ueda2016 the role of gut microbiota in the pathogenesis of obesity & tdm2 - amr mattar
TRANSCRIPT

الرحيمالرحمنهللابسم
الحمد هلل
والصالة والسالم على رسول هللا

The role of gut microbiota in the pathogenesis of obesity and TDM2
Prof.Amr Mattar
President of the EgspenHead of clinical nutrition unit Kasr Aleini T.hospitals
ESPEN teacher

Items
• Introduction
Microbiota – microbiome – gut flora
• Symbiotic relationships and functions
• Evidence connecting microbiota to OB&TDM2
• Mechanisms of causality
• Potential Therapeutic capabilities ?
• Summary
3

• The human microbiota is the aggregate of microorganisms, They include bacteria, fungi, and archaea.
• The human microbiome refer to their genomes =genetic material of an organism.
• The Microbiome is studied via gene sequencing techniques of the DNA/RNA not by culture techniques

Symbiotic Relationships
• Symbiosis means “to live together”
• Describes the relationship between microorganisms and their host
• Three types
– Mutualism
– Commensalism
– Parasitism
dysbiosis (= abnormal microbiota composition)
16-Feb-16 5

GUT MICROBIOTA COMPOSITION
• Bacterial communities show :
similarity in anatmical sites-
considerable inter-individual variability
&intra-individal variability (Robinson et al., 2010)
• The Microbiome is most similar in twins, differing some degree within family members and further differing amongst unrelated family members
• Bacterial groups share functionalities (Turnbaugh et al., 2009b; Burke et al., 2011)
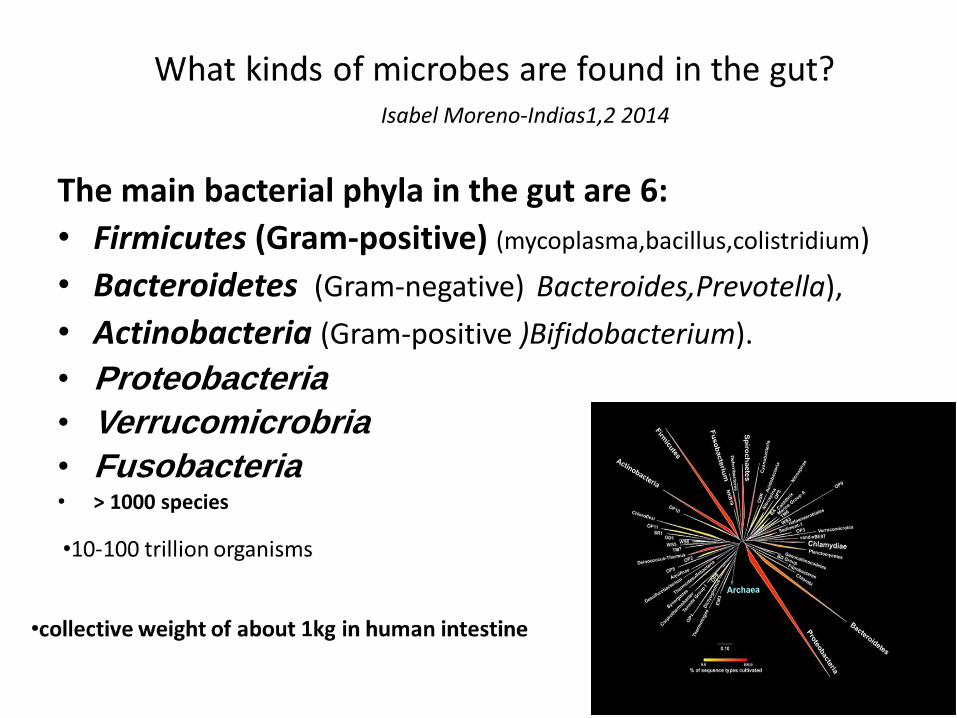
The main bacterial phyla in the gut are 6:
• Firmicutes (Gram-positive) (mycoplasma,bacillus,colistridium)
• Bacteroidetes (Gram-negative) Bacteroides,Prevotella),
• Actinobacteria (Gram-positive )Bifidobacterium).
• Proteobacteria
• Verrucomicrobria
• Fusobacteria• > 1000 species
Isabel Moreno-Indias1,2 2014

