trust board meeting – part 1 public session€¦ · review 10.00: enclosure b 6. chairman’s...
TRANSCRIPT

AGENDA
Trust Board Meeting – Part 1 Public Session Date: Thursday 1st December 2011 Time: 10.00 to 13.30 (approx) Venue: The Hall, Shaw House, Church Road,
Newbury, Berks RG14 2DR
__________________________________________________________________________ No.
Enclosures
1. Chairman’s Welcome and Apologies for Absence
Note (Verbal)
2. Declaration of Directors’ Interest Members are reminded of their obligation to declare any interest they may have in any issue arising at the meeting, which might conflict with the business of the Trust
Confirm (Verbal)
3. Minutes from the Previous Meetings Trevor Jones - Chairman 28 September 2011
Approve
Enclosure A
4. Confirmation of any part of the Minutes that is exempt under the Freedom of Information Act 2000
Confirm (Verbal)
5. Matters Arising (Any items not covered elsewhere on the Agenda)
Review
10.00
Enclosure B
6. Chairman’s Report Trevor Jones - Chairman
Note 10.15 (Verbal)
7. Chief Executive’s Report Will Hancock - Chief Executive
Assurance 10.25 Enclosure C
QUALITY AND PATIENT SAFETY
8. Quality & Patient Safety Report (Month 7) Fizz Thompson - Director of Patient Care
Assurance 10.45 Enclosure D
9. Quality Accounts – 6 month Review Fizz Thompson - Director of Patient Care
Assurance 11.15 Enclosure F
11.30 – 11.40: COMFORT BREAK (10 mins)

No.
Enclosures
FOUNDATION TRUST STATUS 10. FT Status Assurance Report
John Divall - FT Project Director
Assurance 11.40 Enclosure G
11. FT Application - Board Submissions to Monitor John Divall - FT Project Director
Approve
11.45 Enclosure H
FINANCIAL AND SERVICE PERFORMANCE
12. Integrated Performance and Finance Report for the month ended 31 October 2011 (Month 7) Charles Porter - Director of Finance Integrated Performance Report Finance and Estates Report HDD Action Plan - Exception Report
Approve Approve Note
12.00 Enclosure I Enclosure J.1 Enclosure J.2
STRATEGY, POLICY AND IMPLEMENTATION 13. Operations and Clinical Review – Progress Report
Ian Ferguson - Chief Operating Officer
Assurance
12.30 Enclosure K
REGULATORY, COMPLIANCE & CORPORATE GOVERNANCE
14. Strategic Risk Register and Board Assurance Framework - Six Month Review Fizz Thompson - Director of Patient Care
Assurance 13.00 Enclosure L
BOARD SUB COMMITTEE MINUTES AND CHAIR EXCEPTION REPORTS (All Minutes have been duly approved by the respective Committee Chair but owing to the timing of meetings may not have been formally approved by the relevant Committee) 15. Remuneration and Nomination Committee
(Chair’s Exception Report only) Alastair Mitchell-Baker - Committee Chair 20 October 2011
Note (Verbal)
16. Audit Committee Eddie Weiss - Committee Chair 14 November 2011 (Chair’s Exception Report only)
Note
13.10
Enclosure M
17. Quality and Safety Committee Keith Nuttall - Committee Chair 13 October 2011 (Chair’s Exception Report and Minutes)
Note
13.15
Enclosure N
18. Charitable Trust Funds Committee Claire Carless - Committee Chair 22 September 2011 (Minutes only)
Note
13.20
Enclosure O
ANY OTHER BUSINESS (Should only normally include any matters previously notified to the Chairman at least 48 hours prior to the date of meeting).
13.25 (Verbal)

No.
Enclosures
19. Date and Time of Next Meeting held in Public : Date: Wednesday 21 December 2012 Time: 10.00 am Venue: The Hall, Shaw House, Church Road,
Newbury, Berks RG14 2DR
Confirm (Verbal)
RESOLUTION TO EXCLUDE MEMBERS OF THE PUBLIC
20. Members of the Board are invited to resolve : a) THAT the meeting be adjourned to invite informal questions
relating to the business of meeting; and b) THAT representatives of the press and members of the public
be excluded from the remainder of the meeting as any publicity would be prejudicial to the public interest by reason of the confidential nature of the business.
21. 22. 23. Close of public session of the meeting
13.30
13.30 – 14.00: LUNCH BREAK (30 mins)
CONFIDENTIAL PART 2 (The following items will be deliberated in the private session of the meeting. Due to the confidential nature of the business to be transacted, papers and minutes are not published for this part of the meeting).
14.00
General Business 24. Apologies 25. Declaration of Directors’ Interests 26. Confidential Minutes of the Board: 18 November 2011 17 November 2011 26 October 2011 28 September 2011 27. Freedom of Information Exemptions 28. Matters Arising 29. Chief Executive’s Confidential Report
Quality & Patient Safety Report (Month 7) 30. Serious Incident Requiring Investigation Report
Financial and Service Performance 31. Forecast and Recovery Plan 2011/12 - Progress Report 32. Monitor Downside Review 33. Commercial Division Turnaround - Progress Report
Business Development and Strategic Opportunities 34. NHS111 Pilots – Progress Report

No.
Enclosures
Board Sub-Committee Minutes and Chair‘s Exception Reports 35. Audit Committee - Minutes
14 Nov 2011
36. Remuneration and Nomination Committee - Chair’s Verbal Exception Report 20 Oct 2011
Information Items 37. Board Forward Planner 2011/12 38. Draft Agenda for Extraordinary: 21 January 2011
Board Effectiveness 39. Review of Board Meeting Performance
40. Date and Time of Next Board Meeting held in Private: Date: 21 December 2011 Time: 10.00 am Venue: Boardroom
Northern House Bicester

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 1 of 20
Trust Board Meeting
PART 1 SESSION HELD PUBLIC
MINUTES of a meeting of the Trust Board held in public at 10.30 am on Wednesday 28 September 2011
in the Board Room, Winchester & Eastleigh Resource Centre, Units 1-4 Woodside Road, Eastleigh, Hampshire
MEMBERS
Present: Trevor Jones Chairman (TJ) John Black Medical Director (JB) Duncan Burke* Director of Communications and Public
Engagement (DB)
Claire Carless Non Executive Director (CC) Paul Clarke* Interim Business Development Director (PC) Ian Ferguson Chief Operating Officer (IF) Will Hancock Chief Executive (WH) Alistair Mitchell-Burke Non Executive Director (AMB) Keith Nuttall Non Executive Director (KN) Charles Porter Director of Finance (CP) Fizz Thompson Director of Patient Care (FT) Eddie Weiss Non Executive Director (EW) * Non-voting Director In Attendance: Julie Dawes Company Secretarial Consultant (JVD) John Divall, MBE Foundation Trust Project Director (JD) Phil Pimlott MBE Assistant Director of Operation Support Services
(minutes 110 -120 only) (PP)
Sharon Walters Director of HR (minutes 126 -131 only) (SW) Vince Weldon Associate Director of IM&T (minutes 121 -125 only) (VW) Public: 5 members of the public Action Date
WELCOME AND INTRODUCTIONS
11/31 The Chairman welcomed everyone to the meeting and explained that it was a meeting of the Trust Board held in public and not a public meeting. Members were also asked to note that to facilitate the production of more accurate minutes, the proceedings of the meeting would be digitally recorded and that any recordings would be securely destroyed following the approval of the minutes by the Board.
APOLOGIES FOR ABSENCE
11/32 It was CONFIRMED that there were no apologies for absence.
South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 2 of 20
Action Date
DECLARATION OF DIRECTORS’ INTERESTS
11/33 The Chairman reminded members of their obligation to declare any interests in relation to any matter under consideration at the meeting which might conflict with the business of South Central Ambulance Service NHS Trust.
11/34 Subject to the deletion of Claire Carless’s interest in the Vodafone Group, it was CONFIRMED that there were no further declarations of interests. It was NOTED that the Corporate Secretary would update the Register of Directors’ Interests accordingly to reflect this change.
MINUTES FROM THE PREVIOUS MEETING:
27 July 2011 – Public Part 1 11/35 Subject to the following amendment, the Minutes of the Trust Board meeting
held in public on 27 July 2011 were received and APPROVED as a true and accurate record and accordingly signed by the Chair.
Minute 17 – Governance Framework (Page 7) 11/36 The last sentence should be deleted and be replaced with the following
words: “The Board were asked to note for the purpose of inclusion in the Governance Framework document and for completeness, that the Director of Patient Care is the Trust’s nominated Caldicott Guardian and Accountable Officer (Controlled) Drugs).
6 June 2011 – Extraordinary Board Meeting 11/37 The Minutes of the Extraordinary Trust Board meeting held on 6 June 2011
were received and APPROVED as a true and accurate record and accordingly signed by the Chair.
FREEDOM OF INFORMATION
11/38 It was CONFIRMED that no part of the Minutes as produced to the meeting were exempt under the Freedom of Information Act 2000.
MATTERS ARISING
11/39 Members reviewed the schedule of matters arising from the Minutes and the relevant comments against each of the agreed actions and CONFIRMED that the necessary assurances have been obtained from the Executive Team concerning the actions taken.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 3 of 20
Action Date
CHAIRMAN’S REPORT
11/40 The Chairman presented a verbal report and drew specific attention to the following matter:
Health and Social Care Bill 2011 11/41 The Chairman commented that the introduction of the Health and Social
Care Bill in January 2011 (the Health Bill) and the subsequent publication of the report by NHS Future Forum following the Government’s eight week listening exercise represented both risks and opportunities for the Trust and he emphasised the importance of the Ambulance Service being at the heart of the Government’s modernisation plans and for the Trust to be fully engaged with the process.
11/42 Following a brief discussion, it was RESOLVED that :
The Chairman’s verbal report be received and NOTED.
CHIEF EXECUTIVE’S REPORT
11/43 The Board received and considered an exception report from the Chief Executive which provided an update on activities since the previous meeting in July 2011, including the following issues:
Annual Plan Progress NHS Development CQC Stakeholder and Partnership Working Foundation Trust Monitor
In addition to the above, members were asked to NOTE the developments under the following areas:
Clinical and Operations Restructure 11/44 Good progress continues to be made in implementing the new structure. A
key milestone was the successful appointments to the two top tier management levels, including the Area Mangers. The Emergency Service Manager appointments were due to be completed shortly.
11/45 Whilst it was acknowledged that it was imperative for the Trust to limit the inevitable uncertainty for those mangers and staff members involved in the restructuring process, the Chief Operating Officer ASSURED members that

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 4 of 20
Action Date
he was confident that the Trust would achieve 90% of all the required appointments by the end of October 2011. Introduction of new Telephony System in Bicester Control Room
11/46 The introduction of the new telephony system in the Bicester Control Room has been successful resulting in an improvement in the Trust‘s call answering performance in five seconds, from 85% to 94.5%.
11/47 This improved performance is reflected in the recently published national quality indicators, which confirm that the Trust has progressed to middle of the ambulance service sector.
Specialised Networks 11/48 A pre-engagement exercise concerning a number of specialised networks is
currently being conducted on behalf of the three PCT clusters across the South Central region relating to the trauma network and the vascular network proposals. SCAS is currently providing the necessary input into this process.
Oxfordshire Joint Health Overview and Scrutiny Committee 11/49 The Chief Executive, Medical Director and Director of Communications and
Engagement attended the Oxfordshire Joint Health Overview and Scrutiny Committee on 15 September 2011 to provide an update on the Trust’s performance in Oxfordshire and also to highlight to the Committee the recent introduction of the new national performance targets. The Trust’s improved performance in the rural Oxfordshire areas was acknowledged by the Committee.
Following discussion, it was RESOLVED:
11/50 That the report of the Chief Executive be received and accordingly NOTED.
QUALITY AND PATIENT SAFETY REPORT
11/51 The Director of Patient Care presented the Quality and Safety Report for the month ended 31 August 2011 and explained that the purpose of the report was to update and assure Board members on the Trust’s quality, patient safety and clinical performance work stream areas.
11/52 Noting that all quality measures and metrics including the Clinical Performance Indicators and the new clinical outcome measures were now reported through the revised Integrated Performance Report (IPR), members were asked to NOTE the quality performance exceptions outlined in the report. In light of the ongoing concerns raised at previous meetings, specific attention was drawn to the following issue :
Increase in the number of reported complaints
South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 5 of 20
Action Date
11/53 This continues to be a cause of concern for the Trust with staff attitude being ranked as the main reason for a complaint. At the request of board members at the previous meeting, some benchmarking information has been included in the report which compares SCAS performance in relation to complaints against other ambulance services of a similar size.
11/54 The Director of Patient Care ASSURED members that the necessary actions were now in place to raise awareness of the reasons and types of complaints and to improve the areas identified in the recent investigations and that she would continue to benchmark against other Trust’s complaints data. It was REPORTED that whilst no immediate trends had yet been identified it was acknowledged that this would become a key consideration for the Board.
11/55 In response to a request for clarification about the number of days it takes the Trust to respond to complaints, the Director of Patient Care ASSURED members that complainants would receive a response from the Trust within the 25 working days specified nationally.
11/56 It was NOTED that this matter was scheduled for further consideration by the Quality and Safety Committee on 13 October 2011, with a view to the Trust obtaining a more in depth understanding concerning the actions and attitudes associated with complaints.
11/57 On the issue of benchmarking complaints, it was suggested that the Trust might in future wish to consider looking at the volume of complaints received from different sources such as via the Patient Advice and Liaison Service (PALs) and then investigating how this compares with other similar Trusts.
Care Quality Commission 11/58 Referring to the section in the report on the Care Quality Commission (CQC),
the Director of Patient Care informed the meeting that since writing the report the CQC have formally requested that the Trust provides evidence and a Provider Compliance Assessment on Outcome 11 relating to fleet and equipment. It was NOTED that this request appears to be as a consequence of two recently reported Serious Untoward Incidents (SUIs) concerning the malfunctioning of the back doors of specific ambulance vehicles whilst carrying cardiac arrest patients. In addition, it was understood that the CQC had also been copied into a complaint to the Trust concerning a specific piece of equipment which was missing from the back of an ambulance vehicle.
11/59 It was CONFIRMED that a complete review was being undertaken by the Trust and that an appropriate response would be issued to the CQC within the specified five working days. In addition, it was NOTED that this matter would be followed up with the local CQC compliance assessor.
11/60 The Director of Patient ASSURED members that whilst the complaint was still subject to investigation the matter was being taken extremely seriously within the Trust. Mitigating actions implemented include issuing additional

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 6 of 20
Action Date
procedural guidance to relevant staff concerning the door override mechanism, incorporating clear instructions on the vehicles through ‘Make Ready’ and notifying other Ambulance Trusts of the issues.
11/61 Following discussion, it was RESOLVED that:
a) The exceptions as outlined in the report and at the meeting be NOTED;
b) A seminar session focussing on how the Trust deals with three typical complaints case studies would be scheduled in the Board Development Programme;
FT JVD
29/02/12
c) The Board CONFIRMS that it has obtained the necessary assurances at the meeting that appropriate actions were being progressed where any improvements have been identified relating to the Trust’s current patient safety and quality performance; and
d) That the Quality and Patient Safety Report was received and accordingly NOTED.
FOUNDATION TRUST STATUS ASSURANCE REPORT
11/62 The Foundation Trust Project Director presented a report on the key developments since the August 2011 Board meeting held in private.
11/63 He drew attention to some of the feedback received from colleagues following the first week of the assessment meetings with Monitor and highlighted the emerging issues.
11/64 The Foundation Trust Project Director concluded the discussion by confirming that the Trust’s foundation trust application continues to progress to plan and that he was not aware of any further issues to bring to the attention of the Board.
11/65 Following discussion, it was RESOLVED that:
a) That a briefing note would be circulated to members on the proposed plans for the Board to engage with the Council of Governors;
DB 30/11/11
b) The Board CONFIRMS that it has obtained the necessary assurances at the meeting that appropriate actions were being progressed concerning the Trust’s journey towards achieving Foundation Trust status on 1 February 2012; and
c) That the Foundation Trust Assurance Report was received and accordingly NOTED.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 7 of 20
Action Date
CHARITABLE FUNDS COMMITTEE – NOMINATION OF CHAIR
11/66 The Chairman reported that following the resignation of Colin Hazell as a Non-Executive Director on 31 August 2011, a vacancy had arisen for the Chair of the Charitable Funds Committee. He explained that following discussions with Clare Carless she had expressed her willingness to act as Chair of this committee.
11/67 It was CONFIRMED that the membership of the Trust Board’s sub-committees and board lead roles would be reviewed again once both the Non-Executive Director (Designate) and vacant Non Executive Director posts had been filled.
Following discussion it was RESOLVED that :
11/68 In accordance with the terms of reference of the Charitable Trust Funds Committee (the Committee), the Board formally APPROVED the nomination by the Chairman of the Trust Board to appoint Claire Carless as Chair of the Committee, such appointment to take immediate effect.
FT MEMBERSHIP AND GOVERNORS ELECTION UPDATE
11/69 The Director of Communication and Public Engagement presented his report and explained that the purpose the report was to provide an update to the Board on the Trust’s progress in achieving a membership that is representative of its communities, in terms of location, age, gender and ethnicity. In light of the nomination closure date on 26 September 2011, the report also served to provide members with an update on the Governor election process.
11/70 It was REPORTED that confirmation had been received from the Electoral Reform Services (ERS), the Trust’s appointed provider of its governor election process that with the exception of the Oxfordshire, the requisite nominations had been received from all the other constituencies. DB explained that he was aware of two aspirant Foundation Trusts who were required to delay the start of their election process owing to insufficient governor nominations and that he was presently awaiting further guidance from ERS as to whether the Trust’s election could officially commence. It was NOTED that whilst most constituencies had received a large number of nominations, the nominees in three constituency areas would be elected unopposed.
11/71 Members were asked to note the following key dates in the governor election timetable:
Ballot papers issued: 13 October 2011 Closing date by election: 2 November 2011 Election results published: 3 November 2011

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 8 of 20
Action Date
11/72 Following discussion, it was RESOLVED that:
a) The details of the nominations for the Council of Governors would be circulated to Board members.
DB 14/10/11
b) The report of the update report on FT Membership and Governors Election be received and accordingly NOTED.
INTEGRATED PERFORMANCE REPORT (IPR)
11/73 The Director of Finance introduced the IPR for the five month period ended 31 August 2011 and explained that the purpose of the report was to highlight any variances in key performance areas and to outline what actions were being taken.
11/74 Referring to each red risk rated item in the report, the relevant executive lead provided the Board with assurances in relation to their specific area of responsibility. The following comments and challenges were made:
Clinical Performance 11/75 One of the main areas that management is focussing on is the new data set
relating to patients with return of spontaneous circulation. Whilst the new data currently available only relates to patient survival at one hospital, the numbers of actual cases are relatively small. Historically, the Trust’s performance in this area has been within the expected national targets, but new data reporting requires disclosure in relation to patient survival to discharge of which there is presently national benchmarking data available. Work is now being undertaken by both the Clinical Review Group and Quality and Safety Committee over the coming months to gain a better understanding of the position.
11/76 In response to a request for clarification about how the targets were set, it was NOTED that these were based on the historical data from the clinical performance indicators and that this was the first occasion that the patient survival to discharge indicator was being measured by the Trust.
11/77 On a related point about targets, members questioned the legitimacy of relying on management data which inappropriately focused Board attention on certain targets based on relatively small numbers and acknowledged the importance of the Board basing future analysis on appropriate measureable targets.
11/78 Noting that there appeared to be far greater number of items by which the
Trust was being performance measured, assurance was sought as to what steps that were being taken by the executive team to ensure the accuracy and integrity of the data provided to the Board. In response, it was CONFIRMED that all clinical performance data was properly validated and whilst some of this data which was being collected for the first time might

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 9 of 20
Action Date
require further refinement, there was a robust process in place for the Medical Director and Director of Patient Care to sign off all clinical performance data prior to inclusion in any Trust reports either for internal or external consumption.
Operational Performance 11/79 a) Turnaround A significant focus of attention in relation to turnaround has been in the area
of [clear-up] resulting in a 61% improvement on last year for the month. Efforts are now being re-directed on the contribution received from the hospitals. In this connection, a series of workshops involving managers from both SCAS and the hospitals will take place during November 2011 with the objective of improving every ones understanding of the process and how they should be escalating it. It was light of the continuing performance improvements at SCAS, a more proactive approach is being adopted in relation to specific acute hospitals with a view to assisting them in raising their performance.
b) Non-Conveyance 11/80 A recovery plan has been implemented to address the continuing poor non-
conveyance performance, which is being monitored through the Executive Management Committee. Recognising the importance of this issue, a board seminar session was scheduled for 20th October, with the objective of improving the Board’s understanding of the impact of non-conveyance and the different work-streams that underpin the Trust’s recovery plan.
c)Hear and Treat re-contacts in 24 hours 11/81 The Trust is presently working through its understanding of the parameters of
this new performance measure. With a view to improving performance a lead has been appointed to undertake a piece of work to identify the types of patient, and their circumstances, where re-contact occurs.
11/82 A challenge was made that the Board needs to be unambiguous as to what this measure actually means and that operationally, to avoid inconsistency in interpretation, further clarity should be provided throughout the Trust.
d) A & E Performance by PCT and PCT cluster 11/83 The Trust may incur a potential penalty due to the score of 94.5% in the
Hampshire PCT cluster forecast under the A19 performance target of 95%.
Safety and Risk Management a) Incidents reported to NPSA within 30 days. 11/84 It was confirmed that the figures in the report were inaccurate and do not
reflect the actual position.
b) Public liability claims 11/85 In response to a request for further details pertaining to the public liability
claim reported in August, as details were not available at the meeting it was confirmed that legal claim information is routinely reported to the Quality and
South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 10 of 20
Action Date
Safety Committee. Members were reminded that, following discussions at the previous Board meeting, the future reporting of legal claims to the Board from s governance perspective was presently under review by the Corporate Secretary.
c) Long waits (Amber) 11/86 Whilst the overall performance on long waits is under target, the position in
relation to the reported increase in amber waits is not entirely clear but is being actively monitored.
d) RIDDOR reports 11/87 The Quality and Safety Committee is currently reviewing whether the
increase in number of reportable incidents may be as a result of the increased awareness of staff following conflict resolution training and mandatory statutory training.
11/88 As the level of staff sickness absence due to manual handling and lifting incidents is considered to be an area of concern for SCAS, an action plan has been implemented to address this situation.
11/89 It was confirmed that the total number of days lost and the associated costs were being monitored by the Quality and Safety Committee.
e) Non-Physical Assaults 11/90 Whilst it is considered too early to accurately assess the impact of the recent
publicity regarding assaults on staff, assurance was provided that the position was being continually monitored.
Patient Experience 11/91 a) Investigation of complaints and transparency concerning SUIs The last Quality and Safety Committee discussed the outcomes of
investigating complaints specifically in the context of the Trust’s required transparency in relation to the reporting of Serious Untoward Incidents (SUIs). It was confirmed that this continues to be a key consideration for the Committee.
Finance 11/92 a) Surplus and Return on Assets The positions concerning performance on the Surplus and Return on Assets
targets were included the Finance presentation later in the meeting.
b) Debtors more than 90 days 11/93 Whilst a significant improvement was reported with a reduction from £622k to
£373k, the situation is being managed proactively.
c) CAPEX 11/94 Currently CAPEX performance is 75% below plan and this position is
expected to continue. It was acknowledged that the issue for consideration should be understanding the extent to which the Trust is doing something different which avoids expenditure or whether capital expenditure is being

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 11 of 20
Action Date
delayed for other reasons.
Cost Improvement Plans 11/95 a) Dual ECA In response to the request for clarification of whether the use of more private
providers than expected will delay the expected savings, it was confirmed that the numbers would remain static but that the required skills mix would change. It was CONFIRMED that the stringent criteria adopted for Dual ECAs would be applied to private providers and that the projected savings were expected to be realised quickly.
b) Sickness reduction 11/96 The Kronos system is now embedded and the necessary training is virtually
complete. Following the activation of the sickness absence module it is expected that the savings target will be achieved.
c) Hospital delays. 11/97 With reference to the hospital delays that occurred in Oxfordshire over the
previous weekend and in response to a request for further clarification as to how the Trust intends to engage with and support hospitals experiencing delays, it was CONFIRMED that responsibility for all static staff had been transferred to the newly appointed Area Managers. Further assurance was provided to the meeting that local area implementation plans as opposed to the previous Trust-wide plan had been introduced in order to achieve the required resilience in day-to-day operations and improve liaison with acute hospitals.
d) Project cost savings 11/98 Savings are slightly lower than planned owing to some extra TARP costs.
e) Property savings 11/99 Current position owing to phasing, however overall year to date performance
is on schedule.
Commercial Division 11/100 This discussion was deferred to the Part 2 session of the meeting.
Human Resources a) Sickness/absence 11/101 Whilst sickness rates in A&E Emergency Operations Centre were above
target, A&E Operations had shown improvements. Following the implementation of mitigation plans, reductions in sickness rates were expected to start in September. It was AGREED that the discussion concerning PTS performance would be deferred to the Part 2 session of the meeting.
b) Appraisals 11/102 Performance in appraisals has shown some improvement and the necessary
plans are in place to achieve the 95% target. It was emphasised that every effort should be made to avoid the stock-piling of appraisals to the last month

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 12 of 20
Action Date
of the year.
Programme of Change 2011-12 11/103 The Board were appraised on progress in relation to the key milestones in
the Trust’s programme of change for 2011-12.
11/104 Following discussion it was RESOLVED that :
a) A Board seminar session on baseline targets and reporting measures to be scheduled;
FT/IF 26/10/11
b) The Quality and Safety Committee would update the Board in relation to the reported public liability claim;
KN/FT 25/01/12
c) In relation to the Cost Improvement work stream, an update would be provided to the Board on the Corporate Review plans;
CP 21/12/11
d) The Key Milestones table would be produced in a larger font and preferably black type for future reports; and
CP 01/12/11
e) The Integrated Performance report be received and accordingly noted.
FINANCE AND ESTATES REPORT FOR MONTH 5
11/105 The Board received and considered In detail the Finance and Estates Report for the five month period ended 31 August 2011 together with a slide presentation summarising the position.
11/106 The following points were highlighted:
a) The results for the month show a small surplus which is £0.16m adverse of budget but overall, performance is on track with the implemented Recovery Plan. The source of the variation was the underperformance of the Commercial Division which was £0.17m lower than budget in the month.
b) The core A&E business and corporate spend are close to budget. c) The forecast remains in line with budget although there has been a
further adverse movement of £0.1m in the Commercial Division offset by savings in Corporate.
d) There is a recognition that there continues to be significant risk in the budget which means that it is critical that the Trust delivers the agreed actions in the Recovery Plan in order to achieve the required £2.0m surplus.
e) The cash position is currently favourable to plan due to the successful recovery of some long standing debts. Currently ahead of budget by primarily owing to the HART income, the decision to delay the disposal of Battle resulting in a £3.6m effect on the full year forecast and the disposal of Portsea. The resultant year end net cash position is a £2.0m reduction.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 13 of 20
Action Date
f) The cash savings forecast is continually being updated and is on track to meet the projected £6.4m and is ahead of budget overall for the month by £166k. In terms of the forecast, the over performance in the Clinical Support Desk and the overhead cost saving CIPs have helped offset some of the shortfalls in other areas.
g) Although Return on Assets is lower than in budget, overall the results are in line with Monitor requirements.
h) The current view is that the debtors provision of £394k remains appropriate however the debtors position would continue to be reviewed on a monthly basis by the Director of Finance and the Chairman of the Audit Committee.
The following comments and challenges were received in relation to the report:
11/107 a) In light of the wider economic climate and worsening financial position with many other NHS organisations it was considered inevitable that there would be an increased risk exposure in relation to the Trust’s debt position;
11/108 b) Referring to the reported delay in capital expenditure in relation to the modernisation changes to vehicles, clarification was sought as to whether this had been risk assessed and the associated consequences of this evaluated. In response, it was REPORTED that this was primarily a planning issue driven by the operational and fleet teams and that there were no apparent clinical risk issues as a consequence of the delay in expenditure in vehicle modernisation.
11/109 Following discussion it was RESOLVED that :
a) A more in depth discussion on the some of the points raised during the debate would take place in the confidential Part 2 session of the meeting; and
b) The month 5 Finance Report for the period ended 31 August 2011 be received and accordingly APPROVED.
FLEET AND EQUIPMENT STRATEGY
11/110 The Chairman welcomed Phil Pimlott, the Assistant Director of Operation Support Services to the meeting. The Chief Operating Officer introduced the paper and explained that purpose of the paper was to seek the Board’s approval of the proposed Fleet & Equipment Strategy for 2012-2017.
11/111 Mr Pimlott opened his presentation by informing members that the five-year strategy outlined future plans in line with the Trust’s vision, objectives and priorities in order to ensure that SCAS’s fleet and equipment meet the needs of delivering services to patients by ensuring it is fit for purpose, cost effective and fully maintained to high standards.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 14 of 20
Action Date
11/112 Members were asked to note the following points:
The Trust’s mixed fleet currently comprises approximately 880 vehicles and consists of emergency ambulances, rapid response cars and motorbikes as well the patient transport services and specialist vehicles;
The strategy sets out a coordinated, integrated and comprehensively managed approach to fleet and equipment procurement and maintenance, and is a major component to successful business management;
The strategy was built upon the pre-existing strategies (where available) from the former trusts and had been developed to demonstrate the ongoing commitment to maximise the fleet and equipment requirements in supporting the operational requirements of SCAS;
One of the consequences of the strategy was the closure of the Portsmouth workshop and the transfer of this operation into the new workshop based within the new ambulance resource centre at Nursling, Southampton;
The strategy acknowledges the continuing need for the Trust’s vehicles and equipment to be developed to meet the required future changes in the delivery of care and treatment to patients.
A benchmarking exercise would be undertaken against the fleets in other Trusts to identify reference costs.
Key Performance Indicators are considered to be critical to the vehicle replacement programme;
After the conclusion of the presentation, the following comments and challenges were received:
11/113 a) In response to the question whether the proposed strategy before the meeting was considered to be ‘fit for purpose’ or if it had been produced as a holding position, it was CONFIRMED that whilst the Trust’s Clinical Strategy was regarded as the main driver for the Fleet Strategy, both strategies were still very much evolving. It was therefore acknowledged that the Fleet and Equipment Strategy links and supports the Clinical Strategy and would be continually updated to respond and reflect the future changes and developments associated with the Clinical Strategy;
11/114 b) The Director of Patient Care recorded her support for the strategy noting that it represented a cohesive approach towards integrating fleet and equipment and clearly sets out how the Trust will manage key parts of the Trust’s services in order to provide improved patient care.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 15 of 20
Action Date
11/115 c) The importance of integrating SCAS’s strategy with the respective strategies of other ambulance services was emphasised;
11/116 d) The financial and cost reduction implications of implementing the strategy were considered to be key considerations and in response to a request for clarification as to where the required financial support was expected to come from in order to support the structure, it was REPORTED that this aspect was presently in the process of being evaluated by the finance team in conjunction with the fleet team.
11/117 e) Whilst work was currently being undertaken to produce a business case for the van conversions, some of required information was incomplete at this stage.
11/118 f) Recognising that that the Trust may be considered more expensive than other Trust’s reinforces that importance of benchmarking the Trust against ambulance services.
Following a discussion, it was RESOLVED that:
11/119 a) In recognition of the importance of the Fleet and Equipment Services Strategy as being instrumental to the improvement of patient care and to facilitate the Board’s future monitoring of the effectiveness of implementation of the strategy, the Board would be provided, in due course, with the following supplementary information:
IF 25/01/12
an Implementation Plan for the Fleet and Equipment Services Strategy as produced to the meeting;
details of the refurbishment programme key performance indicators (KPIs) including the associated target dates; and
details of SCAS’s vehicle downtimes in relation to other trusts.
11/120 b) Subject to (a) above, the Fleet and Equipment Services Strategy was accordingly APPROVED by the Board.
The Chairman thanked Mr Pimlott for his contribution to the discussion and
he left the meeting at 12.35.
IM&T STRATEGY REVIEW UPDATE
11/121 The Chairman welcomed Vince Weldon, the Associate Director of IM&T to the meeting. The Director of Finance introduced the paper and explained that purpose of the paper was provide a brief update on the main changes and actions that have taken place since the IM&T Strategy 2010-2012 was approved by the Board in June 2010.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 16 of 20
Action Date
11/122 The Associate Director of IM&T drew attention to some the key points contained in the paper, commenting that whilst there had been a number of important IT infrastructure and system developments over the course of the previous four years, the immediate challenge facing the Trust was to capitalise on the recent investment in IT infrastructure and “sweat the assets”.
11/123 By way of providing the required assurance to the Board, the following points
were NOTED:
a) A series of workshops together with a Board Seminar specially on this
topic were being arranged over the coming months to facilitate the future development of the strategy and ensure the necessary engagement with key stakeholders;
b) A detailed IM&T Strategy for the period 2012 to 2015 incorporating the NHS 111 development, Electronic Patient Reporting (ePRF) and improved interoperability between the Trust and provider/commissioner systems etc. would be presented to the Board for consideration and approval in March 2012;
c) The all the potential areas identified in the report for development during 2012 to 2015 have been funded.
11/124 The following comments and challenges were received:
a) The point was raised whether there had been adequate communication to staff concerning access to the Trust’s excellent inter-site telephony facility;
b) Following a request for clarification about the implications for the Trust
following the recent announcement about the proposed abolishment of ‘Connecting for Health’ it was REPORTED that as this was a national issue, urgent guidance was expected shortly from the DoH.
c) Clarification was sought as to whether in the light of limited capital resources there were any activities where either the organisation is heavily reliant on staff doing significant amounts of routine manual data entry or data collection where the introduction of an IT system might deliver improvements in both efficiency and the quality of patient care; or alternatively which have not been already identified as a potential area for development.
11/125 Following discussion it was RESOLVED that: a) Further input would be sought at both board and executive level
prior to the proposed IM&T Strategy being submitted for consideration and approval by the Board in March 2012;
CP 29/02/12
South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 17 of 20
Action Date
b) the Associate Director of IM&T would arrange for staff to be provided with appropriate guidance on the availability of benefits of the Trust’s telephony facility; and
VW 09/12/11
c) The update as provided at the meeting concerning the progress in developing the IM&T Strategy 2012-2015 be received and accordingly NOTED.
The Chairman thanked Mr Weldon for his contribution to the discussion and he left the meeting at 12.50.
EQUALITY AND DIVERSITY QUARTERLY REPORT
11/126 The Chairman welcomed Sharon Walters, Director of HR to the meeting. The Director of HR introduced the report relating to the second quarter and informed members that the purpose of the report was to provide employment statistics to facilitate the Board’s understanding of organisation’s quality and diversity issues Members were ASSURED that whilst there was very little variation in the data contained report compared to the previous quarter, much of this data would be invaluable for benchmarking purposes and to monitor changes to SCAS’s workforce.
11/127 The Director of HR explained that key to improving the quality of this workforce data was by getting improved disclosure by staff in relation to equality and diversity related matters. It was NOTED that to facilitate this process, an Equality and Diversity for Managers training initiative had been introduced at the end of August and further training sessions were being arranged for October 2011.
11/128 Referring to the Equality Act legislation, members were reminded that whilst 90% of the Act came into force on 1 October 2010, on 6 September 2011, Parliament formally approved the Public Sector Equality Duty (PSED), which introduced two specific duties on all NHS organisations:
to publish information to demonstrate compliance with the PSED at least annually starting from 31 January 2012; and
to prepare and publish equality objectives at least every four years starting from 6 April 2012.
11/129 The Director of HR ASSURED the Board that whilst these obligations technically come into effect in 2012, she considered that the Trust was in practice already largely compliant with the new requirements.
11/130 The following comments and challenges were received:
a) A request for further clarification was made around the Trust’s proposed disclosure arrangements, and more specifically in relation to the Trust’s intentions to benchmark with other ambulance trusts for staff in full and part time employment;

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 18 of 20
Action Date
b) In response to the point raised whether the reported increase in staff between 20 and 30 years predominantly related to patient facing staff or across the whole organisation, it was CONFIRMED that the increase reflected the appointment of newly graduated paramedics.
c) Noting that the recruitment profile, appeared to suggest that the number of ethnic minorities appointed was a lower percentage than the equivalent number of applications, a comment was made that the Board should obtain further ASSURANCE that the current position was not as a result of inherent discrimination in the Trust’s recruitment practices or procedures. It was generally acknowledged by members that the immediate challenge for the organisation was in encouraging more suitably qualified individuals from the ethnic minorities to submit applications.
11/131 Following discussion it was RESOLVED that:
a) In order to provide the Board with the necessary assurance concerning the recruitment of ethnic minorities, the next quarterly report would include some more in depth qualitative analyisis concerning applicants; and
WH SW
29/02/12
b) The Equality and Diversity Quarterly Report for the period ending 30 September 2011 be received and accordingly NOTED.
The Chairman thanked Mrs Walters for her contribution to the discussion and she left the meeting at 13.00.
THE BRIBERY ACT 2010 - TRUST STATEMENT
11/132 The Chief Executive REPORTED that as a result of the Bribery Act 2010 (the Act) which came into force on July 2011, one of the key requirements under the legislation was publication of a clear statement of board level commitment to achieving compliance with the Act.
11/133 He explained that that the purpose of the paper was to: propose a clear unequivocal statement as outlined in Appendix A, in
respect of the position of the organisation regarding bribery and the Board’s commitment to the principles of the Act ;and
to provide board members with the necessary assurance that appropriate
measures are currently being undertaken by the Trust to address the requirements of the Act.
11/134 It was NOTED the ongoing evidence of board support was considered to be fundamental to the protection provisions under the Act and that a method of recording such evidence and reporting lines to the Board were in the process of being developed by the Corporate Secretary.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 19 of 20
Action Date
11/135 It was CONFIRMED that whilst the Trust already had a series of policies and procedures in place to mitigate against bribery risks, additional work was currently underway to review and strengthen existing arrangements and introduce new measures as necessary. In this connection, it was NOTED the Corporate Secretary in conjunction with the Trust Local Counter Fraud Specialist (LCFS) were in the process developing an Anti Bribery Policy which would be submitted in due course for Board approval.
11/136 Following discussion, it was RESOLVED that : a) The Board of Directors of South Central Ambulance Service NHS
Trust CONFIRMS that it fully ENDORSES the recommendation that the Trust adopts a zero tolerance approach towards any act of bribery within the organisation and by any others connected with it, whether staff, volunteers, or external companies;
b) The proposed Statement as outlined in Appendix A of the report be APPROVED;
c) The Corporate Secretary be AUTHORISED to make the necessary arrangements with the Communications Team for the approved Statement to be published on the Trust’s corporate website; and
JH 30/11/11
d) The update report on the Trust’s obligations in relation to Bribery Act 2010, be received and accordingly NOTED.
BOARD SUB COMMITTEE MINUTES AND CHAIR REPORTS
Audit Committee Meeting: 5 September 2011 11/137 Eddie Weiss presented the minutes of the Audit Committee meeting held on
5 September 2011 and referring specifically to the Chair’s Exception Report, he drew to the Board’s attention the key areas of discussion and decisions made the meeting.
It was RESOLVED that:
The Minutes and Chair’s Exception Report relating to the Audit Committee held on 5 September 2011 be received and accordingly NOTED by the Board.
Quality and Safety Committee Meeting: 4 August 2011 11/138 Keith Nuttall presented the minutes of the Quality and Safety Committee
meeting held on 4 August 2011 and referring specifically to the Chair’s Exception Report, he drew to the Board’s attention the key areas of discussion and decisions made the meeting.

South Central Ambulance Service NHS Trust (‘SCAS’ or ‘the Board’)
These minutes may be made available to the public and persons outside South Central Ambulance Service NHS Trust in compliance with the Freedom of Information Act 2000.
Trust Board Meeting (Part 1) : 28 Sept 11 Unapproved Draft Minutes Page 20 of 20
Action Date
It was NOTED that following the approved amendments to the Committee’s Terms of Reference in July 2011, the Chief Executive and Director of Patient Care were presently reviewing the accountability and reporting arrangements of a number of the sub committees and working groups at executive level with a view to improving the quality of the assurance that they were now required to provide to the Quality and Safety Committee.
It was RESOLVED that:
The Minutes and Chair’s Exception Report relating to the Quality and Safety held on 4 August 2011 be received and accordingly NOTED by the Board.
Charitable Trust Funds Committee Meeting: 22 September 2011 11/139 Claire Carless gave a verbal update on the deliberations of the Charitable
Trust Funds Committee Meeting held on 22 September 2011.
11/140 Following a challenge as to whether the Trust considered itself sufficiently proactive in terms of fundraising, it was generally acknowledged that this matter required further consideration.
It was RESOLVED that:
a) The topic of charitable fundraising would be included on the Board Forward Planner as a seminar discussion; and
CC CP
29/02/12
b) The Chair’s verbal report relating to the Charitable Trust Funds Committee Meeting held on 22 September 2011 be received and accordingly NOTED by the Board.
ANY OTHER BUSINESS
11/141 It was CONFIRMED that there were no further matters of business for discussion and the meeting closed at 13.15.
Signed by the Chair as a true record of the meeting, subject to any
amendments duly minuted. ……………………… ……………………….. Trevor Jones Date Chairman

South Central Ambulance Service NHS Trust
Enclosure B: (Agenda Item: 5)
Trust Board Meeting – 1 December 2011
MATTERS ARISING: 28 September 2011
KEY: Completion Overdue Completion Scheduled for Current Board Meeting Completion date beyond current Meeting Completed
Page 1 of 6
No. Minute ref.
Agenda Item Action Exec Resp
Date Raised
Target Due Date
Comments/Outcome
Actions arising from 30 March 2011 1. 4 CEO Update Report CEO to provide Board members with further
regarding appointments to PCT Clusters WH 30.03.11 31.08.11 The required formal
nominations by PCT Clusters were received by the Trust during Nov 11 and the relevant Partner Governors have now been appointed to the Shadow Council of Governors. CLOSED ( Nov 11)
Actions arising from 29 June 2011 2. Finance Report The Director of Finance to begin a producing a
mock-up quarterly Monitor reports.
CP 29.06.11 25.01.12 WORK IN PROGRESS
Actions arising from 27 July 2011 3. 9 The Estates Strategy to be submitted for Board
approval in Feb 2012.
CP 27.07.11 29.02.12 WORK IN PROGRESS
4. 11 The Board to be kept regularly updated during implementation of the agreed Ops/Clinical structure.
IF 27.07.11 Ongoing Standing agenda item at Executive Management Committee. Update on implementation also included in the monthly Chief Executive report. ONGOING.

