Notice warning people not to waste their money I went again this morning, arriving at 08.30 (half an hour before the official opening time ) only to find the waiting room completely full with about 70 / 80 people. The service started on time at 09.00 and I eventually left at 10.00 hours By this time the queue had increased to well over 100 with an overflow seated room completely full and elderly people having to stand waiting in the n the corridor. I was told by the Technician that this had been the norm - waiting times of 2 hours or more - for over a week and there was no sign of it reducing. Please respond to the following: • only 2 technicians on duty instead of the
normal 5 • a need to shut the facility down at
15.30 each day because of an inflexible
For 2 weeks we have experienced severe and extraordinary difficulties with staffing resulting from sickness which has impacted both Bournemouth and Christchurch phlebotomy services. This is now resolving. Staff returning from long and short term illness will gain further support from filled vacancies for which an advert closes today. In the longer term we will be implementing an appointment system which will mitigate extended waits for phlebotomy. The practice of closing at 15:30 at Christchurch is long standing and although this does coincide with transport back to RBH it is also aligned to the normal demand. We regularly review the footfall at all sites and will consider amending opening times should there be sufficient requirement to do so.
Updated 06 April 2016 Page 2

transport pick-up arrangement to collect blood samples
Updated 06 April 2016 Page 3
COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Forward Planner
Section on agenda: Information
Officer with overall responsibility: Sarah Anderson
Author(s) of papers: Dily Ruffer
Details of previous discussion and/or dissemination:
Various
Action required: Approve / Discuss / Information/Note
To note
Executive Summary:

Council of Governors Forward Programme 2016
What Who Where Before Jan Apr May Jul Sept Oct Where AfterAnnual PlanAnnual Plan - Draft for Public Consultation RR TMB Part 2 BoDAnnual Plan - Feedback from Consultation to COG RR TMB Part 2 BoD
Annual Report & AccountsAnnual Report & Accounts First Draft SH BoD Part 2 BoDAnnual Report & Accounts - Final draft presented SH BoD & Audit Cttee Part 2 Monitor/Parliament
QualityInpatient Survey Results PS BoD N/AOutpatient Survey Results PS BoD N/AQuality Performance Report PS BoDPLACE Inspection PS HAC N/AQuality Accounts - First Draft PS Clinical Governance Part 2 N/AQuality Accounts - Final Draft presented PS Clinical Governance Part 2 Publication
Election ResultsLead Governor Election DR N/A N/APublic Governor Election DR N/A AMMStaff Governor Election DR N/A AMM
Infection ControlInfection Control - Annual Report PS BoD N/A
Constitutional DocumentsConstitution Trust Sec Constitution Grp/BoD MonitorStanding Orders Trust Sec Constitution Grp/BoD MonitorPolicy on Composition of COG Trust Sec Constitution Grp/BoD BoDMembership Development Strategy CA MDC BoDPolicy on NED Composition Trust Sec NED Nom/RemCo BoD
GovernanceRegister of Interests Trust Sec Trust Secretary FileMeeting Dates for Next Year Trust Sec Trust Secretary N/AForward Programme Trust Sec Trust Secretary N/AActions Matrix Trust Sec Trust Secretary N/AAnnual Members' Meeting Trust Sec MDC TBC N/AGovernor Attendance Trust Sec NED RemCom Part 2* Part 2* Part 2* Part 2* N/A*if required