8Presentation Title Here |
Similarity in anatomical
site with inter and intra
personal variations
Skin and vaginal sites showed smaller diversity than the mouth and gut, these showing the greatest richness
gut bacteria being termed a "forgotten" organ

Bacterial phyla have specific site-distribution in healthy humans
Nature 449, 811-818. 2007
Bacteroidetes
Firmicutes
COLON
SKIN
MOUTH
ESOPHAGUS
STOMACH
VAGINA

Hartstra/nieuwdorp, Diabetes Care 2014. pH dictates bacterial survival and gut microbiota composition
“Functionality”
Each group has a certain fuction in their site

Acquisition of Normal Microbiota
• Intrauterine life is generally free of microorganisms
• Microbiota begins to develop during the birthing process (birth canal)
• Vaginal vs Caesarian
• Similar composition to the adult microbiota at 2–3 years of age with Firmicutes and Bacteroidetes predominating
16-Feb-16 12

TEMPORAL DYNAMICS OF MICROBIOTA
• Stable composition in healthy adults
• Altered transiently by diet, disease,drugs, stress and environment (Delgado et al,2006)
• Dietary changes could explain 57% of the total structural variation in gut microbiota
• Changes in genetics accounted for no more than 12% (Zhang et al., 2010).
• ↑ fat intake produces an increase in the Gram-negative/Gram-positive index of our microbiota

A fine balance of gut microbes PATHOGENS
Dysbiosis=diseases
• Sepsis, infection
• Inflammation
• Liver damage
• Production of carcinogens
• Diarrhea, constipation
• Obesity &diabetes??!
COMMENSALSGut Microbiota Functions
• Inhibit pathogen growth
• Convert pro-drugs to active metabolites
• Degrade polysaccharides of plant origin
• Produce folate and Vitamin K
• Produce short-chain fatty acids SCFA
• Stimulate and modulate immune function
• Regulate body fat storage
• Maintain gut barrier function
• Stimulate gut motility
• Bile acid metabolism

Low diversity and imbalances in gut microbiota are associated with human disease states Simon C,etal.2015
Health• High biodiversity and richness• Stable• Primarily Bacteroides and Firmicutes
Disease• Low biodiversity• Unstable• Increased abundances of Proteobacteria,
Fusobacteria, Verrucomicrobia• C. Difficile colitis, IBD, IBS, obesity, metabolic
syndrome, peripheral vascular disease, renal disease, diabetes and cancer

Evidence connecting microbiota to Obesity and TDM2
Microbiota transplant (MT) to germ free mice increased intestinal absorption of monosaccharides, IR, enhanced triglyceride synthesis (Backhed et al., 2004)
• Dysbiotic gut microbiota may work as a contributing factor in diet-related obesity in mice (Backhed et al., 2004)
Obese mice have different gut microbiota from lean (Ley etal.,2005)
Turnbaugh,etal. (2006). demonstrated that “MT from genetically obese mice to axenic mice provokes a very significant weight increasecompared with transplantation from lean mice”
Germfree mice were shown to be resistant to high-sugar, high-fat, “Western” diet-induced obesity (Backhed et al., 2007).

Evidence connecting microbiota to the obesity and TDM2
In obese mice significant reduction in Bacteroidetes and a corresponding increase in Firmicutes (Ley,2006).
Ley etal. (2007) were the first to report an altered gut microbiota similar to that found in obese mice in humans
• Armougom ,etal.(2009) confirmed a reduction in Bacteroidetes
• Kalliomäki ,etal.(2008) proposed that Staphylococcus aureus may act as a trigger of low-grade inflammation, contributing to the development of obesity and TDM2.
In mice fed a high-fat diet, the activation of liver resident macrophages Kupffer cells promotes hepatic IR and glucose intolerance. (Mayu .S,etal. 2015)

Evidence connecting microbiota to the obesity and TDM2
“MT from obese humans increased fat deposits in lean recipients” (Ridaura et al., 2013).
• “Obesity and IR in mice could be significantly reduced by diminishing the gut microbiota with BS antibiotics” (Cani et al., 2008).
“MT from healthy donors improved insulin resistance in the first six weeks in diabetic human volunteers” (Vrieze et al., 2012).
• “A whole-grains diet,reduces endotoxin producers and enrich beneficial bifidobacteria in the gut of obese adult human volunteers, leading to significant alleviation of inflammation, adiposity and IR. (Xiao et al., 2014, Fei and Zhao, 2013).

