transfer of care around medicines (tcam)
TRANSCRIPT

Transfer of Care around Medicines
(TCAM)Medicines Support (Hospital to Home)
Contractor Launch Event
Herefordshire and Worcestershire STP
1
• Welcome
• Housekeeping
• Evening agenda
2
Welcome and Introductions
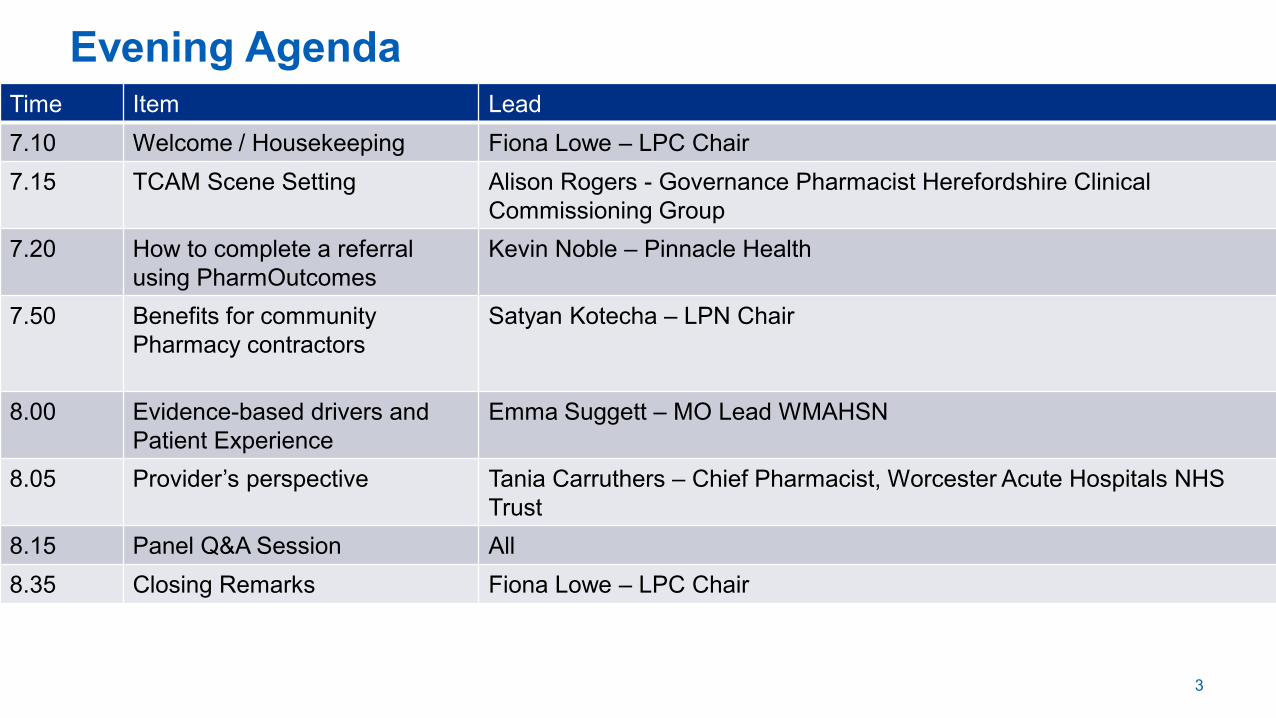
Time Item Lead
7.10 Welcome / Housekeeping Fiona Lowe – LPC Chair
7.15 TCAM Scene Setting Alison Rogers - Governance Pharmacist Herefordshire Clinical
Commissioning Group
7.20 How to complete a referral
using PharmOutcomes
Kevin Noble – Pinnacle Health
7.50 Benefits for community
Pharmacy contractors
Satyan Kotecha – LPN Chair
8.00 Evidence-based drivers and
Patient Experience
Emma Suggett – MO Lead WMAHSN
8.05 Provider’s perspective Tania Carruthers – Chief Pharmacist, Worcester Acute Hospitals NHS
Trust
8.15 Panel Q&A Session All
8.35 Closing Remarks Fiona Lowe – LPC Chair
3
Evening Agenda