South Central Ambulance Service NHS Trust
Enclosure B: (Agenda Item: 5)
Trust Board Meeting – 1 December 2011
MATTERS ARISING: 28 September 2011
KEY: Completion Overdue Completion Scheduled for Current Board Meeting Completion date beyond current Meeting Completed
Page 2 of 6
No. Minute ref.
Agenda Item Action Exec Resp
Date Raised
Target Due Date
Comments/Outcome
5. 13 Foundation Trust Progress Report
Nominations for PCT Cluster Governors The PCT Clusters to be followed up for the names their Governor nominee
JD 27.07.11 31.08.11 The required formal nominations by PCT Clusters were received by the Trust during Nov 11 and the relevant Partner Governors have now been appointed to the Shadow Council of Governors. CLOSED (Nov 11)
6. 17 Governance Framework Charter of Expectations (Appendix 2) The Charter of Expectations to be circulated to board members for comments and submitted to the Sept board meeting for approval.
JD 27.07.11 25.01.12 At the Sept board it was confirmed that this would be submitted to the Nov board. Owing to agenda timing constraints it has been subsequently agreed that this matter would be deferred to the Jan 12 board meeting. WORK IN PROGRESS
7. 29 Procurement Update Final Fees The issue concerning the final fees to be discussed by the Procurement Sub Group and brought t o a future Board meeting for ratification.
CP
27.07.11
25.01.12
Confirmed at the Sept meeting that owing to a separate problem with the Integrated Supply Chain, the final fees were still being negotiated.

South Central Ambulance Service NHS Trust
Enclosure B: (Agenda Item: 5)
Trust Board Meeting – 1 December 2011
MATTERS ARISING: 28 September 2011
KEY: Completion Overdue Completion Scheduled for Current Board Meeting Completion date beyond current Meeting Completed
Page 3 of 6
No. Minute ref.
Agenda Item Action Exec Resp
Date Raised
Target Due Date
Comments/Outcome
As the Trust is no longer working with Mid Assets, the action originally raised relating to the fee issue no longer applies. CLOSED (Nov 11)
Actions arising from 28 September 2011 8. 11/61 Quality and Patient
Safety Report A seminar session focussing on how the Trust deals with three typical complaints case studies to be scheduled in the Board Development Programme.
FT /JVD 28/09/11 29/02/12 WORK IN PROGRESS
9. 11/65 Foundation Trust Status Assurance Report
A briefing note to be circulated to board members on the proposed plans for the Board to engage with the Council of Governors.
DB 28/09/11 31/11/11 Briefing document circulated. Circulated to board members. CLOSED (Nov 11)
10. 11/72 FT Membership and Governors Election Update
The details of the nominations for the Council of Governors to be shared with Board members.
DB 28/09/11 14/10/11 Details of the election nominations circulated to board members. CLOSED (Nov 11)
11. 11/104 (a) Integrated Performance Report
A Board seminar session on baseline targets and reporting measures to be scheduled;
FT/IF 28/09/11 26/10/11 A board seminar session was held on 26 Oct. CLOSED (Nov 11)
12. 11/104 (b) The Quality and Safety Committee would update the Board in due course in relation to the reported public liability claim.
KN/FT 28/09/11 25/01/12 WORK IN PROGRESS

South Central Ambulance Service NHS Trust
Enclosure B: (Agenda Item: 5)
Trust Board Meeting – 1 December 2011
MATTERS ARISING: 28 September 2011
KEY: Completion Overdue Completion Scheduled for Current Board Meeting Completion date beyond current Meeting Completed
Page 4 of 6
No. Minute ref.
Agenda Item Action Exec Resp
Date Raised
Target Due Date
Comments/Outcome
13. 11/104 (c) In relation to the Cost Improvement work stream, an update would be provided to the Board on the Corporate Review plans.
CP 28/09/11 21/12/11 WORK IN PROGRESS
14. 11/104 (d) The Key Milestones table should be produced in a larger font and preferably black type for future reports.
CP 28/09/11 0/12/11 The suggested improvements have been incorporated in the all future reports to the Board. COMPLETED (Nov 11)
15. 11/119 (a) Fleet and Equipment Strategy
a) In recognition of the importance of the Fleet and Equipment Services Strategy as being instrumental to the improvement of patient care and to facilitate the Board’s future monitoring of the effectiveness of implementation of the strategy, the Board would be provided, in due course, with the following supplementary information:
an Implementation Plan for the
Fleet and Equipment Services Strategy as produced to the meeting;
details of the refurbishment
programme key performance indicators (KPIs) including the associated target dates; and
details of SCAS’s vehicle downtimes in relation to other
IF 28/09/11 23/01/12 WORK IN PROGRESS

South Central Ambulance Service NHS Trust
Enclosure B: (Agenda Item: 5)
Trust Board Meeting – 1 December 2011
MATTERS ARISING: 28 September 2011
KEY: Completion Overdue Completion Scheduled for Current Board Meeting Completion date beyond current Meeting Completed
Page 5 of 6
No. Minute ref.
Agenda Item Action Exec Resp
Date Raised
Target Due Date
Comments/Outcome
trusts.
16. 11/125 (a) IM&T Strategy Further input would be sought at both board and executive level prior to the proposed IM&T Strategy being submitted for consideration and approval by the Board in March 2012;
CP 28/09/11 29/02/12 This topic has been scheduled for further discussion at the board seminar on 29/02/12 WORK IN PROGRESS.
17. 11/125 (b) Staff to be provided with appropriate guidance on the availability of benefits of the Trust’s telephony facility.
CP/VW 2809/11 09/12/11 WORK IN PROGRESS
18. 11/131 (a) Equality & Diversity Quarterly Report
In order to provide the Board with the necessary assurance concerning the recruitment of ethnic minorities, the next quarterly report would include some more in depth qualitative analyisis concerning applicants; and
WH SW 28/09/11 29/02/12 WORK IN PROGRESS
19. 11/136 © Bribery Act 2010 The Corporate Secretary to make the necessary arrangements with the Communications Team for the approved Statement to be published on the Trust’s corporate website.
28/09/11 30/11/11 JH Approved statement now published on the website. COMPLETED.
Charitable Funds Committee Minutes: 22 Sept 11
Charitable fundraising to be included on the Board Forward Planner as a seminar discussion.
Cc/CP 28/09/11 29/02/1S2 WORK IN PROGRESS

South Central Ambulance Service NHS Trust
Enclosure B: (Agenda Item: 5)
Trust Board Meeting – 1 December 2011
MATTERS ARISING: 28 September 2011
KEY: Completion Overdue Completion Scheduled for Current Board Meeting Completion date beyond current Meeting Completed
Page 6 of 6
Key: AMB Alastair Mitchell-Baker CC Claire Carless CH Colin Hazell CP Charles Porter DB Duncan Burke EW Eddie Weiss FT Fizz Thompson IF Ian Ferguson JB John Black JD John Divall JVD Julie Dawes KN Keith Nuttall PC Paul Clarke TJ Trevor Jones WH Will Hancock

1
Enclosure: c (Agenda Item: 7)
Board Report 1st December 2011
Title Chief Executive’s Report
Lead Director Will Hancock, Chief Executive
Report Author Will Hancock, Chief Executive
Purpose of the report
The purpose of the Chief Executive’s Report is to update the Board on selected activities undertaken since the last meeting and draw the Board’s attention to other issues of significance. Where relevant, the report also contains a briefing on issues of a national and SCAS perspective. This month’s report contains updates on the following areas:
Annual Plan Business Development Strategy Review NHS Developments Care Quality Commission Stakeholder and Partnership Working Foundation Trust Monitor
Recommendation (eg. Note, approve, endorse)
The Board is asked to receive and NOTE the Chief Executive’s Report as an information item.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure

2
Links to the CQC Essential Standards regulations
Regulation 9: Care and welfare of service users
Details of additional risks associated with this paper:
None identified
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
Patient rights: Access to health services Patient rights: Quality of care and environment
Financial implications/impact None identified
Legal implications/impact None identified
Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
Communication with staff and stakeholders remains a priority for the Trust.
Other
Committees/groups where this item has been presented before
N/A
Other options available and their pros and cons
N/A
Progress monitoring and review Performance is reported and monitored through the Executive Management Committee and reported monthly to the Board.
Background papers

3
CHIEF EXECUTIVE’S REPORT
Annual Plan SCAS’ service performance has been strong over the first seven months; the pace of more strategic development has also increased and major changes in the NHS landscape continue. In addition to managing the day to day service, the Executive Team has been focussed on the Operational and Clinical review process, delivering the commitments in our contracts and dealing with the challenging financial situation. We have also been addressing further organisational development through our ‘culture’ programme and progressing with new business opportunities. In terms of the Clinical and Operational structure review the first launch event has been held. It was well received by around 50 newly appointed team leaders and clinical mentors. We are reviewing the feedback and will make some adjustments for the remaining 3 events. The development prospectuses went down well and managers are looking forward to taking part in the development programme. The Trust’s Emergency Preparedness team have been updating plans for increased resilience over the coming months to address the potential challenges of the Winter weather, Flu and Industrial action. Plans for the Winter and Flu are in place and have been reviewed and approved by the Executive Team. Board members can review the plans on request. The plan for industrial action is in draft form and will evolve through discussion with the Unions now that the ballot results are known to be in favour of industrial action. As it currently stands there is very real risk of ambulance services across England being adversely affected by industrial action on the 30th of November and beyond. The Trust has experienced an increase in 999 workload during October and delays in handover at hospital are increasing. We have taken a proactive approach at a local level to get agreements in place on protocols with each hospital. We have also been raising awareness at the highest levels in acute trusts and with Commissioners and the SHA. It is particularly critical this year with the changes we are making to operational management structures reducing the availability of SCAS supervisors to manage patients in queues at hospital.
Our approach to using the Clinical Support Desk (CSD) to personalise care to individual patients was endorsed as good practice by the national ops and clinical directors groups. Others are now following us and we have been invited by the Association of Ambulance Chief Executives (AACE) to submit a paper outlining the principles and governance of the CSD.
4
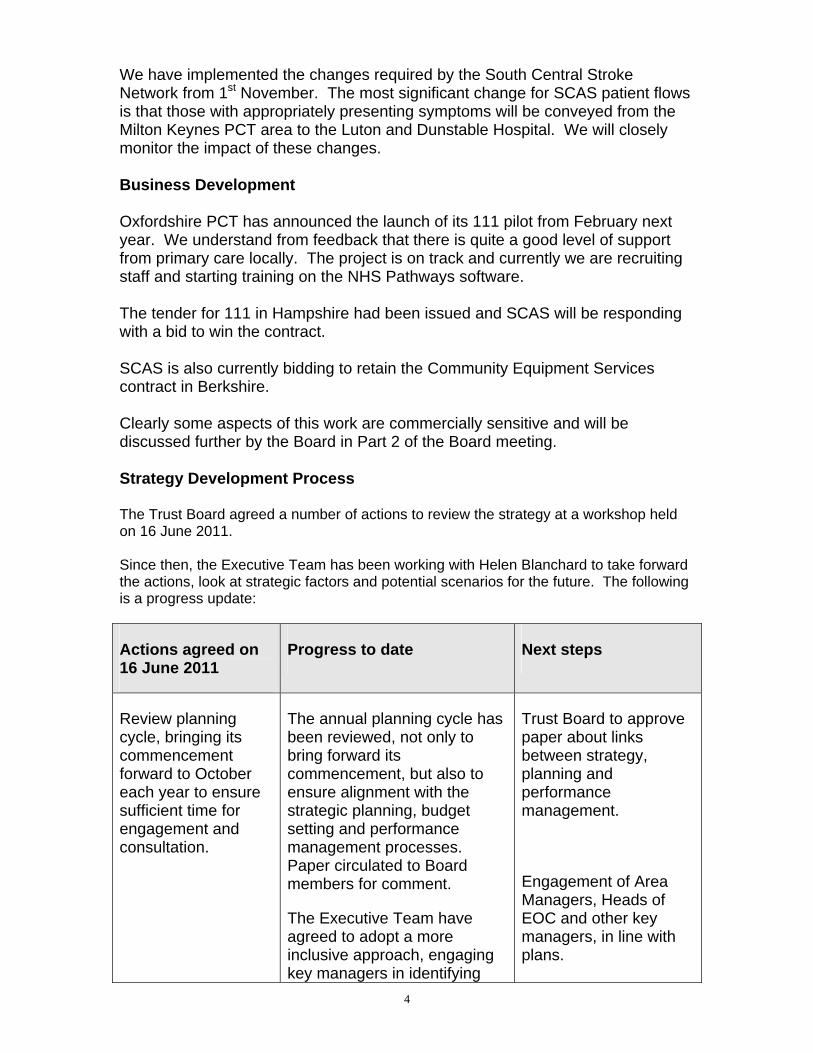
We have implemented the changes required by the South Central Stroke Network from 1st November. The most significant change for SCAS patient flows is that those with appropriately presenting symptoms will be conveyed from the Milton Keynes PCT area to the Luton and Dunstable Hospital. We will closely monitor the impact of these changes. Business Development Oxfordshire PCT has announced the launch of its 111 pilot from February next year. We understand from feedback that there is quite a good level of support from primary care locally. The project is on track and currently we are recruiting staff and starting training on the NHS Pathways software. The tender for 111 in Hampshire had been issued and SCAS will be responding with a bid to win the contract. SCAS is also currently bidding to retain the Community Equipment Services contract in Berkshire. Clearly some aspects of this work are commercially sensitive and will be discussed further by the Board in Part 2 of the Board meeting. Strategy Development Process The Trust Board agreed a number of actions to review the strategy at a workshop held on 16 June 2011. Since then, the Executive Team has been working with Helen Blanchard to take forward the actions, look at strategic factors and potential scenarios for the future. The following is a progress update:
Actions agreed on 16 June 2011
Progress to date Next steps
Review planning cycle, bringing its commencement forward to October each year to ensure sufficient time for engagement and consultation.
The annual planning cycle has been reviewed, not only to bring forward its commencement, but also to ensure alignment with the strategic planning, budget setting and performance management processes. Paper circulated to Board members for comment.
The Executive Team have agreed to adopt a more inclusive approach, engaging key managers in identifying
Trust Board to approve paper about links between strategy, planning and performance management.
Engagement of Area Managers, Heads of EOC and other key managers, in line with plans.

5
Actions agreed on 16 June 2011
Progress to date Next steps
priorities and plans (including highlighting strategic issues for local stakeholders, suggested areas for CQUIN payments, and proposed levers to improve costs or performance).
Discussions commenced with Area Directors and Senior Managers about the business planning process and priorities for 2012/13.
Engagement of shadow Council of Governors
Review SWOT and PESTLE analysis by Executive Team
Share with NEDS in October
Key personnel engaged in SWOT and PESTLE analysis:
Workshop held with Executive Team on 2 August and 11 October
Session held with Senior Leadership Team on 16 August
Feedback sought from commissioners and non-Executive Director
Feedback to stakeholders who have contributed to the strategic review process
Factors to consider in our strategy have been identified by the groups above, and their potential impact and likelihood assessed
Research undertaken of health specific ‘futures’ work, to gain insight about other potential factors from external perspective
Top 3 uncertainties identified in terms of potential impact
Share with non-Executive Directors in December 2011

6
Actions agreed on 16 June 2011
Progress to date Next steps
Undertake scenario planning exercise to test SCAS plans
June to October 2011
2 potential scenarios generated from factors and uncertainties identified
TOWS matrix is being used to match the organisation’s current strengths to the threats and opportunities presented in these hypothetical scenarios, and to create new strategic options to address any weaknesses (in progress)
Complete TOWS (strategy tool) analysis
Present scenario thinking and strategic options to the Board in December

7
Actions agreed Next steps
Undertake a scenario planning exercise to test SCAS plans (continued)
Evaluate the strategic options:
Are they aligned with our vision?
How does our strategy play in each scenario?
Assess potential stakeholder reactions?
Test the options (to destruction)
Establish responsibilities and resources
Identify actions required to prepare for strategic options
Agree priorities
Agree responsibilities and resources to take forward plans
Develop tactical plans Develop outline plans in response to threats and opportunities
Engage key managers and stakeholders in preparing tactical plans
Trust Board to approve tactical plans
Update the Integrated Business Plan
Incorporate plans into SCAS’s programme of change
Communicate with staff and stakeholders as appropriate for nature of any changes planned
Implement plans as agreed
NHS Developments The 2012/13 Operating Plan will be published on the 24th November. Guidance contained within the Plan will set out the critically important financial and operational framework for SCAS next year. We will have an opportunity as a Board to review the key elements of the Operating Plan and the impact on our planning assumptions at the Board meeting.
8
Care Quality Commission (CQC) The Trust received a responsive visit from the CQC on 26th October. Oxford City and Reading stations were inspected. We are awaiting formal feedback from the CQC on the outcome and hope to give the Board a verbal update at the meeting. A further update is provided in the Quality and Safety Report. Stakeholder and Partnership Working We have hosted a number of visits to the Trust's HQ at Bicester, over the last month. These have included Iain Stewart MP, Milton Keynes South and James Naylor, High Sheriff of Buckinghamshire. Both visits gave our guests the chance to visit our Emergency Operations Centre (EOC), meet staff and look round vehicles. Both guests appreciated the chance to learn more about the Trust and find out how we are delivering our service. As part of our programme of engagement with our local Health and Overview Scrutiny Committees (HOSCs), we have visited Bracknell Forest Council, Portsmouth and Buckinghamshire HOSCs and updated members on the new Ambulance Quality Indicators. HOSCs are requesting follow up visits in the Spring to update on performance against the new indicators. We have been identifying opportunities for them to help us through supporting our education and awareness work and supporting the development of co and community responder schemes. Foundation Trust An update will be provided at the meeting under the appropriate agenda item. Monitor Monitor’s Chief Economist Sonia Brown presented at the Ambulance Service Networks Annual Conference on the 8th of November. Sonia spoke on ‘How competition will work in the new market’ outlining the policy perspective and presenting Monitor’s role as regulator in the new market and from the perspective of the Health & Social Care Bill. I chaired the session and Eddie Weiss and myself were able to discuss matters further with Sonia after her presentation. Recommendation The Board is asked to receive and NOTE the Chief Executive’s Report as an information item. Will Hancock 15th November 2011
Enclosure: D (Agenda Item: 8)
Board Report
1st December 2011
Title Quality and Patient Safety Report (Month7)
Lead Director Fizz Thompson, Director of Patient Care
Report Author Fizz Thompson, Director of Patient Care
Purpose of the report To update and assure the Trust Board on the quality and patient safety work stream areas.
Recommendation (eg. Note, approve, endorse)
The Trust Board is asked to receive and NOTE the report.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
Links to all CQC registration and Essential Standards
Details of additional risks associated with this paper:
All clinical risks are detailed in the Trust risk register that link to the quality work streams
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
All areas of Patient Rights
Financial implications/impact None
Legal implications/impact
Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
Quality and Patient Safety work streams are shared with commissioners and stakeholders through regular updates and meetings and performance shared through the Integrated Performance Report
1

Other
Committees/groups where this item has been presented before
Progress of the Quality and Patient Safety work streams is monitored through the Quality and Safety Committee, the Executive Team Committee and the two sub groups, the Clinical Review Group and the Operational Health, Safety and Risk Group
Other options available and their pros and cons
Not applicable
Progress monitoring and review An update will be presented to the Public Trust Board meetings. Further monitoring of the work streams will be undertaken by the Quality and Safety Committee and the Executive Team Committee
Background papers
QUALITY UPDATE
2

Quality and Patient Safety continue to drive forward the Trust’s agenda as we endeavour to deliver the components within our strategy, High Quality Care. This update provides information on progress and, continuation of the work to maintain clinical excellence and high standards of care to the public we serve. Further information and demonstration of delivery of performance can be found in the Integrated Performance Report. Ongoing work will continue to address the self assessment of the Trust position with Quality Governance through the working groups monitored through the Quality and Safety Committee and also with reporting of the improvement actions detailed in the Quality Accounts. All quality measures and metrics including the Clinical Performance Indicators and new clinical outcome measures are now reported through the new Integrated Performance Report. Exceptions to report are outlined below: 1. Drop in performance of the Return of Spontaneous Circulation (ROSC) and witnessed cardiac
arrest indicators. An investigation is underway to determine the reasons for this and understand the root causes and benchmark this position against other ambulance services. This will be monitored through the Clinical Review Group and the Quality and Safety Committee to review the actions and improvements.
2. Performance in the STEMI care bundle has reduced specifically in the area of analgesia (pain
relief). An action plan has been developed to improve the giving and documentation of analgesia to this group of patients. One key area being addressed is a reminder in the Continuous Professional Development Course that is ongoing at present.
3. Performance in care to patients with stroke symptoms (FAST positive patients call to leave
scene target 39 mins and to stroke centre in 60 mins) has dropped in October. More work is being undertaken to understand the reporting of this indicator and a plan will be developed to improve results.
4. There is reduction in the number of complaints reported for September. However, the YTD
total remains above last year’s reported figures. This continues to be monitored through weekly updates and at the Patient Experience Review Group.
5. Non-conveyance – reduction in number of patients that are assessed and offered a different
referral pathway to admission to an Emergency Department. An investigation is ongoing to review the components of this key area. A recovery plan to improve the use of other pathways is now in place and is being monitored through the Executive Team. Non-conveyance was a key focus for the Board seminar in October. Patient safety issues were reviewed in detail following the discussion at the Quality and Safety Committee meeting. A presentation provided the Board with the contractual position, current performance and the areas of assurance around patient safety and how this is monitored. Actions to provide further assurance and improvements were noted by the Board and these will be reviewed by the Executive Team and the Quality and Safety Committee.
6. The number of controlled drugs incidents was higher in September due to accounting issues
rather than unresolved losses. A loss of codeine tablets has been reported from the South West area of Hampshire; this is currently being investigated by the Medicines Management Advisor and has been reported to the Local Intelligence Network. Actions are in place to avoid any further occurrences of this type.
3

SAFETY 1. Introduction The table below shows national benchmarking data for the 11 NHS ambulance trusts in England during 2010/11. The data was submitted by the trusts and obtained from the Quality Governance and Risk Group (QGARD), the NPSA website and the NHS Protect Violence against Staff Statistics. 2. Comparable Data Direct comparison of data between trusts should take account of staff numbers as this will have an impact on the number of incidents reported as a whole. SCAS is ranked 9th with regards to the number of staff employed, as is shown in the table below.
RIDDOR Assaults Trust
No of Staff
SUI NPSA No Reported
Within 10 days
No Reported
Sanctions
NWAS 5381 25 801 226 86 198 68 LAS 4946 NK 393 101 NK 449 93 YAS 4500 19 576 87 42 48 21
WMAS 4252 27 434 153 33 117 30 E of E 3936 27 336 121 NK 136 19 EMAS 3400 70 394 139 44 52 51
SECAS 3065 22 170 103 27 79 23 SWAS 2439 NK 683 133 104 71 4 SCAS 2370 20 148 112 85 62 14 NEAS 2216 NK 31 96 42 40 22 GWAS 1864 22 105 41 41 33 5
Average 3488 29 370 119 56 117 32 3. SUI Reports The Trust registered 20 Serious Untoward Incidents. Although this figure is below the national average of 29, it is consistent with similar sized trusts. Missing data from 3 trusts and a high submission by EMAS will have affected this average. 4. NPSA The Trust submitted 148 NPSA reports. This figure is considerably below the national average of 370 and what could be expected. This shortfall is attributed to poor reporting, an issue which has been addressed by the Risk Department and is now showing considerable improvement. 5. Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) The Trust submitted 112 RIDDOR reports to the HSE. This figure is close to the national average of 119 and consistent with similar sized trusts. A total of 85 reports were submitted within the mandatory 10 days. This is well above the national average of 56 and exceeds expectations. 6. Assaults The Trust submitted 62 reports of physical assault against staff. Although this figure is below the national average of 117, it is consistent with similar sized trusts. There were 14 sanctions applied against the perpetrators. This is below the national average of 32 and what could be expected. The Trust has appointed a full time Local Security Management Service (LSMS) Officer to address this and other security related issues.
4

CARE QUALITY COMMISSION (CQC) The Trust is continuing to maintain a working relationship with the CQC Local Assessment Team. The action plan on the Improvement Notices for outcomes 18 and 20 around incident reporting are being implemented and reporting is monitored through the Integrated Performance Report. Further evidence has been submitted to the CQC on the sustained delivery of timely reporting. The CQC undertook a responsive review on 26 Octoberth of Regulation 16 Outcome 11 Safety, Availability and Suitability of Equipment and Regulation 10 Assessing and monitoring the quality of service provision. Evidence in the form of Provide Compliance Assessment with accompanying information was supplied to support outcomes for both areas. The review was triggered by a letter of complaint regarding a lack of equipment that was received by the Trust and also sent to the CQC. The report is currently awaited. The CQC Quality and Risk profile (QRP) is a tool which gathers a wide range of information about providers and uses this to assess the risk of non-compliance with the Essential Standards of Quality and Safety. Information in the profile is updated monthly. An outline is provided below of our position: The risk level has changed in 2 outcome areas: Outcome 10 (Regulation 15) Safety and suitability of premises: The amount of information available has increased to produce a risk rating of High Neutral. Outcome 14 (Regulation 23) Supporting staff: The amount of information available has increased by 1 item to produce a risk rating of High Neutral. There is insufficient or no data to make a judgement on the risk level in 6 of the outcome areas. The CQC did not publish a QRP in September.
Outcome/Regulation August 2011
Risk level
October 2001
Risk level
Comments
Outcome 1 (R 17) Respecting and involving people who use services
Low Neutral
Low Neutral
No change
Outcome 2 (R18) Consent to care and treatment
No information
No information
No change
Outcome 4 (R9) Care and welfare of people who use service
Low Green
Low Green
No change
Outcome 5 (R14) Meeting nutritional needs
No information
No information
No change
Outcome 6 (R24) Cooperating with other providers
Insufficient data
Insufficient data
No change
Outcome 7 (R11) Safeguarding people who use services from abuse
Insufficient data
Insufficient data
No change
Outcome 8 (R12) Cleanliness and infection control
Insufficient data
Insufficient data
Outcome 9 (R15) Management of medicines
High neutral
High Neutral
Red rating in the detail of the profile, as we have not submitted an annual security management report. Also red rating regarding attendance at regional Counter Fraud and Security Management meetings. Our security management report was submitted, but after the deadline for inclusion in this data set.
Outcome 10 (R15) Safety and suitability of premises
Insufficient data Low Neutral
Information from the annual estates return has been added
5

Outcome 11 (R16) Safety, availability and suitability of equipment
High neutral
High Neutral
Information from NHS Protect. Red rating as we have not submitted an annual security management report. Also red rating regarding attendance at regional Counter Fraud and Security Management meetings. Our annual security management report was submitted after the deadline for inclusion .for inclusion in this data set
Outcome 12 (R21) Requirements relating to workers
Low neutral
Low neutral
No change
Outcome 13 (R22) Staffing
High Amber
High Amber
No change
Outcome 14 (23) Supporting staff
Insufficient data High neutral One additional item has been added to this area and is defined as a comment during a compliance review.
Outcome 16 (R10) Assessing and monitoring the quality of service provision
High Green
High Green
No change
Outcome 17 (R19) Complaints
Low Neutral
Low Neutral No change
Outcome 21 (R20) Records
Insufficient data
Insufficient data
No change
SERIOUS UNTOWARD INCIDENTS The Trust registered 20 Serious Untoward Incidents (SUI). Although this figure is below the national average of 29, it is consistent with similar sized trusts. Missing data from 3 trusts and a high submission by EMAS will have affected this average. The following table provides the board with an update report on the SUI status and the follow up areas are noted. The Trust Board will take further assurance following a detailed discussion in part two of the Board meeting. Actions and learning are reviewed at each SUI Review group and are monitored through the Executive Team. A summary report of all actions and learning will be brought back to the Board in January 2012 and will be shared across the organisation. Incident Date and Reference Number
Nature of Incident
Location
Status
Follow up areas
28/12/10 2011/559
Clinical care Non conveyance Joint incident with Out of Hours (OOH)
Oxford Root Cause Analysis (RCA) completed Reviewed May 11 Ongoing
Outcomes reviewed. Work with OOH service. Ongoing actions with family and OOH. Actions put in place from learning.
11/6/2011 2011/10784
Clinical care Failure of clinical equipment
SW Hampshire RCA completed. . Reviewed Aug 11 Closed
Outcomes reviewed. Actions put in place from learning.
2/7/11 2011/12845
Road Traffic Collision (RTC) – co responder with member of public
SW Hampshire RCA ongoing jointly with fire and police.
Police investigation pending
6

Incident Date and Reference Number
Nature of Incident
Location
Status Follow up areas
car Due to be reviewed Dec 11. Ongoing
2/8/11 2011/14704
Failure of tail lift with critically ill patient
Buckinghamshire RCA completed. Reviewed Nov 11. Ongoing
Outcomes reviewed. Actions put in place from learning.
7/8/11 2011/14887
Failure of tail lift with and inability to open back doors of ambulance with critically ill patient
North Hampshire RCA completed Reviewed Nov 11 Ongoing
Outcomes reviewed Actions put in place from learning
2/9/11 2011/16657
Clinical care Failure to adhere to Trust protocols
Oxford RCA completed Reviewed Nov 11 Closed
Outcomes reviewed. Actions put in place from learning.
1/9/11 2011/16809
Clinical Care Failure clinical of equipment
Oxford RCA completed. Reviewed Nov 11 Closed
Outcomes reviewed. Actions put in place from learning.
23/9/11 2011/17989
Clinical Care Failure of back doors to open
Oxford
RCA ongoing. Due to be reviewed Dec 11 Ongoing
13/10/11 2011/19596
Failure of the Computer Aided despatch system
Trust wide RCA ongoing. Due to be reviewed Dec 11 Ongoing
13/11/11 2011/21788
RTC involving SCAS motorbike and cyclist
South East Hampshire
RCA ongoing Due to be reviewed Dec 11 Ongoing
7

8
CLINICAL EXCELLENCE Trauma Networks Work is continuing to prepare for the implementation of the new trauma networks in April 2012. The education programme has commenced and 470 staff have been trained since the beginning of October. The training is being evaluated well. We remain on track to go live in April 2012. Stroke and Transient Ischaemic Attack (TIA) Pathway The new TIA (mini-stroke) pathway is due to go live on 21st November 2011 across the South Central region. Staff have been trained to assess patients with TIA symptoms and send a faxed referral to the hospital clinics for a further urgent assessment. New forms have been provided for staff to document their assessment and patient leaflets have been produced by the South Central Stroke Network to be left with patients. Restructure of the Clinical Directorate Progress is being made with the restructure changes within the directorate. Slotting in of staff has been undertaken. All appointments have now been made and the new Assistant Director of Quality has been appointed and will start from 1 February 2012. All managers are attending the launch events and will be taking part in the planned leadership training. PATIENT EXPERIENCE AND SATISFACTION The Patients Association has recently published a report, ‘We’ve been listening have you been learning’ that provides 16 patient stories that highlight accounts of unsatisfactory care. The report is a follow on to an earlier version, ‘Listen to Patients, speak up for change’ which brought about the CQC inspections of acute trusts to review standards of dignity. The report can be found at http://patients-association.com The third patient story is told by a patient’s daughter who relates the care given to her father who was very unwell with cancer of the pancreas. She describes her extreme frustration about trying to make health care professionals aware of how poorly her father was and finally someone at the hospital said he should attend the Accident and Emergency Department. A SCAS ambulance crew were called to undertake the transport. The following is provided from the report that outlines the care that our staff provided for her father: ‘The ambulance crew that took him there were absolutely superb. They realised immediately how poorly he was, helped him up and down the stairs to the toilet, and helped him walk to the ambulance at his request, even though he was tired and breathless. They were kind, understanding and let him have his dignity. The care they gave cannot be faulted’. Unfortunately the ongoing care provided for her father was not of a good standard, but this improved once he was transferred to the hospice. The members of staff have been written to, to thank and congratulate them and we will follow this up with further publicity. A new ‘You said we did’ sheet has been developed; this is included in the Quality Accounts report as an appendix.

Enclosure: F (Agenda Item: 9)
Board Report
1st December 2011
Title Quality Accounts – Six month review
Lead Director Fizz Thompson, Director of Patient Care
Report Author Fizz Thompson
Purpose of the report To provide an update and assure the Trust Board on the half year review of the Quality Accounts priorities
Recommendation (eg. Note, approve, endorse)
The Trust Board is asked to receive and NOTE the report.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
Links to all CQC registration and Essential Standards
Details of additional risks associated with this paper:
All clinical risks are detailed in the Trust risk register that link to the quality work streams
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
All areas of Patient Rights
Financial implications/impact None
Legal implications/impact
Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
Quality and Patient Safety work streams are shared with commissioners and stakeholders through regular updates and meetings and performance shared through the Integrated Performance Report
1
Other
Committees/groups where this item has been presented before
Progress of the Quality and Patient Safety work streams is monitored through the Executive Team, the Quality and Safety Committee and through the two sub groups, the Clinical Review Group and the Operational Health, Safety and Risk Group
Other options available and their pros and cons
Not applicable
Progress monitoring and review A yearly report will be presented to the Public Trust Board before publication. Further monitoring of the Quality Accounts priorities will be undertaken by the Quality and Safety Committee
Background papers ‘You said we did 2’
Introduction The paper firstly details the purpose of the Quality Accounts and then provides an overview of the half year activity on the key priorities for quality improvement. Background This Quality Account and report provides the public and the Trust with information about the quality of services we deliver to the public who call 999, use our Patient Transport services or our Commercial services arm. The purpose of the report for the Trust is outlined below:
Demonstrate SCAS’ commitment to continuous evidence based quality improvement
across the whole range of patient services it delivers Explain to our patients and staff where we will improve and need to make improvements Show how we respond to feedback and challenge from patients, the public and
our external stakeholders Be held to account for delivering quality improvements
Following a Board consultation and also consultation with our Quality and Safety Committee, staff and members of the public the following priorities were approved and confirmed for the year 2011/12. An update of progress is provided under the headings Half year Update
Priority 1 Patient Safety To decrease the numbers of patients experiencing a delay in response Delayed responses to patients in both red and amber call categories reduced in the first 5 months of the year and have seen a recent rise which is tracked and monitored through the IPR. Performance management meetings at locality level continue to address and analyse delays and root cause analysis meetings are planned in locality areas to understand the rise in delays and develop actions to address the long waits. Random reviews of patient care records are planned and will be reported through the Clinical Review Group Executive team and Quality and Safety committee
2
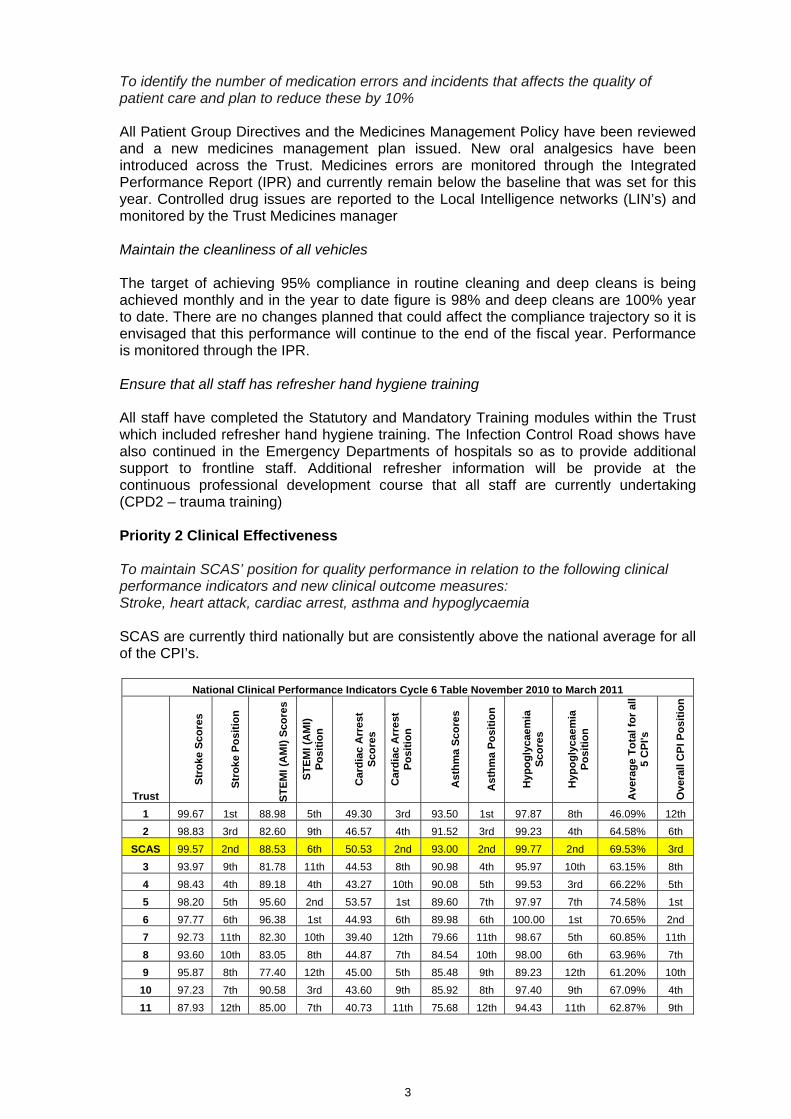
To identify the number of medication errors and incidents that affects the quality of patient care and plan to reduce these by 10% All Patient Group Directives and the Medicines Management Policy have been reviewed and a new medicines management plan issued. New oral analgesics have been introduced across the Trust. Medicines errors are monitored through the Integrated Performance Report (IPR) and currently remain below the baseline that was set for this year. Controlled drug issues are reported to the Local Intelligence networks (LIN’s) and monitored by the Trust Medicines manager Maintain the cleanliness of all vehicles The target of achieving 95% compliance in routine cleaning and deep cleans is being achieved monthly and in the year to date figure is 98% and deep cleans are 100% year to date. There are no changes planned that could affect the compliance trajectory so it is envisaged that this performance will continue to the end of the fiscal year. Performance is monitored through the IPR. Ensure that all staff has refresher hand hygiene training All staff have completed the Statutory and Mandatory Training modules within the Trust which included refresher hand hygiene training. The Infection Control Road shows have also continued in the Emergency Departments of hospitals so as to provide additional support to frontline staff. Additional refresher information will be provide at the continuous professional development course that all staff are currently undertaking (CPD2 – trauma training) Priority 2 Clinical Effectiveness To maintain SCAS’ position for quality performance in relation to the following clinical performance indicators and new clinical outcome measures: Stroke, heart attack, cardiac arrest, asthma and hypoglycaemia SCAS are currently third nationally but are consistently above the national average for all of the CPI’s.
National Clinical Performance Indicators Cycle 6 Table November 2010 to March 2011
Trust
Str
oke
Sc
ore
s
Str
oke
Po
siti
on
ST
EM
I (A
MI)
Sc
ore
s
ST
EM
I (A
MI)
P
osi
tio
n
Car
dia
c A
rre
st
Sco
res
Car
dia
c A
rre
st
Po
siti
on
Ast
hm
a S
co
res
Ast
hm
a P
osi
tio
n
Hyp
og
lyca
em
ia
Sco
res
Hyp
og
lyca
em
ia
Po
siti
on
Ave
rag
e T
ota
l fo
r al
l 5
CP
I's
Ove
rall
CP
I Po
sit
ion
1 99.67 1st 88.98 5th 49.30 3rd 93.50 1st 97.87 8th 46.09% 12th
2 98.83 3rd 82.60 9th 46.57 4th 91.52 3rd 99.23 4th 64.58% 6th
SCAS 99.57 2nd 88.53 6th 50.53 2nd 93.00 2nd 99.77 2nd 69.53% 3rd
3 93.97 9th 81.78 11th 44.53 8th 90.98 4th 95.97 10th 63.15% 8th
4 98.43 4th 89.18 4th 43.27 10th 90.08 5th 99.53 3rd 66.22% 5th
5 98.20 5th 95.60 2nd 53.57 1st 89.60 7th 97.97 7th 74.58% 1st
6 97.77 6th 96.38 1st 44.93 6th 89.98 6th 100.00 1st 70.65% 2nd
7 92.73 11th 82.30 10th 39.40 12th 79.66 11th 98.67 5th 60.85% 11th
8 93.60 10th 83.05 8th 44.87 7th 84.54 10th 98.00 6th 63.96% 7th
9 95.87 8th 77.40 12th 45.00 5th 85.48 9th 89.23 12th 61.20% 10th
10 97.23 7th 90.58 3rd 43.60 9th 85.92 8th 97.40 9th 67.09% 4th
11 87.93 12th 85.00 7th 40.73 11th 75.68 12th 94.43 11th 62.87% 9th
3

4
Cardiac arrest outcome data is now being exchanged between SCAS and the acute Trusts providing the Trust with accurate data which is reported in the Trusts Integrated Performance Report. This is now one of the new Quality Indicators. Progress against the new quality indicators is tracked through the IPR. These are new measurements that are difficult to benchmark nationally at present with some trust not being able to capture all data sets. An improvement plan is in place to improve the Trust’s position on all of the indicators. An update report will be provided with benchmarking data for the January board meeting To engage in Research and Development The Trust has engaged in local and national research projects. The Trust is currently jointly engaged in a privately funded research project on the management of Hypoglycaemia patients and a paper will hopefully be published shortly. The Trust is also part of a national project to review the effectiveness of the Lucas cardiac massage device in the pre-hospital setting. All research projects are reviewed and assessed at the Clinical Review Group and reported at the Quality and Safety Committee. To improve the management of pain Improvement in the STEMI indicator has centred on the provision of analgesia which action has been taken to introduce a new range of analgesics and the production of a “pain ladder”. Liquid and tablet forms of Ibuprofen and Paracetamol have been introduced along with Codeine tablets and oral Morphine. Training has been given by the Trusts Pharmacy Advisor at training sessions and at the universities To implement the new trauma pathway The training for the new trauma pathway has started and is due to be completed by the implementation of the pathway in April 2012. The criteria and assessment tool have been agreed across the South central region. The trust in on track to go live with the new trauma pathways that is planned for April 2012 Priority 3 Patient Experience To effectively engage with patients and stakeholders Two surveys have been completed within the Commercial Division around patient transport services. These have been reported to the Quality and Safety Committee. Plans are in place to undertake further patient satisfaction surveys with patients who receive advice from the Clinical Support desks, Emergency Care practitioners and also those patients who receive care from our front line staff. Focus group work has been undertaken with groups of patients with mental health issues and learning needs patients and also public groups about how they perceive the work of the ambulance service. To improve service delivery and quality of care to patients and their families We continue to share learning from complaints, incidents and feedback through our staff communications and have published our next ‘You said we did ‘publication (attached as Appendix)

You Said……..We Did: Service Improvements across SCAS.
Service Improvements. Oct 2011 Page 1 of 2
No. Improvement Action Outcome REQUEST: WE DID: WHAT THIS MEANS:
1. Better response to babies and young children who have stopped breathing.
Protocols have been changed to enable: Community First Responders to attend
paediatric emergencies for babies and children of any age.
The Air Ambulance to routinely be dispatched for all major paediatric traumas, cardiac arrest or other paediatric emergency requiring paramedic skills.
Emergency assistance is on scene quickly and Paramedic skills are made available routinely. Both of these significantly improve the chances of a good outcome for our young patients; particularly for incidents in rural areas.
2. Air Ambulance Paramedics expressed concern for what happens to bystanders following an incident; in particular whenever a member of the public has given first aid to a victim before the helicopter/ambulance service arrives on scene; or where they unexpectedly experience/witness extremely frightening or dangerous incidents, such as a road/rail accident, a serious illness, injury, crime or sudden death. Members of the public may be left feeling anxious, upset, numb and/or distressed. Although these are recognised as ‘normal’ reactions to stressful situations, they are also common signs/symptoms of Post Traumatic Stress Disorder which may result (in a small number of cases) if allowed to continue or not recognised.
Air ambulance paramedics, front line road staff and the Trust Mental Health & Learning Disability Lead (MH/LD Lead) worked together to produce small cards to give to people in such circumstances; thanking them for their help and advising them on what to do if they are affected by what has happened.
Improved quality of service to members of the public. People giving vital first aid are thanked for what they have done; their actions are acknowledged by the Trust and they are provided with information about how to access further support should this be required.
3. Improve access to information about support services for people who have a learning disability; cannot be left at home but do not need to go to hospital. A crew who had dealt with a difficult situation (when an adult who had a learning disability [LD] was witness to a sudden, unexpected and
The Trust MH/LD Lead has established formal links for emergency access to support services for people with LD (24hrs/day).
Crews can easily access specialist support for people who have a LD (and do not need healthcare intervention), when required.
– Improved quality of service to people with LD.
– Reduction in the amount of time on scene. – Reduced number of inappropriate A&E
attendances.

