traumatic cardiac arrest alex king and kaushik nilakant
TRANSCRIPT
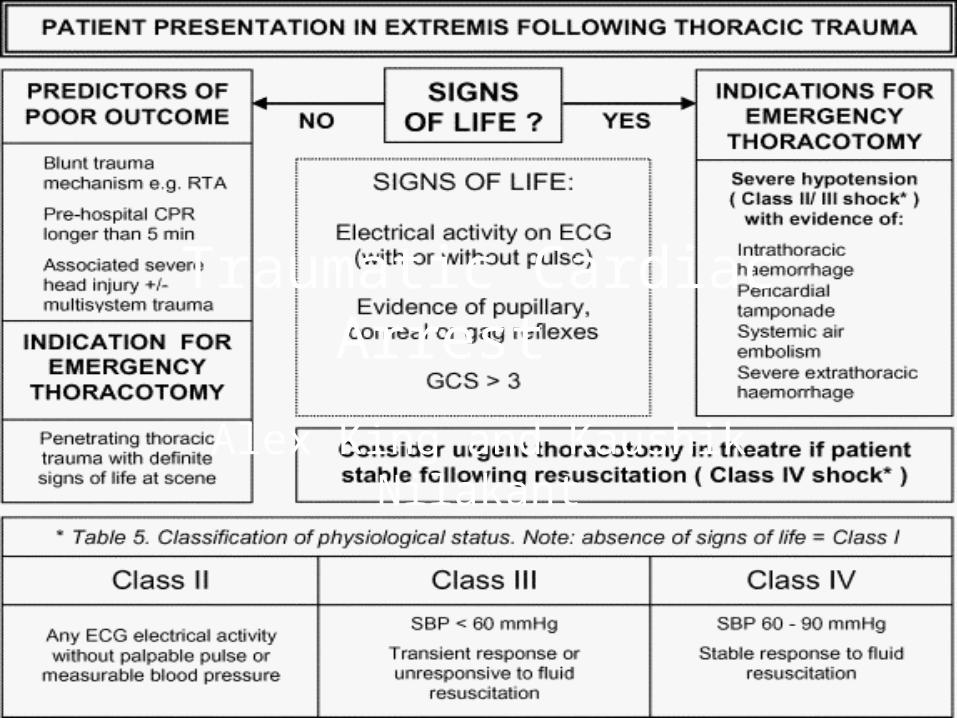
Traumatic Cardiac Arrest
Alex King and Kaushik Nilakant

Is CPR a waste of time?
• Yes.

Why??
• It doesn’t “treat” anything
• It might get in the way of doing something truly lifesaving




• Conventional ACLS based resuscitation focussing on “time on chest” and defibrillation will be a waste of time
• Modified resuscitation might save lives
• Use your judgement and tailor to each case




Reversible causes of cardiac arrest
-Hypoxia-Hypovolaemia-Hyper/hypokalaemia-Hypoglycaemia-Hyper/hypothermia
-Tension pneumothorax-Tamponade-Toxins-Thrombosis - pulmonary-Thrombosis - cardiac
Reversible causes of TRAUMA cardiac arrest
-Hypoxia-Hypovolaemia-Hyper/hypokalaemia-Hypoglycaemia-Hyper/hypothermia
-Tension pneumothorax-Tamponade-Toxins-Thrombosis - pulmonary-Thrombosis - cardiac

The new ABCs in trauma cardiac arrest

A = artificial airway I.e. intubation
B = bilateral finger thoracostomy
C = compression of pelvis and reduce long bone fractures
D = deploy IV fluids (or blood)
E = ECHO
F = FAST

A = artificial airway I.e. intubationHYPOXIA
B = bilateral finger thoracostomyTENSION PNEUMOTHORAX
C = compression of pelvis and reduce long bone fracturesHAEMORRHAGE
D = deploy IV fluids (or blood)HAEMORRHAGE
E = ECHOTAMPONADE
F = FAST

This applies to traumatic cardiac arrest (the cardiac arrest follows the trauma)
What if we cannot be sure of which came first?Are there departmental issues we need to address?



Procedures
• Emergency Thoracotomy
• Finger Thoracostomy
• Chest decompression
CALL FOR HELP!!