tubal and cervical serous carcinoma a pathological
TRANSCRIPT
Annals of Clinical Pathology
Cite this article: Merino J, Alameda F, Mancebo G, Baró T, Navarro G, et al. (2016) Tubal and Cervical Serous Carcinoma A Pathological, Immunohistochemi-cal, and Molecular Study of A Case. Ann Clin Pathol 4(7): 1093.
CentralBringing Excellence in Open Access
*Corresponding author
Alameda F, Department of Pathology, Hospital del Mar, c/ PasseigMaritim 25-2808003 Barcelona, Spain, Tel: 34932483919; Fax 34932483131; Email:
Submitted: 08 September 2016
Accepted: 12 October 2016
Published: 17 October 2016
ISSN: 2373-9282
Copyright© 2016 Alameda et al.
OPEN ACCESS
Case Report
Tubal and Cervical Serous Carcinoma A Pathological, Immunohistochemical, and Molecular Study of A CaseMerino J1, Alameda F1, Mancebo G2, Baró T1, Navarro G1, Salido M1, Serrano L1, and Carreras R2,3
1Departments of Pathology, Hospital del Mar. Autonomous University of Barcelona, Spain2Department of Obstetrics and Gynecology, Hospital del Mar. Autonomous University of Barcelona, Spain
Abstract
We report the pathological, immunohistochemical and molecular study of a primary tubal serous carcinoma with uterine cervical synchronous tumor, corresponding to a 65-year-old woman with metrorrhagia. The cervical lesion was diagnosed erroneously as endometrial serous carcinoma, based on endometrial biopsy. The surgical specimen showed tumor in the right Fallopian tube and cervical tumors without endometrial lesion. Similar changes in both cervical and tubal tumors were observed. We conclude that the lesion located in the cervical canal was a metastasis of the lesion in the right Fallopian tube.
INTRODUCTIONFallopian tube serous carcinoma is the least frequent tumor of
the female genital tract. It has an incidence of between 0.3% and 1.8% of all malignant genital tract tumors and high mortality. The symptoms include metrorrhagia, pelvic pain, and pelvic tumor [1,2]. Preoperative diagnosis is hindered by the low frequency of these tumors and the differential diagnosis with ovarian tumors. In order for an isolated tumor to be classified as a primary tumor in the Fallopian tube, primary ovarian tumor must be excluded and intraepithelial tubal carcinoma must be demonstrated. The most important prognostic factors are stage at diagnosis and the presence of residual disease after initial surgery [3,4]
On the other hand, gynecological synchronous tumors account for only between 1% and 6% of all genital malignant tumors. The etiology is unclear and the “secondary Müllerian system” theory was proposed to explain the common embryological origin of the epithelia of the uterine cervix, endometrium, Fallopian tube, ovarian surface and the common effect of carcinogen stimuli. Furthermore, Cobb et al., [5], in 2015 reviewed the so called “adenocarcinoma” of Müllerian origin setting a common morphological, immunophenotypical and molecular features of these tumors.
Here we undertook a pathological, immunohistochemical, and ultra structural study of a case of primary high grade Fallopian tube carcinoma with synchronous tumor of the cervix uteri.
