traumatic retroperi - department of radiology
TRANSCRIPT

1571ABDOMINAL EMERGENCIES
Kevin P. Daly, MD • Christopher P. Ho, MD • D. Laurie Persson, BA, BScAAM • Spencer B. Gay, MD
Multidetector computed tomography (CT) represents a significant advance in CT technology and can allow the accurate assessment of trauma patients, including the detection of traumatic retroperitoneal injuries, many of which are clinically occult. Retroperitoneal injuries include duodenal, pancreatic, vascular, renal, and adrenal injuries. Abnormal blood, fluid, or air within the retroperitoneal spaces may be isolated findings but can also occur in association with these inju-ries, and their recognition is the key to correctly identifying the injury. Accurate characterization of injury with CT can affect clinical man-agement and can help minimize unnecessary laparotomies. Equivocal findings at initial abdominal CT should prompt close clinical follow-up with possible imaging follow-up, particularly for suspected occult duodenal and pancreatic injuries.©RSNA, 2008 • radiographics.rsnajnls.org
Traumatic Retroperi-toneal Injuries: Review of Multidetector CT Findings1
LEARNING OBJECTIVES FOR TEST 3After reading this article and taking the test, the reader
will be able to:
Discuss the im- ■
portance of imaging in the evaluation and treatment of pa-tients with retroperi-toneal injuries.
Describe typical ■
imaging findings of retroperitoneal injuries.
Identify potential ■
sources of traumatic retroperitoneal hem-orrhage.
Abbreviations: IVC = inferior vena cava, MPR = multiplanar reformatted
RadioGraphics 2008; 28:1571–1590 • Published online 10.1148/rg.286075141 • Content Codes: 1From the Department of Radiology, University of Virginia Health System, Charlottesville, Va. Presented as an education exhibit at the 2006 RSNA Annual Meeting. Received June 21, 2007; revision requested December 11; final revision received April 1, 2008; accepted April 2. S.B.G. is on the advisory board of Onex (Carestream Health) and with the speakers’ bureau of GE Healthcare; all remaining authors have no financial relationships to disclose. Address correspondence to K.P.D., Department of Radiology, Tufts Medical Center, 800 Washington St, Box 299, Boston, MA 02111 (e-mail: [email protected]).
©RSNA, 2008
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this article.
CME FEATURESee accompanying
test at http://www.rsna.org
/education/rg_cme.html
See last page
TEACHING POINTS

1572 October Special Issue 2008 RG ■ Volume 28 • Number 6
IntroductionBlunt abdominal and pelvic trauma can cause significant and sometimes life-threatening inju-ries to retroperitoneal structures. Retroperito-neal injuries are known to occur in a significant minority of abdominal trauma cases (12% of hemodynamically stable patients evaluated at one center [1]). Physical examination and laboratory tests can be unreliable in detecting abdominal injuries, particularly retroperitoneal injuries (2). Bedside tests such as diagnostic peritoneal lavage and focused ultrasonography for the assessment of trauma can yield negative findings or fail to help detect signs of retroperitoneal injury, even in the presence of significant retroperitoneal injury, since these methods principally help assess the peritoneal space (3,4).
Imaging, particularly computed tomography (CT), plays a central role in the assessment of retroperitoneal structures following blunt trauma. Clinically significant imaging findings of retro-peritoneal injury can be subtle initially and thus potentially overlooked unless specifically sought out on CT scans by the radiologist (4). Histori-cally, conventional CT has demonstrated only limited sensitivity in identifying retroperitoneal injuries, particularly injuries of the pancreas. Only 68% of pancreatic injuries were detected with single-section helical CT in the setting of blunt abdominal trauma in a retrospective review of cases from 1996 to 2000 at a major level one trauma center (5). CT technology has improved significantly since then with the introduction of multidetector CT. This modality offers greater acquisition speed, improved spatial resolution, in-travenously administered contrast material bolus timing, and reduced motion artifacts (2). Multi-detector CT has recently been shown to have a high degree of accuracy in the setting of trauma, with a reported sensitivity approaching 100% for the identification of active bleeding as well as bowel, mesenteric, and pancreatic injuries in the initial assessment of blunt abdominal trauma in 252 patients at one center (2). At another center, multidetector CT had an overall sensitivity of 94%, specificity of 100%, and accuracy of 97% in the evaluation of high-energy trauma injuries in 153 patients (6).
Multidetector CT also plays an important role in the triage of trauma patients in the acute setting. Accurate radiologic characterization of injury can help in selecting patients who need urgent surgical intervention, as opposed to those in whom nonoperative management is possible, par-ticularly since the morbidity rate for an unneces-sary laparotomy (ie, completely negative find-ings or nontherapeutic results) in the setting of trauma is between 8.6% and 25.9%. Respiratory complications (atelectasis or pneumonia), pro-longed paralytic ileus, surgical wound infection, and small bowel obstruction are the most com-mon complications (7). The mean length of stay for patients with completely negative laparotomy findings is also considerably increased (average of 4.7 days at one center [4]).
In this article, we review the relevant anatomy of the retroperitoneum and describe imaging technique in the evaluation of retroperitoneal injuries, with multidetector CT as the primary imaging modality. In addition, we discuss and il-lustrate injuries to retroperitoneal structures (du-odenal, pancreatic, adrenal, and vascular injuries) as well as abnormal posttraumatic findings within the retroperitoneum (hemorrhage, paraspinal or spinal injury, air, fluid). We also propose an algorithm for the diagnosis of traumatic retro-peritoneal injuries. Imaging of renal and urinary tract injuries warrants more thorough consider-ation than can be covered here; indeed, reviews of these topics have recently appeared in this journal and elsewhere (8,9).
Relevant AnatomyThe retroperitoneum is that portion of the ab-domen posterior to the peritoneal cavity from the diaphragm to the pelvic inlet. It is separated from the peritoneum anteriorly by the posterior peritoneal fascia and is bounded posteriorly by the transversalis fascia. It contains portions of the colon and duodenum as well as the pancreas, kidneys, adrenal glands, abdominal aorta, and in-ferior vena cava (IVC) (10). The retroperitoneum has traditionally been divided into the posterior pararenal space, containing only fat; the perire-nal spaces, containing the kidneys, renal pelves, proximal ureters, adrenal glands, and perirenal fat; and the anterior pararenal space, containing the retroperitoneal segments of the colon and du-odenum, the pancreas, and the root of the small
TeachingPoint

RG ■ Volume 28 • Number 6 Daly et al 1573
bowel mesentery. The boundaries and contents of the retroperitoneal spaces are shown in Table 1. More recently, the classic tricompartment model has been modified to reflect the understanding that the fascia separating the spaces is laminar, variably fused, and potentially expandable as a result of embryologic partial fusion of the dorsal
mesenteries. The retromesenteric, retrorenal, and lateroconal planes are potential routes of interfas-cial communication between the retroperitoneal spaces (Fig 1). Retroperitoneal hemorrhage or
Table 1 Anatomic Spaces of the Retroperitoneum
Space Boundaries Contents
Anterior pararenal Peritoneum, anterior perirenal fascia, latero-conal fascia
Pancreas, duodenum, ascending colon, descending colon
Perirenal Anterior and posterior renal fasciae Kidneys, adrenal glands, proximal renal collecting systems, renal hilar vessels
Posterior pararenal Posterior renal fascia, transversalis fascia, fascia over the psoas muscle continuous with the transversalis fascia
Fat
Figure 1. Fascial planes and spaces of the retroperitoneum. (a) Drawing illustrates the tra-ditional tricompartment model of the retroperitoneum, which is accordingly divided into the anterior pararenal space (APS), perirenal space (PS), and posterior pararenal space (PPS). The anterior renal fascia (ARF), posterior renal fascia (PRF), and lateroconal fascia (LCF) divide the spaces. (b) Drawing illustrates the recently modified tricompartment model, which reflects the understanding that the perirenal fascia is laminar and variably fused and there are interfascial connections between the spaces. The retromesenteric plane (RMP), retrorenal space (RRS), and lateroconal space are potential interfascial communications. Perinephric septa run between the renal capsule and the perinephric fascia, allowing subcapsular fluid to communicate with the retrorenal space or retromesenteric plane. APS = anterior pararenal space, PPS = posterior pararenal space, PS = perirenal space (11,12).