Service Improvements. Oct 2011 Page 2 of 2
traumatic death at their home) were unable to find emergency support for the person with LD (the person did not need to go to A&E). The incident happened outside of normal working hours.
4. Improved accuracy in recording initial data in the Emergency Operations Centres (EOC). We received a complaint from a member of the public after a Call Taker in one of our EOCs had recorded an address incorrectly. This error was not identified for 10 minutes.
Call Takers receive additional training to ensure they are competent inputting addresses correctly. Greater emphasis during training on appropriate use of the Special Situation (SS) function within the Address field on the computer system used in EOC. (This allows notes about a patient’s medical condition to be added to an address, if necessary, when special circumstances require this).
Improved quality of service: – Reduction in number of inaccuracies. – Reduction in number of delays. – Public involvement in process
(complainant was involved throughout).
5. A member of the public expressed frustration about how calls are processed in EOC and the length of time taken to do this.
A senior manager from EOC spent time speaking with the complainant; was able to explain the process fully and reassure them. A visit to EOC was arranged.
Greater public involvement. Increased opportunities for members of the public to visit one of our EOCs to see the process first hand.
October 2011

Enclosure: G (Agenda Item: 10)
Board Report
1st December 2011
Title FT Status Assurance Report
Lead Director Will Hancock, Chief Executive
Report Author John Divall, FT Project Director
Purpose of the report This report provides an update on the Trust’s FT application progress.
Recommendation (eg. Note, approve, endorse)
The Board is asked to NOTE the content of this report
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
N/A
Details of additional risks associated with this paper:
None identified
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
N/A
Financial implications/impact None identified
Legal implications/impact None identified
Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
None identified

Other
Committees/groups where this item has been presented before
None
Other options available and their pros and cons
N/A
Progress monitoring and review
Background papers None

FT STATUS ASSURANCE REPORT Executive Summary
The Authorisation date has slipped a month and is now planned for 1st March 2012 A full compliment of Governors has been appointed to our Council Historical Due Diligence (HDD) stage 3 commences November
Introduction The Foundation Trust Project is continuing to progress well. Following advice from Monitor our Board to Board date has been rescheduled for the 31st January to allow additional time for Monitor to gather further evidence for their assessment case. This means that the likely authorisation date has now slipped to 1st March 2012. Over the past few months the Monitor assessment team have been conducting interviews and gathering supporting evidence and I would wish to put on record my thanks to everyone involved for their cooperation and responsiveness which has enabled us to meet the various deadlines. Whilst there is still further work to do the Trust remains in a strong position and is confident of achieving FT authorisation this financial year. Council of Governor The election for the Council of Governors has been completed and the results announced on the 3rd November. The Trust now has in place a full compliment of both elected and appointed Governors. The induction programme for Governors has commenced with a days training being held on:
Monday 14th November Saturday 26th November
Each Governor has also received a comprehensive information pack containing key documents to which they can subsequently refer. Further Governor development days have been scheduled for:
Monday 6th February Thursday 16th February Monday 5th March Thursday15th March
The inaugural Shadow Council of Governors meeting is scheduled for 16th January 2012. The agenda for this meeting is still to be finalised but will focus on the statutory responsibilities of the Council of Governors eg appointment of Chairman and Non Executive Directors, appointment of Auditors etc in readiness for the Trust’s Authorisation. Future Timetable / Key Events
9th January - Deloitte’s commence stage 3 Historical Due Diligence 31st January 2012 - Monitor Board to Board 23rd February - Monitor Board Meeting 1st March - Planned Authorisation date.
John Divall FT Project Director 23rd November 2011
Enclosure: H (Agenda Item: 11)
Board Report
1st December 2011
Title FT Application – Board Submissions to Monitor
Lead Director Will Hancock, Chief Executive
Report Author John Divall, FT Project Director
Purpose of the report This report provides an update on the Trust’s FT application progress.
Recommendation (eg. Note, approve, endorse)
1. The Board is asked to APPROVE the following documents for submission to Monitor on 1 December 2011: Schedule 2 – Schedule of Mandatory Services Schedule 3 – Schedule of Non-Mandatory Services Trust Constitution Statement on the outcome of the election process
2. The Board is asked to NOTE the update on the
implementation of the Membership Strategy.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
N/A
Details of additional risks associated with this paper:
None identified
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
N/A

Financial implications/impact None identified
Legal implications/impact The Constitution is a statutory requirement which can only be changed with the permission of the Council of Governors and Monitor
Equality and Diversity implications/impact
The Trust has a duty to ensure that its membership is representative of the communities we serve. The membership analysis covers age, gender, socio economic and geographic groups
Partnership working and public engagement implications/impact
None identified
Other
Committees/groups where this item has been presented before
None
Other options available and their pros and cons
N/A
Progress monitoring and review
Background papers None

FT Application – Board Submissions to Monitor
1.0 Introduction As a Foundation Trust, the Trust will be governed by its Terms of Authorisation (ToA) issued by the FT regulator, Monitor. The ToA consist of 6 parts:
Schedule 1: The Constitution Schedule 2: Mandatory Goods & Services Schedule 3: Mandatory Education & Training Schedule 4: Private charges cap Schedule 5: Limit on borrowing Schedule 6: Information
Following authorisation each of the above schedules will be published by Monitor on their website. At this stage we have been asked by Monitor to submit our Constitution and Schedules 2 and 3. Post authorisation these schedules cannot be varied without agreement of both Monitor and the relevant commissioner. 2.0 Schedule 2 – Schedule of Mandatory Services (Appendix 1) The Schedule records the current commissioned volumes for A&E and PTS and the number of contracts for other services. Recommendation: The Board is asked to formally APPROVE the Schedule of Mandatory Services and its submission to Monitor. 3.0 Schedule 3 – Schedule of Non-Mandatory Services (Appendix 2) This schedule records the provision of education to third parties where contracts which have been signed (or are understood to be going to be signed) with relevant commissioning bodies or other third parties. SCAS has no such contract and is therefore submitting a nil return. Recommendation: The Board is asked to formally APPROVE the Schedule of Non-Mandatory Services and its submission to Monitor. 4.0 Trust Constitution Following feedback from Monitor it has been necessary to amend the previous draft Constitution. Our Solicitors (Beechcroft) have been consulted to ensure that we remain legally constituted. The required changes are shown in Appendix 3 together with confirmation from Monitor that these amendments have been accepted. Due to its size the Constitution has been circulated electronically to Board members. Recommendation: The Board is asked to formally APPROVE the Constitution and its submission to Monitor.

5.0 Statement on the outcome of the election process The Governor election process which closed on the 2nd November was independently managed by the Electoral Reform Service (ERS). All elected governor posts have been filled. The Oxfordshire and Buckinghamshire public governors were elected unopposed as was the Staff: EOC position. With regards to the Appointed Governors the Trust has now received nominations for all governor positions. Further details including the names of governors and the election results are contained in the attached statement (Appendix 4) Recommendation: The Board is asked to formally APPROVE the Statement of Election and its submission to Monitor. 6.0 Update on the Membership Strategy implementation Membership recruitment continues to grow and currently stands at 7,500 public members against our target of 8,000 by 31st March. The distribution of membership of across the spectrum of age, ethnicity, geography etc is strong with a slight shortfall in members from the Asian or Asian British – Pakistani community which is currently being targeted. Further details regarding the analysis of public members is attached in Appendix 5 Recommendation: The Board is asked to NOTE the progress made in implementing the Membership Strategy. John Divall FT Project Director 17th November 2011

Appendix 1 SOUTH CENTRAL AMBULANCE SERVICE NHS TRUST
Schedule 2 – Schedule of Mandatory Services (2011-12)
Year: 2011-12
Trust: South Central Ambulance Service
A&E
Critical care
transfer Priority
PTS Other PTS
Emergency planning
HART / USAR Other
Urgent Care
Service Logistics Service
Equipment Service
Sub care group Currency
A&E Incidents 414,800 - - - - - - - - -
HART Service - - - - - 1 - - - -
PTS Journeys - - - 593,100 - - - - - - Emergency Planning Service - - - - 1 - - - - -
Out of Hours Service - - - - - - - 2 - -
Logistic Services Service - - - - - - - - 2 - Community Equipment Services Service - - - - - - - - - 1
- - - - - - - - - -
- - - - - - - - - -
- - - - - - - - - -
- - - - - - - - - -
Total
414,800 - - 593,100 1 1 - 2 2 1

Appendix 2
SOUTH CENTRAL AMBULANCE SERVICE NHS TRUST
Schedule 3 – Schedule of Non-Mandatory Services (2011-12)
Commissioning body Educational body Contract Length
Expiry date of contract
Student group
Type of training
Number of Students
Contract Value
(Years) (£000s)
0
Total 0

Appendix 3
Review of Draft Constitution 19 October 2011 South Central Ambulance Service NHS TRUST Introduction
Monitor reviews your constitution to ensure that it is in accordance with Schedule 7 of the National Health Service Act 2006 (the ‘2006 Act’) and is otherwise appropriate.
Please note that Monitor has reviewed your constitution on the basis that it is the final draft. We do not expect to review further drafts unless produced as a result of our comments. You may assume that amendments which have not been commented on below are acceptable (however this does not prevent Monitor from re-visiting such amendments at a later stage).
Unless picked up as part of the review and set out below, Monitor has not checked the document for typographical errors, incorrect references, formatting, inconsistencies, or to suggest improvements.
Reference Comment
Main Body
12.5
Check the use of word ‘appointment’ here.
We have amended the wording in 12.5 and removed reference to the words "if that appointment arises from his appointment by the appointing organisation".
The amendment is accepted.
19.8
This paragraph provides that, excluding the Chair, least half the board of directors shall be non-executive directors. This mirrors paragraph A.3.2 of Monitor’s Code of Governance and is therefore acceptable to Monitor.
In light of the discussion at the legal/governance meeting of 14 October, could the Trust confirm that it will be able to comply with this provision? Alternatively could the Trust amend the drafting and provide an explanation if it will unable to meet the Code of Governance in this regard?
The Trust cannot comply with Code provision A.3.2, which provides that at least half the board of directors, excluding the Chairman, shall comprise of non-executive directors determined by the board to be independent. This is because it proposes to have [7 non-executives including the Chair] and 7 executive directors. The Trust believes this approach is appropriate at this time as it will provide the required capacity at Board level to focus on new stakeholders and emerging commercial markets. The Board may seek to review this position once the external environment and NHS reforms become more settled.

Reference Comment
However, due to the fact that there is parity on the board between executive and non-executive directors, we have (in accordance with Appendix B8, paragraph 5 of Monitor's Guide for Applicants) amended paragraph 19 to ensure that the Chair will have the casting vote.
Please see the proposed amendments to paragraph 19 of the draft Constitution shown in tracked changes.
The explanation on A.3.2 of the Code of Governance is noted. Should the Trust be authorised as a foundation trust, it would have to report to Monitor on an annual basis as to its compliance (or not) with A.3.2.
The amendments to paragraph 19 of the main body and paragraph 2.2 of Annex 7 are accepted. Please however check for inconsistency between the new drafting and paragraph 2.6 of Annex 7 (Joint Executive Appointments) which provides for votes to be shared between directors who are in post in a joint capacity.
We note your comment. We believe that the inconsistency to which you refer stems from the fact that paragraph 19.8 of the main body of the Constitution currently states that "The Directors shall at all times have one vote each save that the Chairman shall be entitled to exercise a second and casting vote where there is parity on the Board….", whereas paragraph 2.6 of Annex 7 provides for votes to be shared between jointly appointed directors (i.e. they are entitled to exercise one vote between them).
We have sought to clarify this by amending the wording in paragraph 19.8 as per the below:
"Save where more than one person is appointed jointly to a post of Executive Director and shares a vote in accordance with paragraph 2.6 of Annex 7, the Directors shall at all times have one vote each except that where the number of votes for and against a motion is equal, the Chairman shall be entitled to exercise a second or casting vote".
Annex 4
Annex 3
The organisations appointing the Appointed Governors need to be specified by name.
We have now identified each of the Appointed Governors by name in the Annex 3 of the draft Constitution. Please see the proposed amendments on the attached draft.
PCT governors:
The listing of the PCTs is accepted. However Monitor is unable to accept the Trust’s proposal that both of the PCT governors are joint appointments. Paragraph 9(3) of Schedule 7 of the 2006 Act requires that at least one governor is appointed by a PCT for which the Trust provides services. Monitor’s view of the legislation is that at least one governor must be appointed by a single PCT. Other PCT governors may be joint appointments if that is the Trust’s preference.
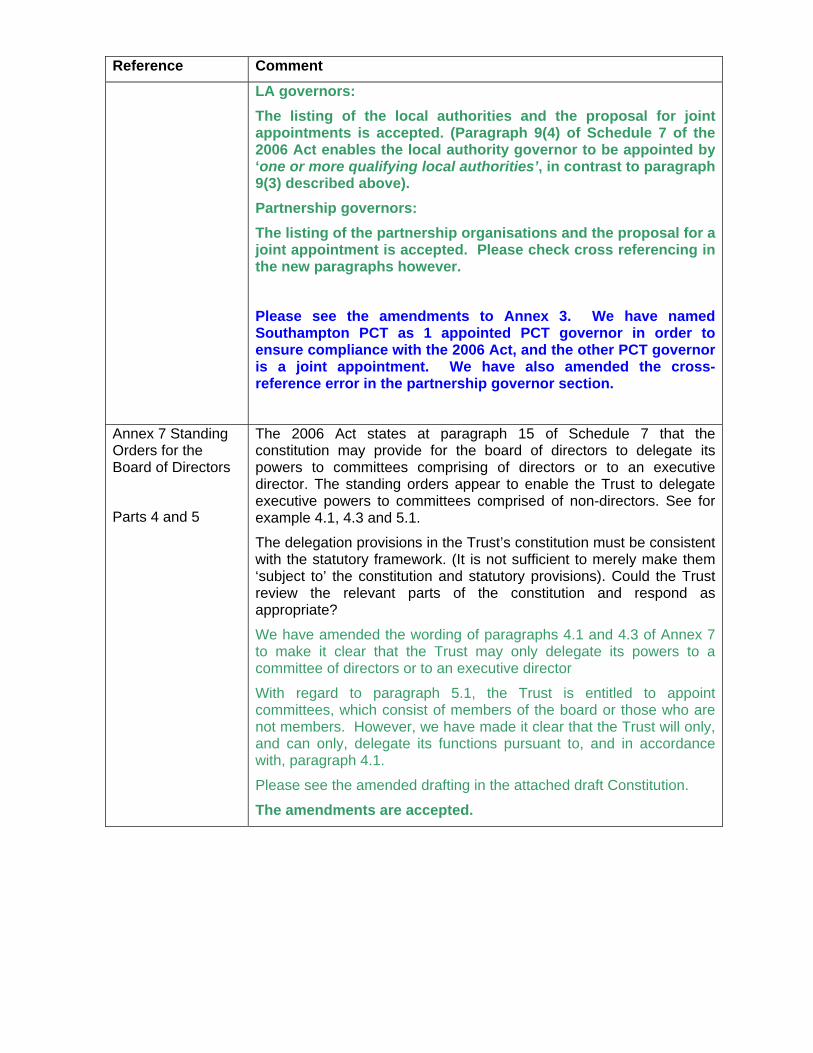
Reference Comment
LA governors:
The listing of the local authorities and the proposal for joint appointments is accepted. (Paragraph 9(4) of Schedule 7 of the 2006 Act enables the local authority governor to be appointed by ‘one or more qualifying local authorities’, in contrast to paragraph 9(3) described above).
Partnership governors:
The listing of the partnership organisations and the proposal for a joint appointment is accepted. Please check cross referencing in the new paragraphs however.
Please see the amendments to Annex 3. We have named Southampton PCT as 1 appointed PCT governor in order to ensure compliance with the 2006 Act, and the other PCT governor is a joint appointment. We have also amended the cross-reference error in the partnership governor section.
Annex 7 Standing Orders for the Board of Directors
Parts 4 and 5
The 2006 Act states at paragraph 15 of Schedule 7 that the constitution may provide for the board of directors to delegate its powers to committees comprising of directors or to an executive director. The standing orders appear to enable the Trust to delegate executive powers to committees comprised of non-directors. See for example 4.1, 4.3 and 5.1.
The delegation provisions in the Trust’s constitution must be consistent with the statutory framework. (It is not sufficient to merely make them ‘subject to’ the constitution and statutory provisions). Could the Trust review the relevant parts of the constitution and respond as appropriate?
We have amended the wording of paragraphs 4.1 and 4.3 of Annex 7 to make it clear that the Trust may only delegate its powers to a committee of directors or to an executive director
With regard to paragraph 5.1, the Trust is entitled to appoint committees, which consist of members of the board or those who are not members. However, we have made it clear that the Trust will only, and can only, delegate its functions pursuant to, and in accordance with, paragraph 4.1.
Please see the amended drafting in the attached draft Constitution.
The amendments are accepted.

Reference Comment
Annex 7 Standing Orders for the Board of Directors
Part 8, opening statement (now numbered 8.1)
Consider whether the reference to HSG 1993/05 will be relevant to the Trust once authorised as a foundation trust.
HSG (93)05 sets out the principles for standard of business conduct for NHS staff. Whilst we appreciate that these are not applicable to, or binding on, Foundation Trusts, the Trust would still like to consider/have regard to the content of these documents to the extent applicable and appropriate.
In view of this, we have amended the wording in Part 8 (opening statement) to make it clear in the standing orders that the Trust will only have regard to this circular to the extent applicable and appropriate.
The explanation and amendment is accepted.
Annex 7 Standing Orders for the Board of Directors
14.6 Code of Conduct
Replace ‘Monitor’s Code of Conduct’ with ‘Monitor’s Code of Governance’.
We have replaced reference to Monitor's 'Code of Conduct' with 'Monitor's Code of Governance' on the attached draft Constitution.
The amendment is accepted.
Annex 8 Further Provisions
A8 2.4
Check cross referencing.
We have checked, and amended, the cross referencing in Annex 8 to make these provisions clearer. Please see amendments in the attached draft Constitution.
The amendments are accepted.
Annex 8 Further Provisions
A8 4.1
Consider whether it is appropriate for the Role of the Secretary to include the following:
‘ensure that the Trust complies with relevant legislation and the Terms of Authorisation issued by Monitor’
We have amended the drafting in A8.4.1 of Annex 8 to make it clear that the role of the Foundation Trust Secretary in this regard is to ensure that the corporate affairs of the FT are undertaken to the highest standards of probity and in accordance with statutory and legislative requirements within the regulatory framework.
Please see the amended wording at A8.4.1 of the attached draft Constitution.
The amendments are accepted.
Please consider these comments and respond as appropriate. Where amendments are made to the constitution (including annexes) please show amendments using tracked changes.

Appendix 4 SOUTH CENTRAL AMBULANCE SERVICE
NHS TRUST
STATEMENT OF ELECTION TO THE COUNCIL OF GOVERNORS 2011
The report of voting in the above election, which closed at 5pm on Wednesday 2nd November 2011, is as follows. 1.0 Public: Hampshire
Number of eligible voters: 2,034 Total number of votes cast: 295 Turnout: 14.5% Number of votes found to be invalid: 1
Blank or Spoilt No declaration form received
10
Total number of valid votes to be counted: 294 Result (6 to elect) ADENUBI, Kemi ..................................................................... 160 Elected ALLEN, Mike ........................................................................... 145 Elected CARNELL, Paul Edward ....................................................... 181 Elected FAROOQ, Khalid..................................................................... 34 HARTRIDGE, Jamie............................................................... 131 Elected IP, Kam ................................................................................... 51 READ, Allan C........................................................................ 118 Elected RYAN, Richard....................................................................... 107 STEED, Paul Anthony............................................................. 107 TOTTLE, Al............................................................................. 135 Elected N.B Following Mike Allen’s resignation as a Governor, due to already being a Governor at another NHS Trust, Richard Ryan was duly elected a Governor in his place. This process was carried out in accordance with our constitution. 2.0 Public: Berkshire
Number of eligible voters: 1,541 Total number of votes cast: 197 Turnout: 12.8% Number of votes found to be invalid: 0
Blank or Spoilt No declaration form received
00
Total number of valid votes to be counted: 197 Result (3 to elect)

ANDERSON, Fiona................................................................. 13 BANNISTER, John.................................................................. 63 CLARK, Gary ......................................................................... 78 Elected COPELAND, Michael John ..................................................... 24 DAVIDSON, Anne ................................................................... 59 HAMPTON, Melanie Caroline Alexandra ............................. 75 Elected HEATH, Michael...................................................................... 1 McDERMOTT, James ............................................................. 66 PLAYFOOT, Benita................................................................ 80 Elected ROWE, Michael David ............................................................ 26
3.0 Uncontested Public Governor Appointments
There were not enough candidates to contest the two remaining constituencies,
therefore the following people have joined the Council of Governors unopposed:
Public: Buckinghamshire:
BOB DUGGAN
RICHARD FRASER
DAVID RIDLEY
Public: Oxfordshire:
PATRICK JOHN CONAFRAY
ROBERT JOHN LASSAM
TIM WINDSOR-SHAW 4.0 Staff: Operational Clinical Staff and Managers
Number of eligible voters: 1,546 Total number of votes cast: 390 Turnout: 25.2% Number of votes found to be invalid: 0
Blank or Spoilt No declaration form received
00
Total number of valid votes to be counted: 390 Result (3 to elect) BROWN, Barry........................................................................ 108 DONNE, John......................................................................... 163 Elected EDMUNDS, Sean Christopher ................................................ 99 LEAHY, Adrian ........................................................................ 114 PALMER, David ..................................................................... 144 Elected WATTS, Carol ........................................................................ 180 Elected

5.0 Staff: Commercial Services (Excluding PTS call centre and OOH) and Support Staff
Number of eligible voters: 508 Total number of votes cast: 166 Turnout: 32.7% Number of votes found to be invalid: 0
Blank or Spoilt No declaration form received
00
Total number of valid votes to be counted: 166 Result (one to elect) CICCI, Rafael .......................................................................... 20 COOPER, Steven ................................................................... 9 FOWLER, Christina ............................................................... 112 Elected JOHNSON, Ludlow ................................................................. 25 6.0 Uncontested Staff Governor Appointments
There were not enough candidates to contest the one remaining staff governor vacancy,
therefore the following person have joined the Council of Governors unopposed:
Staff: Emergency Operations Centres (EOC) EDDIE COTTRELL Electoral Reform Services confirmed that, as far as reasonably practicable, every person whose name appeared on the electoral roll supplied to us for the purpose of the ballot:-
a) was sent the details of the ballot and b) if they chose to participate in the ballot, had their vote fairly and accurately
recorded The elections were conducted in accordance with the rules and constitutional arrangements as set out previously by the Trust, and ERS is satisfied that these were in accordance with accepted good electoral practice. All voting materials will be stored for twelve months.
7.0 Appointed partnership governors Partnership: Local Authority CLLR MARY BALLIN, Bracknell Forest Borough Council CLLR SIMON HOARE, West Oxfordshire District Council CLLR KEITH HOUSE, Eastleigh Borough Council

Partnership: Primary Care Trust (PCT) FRED HUCKER, Oxfordshire PCT PAULINE QUAN-ARROW, Southampton PCT Partnership: Other BARRY LIPSCOMB, Hampshire & Isle of Wight Air Ambulance All members have been informed of results and these have been published on our website

Appendix 5 SOUTH CENTRAL AMBULANCE SERVICE
NHS TRUST
Membership Strategy Progress Report Background information SCAS has successfully implemented its membership strategy over the last year. The four counties covered by SCAS contains a mixture of urban areas of high density population such as Portsmouth, Southampton, Reading, Slough, Oxford and Milton Keynes and large rural areas in parts of Hampshire Oxfordshire and Buckinghamshire. This presents significant variation in population profile with the inner city areas having a larger prevalence of social deprivation than the rural areas which often have a more elderly population. South Central Ambulance Service NHS Trust aims to have a membership that is representative of the diverse communities it serves in terms of age, gender and ethnicity and will therefore strive to achieve:
A membership constituency made upon service users, carers, local people and
staff A governing council elected by members, as well as the people appointed from
other local organisations, known as the council of governors. Table 1 below shows the breakdown by ethnicity of the population within SCAS coverage area. 90.3% of its population is White British, White- Any other White background is the largest ethnic minority (2.83%) followed by Asian or Asian British – Indian (1.35%) and Asian or Asian British – Pakistani (1.25%). Table 1 – Ethnicity background of SCAS coverage area
Ethnicity Percentage of population
within SCAS area White British 90.30% White - Irish 1.05% White - Any other White background 2.83% Mixed - White and Black Caribbean 0.36% Mixed - White and Black African 0.11% Mixed - White and Asian 0.36% Mixed - Any other mixed background 0.28% Asian or Asian British - Indian 1.35% Asian or Asian British - Pakistani 1.25% Asian or Asian British - Bangladeshi 0.21%
Asian or Asian British - Any other Asian background 0.29% Black or Black British - Caribbean 0.53% Black or Black British - African 0.35%
Black or Black British - Any other Black background 0.08%

Other Ethnic Groups - Chinese 0.46%
Other Ethnic Groups - Any other ethnic group 0.37% FT Autumn activities As per SCAS August FT Report during June-August period SCAS concentrated successfully on increasing the membership number for Oxfordshire and ethnic minorities such as Chinese and Indian. During September and October SCAS switched its focus on organising and/or attending a variety of events in Berkshire, Buckinghamshire and Hampshire as follows: September FT EVENTS Thurs 1 Sep Bucks County Show BUCKS Sat 3 Sep Reading Pride BERKS Sun 4 Sep Portsmouth Multicultural Festival HANTS Thurs 8 Sep Employing people from diverse communities, Basingstoke HANTS Fri 9 Sep SCAS FT/CFR Roadhsow, Nicholson Centre, Maidenhead BERKS Sat 10 Sep Waddesdon Emergency Services Day BUCKS Sat 17/Sun 18 Sep The Royal County of Berkshire Show BERKS
Fri 23 Sep SCAS FT Roadshow High Wycombe - Eden Shopping Centre BUCKS
October events
Sat 08 Oct Autumn Pumpkin Festival, Netley, Southampton HANTSSun 16 Oct Sunday Funday 2011, Newbury library BERKS
Fri 21 Oct SCAS FT Roadshow, Princess Square Shopping Centre, Bracknell BERKSMon 31 Oct SCAS FT Roadshow, Milton Keynes Shopping Centre BUCKS
In order to ensure that SCAS has the 14 and above age group represented in its membership all local secondary schools were contacted and invited to include an FT article. A number of schools inserted SCAS information onto their newsletters and SCAS gained quite a few new FT members as a result. Contacts were also made with the Reading Hindu Temple, the Reading Mosque, the Pakistani Group in Oxford and the Berkshire Chinese Association and presentations will be confirmed for early next year. Other activities included mailing SCAS main local suppliers and contacting local companies. As a whole the number of initiatives which were undertaken from September to-date (i.e. 16th November 2011) contributed to an increase in members by over 1,300. The following Tables show the number of members by county and by ethnicity-where SCAS need to increase its membership-as at 16 November 2011 respectively.

Indicators
R At risk - need more members
A
Could cause actual or potential variance to total no. of members
needed
G Good no. of members/or exceeds
expectations
Membership by Geography - As at 16 November 2011
16 November 2011 Year
to date Full year
Actual Plan RAG Forecast Plan RAG
No. No. No. No.
Hampshire 2,138 2,350 A 3,200 3,200 G
Oxfordshire 1,618 1,450 G 1,600 1,600 G
Buckinghamshire 1,956 1,450 G 1,600 1,600 G
Berkshire 1,789 1,450 G 1,600 1,600 G
Total 7,502 8,000 8,000
Membership by Ethnicity – As at 16 November 2011
16 Nov 2011-Year to
date Full year
Actual Plan RAG Forecast Plan RAG
No. No. No. No.
Black or Black British - Caribbean
34 34 G 42 42 G
Asian or Asian British - Indian
91 90 G 108 108 G
Asian or Asian British - Pakistani
51 70 R 100 100 A
Other Ethnic Groups - Chinese
27 27 G 37 37 G

SCAS will continue focusing its attention on ensuring that ethnic minority targets are met in the above groups. Other local profiling by gender, age and ACORN Socio-Economic Category Please find below relevant information. Membership by Gender - As at 16 November 2011
16 Nov 2011-Year to date Full year
Actual Plan RAG Forecast Plan RAG No. No. No. No. Unspecified 27
Male 3,187 3,150 G 4,000 4,000 G
Female 4,291 3,500 G 4,000 4,000 G
Membership by Age - As at 16 November 2011
16 Nov 2011-Year to date Full year
Actual Plan RAG Forecast Plan RAG No. No. No. No. 0-16 155 180 A 286 286 G 17-21 729 600 G 734 734 G 22-29 936 800 G 980 980 G 30-39 1,291 1,180 G 1,265 1,265 G 40-49 1,441 1,400 G 1,597 1,597 G 50-59 1,226 1,200 G 1,300 1,300 G 60-74 1,277 1,170 G 1,223 1,223 G 75+ 414 450 A 615 615 G
Membership by ACORN Socio-Economic Category - As at 16 November 2011
16 Nov 2011-Year to date Full year
Actual Plan RAG Forecast Plan RAG No. No. No. No.
Wealthy Achievers [1] 2,514 2500 G 2,794 2,794 G
Urban Prosperity [2] 673 670 G 797 797 G
Comfortably Off [3] 2,245 2230 G 2,272 2,272 G
Moderate Means [4] 838 830 G 960 960 G
Hard Pressed [5] 1,017 1,000 G 995 995 G
Not available [NA] 218 200 G 196 196 G

FT Winter initiatives Events will continue to be held throughout the whole of SCAS coverage area and the emphasis will be in the following areas:
Hampshire constituency – events in Winchester and Portsmouth have been scheduled in December and more will be scheduled early next year
Pakistani communities – Membership Officer has asked Equality and Diversity Manager to contact various associations and arrange presentations
SCAS has also scheduled a mailing to local GPs, Rotary clubs and the Royal British Legion. SCAS monitors the FT membership data on a monthly basis and this data is included in the company’s IPR (Integrated Performance Report) which is distributed to the Board. It also monitors the membership number on a weekly basis. Duncan Burke Director of Communication and Engagement 17th November 2011

Enclosure: I (Agenda Item: 13)
Board Report
Title
Integrated Performance Report for Month 7 of the 2011-12 Financial Year
Lead Director Charles Porter
Report Author Daphne Thomas
Purpose of the report
This report seeks to highlight the key areas of SCAS performance that are out of line with the plan, and to show what actions are being taken.
Recommendation (e.g. Note, approve, endorse)
The Board is asked to approve the report and actions being taken.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
Outcome 16
Details of additional risks associated with this paper:
As covered in the report
Links to the NHS Constitution (relevant staff/patient rights)
All areas of patient rights

All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
Financial implications/impact Covered in the finance report
Legal implications/impact None identified
Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
None identified
Other
Committees/groups where this item has been presented before
Executive Committee
Other options available and their pros and cons
N/A
Progress monitoring and review Executive Committee
Background papers Annual Plan 2011/12
Executive Summary 1 IPR Development The report has now been live for seven months and most areas of the report are now complete. A small amount of data is still not available and target dates are included in these instances. 2 Performance Summary SCAS continues to exceed both operational performance standards and five of six clinical indicators exceeded target level. Clinical indicators There has been very little change in performance against our clinical indicators in October. All four are within 1% of the performance seen in September, with STEMI performance being the only one below target levels and there is an action plan is place to address this. PPCI performance is lower this month, however this is based on a small sample size (as there is a time lag related to hospitals providing the data) and should not be interpreted at this stage as a downward trend in performance. Activity Demand rose in October, and finished as the second busiest month ever for SCAS, just behind December 2010. Year on year, there has been an increase of 1.6%, but there is a mixed pattern amongst the PCT’s. Three PCTs saw demand drop when compared to October 2010, yet two (Oxfordshire and Berkshire East) saw increases in excess of 5%. Year to date, demand is 3.2% higher than the same period last year.
Response Time
Performance against the RED8 standard was 77.2% for the month of October. This was a minimal deterioration compared to September (77.4%) despite demand rising by 5% month on month. All PCTs are above the A8 national standard on a cumulative basis with the exception of Buckinghamshire which is currently 68.3% year to date – an improvement from last year’s position which was 67.7% at this point.

RED19 performance fell by 0.7% in October although Berks East saw a marked increase, where performance improved by over 1%. Overall, 7 of the 8 PCTs remain above trajectory for the RED19 standard and the clusters are on target to meet the national standard.
Hospital delays
The hospital delay penalties increase in October but, as with demand levels, performance varied across the Trust: Milton Keynes, RHCH and Southampton General, saw significant increases in handover delays, with the rise in Milton Keynes exceeding 60% month on month. However, at the other end of the scale, North Hants saw a fall in delays of almost 25%, and Wexham Park dropped by 20%. Year on year, with the exception of John Radcliffe and Horton, handover delays are almost 80% higher than they were twelve months ago. At the top of the list is Milton Keynes, where delays are five times longer that in October 2010. Clear up times increase by 8% compared to last month, but year on year, the amount of time lost is down by over 60%.
3 Exceptions The Summary from the Integrated Performance Report is shown below:
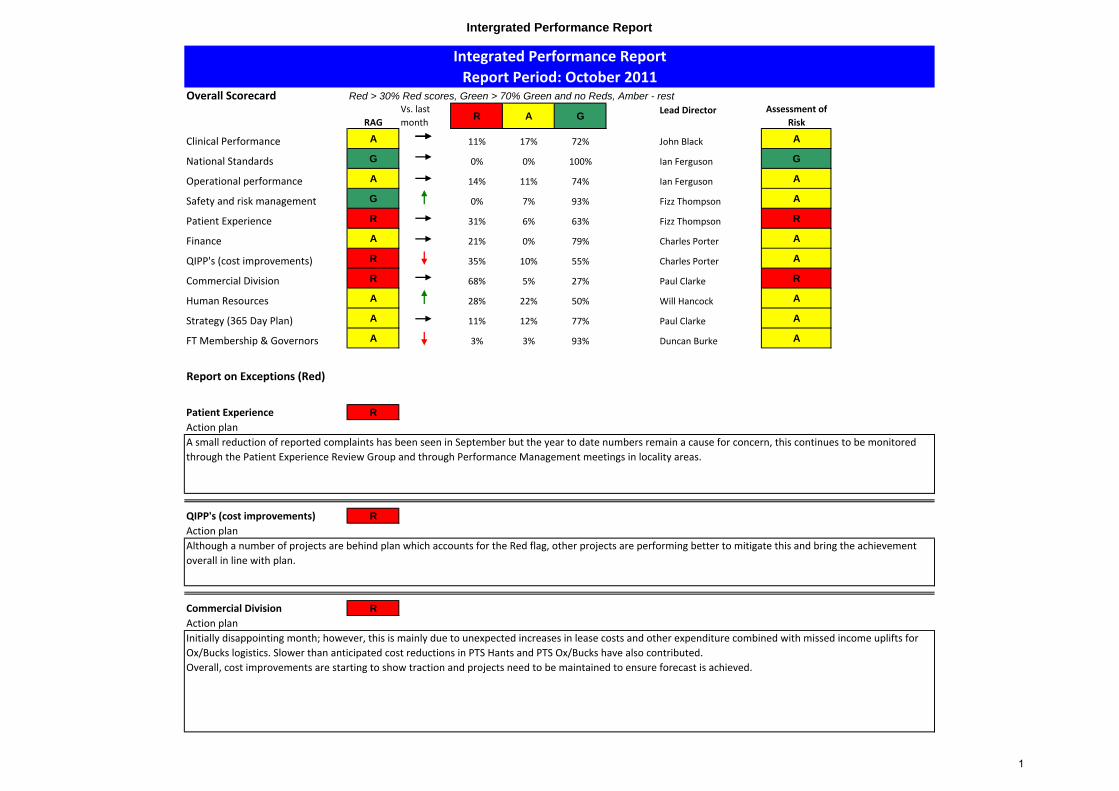
Intergrated Performance Report
Overall Scorecard Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
RAGVs. last month
R A GLead Director Assessment of
Risk
Clinical Performance A 11% 17% 72% A
National Standards G 0% 0% 100% Ian Ferguson G
Operational performance A 14% 11% 74% Ian Ferguson A
Safety and risk management G 0% 7% 93% Fizz Thompson A
Patient Experience R 31% 6% 63% Fizz Thompson R
Finance A 21% 0% 79% Charles Porter A
QIPP's (cost improvements) R 35% 10% 55% Charles Porter A
Commercial Division R 68% 5% 27% Paul Clarke R
Human Resources A 28% 22% 50% Will Hancock A
Strategy (365 Day Plan) A 11% 12% 77% Paul Clarke A
FT Membership & Governors A 3% 3% 93% Duncan Burke A
Report on Exceptions (Red)
Patient Experience R
Action plan
QIPP's (cost improvements) R
Action plan
Commercial Division R
Action planInitially disappointing month; however, this is mainly due to unexpected increases in lease costs and other expenditure combined with missed income uplifts for Ox/Bucks logistics. Slower than anticipated cost reductions in PTS Hants and PTS Ox/Bucks have also contributed. Overall, cost improvements are starting to show traction and projects need to be maintained to ensure forecast is achieved.
Although a number of projects are behind plan which accounts for the Red flag, other projects are performing better to mitigate this and bring the achievement overall in line with plan.
Integrated Performance ReportReport Period: October 2011
John Black
A small reduction of reported complaints has been seen in September but the year to date numbers remain a cause for concern, this continues to be monitored through the Patient Experience Review Group and through Performance Management meetings in locality areas.
1

Intergrated Performance Report
Clinical performance Overall rating A Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Clinical Treatment
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
STEMI care bundle 87.5% 90.0% A 88.1% 90.0% A 90.0% 90.0% G
The cause of the drop in the performance has been identified as analgesic administration and work is ongoing to address this issue by the ASCQI lead. An action plan has been developed.
Stroke care bundle 100.0% 95.0% G 99.1% 95.0% G 99.0% 95.0% G No commentary required
Hypoglycaemia care bundle 100.0% 95.0% G 99.7% 95.0% G 99.0% 95.0% G No commentary required
Asthma care bundle 94.8% 80.0% G 94.0% 80.0% G 93.5% 80.0% G No commentary required
% STEMI with PPCI to centre in 80 min 80.0% 75.0% G 79.7% 75.0% G 82.0% 75.0% G No commentary required
‐ all hospitals except ORH 78.7% 85.0% R 86.2% 85.0% G 86.0% 85.0% GPPCI information not complete for the month so insifficient evidence for concern at present
‐ ORH 87.5% 53.8% G 61.0% 53.8% G 61.0% 53.8% G No commentary required
% STEMI with PPCI to treatment in 150 min 90.5% 75.0% G 98.2% 75.0% G 85.0% 75.0% G No commentary required
% FAST patients call to leave 39 min 57.7% 58.8% A 58.1% 59.1% A 61.6% 56.5% GAction plan to be put in place to review improvements.
% FAST patients to centre in 60 min 51.2% 53.0% A 56.52% 51.7% G 59.0% 51.7% GAction plan to be put in place to review improvements.
Clinical Outcome
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
% patients with return of spont's circul'n by hospital arrive (ROSC)
4.63% 20.5% R 15.42% 19.5% R 19.3% 19.3% G
An investigation is underway to understand the reduction in performance and will be monitored through the CRG and Q and S committee
% patients with return of spont's circul'n by hospital arrive (ROSC) ‐ witnessed cardiac arrest
12.5% 36.7% R 33.14% 37.9% R 40.7% 40.7% G
An investigation is underway to understand the reduction in performance and will be monitored through the CRG and Q and S committee
Cardiac Arrest: % discharged alive following ambulance resus'n (Nationally submitted data for Period July 11)
4.7% tba n/a 5.9% tba n/a tba tba n/a No commentary required
Cardiac Arrest: % discharged alive following ambulance resus'n - witnessed cardiac arrest (Nationally submitted data for period July 11)
14.3% tba n/a 24.2% tba n/a tba tba n/a No commentary required
Outcome Measure Oct‐11 Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐
nil)
Treatment Measure Oct‐11 Full year
Lead Director: John Black
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐
nil)
Year to date
Year to date
2

Intergrated Performance Report
Safeguarding
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Statutory & Mandatory 97.0% 95.0% G 99.0% 95.0% G 95.0% 95.0% GStaff originally ineligible through LTS, career break etc will need additional training
Number of adult referrals 70 90 G 700 630 G 917 917 G
We are reviewing referrals and safeguarding has ben part of the statutory and mandatory training . There are plans to increase staff awareness through support and clincial memos
Number of child referrals 21 27 G 199 168 G 299 299 G
We are reviewing referrals and safeguarding has ben part of the statutory and mandatory training . There are plans to increase staff awareness through support and clincial memos
Hygiene & infection prevention & control
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Vehicle deep cleans 333 288 G 1891 1821 G 4,764 4,764 G
Statistics could not be provided for October performance due a staffing issue in the supplier’s contract team. This issue has had no perceived effect on quality and statistics will be available again in December. Current figures for September
Vehicle routine cleans* 9,873 9,903 A 59,310 60,635 A 116,051 116,051 G As above
Number of cleanliness compliance audits* 43 54 R 322 282 G 552 552 GLower in month due to staff restructure, however, still on track year to date.
Medicines management
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Number of adverse events due to administration errors* 0 1 G 0 10 G 18 18 G No commentary required
Number of controlled drug incidents* 6 3 R 21 26 G 48 48 G5 incidents have been resolved, and one incident continues to be investigated
* These items are reported in the quality accounts as well
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐
nil)
Year to date
Oct‐11 Full year
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐
nil)
Year to dateMeasure
Measure Oct‐11 Full year
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐
nil)
Measure Oct‐11 Year to date Full year
3