Vision for Community Pharmacy
• Less reliance on
dispensing
• More clinical role for
Pharmacists
• Urgent Care
• Prevention
• Medicines Reconciliation
• Local engagement and
integration
• Enablers• IT
• New Contract
• Training & Development
• Changing Mindset
• Skill mix
• Dispensing process efficiencies
• CPWM and 1300 pharmacies
• Changes expected, nationally, to what we do and how we do it
• Move to increase service element of the contractual framework
• Better utilisation of the pharmacy profession and recognition for
community pharmacy
• Opportunity to collaborate with hospital pharmacists and pharmacists
working in GPs and to improve CARE of PATIENTS coming out of
hospital
• NHSE & I CP Framework Announcement 22nd July
• “Introduce a meds reconciliation services as part of TCAM” in 20/21
(p20)
• TCAM services already provided from c30% of Acute Trusts IN England
5
Community Pharmacy

Oct 2019 – Mar 2020 Apr 2020 – Mar 2021 Apr 2021 – Mar 2024
Funding • Flat funding of £2,592bn
• Scoping changes to reimbursement
system
• Flat funding – review in Oct 20
• Establishment payment
phased out
• Flat funding – review in Oct 21
• Increase share of funding for
clinical services
Pharmaceutical
services
• MUR capped at 250
• PCN pharmacists to start SMRs
• MURs capped at 100 and
phased out
• Medicines reconciliation
service
• Palliative care medicines
service
• Scope of NMS expanded
Consultation
service (CPCS)
• NHS 111 service introduced in Oct
19
• Fee of £14 per intervention
• GP referral service due to be
introduced
• Urgent treatment referrals
• A&E referrals
• Point of care testing
Public Health • Hep C testing service • HLP Level 1 status becomes
mandatory
• BP and AF case finding
• Stop smoking referrals
• Early cancer diagnosis
• Possible contraception service
Pharmacy
Quality Scheme
(PQS)
• Prepare to engage with PCNs
• Prescribing safety
• Diabetes patient checks
• Suicide prevention training
• Inhaler technique audit
• Anticoagulation audit
• Details to be confirmed
Regulations Mergers and closures – hub and spoke – original pack dispensing – empower technicians

Transfer of Care around Medicines (TCAM)
Scene Setting
Alison Rogers - Herefordshire Clinical
Commissioning Group
7

8
What's the issue?

9
Leave hospital with a bag of medicines

10
The new meds are united with existing meds at home

11
Which medicine should I take?

12
“Who needs to know the patient is in hospital and when they are going to be discharged?”
With the community pharmacist !
where do we start?
“the community pharmacist / the GP practice / the domcare agency?”

• Ten days after starting a medicine almost a third of patients are already non-adherent, of these;
₋ 55% don’t realise they are not taking their medicines correctly
₋ 45% are intentionally non-adherent
• 5-10% of hospital admissions are medicines related, of which 2/3rd are preventable
• 60% of patients have three or more changes made to their medicines during a hospital stay
• Only 10% of elderly patients will be discharged on the same medication that they were admitted to hospital on
• 30-70% of patients experience unintentional changes to their treatment or an error is made because of a lack of communication or miscommunication
• 20% of patients have been reported to experience adverse events within 3 weeks of discharge, 60% of which could have been ameliorated or avoided
13
Are we therefore surprised by the stats regarding
compliance?

• Transfer of Care Around Medicines
• When patients in hospital are identified as needing extra
support with their medicines, they are referred through a
safe and secure digital platform when they're discharged
for advice from their local community pharmacist
14
TCAM – Medicines Support (Hospital to Home)
How to Complete a Pharmacy Referral
using PharmOutcomes
Kevin Noble – Pinnacle HealthHow to complete a referral using
15

Managing rejected referrals

17
Benefits to Community Pharmacy
Contractors
Satyan Kotecha – West Midlands LPN Chair

18
Benefits to Community Pharmacy Contractors
Improves patient care through:
a) better provision of information to community
pharmacy
b) provision of follow-up information to GPs
https://www.youtube.com/watch?v=N_1lRDS2wt8&fe
ature=youtu.be

Evidence-based drivers and
patient experience
Dr Emma Suggett – Medicines Optimisation Lead
WMAHSN
19
Evidence of Patient Benefits
• Four significant studies published:
• Newcastle
• Leeds
• Cornwall
• Cheshire/Merseyside
• Patients receiving a community pharmacist follow-up consultation compared with those who didn’t demonstrated:
• statistically significant lower rates of readmissions
• shorter hospital stays