1574 October Special Issue 2008 RG ■ Volume 28 • Number 6
the axial images. Alternatively, the thin-section axial data can be reformatted on the interpreting workstation as needed depending on the picture archiving and communication system and work-station configuration in place. The use of oral contrast material is optional. It has been shown to be safe in trauma patients, with a number of studies showing an extremely low risk of aspira-tion (15). Typical agents include 500–600 mL of diluted (2%–5%) water-soluble oral contrast material administered orally or through a na-sogastric tube as the patient is being stabilized or transported to the CT suite. Recent litera-ture suggests that multidetector CT without oral contrast material may be adequate for the detection of bowel and mesenteric injuries and comparable to single–detector row helical CT with oral contrast material (16). If thoracic CT is also needed, thin-collimation scanning is per-formed through the thorax initially during the vascular phase for MPR images of the aorta, fol-lowed immediately by coverage of the abdomen and pelvis during the parenchymal phase with use of the same intravenous contrast material bolus (14). Selective use of delayed scanning (5–8-minute delay) may be helpful in cases of suspected intraabdominal bleeding or in the evaluation of urinary tract injuries when renal or severe pelvic injuries are identified (14).
Injuries to Retro- peritoneal Structures
Duodenal InjuriesAlthough the deep, central, retroperitoneal loca-tion of most of the duodenum protects it against frequent injury, the morbidity and mortality rates for traumatic duodenal injuries remain high. Mortality rates for traumatic duodenal in-jury range from 6% to 25% (4). Complications including abscess, fistula, respiratory failure, and renal failure occur frequently (30%–60% of cases). The high complication rate is due in part to diagnostic delays and missed injuries, since surgical repair becomes more difficult if the in-jury is recognized late. If recognized early, up to
rapidly expanding fluid collections can spread via these interfascial connections (11).
Below the kidneys, the retroperitoneal spaces are in reality a single space with direct contigu-ity between the anterior and posterior portions. Retroperitoneal hemorrhage or fluid can spread from the abdominal retroperitoneum into the extraperitoneal pelvis along the anterior and posterior perirenal fasciae, which combine to form the fascial plane in the iliac fossa (12). Superiorly, the perirenal fasciae are attached to the diaphragm. On the right side, the bare area of the liver is directly connected to the anterior pararenal space. Therefore, hepatic lacerations involving the bare area of the liver can be a source (albeit uncommon) of retroperitoneal hemorrhage (13).
Imaging TechniqueMultidetector CT offers significantly faster scanning times and improved image resolu-tion due to thinner collimation and reduced partial volume and motion artifacts compared with single-section helical CT. The improved coverage speed and z-axis resolution have made angiographic, multiplanar reformatted (MPR), maximum-intensity-projection, and volume-rendered images available for clinical application (14,15).
Depending on the available scanner, a typical protocol for multidetector CT of the abdomen and pelvis in the setting of trauma is as fol-lows: 1–2.5-mm collimation; 1–1.75 pitch; and 100–150 mL (300–370 mg of iodine per mil-liliter) of contrast agent injected intravenously at 3–6 mL/sec (15). Scanning is performed begin-ning 60–70 seconds after the onset of contrast material injection in the portal venous phase from the diaphragm to the lesser trochanters. Images are reconstructed with a 2.5–3-mm thickness at 2–3-mm intervals. Coronal and sagittal reformatted images may be obtained and sent for soft-copy interpretation along with

RG ■ Volume 28 • Number 6 Daly et al 1575
tify signs supporting the presence (or absence) of perforation, since they will influence the management algorithm. Extraluminal air is a re-liable sign of duodenal perforation and is highly predictive of such perforation in the absence of pneumothorax or prior diagnostic peritoneal la-vage. In a small series of patients with duodenal injuries who had undergone CT at the time of admission, extraluminal air, extraluminal oral contrast material, or both were specific signs of duodenal perforation and were useful in differ-entiating duodenal perforation from hematoma (22). In a large trauma series examining small bowel perforation, the reported sensitivity and specificity of extraluminal air for traumatic per-foration were 46% and 99%, respectively (24). It is sometimes difficult to distinguish a duode-nal hematoma from duodenal perforation, since extraluminal air is not always present in cases of traumatic perforation (22,23). Extraluminal fluid in the absence of solid organ injury can be seen in both duodenal hematoma and perfora-tion. A small fluid collection adjacent to the du-odenum can be an indication of a sentinel clot and an indirect sign demonstrating the origin or site of the duodenal injury (23).
Extravasation of oral contrast material is specific for duodenal perforation; however, by itself it has limited sensitivity (only 19% in a retrospective analysis [24]). Furthermore, many institutions no longer use oral contrast material routinely for trauma imaging. As mentioned ear-lier, recent literature suggests that multidetector CT without oral contrast material is adequate for the detection of bowel and mesenteric inju-ries and is comparable to single–detector row helical CT with oral contrast material (16). Fo-cal bowel wall thickening may be an indirect sign of duodenal injury in the setting of blunt trauma. Given the proximity of the duodenum to the pancreas, injuries to the duodenum are often associated with injuries to the pancreatic
80% of duodenal injuries can be safely repaired primarily (4). Delayed diagnosis is often associ-ated with a protracted, difficult clinical course, including the development of pseudocysts, fis-tulas, pancreatitis, septicemia, or organ failure (4,17). Time from injury to definitive treatment is an important factor in the development of late complications and mortality, with markedly in-creased morbidity and mortality rates when the diagnosis is delayed more than 24 hours (18). Fortunately, duodenal injuries are relatively uncommon. A 6-year statewide review in Penn-sylvania found a prevalence of blunt duodenal injury of only 0.2% (206 of 103,864 trauma reg-istry entries), with only 30 of these patients sus-taining full-thickness duodenal injuries (19). A similar prevalence of blunt duodenal injury was observed in Texas over a 10-year period, during which time 35 cases (0.2%) were identified from data on 22,163 patients with blunt trauma (17).
Duodenal injuries range in severity from mi-nor duodenal hematoma and partial-thickness lacerations to complex lacerations and even massive disruption of the duodenopancreatic complex (20). Traumatic duodenal perforation requires emergent surgical intervention, whereas duodenal hematoma is frequently managed conservatively. CT findings of duodenal injury can be subtle. In one study of the accuracy of CT in diagnosing duodenal or other small bowel injuries, only 10 of 17 injuries (59%) were pro-spectively (ie, preoperatively) interpreted as sug-gestive of bowel injury, which increased to 88% (15 of 17 injuries) at retrospective evaluation (21). The authors concluded that CT is sensitive for the diagnosis of bowel rupture from blunt trauma but requires careful inspection of images and attention to technique for the detection of subtle findings (21).
CT findings of duodenal injury include duo-denal wall thickening, periduodenal fluid, fluid in the right anterior pararenal space, diminished bowel wall enhancement of the injured segment, extraluminal air, extraluminal oral contrast ma-terial, and the “sentinel clot” sign (21–23). In addition to detecting injury, it is critical to iden-
TeachingPoint

1576 October Special Issue 2008 RG ■ Volume 28 • Number 6
thirds of blunt pancreatic injuries occur in the pancreatic body, with the remainder occurring with equal frequency in the head, neck, and tail. Complete pancreatic rupture as a result of trau-
head; thus, care should be taken to examine ad-jacent structures (Figs 2–6).
Pancreatic InjuriesTraumatic pancreatic injuries occur in less than 5% of patients with major abdominal injuries. The retroperitoneal location of the pancreas protects it in most instances of blunt abdominal trauma. Blunt injuries usually result from direct impact or deceleration injury, often in conjunc-tion with other visceral injuries, including injuries to the liver, spleen, duodenum, stomach, and kidneys. Pancreatic injury typically results from severe anterior-to-posterior force vectors com-pressing the pancreas against the spine, with the injury commonly occurring just to the left of the mesenteric vessels (10). Steering wheel impact in a motor vehicle collision is a common mecha-nism in adults, whereas bicycle handlebar impact is a common cause in children. Nonaccidental trauma is the major consideration in infants (25). Blunt pancreatic injury is more common in children and young adults because they have a thinner or absent mantle of protective fat, which surrounds the pancreas in older adults (10). Two-
Figures 2, 3. (2) Traumatic duodenal intramural hematoma in a 26-year-old man who had sustained a seat belt injury in a high-speed motor vehicle collision. Abdominal CT scan obtained with oral and intravenous contrast ma-terial shows wall thickening of the third and fourth portions of the duodenum (arrows). No extraluminal air (a find-ing that would have suggested perforation) was seen. The patient was treated conservatively and recovered without intervention. (3) Periduodenal hemorrhage in a 34-year-old man who had sustained blunt trauma in a motor vehicle collision. Abdominal CT scan obtained with intravenous contrast material shows hemorrhagic fluid surrounding the first and second portions of the duodenum (arrowheads) in the right upper quadrant. No extraluminal air (which would have suggested perforation) was identified.
Figure 5. Duodenal hematoma in an 11-year-old boy who had sustained a bicycle handlebar injury. On an abdominal CT scan obtained with oral and intravenous contrast material, the third portion of the duodenum is thickened and edematous (arrowheads). No extraluminal air could be identified to suggest per-foration. The patient was treated conservatively and recovered completely.