CLINICAL HISTORYWe studied the case of a 65-year-old woman who had
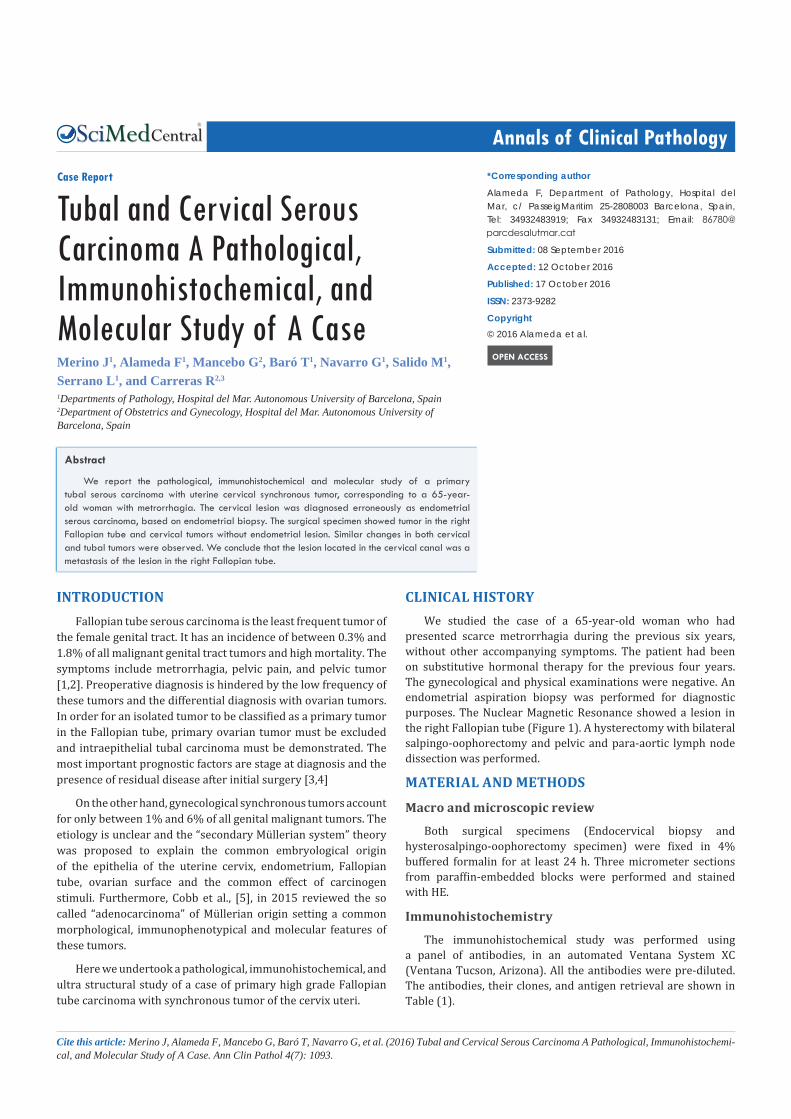
presented scarce metrorrhagia during the previous six years, without other accompanying symptoms. The patient had been on substitutive hormonal therapy for the previous four years. The gynecological and physical examinations were negative. An endometrial aspiration biopsy was performed for diagnostic purposes. The Nuclear Magnetic Resonance showed a lesion in the right Fallopian tube (Figure 1). A hysterectomy with bilateral salpingo-oophorectomy and pelvic and para-aortic lymph node dissection was performed.
MATERIAL AND METHODS
Macro and microscopic review
Both surgical specimens (Endocervical biopsy and hysterosalpingo-oophorectomy specimen) were fixed in 4% buffered formalin for at least 24 h. Three micrometer sections from paraffin-embedded blocks were performed and stained with HE.
Immunohistochemistry
The immunohistochemical study was performed using a panel of antibodies, in an automated Ventana System XC (Ventana Tucson, Arizona). All the antibodies were pre-diluted. The antibodies, their clones, and antigen retrieval are shown in Table (1).
Alameda et al. (2016)Email:
Ann Clin Pathol 4(7): 1093 (2016) 2/5
CentralBringing Excellence in Open Access
Chromosomal study using FISH
Fluorescence in situ hybridization (FISH) was conducted on formalin-fixed and paraffin-embedded (FFPE) tissue sections, as previously described, using two commercially available locus-specific probes for TP53/CEP17 and HER2/CEP17 (Abbott Molecular, Des Plaines, IL), both located in chromosome 17 [6].
Mutation analysis
The DNA of tumoral samples was extracted using the commercial kit QIAamp® DNA Mini Kit (Qiagen) in aQIAcube instrument (Qiagen), following the manufacturer’s instructions. TP53 (complete sequence codifying), KRAS (codons 12, 13) and BRAF (codon 600) mutations were examined using PCR with introns for determining the regions of interest. The PCR product was sequenced using Sanger’s methods with finishing markers (Big Dye v. 3.1) and posterior analysis with capillary electrophoresis in an automated sequencer3500Dx (Applied Biosystems).