Dietary intervention (CHO) corrected the dysbiosis of the gut microbiota,andmetabolic deteriorations in genetic(PWS) as well as simple obesity in chidren .
( Chenhong Zhang etal,2015)
• “Association of T2DM with impaired butyrate production” , as oral supplementation with butyrate can reverse insulin resistance in dietary-obese mice and increase energy expenditure
( Donohoe 2011)
• The gut microbes of obese humans are less diverse than lean twins (Turnbaugh PJ,2009),
RYGB change in the gut microbiota upon transplantation of RYGB-related fecal microbiota directly contributed to reduced weight and adiposity
(Mayu.S,etal. 2015)
• Thus, compelling evidence suggests that the gut microbiota serves as a pivotal contributing factor in the development of diet-related obesity &TDM2 in both mice and humans.

Dominant Gut Microbiota in Obese Individuals
• Lower relative abundance of Bacteroidetes and a proportional increase in Firmicutes in obese mice and humans
(Ley et al. 2005,2007)
• Obesity is associated with increased abundance of Lactobacillus and Staphylococcus ,Firmicutes and Prevotellaceae
(Omotayo,O etal.2014)
• Enrichment of the family Christensenellaceae has been found in lean individuals which, when transplanted to mice, have shown to promote a lean host phenotype [Goodrich, J.K 2014].
• Normal weight is associated with Bifidobacterium, Methanobrevibacter, and Bacteroidetes (Millionem2013)

Gut microbiota composition in DM2
• Enrichment of Lactobacillus gasseri and Streptococcus mutans in fecal sample has predictive value for developing insulin resistance
• Reduced Roseburia species and Faecalibacterium prausnitzii (short-chain fatty acid butyrate producers) in DM2
Karlsson, Nature 2013

Mechanisms by Which MicrobiotaMay Contribute to the Development
of Obesity and TDM2
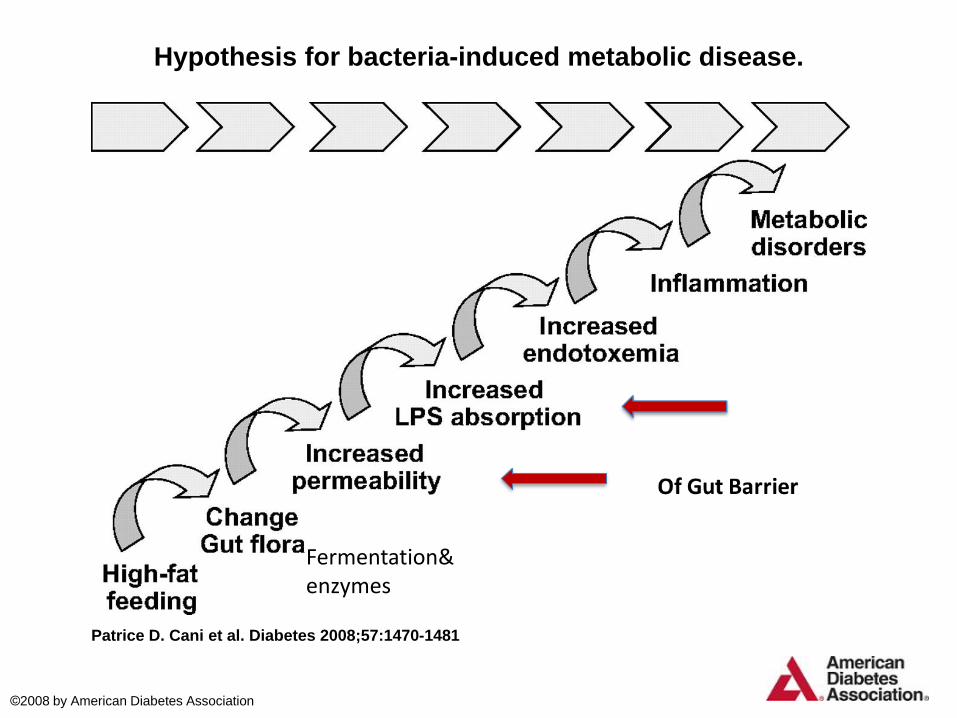
Hypothesis for bacteria-induced metabolic disease.
Patrice D. Cani et al. Diabetes 2008;57:1470-1481
©2008 by American Diabetes Association
Fermentation&enzymes