RG ■ Volume 28 • Number 6 Daly et al 1577
associated with delayed treatment, the trauma team and radiologist should remain vigilant if there is a high degree of suspicion for
pancreatic injury based on injury mechanism, clinical findings, or unexplained hyperamylasemia.
matic transection usually occurs in the line of the superior mesenteric vein at the neck of the gland (26). Many pancreatic injuries are not apparent at initial clinical examination and may become apparent only when complications arise (4).
Mortality rates for pancreatic injuries range from 10% to 30% and have been reported as high as 60% when treatment is delayed (27).
Figure 4. Large traumatic duodenal hematoma in a 49-year-old man who was involved in a motor vehicle collision. The patient was also taking anticoagulants. (a) Abdominal CT scan obtained with oral and intrave-nous contrast material shows a large hematoma (arrowheads) displacing the second portion of the duodenum (arrow) anteromedially and narrowing the duodenal lumen. (b) Coronal reformatted CT image depicts the full extent of the duodenal hematoma (arrowheads).
Figure 6. Duodenal perforation in a 28-year-old man who sustained blunt trauma in a motor vehicle collision. (a) Abdominal CT scan obtained with intravenous and oral contrast material shows extraluminal air (arrows) adja-cent to the duodenum (D). Cholecystectomy clips are also present. (b) Coronal reformatted CT image shows a large amount of fluid in the right anterior pararenal space with a small focus of extraluminal air (arrow), findings that are consistent with a duodenal perforation. The perforation was confirmed and repaired at surgery. D = duodenum.
B cause of the high morbidity and mortality rates
eTeaching
Point

1578 October Special Issue 2008 RG ■ Volume 28 • Number 6
on CT of pancreatic trauma deals with nonhelical or incremental CT, with a reported overall sen-sitivity of 80% for the detection of all grades of pancreatic injury (10,26). In a retrospective study of 50 patients with blunt pancreatic injury at one center, preoperative helical CT was found to be
The reported sensitivity and specificity of CT in the detection of pancreatic injury have been variable, since findings may initially be subtle or unapparent (10). Most of the existing literature
Figure 7. Subtle pancreatic contusion in a 35-year-old woman who was involved in a motor vehicle colli-sion. Abdominal CT scan obtained with intravenous contrast material shows swelling and diminished parenchymal enhancement (arrow) in the pancreatic head. Periportal low attenuation (edema) and periaor-tic low attenuation are also present and likely reflect the effects of resuscitation.
Figure 8. Drawing illustrates a superficial pancreatic laceration (arrow) that involves less than 50% of the thickness of the gland and does not involve the pan-creatic duct. Many of these injuries can be managed conservatively.
Figure 9. Laceration of the pancreatic neck in an 18-year-old man who was involved in a motor vehicle collision. Abdominal CT scans obtained with intravenous contrast material (b obtained just inferior to a) show a linear focus of diminished enhancement at the pancreatic neck (arrow). Subsequent endoscopic retrograde pancreatography showed that the main pancreatic duct was narrowed but not transected. A pancreatic duct stent was placed, and the patient recovered without complication.

RG ■ Volume 28 • Number 6 Daly et al 1579
areas of hypoattenuation surrounded by normally enhancing pancreatic tissue (Fig 7). Lacerations appear as areas of linear hypoattenuation per-pendicular to the long axis of the pancreas (Figs 8–10). Pancreatic transection is a full-thickness laceration that typically results in transection of the pancreatic duct (Figs 11, 12). Specific CT findings of pancreatic injury include fracture of
91% sensitive and 91% specific for the detection of pancreatic ductal injury (28). Multidetector CT, with its faster and higher-resolution scan-ning and its capacity for MPR, has shown greater promise, with sensitivities for pancreatic injury exceeding 90% (2,5,25,28).
Pancreatic injuries include parenchymal con-tusions and lacerations that range in severity from minor to massive disruption of the gland. Pancre-atic contusions appear at CT as focal or diffuse
Figure 10. Drawing illustrates a deep pancreatic lac-eration that involves more than 50% of the thickness of the pancreatic parenchyma, with injury to the pancre-atic duct. These injuries generally require endoscopic or surgical intervention.
Figure 11. Drawing illustrates a pancreatic lacera-tion that involves the full thickness of the gland, with transection of the pancreatic duct. These injuries re-quire endoscopic or surgical intervention.
Figure 12. Pancreatic transection in a 21-year-old man who was involved in a motor vehicle collision. (a) Abdomi-nal CT scan obtained with intravenous contrast material at the level of the pancreas shows a full-thickness linear low-attenuation laceration of the pancreatic neck (arrow) just anterior to the proximal portal vein. (b) Contrast material–enhanced CT scan obtained inferior to a shows a focal hematoma at the transection site that extends into the pancreatic head (arrow). Complete transection with ductal disruption was identified at surgery. The patient un-derwent a spleen-sparing distal pancreatectomy.
1580 October Special Issue 2008 RG ■ Volume 28 • Number 6
perficial lacerations (<50% thickness) had a duc-tal injury, whereas eight of 10 patients with deep lacerations (>50% thickness) had disruption of the main pancreatic duct (31).
Endoscopic retrograde pancreatography or magnetic resonance (MR) pancreatography should be considered for assessment of the integ-rity of the pancreatic duct in the setting of sus-pected pancreatic injury. Focal findings may not be evident at initial CT and may take up to 24 hours to become radiologically apparent (26,28).
Adrenal InjuriesAdrenal injuries are seen in up to 2% of patients with blunt abdominal trauma (32). Although isolated adrenal injuries are uncommon and can be relatively benign and self limited, they are frequently associated with more significant abdominal and thoracic injuries. Liver injuries are the most common associated injury. When an adrenal injury is found, the radiologist should imagine the vector of force needed to cause such an injury and look along this line in the liver or kidney for other injuries. In a review of 73 cases of traumatic adrenal hemorrhage detected at CT, 77% of hemorrhages were right sided, 15% were left sided, and 8% were bilateral (32). Proposed mechanisms of adrenal injury include direct crush injury (ie, between the spine and the liver or spleen), injury due to acutely increased adrenal venous pressure transmitted from a compressed IVC, IVC–adrenal vein thrombosis, and shear injury to small adrenal vessels due to rotational or deceleration forces (32,33). Adrenal injuries are thought to occur more frequently on the right side due to the location of the right
the pancreas, pancreatic laceration, focal or dif-fuse pancreatic enlargement or edema, pancreatic hematoma, and active bleeding or extravasation of intravenous contrast material (25). Fluid sepa-rating the splenic vein and the pancreas is highly suggestive of pancreatic injury (29,30). Normally, the splenic vein is closely apposed to the poste-rior aspect of the pancreas or is separated from the pancreas by a thin layer of fat. When fluid between the splenic vein and the pancreas is seen in the setting of abdominal trauma, a pancreatic injury should be suspected. In the study in which this finding was initially reported, it was observed in nine of 10 patients with surgically or autopsy-proved pancreatic injury (29). It can also be seen in patients with fluid in the anterior pararenal space without pancreatic injury (30) but is rarely the only abnormal CT finding in patients with blunt pancreatic trauma. Additional nonspecific CT signs of pancreatic injury include inflamma-tory changes in the peripancreatic fat and mes-entery; fluid surrounding the superior mesenteric artery; thickening of the left anterior renal fascia; pancreatic ductal dilatation; acute pseudocyst formation or a peripancreatic fluid collection; fluid in the anterior and posterior pararenal spaces; fluid in the transverse mesocolon and lesser sac; hemorrhage into the peripancreatic fat, mesocolon, and mesentery; extraperitoneal fluid; and intraperitoneal fluid (25,29).
Besides helping detect injury, imaging can help distinguish injuries that require surgical management from those that can be managed conservatively. Key to this determination is the integrity of the pancreatic duct. Pancreatic con-tusions and lacerations without pancreatic duct injury have been designated as grade I or grade II by the American Association for the Surgery of Trauma (Table 2) and can frequently be man-aged conservatively. More severe injuries (grades III–V) involve the pancreatic duct or ampulla and generally require intervention, whether surgical or endoscopic. Figure 13 depicts a pancreatic laceration with associated ductal disruption that was confirmed at endoscopic retrograde pancre-atography. The severity of pancreatic laceration has been shown to be predictive of ductal disrup-tion (31). In a retrospective review of 22 cases of pancreatic injury, none of the 10 patients with su-
Table 2 American Association for the Surgery of Trauma Pancreatic Organ Injury Scale
Grade Description
I Minor contusion or laceration without ductal injury
II Major contusion or laceration without ductal injury or tissue loss
III Distal transection or pancreatic parenchy-mal injury with ductal injury
IV Proximal transection or pancreatic paren-chymal injury involving the ampulla
V Massive disruption of the pancreatic head
Source.—Reference 20.