What Who Where Before Jan Apr May Jul Sept Oct Where After
Reports from COG Committees/GroupsGovernor Involvement with Patient and Public Engagement Committee DB N/A N/AMembership Development Committee CA N/A N/ANon-Executive Director Nomination and Remuneration Committee JS N/A Part 2* Part 2* Part 2* Part 2* N/AGovernor Strategy Committee EF N/A N/A*if required
Reports from Trust-led Committees/GroupsCharitable Funds Committee GS N/A N/ADiversity Committee EF N/A N/AEditorial Group Various N/A N/AEnd of Life Strategy Group KM N/A N/AFinance Briefing Group PM/RP/GS N/A N/AHealthcare Assurance Committee EF/IK N/A N/AInfection Control KM N/A N/AOrgan Transplant Committee SB N/A N/APatient Information Group (PIG) DB N/A N/AValuing Staff and Wellbeing KM N/A N/AWorkforce PMc N/A
Performance ReportingFinancial Reporting SH BoD N/APerformance Reporting RR BoD N/AQuality Performance PS BoD N/AWorkforce KA BoD N/A
Review Performance & Terms of Reference of Subordinate Committees and GroupsGovernor Involvement and Patient and Public Engagement Committee DB N/A N/AMembership Development Committee CA N/A N/ANon-Executive Director Nomination and Remuneration Committee JS N/A N/AGovernor Strategy Committee EF N/A
General ReportsNHS Providers All N/ASWGEN All N/A N/A
COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Trust Committee Reports
Section on agenda: Information
Officer with overall responsibility: Committee Chairpersons
Author(s) of papers: Governor Representative who sits on the committee
Details of previous discussion and/or dissemination:
Various
Action required: Approve / Discuss / Information / Note
To note
Executive Summary:

Council of Governors Meeting Part 1 3 February 2016
TRUST COMMITTEE MEETING REPORTS 3 February - 13 April 2016
CHARITABLE FUNDS COMMITTEE Governor Representatives: Graham Swetman Meeting Dates: 4 February 2016 Key Decisions/Discussions/Actions
1. We discussed the performance of our investment manage – Quilter. We concluded that, while the value of invested funds had declined, they had performed reasonably well in turbulent markets.
2. We reviewed a revised long-term plan, with a reduction in the fund raising target from £4million to £3million in 2021. It was noted that even this reduced target would require an increase in the Charities Office staff from 7 to 15. This staffing would be kept under review in the light of progress.
4. The value of the fund had reduced by £284,000 in the period, largely as a result of the reduction in legacies (which are always a volatile source) and the unrealised investment loss of £115,000. Almost half of the fund of £5.2 million is reserved for Jigsaw Building commitments.
5. With the pressure on NHS finances, there is a continuing concern that proposals for charitable funding are being received for items which properly belong within the NHS budget. A set of guidelines for the use of charitable funds was reviewed and agreed.
6. Requests for continued funding for a Film Production Officer and a Community Palliative Care Sister were approved. A request for funds for Intra Aortic Balloon Pumps was referred back for further information
7. There was a discussion around the use of charitable funds for Christmas expenditure for both staff and patients, and also for the Pride Awards.
EQUALITY AND DIVERSITY COMMITTEE Governor Representative: Eric Fisher Meeting Dates: No meeting held since last Council of Governors meeting
Trust Committee Meeting Reports Page 1 of 4

Council of Governors Meeting Part 1 3 February 2016 END OF LIFE STRATEGY GROUP Governor Representatives: Keith Mitchell Meeting Dates: Held Monthly Key Decisions/Discussions/Actions
1. Dying Matters Week: The theme for ‘Dying Matters Week’ is ‘The Big Conversation’ 9-15 May 2016. Some of the ideas bought to the group included a ‘Death Café’ with facilitators, tea and cake. ‘Death Bus’ which can travel around.
2. Where people go to die Audit: An audit of patients of where they die whilst on the personalised care plan for the last days of life (PCPLDL) was discussed.
3. Macmillan unit volunteers Volunteers who spend time with patients undertake two and a half days training before they are able to interact with patients. They also have a volunteer co-ordinator to ensure that everything is running smoothly and are available if the volunteers need advice or information.
4. Understanding Health Talk - Preparing for End of Life Care The event went very well with about 80 people attending. Sean Weaver and Ros Pugh gave an excellent presentation and answered many questions from the public and also stayed on after the presentation to speak to people individually. The event was well supported by several other organisations who had stands on the day. We also had 10 governors helping at the event. A few of the audience also joined the Trust as members.
GOVERNOR FINANCE BRIEFING GROUP Governors: Graham Swetman, Paul McMillan and Roger Parsons Meeting Dates: 1 February 2016 Key Decisions/Discussions/Actions
1. We reviewed the decline in sales at BPH, which was mostly due to one consultant working elsewhere. We learnt of plans to re-launch the programme, with help from an external investor.
2. We discussed Lord Carter’s productivity and efficiency review, which used benchmarking to identify high cost areas of the hospital.
3. We noted the progressive reduction in the deficit which had been achieved during the year, and the success in achieving a better-than-expected result from the CIP.
4. We learnt that the Trust could potentially receive £7.6 million from the Sustainability and Transformation Fund, which would lead to the 2016/7 deficit being reduced to £1.7million. Conditions attached to this funding include a plan to achieve seven-day services, and a credible plan to achieve the control total deficit for next year. Fund release will be subject to a quarterly progress review.
Trust Committee Meeting Reports Page 2 of 4