Simple explanation of the role of microbiota in metabolic disease
causation
Smits/Nieuwdorp, Gastroenterology 2013
F prausznitzii lower
Ruminococcus lower
diabetes
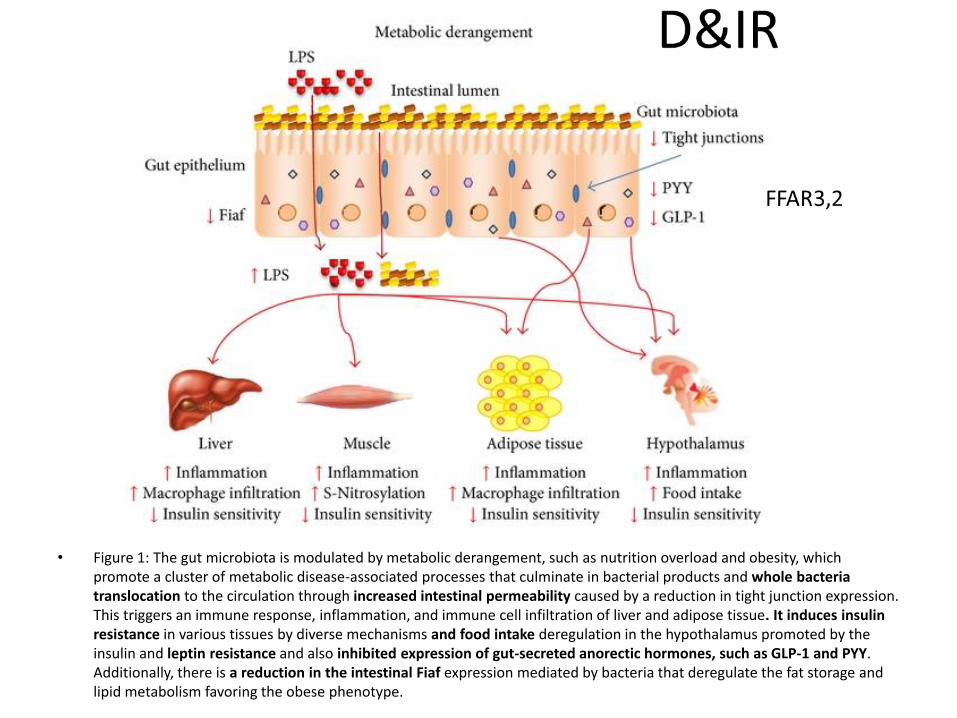
• Figure 1: The gut microbiota is modulated by metabolic derangement, such as nutrition overload and obesity, which promote a cluster of metabolic disease-associated processes that culminate in bacterial products and whole bacteria translocation to the circulation through increased intestinal permeability caused by a reduction in tight junction expression. This triggers an immune response, inflammation, and immune cell infiltration of liver and adipose tissue. It induces insulin resistance in various tissues by diverse mechanisms and food intake deregulation in the hypothalamus promoted by the insulin and leptin resistance and also inhibited expression of gut-secreted anorectic hormones, such as GLP-1 and PYY. Additionally, there is a reduction in the intestinal Fiaf expression mediated by bacteria that deregulate the fat storage and lipid metabolism favoring the obese phenotype.