RG ■ Volume 28 • Number 6 Daly et al 1581
pararenal space, and thickening of the ipsilateral diaphragmatic crus can be seen (32,34). Adrenal hemorrhage is usually hyperattenuating (40–60 HU); does not enhance; is accompanied by peri-adrenal stranding; and will change over time, typically decreasing in size and, perhaps, eventu-ally calcifying (32). An attenuation of less than 10 HU at unenhanced CT or washout of over 50% of contrast material after a 10-minute delay is consistent with an adrenal adenoma (35,36). If the cause of trauma is in doubt, adrenal proto-col CT or MR imaging can be used to confirm the diagnosis or a follow-up examination can be performed in 6–8 weeks. An adrenal hemorrhage should resolve or shrink considerably in that time and will not enhance after contrast material administration, whereas an adrenal adenoma or malignant lesion will persist over time and will enhance (32,34). Figure 14 shows a typical right adrenal hemorrhage with periadrenal hemorrhage and stranding.
adrenal gland (making it more susceptible to compression between the liver and the spine) as well as to differences in venous drainage between the two adrenal glands. The right adrenal vein is shorter than the left and is connected directly to the IVC, so that pressure from the IVC is trans-mitted more directly, making the right adrenal gland more susceptible to venous congestion injury (32,33). Although bilateral adrenal hemor-rhage is uncommon, it can result in life-threaten-ing adrenal insufficiency in rare cases (32).
Typical CT findings include a round or oval hematoma expanding the adrenal gland, irregular hemorrhage obliterating the normal margin of the gland, glandular swelling, an adrenal mass, and periadrenal hemorrhage. Periadrenal strand-ing is a common associated finding. Retroperito-neal hemorrhage, particularly into the posterior
Figure 13. Pancreatic laceration in a 49-year-old man who had suffered penetrating trauma 5 days earlier. (a) Ab-dominal CT scan obtained with oral and intravenous contrast material shows laceration of the pancreatic neck with a pancreatic duct leak (arrow) and a peripancreatic fluid collection (arrowheads). There was also a common bile duct injury with a bile leak responsible for the peritoneal fluid. A pigtail drainage catheter was placed for drainage of the pancreatic injury and is seen just behind the pancreatic head. (b) Endoscopic retrograde pancreatogram shows the extravasation of contrast material (arrows) that had been injected into the pancreatic duct (arrowheads), a find-ing that confirmed the pancreatic duct injury.
Figure 14. Traumatic adrenal hemorrhage in a 46-year-old man who was involved in a motor vehicle collision. Ab-dominal CT scan obtained with intravenous contrast mate-rial shows a right adrenal hemorrhage (arrowheads) with periadrenal hemorrhage (arrow). An associated hepatic con-tusion and lower posterior rib fractures were also present.

1582 October Special Issue 2008 RG ■ Volume 28 • Number 6
Figure 15 shows an infrarenal aortic injury with a concentric intimal flap due to lab belt use. More severe injuries include vessel lacera-tion and transection, which necessitate emergent intervention.
Blunt injuries to the IVC are also rare, with only a few published reports in the literature (41,42). In a retrospective review of 5059 pa-tients with blunt trauma over a 10-year period at a single center, 10 patients with blunt IVC injuries were identified (41). CT findings of blunt IVC injury vary depending on the location of the injury. Retroperitoneal hematoma with a paracaval epicenter, irregular IVC contour, and extravasation of contrast material have been de-scribed with infrahepatic IVC injury (41). With retrohepatic IVC injuries, severe associated liver trauma is often seen. Signs that are suggestive of retrohepatic IVC injury include extensive liver laceration into the porta hepatis and retrohepatic IVC region or an irregular contour of the retro-hepatic IVC (41). Blunt IVC injuries can be diffi-cult to diagnose, since many of the reported cases lack contrast material extravasation as direct evi-dence of vascular injury (41).
Abnormal Findings within the Retroperitoneum Following Trauma
Retroperitoneal HemorrhageRetroperitoneal hemorrhage can be the source of significant but clinically occult blood loss in the trauma patient. Retroperitoneal hemorrhage was identified in 12% of 466 stable patients undergo-ing abdominal CT for blunt trauma at a major
Vascular InjuriesMajor retroperitoneal vascular structures in-clude the abdominal aorta, IVC, renal vessels, proximal celiac axis and superior mesenteric arteries, superior mesenteric vein, lumbar arter-ies and veins, and iliac vessels within the pelvis (Table 3). Blunt injury to the abdominal aorta is uncommon, with thoracic aortic injuries occur-ring 20 times more frequently than abdominal aortic injuries in several autopsy series (37). A 1997 review by Roth et al identified 62 cases of blunt abdominal aortic injury reported in the English medical literature, half of which were as-sociated with lap belt use or steering wheel im-pact (38,39). The infrequency with which blunt abdominal aortic injury occurs is likely due to the central protected position of the abdomi-nal aorta. Most injuries result in damage to the intima, with creation of an intimal flap. The de-gree of injury may range from subtle intimal in-juries to frank transection. Thrombus formation may occur with partial or total aortic occlusion. A mortality rate of up to 24% has been reported for these injuries (37). Injuries involve the infra-renal abdominal aorta in almost all cases (98%) (37). Proposed mechanisms for traumatic rup-ture of the abdominal aorta include direct forces on the abdominal aorta, such as between a lap belt and the lumbar spine, as well as indirect forces generated by transmission of the pressure of the initiating force through adjacent organs to the aortic wall (38). Neurologic deficits ranging from sensory loss to paraplegia have also been associated with abdominal aortic injuries (40).
Table 3 Anatomic Zones of the Retroperitoneum
Zone Vascular Contents Visceral Contents
I (midline retroperitoneum)Supramesocolic area Suprarenal abdominal aorta, celiac axis, proximal
superior mesenteric artery, superior mesenteric vein, proximal renal arteries
Pancreas, duodenum
Inframesocolic area Infrarenal abdominal aorta, infrahepatic IVC . . .II (upper lateral retroperi-
toneum)Renal arteries, renal veins Kidneys, adrenal glands,
renal pelves, proximal ureters
III (pelvic retroperitoneum) Iliac arteries, iliac veins . . .
Sources.—References 46 and 47.

RG ■ Volume 28 • Number 6 Daly et al 1583
and stability, and the hemodynamic status of the patient. Options include surgical intervention, angiographic embolization, and observation with fluid support. The goals of imaging are to iden-tify the retroperitoneal hemorrhage, its location, and its possible source and to assess its relative stability on the basis of the size and presence (or absence) of active extravasation of intravascular contrast material (45).
From a surgical standpoint, the retroperito-neum can be divided into zones because hema-toma location has therapeutic implications (Fig 16; Table 3) (46). This classification scheme was initially described in the surgical literature in 1982 (46,47).
trauma center (43). Retroperitoneal hemorrhage may arise from injuries to major vascular structures, hollow viscera, solid organs, or musculoskeletal structures or a combination thereof (44). Clinical management depends on the presence of active contrast material extravasation, hematoma size
Figure 15. Traumatic infrarenal aortic injury caused by a lap belt in a 22-year-old man who was involved in a motor vehicle collision. (a) Contrast-enhanced abdominal CT scan obtained through the midabdomen shows a concentric intimal flap (arrowhead) within the infrarenal abdominal aorta. (b) Coronal reformatted CT image shows the infrarenal intimal flap (arrowheads). The right kidney was devascularized, with hemorrhage and fluid in the right perirenal space (arrows). The patient was treated conservatively and the infrarenal aortic injury became stable. The intimal flap was not seen at follow-up imaging performed 6 weeks later.
Figure 16. Drawing illustrates the zonal anatomy of the retroperitoneum, which can be divided into three zones from a surgical standpoint for the management of retroperitoneal hemorrhage. Zone I is the central midline retroperitoneum and con-tains the abdominal aorta, the IVC, the root of the mesentery, and portions of the pancreas and duo-denum. Zone II is the lateral retroperitoneum and contains the kidneys, adrenal glands, renal vascula-ture, and ascending and descending colon. Zone III is the pelvic retroperitoneum (46–48).
TeachingPoint

1584 October Special Issue 2008 RG ■ Volume 28 • Number 6
severity of the hemorrhage and may include ex-ploration or angiographic embolization for large or expanding hematomas (48). Many perirenal and pericolonic hematomas are self limiting, and patients can be treated with observation alone if they remain hemodynamically stable and no ex-traluminal gas or active extravasation of contrast material is identified at initial imaging (46,48). Follow-up imaging can be used to assess the sta-bility of retroperitoneal hemorrhage when obser-vation is chosen (45). Figure 19 shows a zone II hemorrhage from a renal laceration.
Zone III encompasses the pelvic retroperito-neum and is the most common location of retro-peritoneal hemorrhage, frequently in association with pelvic fractures (43,44,48). Surgical inter-
Zone I retroperitoneal hemorrhage includes the midline area between the aortic hiatus and sacral promontory and carries the highest risk of vascular injury because the major abdominal ves-sels lie in this zone (46). Unless they are small or stable, many zone I retroperitoneal hemorrhages are investigated with a surgical approach that is influenced by whether the hematoma is above or below the transverse mesocolon (48). Figure 17 shows a large zone I retroperitoneal hemorrhage with active extravasation of intravascular contrast material indicating active bleeding. Figure 18 shows an example of a small zone I retroperito-neal hemorrhage that was successfully managed with observation alone.
Zone II encompasses the flank or lateral retro-peritoneum, including the right and left perirenal spaces, and represents the second most com-mon site of retroperitoneal hemorrhage after the pelvis. Renal injuries account for the majority of these hemorrhages. Management depends on the
Figure 17. Large zone I (central) retroperitoneal hematoma with active extravasation in a 26-year-old woman who was involved in a high-speed motor vehicle collision. (a) Abdominal CT scan obtained with in-travenous contrast material shows a large, central midline retroperitoneal hematoma (arrowheads) with a large focus of active extravasation (arrow) displacing the duodenum and pancreas anteriorly. (b) Coronal reformat-ted CT image shows active extravasation of intravascular contrast material adjacent to the central superior mesenteric vein (arrow), which proved to be lacerated and was repaired at surgery.
Figure 18. Small zone I (central) retroperitoneal hematoma in a 41-year-old man who was involved in a motor vehicle collision. Abdominal CT scan obtained with intravenous contrast material shows a small amount of intermediate-attenuation fluid (arrowheads) between the aorta and IVC, a find-ing that presumably represents venous hemorrhage. The patient was observed clinically and remained hemodynamically stable.