Intergrated Performance Report
Operational performance Overall rating (national) G Overall rating (other) A
Performance Pressures
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Incidents 1.6% 3.0% G 3.2% 3.0% A 3.0% 3.0% GAnnual growth was below plan for October, reflecting an improving trend
Calls 0.1% 3.0% G 0.9% 3.0% G 3.0% 3.0% G No commentary required
Hospital delays
‐ Handover improvement % vs PY ‐27.7% n/a n/a ‐27.3% n/a n/a 0.0% n/a n/a
Handover performance continues to be a concern. The Chairman has now written to all acutes and made personal contact with those which have greatest improvement opportunities. We are optimistic that this increased focus at Chair level will lead to more vigorous action further down.
‐ Clear‐up improvement % vs PY 68.6% n/a n/a 61.8% n/a n/a 60.0% n/a n/a No commentary required
‐ Turnaround improvement % vs PY ‐2.6% 30.0% R ‐6.3% 30.0% R 30.0% 30.0% GSee above. Clear up continues to improve but is being offset by worsening handover.
Perf (%) Perf (%) RAG Actual Plan RAG Forecast Plan RAG
Actual Plan
Red A8: on scene within 8 minutes (standard = 75%, plan = SCAS trajectory)
77.2% 77.7% A 78.5% 76.3% G 77.3% 77.3% GPerformance slightly below trajectory but above national standards. SeePCT section for detailed comments and action plans
Red A19: conveying response within 19 minutes(standard = 75%, plan = SCAS trajectory)
95.4% 95.8% A 96.2% 95.3% G 95.4% 95.4% GPerformance slightly below trajectory but above national standards. SeePCT section for detailed comments and action plans
Amber 20: response within 20 minutes 90.6% 90.0% G 93.0% 90.0% G 90.0% 90.0% G No commentary required
A Time to Treat ‐ 99th percentile 00:30:15 00:28:00 A 00:27:45 00:28:00 G 00:28:00 00:28:00 G
A Time to Treat ‐ 95th percentile 00:18:32 00:17:30 A 00:17:22 00:17:30 G 00:17:30 00:17:30 G
A Time to Treat ‐ 50th percentile 00:06:03 00:06:00 A 00:05:58 00:06:00 G 00:06:00 00:06:00 G
Performance Measure
Pressure Measure Oct‐11 Full yearYear to date
Year to date
Time to Respond ‐ front‐lineOct‐11
Lead Director: Ian Ferguson
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Full year
Increased volumes and reduced resources on the road have combined to push out time to treatment performance. An action plan has been developed but as
predicted this will remain a challenge in the current economic climate.
4

Intergrated Performance ReportTime to Respond ‐ EOC
Perf (%) Perf (%) RAG Actual Plan RAG Forecast Plan RAG
Actual Plan
Call connect to call answer in 5 sec (95%) 91.7% tba n/a 87.1% tba n/a tba tba n/a No commentary required
Call connect to call answer ‐ 99th percentile 00:01:40 00:01:17 R 00:01:29 00:01:27 A tba 00:01:22 n/a
This is a very disappointing result given that the new integrated telephony system went live in September and initially performance improved as expected. We are currently analysing what has gone wrong and a detailed action plan is being put together.
Call connect to call answer ‐ 95th percentile 00:00:29 00:00:19 R 00:00:25 00:00:28 G tba 00:00:23 n/a see above
Call connect to call answer ‐ 50th percentile 00:00:03 00:00:02 R 00:00:03 00:00:03 G tba 00:00:02 n/a see above
% calls abandoned n/a n/a n/a tba n/a n/a tba tba n/a No commentary required
Quality Control Measures
Perf (%) Perf (%) RAG Actual Plan RAG Forecast Plan RAG
Actual Plan
% non‐conveyance 42.2% 43.7% R 42.0% 43.7% R 43.7% 43.7% G
Non conveyance remains below the planned targets. There has been a small rise in October performance and this is being reviewed across all locality areas. The action plan for improvment is monitored through the executive team and BPPB
% calls with telephone advice only (Hear & Treat)
5.0% 5.0% G 5.5% 5.0% G tba 5.0% n/a No commentary required
% resolved without convey to Type 1/2 A&E (See & Treat)
39.0% tba n/a 38.6% tba n/a tba tba n/a No commentary required
% Hear & Treat re‐contacts in 24 hours 13.3% 13.5% G 14.6% 13.5% A tba 13.5% n/aThe hear and treat recontact rate has reduced this month and is below trajectory. However the YTD performacne is above plan. Work is ongoing to review trends and reasons for recontact.
% See & Treat re‐contacts in 24 hours 6.3% 5.0% G 6.1% 5.0% G tba 5.0% n/a No commentary required
% calls from patients at risk 1.36% n/a n/a 1.36% n/a n/a n/a n/a n/a No commentary required
Performance Measure Oct‐11 Year to date Full year
Performance Measure Oct‐11 Year to date Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
5

Intergrated Performance ReportA&E Performance by PCT and PCT Cluster
Perf (%) Perf (%) RAG Actual Plan RAG Forecast Plan RAG
Actual Plan
RED8
Berkshire Cluster 73.8% 78.4% R 77.2% 76.7% G 76.9% 77.5% A
Berkshire's performance has been poor during September and October. This was partly due to the EOC and Ops restructures which combined with sick absence of key managers to produce a leadership challenge. This has now been redressed and a detailed action plan is in place to tackle the underlying issues. As a result, performance in November has picked back up with Red 8 at 78% and Red 19 at 97.8%. While this is very encouraging, there are still a number of actions in hand to ensure that performance is maintained.
Berkshire East PCT 74.0% 81.6% R 77.3% 79.9% A 77.0% 79.2% A See above
Berkshire West PCT 73.6% 77.8% R 77.1% 75.9% G 76.7% 75.7% G See above
Hampshire Cluster 79.9% 77.1% G 80.3% 77.2% G 78.6% 76.4% G No commentary required
Hants PCT 77.0% 72.8% G 77.5% 73.1% G 75.6% 72.3% G No commentary required
Southampton City PCT 84.5% 82.2% G 83.3% 82.5% G 81.8% 81.8% G No commentary required
Portsmouth City PCT 83.9% 84.9% A 86.5% 85.2% G 85.2% 84.5% GAlthough slightly below trajectory, Portsmouth performance remains very strong
OxBucks Cluster 75.9% 78.2% A 77.0% 74.9% G 77.3% 75.7% G see comments on Bucks performance
Bucks PCT 66.0% 71.9% R 67.9% 68.4% R 68.2% 70.0% R
Bucks performance has not picked up again fully since iCAD went live. The new Area Manager is now in place and we have reviewed and refreshed the Bucks action plan. Details are available if required. There is now a major risk we will not hit 70% for the full year.
Milton Keynes PCT 85.7% 85.8% A 86.5% 82.4% G 86.0% 83.9% GMilton Keynes performance remains very strong despite being 0.1% below trajectory
Oxfordshire PCT 78.0% 77.9% G 79.1% 74.5% G 78.3% 76.3% G No commentary required
RED19
Berkshire Cluster 96.4% 97.0% A 97.1% 96.1% G 96.9% 96.7% G see comments on Berks performance above
Berkshire East PCT 96.7% 97.9% A 97.1% 97.1% G 96.9% 96.9% G see comments on Berks performance above
Berkshire West PCT 96.0% 97.4% A 97.1% 96.5% G 96.9% 96.5% G see comments on Berks performance above
Hampshire Cluster 94.9% 94.6% G 95.7% 94.7% G 95.0% 95.0% G No commentary required
Hants PCT 92.5% 93.0% R 94.0% 93.1% R 93.1% 95.0% R
We have revisited the action plan for Hants PCT Red 19 and are aiming to focus more resources in the area. A detailed plan is now in place. However, there is a major risk that we will not hit Red 19 target of 95% for Hants PCT for the full year.
Southampton City PCT 99.2% 97.2% G 98.6% 97.3% G 98.2% 97.3% G No commentary required
Portsmouth City PCT 97.7% 97.0% G 98.2% 97.1% G 98.1% 97.1% G No commentary required
OxBucks Cluster 95.4% 96.3% A 96.2% 95.1% G 95.8% 95.3% G See comments on Bucks performance
Bucks PCT 93.1% 96.3% R 94.3% 95.1% R 94.0% 95.1% R See comments on Bucks performance
Milton Keynes PCT 98.7% 98.9% A 99.0% 97.6% G 98.9% 98.1% GMilton Keynes performance remains very strong despite being 0.2% below trajectory
Oxfordshire PCT 95.4% 95.0% G 96.3% 93.8% G 95.7% 95.0% G No commentary required
Year to date Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Performance Measure Oct‐11
6

Intergrated Performance Report
Safety and Risk Management Overall rating G Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Patient Safety
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Number of IR1s 141 229 G 1390 1603 G 2744 2744 GMonthly figures are reducing, at this rate we will be below full year forcast.
Number of incidents reported to the NPSA (CQC/NPSA reportable)
20 15 G 132 105 G 180 180 A
Being above plan in this instance is a good thing as nationally it shows we are reporting more potential patient safety incidents. The NPSA look for an increase in reporting year on year
Number of incidents reported to the NPSA within 30 days (CQC/NPSA reportable)
20 20 G 98 105 G 180 180 GWe now report twice a month so should capture all incidents within the 30 day deadline
Number of Serious Untoward Incidents (SUI) reported (CQC/NPSA/SHA reportable)
1 2 G 10 14 G 24 24 GNo Comment Required
Number of SUI investigations outstanding after 60 days 1 1 G 3 3 G 4 4 GNo Comment Required
Number of Never Events (CQC/NPSA/SHA reportable)
0 0 G 0 0 G 0 0 GNo Comment Required
Clinical negligent claims (CNST) 0 1 G 3 7 G 12 12 G No Comment Required
Public liability claims 1 1 G 4 7 G 12 12 G No Comment Required
Long waits (RED 8)* 34 31 A 155 178 G 324 324 GLong waits rose in October compared to September pretty well across SCAS, reflecting higher demand and
Long waits (RED 19)* 83 86 G 409 589 G 979 979 G No Comment Required
Long waits (Amber)* 55 48 R 214 299 G 446 446 G See above
Staff Safety
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Number of RIDDOR reports (HSE reportable)
5 8 G 60 56 A 94 94 GReportable incident trends are reviewed by the Health & Safety Group where actions plans would be agreed if necessary
Number of Physical Assaults (NHS Protect reportable)
6 6 G 38 42 G 72 72 GNo Comment Required
Number of Non‐Physical Assaults (NHS Protect reportable)
13 16 G 104 112 G 192 192 G No Comment Required
Number of Security Incidents (NHS Protect reportable)
4 6 G 27 42 G 72 72 GNo Comment Required
* These items are reported in the quality accounts as well
Patient Safety Measure Oct‐11 Full yearYear to date
Lead Director: Fizz Thompson
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Staff Safety Measure Oct‐11 Year to date Full year
7
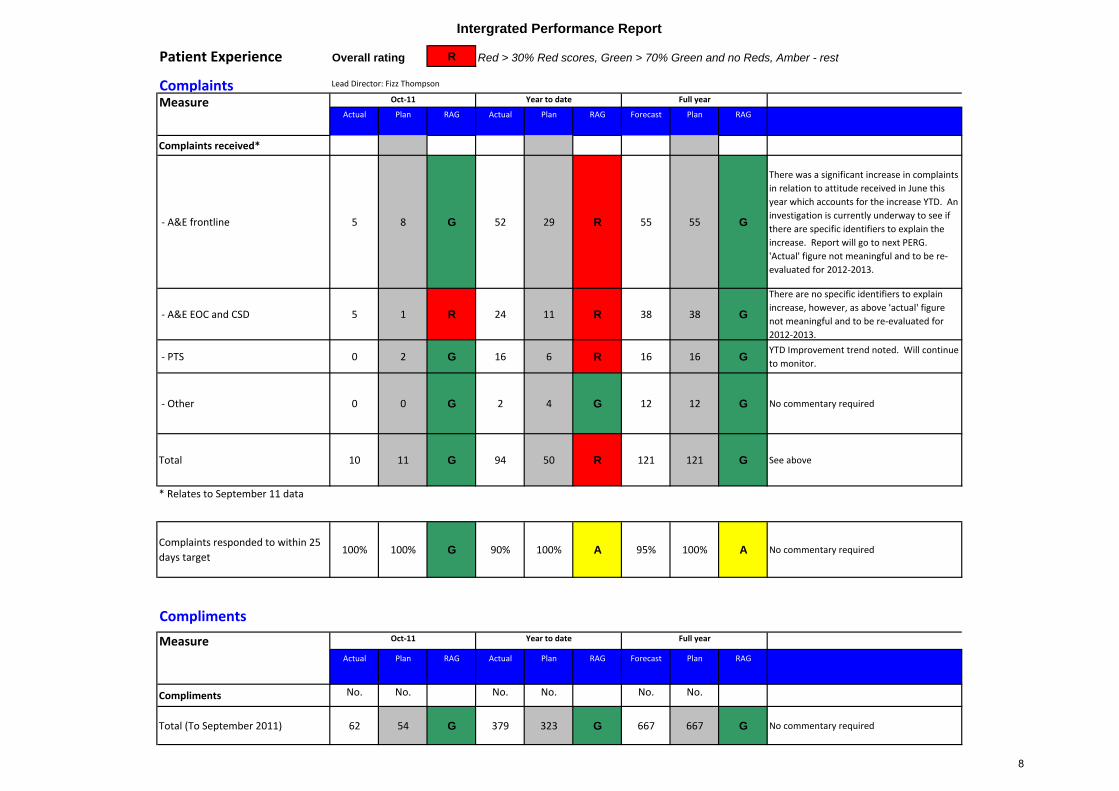
Intergrated Performance Report
Patient Experience Overall rating R Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Complaints
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Complaints received*
‐ A&E frontline 5 8 G 52 29 R 55 55 G
There was a significant increase in complaints in relation to attitude received in June this year which accounts for the increase YTD. An investigation is currently underway to see if there are specific identifiers to explain the increase. Report will go to next PERG. 'Actual' figure not meaningful and to be re‐evaluated for 2012‐2013.
‐ A&E EOC and CSD 5 1 R 24 11 R 38 38 G
There are no specific identifiers to explain increase, however, as above 'actual' figure not meaningful and to be re‐evaluated for 2012‐2013.
‐ PTS 0 2 G 16 6 R 16 16 GYTD Improvement trend noted. Will continue to monitor.
‐ Other 0 0 G 2 4 G 12 12 G No commentary required
Total 10 11 G 94 50 R 121 121 G See above
* Relates to September 11 data
Complaints responded to within 25 days target
100% 100% G 90% 100% A 95% 100% A No commentary required
Compliments
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Compliments No. No. No. No. No. No.
Total (To September 2011) 62 54 G 379 323 G 667 667 G No commentary required
Lead Director: Fizz Thompson
Full year
Measure Oct‐11 Year to date
Measure Oct‐11 Year to date
Full year
8
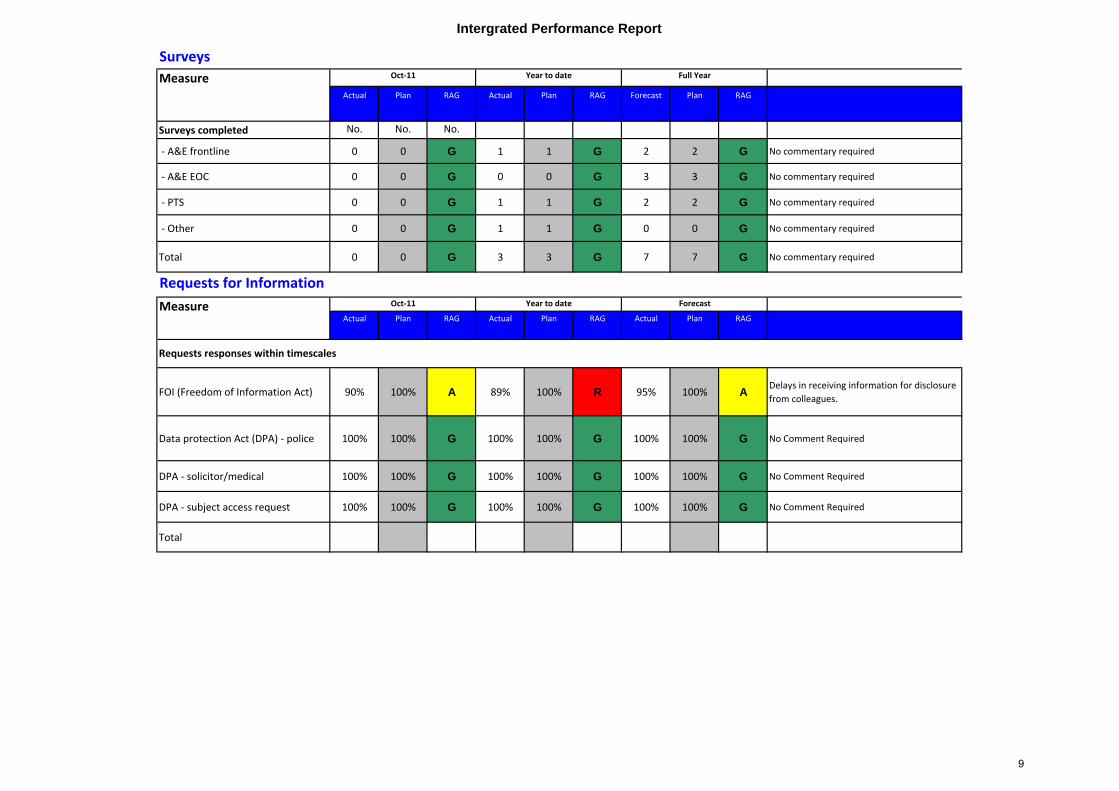
Intergrated Performance Report
Surveys
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Surveys completed No. No. No.
‐ A&E frontline 0 0 G 1 1 G 2 2 G No commentary required
‐ A&E EOC 0 0 G 0 0 G 3 3 G No commentary required
‐ PTS 0 0 G 1 1 G 2 2 G No commentary required
‐ Other 0 0 G 1 1 G 0 0 G No commentary required
Total 0 0 G 3 3 G 7 7 G No commentary required
Actual Plan RAG Actual Plan RAG Actual Plan RAG
FOI (Freedom of Information Act) 90% 100% A 89% 100% R 95% 100% ADelays in receiving information for disclosure from colleagues.
Data protection Act (DPA) ‐ police 100% 100% G 100% 100% G 100% 100% G No Comment Required
DPA ‐ solicitor/medical 100% 100% G 100% 100% G 100% 100% G No Comment Required
DPA ‐ subject access request 100% 100% G 100% 100% G 100% 100% G No Comment Required
Total
Requests responses within timescales
Requests for Information
Measure Oct‐11
Measure Oct‐11 Year to date Forecast
Year to date Full Year
9

Intergrated Performance ReportFinance Finance rating A QIPP rating R
Financial Measures
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Surplus (£k) 111 88 G 1226 1495 R 2050 2050 GRecovery plan in place to rectify this position and budget gap closed by 8% this month.
Financial Risk Rating 3 3 G 3 3 G 3 3 G No comment required
Liquidity ratio n/a n/a n/a 1 1 G 3 3 G No comment required
Return on Assets (ROA) 5% 5.0% G 6% 6.0% G 6% 6.0% G No comment required
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Unplanned EBITDA variance for 2 Q's No No G No No G No No GNo commentary required
FRR forecast variance < 3 No No G No No G No No G No commentary required
FRR 2 in any quarter No No G No No G No No G No commentary required
Overdraft used last quarter No No G No No G No No G No commentary required
Debtors > 90 days> 5% total balance Yes No R Yes No R No No GContinued improvement down to £271k ‐ see Finance Reoprt for further details on actions being progressed
Creditors > 90 days> 5% total balance No No G No No G No No G No commentary required
2 or more change FD in last 12m No No G No No G No No GNo commentary required
Interim FD > one quarter No No G No No G No No GNo commentary required
Q end cash<10 days of op expenses or <£4m
No No G No No G No No GNo commentary required
Capex<75% of ytd plan Yes No R Yes No R No No GLower capex as part of plan to mitigate the potential delay in the Battle disposal.
Full year
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Measure Oct‐11 Year to date Full year
Lead Director: Charles Porter
Monitor Forward Financial Risk Ratings
Measure Oct‐11 Year to date Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
10

Intergrated Performance Report
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
£k £k £k £k £k £k
Total CIP's 830 677 G 3,309 2,788 G 6,369 6,365 GOverall on target
Dual ECA 11 106 R 75 250 R 266 779 R
All divisions are behind plan for the period. Dual ECA private providers to increase savings from November, which will recover some of the CIP but still expected to fall behind plan
TARP 6 67 R 6 67 R 86 400 RThe unsocial hours part of this project has been removed as no savings are now expected by reviewing our unsocial hours payments
Sickness reduction 0 46 R 0 130 R 259 417 R
Savings are not yet being achieved, however the module roll out has been completed. Delays are now due to the Ops restructure and the related line management changes.
Hospital delays 20 30 R 108 152 R 222 286 A
Delays are above the targeted 15% under 15 minutes delay in all divisions. Ops directors to review using Qlikview with area managers to improve
Ops/clinical restructuring 0 58 R 0 58 R 237 351 R This CIP has reduced further this month as the admin posts are now band 4, not band 3. Additional resource
EOC restructuring 47 52 A 75 52 G 311 310 G Phasing difference in the month but ahead cumulatively
PP replacement 0 19 R 44 75 R 193 187 GRecruitment behind plan YTD, however expected to catch up later in the year.
Consumables 47 27 G 234 190 G 337 325 G No commentary required
Ops efficiency 40 11 G 106 44 G 345 100 G No commentary required
Non-conveyance improvement 0 0 G 0 0 G 138 0 G No commentary required
CSD 387 67 G 1,380 469 G 1,871 804 G No commentary required
Commercial division 29 89 R 129 624 R 271 1,069 R See Commercial tab
Overheads savings 74 59 G 672 324 G 1,137 600 G No commentary required
Project management saving 17 17 G 149 149 G 200 200 G No commentary required
Project cost saving 27 ‐9 G ‐68 ‐64 A 43 94 RReduction in CAD, TARP and other expected projects have caused this project to fall behind expectations
Telephony saving 103 3 G 241 156 G 431 168 GNew telephony contract due to be signed end of October, additional savings expected following implementation
Fleet savings 11 11 G 78 78 G 163 163 G No commentary required
Property savings 0 2 R 5 7 A 11 35 RSavings are now expected to be lower due to the delay in closing Deanshanger and the delay in sale of Battle
Corporate savings 12 22 R 74 27 G 150 78 G In line YTD and expected to achieve planned savings
Contingency n/a n/a ‐300 n/a No commentary required
Measure Oct‐11 Year to date Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Cost Improvement Plans (QIPP's)
11

Intergrated Performance Report
Commercial Division Overall rating R Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Savings vs Prior Year
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
£k £k £k £k £k £k
Total Commercial Division 29 144 R 129 290 R 271 1,180 R
Steady performance v p5 revised plan. It is expected for PTS Hants to pick up and for PTS Berks to continue improvements. There are concerns PTS Ox Bucks will not maintain levels
PTS Hants (25) 16 R (145) 5 R (163) 96 R
Contractual income further down but increased ECR activity, however pay & overtime remain a concern due to dedicated resource requirements in contract.
PTS Berks 39 46 A 30 142 R 50 403 RIncrease in ECR income on track, cost reduction measures now slowly showing traction; however overtime still a concern.
PTS Ox/Bucks 22 58 R 236 242 A 323 585 R
Revised rotas now in place but effect on overtime and private provider usage not yet visible. New staff started which will increase pay costs and new vehicle/equipment lease costs a concern
OOH ‐ Berks 11 8 G 21 36 R 30 82 RAlternative plan as agreed with EBPC to bring plan back on track starting to show in month.
OOH ‐ Oxfordshire 11 4 G 32 12 G 87 36 G Plan is on track
Logistics ‐ Berks (18) 7 R (76) (4) R (136) 38 RNegative result due to additional management resource charged to Comm Div.
Logistics ‐ Ox/Bucks 0 9 R 45 62 R 129 106 G
Difficult month due to sickness absence and additional agency spend. Staff and contractual situation now resolved and additional income secured. Should get back on track next month
Equipment Services (13) 33 R 12 182 R 133 357 RContract now out to tender. Income situation has been escalated with Slough Borough Council and closure expected next month
Training (12) 7 R (82) 36 R (103) 91 RDrop in expected uptake this month due to resource constraints; increase expected for November.
Events Management 1 0 G 25 4 G 26 4 G No comment required
Pay inflation in budget 28 n/a 193 n/a 330 n/a No comment required
Contingency 0 n/a 0 n/a (244) n/a No comment required
Project costs/Pay costs (14) (43) G (162) (426) G (190) (619) G No comment required
Lead Director: Paul Clarke
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Measure Oct‐11 Year to date Full year
12

Intergrated Performance Report
Savings ‐ milestones
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
£k £k £k £k £k £k
Total Commercial Division
PTS Hants ‐ contract maximisationNot
realisedDue R
Not realised
Due R No Yes R
Additional ECR income from SUHT continues; however, WEHCT now scrutinising contract activity heavily through managed service provider Coperforma making auto planning difficult
PTS Berks ‐ change to lease vehicles Realised Realised G Realised Realised G Yes Yes GDone, entire fleet now leased, however, higher then expected fleet cost allocations still appear under operational overheads
PTS Berks ‐ improve staff rosteringNot
realisedDue R
Not realised
Due R Yes Yes GCost reductions now showing traction. Autoplan now rolled out.
PTS Ox/Bucks ‐ improve staff rosteringNot
realisedDue R
Not realised
Due R Yes Yes G Model rotas started 7th November.
OOH Berks ‐ contract renegotiationNot
realisedDue R
Not realised
Due R Yes Yes GAgreed additional income lower than anticipated; however, costs now better managed. 111 will be main factor for continuation (if any) for 12/13
OOH Ox‐ improve rostering Realised Realised G Realised Realised G Yes Yes G New rosters in place showing effect
Logistics Berks ‐ vehicle utilisationNot
realisedDue R
Not realised
Due R No Yes RIt is expected that further utilisation improvementswithin existing routes will be minimal
Logistics Ox/Bucks ‐ additional income Realised Realised G Realised Realised G Yes Yes GAdditional income secured through additional Berks/Ox route
Equipment Services ‐ contract changesNot
realisedDue R
Not realised
Due R Yes Yes G Now escalated to Exec level within SBC
Training ‐ business developmentIncome behind budget
Due RIncome behind budget
Due R No Yes RIncome situation reflected in changes to the market. Only slight improvements expected
Oct‐11 Year to date Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Measure
13

Intergrated Performance Report
Human Resources Overall rating A Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Sickness/absence
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
% % % % %
Trust 5.6% 5.0% R 5.2% 5.0% A 5.0% 5.0% G
Sickness module of Kronos has now been implemented and managers have been trained. The focus is now on using this tool to help manage sickness.
‐ A&E Operations 6.4% 5.0% R 5.7% 5.0% R 5.0% 5.0% G As above
‐ A&E EOC 5.1% 5.0% A 5.7% 5.0% R 5.0% 5.0% G As above
‐ PTS 3.3% 5.0% G 6.0% 5.0% R 5.5% 5.0% APlan by area is being developed for the Commercial Division and 26 staff are on the sickness management programme.
‐ Other Commercial Division 5.3% 5.0% A 3.5% 5.0% G 3.5% 5.0% G As above
‐ Other 2.7% 5.0% G 2.3% 5.0% G 2.5% 5.0% G Not required
Appraisals
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
% % % % %
Trust 94.0% 95.0% A 94.0% 95.0% A 95.0% 95.0% GThe biggest concern is the stock‐piling of appraisals in Nov‐Jan and March in Operations, 95% will be achieved through a concerted effort by the Trust.
‐ A&E Operations 96.0% 95.0% G 96.0% 95.0% G 95.0% 95.0% G As above
‐ A&E EOC 84.0% 95.0% R 84.0% 95.0% R 95.0% 95.0% G As above
‐ PTS 96.0% 95.0% G 96.0% 95.0% G 95.0% 95.0% G As above
‐ Other Commercial Division 95.0% 95.0% G 95.0% 95.0% G 95.0% 95.0% G As above
‐ Other 90.0% 95.0% A 90.0% 95.0% A 95.0% 95.0% G As above
Measure Oct‐11 Year to date Full year
Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Lead Director: Will Hancock
Measure‐ Data refers to previous month (September 2011)
Oct‐11 Year to date
14

Intergrated Performance Report
Recruitment
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Front‐line recruitment 30 32 A 121 132 A 196 196 GAdditional ECA course planned in order to bring numbers in on traget for end of year
CSD recruitment 0 n/a n/a 11 11 G 20 20 G Recruitment on‐going ‐ no monthly plan
PTS recruitment 15 n/a n/a 22 22 G 30 30 G Recruitment on‐going ‐ no monthly plan
Training
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
Statutory & Mandatory 97.0% 95.0% G 99.0% 95.0% G 95.0% 95.0% GStaff originally ineligible through LTS, Career break etc will need additional training
Clinical Development 1 93.0% 90.0% G 93.0% 90.0% G 95.0% 95.0% GOn‐Track. Attendance on courses needs to be increased to make up difference if we are to achieve 95%.
Conflict Resolution 80.0% 80.0% G 70.0% 80.0% R TBA TBA n/aCourses planned for delivery from June 2011 onwards. Predicted finish date September 2011
Clinical Development 2 N/A N/A n/a N/A N/A n/a N/A N/A n/a This programme does not commence until Sept 2011
Trauma Training tba tba n/a tba tba n/a tba tba n/a To be Confirmed
Corporate Induction N/A N/A n/a N/A N/A n/a N/A N/A n/aLegacy data not available in ESR, to be resolved. Expected to report in October 2011
Equality & Diversity
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
E&D patient information 65.4% 85.0% R 64.0% 85.0% R 85.0% 85.0% GPlan is in place 50 booked in, 19 trained so far.
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Full year
Measure Oct‐11 Full year
Measure Oct‐11 Year to date Full year Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐ nil)
Measure Oct‐11 Year to date
Year to date
15

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
CNew EOC structure approved
C
Business case for further CSD expansion approved
CICAD user training completed
CICAD rolled out in O&B
C
Fully implemented new EOC structure completed
G
£52k saved per month following EOC restructure (ongoing)
0 0 GICAD project closed
A
6.7% 999 calls closed on telephone following clinical assessment by CSD Practitioner
c
2010-11 CSD expansion complete, £67k CIP per month
C
Project definition document agreed for development of hubs including 111 service
0 0 C
ICAD incoming patient handover screen go live OxBucks
0
?% 999 calls answered within 5 seconds
0 0 G
95% 999 calls answered within 5 seconds
G
111 calls being received and appropriately handled by SCAS
G
£564k CIPs delivered in 2011-12 (310k EOC, 254k CSD)
A
CSD business case revisited with further information about NHS Pathways
G
Benefits and risks of NHS Pathways triage tool for 999 calls appraised (subject to national guidance)
Ian Ferguson
Rob Ellery 15.11.11
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
Clinical healthcare hubs
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
16

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
0 0 C
Trauma project scope, brief and milestones agreed
C
Approval secured for single regional TIA referral form
C
Stroke pathway and policies agreed
CLocation of Trauma CSD agreed
C
Trauma - clinical training content agreed for EOC and Ambulance staff
C
Staff recruited and trained to work on Trauma Desk
A
Front line staff trained on trauma triage tool
0 0 C
PPCI action plan agreed for Ox & Bucks
G
Reporting and audit processes agreed for trauma
GTrauma triage tool implemented
C
Any adaptions to service delivery model implemented as required for new indicators
C
Measurement system in place for all new indicators (except call answering, recontact and survival to discharge)
C
Outline plans agreed for stakeholder engagement event on new indicators
0
Stakeholder workshop held on new indicators
C
Survival to discharge following cardiac arrest data available and analysed
C
Stakeholder meetings held (if agreement to proceed with this)
Stakeholder workshop held
C
Improvement plan prepared to address any underperformance against national indicators
C
Improvement plan against new indicators agreed by Exec Team, ready for submission to DH
R
Scorecard revised to incorporate all new indicators (including clinical outcomes)
C
Detailed plans agreed for stakeholder engagement event on new indicators
C
Improvement plan agreed for any indicators where SCAS performance below average
0
Commissioners provided technical guidance on measurement of local indicators
John BlackDave Sherwood
15.11.11
Improving outcomes
Isobel WroeIan Ferguson
30.10.11
17

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
C
KRONOS absence management module implemented
C
Report received from Optima on deployment model and analysis
C
Changes agreed following Optima analysis
C
Agreed changes implemented on basis of Optima analysis
C
KRONOS training for managers completed on sickness absence module
A
0.5% improvement achieved in control, A&E mgrs, frontline staff and ECP sickness
A
Expanding to dual ECA 2300 weekly hours of "released" paramedics in Hampshire division
G
Modelling tool provider selected and contract awarded
A
0.5% improvement achieved in PTS sickness
R
£286k CIPs delivered through reduced delays at hospitals
R
476 hours per week of dual ECA crew introduced in Hampshire
C
Automatic sickness alerts in place for managers
0 0 C
KRONOS absence management module fully implemented and system in use by managers
G
Implementing 494 weekly hours of dual ECAs "released" paramedics in O&B division
A
£779k CIPs delivered through expansion of dual ECA scheme
C
Tenders received for modelling package
G
Expanding to 228 weekly hours of dual ECAs "released" paramedics in Berkshire division
G
£187k CIPs delivered through replacement of privates with staff
G
Private providers reduced in Hampshire
A
£417k CIPs delivered through improved sickness management
5.10.11Ian Ferguson
Andy JonesA&E efficiency
18

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
C
Heads of Terms signed, providing context and priorities for this workstream
C
workstream objectives aligned with Heads of Terms and local contexts
C
clear set of activities and benefit measures agreed internally
CRecovery Plan agreed by BPPB
C
All resource centres in Oxon and MK visited to discuss management of urgent care patients
A
Map and review alternative care pathways and services available
G
AACP (care plan) process implemented across SCAS
G
80% of patients who meet criteria referred to local fall team
G
40% of Level 3 callers have AACP in place
G
Increased use of CSD by crews to identify alternative services available
Fizz Thompson
Tehmeena Ajmal
17.10.11
C
develop programme of activity to deliver measureable and quantifiable benefits
G
Resources agreed to support face to face engagement with front line staff
G
Decision support tools developed for top 20 clinical presentations
R
Information made available on alternative care pathways and services available
GIntroduce GP Referral into Bucks
A
25% of Level 2 callers have AACP in place in Hampshire and Oxfordshire
G
Mental health pathways in place and accessible
0 0 R
Reporting and data issues addressed and "single source of truth" agreed
G
Decision support tools made available to SCAS clinicians
A
resource centres across SCAS visited to discuss management of urgent care patients
G
Number of level 3 patients reduced
G
Peer review process established (5 PCR per quarter per clinician)
C
Review of ECP rota in MK completed
G
Mechanism in place for crews to identify patient who would benefit from AACP
G
Feedback process in place and in use for outcomes of good conveying decisions
RRelaunch GP Referral in MK and Oxon
G
GP Triage rolled out in Buckinghamshire
G
Enhanced GP Triage rolled out across SCAS (except Bucks)
Pathways of care
19

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
G
Mechanism for identifying NHS number in place and in use
Fizz Thompson
Tehmeena Ajmal
17.10.11
G
Patient contact and clinical records automatically reported to relevant GP
A
conveyance rates to type 1&2 decreased to level required in contract
Pathways of care (continued)
20

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
0 C
Evaluation report prepared on ECP pilot
0
Unsocial payment issues assessed and quantified
0 0 0 0 0
Consultation on unsocial hours completed
CTraining plan agreed
C
Ops meal break milestones agreed
0 0 0
0 0 0 0 C
Appraisal improvement plan and timetable set
0 0 R
Appraisal improvements implemented
0 0 G
7 Habits and possible e-appraisal system to be considered. Implementation to be agreed at WFDB on 7 Nov
0 0 0 0 0 0 G
Review feedback from 2011 Staff Survey to assess effectiveness of changes
CMilestones agreed for Qlickview
G
User group permissions set up for access to specific data
G
Trend analysis reports enhanced
R
Date for Kronos data to be introduced
RESR data introduced
RProactis data introduced
GUser manual published - Complete
GICAD O&B data introduced
RWall Board rolled out
C
National quality indicators reported
RSentinel data introduced
RUser workshops completed
RSLA Scorecard in place
5.10.11InformationCharles Porter
James Brannan
Workforce Development
21

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
CInternational calls barred in SH
C
Further telephony savings identified
A
Winchester AS and Eastleigh completed
CTelephony savings delivered
0Battle AS exchanged
0Battle AS completed
AEstates CIPs rise to £8k pm
G£168k telephony CIP delivered
C
Winchester AS and Eastleigh exchanged
ACorporate review plans agreed
A
£17k pm estates savings achieved
RBattle AS exchanged
G
£600k CIP delivered through savings on indirect costs
C
Board approval secured for change in fleet policy
A
Corporate review consultation commenced
G
£78k CIP delivered through review of corporate overheads
C
£11k pm fleet CIP achieved through purchase of 20 vehicles to depreciate over 10 years
G
£200k CIP delivered through reduction in TE staffing
C
£27k pm saved through increased awareness of consumable usage
A
£93k CIP delivered through reduction in external project costs
RBattle AS completed
A
£644k cash released from Berkshire for reinvestment in front-line
Daphne Thomas / Alan Monks
23.9.11Cost improvementCharles Porter
22

Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
C
Consssultation on proposed structure starts
C
Consutlation on propsoed structure ends
C
Feedback period on revised proposal ends
C
Staff appointments process starts
C
Staff appointments process continues
CStaff appointments process ends
C
Staff SAE and/or redundancy process take place
ABenefits begin to be realised
GMajority of training completed
C
Revised proposal published for feedback
CAppointments process agreed
C
90% of affected staff are appointed to a post by 01/11/11
CLaunch event takes place
A
Resilience On Call Rota Revised
CTrust Board signs off final proposal
A
Project Board Approval of Ops Restructure Outcomes
A
£351k CIP delivered through restructure
A
Investigations Unit functioning with interim process in place
GSupport Services Desk is live
AResilience On Call Rota Revised
A
New Adverse Incident and Investigations Policy agreed
A
Configuration of Qlikview to allow reporting by new areas
0 0
15.11.11RestructureIan Ferguson
David Perrett
23
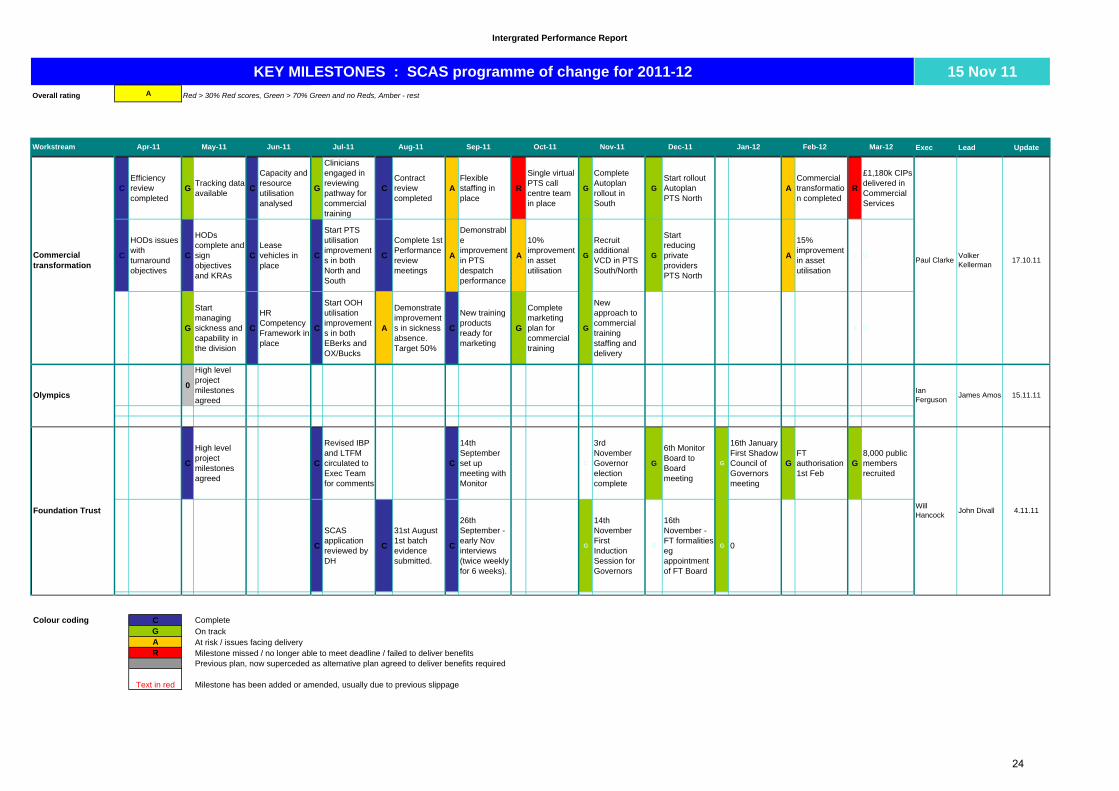
Intergrated Performance Report
Overall rating Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Exec Lead Update
15 Nov 11KEY MILESTONES : SCAS programme of change for 2011-12
Jan-12Nov-11 Mar-12Oct-11 Feb-12Dec-11Workstream
A
Sep-11May-11 Jun-11 Jul-11 Aug-11Apr-11
CEfficiency review completed
GTracking data available
C
Capacity and resource utilisation analysed
G
Clinicians engaged in reviewing pathway for commercial training
CContract review completed
AFlexible staffing in place
R
Single virtual PTS call centre team in place
G
Complete Autoplan rollout in South
GStart rollout Autoplan PTS North
ACommercial transformation completed
R
£1,180k CIPs delivered in Commercial Services
C
HODs issues with turnaround objectives
C
HODs complete and sign objectives and KRAs
CLease vehicles in place
C
Start PTS utilisation improvements in both North and South
C
Complete 1st Performance review meetings
A
Demonstrable improvement in PTS despatch performance
A
10% improvement in asset utilisation
G
Recruit additional VCD in PTS South/North
G
Start reducing private providers PTS North
A
15% improvement in asset utilisation
0 0
G
Start managing sickness and capability in the division
C
HR Competency Framework in place
C
Start OOH utilisation improvements in both EBerks and OX/Bucks
A
Demonstrate improvements in sickness absence. Target 50%
C
New training products ready for marketing
G
Complete marketing plan for commercial training
G
New approach to commercial training staffing and delivery
0 0
0
High level project milestones agreed
C
High level project milestones agreed
C
Revised IBP and LTFM circulated to Exec Team for comments
C
14th September set up meeting with Monitor
C
3rd November Governor election complete
G
6th Monitor Board to Board meeting
G
16th January First Shadow Council of Governors meeting
GFT authorisation 1st Feb
G8,000 public members recruited
C
SCAS application reviewed by DH
C
31st August 1st batch evidence submitted.
C
26th September - early Nov interviews (twice weekly for 6 weeks).
G
14th November First Induction Session for Governors
0
16th November - FT formalities eg appointment of FT Board
G 0
0
Colour coding C CompleteG On trackA At risk / issues facing deliveryR Milestone missed / no longer able to meet deadline / failed to deliver benefits
Previous plan, now superceded as alternative plan agreed to deliver benefits required
Text in red Milestone has been added or amended, usually due to previous slippage
Ian Ferguson
James Amos 15.11.11
Commercial transformation
Paul ClarkeVolker Kellerman
4.11.11Foundation TrustWill Hancock
John Divall
17.10.11
Olympics
24