GUT BARRIER FUNCTIONAND MICROBIOTA
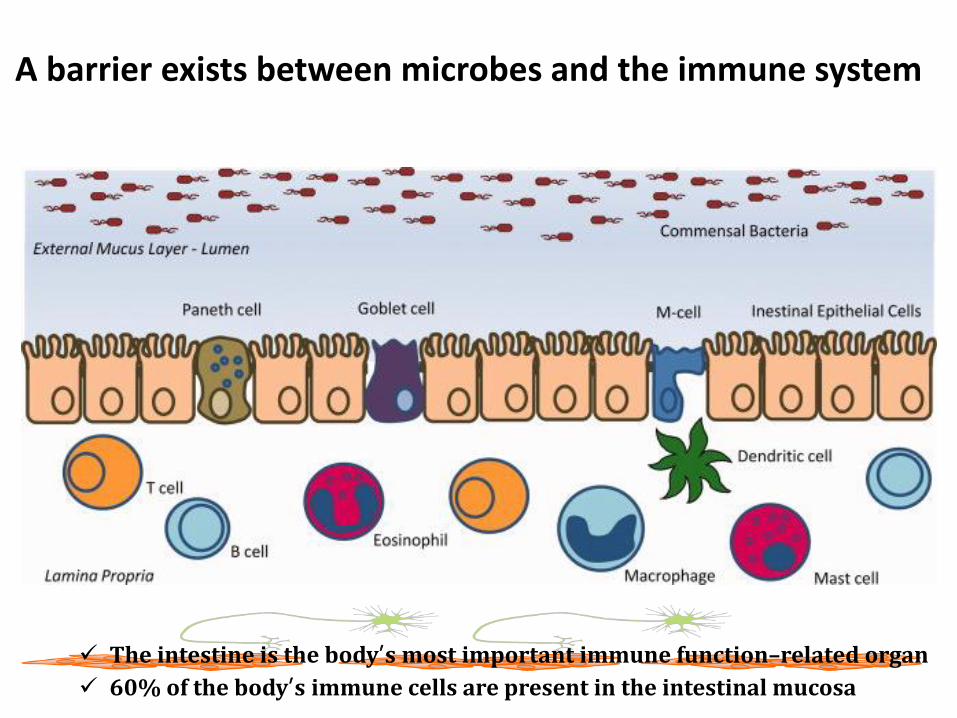
A barrier exists between microbes and the immune system
The intestine is the body’s most important immune function–related organ
60% of the body’s immune cells are present in the intestinal mucosa

Components of the intestinal barrier
Image adapted from: Hooper LV (2009) Nat Rev Microbiol 7(5):367-74
Physical barrier(the epithelium)
Chemical barrier(mucus layer)
Immunological
barrier(immune cells of the lamina
propria)
Microbial barrier(commensal bacteria)
Muscle layers (smooth muscle intestinal
wall)

Tight junctions maintain barrier between epithelial cells
It acts as a gate-keeper that allows the translocation of essential macronutrients but restricts the passage of bacteria, toxic molecules and luminal antigens such as LPS (Moran,2014] which may induce the production of numerous inflammatory cytokines[Moran, C.; 2014)

A breakdown in gut barrier function has been linked with numerous diseases
• Inflammatory bowel disease
• Chronic kidney disease
• Sepsis
• Necrotizing pancreatitis
• Celiac disease
• Type 1 diabetes
• Food allergies
• Alcoholic liver disease
• Obesity&TDM2
Local and systemic inflammation

Gut Microbiota and the Innate Immune System Link Metabolic Endotoxemia to Insulin Resistance

mechanism
DietDrugs

1.Suppression of fasting-induced adipose factor (Fiaf)
• Fiaf is produced by white and brown adipose tissue and the intestines
• Stimulates fatty acid oxidation& uncoupling in fat
• Causes Up to 50%reduction in adipose tissue weight
(Conterno, L. 2011).
• Fiaf suppression by microbiota induces fat storage.