RG ■ Volume 28 • Number 6 Daly et al 1585
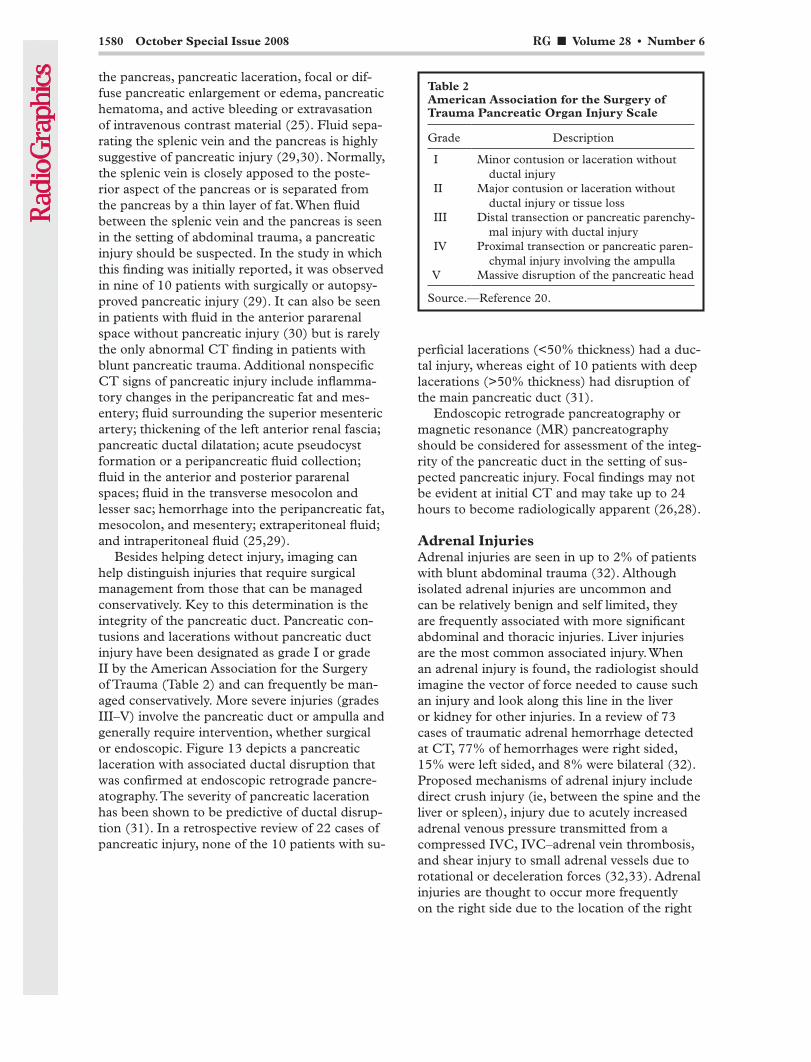
data were shown to be 95% sensitive for the de-tection of thoracic spine fractures and 97% sensi-tive for the detection of lumbar spine fractures, compared with sensitivities of 62% and 86%, respectively, for conventional radiographs of the thoracic and lumbar spine (50). Similar sensitivi-ties for the detection and classification of tho-racic and lumbar spinal fractures were achieved with MPR images of the thoracic and lumbar spine from thoracoabdominal multidetector CT data, provided both thin (≤3-mm) sections and MPR images were used (51). The presence of a paraspinal hematoma is an important sign of spi-nal injury and should prompt careful evaluation of the adjacent spinal elements and paraspinal musculature (52). Figures 20–22 show paraspinal hematomas due to spinal injuries following blunt abdominal trauma.
vention is avoided in most cases of blunt pelvic trauma, with external fixation and angiographic embolization being the preferred methods for addressing large, expanding, or actively bleeding pelvic hematomas (48). Surgical intervention is generally reserved for major arterial injury, ex-sanguinating pelvic bleeding, or bleeding into a peritoneal wound (48).
Paraspinal or Spinal InjuriesThoracic and lumbar spinal injuries affect 2%– 3% of blunt trauma victims and can be associ-ated with neurologic deficit in up to 40%–50% of cases (49). Thoracolumbar spinal injuries with resultant paraspinal hematoma may account for the appearance of a retroperitoneal hematoma, particularly one that displaces the aorta and IVC anteriorly. Sagittal and coronal MPR images cre-ated at 2.5-mm intervals from visceral helical CT
Figure 19. Large zone II (lateral) retroperitoneal he-matoma in a 17-year-old boy who was involved in a high-speed motor vehicle collision. Contrast-enhanced CT scan shows right-sided perirenal and posterior pararenal retroperitoneal hematoma (white arrowheads) from a right renal laceration, with active extravasation of intravascular contrast material (black arrow) from a renal parenchymal injury. A laceration of the right kidney is also visible (black arrowhead). Note the hyperenhancing, thickened small bowel (white arrows) due to shock.
Figure 20. Paraspinal hematoma due to a burst fracture in a 19-year-old woman who was involved in a motor ve-hicle collision. (a) Contrast-enhanced CT scan obtained through the upper pelvis shows a paraspinal hematoma (ar-rowheads) that surrounds the L5 vertebral body. (b) CT scan (bone window) shows a burst fracture of L5 (arrow). (c) Sagittal reformatted CT image of the lumbar spine obtained from the initial acquisition data set better depicts the burst fracture, with posterior cortex retropulsion (arrow) and narrowing of the central spinal canal (arrowheads).
1586 October Special Issue 2008 RG ■ Volume 28 • Number 6
the thorax is more commonly seen, particularly in patients with a pneumothorax who are on me-chanical ventilation (53). Airway injury anywhere from the pharynx to the alveolus can produce pneumomediastinum and, in turn, pneumoret-roperitoneum. Esophageal perforation producing pneumomediastinum is another potential source of retroperitoneal air. The finding of pneumoret-roperitoneum in the setting of trauma should be accounted for on the basis of retroperitoneal injury or air tracking into the retroperitoneum from the chest. Figure 23 shows pneumoretro-peritoneum from mediastinal air tracking into the retroperitoneum following an airway injury.
Retroperitoneal AirThe presence of retroperitoneal air should raise suspicion for a perforated retroperitoneal vis-cus in the setting of both blunt and penetrating abdominal trauma. Isolated pneumoretroperi-toneum in the anterior pararenal space adjacent to the duodenum is suggestive of a duodenal perforation (53). Likewise, localized pericolonic retroperitoneal air is suggestive of colonic perfo-ration (54). Pneumoretroperitoneum from com-munications between the retroperitoneum and
Figure 21. Paraspinal hematoma from a traumatic compression fracture. (a) Abdominal CT scan shows a paraspi-nal hematoma (arrowheads) surrounding the T12 vertebral body. (b) Abdominal CT scan (bone window [window width = 1200 HU, window level = 300 HU]) shows a traumatic compression fracture of T12 (arrows). (c) Lateral scout image also depicts the fracture (arrow).
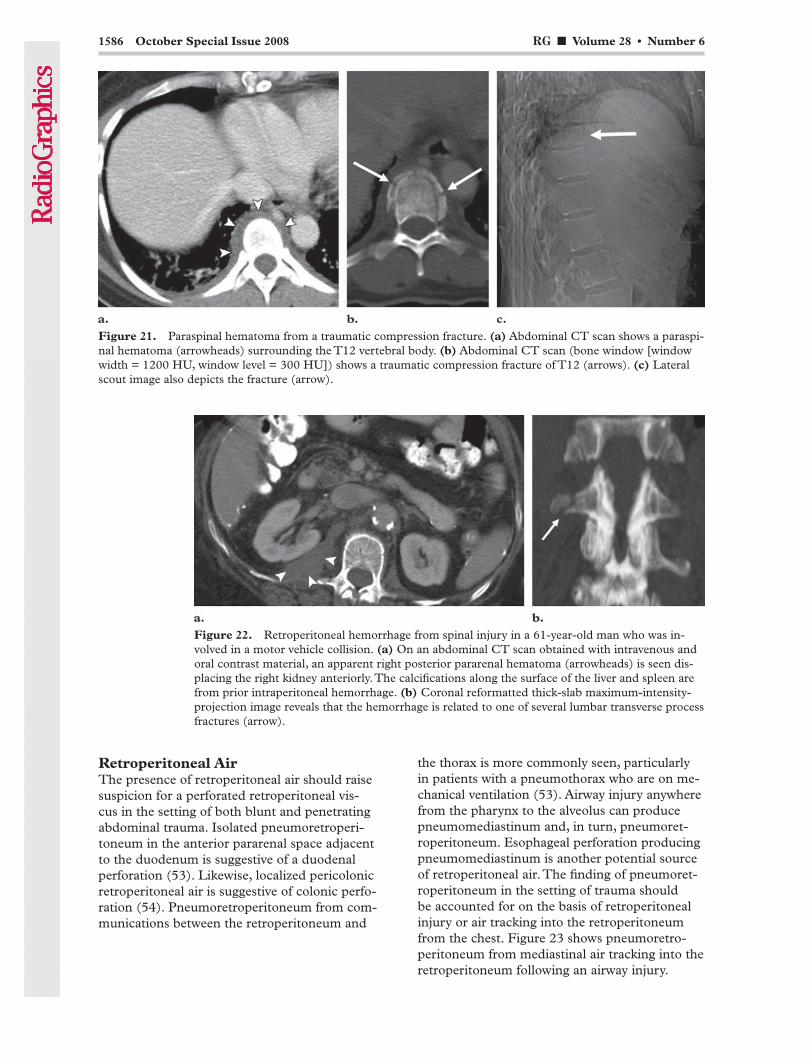
Figure 22. Retroperitoneal hemorrhage from spinal injury in a 61-year-old man who was in-volved in a motor vehicle collision. (a) On an abdominal CT scan obtained with intravenous and oral contrast material, an apparent right posterior pararenal hematoma (arrowheads) is seen dis-placing the right kidney anteriorly. The calcifications along the surface of the liver and spleen are from prior intraperitoneal hemorrhage. (b) Coronal reformatted thick-slab maximum-intensity-projection image reveals that the hemorrhage is related to one of several lumbar transverse process fractures (arrow).