RESULTSMacroscopical study
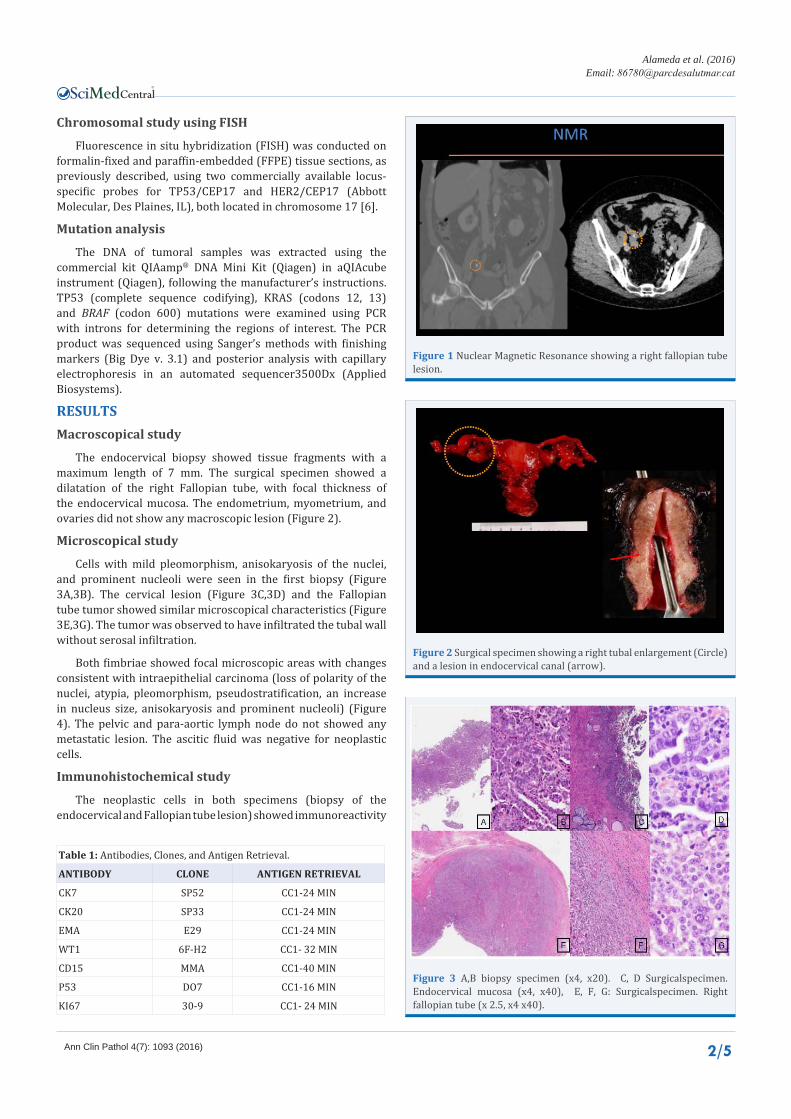
The endocervical biopsy showed tissue fragments with a maximum length of 7 mm. The surgical specimen showed a dilatation of the right Fallopian tube, with focal thickness of the endocervical mucosa. The endometrium, myometrium, and ovaries did not show any macroscopic lesion (Figure 2).
Microscopical study
Cells with mild pleomorphism, anisokaryosis of the nuclei, and prominent nucleoli were seen in the first biopsy (Figure 3A,3B). The cervical lesion (Figure 3C,3D) and the Fallopian tube tumor showed similar microscopical characteristics (Figure 3E,3G). The tumor was observed to have infiltrated the tubal wall without serosal infiltration.
Both fimbriae showed focal microscopic areas with changes consistent with intraepithelial carcinoma (loss of polarity of the nuclei, atypia, pleomorphism, pseudostratification, an increase in nucleus size, anisokaryosis and prominent nucleoli) (Figure 4). The pelvic and para-aortic lymph node do not showed any metastatic lesion. The ascitic fluid was negative for neoplastic cells.
Immunohistochemical study
The neoplastic cells in both specimens (biopsy of the endocervical and Fallopian tube lesion) showed immunoreactivity
Table 1: Antibodies, Clones, and Antigen Retrieval.
ANTIBODY CLONE ANTIGEN RETRIEVAL
CK7 SP52 CC1-24 MIN
CK20 SP33 CC1-24 MIN
EMA E29 CC1-24 MIN
WT1 6F-H2 CC1- 32 MIN
CD15 MMA CC1-40 MIN
P53 DO7 CC1-16 MIN
KI67 30-9 CC1- 24 MIN
Figure 1 Nuclear Magnetic Resonance showing a right fallopian tube lesion.
Figure 2 Surgical specimen showing a right tubal enlargement (Circle) and a lesion in endocervical canal (arrow).
Figure 3 A,B biopsy specimen (x4, x20). C, D Surgicalspecimen. Endocervical mucosa (x4, x40), E, F, G: Surgicalspecimen. Right fallopian tube (x 2.5, x4 x40).