21
Implementation toolkit: existing guidance

22
Patient Experience
• The following case studies are taken from Wessex and North East and
North Cumbria AHSNs
• These cases illustrate examples of:
• Patient actions on discharge that could have led to their readmission
or harm
• The community pharmacist proactively intervening to ensure the
patient was not at risk from medication problems
• The patient needing support with their medicines when they got home

“The hospital referral stated that the patient’s warfarin had been stopped
and dabigatran started and when I followed up this referral I realised that
the repeat prescription for warfarin had not been cancelled”
“When I was in hospital the doctors started me on a new blood thinner, it
wasn’t until I received a phone call from my community pharmacist that I
realised I should have stopped my warfarin. It was really lucky that we
caught it in time as I was just about to order more and the pharmacist asked
me to return the unused tablets back to her”
23
Case study one

“The hospital referral stated the patient was an insulin dependent diabetic who had experienced fluctuations in blood glucose levels whilst in hospital. They suggested I followed up the patient on discharge to check that this had settled down”
“The pharmacist phoned me and asked me about my blood glucose levels. I always monitor this quite closely and had noticed that my blood glucose went low, particularly after eating. I had assumed this was because I had been trying to lose weight by eating smaller meals, and so was putting extra sugar in my drinks to bring this back up. But the pharmacist pointed out that my insulin dose was probably too high and suggested I made an appointment with my GP. My blood glucose control is much better now”
24
Case study two
“The hospital referral stated that a new medicine has been started and the amitriptyline dose had been reduced. When I called the patient I was concerned to learn that they were not taking their amitriptyline as prescribed”
“I take 12 different tablets each day and really thought I knew what I was doing. When I was in hospital I was told they were going to increase my pain killers, so I had been taking three instead of two. It wasn’t until I had a phone call from my own chemist that I realised I’ve actually got 13 tablets now and should have only been taking one of the painkillers and not 3! I don’t know what I’d have done without my pharmacist as there were a number of other changes to my medicines I’d missed”
Case study three
The Providers’ Perspective
Tania Carruthers – Chief Pharmacist
Worcester Acute Hospitals NHS Trust
26

Acute Trusts: Implementation behind the scenes
• Seek Approval from Trust Board / Senior Managers
• Determine and confirm IT requirements and method of implementation
• Determine IG requirements; DPIA
• Liaise with Trust ‘Patient Advice and Liaison Services (PALS)’
• Each patient must provide their consent
• Each patient must be provided with relevant information
• Develop a standard operating procedure (SOP)
• Identify behaviour changes required
• Identification resources within the clinical services team
• Develop and deliver appropriate training

28
Acute Trusts: Patient Cohorts and Number of Referrals
• Go live – January 2020
*based on annual admissions 2016-17, 1.5% referral rate (Newcastle Study)
Trust Patient GroupNumber of referrals
made/ day
Approximate number
of referrals per
community
pharmacy/month
Hereford County
Hospital
Frailty and identified as
high risk patients3 1
Worcestershire Royal
Hospital
Frailty and identified as
high risk patients5 1- 2
Alexandra HospitalFrailty and identified as
high risk patients2 1
Kidderminster
HospitalTBC 1 1

• Trust collaboration to develop standard STP template ensuring consistent referrals
• Approval of implementation plan by executive team members
• Internal communication plan developed
• Future-proofing TCAM
• SLA with WMAHSN for first 12 months; funding required thereafter
• Integration with local ePMA to improve efficiency
• Integration will enable more patients to benefit
29
Acute Trusts: Implementation behind the scenes

• Opportunities for collaboration
• Patient Flow
• Efficiency savings for Acute Trusts and CCGs
• Reduced length of stay
• Reduction in re-admission rates
30
Benefits
How should you communicate with us?
• PharmOutcomes will tell you which clinical pharmacist made the referral

Panel Q&A
Any Questions??
15 minute interactive session providing opportunity to
ask questions
31

Closing Remarks
32

• Change: preparedness and willingness
• Patient CARE
• Opportunity
• Recognition for community pharmacy in the new world
• Collaboration inter and intra professionally
• Shaping the national agenda
• New revenue stream
• Risk
• Non-delivery and high “rejections”
• Reputational damage
33
Community Pharmacy Closing Remarks