Intergrated Performance Report
FT Membership Overall rating A Red > 30% Red scores, Green > 70% Green and no Reds, Amber - rest
Public membership
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
No. No. No. No. No. No.
Public 398 250 G 7,417 7,250 G 8,000 8,000 GEvents have been scheduled for the remainder of the year
Representation
‐ Age (no. of people in under‐represented categories) n/a n/a n/a n/a n/a n/a n/a n/a n/a Not required
‐ Gender (no. of people in under‐represented categories)
100 100 G 3,133 3,100 G 4,000 4,000 G Males are currently under‐represented
‐ Ethnicity (no. underpresented categories) Ethnicity
White ‐ Irish n/a n/a n/a 86 80 G 84 84 G Not required
White ‐ Any other White background n/a n/a n/a 212 210 G 226 226 G Not requiredMixed ‐ White and Black Caribbean n/a n/a n/a 33 29 G 29 29 G Not required
Mixed ‐ White and Black African n/a n/a n/a 15 8 G 8 8 G Not required
Mixed ‐ White and Asian n/a n/a n/a 35 28 G 28 28 G Not required
Mixed ‐ Any other mixed background n/a n/a n/a 32 25 G 25 25 G Not required
Asian or Asian British ‐ Indian n/a n/a n/a 89 89 G 108 108 G Not required
Asian or Asian British ‐ Pakistani n/a n/a n/a 51 60 R 100 100 G Focus will be on targeting this group
Asian or Asian British ‐ Bangladeshi n/a n/a n/a 16 16 G 17 17 G Not required
Asian or Asian British ‐ Any other Asian background n/a n/a n/a 44 23 G 23 23 G Not required
Black or Black British ‐ Caribbean n/a n/a n/a 31 31 G 42 42 G Not required
Black or Black British ‐ African n/a n/a n/a 95 28 G 28 28 G Not required
Black or Black British ‐ Any other Black background n/a n/a n/a 18 7 G 7 7 G Not required
Other Ethnic Groups ‐ Chinese n/a n/a n/a 27 27 G 37 37 G Not required
Other Ethnic Groups ‐ Any other ethnic group n/a n/a n/a 24 24 G 30 30 G Not required
‐ Socio‐economic (no. underpresented categories)
Urban Prosperity [2] n/a n/a n/a 673 670 G 797 797 G Not required
Moderate Means [4] n/a n/a n/a 838 830 G 960 960 G Not required
‐ Geography
Hampshire 91 275 R 2,134 2,350 A 3,200 3,200 G More events have been planned in Hants
Oxfordshire 24 25 A 1,573 1,350 G 1,600 1,600 GMore events have been planned in Oxon for next month
Buckinghamshire 60 50 G 1,916 1,375 G 1,600 1,600 G Not required
Berkshire 240 75 G 1,791 1,400 G 1,600 1,600 G Not required
Staff membership
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
No. No. No. No. No. No.
Staff membership n/a n/a n/a 2,407 2,400 G 2,431 2,431 G Not required
Staff opt‐outs n/a n/a n/a 15 15 G 15 15 G Not required
Governors
Actual Plan RAG Actual Plan RAG Forecast Plan RAG
No. No. No. No. No. No.
Governor nominations 37 35 G 311 300 G 300 300 G No comment required
Aspirant governors attended workshop 33 25 G 33 25 G n/a n/a n/a No comment required
Governors elected 0 0 G 0 0 G 20 20 G Governor figures available next month.
Governors attended gov't induction 0 0 G 0 0 G 20 20 G Governor figures available next month.
Please note: 90.3% of the population within SCAS area is White British
Commentary on exceptions (Red ‐ action to correct, Amber ‐ action to reduce risk, Green ‐
nil)
Measure
Lead Director: Duncan Burke
Oct‐11 Year to date Full year
Measure Oct‐11 Year to date Full year
Measure Oct‐11 Year to date Full year
25

Enclosure: J (Agenda Item: 12)
Board Report
Title Finance & Estates Report for the month ended 31 October 2011
Lead Director Charles Porter
Report Author Daphne Thomas
Purpose of the report To update the Board on the financial results of the Trust for the first half of the financial year.
Recommendation (eg. Note, approve, endorse)
The Board is asked to note the financial results and the full year forecast.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
Outcome 16
Details of additional risks associated with this paper:
QIPP programme for 11/12 in particular the Commercial Division turnaround programme. Variable activity income in the 2011/12 E&U contract
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
All areas of patient rights
Financial implications/impact See paper
Legal implications/impact None identified
1

Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
None identified
Other
Committees/groups where this item has been presented before
None
Other options available and their pros and cons
N/A
Progress monitoring and review Executive Committee
Background papers Annual Plan 2011/12
A. Executive Summary
Actual Budget Variance Actual Budget Variance Forecast Budget Prior Year Variance to budget
Variance to Prior
YearProfitability
SCAS Income £k 11,534 11,395 140 80,120 79,656 464 137,315 136,628 137,941 687 (626)
(508) (218)
-1% 0%
(21) (1,058)
SCAS Contribution £k 2,834 2,790 44 19,326 19,834 33,887 34,104 31,860 2,026
% Contribution % 25% 24% 0% 24% 25% 25% 25% 23% 2%
Corporate overheads £k 2,723 2,702 18,100 18,339 239 31,837 32,054 30,469 218
EBITDA £k 859 838 21 6,438 6,445 10,787 10,753 10,385 34 402EBITDA % % 7% 7% 8% 8% 8% 8% 8%
Overall Surplus £k 111 88 23 1,226 1,495 2,050 2,050 1,306 659
% Surplus % 1% 1% 0% 2% 2% 1% 2% 0.9% 1%
Memo: tech'l acc'ting surplus (£k) 111 88 23 1,226 1,495 1,447 2,050 177 1,270
Month Year to date Full Year
(8)
(269) (0)
0% 0%
(269) (603) The results for the month show a surplus of £111k which is favourable to budget and reduces the year to date budget gap from £292k last month to £269k. The contribution in the month from A&E is similar to last month £2.7m but the Commercial Division is lower by £65k due to higher costs as a result of benefits in the previous month (rent credit and lease credit) and additional turnaround support costs now being full charged against this division (key account managers). Overall the Commercial Division out-turn is £15k worse than estimated in last month’s forecast. Corporate overheads are within 1% of budget and remain underspent year to date by £0.65m before the contingency and property disposal effects. The forecast remains in line with budget and materially unchanged from last month. A detailed review was undertaken as part of our half year review process which confirmed our understanding of the full year forecast. Compared to last month’s forecast Commercial Division is largely unchanged (£10k improvement), an improvement of £100k in A&E (income), and central costs are £16k lower before contingency. These movements have facilitated the increased of the central contingency by £126k with £510k of this unallocated.
2

Actual Budget Variance Actual Budget Variance Forecast Budget Prior Year Variance to budget
Variance to Prior
Year
Cash and capital position
EBITDA £k 859 838 21 6,438 6,445 (8)(96) (3,431)
(249)(3,343)
(21) (41)(18) (29)
(4) (4) 0
10,787 10,753 10,385 34 402Working capital mov't £k 413 (434) 847 (1,262) (1,704) 442 (1,166) (1,070) 2,265Capital Expenditure £k (560) (311) (1,583) (3,188) 1,605 (5,260) (6,970) (7,630) 1,710 2,370Disposals £k 0 0 0 188 180 8 1,508 4,851 39 1,469PDC paid £k 0 0 0 (950) (929) (1,900) (1,859) (1,957) 57Interest £k 2 (1) 3 (96) (78) (205) (176) (254) 49Repayments of loans £k (4) 0 (721) (717) (1,435) (1,435) (1,436) 1Other £k 1 0 1 0 0 (3) 1 (26) 23PDC & DOH Loans £k 0 0 0 0 0 0 0 123Cashflow £k 711 92 619 2,014 9 2,004 2,326 4,095 1,509 817
Cash balance £k 6,991 4,925 2,066 6,991 4,925 2,066 7,303 9,011 4,977 2,326
Liquidity ratio 1.0 3.0
Month Year to date Full Year
(4)0 0 (123)
(1,769)
(1,708)
The Trust’s cash balance at the end of October was £7m, which was higher than the September balance (£6.3m) and better than the planned budget (£4.9m) and higher than the forecast in September (5.5m). The net cash inflow was due to higher than expected cash receipts for quarter one/quarter 2 A&E activity money and other receipts relating to non A&E service level agreements. Capital expenditure remains below budget and the forecast has been further reduced by the Trust’s decision to lease 6 front line ambulances that were originally included within the capital budget. Thus the year end capital forecast has been reduced to £4.9m from £5.2m with a commensurate increase in the year end cash forecast from £7m to £7.3m.
Actual Budget Variance Actual Budget Variance Forecast Budget Prior Year Variance to budget
Variance to Prior
Year
FT Financial ratings
ROA % 5% 5% 0% 6% 6% 0% 6% 6% 4% 0% 1%
Overall Score 3.0 3.0 0.0 3.4 3.0 2.9 0.4 0.5
Month Year to date Full Year
Return on Assets is in line with budget overall and with Monitor requirements.
3

B. Supporting Information FINANCIAL REPORT – DETAILED REVIEW Income The variances to budget can be analysed in further detail as follows:
Month Year to date Comments£k £k
Fav/ (adv) Fav/ (adv)
Budget income 11,395 79,656A&E activity increase (57)
(65) (270)
(13) (90)
(45)
70
A&E non-conveyance
A&E delays 99 292
A&E clinincal incentive 0 0
A&E other
Commercial division 54 43
Training monies from NESC 60
Miscellaneous 61 464
Actual income 11,534 80,120
Higher in the month due to events and higher RTA recoveries. Higher year to date due to insurnace redunds, stroke training and RTA recoveries
Lower number of students in education year to date but additional revenues in the second half from new funding
Volumes up 3.2% year to date and 1.6% in the month
Higher due to high handover delays - this has reached the contract cap of £700k this month
Offsetting variances - main items are higher ECR's in PTS (£70k positive) offset by lower training income
One-offs in previous months
Assumes 100% achievement of plan
Non-conveyance income tracking below plan conveyances to A&E not reducing compared to last year
Overall income is better than budget with a number of compensating variances are set out above. The continued adverse variance on the non-conveyance incentive is a risk to the year end forecast and is subject to a number of initiatives to bring this back on track. The year end forecast for income remains similar to last month £137.3m versus £137.2m last month: the principal risks within this are analysed in the Risks section below. Operational and clinical performance against national targets was extremely good and is further reported on in the Integrated Performance Report. Expenditure The principal expenditure variances can be analysed as follows:
4
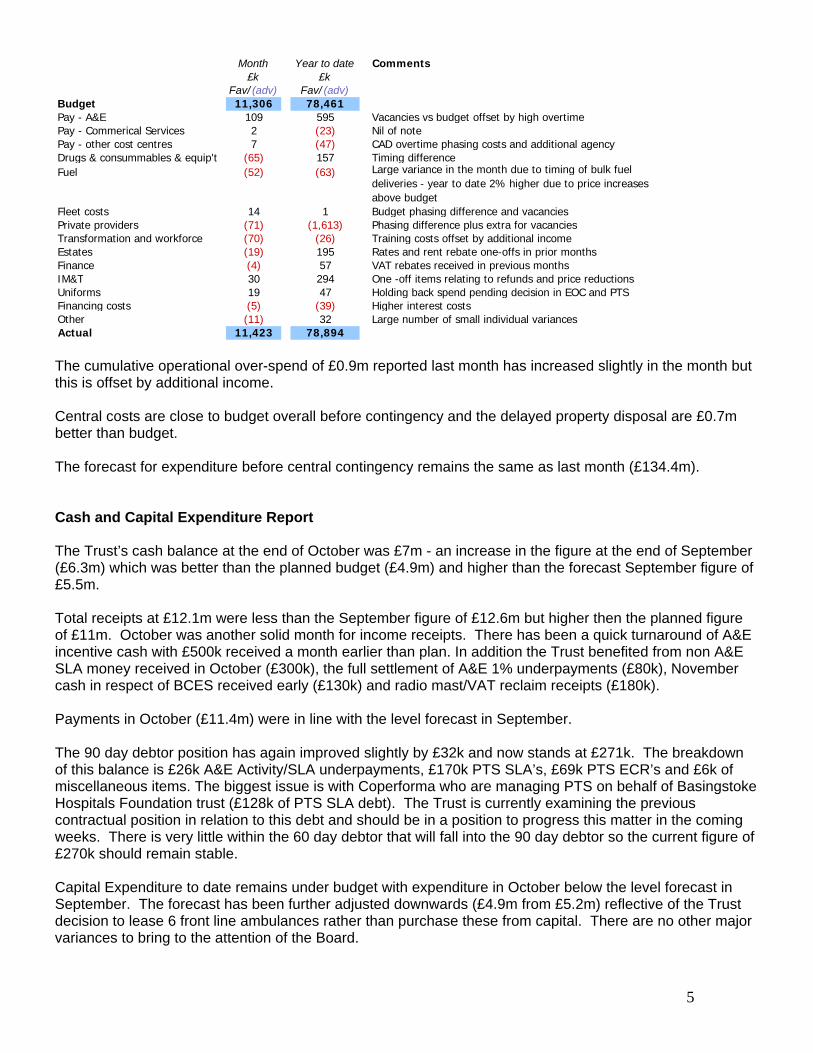
Month Year to date Comments£k £k
Fav/ (adv) Fav/ (adv)Budget 11,306 78,461Pay - A&E 109 595 Vacancies vs budget offset by high overtimePay - Commerical Services 2 (23)
(47)Nil of note
Pay - other cost centres 7 CAD overtime phasing costs and additional agencyDrugs & consummables & equip't 157(65) Timing difference Fuel Lar(52) (63) ge variance in the month due to timing of bulk fuel
deliveries - year to date 2% higher due to price increases above budget
Fleet costs 14 1 Budget phasing difference and vacanciesPrivate providers Phasin(71) (1,613) g difference plus extra for vacanciesTransformation and workforce (70) (26) Training costs offset by additional incomeEstates 195 Rates and rent rebate one-offs in prior monthsFinance 57 VAT rebates received in previous monthsIM&
(19)(4)
T 30 294 One -off items relating to refunds and price reductionsUniforms 19 47 Holding back spend pending decision in EOC and PTSFinancing costs Hi(5) (39) gher interest costsOther 32 Lar(11) ge number of small individual variancesActual 11,423 78,894 The cumulative operational over-spend of £0.9m reported last month has increased slightly in the month but this is offset by additional income. Central costs are close to budget overall before contingency and the delayed property disposal are £0.7m better than budget. The forecast for expenditure before central contingency remains the same as last month (£134.4m). Cash and Capital Expenditure Report The Trust’s cash balance at the end of October was £7m - an increase in the figure at the end of September (£6.3m) which was better than the planned budget (£4.9m) and higher than the forecast September figure of £5.5m. Total receipts at £12.1m were less than the September figure of £12.6m but higher then the planned figure of £11m. October was another solid month for income receipts. There has been a quick turnaround of A&E incentive cash with £500k received a month earlier than plan. In addition the Trust benefited from non A&E SLA money received in October (£300k), the full settlement of A&E 1% underpayments (£80k), November cash in respect of BCES received early (£130k) and radio mast/VAT reclaim receipts (£180k). Payments in October (£11.4m) were in line with the level forecast in September. The 90 day debtor position has again improved slightly by £32k and now stands at £271k. The breakdown of this balance is £26k A&E Activity/SLA underpayments, £170k PTS SLA’s, £69k PTS ECR’s and £6k of miscellaneous items. The biggest issue is with Coperforma who are managing PTS on behalf of Basingstoke Hospitals Foundation trust (£128k of PTS SLA debt). The Trust is currently examining the previous contractual position in relation to this debt and should be in a position to progress this matter in the coming weeks. There is very little within the 60 day debtor that will fall into the 90 day debtor so the current figure of £270k should remain stable. Capital Expenditure to date remains under budget with expenditure in October below the level forecast in September. The forecast has been further adjusted downwards (£4.9m from £5.2m) reflective of the Trust decision to lease 6 front line ambulances rather than purchase these from capital. There are no other major variances to bring to the attention of the Board.
5

Cost Savings Plans Progress against the plan can be summarised as follows:
Actual Budget Var Actual Budget Var Forecast Budget Var29 89 -60 -494 -798
-94 -175 -513
-46 -130 -158 -61 -61 -314 -58 -58 -114
-5 -10 -45 -65
-19 -31
-9 -64 -4 -51 -10 -2 -2 -24
-300 -300
-143 -14 -96
129 624 271 1,069387 67 320 1,380 469 911 1,871 804 1,06711 106 75 250 266 77974 59 15 672 324 349 1,137 600 5370 46 0 130 259 4176 67 6 67 86 4000 58 0 58 237 351
47 27 19 234 190 45 337 325 1247 52 75 52 24 311 310 120 30 108 152 222 28617 17 0 149 149 0 200 200 00 19 44 75 193 187 6
103 3 100 241 156 86 431 168 26311 11 0 78 78 0 163 163 040 11 29 106 44 61 345 100 24527 36 -68 43 9412 22 74 27 47 150 78 72-0 2 5 7 11 350 0 0 0 0 0 138 0 138
0
Total 830 677 154 3,309 2,788 522 6,369 6,365 413.0% 10.6% 52.0% 43.8%
Total recurrent 733 691 42 3,289 2,884 406 6,214 6,357Total non recurrent 98 112 20 116 155 8 147
Month YTD Full YearProject
Commercial DivisionCSDDual ECA CrewsOverhead Cost SavingsSicknessTARP - UnsocialOperational RestructureConsumable ReductionEOC RestructureHospital DelaysProject Management Reduction Private Provider ReplacementTelephonyFleet SavingsResource Utilisation
Contingency
Project Cost ReductionCorporate SavingsProperty SavingsNon Conveyance Improvement
£830k of savings were achieved in the month which is £154k ahead of budget. The CSD, overheads and telephony savings continue significantly ahead of plan. The CSD and telephony forecasts have been upgraded this month (total of £468k). This has facilitated the set-up of a central contingency of £300k after forecast degradations due to delays in other projects - total of £200k with the largest being dual ECA (£100k) and sickness (£50k). Risks The risks identified in the forecast can be summarized as follows:
6

RisksPotential Weighting Expected after
mitigationWeighting Possible after
mitigation£k % %
Non-conveyance 250 75% 188 70% 175Activity in forecast (diff to ytd run-rate) 200 50% 100 75% 150CQUINN 225 0% 0 50% 113Hants A&E overspend 500 0% 0 25% 125Penalty risk 500 0% 0 0% 0Other costs 100 0% 0 50% 50Sub total 999 1,775 288 613
PTS South costs 103 60% 62 60% 62Ox OOH new rotas 25 25% 6 80% 20Additional ECR's PTS Hants (net effect) 35 25% 9 80% 28Additional Ox Logistics businss 50 25% 13 50% 25BCES income 145 50% 73 90% 131Extra net risk 200 0% 0 50% 100Sub total Commercial 558 162 365
VAT liability 455 0% 0 19% 86Winchester property disposal 300 0% 0 0% 0Unfunded 111 costs 300 0% 0 0% 0Sub total corporate 1,055 0 86
Total risks 3,388 449 1,064
Other mitigating factors
Additional insurance refunds 200 95% 190 95% 190Sub total Other mitigating factors 200 190 190
Risks after full mitigation (negative) (259) (874)
Unused contingency (less earmarked ops/clinical support) 510 100% 510 100% 510Recovery plan used 1,083 0% 0 0% 0Additional recovery plan unused 720 80% 576 80% 576
Net position - positive 827 212 Overall the “expected” position is similar to last month (was £788k net versus £827k above). Two additional risks have been included:
risk on E&U activity income to reflect the slowing of growth experienced this month (1.6% this month and 3.1% year to date) – the risk has been calculated as the difference between year to date run-rate and the current forecast; and
risk on CQUIN income based on detailed review of achievement by PCT at the half year. The half year position has been extrapolated on a straight line basis to estimate the potential risk however, there are actions that SCAS is taking to ensure that this gets back on track.
Other risks remain similar to last month. The net risks in the possible case have deteriorated by £90k as a result of the above to £212k. This would still allow potential costs for the 111 bid team. Work on the recovery plan continues and a further update will be provided at the Board meeting. Procurement Update Following the termination of negotiations with Med assets, plans to pursue an alternative internal NHS solution to be led by the South SHA cluster have progressed. The major acute hospitals have developed outline strategic principles which were discussed on 30th October. The proposed solution is expected to deliver the same net benefit with lower projected scope being offset by lower fees.
7

Foundation Trust Preparedness SCAS was approved by the Medical and Applications Committees at the DoH in July to proceed to the next stage of our FT Application and was subsequently approved by the Secretary of State in August. The Monitor review commenced at the beginning of September and is ongoing to review all aspects of the organization. A target date of 1st of February 2012 has been set for the achieving Foundation Trust status. ESTATES REPORT Projects Estates Strategy
Estates Strategy revision being finalised, copies will be sent to portfolio holders in December, for comment before Execs and then Board approval.
To Trust Board in February 2012
Portsmouth Resource Centre
Updated business agreed with OP’s to satisfy concerns around cover in the Gosport peninsular.
Costs obtained for new options.
Battle Fleet facility.
Options being considered for shortlisting the preferred option. Preferred option will dictate Estates solution.
Head of Fleet reviewing business case options.
Basingstoke AS
Make Ready area, heating scheme. Quotations received and work due to start end November.
Oxford City Installation of new heating system underway. Improvements to NEPTS area completed, 40% done.
Portsmouth AS
Roof renewal and pigeon netting works underway. New roof, heating system and lighting systems required.
Battle site Fleet options business case with Exec team. Our own ground investigations underway.
Site survey’s reveal old Victorian waste dump on site.
S/B points New s/b points created in Beaconsfield,Hazlemere, Milton Keynes and Buckingham
New units in preferred drive zones
Acquisitions / Disposals Site Comment Book
Value Est. Gross disposal value
Estimated Disposal Date
Portsea AS Unconditional offer of £3K has been signed. Completion date set for 8th December.
£270K £0.3M Retained costs £6.5 pa
Battle Hospital TaylorWimpey offer reduced significantly to reflect remediation works. Wates testing due end November.
£3.6M £3.8M Tests show high levels of contamination, report being
8

9
validated. Deanshanger Re market summer 2012. £665K £0.7M Retained costs
£60Kpa Totton AS Agreement reached with
Hants CC on access rights. Re market in January.
£250K £250K Retained costs £11.5K pa.
Winchester AS
Planning application has now been placed by purchaser. Decision due early December.
£700K £1.03K Only two objections received by end of consultation. Officers still have delegated powers to give planning permission.
Banbury AS OX. C.C. have now agreed terms to release restraint to sale.
£181K £350K Contact made with Strategic planning manager at OXCC Retained costs £6k pa

Appendix A1
Actual Budget Variance Actual Budget Variance Forecast Budget Prior Year Variance to budget
Variance to Prior Year
£000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's
TOTAL SCAS INCOME 11,534 11,395 140 80,120 79,656 464 137,315 136,628 137,941 687 (626)
Emergency ServicesIncome 9,610 9,525 85 66,989 66,568 422 114,509 114,192 115,536 317 (1,028)
Direct costs 6,936 7,002 65 48,760 48,557 (203) 82,794 83,298 85,406 503 2,612
Gross contribution 2,674 2,523 150 18,229 18,011 218 31,715 30,894 30,130 821 1,58428% 26% 1% 27% 27% 0% 28% 27% 26%
Non-Emergency ServicesIncome 1,924 1,870 54 13,131 13,088 43 22,807 22,437 22,405 370 401
Direct costs 1,764 1,603 (161) 12,034 11,265 (769) 20,635 19,226 20,675 (1,409) 40
Gross contribution 161 267 (106) 1,097 1,823 (726) 2,172 3,210 1,730 (1,039) 4428% 14% -6% 8% 14% -6% 10% 14% 8%
Contribution Operational Activities 2,834 2,790 44 19,326 19,834 (508) 33,887 34,104 31,860 (218) 2,026
()
Central Costs (inc op overheads)Fleet 669 716 47 4,795 5,015 220 8,599 8,597 7,955 (2) (643)Clinical Services 135 147 12 1,036 1,029 (7) 1,779 1,764 1,758 (15) (20)Finance 245 267 22 1,569 1,628 59 2,698 2,698 2,528 (0) (170)Estates 464 433 (31) 2,886 3,041 155 5,003 5,205 5,148 201 145IM&T 442 470 28 3,010 3,289 279 5,190 5,682 5,345 492 154Transformation & OD 470 400 (70) 2,780 2,754 (26) 4,764 4,755 4,524 (9) (240)Communications & Public Engag't 59 65 5 411 452 41 745 742 597 (3) (148)Corporate 44 35 (8) 261 246 (15) 484 421 472 (62) (11)Contingency 21 0 (21) 129 0 (129) 810 460 0 (350) (460)Loss/(Profit) on disposal 0 0 0 (1) (300) (299) (340) (300) (8) 40 292Financing Costs 174 169 (5) 1,223 1,185 (39) 2,105 2,031 2,150 (74) 45
Total overhead costs 2,723 2,702 (21) 18,100 18,339 239 31,837 32,054 30,469 218 (1,058)
Net surplus 111 88 23 1,226 1,495 (269) 2,050 2,050 1,391 (0) 659
Memo: technical accounting surplus (£k) 111 88 23 1,226 1,495 (269) 1,447 2,050 177 (603) 1,270
Memo:Depreciation 576 581 5 3,992 4,065 73 6,968 6,968 6,852 (0) (116)
Other interest 2 0 (2) 3 (1) (4) (4) (4) 0 0 4
Profit on disposal 0 0 0 1 300 299 340 300 8 (40) 332
EBITDA 859 838 21 6,438 6,445 (8) 10,787 10,753 10,385 34 402
% 7.5% 7.4% 8.0% 8.1% 7.9% 7.9% 7.5%
South Central Ambulance Service NHS TrustFinancial results for Month 7 ended 31 October 2011
Month Year to date Full Year

Actual Budget Variance Actual/ forecast
Budget Variance Forecast Budget Variance Forecast Budget Variance Forecast Budget Variance
£000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's
TOTAL SCAS INCOME 34,202 34,122 80 34,384 34,139 245 34,412 34,183 229 34,318 34,184 134 137,316 136,628 688
Emergency ServicesIncome 28,600 28,513 87 28,779 28,530 249 28,618 28,574 44 28,511 28,575 (64) 114,509 114,192 317
Direct costs 20,955 20,673 (282) 20,869 20,882 13 20,617 20,938 321 20,354 20,805 451 82,795 83,298 503
Gross contribution 7,646 7,840 (194) 7,910 7,648 262 8,002 7,636 366 8,157 7,770 387 31,714 30,894 8200% 0% 0%
Non-Emergency ServicesIncome 5,602 5,609 (7) 5,605 5,609 (4) 5,793 5,609 184 5,807 5,609 198 22,807 22,436 371
Direct costs 5,001 4,878 (123) 5,269 4,812 (457) 5,251 4,819 (432) 5,118 4,772 (346) 20,640 19,281 (1,359)
Gross contribution 600 731 (131) 336 797 (461) 542 790 (248) 688 837 (149) 2,167 3,155 (988)0% 0% 0%
Contribution Operational Activities 8,246 8,571 (325) 8,245 8,445 (200) 8,544 8,426 118 8,846 8,607 239 33,881 34,049 (168)
Central Costs (inc op overheads)Central Costs 0 0Fleet 888 963 75 973 961 (12) 953 961 8 1,038 961 (77) 3,853 3,846 (7)Clinical Services 436 441 5 465 441 (24) 433 441 8 445 441 (4) 1,778 1,764 (14)Finance 552 631 79 673 631 (42) 654 627 (27) 622 611 (11) 2,500 2,500 0Estates 835 983 148 942 980 38 1,011 976 (35) 981 976 (5) 3,769 3,915 146IM&T 954 1,163 209 1,108 1,163 55 1,053 1,163 110 1,087 1,207 120 4,201 4,696 495Transformation & OD 1,114 1,178 64 1,195 1,176 (19) 1,261 1,200 (61) 1,192 1,200 8 4,763 4,754 (9)Communications & Public Engag't 176 194 18 177 200 23 189 190 1 204 172 (32) 745 756 11Corporate 96 105 9 121 105 (16) 137 105 (32) 130 105 (25) 484 420 (64)Contingency 11 0 (11) 97 0 (97) 278 310 32 423 149 (274) 809 459 (350)Loss/(Profit) on disposal (14) (300) (286) 14 0 (14) 0 0 0 (340) 0 340 (340) (300) 40Depreciation 1,698 1,740 42 1,718 1,740 22 1,717 1,740 23 1,835 1,738 (97) 6,968 6,958 (10)PDC 465 464 (1) 485 465 (20) 475 465 (10) 475 465 (10) 1,900 1,859 (41)Interest 43 43 0 56 43 (13) 52 43 (9) 54 43 (11) 205 172 (33)Injury benefit 50 50 0 50 50 0 50 50 0 50 50 0 200 200 0
Total overhead costs 7,303 7,655 352 8,075 7,955 (120) 8,262 8,271 9 8,196 8,118 (78) 31,835 31,999 164
Net surplus 943 916 27 171 490 (319) 282 155 127 650 489 161 2,048 2,050 2
South Central Ambulance Service NHS Trust (Appendix A2)
Q1 Q2 Q3 Q4 Full Year
Financial results for Month 7 ended 31 October 2011

Appendix B
Income analysis
Actual Budget Variance Actual Budget Variance Forecast Budget Prior Year Variance to budget
Variance to Prior
Year£000's £000's £000's £000's £000's £000's £000's £000's £000's £000's £000's
Emergency ServicesE&U Contract 2011/2012 8,978 9,014 (36) 63,068 63,059 9 107,996 108,127 108,703 (130) (706)HART income 257 258 (1) 1,802 1,808 (6) 3,089 3,100 3,142 (11) (53)Fire schemes income 0 0 0 0 0 0 0 0 0 0 0Public Events 37 18 18 132 129 3 227 221 233 6 (7)CBRN/Flu funding 32 25 7 179 174 5 307 298 682 9 (375)RTA Recoveries 42 21 21 292 146 146 500 250 523 250 (23)Training Monies from NESC 199 139 60 927 972 (45) 1,745 1,666 1,577 79 168Workshop Income 3 7 (4) 57 46 11 88 79 82 9 5TVEA 17 28 (11) 153 197 (44) 239 338 338 (99) (99)Other Income 76 46 30 591 248 342 681 476 619 205 62AfC Transfer (30) (30) 0 (211) (211) 0 (363) (363) (363) 0 0Total Emergency Services 9,610 9,525 85 66,989 66,568 422 114,509 114,192 115,536 317 (1,028)
Non-Emergency ServicesPTS Hampshire 296 309 (13) 1,969 2,163 (194) 3,416 3,708 3,438 (291) (22)PTS Berkshire 303 281 23 2,022 1,965 56 3,469 3,369 3,633 100 (164)PTS Ox & Bucks 673 611 62 4,705 4,276 430 8,102 7,330 7,583 772 519Out of Hours - Berkshire 77 65 13 506 453 53 861 776 888 85 (27)Out of Hours - Ox & Bucks 64 64 0 445 445 0 763 763 751 0 12Logistic Services - Berkshire 114 109 5 781 762 19 1,346 1,307 1,323 39 23Logistic Services - Ox & Bucks 86 84 2 573 589 (16) 1,024 1,010 976 14 48Community Equipment Provision 249 250 (1) 1,684 1,753 (69) 3,052 3,005 2,881 48 171Commercial Training 32 67 (36) 235 471 (236) 411 808 569 (397) (158)Events Management 0 0 0 0 0 0 0 0 1 0 (1)AfC Transfer 30 30 0 211 211 0 363 363 363 0 0Total Non-Emergency Services 1,924 1,870 54 13,131 13,088 43 22,807 22,437 22,405 370 401
Total income 11,534 11,395 140 80,120 79,656 464 137,315 136,628 137,941 687 (626)
South Central Ambulance Service NHS TrustFinancial results for Month 7 ended 31 October 2011
Month Year to date Full Year

South Central Ambulance Service NHS Trust Appendix C
Actual Budget Variance Actual Budget Variance Forecast Budget Prior year
Key Operational Ratios Sep-11 Sep-11 Sep-11 YTD YTD YTD Full Yr Full Yr Full Yr
+/(-) +/(-)
Activity - % year on year 1.6% 3.0% n/a 3.2% 3.0% 0.2% 3.5% 3.5% 6.4% - income from growth (£k) 45 102 (57) 685 615 70 1,400 1,230 2,469Non conveyance - non-conveyance above baseline (£k) 96 96 0 696 575 121 1,150 1,150 n/a - non-conveyance increase in rate (£k) 0 65 (65) 0 391 (391) 255 783 372Delays at hospitals - income from delays (£k) 157 58 99 700 408 292 700 700 1,726
Clinical quality incentive 128 128 0 897 897 0 1,500 1,537 1,500
Performance penalty 0 0 0 0 0 0 0 0 0
Total income from activity related measures 426 353 73 2,978 2,886 92 5,005 5,400 6,067
Actual Budget Variance Actual Budget Variance Forecast Budget Prior year
Key Operational Spend (£k) Sep-11 Sep-11 Sep-11 YTD YTD YTD Full Yr Full Yr Full Yr
+/(-) +/(-)
Overtime
- A&E - Hants 141 90 (52) 1,113 752 (360) 1,598 1,194 1,779 - A&E - Bucks/Ox 131 81 (50) 919 662 (257) 1,351 1,066 1,433 - A&E - Berks 87 43 (45) 546 381 (164) 946 595 934 - A&E - Control 22 24 1 166 166 (0) 330 284 542 - A&E - Comm Resp/Emer Plan/Fleet 18 12 (6) 143 87 (56) 254 149 315 - Commercial Division - PTS 46 25 (21) 336 176 (160) 446 300 625 - Commercial Division - non-PTS 11 9 (2) 75 67 (8) 127 114 215 - Other 22 10 (2) 266 64 (16) (30) 108 230Total Overtime 480 293 (176) 3,563 2,355 (1,022) 5,022 3,810 6,072
Private Providers - A&E - Hants 201 279 78 2,422 1,956 (466) 3,213 3,353 4,713 - A&E - Bucks/Ox 60 79 19 567 530 (38) 874 906 2,167 - A&E - Berks 221 161 (61) 1,619 1,219 (400) 2,152 1,804 3,222 - PTS 279 172 (107) 1,912 1,203 (709) 3,281 2,056 3,400Total private providers 761 690 (71) 6,521 4,907 (1,613) 9,520 8,118 13,502
Fuel- A&E 296 258 (37) 1,879 1,808 (71) 3,250 3,100 2,798- Commercial Services 102 88 (14) 647 615 (32) 1,096 1,055 1,023- Fleet central 4 3 (0) 37 24 (13) 60 41 28- Other 26 26 0 131 184 53 224 315 149Total fuel 428 376 (52) 2,694 2,631 (63) 4,629 4,510 3,999

South Central Ambulance Service NHS Trust
Sep-11 Sep-11 Variance YTD YTD Variance Full year Full year Prior year Comments Rating Weighted Rating Weighted
Key Financial Ratios Actual Budget Actual Budget Forecast Budget YTD Rating Forecast Rating
I&E Surplus (k) 111 88 23 1,226 1,495 (269) 2,050 2,050 612
I&E Surplus Margin 1.0% 0.8% -12% 1.5% 1.9% -0.3% 1.5% 1.5% 0.5% Tracking slightly behind plan 3 0.6 3 0.6
External Finance Limit 92 (645) 737 9 1,236 (1,227) 2,326 4,095 (1,769) Lower in forecast due to disposal delays
Return on Assets 5.0% 4.6% 0.4% 6.2% 6.0% 0.1% 5.6% 5.6% 4.3% One would expect this mesasure to be relatively low in a not for profit organisation.
5 1 4 0.8
EBITDA margin 7% 7% 0% 8% 8% 0% 8% 8% 6% This measures the Trust's fundamental earning power and is in line with budget.
3 0.75 3 0.75
EBITDA % achieved 103% 100% 3% 96% 100% -4% 101% 96% 90% This measures the performance of EBITDA to budget and this is moving in line with profitability - hence higherin month but lower year to date.
4 0.4 5 0.5
Liquidity Ratio (days) -11.2 -11 0 -11.2 -11.2 0 18.8 18.8 0.1 This measures the ability of the Trust to pay its costs based on its net current assets.
1 0.25 3 0.75
Total out of maximum score of 5 3.0 3.4
Target 3 3
Sep-11 Aug-11 Jul-11 Last Year
YTD YTD YTD Full year
Better payment practice target
- Non-NHS by number 90% 90% 91% 83%
- Non-NHS by £ value 95% 94% 94% 92%
- NHS by number 97% 97% 96% 87%
- NHS by £ value 98% 97% 97% 91%
Debtors > 90 days (£k) 271 307 373 353
% cost improvements secured (actual) 52% 39% 28% 100%
% cost improvements secured (plan) 44% 33% 27% 100%
For information only:Ratings applied to financial ratings
Metric Weight 5 4 3 2 1EBITDA margin 25% 11% 9% 5% 1% <1%EBITDA, % achieved 10% 100% 85% 70% 50% <50%ROA 20.0% 6% 5% 3% 2% < 2%I&E surplus margin 20.0% 3% 2% 1% -2% < -2%Liquid ratio 25.0% 35 25 15 10 <10
100%
Appendix D
Comments
Current Risk Ratings:
Nil of note
Continued improvement this month - of the remaining old balances, PTS accounts for 75% of which Coperforma is the largest at £128k.
Ahead of plan - strong contribution from the CSD and overheads savings has compensated for delays in the sickness, dual ECA and commercial division projects.