2.Short chain Fatty acid production (SCFA =energy harvest)
• Colonic fermentation of indigestible saccharides SCFA production
• Acetate, propionate and butyrate, formate, lactate and ethanol and mixed gases(e.g., CO2, CH4 and H2) and are ligand for GPCRs [Payne, 2011]
• SCFA provide daily 5%–15% of dietary energy to the host
• Butyrate is the main energy source to colonocytes 70% of their energy needs [Scheppach 1998]
• 95% of the SCFA are absorbed, and only 5% is excreted in feces
• The liver takes up to 30% of SCFA from the portal circulation
• A microbiota with greater energy extraction efficiency resulted in less energy left over in feces and greater levels of short-chain fatty acids (SCFAs) in the cecum e higher energy storage

3. Adenosine Monophosphate Activated Protein Kinase (AMPK)
• AMPK -is a key enzyme that controls cellular energy -increases energy utilization -increases beta oxidation of fatty acids leading to -depletion of fat and glycogen stores.
(Kotzampassi, K.; 2014)
• The down-regulated expression of AMPK by gut microbiota, inhibiting FA oxidation increases adipose tissue storage obesity
(Chen, J.; 2014 )

4.Activation of G-protein coupled receptors (GPCR41&GPCR43)
• Are indulged in glucose and lipid metabolism (Den Besten,2013)
• SCFA Acetate, propionate and butyrate are the ligandsfor these receptors (also known as free fatty acid receptors (FFAR)-3 and FFAR-2, respectively)
(Brown, A.J.; 2003)• The activation of GPCR41 and GPCR43 may increase
gut hormones such as glucagon-like peptide-1 (GLP-1) and peptide YY (PYY) (Den Besten,2013)

• GLP1 stimulates insulin secretion which slows down gastric emptying and promotes satiety (vectoza&succenda)
• PYY secretion -decelerates intestinal transit and -suppresses gut motility, and in turn, -food digestion and absorption of nutrients are +also it boosts the action of insulin on glucose absorption in
adipose and muscle tissue [Den Besten,2013 ]
• GPCR may also regulate the inhibition of lipolysis by a joint action on
-hormone-sensitive lipase (HSL) and -adipose triglyceride lipase (ATGL)(Amisten, S.; 2015).
• The GPCR41 ligand butyric acid has been reported to inhibit lipolysis (Ohira, H.;2013)

5. Leaky-Gut and Inflammation
• LPS is continuously produced by Gram-negative bacteria in the gut and is translocated through the intestinal capillaries by a mechanism involving Toll-Like receptor 4 (TLR-4) (Neal, M.D 2006].
• The increase in the uptake of LPS and the permeability of the intestine induces :
-a systemic inflammation with elevated fat deposition in the liver - high circulating levels of IL-1, IL-6, plasminogen
activator inhibitor-1 (PAI-1) (TNF-α) in the blood [Gordon etal,2014].
• Low grade inflammation is associated with leptin and insulin resistance (Hotamisligil,etal. 2006)
• plasma levels of LPS have also been associated with induction of hyperphagia and obesity (Dockray, G.J. 2013)

6. Endocannabinoid System
• This system regulates metabolism and appetite by the microbiota-gut-brain axis, playing a major role in energy homeostasis
• The eCB system shows very high tone in obesity.
• LPS has been found as a potent stimulator of the synthesis of eCBs (Geurts, L.; 2011)
appetite &hyperphagia
• Rimonabant (Acomplia) CB1 antagonists

7.Microbiota controlling eating behaviour and satiety[Alcock,2014]
mechanisms • microbial manipulation of reward
pathways,=motivation (reward) to eat
• production of toxins that alter mood
• changes to receptors including taste, cannabinoid and opioid receptors
• hijacking of neurotransmission via the vagus nerve , which is the main neural axis between the gut and the brain. Maestro Rechargeable System

• Antibiotics– Kill both good and bad bacteria– Original microbiota usually return once drugs are removed– Can allow for the growth of pathogens
• Probiotics – Giving back live beneficial microorganisms– Do not colonize
• Prebiotics– Non-digestible food substances that provide substrate for existing beneficial
microbes already present in the gut NM504,5
• Diet– Changes activity of existing microbes
• Fecal transplants– Changing complete gut ecosystem
Methods to manipulate gut microbiota

faecal transplantation studies have implicated that butyrate-producing intestinal bacteria can be considered as key players in human glucose and lipid metabolism.