RG ■ Volume 28 • Number 6 Daly et al 1587
vere trauma that can result as a response to shock (55). Imaging findings of hypoperfusion shock complex include diffusely thickened, enhancing bowel; hyperenhancing parenchymal organs; and decreased caliber of the aorta and IVC. Extracel-lular fluid is frequently present and can be seen surrounding the pancreas, within other retroperi-toneal spaces, and within the pelvis in the ab-sence of retroperitoneal injury (Fig 24) (55,58).
Retroperitoneal FluidThe presence of fluid within the retroperitoneum in the setting of trauma should raise suspicion for pancreatic injury, duodenal injury, renal collect-ing system injury (with urine leakage), or retro-peritoneal hemorrhage. However, low-attenuation (<20 HU) retroperitoneal fluid accumulation can be seen in the absence of retroperitoneal injury (55–57). Hypoperfusion shock complex is an infrequently encountered entity in victims of se-
Figure 23. Retroperitoneal air in a 40-year-old man who was involved in a motor vehicle collision. The patient, who had bilateral pneumothoraces, underwent bilateral chest tube placement and was placed on mechanical ventila-tion. (a) Abdominal CT scan obtained with intravenous contrast material shows extraluminal air (arrowheads) in the right perirenal space, in the anterior pararenal space, and along the fascial planes of the abdominal musculature. (b) Coronal MPR CT image of the chest and abdomen (lung window) shows extensive pulmonary contusions, sub-cutaneous emphysema, and mediastinal and retroperitoneal air. A right upper lobe bronchial laceration with a resul-tant air leak was discovered.
Figure 24. Retroperitoneal fluid without retroperitoneal organ injury. (a) Abdominal CT scan shows fluid within the anterior pararenal space (arrowheads) diffusely surrounding the pancreas. (b) CT scan shows thickening and hyperenhancement of the small bowel (arrows), findings that are due to hypoperfusion shock complex with extracel-lular fluid accumulation following shock and resuscitation. Pancreatic enzyme levels were not elevated. No intraab-dominal injury could be identified.

1588 October Special Issue 2008 RG ■ Volume 28 • Number 6
rising serum amylase level, persistent abdominal pain, or clinical signs of retroperitoneal injury (4,17,42).
3. If fluid is found in the retroperitoneum, try to determine the source and note whether the fluid is diffuse or focal.
4. Look for a sentinel clot.5. Seek out active extravasation near the larg-
est clot or the sentinel clot.6. Duodenal perforation and complete pancre-
atic transection necessitate urgent surgery (4).7. Active extravasation can be managed angio-
graphically or surgically.
ConclusionsAssessment of the retroperitoneum is critical in the radiologic evaluation of patients who have sustained blunt abdominal trauma. Multidetector CT can allow accurate posttraumatic assessment of patients, including the detection of retroperi-toneal injuries, which can be subtle (2). Recogni-tion of abnormal blood, fluid, or air within the retroperitoneal spaces is the key to correctly iden-tifying duodenal, pancreatic, vascular, renal, ad-renal, and paraspinal injuries (1,7,10). Equivocal findings at initial abdominal CT should prompt close clinical follow-up with possible imaging follow-up, particularly for suspected occult duo-denal and pancreatic injuries (4,17,42).
References 1. Porter JM, Singh Y. Value of computed tomography
in the evaluation of retroperitoneal organ injury in blunt abdominal trauma. Am J Emerg Med 1998; 16(3):225–227.
2. Fang JF, Wong YC, Lin BC, Hsu YP, Chen MF. Usefulness of multidetector computed tomogra-phy for the initial assessment of blunt abdominal trauma patients. World J Surg 2006;30(2):176–182.
3. Friese RS, Malekzadeh S, Shafi S, Gentilello LM, Starr A. Abdominal ultrasound is an unreliable modality for the detection of hemoperitoneum in patients with pelvic fracture. J Trauma 2007;63(1): 97–102.
4. Jurkovich GJ, Bulger, EM. Duodenum and pan-creas. In: Moore EE, Feliciano DV, Mattox KL, eds. Trauma. 5th ed. New York, NY: McGraw-Hill, 2004;709–733.
5. Ilahi O, Bochicchio GV, Scalea TM. Efficacy of computed tomography in the diagnosis of pancre-atic injury in adult blunt trauma patients: a single-institutional study. Am Surg 2002;68(8):704–707.
6. Ahvenjarvi L, Mattila L, Ojala R, Tervonen O. Value of multidetector computed tomography in assessing blunt multitrauma patients. Acta Radiol 2005;46(2):177–183.
7. Demetriades D, Velmahos G. Indications for lapa-rotomy. In: Moore EE, Feliciano DV, Mattox KL, eds. Trauma. 5th ed. New York, NY: McGraw-Hill, 2004;593–612.
Retroperitoneal fluid accumulation can be seen in the setting of abdominal compartment syndrome, resulting from pathologic elevation of intraabdominal pressure. In a small retrospec-tive review of four patients with surgically proved abdominal compartment syndrome, common CT findings included dense infiltration of the retro-peritoneum out of proportion to the peritoneal disease, extrinsic compression of the IVC by ret-roperitoneal hemorrhage or exudates, and mas-sive abdominal distention (56). Renal compres-sion, inguinal herniation, and bowel wall thicken-ing with enhancement can also be seen. Because abdominal compartment syndrome requires emergent surgical decompression, radiologic findings of increased intraabdominal pressure should be promptly communicated to other phy-sicians involved in treating the patient (56,59).
Resuscitation effects alone can result in the appearance of low-attenuation retroperitoneal fluid (58). Concomitant intrahepatic peripor-tal low attenuation (ie, edema) may be present, even in the absence of hepatic injury (58). The proposed mechanism is elevated central venous pressure caused by rapid expansion of intravas-cular volume (60). In addition, small amounts of fluid can be seen in the dependent portion of the peritoneal pelvic cavity due to the same mecha-nism (57). The radiologist must exclude underly-ing injury—particularly injury to the pancreas, duodenum, or renal collecting system—before concluding that the presence of low-attenuation retroperitoneal fluid is likely the result of resusci-tation or shock. Because both pancreatic and du-odenal injuries can be subtle at initial CT, close clinical observation with possible imaging follow-up should be considered in cases of equivocal CT findings (17,42).
Diagnostic ApproachOur proposed algorithm for the diagnosis of trau-matic retroperitoneal injuries includes the follow-ing considerations:
1. Recognize abnormal blood, fluid, or air in the retroperitoneum that may be the clue to subtle organ injury.
2. If initial CT yields abnormal but equivocal retroperitoneal findings, close clinical observa-tion with possible imaging follow-up should be considered, particularly in the presence of an ap-propriate injury mechanism, associated injuries, a
TeachingPoint