South Central Ambulance Service NHS TrustAppendix E
CASHFLOW Q1 Q1 Q1 Jul-11 Aug-11 Sep-11 Q2 Q2 Q2 Oct-11 Nov-11 Dec-11 Q3 Q3 Q3 Jan-12 Feb-12 Mar-12 Q4 Q4 Q4
Sep-11 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000
Actl Budget Variance Actl Actl Actl Actl Budget Variance Actl Fcst Fcst Fcst Budget Variance Fcst Fcst Fcst Fcst Budget VarianceIncomeSL Receipts 32,443 32,488 (45) 10,579 11,164 10,640 64,826 64,104 722 11,227 10,461 10,461 96,975 95,719 1,256 10,566 10,466 10,449 128,456 127,335 1,121HART 344 1,051 1,693 3,088 1,550 1,538 3,088 2,325 763 3,088 3,100 (12)Incentives 1,050 750 300 128 161 1,339 2,700 (1,361) 561 715 513 3,128 4,050 (922) 768 238 1,038 5,172 5,400 (228)Fixed Asset Receipts 180 180 0 11 191 180 11 297 488 180 308 1,020 1,508 4,851 (3,343)Interest 5 4 1 2 2 2 11 7 4 2 2 2 17 10 7 2 2 3 24 13 11Capital Loan From HA 0 0 0 0 0 0 0 0 0 0Other Income/PDC/VAT/RTA 798 603 195 248 226 276 1,548 1,103 445 311 279 200 2,338 1,703 635 200 250 200 2,988 2,300 688Advance of SLA/brokerage
Total Cash In 34,476 34,025 451 11,301 12,615 12,611 71,003 69,644 1,359 12,101 11,457 11,473 106,034 103,987 2,047 11,536 10,956 12,710 141,236 142,999 (1,763)
ExpenditurePay expenditure 21,101 21,164 63 7,124 7,128 7,119 42,472 43,376 904 7,104 7,120 7,200 63,896 64,839 943 7,200 7,264 7,284 85,644 86,826 1,182Non Pay expenditure 12,490 11,826 (664) 3,851 3,883 4,254 24,478 21,743 (2,735) 3,713 3,250 3,250 34,691 31,995 (2,696) 3,250 3,250 3,231 44,422 41,626 (2,796)Capital expenditure 717 739 22 135 82 89 1,023 2,877 1,854 560 778 1,051 3,412 4,075 663 851 373 624 5,260 6,970 1,710Dividends on PDC 0 950 950 929 (21) 950 929 (21) 950 1,900 1,859 (41)PDC/Loan Repayment 0 664 664 717 53 664 717 53 771 1,435 1,435 0Working Capital Loan 0 0 0 0 0 0 0 0 0 0Interest on DH Loans 0 99 99 85 (14) 99 85 (14) 123 222 188 (34)Other expenditure 1 0 (1) 3 6 4 14 (14) 13 27 (27) 27 0 (27)Total Cash Out 34,309 33,729 (580) 11,113 11,099 13,179 69,700 69,727 27 11,390 11,148 11,501 103,739 102,640 (1,099) 11,301 10,887 12,983 138,910 138,904 (6)
Net Cash In/(Out) 167 296 (129) 188 1,516 (568) 1,303 (83) 1,386 711 309 (28) 2,295 1,347 948 235 69 (273) 2,326 4,095 (1,769)
Balance B/fwd 4,977 4,916 61 5,144 5,332 6,848 4,977 4,916 61 6,280 6,991 7,300 4,977 4,916 61 7,272 7,507 7,576 4,977 4,916 61
Balance C/fwd 5,144 5,212 (68) 5,332 6,848 6,280 6,280 4,833 1,447 6,991 7,300 7,272 7,272 6,263 1,009 7,507 7,576 7,303 7,303 9,011 (1,708)
CASHFLOW Q1 Q1 Q1 Jul-11 Aug-11 Sep-11 Q2 Q2 Q2 Oct-11 Nov-11 Dec-11 Q3 Q3 Q3 Jan-12 Feb-12 Mar-12 Q4 Q4 Q4
RECONCILIATION Actual Budget Variance £000 £000 £000 Actual Budget Variance £000 £000 £000 Fcst Budget Variance £000 £000 £000 Fcst Budget VarianceEBIT 1,434 1,122 312 1,616 1,796 2,161 2,161 2,125 36 2,446 2,736 2,915 2,915 2,790 125 3,101 3,472 3,816 3,816 3,786 30Depreciation & Amortisation 1,698 1,742 (44) 2,263 2,840 3,416 3,416 3,484 (68) 3,992 4,568 5,144 5,144 5,226 (82) 5,720 6,351 6,968 6,968 6,968 0EBITDA 3,132 2,864 268 3,879 4,636 5,577 5,577 5,609 (32) 6,438 7,304 8,059 8,059 8,016 43 8,821 9,823 10,784 10,784 10,754 30Impair/Other Non Cash 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Stock (Inc)/dec (63) 0 (63) (72) (49) (55) (55) (55) (32) (55) (55) (55) (55) (55) (55) (20) (20) (20) 0Debtors (Inc)/dec (2,477) (1,572) (905) (2,584) (1,169) (478) (478) (197) (281) 105 100 105 105 (197) 302 500 (300) (225) (225) (197) (28)Creditors Inc/(dec) 193 (463) 656 45 (512) (880) (880) (973) 93 (948) (781) (760) (760) (455) (305) (723) (375) 79 79 147 (68)Provisions Inc/(dec) (105) 0 (105) (262) (298) (262) (262) (100) (162) (387) (300) (350) (350) (400) 50 (450) (550) (1,000) (1,000) (1,000) 0Capital expenditure (717) (739) 22 (852) (936) (1,023) (1,023) (2,877) 1,854 (1,583) (2,361) (3,412) (3,412) (4,075) 663 (4,263) (4,636) (5,260) (5,260) (6,970) 1,710Capital disposals 201 180 21 196 191 188 188 180 8 188 188 488 488 180 308 488 488 1,508 1,508 4,851 (3,343)
Free Cashflow pre financ 164 270 (106) 350 1,863 3,067 3,067 1,642 1,425 3,781 4,095 4,075 4,075 3,069 1,006 4,318 4,395 5,866 5,866 7,565 (1,699)
Interest 3 3 0 5 8 (97) (97) (79) (18) (96) (87) (86) (86) (76) (10) (85) (84) (205) (205) (176) (29)Dividends on PDC 0 0 0 0 0 (950) (950) (929) (21) (950) (950) (950) (950) (929) (21) (950) (950) (1,900) (1,900) (1,859) (41)Free Cashflow 167 296 (106) 355 1,871 2,020 2,020 634 1,386 2,735 3,058 3,039 3,039 2,064 975 3,283 3,361 3,761 3,761 5,530 (1,769)PDC Payment/(Repayment) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Loan repayments 0 0 0 0 0 (717) (717) (717) 0 (721) (735) (744) (744) (717) (27) (753) (762) (1,435) (1,435) (1,435) 0Lease Borrowings 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Capital Loan from DH 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Net Cash In/(Out) 167 296 (106) 355 1,871 1,303 1,303 (83) 1,386 2,014 2,323 2,295 2,295 1,347 948 2,530 2,599 2,326 2,326 4,095 (1,769)

South Central Ambulance Service NHS TrustAppendix E
CASHFLOW Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Full Year Full Year
Apr-12 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000
Fcst Fcst Fcst Fcst Fcst Fcst Fcst Fcst Fcst Fcst Fcst Fcst Fcst BudgetIncomeSL Receipts 10,681 10,681 10,681 10,681 10,681 10,681 10,681 10,681 10,681 10,681 10,681 10,680 128,171 128,171HART 258 258 258 258 258 258 258 258 258 258 258 262 3,100 3,100Incentives 425 425 425 443 443 443 443 443 443 443 443 443 5,262 5,262Fixed Asset Receipts 3,696 3,696 3,696Interest 2 2 2 2 2 2 2 2 2 2 2 2 24 24Capital Loan From HA 0 0Other Income/PDC/VAT/RTA 151 200 200 200 200 200 200 200 200 200 200 196 2,347 2,347Advance of SLA/brokerage 0 0 0Total Cash In 11,517 11,566 11,566 11,584 11,584 11,584 11,584 11,584 11,584 11,584 11,584 15,279 142,600 142,600
ExpenditurePay expenditure 7,545 7,545 7,545 7,545 7,545 7,545 7,545 7,545 7,545 7,545 7,545 7,546 90,541 90,541Non Pay expenditure 3,394 3,106 3,030 3,030 3,030 3,016 3,016 3,016 2,986 2,986 2,986 2,977 36,573 36,573Capital expenditure 664 713 825 305 533 447 609 633 1,268 198 445 1,540 8,180 8,180Dividends on PDC 929 930 1,859 1,859PDC/Loan Repayment 703 703 1,406 1,406Working Capital Loan 0Interest on DH Loans 76 75 151 151Other expenditure 604 604 604Total Cash Out 11,603 11,364 11,400 10,880 11,108 12,716 11,170 11,194 11,799 10,729 10,976 14,375 139,314 139,314
Net Cash In/(Out) (86) 202 166 704 476 (1,132) 414 390 (215) 855 608 904 3,286 3,286
Balance B/fwd 7,303 7,217 7,419 7,585 8,289 8,765 7,633 8,047 8,437 8,222 9,077 9,685 7,303 7,303
Balance C/fwd 7,217 7,419 7,585 8,289 8,765 7,633 8,047 8,437 8,222 9,077 9,685 10,589 10,589 10,589
CASHFLOW Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Forecast Budget
RECONCILIATION £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000Operating Surplus 419 852 1,595 2,047 2,451 2,783 3,085 3,312 3,569 3,819 4,267 4,390 4,390 4,390Depreciation & Amortisation 596 1,192 1,788 2,384 2,980 3,576 4,172 4,768 5,364 5,960 6,556 7,155 7,155 7,155
1,015 2,044 3,383 4,431 5,431 6,359 7,257 8,080 8,933 9,779 10,823 11,545 11,545 11,545Impair/Other Non Cash 0
Stock (Inc)/dec 0 0Debtors (Inc)/dec (162) (528) (985) (1,196) (1,279) (291) (338) (310) (282) (247) (410) (201) (201) (201)Creditors Inc/(dec) (277) (27) 80 250 340 (540) (370) (200) (30) 140 310 (370) (370) (370)Provisions Inc/(dec) 200 200 200Capital expenditure (664) (1,377) (2,202) (2,507) (3,040) (3,487) (4,096) (4,729) (5,997) (6,195) (6,640) (8,180) (8,180) (8,180)Capital disposals 0 3,696 3,696 3,696
Free Cashflow pre finance (88) 112 276 978 1,452 2,041 2,453 2,841 2,624 3,477 4,083 6,690 6,690 6,690
Interest 2 4 6 8 10 (80) (78) (76) (74) (72) (70) (143) (143) (143)Dividends on PDC 0 0 0 0 0 (928) (928) (928) (928) (928) (928) (1,855) (1,855) (1,855)Free Cashflow (86) 116 282 986 1,462 1,033 1,447 1,837 1,622 2,477 3,085 4,692 4,692 4,692PDC Payment/(Repayment) 0 0 0 0 0 0 0 0 0 0 0 0 0 0Loan repayments 0 0 0 0 0 (703) (703) (703) (703) (703) (703) (1,406) (1,406) (1,406)Lease Borrowings 0 0 0 0 0 0 0 0 0 0 0 0 0 0Capital Loan from DH 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Net Cash In/(Out) (86) 116 282 986 1,462 330 744 1,134 919 1,774 2,382 3,286 3,286 3,286

SOUTH CENTRAL AMBULANCE NHS TRUSTCapital resources available F1 Budget Exp summary F1 Budget
CAPITAL EXPENDITURE BUDGET 2011/2012 core depreciation estima 6,968 6,600 Clinical 0book value asset sales Estates 769 1,323Surplus Operations 401 761
Reversal of 0809 Brokerage Fleet 2,795 3,300Month Total capital resources available 6,968 6,600 IT 821 965Oct-11 Other 115 252
Surplus/(Shortfall) 2,068 0 4,900 6,600
Actual/Forecast Spend ProfileScheme Description Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Forecast Budget
£000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000
ESTATESBicester EOC 66 29 3 1 2 90 90 280 279MK Resource Centre and Bletchley 0 150HART Southampton -54 3 2 9 45 5 52Battle (new) fit out 0 100Estates data base 0 40HW Roof 25 25 50 50HW Roller shutters 10 10 20 20High Wycombe Improvements 5 7 -1 2 13 0Oxford Heating 85 85 85Oxford City Make Ready 0 0SM drainage 10 10 10Didcot ventilation 0 15Box charging points 9 9 9Box power washers 16 16 16Box lighting upgrades 10 10 10All ASAPs 1 36 25 15 77 100Beaconsfield ASAP 2 1 6 9 0West Wycombe SSP 5 4 9 0Waterlooville Standby Point 1 1 0Winchester ASAP (part of HART) 12 1 1 13 0Newbury Garage 0 85Berks lighting systems 15 15 15Hants lighting controls 15 15 15Basingstoke make ready heating 40 40 40Portsmouth refurb 22 22 170Andover heating and roof 21 21 21Commercial Training Upgrade 0 40Oxford City -3 9 6 0Wexham Station upgrade 9 9 0Hightown External refurbish -5 5 0 0Bracknell Refurbishment 20 13 33 0FLEET12 x Front Line Ambulances - Mercs 406 78 364 434 588 124 1,994 1,9946 x Front Line Amb's - Van Converts 320 320 697Berkshire Recovery Vehicle 0 80IDR fitment for SRV Ox Bucks 15 15 15Ambulance CCTV hard drive upgrade 31 31 56Service Vans 29 29 58Modernisation of ambulances 9 19 11 20 6 46 46 46 46 250 400Fleet Management system 5 5 5 14 10 39 020 new DMA Ambulances 98 19 117 0OPERATIONSPatient Monitoring Sol's/Mobimeds (5) 55 55 55Intra Osseus Infusion Devices 70 70 70Clinical Equipment General 5 80 85 80Equipment on Vehicles (RRVs) 48 25 25 25 25 148 556CAD 7 36 43 0ITRADIO/MICROWAVELINK 0 220Operational Forecasting IT System 80 70 150 150Final CAD implementation 5 42 47 90CAD Developments 70 70 70TARP 5 20 1 6 17 49 15Relocation - EOC Changes 0 150Hardware refresh 22 12 12 12 12 70 120PTS Mobile Units 48 48 150Data Store Severs 20 20 0Emergency 111 90 90 0Vitual Contact Centre 14 61 54 8 136 0cad software upgrade 7 1 2 11 21 0Centricty 14 14 0ICT Helpdesk (HOTH) 4 3 2 9 0Bicester EOC I/CAD 47 47 0NHS Pathways I/CAD 11 37 48 0Make ready scanner replacement 2 2 0Unallocated 10 105 115 252TOTAL PROGRAMME 84 45 214 135 82 469 195 1032 797 851 373 623 4,900 6,600
Appendix F

South Central Ambulance Service NHS Trust Appendix G
BALANCE SHEET Actual Actual ForecastOct-11 Oct-11 Mar-11 Mar-12
(£k) (£k) (£k)
FIXED ASSETS
Property, Plan & Equipment 60,301 63,885 61,304Intangible assets 1,703 894 1,395
62,004 64,779 62,699
CURRENT ASSETS
Stocks & Work In Progress 1,052 1,020 1,040
Assets held for resale 5,766 5,952 4,193
Sales Ledger Debtors 2,024 3,054 3,241Prepayments & Accrued Income 4,621 3,473 3,572Other Debtors 325 549 488Trade & Other Receivables 6,970 7,076 7,301Cash and cash equivalents 6,991 4,977 7,303
TOTAL CURRENT ASSETS 20,779 19,025 19,837
CREDITORSPurchase Ledger Creditors (1,580) (1,783) (1,876)Accruals & deferred income (6,312) (6,869) (6,856)Other Creditors Incl Pensions, PAYE & NI (2,962) (2,976) (2,975)Capital Accruals (59) (418) (58)Borrowings < 1 year (1,426) (1,435) (1,435)Provisions < 1 year (2,364) (2,449) (1,225)CURRENT LIABILITIES (14,703) (15,930) (14,425)
NET CURRENT ASSETS/(LIABILITIES) 6,076 3,095 5,412
TOTAL ASSETS LESS CURRENT LIABILITIES 68,080 67,874 68,111
Borrowings (3,538) (4,255) (2,820)Provisions (2,243) (2,546) (2,770)Other Financial Liabilities (26) (26) (26)Non-Current Liabilities (5,807) (6,827) (5,616)
TOTAL ASSETS EMPLOYED 62,273 61,047 62,495
FINANCED BY:TAXPAYER'S EQUITYPublic Dividend Capital (57,874) (57,874) (57,874)Revaluation Reserve (6,771) (6,771) (6,771)Donation Reserve (1,615) (1,615)Other Reserve 350 350 350Govt Grant Reserve- bfwd (208) (208)Retained Earnings 5,071 5,839 3,248I & E YTD (1,226) (768) (1,448)
TOTAL TAXPAYERS EQUITY (62,273) (61,047) (62,495)
Adjusted net current assets/liabilities for Liquidity (742) (3,877) 179Liquidity (days) using prior year assets (11.2) (11.2)Liquidity ratio 1.0 1.0
Liquidity with wc facility (days) 18.8 18.8Liquidity ratio 3.0 3.0
Liquidity using current year assets (2.1) 0.5 27.9 30.5

Enclosure: J.2
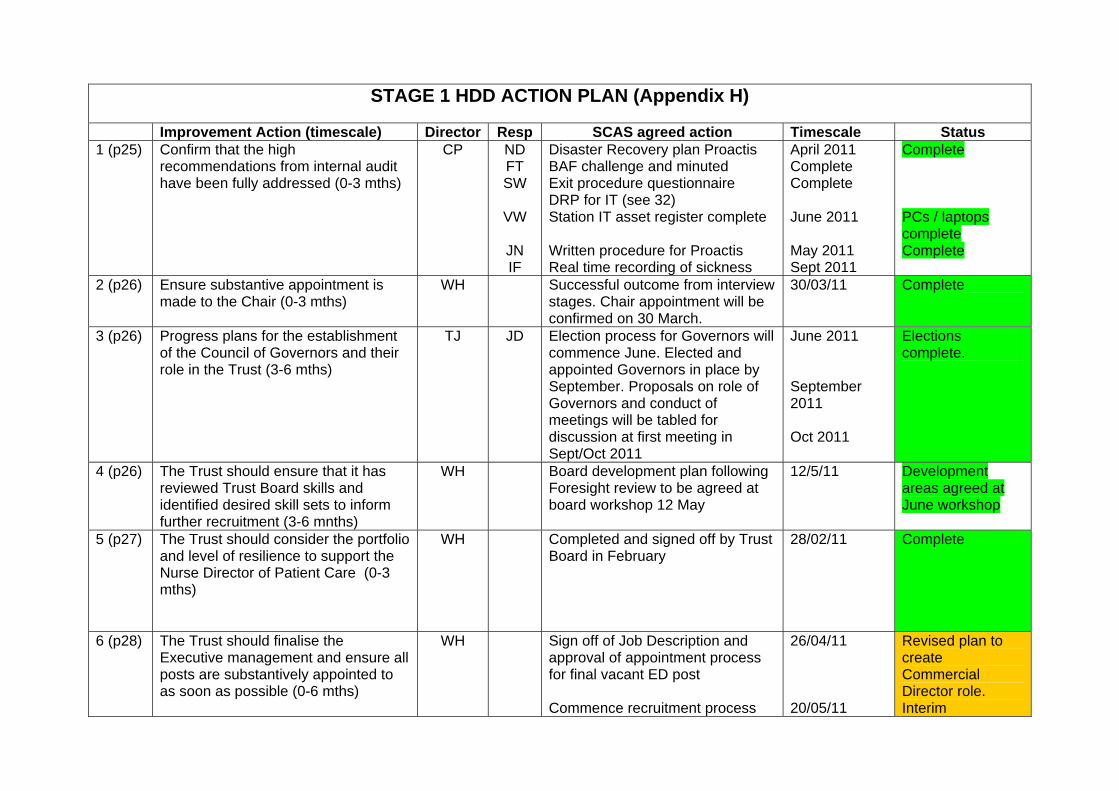
STAGE 1 HDD ACTION PLAN (Appendix H)
Improvement Action (timescale) Director Resp SCAS agreed action Timescale Status 1 (p25) Confirm that the high
recommendations from internal audit have been fully addressed (0-3 mths)
CP ND FT SW
VW
JN IF
Disaster Recovery plan Proactis BAF challenge and minuted Exit procedure questionnaire DRP for IT (see 32) Station IT asset register complete Written procedure for Proactis Real time recording of sickness
April 2011 Complete Complete June 2011 May 2011 Sept 2011
Complete PCs / laptops complete Complete
2 (p26) Ensure substantive appointment is made to the Chair (0-3 mths)
WH Successful outcome from interview stages. Chair appointment will be confirmed on 30 March.
30/03/11 Complete
3 (p26) Progress plans for the establishment of the Council of Governors and their role in the Trust (3-6 mths)
TJ JD Election process for Governors will commence June. Elected and appointed Governors in place by September. Proposals on role of Governors and conduct of meetings will be tabled for discussion at first meeting in Sept/Oct 2011
June 2011 September 2011 Oct 2011
Elections complete.
4 (p26) The Trust should ensure that it has reviewed Trust Board skills and identified desired skill sets to inform further recruitment (3-6 mnths)
WH Board development plan following Foresight review to be agreed at board workshop 12 May
12/5/11
Development areas agreed at June workshop
5 (p27) The Trust should consider the portfolio and level of resilience to support the Nurse Director of Patient Care (0-3 mths)
WH Completed and signed off by Trust Board in February
28/02/11 Complete
6 (p28) The Trust should finalise the Executive management and ensure all posts are substantively appointed to as soon as possible (0-6 mths)
WH Sign off of Job Description and approval of appointment process for final vacant ED post Commence recruitment process
26/04/11 20/05/11
Revised plan to create Commercial Director role. Interim
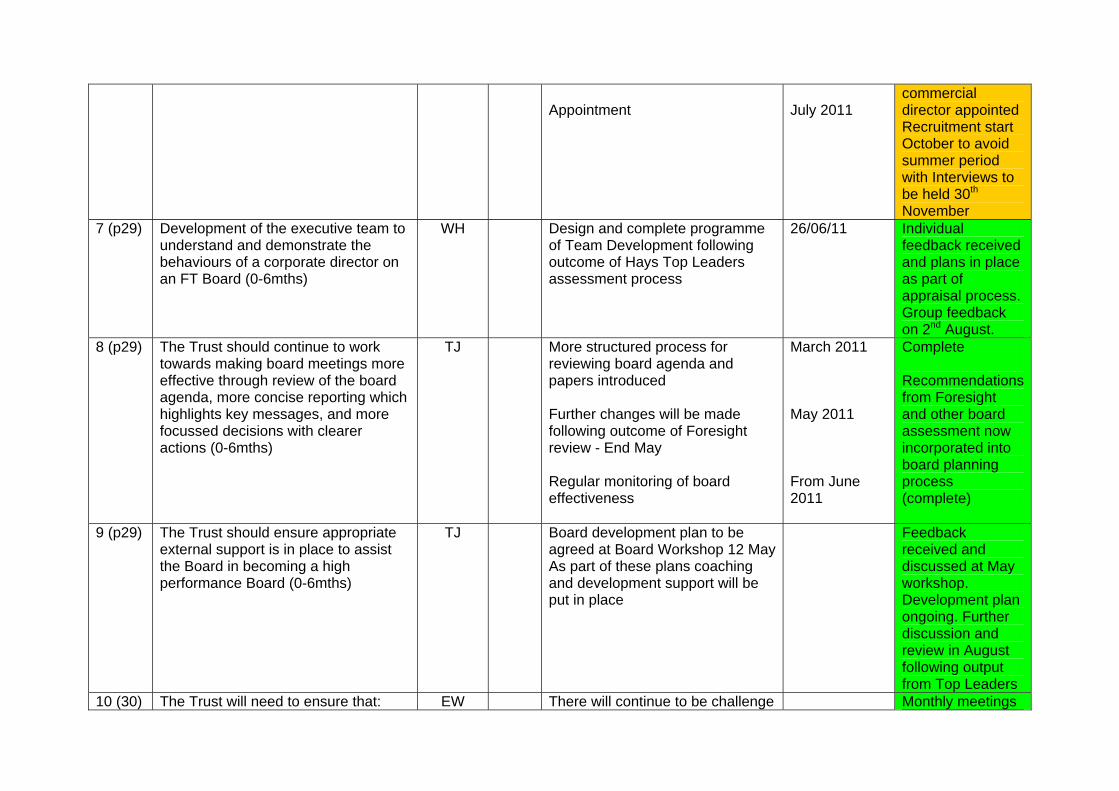
Appointment
July 2011
commercial director appointed Recruitment start October to avoid summer period with Interviews to be held 30th November
7 (p29) Development of the executive team to understand and demonstrate the behaviours of a corporate director on an FT Board (0-6mths)
WH
Design and complete programme of Team Development following outcome of Hays Top Leaders assessment process
26/06/11 Individual feedback received and plans in place as part of appraisal process. Group feedback on 2nd August.
8 (p29) The Trust should continue to work towards making board meetings more effective through review of the board agenda, more concise reporting which highlights key messages, and more focussed decisions with clearer actions (0-6mths)
TJ More structured process for reviewing board agenda and papers introduced Further changes will be made following outcome of Foresight review - End May Regular monitoring of board effectiveness
March 2011 May 2011 From June 2011
Complete Recommendations from Foresight and other board assessment now incorporated into board planning process (complete)
9 (p29)
The Trust should ensure appropriate external support is in place to assist the Board in becoming a high performance Board (0-6mths)
TJ Board development plan to be agreed at Board Workshop 12 MayAs part of these plans coaching and development support will be put in place
Feedback received and discussed at May workshop. Development plan ongoing. Further discussion and review in August following output from Top Leaders
10 (30) The Trust will need to ensure that: EW There will continue to be challenge Monthly meetings

within the revised Committee structure there is clarity of where formal scrutiny and challenge of financial reporting is undertaken and sufficient focus is maintained (ongoing)
at the Board and by the Audit Committee chair at the Finance meeting prior to each Board meeting.
continue prior to each Board
11 (30)
The Audit Committee should ensure that it is receiving sufficient assurance on the Trust’s progress in implementation of recommendations and this information is subject to periodic scrutiny by internal audit (0-3mths)
EW The progress on audit recommendations is reviewed by internal audit with the Director of finance prior to the audit committee meeting. Internal audit then cover this in the their report and show high importance recommendations which have not been implemented. More attention will be given to ensuring sufficient assurance.
This continues prior to each Audit Committee meeting, with focus on high priority recommendations at the Audit Committee meeting
12 (31)
There should be a continued focus on ensuring Committee roles are clear with BAF risks being fully covered (0-3mths)
TJ Com chairs
Board committee performance and terms of reference will be reviewed and assessed against BAF at next meeting of each and subsequent board
25 May 2011 Board committee members carrying out annual review of performance and TOR. These were presented to the July Board
13 (31) Performance of the new structure should be reviewed after a period of operation to ensure it is operating effectively and that the QSC is effectively undertaking the required role (0-6mths)
TJ New QSC terms of reference will be approved by board on 30 March Effectiveness of meeting will be regularly reviewed at meeting and board
30 March 2011 Ongoing
Further review following input from SHA and board assessment process. Final proposal was presented for approval to July board
14 (32)
The Trust should report to the Board on a more timely basis by reviewing the timing of Board meetings (0-6mths)
TJ The Board meetings have been moved to the fourth Wednesday of the month.
March 2011 Complete
15 (32) The Finance Report should continue CP DT New summary section introduced March 2011 Complete

to be refined with a focus on ensuring that the key messages are more clearly communicated (0-6mths)
with focus on cash. The report will continue to be improved on an ongoing basis.
16 (32)
The Trust should continue to progress the development of Service Line Reporting (SLR) (Ongoing)
CP DT We are continuing to improve the service line reporting with the focus on the commercial area ensuring cost allocations are correct.
Plan for SLR completed, discussed with Exec Sept 11, and Board in Oct 11
17 (33)
The Board should be provided with a 12 month rolling cashflow forecast as part of the monthly finance report (0-3mths)
CP ND This will be in place for March reporting
April 2011 Complete
18 (34)
The Trust should undertake a self assessment for compliance against the Monitor Code of Governance and address any areas for improvement (0-3mths)
JD Self assessment against Monitor Code of Governance to be undertaken and approved by the Board
May 2011 SA complete Board approval May
19 (35)
The Trust should keep reporting against standards and targets under review to ensure that it continues to comply with national and local requirements (Ongoing)
CP DT Agreed Complete
20 (35)
An Information Assurance Framework should be implemented to map the data and provide assurance on the data quality for different performance measures used by the Board used to report on performance against KPI’s (0-6mths)
CP DT Agreed Sept 2011 Plan in place as part of the IG 8 improvements
21 (35)
Forecast information in the Finance and Estates Report should be further developed to include a quantified analysis of risks/sensitivities to the forecast position (0-3mths)
CP DT The report has already been amended to include quantified risks on the front sheet. The forecast section will be further improved to clarify the risks to the forecast.
June 2011 Complete – incorporated in June 2011 report
22 (36) Reporting on performance on against CP DT Agreed for March reporting April 2011 Complete

CRES schemes should provide a split between recurrent and non-recurrent schemes (0-3mths)
23 (37)
The Trust should ensure action is taken to address weaknesses identified from the internal audit of the PTS contract (0-3mths)
IF VK Internal audit report due March 2011, implement improvement actions immediately but latest by May 2011.
May 2011 High priority actions implemented and audited.
24 (39)
The Trust should ensure there is sufficient detail to support suggested mitigations with detailed implementation plans and consideration of timescales and ownership (0-3mths)
CP The detail is complete. Plans with timescales to follow. Agreed
May 2011 Complete.
25 (40)
The Trust should review capital programme reporting to the Board to ensure it enables the Board to undertake appropriate scrutiny and challenge (0-3mths)
CP ND The Board reporting will be improved by giving greater clarity around variances to budget by project, and changes from the last forecast.
March 2011 Complete
26 (42)
The Trust will need to ensure that Financial Management support is structured to effectively support the operational divisions and that any changes have the desired impact (0-6mths)
CP DT We will adapt the structure ready for the implementation of the new operations structure
Sept 2011 Financial management is currently supporting the new operations structure. A revised structure will be consulted on as part of the corporate review.
27 (43)
The Trust should ensure that all improvement actions identified to address performance issues with the payroll service are fully addressed and overpayments recovered (0-6mths)
CP ND
SW
The overpayments are recovered over a period ranging from 1 month to 3 years. Receipts are in line with the individual recovery plans. The key actions still to be addressed are as follows: Introduction of SCAS wide expenses form to cover lease car holders
July 2011
Now expected in December due to

ND
ND
Access to Mckesson system that tracks outstanding issues to be improved Requests from Mckesson archives to be turned round within 4 weeks of request
June 2011 May 2011
consultation on mileage definition Partially achieved. Still further work required. Due Dec 11 Complete
28 (44)
The Trust should ensure that the controls weaknesses in accounts payable and journals highlighted by External Audit have been fully addressed (0-3 mths)
CP ND Already completed March 2011 Complete
29 (45)
The Trust should ensure that internal audit recommendations from the SLA/Debtors review and Standards for Better Health review are implemented and follow-up reviews undertaken to confirm concerns have been fully addressed (0-3mths)
CP
CP IF
SLA / debtors – significant contracts to be signed by April 2011 A&E by March 2011 Bucks and Berks PTS by April 2011 SfBH superseded by QQC standards registration
March 2011 April 2011
A&E contract signed Berks signed Letter received from Bucks with contract variation to be signed by Dec 11.
30 (48)
Management should initiate a project to remove all unsupported operating system software (0-6 mths)
CP VW A review of all operating systems and software has been instigated by the Head of ICT. We anticipate the removal of all unsupported by September 2011 across SCAS.
September 2011
Complete
31 (51)
Complete the planned work to ensure compliance to license agreements (0-6mths)
CP VW Subject to the NHS Enterprise Wide Agreement (EWAT) we anticipate having full visibility of deployed licences during the first quarter 2011/12 (connected with the introduction of the ICT Helpdesk system) During the second quarter action will be taken
September 2011
The EWAT Agreement nationally has not yet delivered a final outcome so this is delayed. They have requested further

to resolve any outstanding issues. information. Subject to the national agreement this is expected Q4 FY
32 (53)
A full BCP test for the Trust should be arranged (0-3 mths)
IF JD JD to scope which areas have been tested by 1st week April. Then tests will be carried out for untested areas by June 2011
30th June 2011
Tests for non ICT areas carried out during July. For ICT Bicester paper exercise commenced August, to be followed by desk top exercise with suppliers and planned outage in November with all parties involved.
33 (55)
A method to ensure 95% compliance with the requirement for Information Governance training will need to be developed (0-3mths)
CP VW A plan for achieving 95% by the end of June 2011 is required by the end of March to attain Level 2 IG8 – it is uncertain at this time whether such a plan can be agreed for all road staff. The longer term ambition to attain this level of IG score requires all staff to be tested annually. In March options for delivering this or to decide to set an alternative target will be reviewed. This proposal will then be taken to the Board in April for sign off
April 2011 Complete
STAGE 2 HDD ACTION PLAN
20 Make adjustments to the LTFM relating to CP AM 1 Custody Suite May 2011 Complete

normalising items 3 Flu pandemic 9 HQ move 13 A4C provision

commenced August, to be followed by desk top exercise with suppliers and planned outage in November with all parties involved.
33 (55)
A method to ensure 95% compliance with the requirement for Information Governance training will need to be developed (0-3mths)
CP VW A plan for achieving 95% by the end of June 2011 is required by the end of March to attain Level 2 IG8 – it is uncertain at this time whether such a plan can be agreed for all road staff. The longer term ambition to attain this level of IG score requires all staff to be tested annually. In March options for delivering this or to decide to set an alternative target will be reviewed. This proposal will then be taken to the Board in April for sign off
April 2011 Complete
STAGE 2 HDD ACTION PLAN
20
Make adjustments to the LTFM relating to normalising items
CP AM 1 Custody Suite 3 Flu pandemic 9 HQ move 13 A4C provision
May 2011 Complete

Enclosure: K (Agenda Item: 13)
Board Report
1st December 2011
Date 1 December 2011
Title Operations/Clinical Structure Review - Benefits Realisation Plan
Lead Director(s) Ian Ferguson and Fizz Thompson
Report Author(s) Ian Ferguson and Fizz Thompson
Purpose of the report
This paper updates on progress in the Ops/Clinical Structure Review and outlines the deployment plan to secure the benefits. It proposes a measurement system to track benefits realisation.
Recommendation (eg. Note, approve, endorse)
The Board is invited to: NOTE the progress made to date with the Review; NOTE that detailed deployment plans will be developed
for each new Area; AGREE the approach to benefits realisation; AGREE the approach to benefits measurement; and NOTE that the Board will be provided with monthly
progress updates.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
Links to Outcomes 1.4.6.7.8.9.11.12.13.16.17
1

Details of additional risks associated with this paper:
Risks for the Restructure programme are outlined in the project risk log. The Clinical and Operational restructure is on the corporate risk register
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
Links to all patient and staff rights
Financial implications/impact The savings as a result of the restructure are in the CIPs plans and we are on track to deliver the forecast agreed with the Board
Legal implications/impact None
Equality and Diversity implications/impact
None
Partnership working and public engagement implications/impact
The new structure will improve partnership working and engagement.
Other
Committees/groups where this item has been presented before
Operational/Clinical Review Structure Board and Senior Operations Team Executive team for comments
Other options available and their pros and cons
Progress monitoring and review Monthly reports to the Board are proposed
Background papers Previous Board report on Review
2

Operations/Clinical Structure Review Benefits Realisation Plan
Executive Summary
1. The vision for the Operational/Clinical Structure Review is to deliver
Better quality of care Better operational delivery and performance Better productivity and financial performance Improved assurance of organisational delivery
through teamworking and supportive leadership at the front line.
In addition, the new Area Manager structure will enable better engagement with external stakeholders through a more locally based focus.
This paper updates on progress and outlines the deployment plan to secure the benefits. It proposes a measurement system to track benefits realisation.
Introduction
2. In March 2011, we launched the Operational/Clinical Structure Review. There were 3 phases:
Phase 1 – Consultation Phase 2 – Appointment process Phase 3 – Deployment, staff development and benefit
realisation
3. The consultation phase ended as planned on 30 June although an extra 3 weeks were allowed for final comments. The appointments phase has progressed to time table and we have met the target of 90% of all affected managers, appointed by 30 October, ending with 98%. The deployment and staff development phase has now begun.
4. The restructure is on track to deliver the savings forecast agreed by the
Board, adjusted for the impact of the extra interim managers requested by the Board to protect service during the transition. This equates to £248k this year and £682k in the full year.
5. The Restructure is overseen by a Restructure Programme Board. There is
a detailed project plan and risk register for the project and the main risks are logged on the Board Assurance Framework and the Corporate Risk Register.
3

Deployment
6. By 1 November, the following restructure building blocks were in place:
Senior operations team Area managers Emergency Services Managers 90% of all appointments made New EOC structure Senior clinical team Qlikview producing new Area results ESR and KRONOS aligned to Areas Financial systems (proactis) aligned to areas Operational support help desk up and running Investigation unit in place
Staff Development
7. In addition, we will be supporting deployment by an extensive development programme designed to inspire and equip the new management team for the challenges ahead. This will include:
A series of launch events through November for all managers,
team leaders and clinical mentors designed to explain how the new structure will be different and what their new roles will be.
A leadership development cascade for all managers and team leaders that will enable them to reflect on and develop their leadership and team building skills.
A series of training interventions specifically built for the new job roles and designed to give managers the skills to do their new jobs.
A personal development programme tailored to the needs of each individual and built from a prospectus of development interventions that will be agreed by each manager, team leader and clinical mentor with their new line manager.
8. With these building blocks and development plans in place, we have now
invited the Area Managers to take on the challenge of deploying the aims and principles of the review and realising the benefits in their own Areas. Each Area is in a different position with different challenges. Equally, our new approach is to take forward the principles of the review by empowering managers and staff to make decisions for themselves within an agreed framework. It is therefore right to allow Area Managers and their teams to develop their own local plans for realisation of the benefits, tailored to their needs and opportunities. Area managers will therefore work up their local plans within a SCAS framework and have them approved by the end of November.
4

Benefits Realisation
9. The key task for the Area Managers will be to put together plans to deliver the benefits that will flow from the Review. The Review has been designed to strengthen teamworking and leadership at front line level. This will yield significant benefits by providing better support, clinical education and development, communication and engagement for our staff. These benefits have been grouped under 5 headings:
Quality Operational Performance Staff engagement Financial performance Leadership and culture
10. Details of how we will measure these benefits are in Annex A. Initially the
benefits will be set at Area level but they will be cascaded down to team level as the new structures evolve.
11. Key to successful benefits realisation will be the successful
implementation of teams. This is defined as: Team leaders in place Every team member tagged to the team leader Clinical mentor embedded in every team Performance, quality and clinical competence measured by
team Individual performance fed back to each team member Plans in place for team leader to work 2 shifts per year with
each individual Team regularly work together Quarterly team meetings planned
12. Area plans will be expected to deliver effective teams as defined and the
above criteria will be milestones in the plans against which progress will be tracked.
13. Area Managers will also be expected to engage effectively with a wide
range of local stakeholders. They will be empowered within an overall SCAS framework to work with local partners to tailor services to local needs – eg developing local care pathways, reducing hospital turnaround etc.
5

6
Annex A
Benefits Measurement
Area Team
Quality Clinical performance indicators including new care pathways (PCI, stroke and trauma)
Patient experience feedback See and treat % Improvement in the priority areas of
the quality accounts Improved management of risk
through incident reporting and feedback to staff
Increased safeguarding reporting
Clinical performance indicators Patient experience feedback See and treat % Evidence of staff clinical
competence Improved management of risk
through incident reporting and feedback to staff
Increased safeguarding reporting
Operational performance
Hospital clear up times Mobilisation times
Hospital clear up times Mobilisation times
Staff engagement % appraisals completed % training completed Employee Opinion Survey (EOS) -
staff engaged
% appraisals completed % training completed
Financial performance Sick absence Delivery of CIP’s Job cycle time
% return to work interviews carried out
Job cycle time
Leadership and culture Reduction in staff grievances EOS – support from line manager Positive feedback from leadership
walk rounds
External stakeholder engagement
Local CQUIN plans in place

closure: L En (Agenda Item: 14)
Board Report
1st December 2011
Title Strategic Risk Register and Board Assurance Framework - Six Month Review
Lead Director Fizz Thompson, Director of Patient Care
Report Author Fizz Thompson
Purpose of the report To provide an update on the Strategic Risk register and Board Assurance Framework
Recommendation (eg. Note, approve, endorse)
The Trust Board is asked to receive and NOTE the report.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
Links to all CQC registration and Essential Standards
Details of additional risks associated with this paper:
All clinical risks are detailed in the Trust risk register that link to the quality work streams
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
All areas of Patient Rights
Financial implications/impact None
Legal implications/impact
Equality and Diversity implications/impact
None identified
Partnership working and public engagement implications/impact
Quality and Patient Safety work streams are shared with commissioners and stakeholders through regular updates and meetings and performance shared through the Integrated Performance Report

Other
Committees/groups where this item has been presented before
Progress of the Quality and Patient Safety work streams is monitored through the Executive Team, the Quality and Safety Committee and through Serious Incident Review group
Other options available and their pros and cons
Not applicable
Progress monitoring and review Further monitoring of the Strategic Risk Register and Board Assurance Framework is undertaken by the Executive Management Committee, the Quality and Safety Committee and the Audit Committee
Background papers The Strategic Risk Register and Board Assurance Framework are provided as appendices to this document.
Introduction The Strategic Risk register and Board Assurance Framework are provided to update the board on the position with the risks to the organisation and also with achieving the strategic objective set out in the business plan. The two documents also provide evidence for the trust’s statement of internal control, provide a focus for performance management and the development of actions to address the areas of concern. A summary sheet of the Strategic Risk Register and Board Assurance Framework has been developed to provide an overview of the levels of risk and a half yearly position

Ref No BAF no.
Date Identified
Date of Latest Update
Description of Risk Likely Outcomes for SCAS Category
ImpactProbabili
tyRisk
Score
Counter-measuresRevised Impact
Revised Probabili
ty
Revised Risk
Score
Timescale Owner/ Director
Author Investigation Allocated to
Risk Status
Supporting Evidence for mitigation
(1-5) (1-5) (I*P)Brief description of the risk. Brief description on what would occur if the risk
happens.What is the risk type? E.g. Economic / Financial / MarketLegal / RegulatoryOrganisational / Management / Human FactorsPoliticalEnvironmentalTechnical / Operational / Infrastructure
What will be the consequences on the prog/ project/ organisat-ion IF the risk were to occur.
What is the likelihood of the risk occurring?
Combined risk score (impact X probability)
What actions have been taken/will be taken to counter this risk? Accept / Reduce / Transfer / Prevent / Contingency
Rev by Project Board
Rev by Project Board
Rev by Project Board
When is the risk likely to occur?
Who has been appoint-ed to keep an eye on this risk?
Who submit-ted the risk?
Open Descending Ascending New Closed
1) Inability to track, age and replacement ,repair, schedules for equipment leading to outdated equipment remaining in use
1) Compilation of computerised data sheets and an asset register is in progress and near completion
1) Clinical Review Group monitor progress of Equipment Committee and report up to the Q&S highlighting risks and issues
2) Incomplete Asset management register 2) RFID system due to roll out via Make Ready service to track and monitor all equipment
2) Incidents reported through equipment group and CRG
3) Risk to patient safety and care through equipment not working
3) Incident reporting system highlights trends and issues 3) Action plan
4) Investigations in to faults and work round or solutions found 4) Hot new and memos
5) Alerts and communication sent to staff when equipment and vehicle faults are identified 6) Evidence provided that staff have read and understood information 7) Information cascaded to other trusts
Breach of obligations under the Medicines Act and Misuse of Drugs Act
1) Medicines Management action plan in place and monitored through the Clinical Review Group
Monitored through the Clinical Review Group and Quality and Safety Committee
2) Medicines Management Adviser monitors storage and control of drugs through resource centre audits
3) Medicines management clearly outlined in medicines management strategy
Potential serious risks to patients and poor long term outcomes
1) Business case in development.
Trauma network to be developed in South Central to develop and monitor system wide progress
2) Tabled at the CRG to be forwarded to Executive Committee and Quality and Safety Committee. Presentation to Trauma Network Confirm & Challenge event and Trust board
Tracked through Executive Team, Trauma boards and Trust board
3) Integrated governance framework developed for pre hospital critical care4) Appointment of programme manager todevelop and implement pathways
1) Lack of staff development and education 1) Clinical metrics will support the measurement of clinical standards and provide a focus for continuous improvement programmes
Minutes of the Quality and Safety Committee demonstrate this process.
2) Poor patient experience in their pre-hospital care
2) The quality of care is monitored through Quality and Safety Committee. Audit of practices occur on a quarterly basis.
Patient Safety and Clinical Quality is now an agenda item on the Board agenda
3) Increased risk of civil action for clinical negligence
3) Clinicians are being developed to provide leadership and supervision to all staff whilst being clinical champions in their chosen speciality
Managers training programme to enable leadership to be fostered.
4) Increased incidence of adverse media 4) SCAS is now one of the leaders I the country however sustainability needs to be maintained.
Action plans in place to improve quality indicators
new quality indicators now providing more Integrated performance report.Audits on delays and patient records.Leadership walk rounds.
1) Poor stakeholder perception 1) Delays in delivery of care monitored at EOC level on a daily basis Level 2 and 3 meetings documented and actions tracked
2) Increased patient suffering 2) RCA at divisional level 2 meetingsDelays monitored through Integrated Performance Report at Board, executive, divisional and station level through the use of Qlikview
3) Non compliance with national targets 3) Actions put in place to improve performance and responses – evaluated at next level 2
rnadom reviews of pateitn care records of delayed responses
4) Patient safety issues 4) Monitoring of all delays at Level 3 trust wide meetings and through Integrated Performance Report
CORPORATE RISK 1 - QUALITY OF CARE, PATIENT OUTCOMES, SAFETY, EXPERIENCE AND EXCELLENCE
FT FT OpenJan-12
65 1.10 transferred from old register
FT164452 1.11 transferred from old register 06/11/2011
06/11/2011 FT FTregulatory clinical 4
Failure of clinical equipment and to provide assurance of servicing, maintenance, replacementand repair.
4 2 8
Open3 2 6
93 Inc. 94 1.6 transferred from old register 06/11/2011 Open
FT FT FT open
Apr-12 JB JB
Open
6
2 23 4
regulatory clinical
2
Availability of medical carein the pre hospital environment to enable seamless interventions whereby the patient receives the most appropriate referral i.e. PPCI referral and stroke care
Failure to provide effective systems for the storage and management of medicines
12
124clinical
8
3
2
Failure to provide and manage the quality of care, patient outcomes, safety and experience
Delays in the delivery of care to patients due to poor performance resulting in morbidity or poor patient experience
regulatory clinical 44 1.1 transferred from old register 06/11/2011
FT FT1.6 transferred from old register 3 312104 Inc. 79 93regulatory clinical 406/11/2011
FT
JB
FT
3