Alameda et al. (2016)Email:
Ann Clin Pathol 4(7): 1093 (2016) 3/5
CentralBringing Excellence in Open Access
for p53, keratin 7, EMA, WT1 and a proliferative index (ki67) around 80%. No immunoreactivity was observed for keratin 20 or CD15 (Figure 5).
The intraepithelial component showed strong immunoreactivity for ki67 and p53 (Figure 6).
The patient was diagnosed with high grade serous carcinoma of the right Fallopian tube, and high grade serous carcinoma of the endocervix.
FISH study
The analysis of fifty non-overlapping cells for both biopsies revealed that the cervical sample showed non-chromosomal abnormalities, whereas the Fallopian tube harbored a monosomy of chromosome 17 in 89% of cells (only one copy of TP53, Her2, and centromere for chromosome 17) (Figure 7).
Mutation analysis
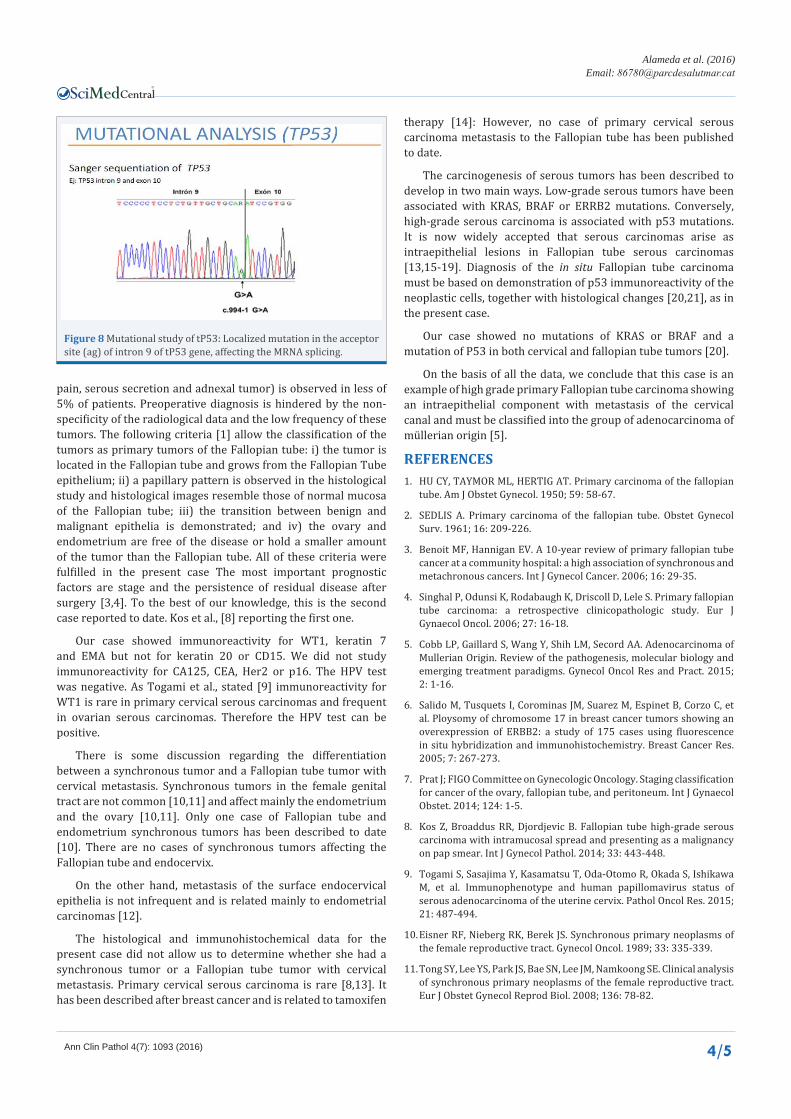
The mutation analysis of the cervical tumor and Fallopian tube tumor detected an alteration in the TP53 gene in the acceptor site of the intron (c.994-1G>A), affecting mRNA splicing
(Figure 8). There were no other alterations in the codons 12 or 13 of the KRAS gene or in the codon 600 of BRAF.
On the basis of these new data, the final diagnosis was serous carcinoma of the Fallopian tube with an intraepithelial component and metastasis to the endocervical canal.
According to the staging classification for cancer of the ovary, fallopian tube and peritoneum [7], the case was staged as T2a N0 M0. The patient was treated with chemotherapy (Carbotaxol, 6 cycles). At the time of writing this paper, the patient was free of the disease.
DISCUSSIONPrimary Fallopian tube carcinomas are infrequent tumors.
