title - xxx speaker’s name etc implementing paediatric procedural sedation in emergency...
TRANSCRIPT
Title - xxx
Speaker’s name etc
Implementing paediatric procedural sedation in emergency departments- 2013
Nitrous oxide
Gerry SilkPaediatric Nurse Consultant
Nitrous oxide

What is it?
• Anaesthetic gas with analgesic/sedative properties
• Rapid onset/offset
• Delivered in variable concentrations with oxygen
• Requires some degree of cooperation
• 2 forms: • Continuous flow
• 0-70% N20: 100%-30% 02• Demand flow
• Entonox (50% N20: 50% 02)
• Piped or cylinder

Nitrous oxide – indication and contra indication
INDICATION:
• Short painful procedures in cooperative children
• Useful for suturing, IV insertion, foreign body removal, minor fracture
CONTRAINDICATIONS:
• Child < 1 year
• Acute respiratory infection (URTI) or exacerbation of asthma
• Risk of expansion of air-filled closed space
– Pneumothorax, lung cyst, bowel obstruction, middle ear disease
• Increased risk of neuro-toxicity or bone marrow depression
Nitrous oxide – adverse effects
• Vomiting and aspiration
• Dizziness, light-headedness
• Excessive drowsiness with loss of airway
• Expansion of air-filled closed space: • pneumothorax, bowel, middle ear
• Increased intracranial pressure
• Risk to staff
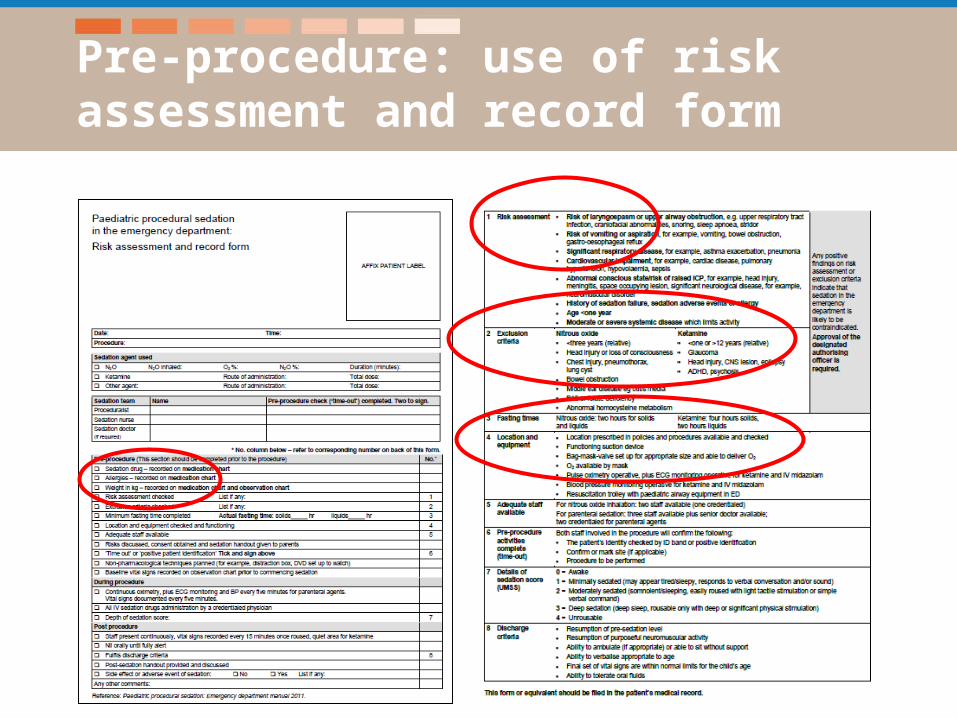
Pre-procedure: use of risk assessment and record form
Pre-procedure: child suitable for sedation
Positive feature(s) on risk assessment or
exclusion criteria
Procedural sedation in ED not
appropriate for this patient!!!

Pre-procedure: fasting
• Somewhat controversial
• Nitrous oxide• 2 hours solids and liquids
Pre-procedure: parent information and consent
• Local context/policy needs to include
• explain the procedure to the child and parent
• gain parent/family consent
• consent must be informed
• consent should be documented
Staff
• Trained in paediatric life support• Staff trained and credentialed in use of sedation• Correct mix of staff to carry out the procedure
and sedation• Team approach
A clinician (doctor or nurse) credentialed in nitrous oxide use to perform the sedation and monitor the child
A clinician (doctor or nurse) to perform the procedure
Prepare child and parent for the procedure with sedation
• Build trust and rapport with the parent and child
• Explain the procedure and sedation to the parent and child
• Useful for the child to play with the nitrous tubing and mask
• Use age appropriate language and other distraction techniques
• Appropriate positioning of the child

• The procedure and sedation needs to be undertaken in an appropriate location eg procedure room
• Location needs to have monitoring equipment, oxygen, suction and airway support equipment and access to paediatric resuscitation equipment and drugs
• Scavenging unit
Location
Equipment: general
• Bag–mask-valve setup appropriate for child age and size attached to separate oxygen source
• Operating suction with a yankauer sucker attached
• Pulse oximeter operative
• Equipment must be checked and available prior to commencing sedation episode
Equipment: nitrous oxide specific
• Nitrous oxide equipment is checked and working
• Bacterial filter filters for use in N2O circuit
• Apply scented essence to mask NOT filters
• Scavenging unit is set up
• Specific details of nitrous set will be covered in practical demonstration
During the procedure
• All medication used in sedation episode (including nitrous) require written orders and documented once administered
• Adjust flow of oxygen/N2O to achieve the desired concentration and sedation level
• Monitor the child’s level of sedation
• Monitor the child’s respiration, O2 saturation, heart rate and level of sedation
• Document every 5 minutes
• Identify and manage of any adverse events

Depth of sedation score
0 Awake and alert
1 Minimally sedated: may appear tired/sleepy, response to verbal stimulus
2 Moderately sedated: somnolent/sleeping, roused with light tactile stimulation
3 Deep sedation: deep sleep, rousable only with deep physical stimulation
4 Unrousable

Post procedure
• Administer 100% O2 for 2 minutes post procedure
• Monitor the child until their conscious state returns to baseline, 5 minutely observations documented until awake
• Once awake, monitor the child 15 minutely until fully recovered
• Nil orally until fully alert
• Document procedure and sedation on risk assessment and record form
• Manage and document any side effects or adverse events
Discharge
• Procedure completed successfully
• Child meets discharge criteria
• Discharge instructions discussed and provided to parent
• GP letter to parent (if required)
• Follow-up arrangements (e.g. GP, fracture clinic, etc)
• Ensure all documentation is complete included the risk assessment and record form
Questions