Ref No BAF no.
Date Identified
Date of Latest Update
Description of Risk Likely Outcomes for SCAS Category
ImpactProbabili
tyRisk
Score
Counter-measuresRevised Impact
Revised Probabili
ty
Revised Risk
Score
Timescale Owner/ Director
Author Investigation Allocated to
Risk Status
Supporting Evidence for mitigation
(1-5) (1-5) (I*P)Brief description of the risk. Brief description on what would occur if the risk
happens.What is the risk type? E.g. Economic / Financial / MarketLegal / RegulatoryOrganisational / Management / Human FactorsPoliticalEnvironmentalTechnical / Operational / Infrastructure
What will be the consequences on the prog/ project/ organisat-ion IF the risk were to occur.
What is the likelihood of the risk occurring?
Combined risk score (impact X probability)
What actions have been taken/will be taken to counter this risk? Accept / Reduce / Transfer / Prevent / Contingency
Rev by Project Board
Rev by Project Board
Rev by Project Board
When is the risk likely to occur?
Who has been appoint-ed to keep an eye on this risk?
Who submit-ted the risk?
Open Descending Ascending New Closed
5) Non delivery of clinical excellence 5) Safety reviews of Patient Care records undertaken to identify poor and sub standard practice - actions put in place toimprove delivery of care
1) Lack of access to clinical outcomes from Acute Trusts
1) Electronic patient records being rolled out across SCAS and the development of the CARS system in relation to identification of Demand Management
Whole systems working with Unscheduled Care Boards to work to QIPP agenda
2) Commissioning data not sufficient to explain increasing demands on SCAS service
2) Commissioning to request access for their analysts to review data from inpatiensettings
Integrated Performance Report provides data and information on progress
3) Clinical records paper based 3) New national standards now in place Demand management managed through programme of work under Business Programme Board and Executive Team
4) Inability to accurately assess pre hospital care and its attendant outcomes
4) Links being made to local Acute Trusts to obtain outcome data for cardiac arrest
5) Patients at risk registers in place to highlight whole systems issues and priority work areas6) Emerging new unscheduled care groups/boards with QIPP plans
1) Poor patient experience in their pre-hospital care
1) Education and training of staffReporting of incidents, RCA’s
2) Increased risk of civil action for clinical negligence
2) Root cause analysis of incidents and application of learning. Complaints feedback
3) Increased incidence of adverse media 3) Provision of assessment criteria for staff. PRF review of non conveyance
4) Potential SUIs and legal claims 4) Review of patient care records Development of new care pathways 5) Plans in place to increase GP triage, and CSD hear and treat and improve deployment of ECP’s
Implementation GP triage
1) Poor patient care, adverse publicity, financial penalties for underperforming against contracted levels
1) Measurement system in place for all indicators Minutes of Business Plan Programme Board and Level 3s
2) Initial benchmarking shared nationally Report on SCAS performance v new indicators, assessment against benchmarking data and improvement plans for each area
3) SCAS is generally performing well against the indicators, and the top 3 performing Trusts for A8, telephone resolution and frequent users Action plans in place for areas of improvement 4) Improvement plans in place for all otheindicators, especially Time to Treatment and call answering.5) Common telephony system implemented in September, which has resulted in improved performance against call answering but still need to exploit benefits of new system6) Monitoring in place through national Benchmarking, IPR and Qlikview7) Meetings with HOSCs and commissioners in September and Octobeto explain new indicators and implications
Poor patient care experience, adverse publicity, financial penalties, adverse impact on response times and delays in getting to patients
1) Incoming patient screens and electronic handover recording systems have been installed at A&E departments. Reports on Qlikview
2) Joint hospital escalation plans have been agreed with PCTs and local hospital management.
escalation plans in place
3) Joint workshops for ambulance, hospital, PCT management have been organised.
engagement plans in place with stakeholders and commissioners
4) Training exercises will be run for SCASmanagement in how to respond when escalation plans are being used.
CORPORATE RISK 2 - EMERGENCY PERFORMANCE COMMERCIAL VIABILITY AND OPERATIONAL EXCELLENCE
4 3 open3 FT12 12 FT FT4
Insufficient clinical data regarding demand profile and clinical outcomes
regulatory clinical5 transferred from old register 06/11/2011
openFT FT FT14 4 323/03/2011 06/11/2011
Risk of patient safety and outcome from assessmentand non-conveyance of patients to other health provider
operational 4
12 63 2regulatory clinical
IF3
Failure to perform well against the new national quality performance indicators which were implemented from 1 April 11
2.1 10/11/2011 3 312 openIF IF
Failure to manage and eradicate ambulance turnaround delays at A&E departments
9

Ref No BAF no.
Date Identified
Date of Latest Update
Description of Risk Likely Outcomes for SCAS Category
ImpactProbabili
tyRisk
Score
Counter-measuresRevised Impact
Revised Probabili
ty
Revised Risk
Score
Timescale Owner/ Director
Author Investigation Allocated to
Risk Status
Supporting Evidence for mitigation
(1-5) (1-5) (I*P)Brief description of the risk. Brief description on what would occur if the risk
happens.What is the risk type? E.g. Economic / Financial / MarketLegal / RegulatoryOrganisational / Management / Human FactorsPoliticalEnvironmentalTechnical / Operational / Infrastructure
What will be the consequences on the prog/ project/ organisat-ion IF the risk were to occur.
What is the likelihood of the risk occurring?
Combined risk score (impact X probability)
What actions have been taken/will be taken to counter this risk? Accept / Reduce / Transfer / Prevent / Contingency
Rev by Project Board
Rev by Project Board
Rev by Project Board
When is the risk likely to occur?
Who has been appoint-ed to keep an eye on this risk?
Who submit-ted the risk?
Open Descending Ascending New Closed
5) Despite work with the hospitals over the past two years, several hospitals in the SCAS region, are starting to experience bed blocking due to delayed transfer of care which SCAS has no control over. This has been escalated to Chairman level. This has a negative impact on handover times (arrival at hospital to patient handover) and affects the ability of SCAS to respond to outstanding emergencies.
6) Using Qlikview, we can now drill down to individual staff member for delay performance7) Clear up times (handover to clear hospital) have improved significantly.8) Issue of hospital handover raised with external commissioners
Could adversely impact on patient care, performance and reputation
1) We are working with National Operations Directors to assess the likely requirement to support LAS and distributethat equitably among the other English services.
Agreed Numbers to LAS 7 Paramedics, 5 Technicians and 3 ECA’s.Agreed Backfill by Private providers.
2) We have formed an Olympic planning board to ensure that we have robust plansin place to mitigate any risks.
2.3 10/11/2011
New operational/clinical structures may have an adverse impact on the delivery of operational andclinical service
possible adverse effects on locality performance
operational 4 4
1)restructure board monitoring progress
4 3 IF IF IF open
poor staff morale 2) risk register and mitigating action plan in place
possible issues with reduction in leadership prescence across the trust
3) Launch and leadership development plans in place4) Area Managers developing plans to embed the new structures and secure the benefits
Could adversely impact on patient care, performance and reputation
1) We have a clear resourcing plan that ismatched to demand and integrates recruitment with abstractions and private providers
OPAS
2) We have identified learning from previous years and built into our plans REAP
3) We have reviewed our REAP plans Hospital clear times from Qlikview4) A&E turnaround project is delivering a reduction in clearance times CSD stand downs
5) Introduction of KRONOS will give us better control over hours deployed.6) We have expanded role of CSD and they now afford the opportunity for giving greater resilience if needed.
Poor reputation amongst stakeholders. 1) The development of a stakeholder strategy including: a) Stakeholder engagement plan; � Media plan; b) Staff Ambassador plan; c) Public Engagement plan; d) Issues and Crisis management plan; e) Strategy has been strengthened by separate plan for developing relationships with GPs and Local Authorities (potential commissioners)
Risk to Foundation Trust application 2) The development of stakeholder management process including: a) Database; b) Stakeholder conference calls; c) Programme of stakeholder visits; d) Quarterly stakeholder visits
Relationship with CQC (new regional contacts)
3) Develop working relationship with CQC regional contacts
CORPORATE RISK 3 - STAKEHOLDER PERCEPTIONS AND TRUST REPUTATION
3 3 open612 2 DB DB
10/11/2011 12
100 06/11/2011
Failure to engage fully withstakeholders and to build effective relationships leading to enhanced organisational reputation
4
operational
Inadequate resources and resilience to meet demand
2.2 4 34 4 16 openIF IF IF
2 IF IF IF
16
operational 312 01/01/2011 10/11/2011
Need to provide support toLAS during the Olympic Games plus the need to handle our own Olympic events. 62 2 1
1210/11/2011
12
3 3 IF IF openoperational 3 4 9 IF

Ref No BAF no.
Date Identified
Date of Latest Update
Description of Risk Likely Outcomes for SCAS Category
ImpactProbabili
tyRisk
Score
Counter-measuresRevised Impact
Revised Probabili
ty
Revised Risk
Score
Timescale Owner/ Director
Author Investigation Allocated to
Risk Status
Supporting Evidence for mitigation
(1-5) (1-5) (I*P)Brief description of the risk. Brief description on what would occur if the risk
happens.What is the risk type? E.g. Economic / Financial / MarketLegal / RegulatoryOrganisational / Management / Human FactorsPoliticalEnvironmentalTechnical / Operational / Infrastructure
What will be the consequences on the prog/ project/ organisat-ion IF the risk were to occur.
What is the likelihood of the risk occurring?
Combined risk score (impact X probability)
What actions have been taken/will be taken to counter this risk? Accept / Reduce / Transfer / Prevent / Contingency
Rev by Project Board
Rev by Project Board
Rev by Project Board
When is the risk likely to occur?
Who has been appoint-ed to keep an eye on this risk?
Who submit-ted the risk?
Open Descending Ascending New Closed
Contract negotiations delayed. 1) Ensuring we maintain a balance between relationships with existing relationships and building relationships with new commissioners.
stakeholder engagement plan
Uncertainty in commissioning relationships 2) Continuing to meet with external review board and specialist commissioning to develop contract for 2011/12.
GP engagement through 111 discussions
1) Risk to progression towards Foundation T 1) Extensive FT membership and consultation plan implemented and on track. plans in place for inducation and preparation for governors 2) Supported by Continual relationship with PCTS to ensure their support with the application. Membership secretary implementing membership plan
1) Closer external scrutiny 1) CIPs included on 100 day plan2) Loss of access to become an FT. 2) Strengthened CIP governance tracking
process implemented.finance and CIP recovery plan
3) Reputation issues 3)Monthly reviews of Commercial Division
Monitoring through project board and executive team
4) non recovery of bad debts 4) Divisions to ensure deliver of plan Service Line reporting introduced5) Increased performance management olate payments and debtors
1) Loss of access to become an Ft 1) Updated version of LTFM March 2011 LTFM revewied and deveveloped in line with IBP
2) Closer external scrutiny 2) Consultation with DH on key issues Dec 2010 and again in May 2011
3) Reputation issues 3) Change LTFM following feedback from SHA and DH4) Further changes June 2011 relating to new monitor assumptions
90 06/11/2011
Failure to provide suitable premises particularly in relation to stand by points and staff facilities
1) Health and Safety of staff possible leagisaltive issues
regulatory 4 2 8
1) Delivered new Hart station Jan 2011. estates strategy review improvement plan in place for resource centres 3 2 6 CP CP
estate improvement action in place
1) Price competition with other ambulance providers
1) Develop organizational delivery action plan
engagament plans in place with South Midlands locality and acute and primary care providers
2) Possible loss of income 2) Work with PCT’ to ensure delivery of best care
3) Destabilization of the health economy 3) Review pathways of care across borders
4) Potential clinical risks due to need to develop new clinical pathways
4) Maintain excellent working relationshipswith bordering trusts and commissioners
1) Inability to provide required surplus 1) CIP’s tracked through business programme board and Executive team
CIP plan in place monitored by CIP board and Executive meeting
2) Risk to achieving year end budget 2) Quality impact assessment undertaken
3) Potential risks to service delivery if further savings required1) Potential disruption to radio servicing and provision of equipment
1) Review of premises and scoping of alternatives
2) Reduction in input from community responders
2) Identify plan for renew of lease
3) Reduced maintenance of vehicles 3) Identify plan for move of fleet and radio resources
4) Potential financial risk 4) Plan for additional support for CFR
1) Loss of staff motivation 1) Education and training programme has been developed and approved and is being rolled out across the Trust.
Updated Recruitment Plan
2) Reduction in staff competency 2) nduction contains mandatory training for all new staff – plan in place for completion for all staff by June 2011 IBP Section 8 - Training Plan
3) Breach of statutory duties under health and Safety legislation
3) Engagement with operations to produce staff release action plan. Statutory and Mandatory training plan
4) Increased risk of clinical negligence claims
4) Integrated work force plan provides staff v training v budget
Integrated Workforce plan monitored through Workforce Board, Executive Team and Quality & Safety Committee
CORPORATE RISK 4 - COST PRESSURES RELATED TO THE ECONOMIC CLIMATE AND CHANGES IN THE WIDER HEALTH ECONOMY. INTEGRATED GOVERNANCE AND 'VALUE FOR MONEY'
CORPORATE RISK 5 - WORKFORCE AND DEVELOPMENT, LEADERSHIP AND CULTURE
12 6 CP
open69 3 235 WH/ SW WH/SW5.2 06/11/2011
Failure to provide access to education and training to meet mandatory, clinicaand organisational needs
3
12
Failure to renew building leases
financial 4 3
3
63 2 CP06/11/2011
3 3 2
68
06/11/2011
Failure to realize the cost improvement plans (CIP’s)
financial 4
CP CP3 206/11/2011
Possible loss of part of theA&E contract
financial 4 2
CP open9
Inability to develop a viableLong Term Financial Model (LTFM) approved by the DH & Monitor
3 CP12 3financial 4 313 4.1.1 05/01/2011 06/11/2011
CP open153 CP
12 6
20 571 06/11/2011
Failure to achieve financiatargets including lack of payment of debts and late payment of income streams and impact this will have on gaining FT status
financial 5 4
10 04/01/2011 06/11/2011 4 3
Failure to ensure well briefed and inducted council of governors and increase numbers of Foundation Trust members
open69
openDB DB3 2
DB DB3 3 3 2
Risk that commissioners will go into a period of unsustainability due to coalition changes and uncertainty for the future as a result of the White Paper and Forthcoming spend review.
7 06/11/2011
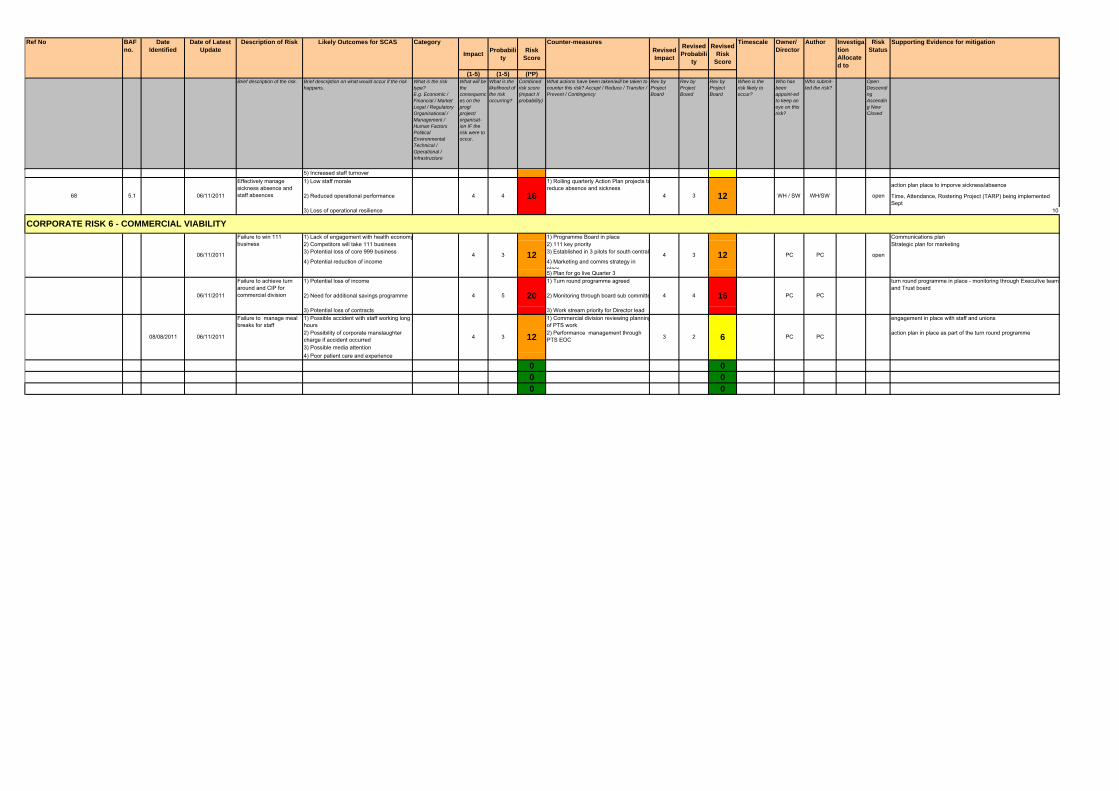
Ref No BAF no.
Date Identified
Date of Latest Update
Description of Risk Likely Outcomes for SCAS Category
ImpactProbabili
tyRisk
Score
Counter-measuresRevised Impact
Revised Probabili
ty
Revised Risk
Score
Timescale Owner/ Director
Author Investigation Allocated to
Risk Status
Supporting Evidence for mitigation
(1-5) (1-5) (I*P)Brief description of the risk. Brief description on what would occur if the risk
happens.What is the risk type? E.g. Economic / Financial / MarketLegal / RegulatoryOrganisational / Management / Human FactorsPoliticalEnvironmentalTechnical / Operational / Infrastructure
What will be the consequences on the prog/ project/ organisat-ion IF the risk were to occur.
What is the likelihood of the risk occurring?
Combined risk score (impact X probability)
What actions have been taken/will be taken to counter this risk? Accept / Reduce / Transfer / Prevent / Contingency
Rev by Project Board
Rev by Project Board
Rev by Project Board
When is the risk likely to occur?
Who has been appoint-ed to keep an eye on this risk?
Who submit-ted the risk?
Open Descending Ascending New Closed
5) Increased staff turnover1) Low staff morale 1) Rolling quarterly Action Plan projects to
reduce absence and sickness action plan place to imporve sickness/absence
2) Reduced operational performance Time, Attendance, Rostering Project (TARP) being implemented Sept
3) Loss of operational resilience 10
1) Lack of engagement with health economy 1) Programme Board in place Communications plan2) Competitors will take 111 business 2) 111 key priority Strategic plan for marketing3) Potential loss of core 999 business 3) Established in 3 pilots for south central
4) Potential reduction of income 4) Marketing and comms strategy in place5) Plan for go live Quarter 3
1) Potential loss of income 1) Turn round programme agreed turn round programme in place - monitoring through Execuitve team and Trust board
2) Need for additional savings programme 2) Monitoring through board sub committe
3) Potential loss of contracts 3) Work stream priority for Director lead1) Possible accident with staff working long hours
1) Commercial division reviewing planningof PTS work
engagement in place with staff and unions
2) Possibility of corporate manslaughter charge if accident occurred
2) Performance management through PTS EOC
action plan in place as part of the turn round programme
3) Possible media attention4) Poor patient care and experience
0 0 0 0 0 0
CORPORATE RISK 6 - COMMERCIAL VIABILITY
12 63 2
PC
PC PC
PC PC
08/08/2011 06/11/2011
Failure to manage meal breaks for staff
34
Failure to achieve turn around and CIP for commercial division 4 4 162006/11/2011
12
54
4 3 4 3 PC
open
Failure to win 111 business
06/11/2011 open12
4 4 124 316
Effectively manage sickness absence and staff absences68 5.1 06/11/2011 WH / SW WH/SW

Impact
Insignificant (1) 1 2 3 4 5
Minor (2) 2 4 6 8 10
Moderate (3) 3 6 9 12 15
Major (4) 4 8 12 16 20
Catastrophic (5) 5 10 15 20 25
1 to 3 4 to 7 8 to 14 15 to 25
Likely (4)Almost
certain (5)
Coding risk scores
ProbabilityRare (1) Unlikely (2)
Possible (3)
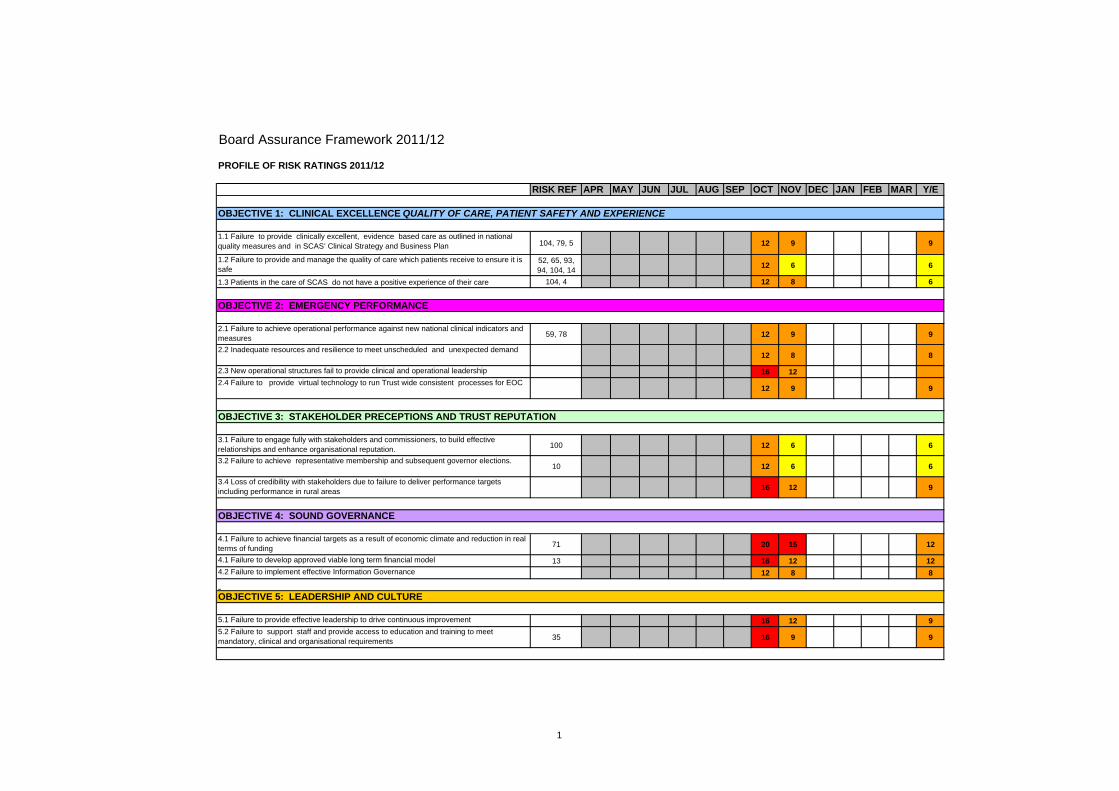
Board Assurance Framework 2011/12
PROFILE OF RISK RATINGS 2011/12
RISK REF APR MAY JUN JUL AUG SEP OCT NOV DEC JAN FEB MAR Y/E
1.1 Failure to provide clinically excellent, evidence based care as outlined in national quality measures and in SCAS’ Clinical Strategy and Business Plan 104, 79, 5 12 9 9
1.2 Failure to provide and manage the quality of care which patients receive to ensure it is safe
52, 65, 93, 94, 104, 14
12 6 6
1.3 Patients in the care of SCAS do not have a positive experience of their care 104, 4 12 8 6
2.1 Failure to achieve operational performance against new national clinical indicators and measures 59, 78 12 9 9
2.2 Inadequate resources and resilience to meet unscheduled and unexpected demand 12 8 8
2.3 New operational structures fail to provide clinical and operational leadership 16 12
2.4 Failure to provide virtual technology to run Trust wide consistent processes for EOC 12 9 9
3.1 Failure to engage fully with stakeholders and commissioners, to build effective relationships and enhance organisational reputation. 100 12 6 6
3.2 Failure to achieve representative membership and subsequent governor elections.10 12 6 6
3.4 Loss of credibility with stakeholders due to failure to deliver performance targets including performance in rural areas 16 12 9
4.1 Failure to achieve financial targets as a result of economic climate and reduction in real terms of funding 71 20 15 12
4.1 Failure to develop approved viable long term financial model 13 16 12 12
4.2 Failure to implement effective Information Governance 12 8 8
5.1 Failure to provide effective leadership to drive continuous improvement 16 12 9
5.2 Failure to support staff and provide access to education and training to meet mandatory, clinical and organisational requirements 35 16 9 9
OBJECTIVE 1: CLINICAL EXCELLENCE QUALITY OF CARE, PATIENT SAFETY AND EXPERIENCE
OBJECTIVE 2: EMERGENCY PERFORMANCE
OBJECTIVE 3: STAKEHOLDER PRECEPTIONS AND TRUST REPUTATION
OBJECTIVE 5: LEADERSHIP AND CULTURE
OBJECTIVE 4: SOUND GOVERNANCE
1

Board Assurance Framework V1 – 21.11.11
1
Board Assurance Framework
21 November 2011
Version 1
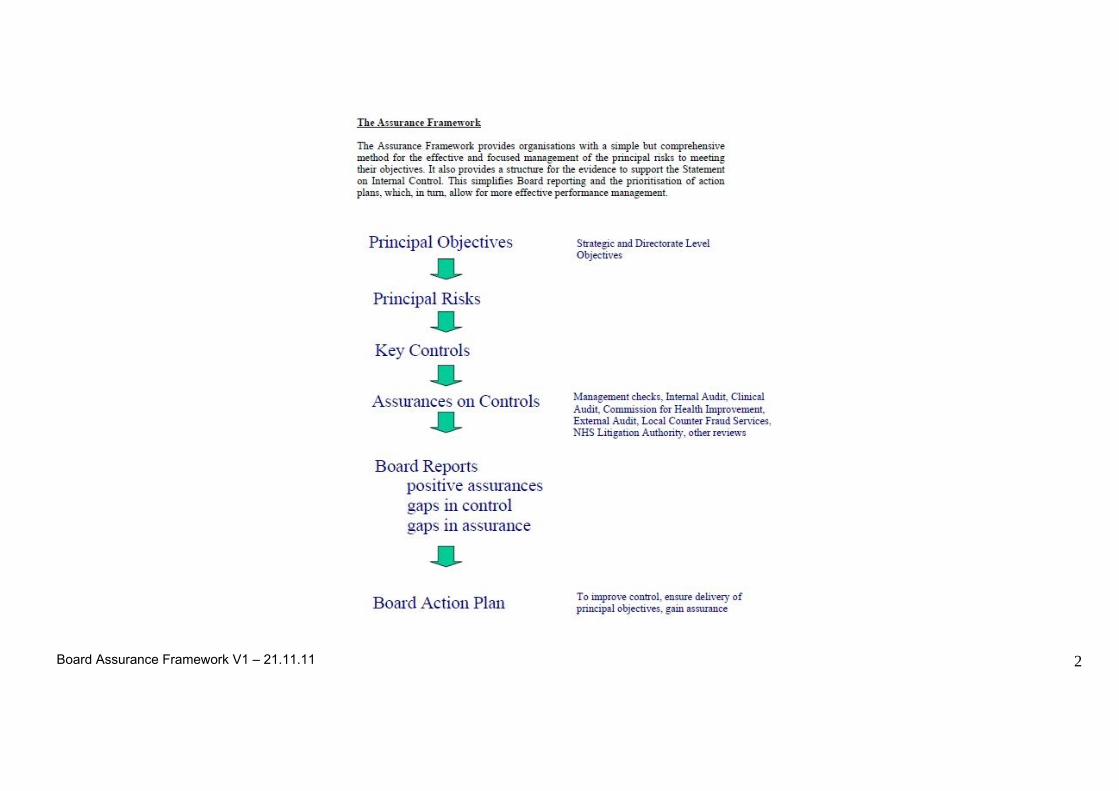
Board Assurance Framework V1 – 21.11.11
2

Board Assurance Framework V1 – 21.11.11
3
Whole Systems Assurance Framework
Responsible Exec Director
Principle Risk Risk Ref Ref to CQC Stds
Level of Risk before mitigating
risks
Key controls Positive Assurances Ass Level Gaps in Control Gaps in Assurance Actions
planned/update
No What could prevent this
objective being achieved
What controls/systems, we have in place to assist in securing
delivery of the objective
We have evidence that shows we are reasonably managing our risks and
objectives are being delivered
RAG rating
Where we are failing to put controls/systems in place.
Where we are failing in making them effective
Where we are failing to gain evidence that our controls/systems, on
which we place reliance, are effective
Dates, notes on slippage or
controls/assurance failing
Assurance Level: Effective controls definitely in place and Board satisfied that appropriate assurances are available = GREEN (=Add review date) Effective controls thought to be in place but assurances are uncertain and/or possibly insufficient = AMBER
Effective controls many not be in place and/or appropriate assurances are not available to Board = RED (NB The Board will need to periodically review the GREEN controls/assurances to check that these remain current/satisfactory).
Objective:1 Clinical excellence Quality of care, patient safety and experience
1.1 Fizz Thompson, Director of Patient Care John Black Medical Director
Failure to provide clinically excellent, evidence based care as outlined in national quality measures and in SCAS’ Clinical Strategy and Business Plan
104/ 79 5
Regulation 9. Outcome 4 Care and welfare of people who use services
12 CQC essential standards
DH quality indicators and measures
Quality accounts JRCALC guidelines CAS Clinical Strategy Trust Board and
Quality and Safety Committee assures clinical and quality governance processes
Audit committee reviews and cross references quality domain
Executive Team monitors all quality and clinical processes and policies and performance
Internal audit reviews of processes
Clinical Review Group reviews and
All front line staff have JRCALC manuals and pocket books
PCI indicators benchmarked nationally – performing above national measures May 2011
Individual scorecard for staff through the CARS system
Performance, complaints and incidents reviewed by the PERG and Quality and Safety Committee
CQC compliance with Essential Standards
Cycle 5/6 CPI performance rated 3rd nationally June 2011 awaiting cycle 7 results
Patient experience surveys covering CSD, front line and non emergency transport - annual
9
Improvement notice on Reg 9 outcome 4 and compliance notice on Reg 23 outcome 14. –now removed by CQC New National Standards and Clinical outcomes – first results show above average performance
- action plan in place for STEMI and stroke (in IPR) rate SCAS performance mid table
New trauma network to be implemented in 2011/12 – new processes, technology and training to be implemented by SCAS before activation of new pathway
Insufficient clinical outcome data - now addressed for cardiac arrest survival to discharge
None identified Currently third nationally for clinical performance and first for operational Red 8 performance Clinical audit plan in place Action plan to develop mew measures for national quality indicators including outcomes Project plan to develop new processes, training and preparation for trauma network

Board Assurance Framework V1 – 21.11.11
4
sub committee develops new policy
Integrated performance report
Processes and education for all staff to raise awareness
Monitoring of clinical work streams through Business Programme Board
Quality and clinical metrics embedded in Integrated Performance Report
CQC Quality Risk Profiles
New evidence supporting new care pathways (STEMI, stroke and trauma)
Review of operational and clinical structures will improve clinical leadership at the front line
survey plan in place New integrated
performance report has clinical metrics monitored through Trust Board
Research and development strategy in place with research resource developing
Clinical Audit plan in place May 2011
Internal audit provided substantial assurance against CQC standards
External clinical peer review demonstrated high standards of care may 2011
New pathways of care in place for PCI. And Stroke with demonstrated outcome benefits
New quality indicators providing information on outcome measures
1.2 Failure to
provide and manage the quality of care which patients receive to ensure it is safe
52,65,93, 94, 104,14
Regulation 9. Outcome 4 Care and welfare of people who use services
12 CQC essential standards
DH quality indicators and measures
IPR Quality accounts Trust Board and
Quality and Safety Committee assures clinical and quality governance processes
Audit Committee reviews and cross references quality domain
Executive Team
Complaints and concerns reduced 2010/11 – increase in reported complaints April, May
SUI’s reduced in 2010/11
Incidents reported increased demonstrating more open and learning culture may 2011 newsletter
Information on complaints and incidents shared with staff as case studies to
6
Potential risks identified with not conveying patients. Mitigating actions in place to support front line and CSD staff in safe assessment, treatment, advice and onward referral - care plans, GP triage, falls referrals, GP auto referral, EPRF
None identified Care pathways work stream in place to increase new care pathways and associated technology and processes to support the patient journey

Board Assurance Framework V1 – 21.11.11
5
monitors all quality and clinical processes and policies and performance
Internal audit reviews of processes
Clinical Review Group reviews sub committee develops new policy
Corporate and operational risk registers with clear risk management processes and policies
Random reviews of patient care records tracked through reporting lines
RCA processes to analyse incidents and identify learning
Clear accountability lines across the organisation for patient safety
Delays in response performance managed
Education programmes applicable to roles now planned and being implemented through Integrated Workforce plan
Patient safety metrics embedded in Integrated Performance Report
Support staff to help in assessment and decision making - care plans for
share learning Production of ‘you said
we did ‘ news letters Reduction in numbers
of patients who experience a delayed response
Trust lead human factors work stream across south central – DVD on handovers conference April 2011
Research on handovers – identifying learning actions to improve safety
100% staff had appraisal in 2010/11
100% eligible staff had statutory and mandatory training June 2011
Random reviews of delays provided assurance of quality of care, but also identified learning or improvement areas – (key priorities for quality accounts)
Internal audit of medicines management – substantive assurance of safety of medicines storage and administration processes
Triangulation by SHA in Quality Governance Framework provides assurance on safety metrics, policies and processes
Quality assurance process of all private

Board Assurance Framework V1 – 21.11.11
6
frequent callers, complex long term needs, GP triage, CSD, directory of services
Review and risk assessment of CIPs for quality impact
Review of operational and clinical structures will improve clinical leadership at the front line and provide further assurance on patient safety
ambulance providers
1.3
Fizz Thompson Director of Patient Care
Patients in the care of SCAS do not have a positive experience of their care
104, 4 Reg 19 Outcome 17 Complaints
12 CQC essential standards
DH quality indicators and measures
Quality Accounts, Trust Board and
Quality and Safety Committee assures clinical and quality governance processes
Audit Committee reviews and cross references quality domain
Executive Team monitors all quality and clinical processes and policies and performance
Complaints, concerns, comments and compliments monitored through the PERG
Audits of patient care records and delays to care
Positive media stories about quality of care
Improved CQC QRP Patient satisfaction
surveys Staff satisfaction
surveys External Clinical Peer
review Complaints and
concerns reduced 2010/11 however rise in complaint in April and May
SUI’s reduced in 2010/11
Incidents reported increased demonstrating more open and learning culture May 2011
Information on complaints and incidents shared with staff as case studies to share learning
Production of ‘you said we did ‘ news letters
Reduction in numbers
8
Negative media stories Increase in complaints
and incidents in April and May - drill down to reasons – staff attitude, delay and not sending an ambulance main reasons
Risk identified with non conveyance current theme for experience - learning identified with CSD surveys
None identified Actions in place to analyse reasons for increases in numbers for 2011/12 – Plan to increase customer care and communications skills in education programme Annual survey plan in place

Board Assurance Framework V1 – 21.11.11
7
Compliance with JRCALC
Research tools and methodologies are used to demonstrate care provision
of patients who experience a delayed response
100% staff had appraisal in 2010/11
100% eligible staff had statutory and mandatory training June 2011
Random reviews of delays provided assurance of quality of care, but also identified learning or improvement areas – (key priorities for Quality Accounts)
Review of CSD experience shows good experience, but identified areas for improvement April 2011
Objective 2: Emergency Performance
2.1 Ian
Ferguson, Chief Operating Officer
Failure to achieve operational performance against new national clinical indicators and measures
59 78 Regulation 9. Outcome 4 Care and welfare of people who use services
12 Performance delivery plans based on area and locality
Trajectories developed for delivery of performance aligned to PCT commissioning areas
Regular monitoring through Executive Team and Business Programme Board. Reporting and measuring of new national standards and clinical measures
Performance management framework with
Maintenance of current performance in Red 8 and 19 against national standards for SCAS and by PCT cluster
In top 3 performing Trusts for A8, telephone resolution and frequent user indicators.
Regular benchmarking of performance against other trusts reported to Board
REAP level 1
9
Some areas still reliant
on manual data validation or collection
Some reporting functionality on Qlikview still to be developed
Not performing
well compared to other trusts for time to treatment or answering calls.
Single ICAD system successfully implemented as per project timeframe on 5 July 11, evidence of no major ops performance impact - post go live robust monitoring in place under BAU
New SCAS EOC restructure rolled out in June 11 all EOC sites and new AD EOC in post end of August 11

Board Assurance Framework V1 – 21.11.11
8
operational teams New operational and
clinical structures review to address and develop performance management
Metrics now monitored through Integrated Performance Report
National performance report now available on SCAS website
Qlikview enables performance to be tracked and managed at all levels in SCAS, down to individual
Standardised virtual telephony platform implemented successfully on 7 September 11, with some evidence of improved call answering times; however, new action plan is being developed in light of experience to date Trajectory and improvement plans across all service delivery areas Action plan in place to improve call answering and time to treatment indicators Telephony system replaced in September to enable collection of call abandonment data
2.2 Ian Ferguson, Chief Operating Officer
Inadequate resources and resilience to meet unscheduled and unexpected demand
New risk June 2011
Regulation 22 outcome 13 Staffing
16 Clear resourcing plan matched to demand Rota hours sustained when compared to last year, despite significant reduction in private provider hours
Identified learning from past years
Integrated workforce plan to linked to budget
Integrated workforce plan monitored through workforce board and executive team
Reduction in hospital delays – monitored through business programme board and executive team. Many hospitals now close to 85% clear up in 15 minutes
Maintenance of
12
Project for A&E
Turnaround not delivering any real improvement in hospital handovers
Demand continues to increase
Contract need to increase use of alternative pathways
CIP slippage identified
Unknown position of adverse weather for winter
Monitoring through Business Programme Board – deliverables and benefits outlined in plans for alternative care pathways Action plans in place to address CIP slippage Action plans in

Board Assurance Framework V1 – 21.11.11
9
REAP plans Modelling tool to
improve resourcing planning
A&E turnaround project delivering reduction in ambulance clear up delays in hospital;
Introduction of Time Attendance Recording Process (TARP) with focus on Sickness Management
Increased focus of the CSD on hear and treat
Deployment of ECPs in Hampshire
Service development plans to manage demand (care plans frequent callers GP triage)
Cost improvement plans for dual ECA;s and sickness. absence
national standards currently 1st nationally for Red 8 performance
Clear escalation processes through bronze, silver and gold command structures
Increase in GP triage use
Availability of private providers for short term use
place to improve Kronos reporting
2.3 Ian Ferguson, Chief Operating Officer
New operational structures fail to provide clinical and operational leadership
New risk June 2011
Regulation 22 Outcome 13 Staffing
16 Consultation on new structures across organisation and with staff
Benchmarking with other ambulance trusts
External assurance of structures’
Works streams to develop detail and challenge proposals
Financial costs modelled
Development and training plan in place
Modelling of costs meet projections
Staff side support Proposals changed as
a consequence of staff feedback
Challenge of proposal s has strengthened structures
Assurance from external review
Project plan on track Appointment targets
met
12
Not all team leaders yet taken up appointment and team structures not yet in place
Assurance not in place as new structures yet untested Impact of the disruption caused by the appointments process uncertain
Transition plan in place Area plans being developed to embed new structures and deliver the benefits Development and training plan in place Project plan in place and being achieved for appointments process
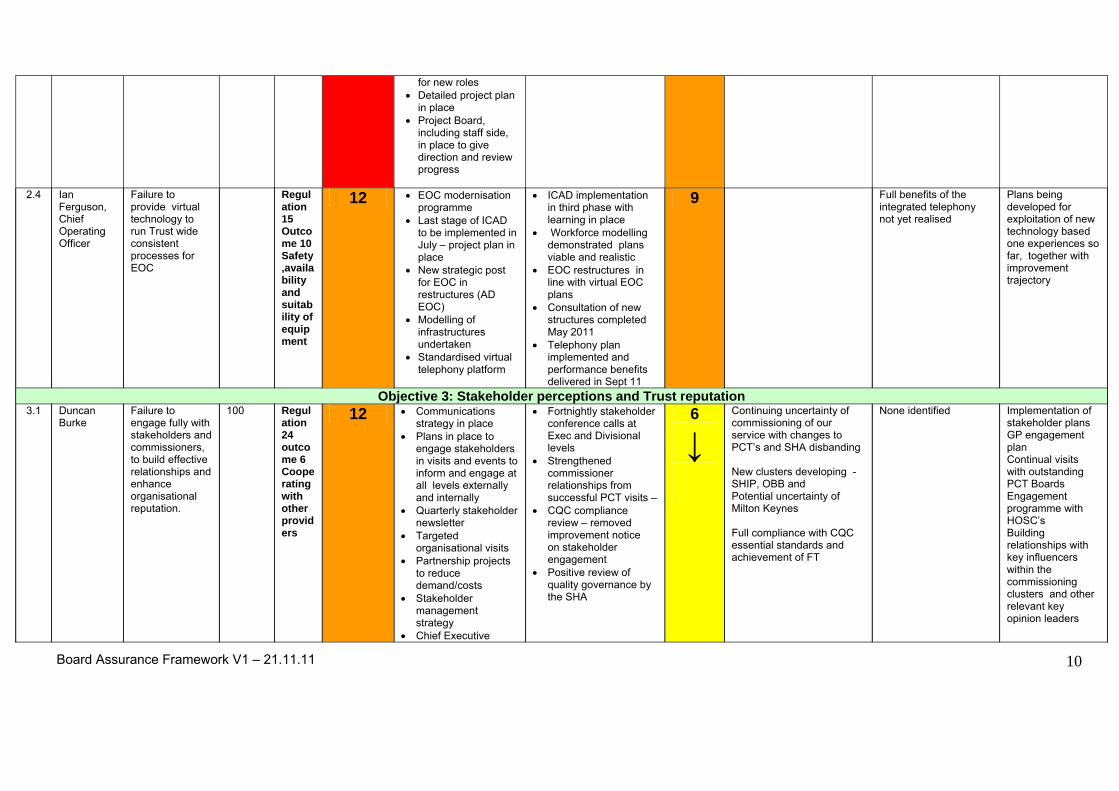
Board Assurance Framework V1 – 21.11.11
10
for new roles Detailed project plan
in place Project Board,
including staff side, in place to give direction and review progress
2.4 Ian
Ferguson, Chief Operating Officer
Failure to provide virtual technology to run Trust wide consistent processes for EOC
Regulation 15 Outcome 10 Safety ,availability and suitability of equipment
12 EOC modernisation programme
Last stage of ICAD to be implemented in July – project plan in place
New strategic post for EOC in restructures (AD EOC)
Modelling of infrastructures undertaken
Standardised virtual telephony platform
ICAD implementation in third phase with learning in place
Workforce modelling demonstrated plans viable and realistic
EOC restructures in line with virtual EOC plans
Consultation of new structures completed May 2011
Telephony plan implemented and performance benefits delivered in Sept 11
9 Full benefits of the integrated telephony not yet realised
Plans being developed for exploitation of new technology based one experiences so far, together with improvement trajectory
Objective 3: Stakeholder perceptions and Trust reputation 3.1 Duncan
Burke Failure to engage fully with stakeholders and commissioners, to build effective relationships and enhance organisational reputation.
100 Regulation 24 outcome 6 Cooperating with other providers
12 Communications strategy in place
Plans in place to engage stakeholders in visits and events to inform and engage at all levels externally and internally
Quarterly stakeholder newsletter
Targeted organisational visits
Partnership projects to reduce demand/costs
Stakeholder management strategy
Chief Executive
Fortnightly stakeholder conference calls at Exec and Divisional levels
Strengthened commissioner relationships from successful PCT visits –
CQC compliance review – removed improvement notice on stakeholder engagement
Positive review of quality governance by the SHA
6
↓
Continuing uncertainty of commissioning of our service with changes to PCT’s and SHA disbanding New clusters developing - SHIP, OBB and Potential uncertainty of Milton Keynes Full compliance with CQC essential standards and achievement of FT
None identified Implementation of stakeholder plans GP engagement plan Continual visits with outstanding PCT Boards Engagement programme with HOSC’s Building relationships with key influencers within the commissioning clusters and other relevant key opinion leaders

Board Assurance Framework V1 – 21.11.11
11
broadcasts 3.2 Failure to
achieve representative membership and subsequent governor elections.
10 Regulation 24 outcome 6 Cooperating with other providers
12 Use of best practice from other Foundation Trusts;
SHA support; Robust membership
strategy; Communication
Strategy and Plan Engagement with
active community groups
Appointed membership officer
Planned governor meetings and induction programme
Membership numbers increase p strategy and plan in place
Schedule of membership events
Success with consultation meetings
Consultation activity report for monitor
Consultation report on trust website
6
Membership not fully representative
Foundation Trust process ongoing with preparation for governing body
None identified Action plan to increase representative membership Successful representative election of governors completed induction programme preparation continue
3.4 Loss of credibility with stakeholders due to failure to deliver performance targets including performance in rural areas
New risk area
Regulation 24 outcome 6 Cooperating with other providers
16 Quarterly stakeholder letter
Performance packs to PCT clusters - development of Integrated Performance Report
Whole systems care Turnaround project to
optimise resources and reduce waste
Commissioner external review meetings with commissioners
Joint and local HOSCs communication and meetings
Trajectories agreed with commissioners for rural areas – contract 2011/12
Improved working relationships;
Positive response from stakeholders including HOSCs
SCAS involved in whole system planning through QIPP plans – ongoing with contract 2011/12
Stakeholder event planned for September
12
New national standards this year – need to inform and educate stakeholders of implications of the new Clinical Quality Indicators – engagement plan in place with HIOSC and other key stakeholders
None identified Action plan in place to address
improvements outlined in contract
Objective 4: Sound Governance 4.1 Charles
Porter Failure to achieve financial
71 20 Cost improvement plans agreed for next
History of good financial management
15 Further development of Cashflow reporting and
None identified Action plan in place to mitigation

Board Assurance Framework V1 – 21.11.11
12
targets as a result of economic climate and reduction in real terms of funding
2 years Board approved
budget & performance management of budget
LTFM aligned to Monitor framework
Monthly financial monitoring by Board and Executive Team
Challenge by Audit committee
Internal Audit reviews or accounts
Local Counter Fraud work
External Audit & SIC
Board approved budget on 31 March 2010
CIP workshops Internal and external
audits inc. year end audit reports
Minutes of Board, audit committee and executive committee
6 monthly budget reviews
External Review Boards each month with commissioners
Benchmarking against peers
Improved SLR Performance
management of CIP’s through business programme board and executive team
Clean audit report and value for money conclusion
analysis Performance
management of CIP’s – to address slippage
forecast pressures and any CIP slippage
4.1 Failure to develop approved viable long term financial model
13 16 Monitor Framework SHA Board to Board
meetings Executive team
challenge Board seminar and
development meetings to develop strategy and model
SHA review Internal challenge from
the Board and external experts – March 2011
Feedback from SHA Board to Board
External Feedback from other F Trusts
Shadow HDD report March 2011
Work and networking with other ambulance F Trusts
Integrated Business plan
12
Monitor approval `
Need to roll forward an extra year and then get sign off of revised LTFM, CIP plans and downside
DH sign off achieved 2 year contract signed Revised LTFM now Board approved with new Monitor assumptions
4.2 Failure to implement effective
Regulation 21
12 Information Governance Steering Group (IGSG)
IGSG minutes are processed though Exec and Audit
8
Not all staff yet trained in information governance e
Ability to ensure 95% of staff have completed Information
Annual IG work programme to ensure compliance

Board Assurance Framework V1 – 21.11.11
13
Information Governance
outcome 20 Records
Associate Director of IM&T appointed as Senior Information Risk Owner (SIRO)
Annual assessment against national IG Toolkit
Committees SIRO reports to IGSG,
Exec, and Board as required
Annual performance reported to Trust Board at green rating 68%
Mandatory training for staff in place
Governance training by end of June 2011
with, and national standards maintained
Objective 5: Leadership and Culture 5.1 Failure to
provide effective leadership to drive continuous improvement
New risk area
Regulation 22 outcome 13 Staffing Regulation 23 outcome 14 Supporting workers
16 Programme of leadership development and networking days
Operational and clinical restructure plan in progress – with clear development plans
Corporate review planned
IBP outlines vision and strategy for future leadership
development plans for Trust board
Restructures consultation concludes 30 June 2011
Board sign off July 2011
Board development programme in place
Leadership days planned for September
Launch of new structures planned to outline transition to new leadership
External assurance of new structures and leadership approach
Continued improvement in clinical and operational improvement
12 Restructures yet to be implemented – uncertainty for some levels of management
Evaluation of new structures and leadership to be determined for assurance of leadership and resilience
Evaluation plan to be developed
5.2 Failure to support staff and provide access to education and training to meet mandatory, clinical and organisational requirements
35 Regulation 23 Outcome 14 Supporting workers
16 Education training programme
Statutory and mandatory training for all staff
Integrated workforce plan
Rostering system will ensure correct availability of staff
Appraisals and training monitored through scorecard by Exec Committee and Board
Training remains on trajectory adhering to programme
Reached 100% S and M training June 2011
Staff feel valued and have received training applicable to role – as reviewed by SHA and CQC visit
Recruitment plan trajectory aligned to integrated workforce plan
9
Operational pressures
undermines ability to deliver against the trajectory
Sustainability of provision of training
CQC compliance notice New rostering system
behind schedule
Non compliance with CQC standards
Loss of hours due to recovery action plans
Plans in place to deliver statutory and mandatory training by June 2011
Recruitment Action Plan in place included in IWP.