Patients with this condition have a mean age of 58 years (range 26-85). Clinical symptoms include metrorrhagia, pelvic pain, and pelvic mass. The clinical triad (Hydrops tubaeprofluens: pelvic
Figure 4 Intraepithelial Carcinoma of the Fallopian tube (x 4 and x 40).
Figure 5 Immunohistochemical study (X 20).Figure 6 Immunohistochemical study of the intraepithelial tubal carcinoma (x 4 and x 10).
Figure 7 Fish and Sish chromosomal study (ERBB2 and TP53). Monosomy of chromosome 17 in fallopian tube sample.
Alameda et al. (2016)Email:
Ann Clin Pathol 4(7): 1093 (2016) 4/5
CentralBringing Excellence in Open Access
pain, serous secretion and adnexal tumor) is observed in less of 5% of patients. Preoperative diagnosis is hindered by the non-specificity of the radiological data and the low frequency of these tumors. The following criteria [1] allow the classification of the tumors as primary tumors of the Fallopian tube: i) the tumor is located in the Fallopian tube and grows from the Fallopian Tube epithelium; ii) a papillary pattern is observed in the histological study and histological images resemble those of normal mucosa of the Fallopian tube; iii) the transition between benign and malignant epithelia is demonstrated; and iv) the ovary and endometrium are free of the disease or hold a smaller amount of the tumor than the Fallopian tube. All of these criteria were fulfilled in the present case The most important prognostic factors are stage and the persistence of residual disease after surgery [3,4]. To the best of our knowledge, this is the second case reported to date. Kos et al., [8] reporting the first one.
Our case showed immunoreactivity for WT1, keratin 7 and EMA but not for keratin 20 or CD15. We did not study immunoreactivity for CA125, CEA, Her2 or p16. The HPV test was negative. As Togami et al., stated [9] immunoreactivity for WT1 is rare in primary cervical serous carcinomas and frequent in ovarian serous carcinomas. Therefore the HPV test can be positive.
There is some discussion regarding the differentiation between a synchronous tumor and a Fallopian tube tumor with cervical metastasis. Synchronous tumors in the female genital tract are not common [10,11] and affect mainly the endometrium and the ovary [10,11]. Only one case of Fallopian tube and endometrium synchronous tumors has been described to date [10]. There are no cases of synchronous tumors affecting the Fallopian tube and endocervix.
On the other hand, metastasis of the surface endocervical epithelia is not infrequent and is related mainly to endometrial carcinomas [12].
The histological and immunohistochemical data for the present case did not allow us to determine whether she had a synchronous tumor or a Fallopian tube tumor with cervical metastasis. Primary cervical serous carcinoma is rare [8,13]. It has been described after breast cancer and is related to tamoxifen
therapy [14]: However, no case of primary cervical serous carcinoma metastasis to the Fallopian tube has been published to date.
The carcinogenesis of serous tumors has been described to develop in two main ways. Low-grade serous tumors have been associated with KRAS, BRAF or ERRB2 mutations. Conversely, high-grade serous carcinoma is associated with p53 mutations. It is now widely accepted that serous carcinomas arise as intraepithelial lesions in Fallopian tube serous carcinomas [13,15-19]. Diagnosis of the in situ Fallopian tube carcinoma must be based on demonstration of p53 immunoreactivity of the neoplastic cells, together with histological changes [20,21], as in the present case.
Our case showed no mutations of KRAS or BRAF and a mutation of P53 in both cervical and fallopian tube tumors [20].
On the basis of all the data, we conclude that this case is an example of high grade primary Fallopian tube carcinoma showing an intraepithelial component with metastasis of the cervical canal and must be classified into the group of adenocarcinoma of müllerian origin [5].
REFERENCES1. HU CY, TAYMOR ML, HERTIG AT. Primary carcinoma of the fallopian
tube. Am J Obstet Gynecol. 1950; 59: 58-67.
2. SEDLIS A. Primary carcinoma of the fallopian tube. Obstet Gynecol Surv. 1961; 16: 209-226.
3. Benoit MF, Hannigan EV. A 10-year review of primary fallopian tube cancer at a community hospital: a high association of synchronous and metachronous cancers. Int J Gynecol Cancer. 2006; 16: 29-35.
4. Singhal P, Odunsi K, Rodabaugh K, Driscoll D, Lele S. Primary fallopian tube carcinoma: a retrospective clinicopathologic study. Eur J Gynaecol Oncol. 2006; 27: 16-18.