Council of Governors Meeting Part 1 3 February 2016 HEALTHCARE ASSURANCE COMMITTEE Governor Representatives: Eric Fisher and Ian Knox Meeting Dates: 25 February 2016 and 31 March 2016 Key Decisions/Discussions/Actions
1. Regular reports on improvements and issues on the Quality Dashboard and patient feedback were presented by the responsible Head of Nursing with assurance being made on the actions being taken. Additionally, the Trust’s Risk Management processes are reviewed and mitigation against new risks considered.
2. Continuing emphasis is being placed on the proven methodology on Quality Improvement (QI) and this was highlighted by the work from the Improvement Team on removing discharge delays and encouraging each clinical group to take responsibility to comply with the Five Daily Actions
3. The Information Governance return required for the year ending 31 March 2016 demonstrated enormous progress (including on mandatory training) since this was highlighted as a key risk. The Trust has concluded that a satisfactory standard has been reached with work still to do. The Trust will not sign off the final contingency plans until they have been fully tested, but this will be a priority in the new financial year.
4. A final report on the PLACE survey for 2015 was presented and discussed against other evidence produced. Given the nature of the assets, it will not be possible to make further improvements without a large investment (estimated at in excess of £1m).
5. Response times on responding to complaints have improved, but there is still a long way to go. The publication on the Trust web site of “learning from complaints” was approved.
6. The quality trajectories for 2016/17 were discussed, having first been reviewed by Quality Audit & Review Committee (QARC). Some progress had been made on key quality priority areas, but relatively high levels of significant pressure ulcers continue to be a matter of concern.
7. CQC Action Plans were recommended for approval 8. A reports were received from the Medication Governance Committee
and on the monthly mortality
Trust Committee Meeting Reports Page 3 of 4
Council of Governors Meeting Part 1 3 February 2016 INFECTION PREVENTION AND CONTROL COMMITTEE Governor Representative: Brian Young Meeting Dates: No report submitted ORGAN TRANSPLANT COMMITTEE Governor Representative: Sarah Berridge Meeting Dates: No report submitted PATIENT INFORMATION GROUP (PIG) Governor Representative: David Bellamy Meeting Dates: No report submitted VALUING STAFF AND WELLBEING Governor Representative: Keith Mitchell Meeting Dates: KM unavailable to attend the last meeting held WORKFORCE COMMITTEE Governor Representative: David Triplow Meeting Dates: No meeting held since last Council of Governors meeting
Trust Committee Meeting Reports Page 4 of 4