• No adverse effects!
A.Vrieze, Gastroenterology 2012

Eubacterium Halli as novel therapeutic in in insulin resistance?
• Has beneficial effects on insulin sensitivity
• Potential mechanism via bileacids and brown fat (Increased Energy Expenditure)
• Human intervention phase 1 dosefinding trial with E.hallii curently ongoing at AMC
•
De Vos WM and Nieuwdorp M. Nature 2013; 498(7452):48-9
Eubacterium hallii


Our gut Microbiota can
be pictured as a
MICROBIAL
hidden metabolic
‘organ
“small world within",

هلل الحمد
Thank you
The intestine is the body’s most important immune
function–related organ
60% of the body’s immune cells are present in the
intestinal mucosa
The immune system controls immune responses
against:
Dietary proteins
Prevention of food allergies
Pathogenic microorganisms
Viruses (Rotavirus, Poliovirus)
Bacteria (Salmonella, Listeria, Clostridium etc.)
Parasites (Toxoplasma)
Contd….
50
51/30
FMT for treatment of disease• Where we are now
– Published data and studies encouraging for treatment
of refractory C. difficile colitis
• What is needed – Adequate and well-controlled clinical trials to evaluate
therapeutic potential of FMT for treatment of C. difficile colitis and other diseases
• What would be ideal – Identify the key microbes in fecal material responsible
for beneficial effects leading to efficacious, defined products targeted for specific diseases

52/30
Potential long-term effects of alterations
in the gut microbiome
• immune status
• nutritional status– body weight
– nutrient absorption
– diabetes risk
– cardiovascular risk
• autoimmune status
• wound repair/fibrosis
• cognition/mood
• cancer risk
• other?

53/30
Gut microbiota synthesizes a large amount of glycoside hydrolases
break down complex plant polysaccharides to monosaccharides and short-chain
fatty acids, mainly acetate, propionate, and butyrate.-
1-important source of energy for de novo lipogenesisa,
2-ligands for 2 important G protein-coupled receptors
Gpr41&Gpr43 of gut enteroendocrine cell(samuel 2008)
stimulate secretion of PYY, which inhibits gut motility and slows intestinal
transit thereby enhancing nutrient absorption.
Gpr41 deficiency was associated with decreased expression of PYY, faster
intestinal transit rate, and reduced harvest of energy from the diet
PPYGut microbiota modulates gut-derived peptide secretion
PYY.

54/30
GLP-1 secretion.
Gut microbiota fermentation of prebiotics promoted L-cell differentiation in the
proximal colon of rats and increased glucagon-like peptide (GLP)-1 response
to a meal in healthy humans (45,46). Ob/ob mice treated with prebiotic
carbohydrates had altered gut microbiomas and increased circulating GLP-1
and GLP-2 (47). Further supporting the relevance of GLP-1 in mediating
prebiotic action, genetic or pharmacological deletion of GLP-1 prevented the
beneficial effects of prebiotics on weight gain, glucose metabolism, and
inflammatory pathway activation

55/30
GLP2

Introduction
GUT MICROBIOTA
COMPOSITION ↑• Bacterial communities at a particular body site have more similarity among different
subjects than in the same subject but at different body sites; i.e., there is more similarity between oral bacterial communities of different individuals than between the bacterial communities of the skin and the mouth in a single individual (Costello et al., 2009), although there is also consid- erable inter-individual variability (Costello et al., 2009; Robinson et al., 2010).
• Metagenomic studies have established that in spite of the high interpersonal vari- ability, some bacterial groups share functionalities (Turnbaugh et al., 2009b; Burke et al., 2011). The main bacterial phyla are: Firmicutes (Gram-positive), Bacteroidetes (Gram-negative), and Actinobacteria (Gram-positive).
• Firmicutes is found in the highest proportion(60%),with more than200genera,the most important of which are:Mycoplasma, Bacillus, and Clostridium;
• Bacteroidetes and Actinobacteria each comprise about 10%of the gut microbiota, with the rest belonging to over10 minority families.In total there are more than 1000 different species in the gut
• It has also been suggested that the microbiota of most individuals can be categorized into three predominant enterotypes dominated by three different genera: Bacteroides, Prevotella, and Ruminococcus, which are independent of age,gender, ethnicity,or body mass index(BMI; Benson etal.,2010; Arumugametal.,2011).
• Isabel Moreno-Indias1,2 2014