5. Cobb LP, Gaillard S, Wang Y, Shih LM, Secord AA. Adenocarcinoma of Mullerian Origin. Review of the pathogenesis, molecular biology and emerging treatment paradigms. Gynecol Oncol Res and Pract. 2015; 2: 1-16.
6. Salido M, Tusquets I, Corominas JM, Suarez M, Espinet B, Corzo C, et al. Ploysomy of chromosome 17 in breast cancer tumors showing an overexpression of ERBB2: a study of 175 cases using fluorescence in situ hybridization and immunohistochemistry. Breast Cancer Res. 2005; 7: 267-273.
7. Prat J; FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet. 2014; 124: 1-5.
8. Kos Z, Broaddus RR, Djordjevic B. Fallopian tube high-grade serous carcinoma with intramucosal spread and presenting as a malignancy on pap smear. Int J Gynecol Pathol. 2014; 33: 443-448.
9. Togami S, Sasajima Y, Kasamatsu T, Oda-Otomo R, Okada S, Ishikawa M, et al. Immunophenotype and human papillomavirus status of serous adenocarcinoma of the uterine cervix. Pathol Oncol Res. 2015; 21: 487-494.
10. Eisner RF, Nieberg RK, Berek JS. Synchronous primary neoplasms of the female reproductive tract. Gynecol Oncol. 1989; 33: 335-339.
11. Tong SY, Lee YS, Park JS, Bae SN, Lee JM, Namkoong SE. Clinical analysis of synchronous primary neoplasms of the female reproductive tract. Eur J Obstet Gynecol Reprod Biol. 2008; 136: 78-82.
Figure 8 Mutational study of tP53: Localized mutation in the acceptor site (ag) of intron 9 of tP53 gene, affecting the MRNA splicing.

Alameda et al. (2016)Email:
Ann Clin Pathol 4(7): 1093 (2016) 5/5
CentralBringing Excellence in Open Access
Merino J, Alameda F, Mancebo G, Baró T, Navarro G, et al. (2016) Tubal and Cervical Serous Carcinoma A Pathological, Immunohistochemical, and Molecular Study of A Case. Ann Clin Pathol 4(7): 1093.
Cite this article
12. X.Matias Guiu. Endometrial Neoplasia. Chap 7 in Gynecologic Pathology. Ed. M.R.Nucci and E.Oliva. Churcill Livingstone 2009.
13. Tang S, Onuma K, Deb P, Wang E, Lytwyn A, Sur M, et al. Frequency of serous tubal intraepithelial carcinoma in various gynecologic malignancies: a study of 300 consecutive cases. Int J Gynecol Pathol. 2012; 31: 103-110.
14. Watrowski R1, Striepecke E, Jäger C, Bauknecht T, Horst C. Papillary serous adenocarcinoma of the uterine cervix during tamoxifen therapy after bilateral breast cancer. Anticancer Res. 2012; 32: 5075-5078.
15. Vang R, Shih I, Kurman R. Ovarian low-grade and high-grade serous carcinoma: pathogenesis, clinicopathologic and molecular biologic features, and diagnostic problems. Adv Anat Pathol. 2009; 16: 267-282.
16. Crum CP, Drapkin R, Kindelberger D, Medeiros F, Miron A, Lee Y. Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer. Clin Med Res. 2007; 5: 35-44.
17. Kurman RJ, Shih IeM. The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol. 2010; 34: 433-443.
18. Maeda D, Ota S, Takazawa Y, Ohashi K, Mori M, Imamura T, et al. Mucosal carcinoma of the fallopian tube coexists with ovarian cancer of serous subtype only: a study of Japanese cases. Virchows Arch. 2010; 457: 597-608.
19. Przybycin CG, Kurman RJ, Ronnett BM, Shih IeM, Vang R. Are all pelvic (nonuterine) serous carcinomas of tubal origin? Am J Surg Pathol. 2010; 34: 1407-1416.
20. Kuhn E, Kurman RJ, Vang R, Sehdev AS, Han G, Soslow R, et al. TP53 mutations in serous tubal intraepithelial carcinoma and concurrent pelvic high-grade serous carcinoma--evidence supporting the clonal relationship of the two lesions. J Pathol. 2012; 226: 421-426.
21. Vang R, Visvanathan K, Gross A, Maambo E, Gupta M, Kuhn E, et al. Validation of an algorithm for the diagnosis of serous tubal intraepithelial carcinoma. Int J Gynecol Pathol. 2012; 31: 243-253.