Annual recruitment plan
Objective 6: Commercial viability
6.1 Failure to improve current financial margins and quality of care in the commercial arm
New risk area
Regulation 9. Outcome 4 Care and welfare of people who use services
20 Monthly finance reports detailing margin and other performance information as part of the reporting system
New detailed reporting system introduced June 2011
Turn round programme in place
External consultancy providing expert guidance to management team
progress in margin improvement and patient experience highlighted at Trust board June 2011 monthly reporting commenced
15
Time lag in activity
versus reporting due to provision of external invoicing
Review all non guaranteed -income -secured 50% of total
Further market analysis is being undertaken
Provide business tools to capture and charge additional activity
Develop a ‘go to market’ proposition to generate interest for additional activity
6.2 Failure to achieve market growth in new business areas
New risk area
12 Development of a marketing strategy
Appointment of a business development director
Creation of a pipe line of opportunities
IBP outlining vision Clinical strategy
alignment with commercial growth
IPR Review of
management team
Training programmes in place to update managers in finance and HR Fortnightly business reviews with each head of department Monthly RAG rated reporting to executive and Trust board Support to provide 111 pilot in 2 areas of the trust – may 2011 New business achieved New commercial training contract July 2011-06-30 New Bucks PCT contract July 2011
9 Improvement plan in place to improve business competency of exiting
management team Scope further
possibilities and further development of pipeline
Marketing activities around potential 111 business
Marketing strategy in development
Action plans in place to further 111 business
Board Assurance Framework V1 – 21.11.11
14

Board Assurance Framework V1 – 21.11.11
15
Board Assurance Framework 2011/12 PROFILE OF RISK RATINGS 2011/12
RISK REF APR MAY JUN JUL AUG SEP OCT NOV DEC JAN FEB MAR Y/E
OBJECTIVE 1: CLINICAL EXCELLENCE QUALITY OF CARE, PATIENT SAFETY AND EXPERIENCE 1.1 Failure to provide clinically excellent, evidence based care as outlined in national quality measures and in SCAS’ Clinical Strategy and Business Plan 104, 79, 5
12 9
1.2 Failure to provide and manage the quality of care which patients receive to ensure it is safe
52, 65, 93, 94, 104,
14 12 6
1.3 Patients in the care of SCAS do not have a positive experience of their care 104, 4 12 8 OBJECTIVE 2: EMERGENCY PERFORMANCE 2.1 Failure to achieve operational performance against new national clinical indicators and measures 59, 78 12 9 2.2 Inadequate resources and resilience to meet unscheduled and unexpected demand 16 12 2.3 New operational structures fail to provide clinical and operational leadership 16 12 2.4 Failure to provide virtual technology to run Trust wide consistent processes for EOC 12 9 OBJECTIVE 3: STAKEHOLDER PRECEPTIONS AND TRUST REPUTATION 3.1 Failure to engage fully with stakeholders and commissioners, to build effective relationships and enhance organisational reputation. 100 12 6
3.2 Failure to achieve representative membership and subsequent governor elections. 10 12 6
3.4 Loss of credibility with stakeholders due to failure to deliver performance targets including performance in rural areas 16 12

Board Assurance Framework V1 – 21.11.11
16
OBJECTIVE 4: SOUND GOVERNANCE 4.1 Failure to achieve financial targets as a result of economic climate and reduction in real terms of funding 71 20 15 4.1 Failure to develop approved viable long term financial model 13 16 12 4.2 Failure to implement effective Information Governance 12 8 OBJECTIVE 5: LEADERSHIP AND CULTURE 5.1 Failure to provide effective leadership to drive continuous improvement 16 12 5.2 Failure to support staff and provide access to education and training to meet mandatory, clinical and organisational requirements 35 16 9 OBJECTIVE 6: COMMERCIAL VIABILITY 6.1 Failure to improve current financial margins and quality of care in the commercial arm 20 15 6.2 Failure to achieve market growth in new business areas 12 9

Enc (Agenda Item: 16)
losure: M Board Report
1st December 2011
Title Chairman’s Report on the Audit Committee meeting held on Monday 14th November 2011
Report Author Edward Weiss, Chairman of the Audit Committee
Purpose of the report
The Audit Committee are required to provide a Summary Report outlining key matters the committee have agreed to bring to the attention of the Board.
Recommendation (eg. Note, approve, endorse)
The Board is requested to NOTE the report.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Sound Governance
Risk evaluation
Adequacy, relevance and accuracy of financial reporting
Links to the CQC Essential Standards regulations
N/A
Details of additional risks associated with this paper:
N/A
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
N/A
Financial implications/impact N/A
Legal implications/impact N/A
Equality and Diversity implications/impact
N/A
Partnership working and public engagement implications/impact
N/A
1

Report of the Audit Committee following its meeting of 14th November 2011
Key areas of discussion and decision included the following: Agenda item/title
Background information Action
Internal Audit Report
The Committee received and discussed the progress report 2011/12. The report commented on several routine matters but nothing of significance needs to be bought to the Board’s attention.
The Board to NOTE.
External Audit Report
The report noted emerging issues associated with the preparation of part year accounts for the NHS Trust and FT. Carol Ryan and the finance team would continue to discuss issues as they arise. Maria Grindley discussed the future of the Audit Commission; she noted that the Audit Commission would have to resign as soon as SCAS achieved FT status (hopefully as from 1 February 2012 or 1 March 2012) but would carry out the audit for the period up to the date when SCAS became an FT. Arrangements will need to be made for the audit between SCAS becoming an FT and the end of this financial year and then for the future. Action by CP/EW
The Board to NOTE.
Review of BAF and Risk Register
The Committee received the BAF and Risk Register. Nothing of significance to be reported to the Board.
The Board to NOTE.
Policies Dave Watts (Operations Programme Manager) attended the meeting to update the Committee on the progress of Operational policies. He explained that some good progress had been made and he would ensure that all the policies were updated on both the intranet and internet.
The Board to NOTE.
2
3
The Chair of the Committee asked for a member of HR to attend the next Audit Committee.
Counter-Fraud report
The report noted the fraud risk associated with the Creditors Bank account amendments (NPE). The LCFS explained that NHS Protect had issued fraud warnings following a new ‘scam’ targeting NHS Trusts in relation to amending creditors bank account details. A check had been made to all amended bank accounts for the last 6 months and there were no concerns with these. TS and CP had met to review the process to ensure this did not happen within SCAS. It was noted that processes had already been tightened following the initial warning and the documentation procedure required amendment to reflect this.
The Board to NOTE.
Information governance
The Committee were asked to note the Minutes of the meeting held 31st October. Nothing of significance to be reported to the Board.
The Board to NOTE.
Other reports No additional reports were submitted to the Committee.
The Board to NOTE.

Enclosure: N (Agenda Item: 17)
Board Report
1st December 2011
Title Chairman’s Report on the Quality and Safety Committee meeting held on 13 October 2011
Lead Director Fizz Thompson Director of Patient Care
Report Author Keith Nuttall, Chairman of the Quality and Safety Committee
Purpose of the report
The Quality and Safety Committee are required to submit the Minutes of each meeting to the Board and to provide a Summary Report outlining key matters the committee have agreed to bring to the attention of the Board.
Recommendation (eg. Note, approve, endorse)
The Board is requested to NOTE this report.
Links to the Business & Risks
Strategic Objectives: (please mark in bold)
Clinical Excellence Operational Excellence Stakeholder perception & Trust Reputation
Sound Governance Leadership & Culture Commercial Viability
Corporate Risk Register priorities: (please mark in bold)
Quality of Care Emergency performance Stakeholder perceptions
Cost pressures related to economic climate & changes in the wider health economy
Workforce development Completion of IT infrastructure
Links to the CQC Essential Standards regulations
All
Details of additional risks associated with this paper:
N/A
Links to the NHS Constitution (relevant staff/patient rights) All NHS organisations are required by law to take account of the NHS Constitution in performing their NHS functions.
Financial Implications/impact N/A
Legal implications/impact N/A
Equality and Diversity implications/impact
N/A
1

Partnership working and public engagement implications/impact
N/A
Other
Committees/groups where this item has been presented before
Other options available and their pros and cons
Progress monitoring and review
Background papers Policies, Procedures and Papers relevant to this report can be obtained from the Trust’s Corporate Secretary
2

Quality and Safety Committee Report from the meeting held on 13 October 2011
Agenda item/title
Background information Action
2.1 Corporate Risk Register: Review of Clinical Quality, Safety Risks and Action Plans 5.7 Non Conveyance Safety Review 7.1 Clinical Review Group Minutes (CRG) 21 September 2011
Serial Number 52 - Failure in the locking mechanism on back doors of WAS Mercedes vehicles. Assurance was provided that communication had been sent to staff with instruction on how to operate and override system should this problem occur. This is an interim solution and WAS are currently working to provide a long term solution. The Care Quality Commission and the Trust’s commissioners have been formally notified of the problem. The Committee received and discussed the findings from a review of care records of patients who had not been conveyed to secondary care. Concerns were raised that the report did not provide assurance to the committee regarding process and practice relating to non conveyance and that further assurance was required. It was agreed that the matter should be discussed at the October Board seminar. Keith Nuttall to raise at Trust Board level The following were approved by the Committee: The combined Clinical Governance document. Discontinuation of the use of the AMPDS Aspirin administration tool in EOC’s Hepatitis B immunisation of staff
Board to NOTE For further discussion at Board Board to NOTE
3
Agenda item/title Background information Action 8.1 Update on the current position with the Care Quality Commission Registration 9.1 Update on progress with Quality Accounts 10.1 Resilience and Specialist Operations Strategy 2011 - 2015
policy Dual ECA policy. The following items were noted by the Committee: Clinical memo on the benefits of cooling patients in cardiac arrest CRG approval of pain management guidance for the CSD Clinical Directive in child death procedure CRG approval of the iGels as the supraglottic airway of choice. CRG approval of the use of LifePak 15 for measuring Carbon Monoxide levels in the bloodstream There has been improvement in monthly reporting to the NPSA . The CQC has issued 2 minor improvement notices on reporting (Regulation 16, outcome 18 and Regulation 18, outcome 20) .The CQC has also requested further information on the Safety, availability and suitability of equipment (Regulation 16 , outcome 11). The Director of Patient Care updated the Committee to provide assurance that the Trust is on track with progress in the areas of Patient Safety, Clinical Effectiveness and Patient Experience. The Committee received and discussed the five year Resilience and Specialist Operations Strategy 2011 – 2015. It was noted that delivery of the proposed strategy would be based on the four pillars of resilience, namely:
Board to NOTE Board to NOTE Board to NOTE
4
5
Agenda item/title
Background information Action
10.2 Policies for Board Approval/Ratification. Health and Safety Policy Risk Management Strategy 11. Recording and identification of risks from the Agenda items
Risk Assessment Preparedness Response Recovery.
Further work is required to establish timescales for each resilience pillar; assurance was given that a detailed implementation plan would underpin the strategy. It was confirmed that the Executive management team had considered the strategy and would recommend its approval. The Committee suggested that there needs to be a better understanding at Executive level as to the distinction between policy and strategy documents. The Committee approved the Resilience and Specialist Operations Strategy 2011 – 2015. It was resolved that the Chief Operating Officer would submit the strategy to the Board for information The Committee received a report on the annual review of the Heath and Safety Policy and the Risk Management Strategy. It was resolved that the policies should be amended to reflect minor changes outlined. The Director of Patient Care to submit a report to the Board on 21 December 2011 It was agreed that the current risk rating for non – conveyance would be reviewed as part of the discussion scheduled to take place at the Board development session on 26 October 2011.
Report to be SUBMITTED to Board Board to NOTE
UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
1.
QQuuaalliittyy && SSaaffeettyy CCoommmmiitttteeee MINUTES of the Quality & Safety Committee held on Thursday 13 October 2011 at 13.30 pm
in the Board Room, Northern House, Bicester Members Present: Keith Nuttall Claire Carless In Attendance: Gavin Bashford Simon Brown (on behalf of JB ) John Dyer Ian Ferguson Trevor Jones Paul Phillips Alison Taylor Fizz Thompson June Roberts Invited: Colin Hill (on behalf of Garry Williams) Observers: Julie Dawes
KN CC GB SB JD IF TJ PP AT FT JR CH JVD
Non Executive Director (Chair) Non Executive Director Unison Staff Side Assistant Medical Director - North Head of Resilience and Specialist Operations. Chief Operating Officer Chairman Investigation Officer Interim Head of Governance & Risk Management Director of Patient Care Minute Taker (until minute 8.3 only) Patient Involvement Panel Company Secretarial Consultant and Minute Taker (from minute item 9.1 only)
1.0 Welcome, Introduction and Apologies
The Chairman welcomed members to the meeting and reported that apologies had been received from Mr Mitchell-Baker. It was CONFIRMED that the meeting was accordingly quorate. Declarations of Interest It was CONFIRMED that there were no declarations of interests.
1.1 Minutes of Meeting held on 4 August 2011 The minutes were agreed as an accurate record of the meeting.
1.2 Matters Arising Members reviewed the schedule of matters arising from the Minutes and subject to the comments below, CONFIRMED that the necessary assurances have been obtained by the Committee: Emergency lighting (5.1) The work is still out to tender to improve station lighting following a legal claim being received due to lack of lighting and a member of staff injuring their ankle. An update to be provided at the next meeting. Action: AT
UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
2.
Review of Private Providers governance arrangements(4.8) The meeting planned in September with all Private Providers has been rearranged to November due to the meetings taking place with Monitor. An update will be provided at the next meeting. Action: FT BAF: Overview of clinical quality safety section and red rated areas for action Weight of Response Bags (3.2) This matter has been referred to the Health, Safety and Risk group for further consideration which will formally report back to the Executive Management Committee under the revised governance arrangement. Item closed for this report. Fire Alarm Panel (5.2) The issue concerning fire alarm testing has been referred to the Health, Safety and Risk group for further consideration which will formally report back to the Executive Management Committee under the revised governance arrangement. Item closed Internal transfers Confirmed that the necessary work has been completed regarding the securing of stretchers and other equipment in vehicles. Item closed EOC Staff – Corporate Induction Assurance provided that progress is being made with EOC staff not attending Corporate Induction, but not completed. IF to confirm when complete. Action: IF Claims Report: Summary of key claims and identified risks – Agenda item. Item closed Serial Number 68 (Sickness and Absence) Sickness and absence remains at a high level. Managers are receiving alerts and also a coaching and guidance DVD to help manage the staff. An exception report to be provided at the next meeting. Action: SW Managing demand across the health system (5.3) – Carried forward from Aug meeting Confirmed that demand and commercial business for the Trust is tracked through the Commercial Turnaround Project. The Committee discussed a representative from the Commercial department attending future meetings. It was noted the TOR would have to be updated to reflect any changes in membership. KN and FT to discuss with the Interim Business Development Director. Action: KN, FT
Corporate Risk Register: Review of Clinical Quality, Safety Risks and Action Plans (2.1) The results from the safety review of care are on the agenda. Item closed BAF: Overview of clinical quality safety section and red rated areas for action (3.1) 6.2 – Assurance provided that the identified risk has been reviewed and re evaluated in view of
the 111 service. Item closed Integrated Performance Report (IPR): Identification /summary of exceptions and concerns (4.1) – Exceptions included on agenda. Action closed for this report Summary of Health, Safety and Risks Meeting minutes: Operational Health, Safety and Risk Group Minutes – 14 July 2011 (5.1/ 5.2) It was reported in the past year there have been 2 incidents of staff receiving back strain injuries from using the Mangar Elk. To be reviewed at Health, Safety and Risk group meetings. Item closed Summary of health, safety and risks - overview of red rated risks (5.3) 1.3 Patient Handling: Refer to agenda. Item closed for this report
UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
3.
4.4 Station Keys: This will be managed through the Health, Safety and Risk group. The responsibility of all station and ID security is now with the Assistant Director of Support Services who will lead the process. 5.21 Internal Transfers: All vehicles have been CEN tested and SCAS meets all the required standards. Item closed for this report Summary of SUI Review Group Minutes 6 July and Identification of Risks and Action Plan (5.4) Informing coroners; A Directive has been cascaded to staff informing them to contact the Police. Item closed The new structure with Clinical Mentors in place will resolve the issues regarding new staff and staff transfer between Divisions and ensuring they are updated with any clinical / operational changes in practice. Item closed Claims Report: Summary of key claims and identified risks (5.6) and Executive/NED Walk Arounds: Update on visits and identified trends (5.8) – refer to agenda Safeguarding Performance Report (7.4) – Action complete. Item closed QRP update and identification of key risk areas – review of Performance Accelerator (8.2)Confirmed that definitions are provided as part of the report for the agenda. Item closed Update on progress with Quality Accounts (9.1) – Action complete. Item closed 4C’s Policy (10.1) Due to the restructure, the policy has been delayed, but will go to the PERG meeting for approval in November.
Annual Report and Quarterly Reporting to Monitor (12.1) – Carried forward from Aug meeting Reporting may need to change in view of the Monitor process. KN and FT will progress and provide a new style report at the October meeting. Action: KN, FT
1.3 Quality and Safety Board Report to the Trust Board The Committee received and NOTED the Quality and Safety Report that had been submitted to the Trust Board meeting on 30 September 2011.
2.1 Corporate Risk Register: Review of Clinical Quality, Safety Risks and Action Plans The Committee reviewed the red risk areas contained in the corporate risk register and accompanying action plan. The Interim Head of Governance & Risk Management provided a comprehensive update on each identified key risk area and assured members of the mitigating actions that have been implemented. It was REPORTED that Serial Number 52 was the only risk to change with the main issue relating to back door locking mechanism on WAZ vehicles. Assurance was provided that WAZ were now providing a long-term solution to resolve this issue and that in the interim an internal ‘Hot News communication providing information on how to override the problem had been cascaded to staff. It was CONFIRMED that the Care Quality Commission and the Trust’s Commissioners have been formally notified of the matter and that to facilitate wider learning across the sector, other Ambulance Services have also been informed. It was RESOLVED that the Corporate Risk Register and accompanying Action Plan be received and NOTED.
UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
4.
3.1 BAF: Overview of clinical quality safety section and red rated areas for action The Committee reviewed the updated Board Assurance Framework focussing on each of the red rated areas contained in the report. The following key points were highlighted: Clinical Excellence – There were no red risks in the Clinical excellence, Quality of Care section of the report Emergency Performance 2.3 Ops/Clinical Review : A risk register in relation to the implementation of the new Operations and Clinical Structure is in place and which is being proactively managed. The Area Managers that have recently been appointed under the new structure have been consulted in connection with a draft Benefits Realisation Plan which outlines the deployment plan to secure the benefits from the new structure and proposes a measurement system to track benefits realisation. It was noted that this document was scheduled for discussion at a Board Development Seminar on 26 October with a view that it be submitted for approval at the Trust Board meeting on 1st December 2011 In response to a request for clarification regarding the training and development implications associated with the new structure, the Chief Operating Officer assured the Committee that the new structure would provide better opportunities for development and training to the improved standards and ways of working. However it was acknowledged that the new operational and financial environment might prove challenging for the front line teams l.
4.1 Integrated Performance Report (IPR): Identification /summary of exceptions and concerns The Committee noted the report and the overview of the IPR that confirmed the exception area rated red in HR was due to sickness and absence levels. The committee asked for an exception report and update to be provided at the next meeting. Action: SW
5.1 Summary of health, safety and risks - overview of red rated risks The Committee noted and reviewed the red rated risks. It was noted the risk register is being reformatted and will be brought to the next meeting. An issue was raised that the report was in incomplete with missing and out dated information. This to be addressed for the next meeting.
Action: ATThe following key points and actions resulted from the review: 1.3 Patient Handling: Remains to be a high proportion of the IR1’s and 51% of claims are
due to manual handling. Manual handling equipment is being reviewed and risk assessed. It was noted the Planned Outcome column of the register was out of date and to be updated. Action: AT
1.3b Weight of Response Bags: A trial of prototypes has been undertaken and the next stage is preparing a business case. A concern was raised around the possibility of managers carrying out the trials of the new bags and not operational staff. FT to review the position and report back at the next meeting. Action: FT
1.4 IR1 Completion: To remain red rated as although there are improvements with ongoing training, there is more work to be undertaken to improve reporting of incidents
1.7-1.10: These are HR issues and are reviewed at the Workforce Development Board and Executive Management Committee
5.10 Clinical Waste: Work is underway with Acute Trusts regarding the possibility of leaving clinical waste at the hospitals.
5.15 Charging Points: These are still under review. Head of Fleet is looking at a different system to resolve the issues and will report back at the next Health, Safety and Risk group meeting.
5.2 Meeting minutes: Operational Health, Safety and Risk Group Minutes – 15 September
2011 The Committee noted the report that provided a summary of the meeting minutes of 15 September 2011 and in particular the following points:
E-learning package not in place for staff’s annual refresher fire training and raised as a

UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
5.
risk on the risk register A concern with access to morphine being wider than necessary, but being reviewed by
the Assistant Director of Support Services Noise at work: Ear plugs are available for staff and vehicle sirens have been tested and
are compliant. Staff who have a concern are being referred to Occupational Health and the particular vehicle being inspected
Concern with the non attendance at meetings from particular Directorates
5.3 Summary of SUI Review Group Minutes 5 October and Identification of Risks and Action Plan The Committee noted the report and the minutes of the October meeting and discussed the recent incident regarding a tail lift failure when attending a patient in cardiac arrest that caused a delay in transporting the patient. Following a review it was believed the incident did not impact on the patient’s outcome. All vehicles of the particular model in the north have been adjusted and the fault rectified. One of the outcomes following the SUI meeting is to check all vehicles Trustwide and, in future, any such incident to be immediately reported to the fleet department and nationally to avoid a recurrence. FT to ask PP to include tail lift checks as part of the regular maintenance check and provide assurance of the checks. Action: FT,PP
5.4 Education and Training Report and summary of risks including Appraisals, Statutory & Mandatory Training, Sickness/Absence and Staff Turnover The Committee noted the report and in particular the following points:
Recruitment is on plan Trauma training commenced 4 October with positive feedback being received. A
concern was raised regarding the capacity for 2 big training programmes (trauma and restructures development), but reassurance was given that a robust training plan is in place and is being monitored through the Workforce Development Board and the Executive Management Committee. Staff are also attending the trauma training in their own time with future planned time off. There is also an increased risk of bad weather which will increase the REAP level and thus reduce numbers for extraction
A total of 12 students have enrolled on the Open University Paramedic programme Appraisals have dropped below 90% and a report is being prepared for the Executive
Management Committee to undertake a review of the current position and take performance management action
Sickness/absence rates are still high, but September figures are outstanding and will be reviewed when reported
5.5 Claims Report: Summary of key claims and identified risks
The Committee noted the report that provided a summary on the number and types of outstanding claims which ranged from 2006 -2011. The responsibility of handling the legal claims transferred to the Clinical Directorate in early October. Work is underway to see if any claims need to be reviewed as a serious incident. An analysis of the claim will be undertaken by date of incident and not date of claim. A request was made for the information to be categorised to the different SCAS departments and also include the financial information.
Action: ATIt was confirmed there is a contingency in budget for claims and employment tribunal claims come under public liability following a question raised.
5.6 Leadership Walk Arounds: Update on visits and identified trends The Committee noted the report. A trend analysis requested at the last meeting was provided on 5 ambulance stations that had been visited. Overall there is good scoring, but there are concerns with Basingstoke that the Operations team are aware of. It was confirmed that the EOC’s are also included in the leadership walk round process. Reassurance was provided that the review and scoring process is consistent due to the template and criteria for the visit. The schedule to be re-circulated to Non Executive and Executive Directors to maintain focus on the visits. Action: JR

UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
6.
5.7 Non Conveyance Safety Review The Committee received and discussed the report that provided the background and actions taken forward, following the findings from a review undertaken on care records of patients that had not been taken to the Emergency Department. The report provided a retrospective and subjective review of the workshop findings and also included learning and actions for improvement. Non conveyance is noted on the clinical effectiveness section of the risk register A discussion was undertaken around the evidence of care from the documentation on the care records and how the review was subjective and did not take into account the other factors that staff take into account when making a decision to take to hospital or try another care pathway. Concerns were raised that the report did not provide reassurance to the Committee around the processes and practice of non conveyance and it was agreed that further assurance around patient safety should be fully discussed at the board seminar meeting planned for 26 October. Reassurance was provided that the main issue is document completion and the new structure with Team Leaders in place will help as they will work with staff and review paperwork completion. Recent education sessions have provided an update on documentation, and random reviews of patient care records continue to monitor form completion. Actions arising from these reviews are followed through with staff in the form of a reflective session. KN to raise at Trust Board level. Action: KN
5.8 Medicines Management The Committee received and noted the report that provided an update on the workstream areas of medicines management and the quarterly returns of controlled drug self declarations to the Local Intelligence Networks.
6.1 Summary of Patient Experience Review Group Meeting Minutes – 18 August 2011 The Committee received and noted the report that provided an update and in particular to risk areas and trends of outcomes of complaints and also the request for full attendance at meetings. The number of complaints remains a concern; however the number is lower than the number of incidents.
6.2 Update on Complaints PP, the new Investigation Officer was introduced to the group and gave a presentation on an analysis of attitude complaints received in the southern division during the first quarter of 2011. The analysis looked at the length of time, call details, time of call vs shift times, grade of staff, breakdown of the call time (incident not actual complaint) and meal break status. Further work is being undertaken with the Aqua team reviewing all the calls and a questionnaire is being produced for complainants. To date the results show that complaints occur on the longer shifts and when a paramedic in attendance. A recommendation to be made to the Q&S Committee after further progress has been reviewed by the PERG.
6.3 PTS Surveys The Committee reviewed and discussed the results of a patient satisfaction survey for patients using the Patient Transport Service for journeys to and from the Milton Keynes and the Churchill (Oxford) Renal Units. Overall the results gave a positive view; however there are points of learning around planning and turnarounds. The report was noted. Further evidence of feedback to staff and an update on the recommendation to review the journey plans will be monitored through the PERG.
7.1 Clinical Review Group (CRG) Minutes – 21 September 2011 and identification of risks and trends The Committee received and noted the minutes of the September meeting. The group discussed the summary report and ratified the following:
The Combined Clinical Governance document that clearly sets out what is expected of Doctors working for SCAS
UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
7.
Hepatitis B Immunisation of Staff policy and Dual ECA policy which has been modified so ECA’s can attend a patient of any age in line with new guidance for the CFR’s
Discontinuation of use of AMPDS Aspirin administration tool in the EOC Following a request from the NPSA, a clinical risk assessment of medication loading doses has been completed and a report returned to the NPSA. A concern was raised regarding national CPI data being 6 months old. It was confirmed that this is the most recent national data available, however up to date SCAS data can be provided. SB to ask if national CPI data can be provided in a more timely manner. Action: SB New drugs for staff to administer and issued with PGD’s were noted. Progress and the benefits to patients of the Enhanced Medical Care and Air Ambulance Project and that it was not currently a business case was noted. JB to progress with the PCT’s and Commissioners. Action: SB/JB An overview on the Trauma Bypass Tool was provided and how it will be used by staff. A presentation on trauma to be included as a topic for discussion at the January Trust Board Seminar. Action: JH/JVD The following items to be noted on behalf of the Trust Board:
Q&S approval of the Combined Clinical Governance document Clinical Memo produced to provide guidance to staff on patient cooling which benefits
patients in cardiac arrest Q&S approval of Hepatitis B Immunisation of staff Policy and Dual ECA policy Q&S agreement for the discontinuation of use of AMPDS Aspirin administration tool in
the EOC CRG approval of pain management guidance for the CSD Clinical Directive in child death procedure CRG approval of iGels as the supraglottic airway of choice. CRG approval of the use of LifePak 15 for measuring Carbon Monoxide levels in
bloodstream Action: KN
7.2-7.6
Clinical Performance Indicators, PCI Performance, Safeguarding Performance, Infection, Prevention and Control and Annual Clinical Audit Reports The Committee received and noted the reports provided for information on the clinical performance of the Trust.
8.1
Update on current position with CQC registration The Committee received and noted the report. Improvements have been made with monthly reporting sustained to date and performance against the target of reporting within 30 days improved, following the CQC issuing 2 minor Improvement Notices on notification of death of a person who uses service - Regulation 16 outcome 18 Notification of other incidents - Regulation 18 outcome 20 Further information has been requested on Outcome 11 Safety, Availability and Suitability of Equipment and further information is awaited from the CQC local assessor. A discussion took place on whether SCAS should review mortality numbers, but no decision made.
8.2 QRP Update and Identification of Key Risk Areas The Committee noted the update provided for information which showed the Trust overall as ‘High Neutral’. A key was provided to provide clarity on the ratings. Concerns were raised regarding August 2011 being the latest information available to SCAS and the quality of the data which did not relate to feedback provided to the CQC on the outcomes. The Trust undertakes to provide updates and additional information to the CQC to help inform the risk profile.

UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
8.
8.3 Incident Reporting The Committee noted the Patient Safety Incident report from the NPSA which detailed incidents from 1 October 2010 – 31 March 2011. The number of incidents was much lower than expected, but reporting has now improved and the next 6 months will see an improvement.
9.1 Update on progress with Quality Accounts By way of providing the necessary assurance to the Committee, the Director of Patient Care presented an update on progress by those work streams involved in the production of the Trust’s Quality Accounts for the year ending 31 March 2012. She drew attention to the following three specific areas identified in the report and confirmed that the Trust was on track to complete these priorities:
Patient Safety Clinical Effectiveness Patient Experience
Referring to Patient Experience, it was NOTED that whilst there had been some slippage in the timetable for conducting the required Patient Survey, members were assured that an appropriate action plan had been implemented to address the position. It was RESOLVED that the progress report on the Quality Accounts 2011/12 be received and NOTED.
9.2 Quality Improvement Plan By way of providing the necessary assurance to the Committee, the Director of Patient Care presented a quarterly update for the period ended 31 September 2011 in relation to the Quality Improvement Plan for the Trust’s 2011/12 Quality Accounts. It was RESOLVED that the second quarter update on the Quality Improvement Plan be received and NOTED.
10.1 Resilience and Specialist Operations Strategy 2011-2015 The Head of Resilience and Specialist Operations presented the five year Resilience and Specialist Operations Strategy for the period 2011 to 2015 and informed the Committee that the Civil Contingencies Act (2004) (the Act) sets out clear responsibilities for those organisations who directly respond to emergencies (category 1 responders) and those that have a supporting role (category 2 responders). He explained that the purpose of the proposed strategy was to ensure that there was an appropriate framework in place which enables the Trust to discharge its duties under the Act. It was noted that this responsibility also included directly responding to emergencies while maintaining a high quality, clinically focussed service to the Trust’s patients. Assurance was provided to the Committee that the proposed strategy served to ensure that the Trust would be fully integrated with both national and regional structures such as the National Ambulance Resilience Board (NARB), the Department of Health’s Emergency Preparedness Division (EPD) and the Cabinet Office’s Civil Contingencies Secretariat (CCS). It was NOTED that delivery of the proposed strategy would be based on four pillars of resilience, namely:
Risk Assessment - ensuring the Trust as an adequately resourced Resilience and Specialist Operations (previously Emergency Preparedness) team which assesses risks from hazards and threats and identifies the mitigation needed;
Preparedness – ensuring the Trust’s staff have the education and training to effectively deal with emergencies or adverse incidents that endanger the delivery of its services;
Response – ensuring the Trust has the appropriate quantity and type of resource needed to deal with emergencies or adverse incidents that endanger the delivery of our services; and

UNAPPROVED Quality and Safety Committee Minutes – 13 Oct 2011
9.
Recovery – ensuring the Trust’s business continuity management (BCM) arrangements are compliant with the British Standard BS NHS 2599-1.
It was FURTHER NOTED that whilst work was still required to establish the precise timescale for each resilience pillar members were assured that underpinning the proposed strategy would be a detailed implementation plan The following comments and challenges were received :
a) In response to a request for clarification as to the prior consultation and approval process of the proposed strategy, it was CONFIRMED that the Executive Management Committee had previously considered the strategy and resolved to recommend its approval; and
b) Noting the length (some 32 pages) and content of the document as produced to the meeting, it was suggested that there needs to be a greater clarity and understanding at executive level as to the distinction between strategy and policy documents.
Following discussion it was RESOLVED that : a) The Resilience and Specialist Operations Strategy for the period 2011 to 2015 as produced
to the meeting be APPROVED by the Committee; and b) As a means of providing assurance, the Chief Operating Officer would submit the approved
Resilience and Specialist Operations Strategy for the period 2011 to 2015 to the Board for information.
10.2 Update on Review of Health & Safety Policy and Risk Management Strategy
The Director of Patient Care presented a report on the outcome of the annual review undertaken in relation to the Trust’s Health and Safety Policy and the Risk Management Strategy. It was REPORTED that following the review, a number of minor changes had been identified which were briefly outlined to the meeting. Following discussion, it was RESOLVED that: a) The Trust’s Health and Safety Policy and the Risk Management Strategy be amended as
necessary to reflect the minor changes to these documents as outlined to the meeting, and b) The Director of Patient Care be authorised to submit on behalf of the Committee a report to
the Trust Board on 30 November on the outcome of the annual review that has been undertaken of the Trust’s Health and Safety Policy and the Risk Management Strategy
Action: FT
c) The report on the outcome of the required annual review of Health and Safety Policy and Risk Management Strategy be accordingly received and NOTED.
11 Recording and Identification of Risks from Agenda Items
It was AGREED that the current risk rating level for non – conveyance would be reviewed as part of the discussion scheduled to take place at the forthcoming Board Development session on 26 October 2011.
Action: Trust Board12 Any Other Business
It was confirmed that there were no further matters to report.
13 Date of Next Meeting 8 December 2011 10.00hrs - 13.00hrs Southern House

UNAPPROVED MINUTES
Registered Headquarters: Units 7 and 8, Talisman Business Centre, Talisman Road, Bicester, OX26 6HR
1
MINUTES Title of the meeting: Charitable Trust Funds Committee Date and Time: Thursday 22nd September, 2pm Venue: Board Room, Bicester Present:
Claire Carless Eddie Weiss Nick Dolden John Divall Charles Porter
CC EW ND JD CP
Non-Executive Director (Chair Non-Executive Director Assistant Finance Director FT Project Director Director of Finance
In Attendance: Julie Dawes Amy Shearman Apologies: Graham Wilson
JDa
AS
GW
Company Secretarial Consultant (for part of meeting) Personal Assistant (Minutes) Chair – Ox/Bucks League of Friends
Item No:
Description:
Action:
1.
Appointment of the Chair: The Committee formally noted that Colin Hazell had left the Trust and welcomed the new Chair of the Committee, Claire Carless.
2.
Apologies: Apologies were received from Graham Wilson (League of Friends).
3.
Minutes: The Minutes of the meeting held 25th May 2011 were approved.

UNAPPROVED MINUTES
Registered Headquarters: Units 7 and 8, Talisman Business Centre, Talisman Road, Bicester, OX26 6HR
2
Matters arising: Executive Summary ND discussed Charity Sub Committee Report. It was noted that as a result of the Charity attracting funds, namely the First Responder schemes in Berkshire, the Charity has an excess income over expenditure of £12k. Exec Team to make further contact with Keith Boyes to see if a plan could be put together for future spending priorities. Tuffsats There remains an outstanding issue in relation to providing tuffsats within the Bucks/Oxon area. It had been agreed that Dick Tracy would contact ND re funding requirements as the trustees had already agreed to fund one per scheme. ND would make contact with DT to send over exact requirements.
CP
ND
4.
Charity Sub Committee Report It was noted that the main purpose of the report was to consider the latest financial report, approve the unaudited accounts for 2010/11 and to consider the Swallowfield First Responder vehicle business case.
5.
Executive Summary: ND was asked to circulate scheme of delegation to the committee members
ND
6.
Charity Accounts: ND noted that there had been a lot of movement in funds with high levels of expenditure on equipment, and in particular Hampshire tuffsats. It was also noted that the Charity had continued to receive a steady income via donations. Overall the Charity turned over £121 which was £12k in excess of expenditure, balances stood at £388k.
7.
Business Case for Swallowfield vehicle The Trustees considered the Swallowfield First Responder’s business case for purchase of a vehicle dedicated to the scheme. ND explained that the Swallowfield Community First Responder Group had been very successful in getting funding for the proposed 4x4 vehicle. It was noted that the group had individual sums of £15,000 either paid or promised and a further guaranteed

UNAPPROVED MINUTES
Registered Headquarters: Units 7 and 8, Talisman Business Centre, Talisman Road, Bicester, OX26 6HR
3
offer from the National Lottery of £10,000 to fund the purchase of vehicle and running costs for at least 12 months. After this period the Group would raise funds to keep the vehicle on the road. The committee approved the business case for a BMW X3. Clarity was sought regarding the insurance of other CRF vehicles and the accounting for such vehicles. For example should purchase of vehicles be shown as a fixed asset within the Charity accounts. ND would check and report back at the next Charitable Funds Committee meeting.
ND
8.
AOB: Ambies Funds for the gifts were approved £400.00
9.
Date and time of Next Meeting: Wednesday 30th November, 4pm.