RG ■ Volume 28 • Number 6 Daly et al 1589
26. Wilson RH, Moorehead RJ. Current management of trauma to the pancreas. Br J Surg 1991;78(10): 1196–1202.
27. Wolf A, Bernhardt J, Patrzyk M, Heidecke CD. The value of endoscopic diagnosis and the treatment of pancreas injuries following blunt abdominal trauma. Surg Endosc 2005;19(5):665–669.
28. Teh SH, Sheppard BC, Mullins RJ, Schreiber MA, Mayberry JC. Diagnosis and management of blunt pancreatic ductal injury in the era of high-resolution computed axial tomography. Am J Surg 2007;193(5):641–643.
29. Lane MJ, Mindelzun RE, Sandhu JS, McCormick VD, Jeffrey RB. CT diagnosis of blunt pancreatic trauma: importance of detecting fluid between the pancreas and the splenic vein. AJR Am J Roent-genol 1994;163(4):833–835.
30. Sivit CJ, Eichelberger MR. CT diagnosis of pan-creatic injury in children: significance of fluid sepa-rating the splenic vein and the pancreas. AJR Am J Roentgenol 1995;165(4):921–924.
31. Wong YC, Wang LJ, Lin BC, Chen CJ, Lim KE, Chen RJ. CT grading of blunt pancreatic injuries: prediction of ductal disruption and surgical cor-relation. J Comput Assist Tomogr 1997;21(2):246–250.
32. Sinelnikov AO, Abujudeh HH, Chan D, Novelline RA. CT manifestations of adrenal trauma: experi-ence with 73 cases. Emerg Radiol 2007;13(6):313–318.
33. Rana AI, Kenney PJ, Lockhart ME, et al. Adrenal gland hematomas in trauma patients. Radiology 2004;230(3):669–675.
34. Burks DW, Mirvis SE, Shanmuganathan K. Acute adrenal injury after blunt trauma: CT findings. AJR Am J Roentgenol 1992;158(3):503–507.
35. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F. CT time-attenuation wash-out curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol 1998;170(3):747–752.
36. Caoili EM, Korobkin M, Francis IR, Platt JF, Dun-nick NR, Raghupathi KI. Adrenal masses: charac-terization with combined unenhanced and delayed enhanced CT. Radiology 2002;222(3):629–633.
37. Steenburg SD, Ravenel JG. Multi-detector com-puted tomography findings of atypical blunt trau-matic aortic injuries: a pictorial review. Emerg Radiol 2007;14(3):143–150.
38. Roth SM, Wheeler JR, Gregory RT, et al. Blunt injury of the abdominal aorta: a review. J Trauma 1997;42(4):748–755.
39. Lalancette M, Scalabrini B, Martinet O. Seat-belt aorta: a rare injury associated with blunt abdomi-nal trauma. Ann Vasc Surg 2006;20(5):681–683.
40. Mozingo JR, Denton IC Jr. The neurological deficit associated with sudden occlusion of abdominal aorta due to blunt trauma. Surgery 1975;77(1): 118–125.
41. Netto FA, Tien H, Hamilton P, et al. Diagnosis and outcome of blunt caval injuries in the modern trauma center. J Trauma 2006;61(5):1053–1057.
8. Kawashima A, Sandler CM, Corl FM, et al. Imag-ing of renal trauma: a comprehensive review. Ra-dioGraphics 2001;21(3):557–574.
9. Park SJ, Kim JK, Kim KW, Cho KS. MDCT find-ings of renal trauma. AJR Am J Roentgenol 2006; 187(2):541–547.
10. Killeen KL, DeMeo JH, Cole TJ. Computed to-mography of traumatic and nontraumatic retro-peritoneal emergencies. Emerg Radiol 1999;6(4): 232–243.
11. Ishikawa K, Tohira H, Mizushima Y, Matsuoka T, Mizobata Y, Yokota J. Traumatic retroperitoneal hematoma spreads through the interfascial planes. J Trauma 2005;59(3):595–608.
12. Scialpi M, Scaglione M, Angelelli G, et al. Emer-gencies in the retroperitoneum: assessment of spread of disease by helical CT. Eur J Radiol 2004; 50(1):74–83.
13. Patten RM, Spear RP, Vincent LM, Hesla RB, Jurkovich GJ. Traumatic laceration of the liver lim-ited to the bare area: CT findings in 25 patients. AJR Am J Roentgenol 1993;160(5):1019–1022.
14. Mullinix AJ, Foley WD. Multidetector computed tomography and blunt thoracoabdominal trauma. J Comput Assist Tomogr 2004;28(suppl 1):S20–S27.
15. Stuhlfaut JW, Anderson SW, Soto JA. Blunt ab-dominal trauma: current imaging techniques and CT findings in patients with solid organ, bowel, and mesenteric injury. Semin Ultrasound CT MR 2007;28(2):115–129.
16. Stuhlfaut JW, Soto JA, Lucey BC, et al. Blunt ab-dominal trauma: performance of CT without oral contrast material. Radiology 2004;233(3):689–694.
17. Allen GS, Moore FA, Cox CS Jr, Mehall JR, Duke JH. Delayed diagnosis of blunt duodenal injury: an avoidable complication. J Am Coll Surg 1998; 187(4):393–399.
18. Shorr RM, Greaney GC, Donovan AJ. Injuries of the duodenum. Am J Surg 1987;154(1):93–98.
19. Ballard RB, Badellino MM, Eynon CA, Spott MA, Staz CF, Buckman RF Jr. Blunt duodenal rupture: a 6-year statewide experience. J Trauma 1997; 43(2):229–232.
20. Moore EE, Cogbill TH, Malangoni MA, et al. Or-gan injury scaling. II. Pancreas, duodenum, small bowel, colon, and rectum. J Trauma 1990;30(11): 1427–1429.
21. Mirvis SE, Gens DR, Shanmuganathan K. Rup-ture of the bowel after blunt abdominal trauma: diagnosis with CT. AJR Am J Roentgenol 1992; 159(6):1217–1221.
22. Kunin JR, Korobkin M, Ellis JH, Francis IR, Kane NM, Siegel SE. Duodenal injuries caused by blunt abdominal trauma: value of CT in differentiating perforation from hematoma. AJR Am J Roentgenol 1993;160(6):1221–1223.
23. Orwig D, Federle MP. Localized clotted blood as evidence of visceral trauma on CT: the sentinel clot sign. AJR Am J Roentgenol 1989;153(4):747–749.
24. Sherck J, Shatney C, Sensaki K, Selivanov V. The accuracy of computed tomography in the diagnosis of blunt small-bowel perforation. Am J Surg 1994; 168(6):670–675.
25. Venkatesh SK, Wan JM. CT of blunt pancreatic trauma: a pictorial essay. Eur J Radiol 2007 Aug 18 [Epub ahead of print].

1590 October Special Issue 2008 RG ■ Volume 28 • Number 6
does thin-slice multidetector-row CT increase di-agnostic accuracy? Eur Radiol 2004;14(10):1751–1760.
52. Roos JE, Hilfiker P, Platz A, et al. MDCT in emer-gency radiology: is a standardized chest or abdomi-nal protocol sufficient for evaluation of thoracic and lumbar spine trauma? AJR Am J Roentgenol 2004;183(4):959–968.
53. Cho KC, Baker SR. Extraluminal air: diagnosis and significance. Radiol Clin North Am 1994; 32(5):829–844.
54. Cothren C, Moore EE, Huerd SS, Gunberg S. Is laparotomy mandated for retroperitoneal free air following blunt abdominal trauma? J Trauma 2001; 51(5):994–996.
55. Ryan MF, Hamilton PA, Sarrazin J, Chu P, Benja-minov O, Lam K. The halo sign and peripancreatic fluid: useful CT signs of hypovolaemic shock com-plex in adults. Clin Radiol 2005;60(5):599–607.
56. Pickhardt PJ, Shimony JS, Heiken JP, Buchman TG, Fisher AJ. The abdominal compartment syn-drome: CT findings. AJR Am J Roentgenol 1999; 173(3):575–579.
57. Chapman VM, Rhea JT, Sacknoff R, Novelline RA. CT of nontraumatic abdominal fluid collections after initial fluid resuscitation of patients with major burns. AJR Am J Roentgenol 2004;182(6):1493–1496.
58. Karcaaltincaba M, Haliloglu M, Akpinar E, et al. Multidetector CT and MRI findings in periportal space pathologies. Eur J Radiol 2007;61(1):3–10.
59. Sivit CJ, Taylor GA, Bulas DI, Kushner DC, Potter BM, Eichelberger MR. Posttraumatic shock in chil-dren: CT findings associated with hemodynamic instability. Radiology 1992;182(3):723–726.
60. Shanmuganathan K, Mirvis SE, Amoroso M. Peri-portal low density on CT in patients with blunt trauma: association with elevated venous pressure. AJR Am J Roentgenol 1993;160(2):279–283.
42. Huerta S, Bui TD, Nguyen TH, Banimahd FN, Porral D, Dolich MO. Predictors of mortality and management of patients with traumatic inferior vena cava injuries. Am Surg 2006;72(4):290–296.
43. Goins WA, Rodriguez A, Lewis J, Brathwaite CE, James E. Retroperitoneal hematoma after blunt trauma. Surg Gynecol Obstet 1992;174(4):281–290.
44. Madiba TE, Muckart DJ. Retroperitoneal haema-toma and related organ injury: management ap-proach. S Afr J Surg 2001;39(2):41–45.
45. Mirvis SE. Injuries to the urinary system and ret-roperitoneum. In: Mirvis SE, Shanmuganathan K, eds. Imaging in trauma and critical care. 2nd ed. Philadelphia, Pa: Saunders, 2003; 507–516.
46. Feliciano DV. Abdominal vascular injury. In: Moore EE, Feliciano DV, Mattox KL, eds. Trauma. 5th ed. New York, NY: McGraw-Hill, 2004; 755–777.
47. Selivanov V, Chi HS, Alverdy JC, Morris JA Jr, Sheldon GF. Mortality in retroperitoneal hema-toma. J Trauma 1984;24(12):1022–1027.
48. Feliciano DV. Management of traumatic retroperi-toneal hematoma. Ann Surg 1990;211(2):109–123.
49. Bagley LJ. Imaging of spinal trauma. Radiol Clin North Am 2006;44(1):1–12.
50. Sheridan R, Peralta R, Rhea J, Ptak T, Novelline R. Reformatted visceral protocol helical computed tomographic scanning allows conventional radio-graphs of the thoracic and lumbar spine to be elim-inated in the evaluation of blunt trauma patients. J Trauma 2003;55(4):665–669.
51. Herzog C, Ahle H, Mack MG, et al. Traumatic in-juries of the pelvis and thoracic and lumbar spine:
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see accompanying test at http://www.rsna.org/education/rg_cme.html.