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Reports from Appointed Governors
Section on agenda: Information
Officer with overall responsibility:
Author(s) of papers: Appointed Governors
Details of previous discussion and/or dissemination:
Action required: Approve / Discuss / Information / Note
To note
Executive Summary:
Council of Governor – Part 1 13 April 2016
Report of activities from Appointed Governors
Philip Copson The Royal Bournemouth and Christchurch Hospitals Volunteers Group
The Patient Engagement and Voluntary Services Team Since my last report for the 5 November CoG, among many other things, members of the Patient Engagement and Voluntary Services Team: - have received the Trust Pride Award - risk assessments have been updated - made preparations for the Smile magazine presentation - have contributed to the NHS Recruitment Day - have conducted Essential Core Skills training - had support meetings with various specialist volunteer groups - have arranged Dementia Training for volunteers - have provided Twiddle Mitts for Dementia Patients and baby hats for the Birth Unit - held a young volunteers Stakeholder Event in the Conference Room - have conducted specific training sessions for end of life care and major incident volunteer groups - introduced Hydration volunteering - attended NAVSM meeting and presented on "Developing Youth Volunteering In Health and Care - presented to governors on the February Training Day - attended volunteer recruitment events at St. Peter's School and Brockenhurst and Bournemouth/Poole Colleges. My Personal Involvement I have continued the activities I outlined in "My Initial Involvement" in the 5 November CoG report but have also:
- increased my meetings with individual volunteers in different hospital environments to ensure their satisfaction and to convey our gratitude
- visited volunteers at Christchurch Hospital - assisted at the End Of Life Care presentation at Kinson Community Centre. - Monitored the progress of Keith Mitchell's "Time To Care" report in informing RTPF
practice - advertised Trust Membership at Essential Core Skills sessions.

COUNCIL OF GOVERNORS
Meeting Date: Wednesday 13 April 2016 - Part 1
Subject: Governor Additional Activity Report
Section on agenda: Information
Officer with overall responsibility: Bob Gee
Author(s) of papers: Eric Fisher
Details of previous discussion and/or dissemination:
Public Engagement Event organised by Dorset Clinical Commissioning Group (CCG) in connection with the Clinical Services Review and Vanguards
Action required: Approve / Discuss / Information/Note
To note
Executive Summary:
Report by Eric Fisher to Council of Governors 13 April 2016
Public Engagement Event at Wimborne 30 March 2016
Organised by Dorset Clinical Commissioning Group (CCG) in connection with the Clinical Services Review and Vanguards
Wimborne is one of nine public engagement events organised by Dorset CCG across Dorset, including Bournemouth, Christchurch, Poole at the end of March/ beginning of April; The public event at Wimborne attracted some 70 people to the Allendale Centre, Wimborne, starting at 6 pm and finishing 8.30.
The format consisted of : o Asking attendees to complete a card on “What do you think – 5 areas “you
feel we need to consider when developing community health & care services in East Dorset”; this was then discussed in small groups with key themes shared by CCG facilitators;
o The (short) presentation by Sally Sandcraft (Deputy Director Review Design and Delivery from Dorset CCG) on health & care community services, a copy of the poster walk through displays and making your views known can be accessed by http://www.dorsetccg.nhs.uk/involve/current-engagement/ICS%20events%20have%20your%20say.htm
o An hour plus was allocated to allow attendees view the displays covering “Our vision..informed by local people”; Different care models; Castleman Community Vanguard covering integration of the
Wimborne Minor Injuries Unit, Out of Hours and GP services, developing the Victoria Hospital, Wimborne into a hub, community diabetes and integrated Orthopaedic, Rheumatology & Musculoskeletal (MSK) services ;
Virtual wards; Voluntary Sector, young people, blood services, Mental Health,
maternity and Paediatric. o Attendees were given yellow stickers to comment upon where they supported
the proposals and pink ones where there were questions; these were supported by CCG facilitators (as well as me as a patient & public rep on the Castleman Community Vanguard) answering questions and encouraging attendees to make comments;
Members of the public are encouraged to make their views known through completing a “What do you think?” card in writing or through the web site link (see above);
Dorset CCG has stated that it will review the proposals as part of the Clinical Services Review at its Governing Body meeting on 18 May 2016;
Dorset CCG has also stated that if the proposals are approved, they will be independently scrutinised as part of a national assurance process. Subject to this assessment, public consultation will begin in September 2016 at the earliest.
Eric Fisher 1 April 2016