RG Volume 28 • Volume 6 • October 2008 Daly et al
Traumatic Retroperitoneal Injuries: Review of Multidetector CT Findings Kevin P. Daly, MD, et al
Page 1572 Accurate radiologic characterization of injury can help in selecting patients who need urgent surgical intervention, as opposed to those in whom nonoperative management is possible, particularly since the morbidity rate for an unnecessary laparotomy (ie, completely negative findings or nontherapeutic results) in the setting of trauma is between 8.6% and 25.9%. Page 1575 Extraluminal air is a reliable sign of duodenal perforation and is highly predictive of such perforation in the absence of pneumothorax or prior diagnostic peritoneal lavage. Page 1577 Because of the high morbidity and mortality rates associated with delayed treatment, the trauma team and radiologist should remain vigilant if there is a high degree of suspicion for pancreatic injury based on injury mechanism, clinical findings, or unexplained hyperamylasemia. Page 1583 The goals of imaging are to identify the retroperitoneal hemorrhage, its location, and its possible source and to assess its relative stability on the basis of the size and presence (or absence) of active extravasation of intravascular contrast material. Page 1588 Recognition of abnormal blood, fluid, or air within the retroperitoneal spaces is the key to correctly identifying duodenal, pancreatic, vascular, renal, adrenal, and paraspinal injuries.
RadioGraphics 2008; 28:1571–1590 • Published online 10.1148/rg.286075141 • Content Codes:

RadioGraphics 2008 This is your reprint order form or pro forma invoice
(Please keep a copy of this document for your records.)
Author Name _______________________________________________________________________________________________ Title of Article _______________________________________________________________________________________________ Issue of Journal_______________________________ Reprint # _____________ Publication Date ________________ Number of Pages_______________________________ KB # _____________ Symbol RadioGraphics Color in Article? Yes / No (Please Circle) Please include the journal name and reprint number or manuscript number on your purchase order or other correspondence. Order and Shipping Information Reprint Costs (Please see page 2 of 2 for reprint costs/fees.) ________ Number of reprints ordered $_________ ________ Number of color reprints ordered $_________ ________ Number of covers ordered $_________ Subtotal $_________ Taxes $_________ (Add appropriate sales tax for Virginia, Maryland, Pennsylvania, and the District of Columbia or Canadian GST to the reprints if your order is to be shipped to these locations.) First address included, add $32 for each additional shipping address $_________
TOTAL $_________
Shipping Address (cannot ship to a P.O. Box) Please Print Clearly Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ____________________ State _____ Zip ___________ Country ___________________________________________ Quantity___________________ Fax ___________________ Phone: Day _________________ Evening _______________ E-mail Address _____________________________________ Additional Shipping Address* (cannot ship to a P.O. Box) Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ________________ State ______ Zip ___________
Country _________________________________________ Quantity __________________ Fax __________________ Phone: Day ________________ Evening ______________ E-mail Address ____________________________________ * Add $32 for each additional shipping address
Payment and Credit Card Details Enclosed: Personal Check ___________ Credit Card Payment Details _________ Checks must be paid in U.S. dollars and drawn on a U.S. Bank. Credit Card: __ VISA __ Am. Exp. __ MasterCard Card Number __________________________________ Expiration Date_________________________________ Signature: _____________________________________ Please send your order form and prepayment made payable to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box.
FEIN #:541274108
Invoice or Credit Card Information Invoice Address Please Print Clearly Please complete Invoice address as it appears on credit card statement Name ____________________________________________ Institution ________________________________________ Department _______________________________________ Street ____________________________________________ City ________________________ State _____ Zip _______ Country ___________________________________________ Phone _____________________ Fax _________________ E-mail Address _____________________________________ Cadmus will process credit cards and Cadmus Journal
Services will appear on the credit card statement. If you don’t mail your order form, you may fax it to 410-820-9765 with
your credit card information. Signature __________________________________________ Date _______________________________________ Signature is required. By signing this form, the author agrees to accept the responsibility for the payment of reprints and/or all charges described in this document.
Reprint order forms and purchase orders or prepayments must be received 72 hours after receipt of form either by mail or by fax at 410-820-9765. It is the policy of Cadmus Reprints to issue one invoice per order.
Please print clearly.
Page 1 of 2 RB-9/26/07

RadioGraphics 2008 Black and White Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $221 $233 $268 $285 $303 $323 5-8 $355 $382 $432 $466 $510 $544 9-12 $466 $513 $595 $652 $714 $775
13-16 $576 $640 $749 $830 $912 $995 17-20 $694 $775 $906 $1,017 $1,117 $1,22021-24 $809 $906 $1,071 $1,200 $1,321 $1,47125-28 $928 $1,041 $1,242 $1,390 $1,544 $1,68829-32 $1,042 $1,178 $1,403 $1,568 $1,751 $1,924
Covers $97 $118 $215 $323 $442 $555
International (includes Canada and Mexico) # of
Pages 50 100 200 300 400 500
1-4 $272 $283 $340 $397 $446 $506 5-8 $428 $455 $576 $675 $784 $884 9-12 $580 $626 $805 $964 $1,115 $1,278
13-16 $724 $786 $1,023 $1,232 $1,445 $1,65217-20 $878 $958 $1,246 $1,520 $1,774 $2,03021-24 $1,022 $1,119 $1,474 $1,795 $2,108 $2,42625-28 $1,176 $1,291 $1,700 $2,070 $2,450 $2,81329-32 $1,316 $1,452 $1,936 $2,355 $2,784 $3,209
Covers $156 $176 $335 $525 $716 $905 Minimum order is 50 copies. For orders larger than 500 copies, please consult Cadmus Reprints at 800-407-9190. Reprint Cover Cover prices are listed above. The cover will include the publication title, article title, and author name in black. Shipping Shipping costs are included in the reprint prices. Domestic orders are shipped via UPS Ground service. Foreign orders are shipped via a proof of delivery air service. Multiple Shipments Orders can be shipped to more than one location. Please be aware that it will cost $32 for each additional location. Delivery Your order will be shipped within 2 weeks of the journal print date. Allow extra time for delivery.
Color Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $223 $239 $352 $473 $597 $719 5-8 $349 $401 $601 $849 $1,099 $1,3499-12 $486 $517 $852 $1,232 $1,609 $1,992
13-16 $615 $651 $1,105 $1,609 $2,117 $2,62417-20 $759 $787 $1,357 $1,997 $2,626 $3,26021-24 $897 $924 $1,611 $2,376 $3,135 $3,90525-28 $1,033 $1,071 $1,873 $2,757 $3,650 $4,53629-32 $1,175 $1,208 $2,122 $3,138 $4,162 $5,180
Covers $97 $118 $215 $323 $442 $555
International (includes Canada and Mexico)) # of
Pages 50 100 200 300 400 500
1-4 $278 $290 $424 $586 $741 $904 5-8 $429 $472 $746 $1,058 $1,374 $1,6909-12 $604 $629 $1,061 $1,545 $2,011 $2,494
13-16 $766 $797 $1,378 $2,013 $2,647 $3,28017-20 $945 $972 $1,698 $2,499 $3,282 $4,06921-24 $1,110 $1,139 $2,015 $2,970 $3,921 $4,87325-28 $1,290 $1,321 $2,333 $3,437 $4,556 $5,66129-32 $1,455 $1,482 $2,652 $3,924 $5,193 $6,462
Covers $156 $176 $335 $525 $716 $905 Tax Due Residents of Virginia, Maryland, Pennsylvania, and the District of Columbia are required to add the appropriate sales tax to each reprint order. For orders shipped to Canada, please add 7% Canadian GST unless exemption is claimed. Ordering Reprint order forms and purchase order or prepayment is required to process your order. Please reference journal name and reprint number or manuscript number on any correspondence. You may use the reverse side of this form as a proforma invoice. Please return your order form and prepayment to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box. FEIN #:541274108 Please direct all inquiries to:
Rose A. Baynard 800-407-9190 (toll free number) 410-819-3966 (direct number) 410-820-9765 (FAX number)
[email protected] (e-mail)
Reprint Order Forms and purchase order or prepayments must be received 72 hours after receipt of form.
Page 2 of 2