unclassified transfusion practices with combat wounded francis (frank) m. chiricosta, ltc, mc...
TRANSCRIPT
UNCLASSIFIED www.milblood.mil ASBPO
Transfusion Practices with Combat Wounded
Francis (Frank) M. Chiricosta, LTC, MC
Transfusion Medicine Consultant, US Army
UNCLASSIFIED www.milblood.mil ASBPO
Overview
• Massive Transfusion / Coagulopathy
• Resuscitation change in practices
• Traditional Guidelines / Practices
• Use of plasma
• Use of Fresh Whole Blood
• Factor VIIa
• Age of blood
UNCLASSIFIED www.milblood.mil ASBPO
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Prehospital First 24 hours After 24 hours
Per
cent
age
of d
eath
s
Hemorrhage CNS Other
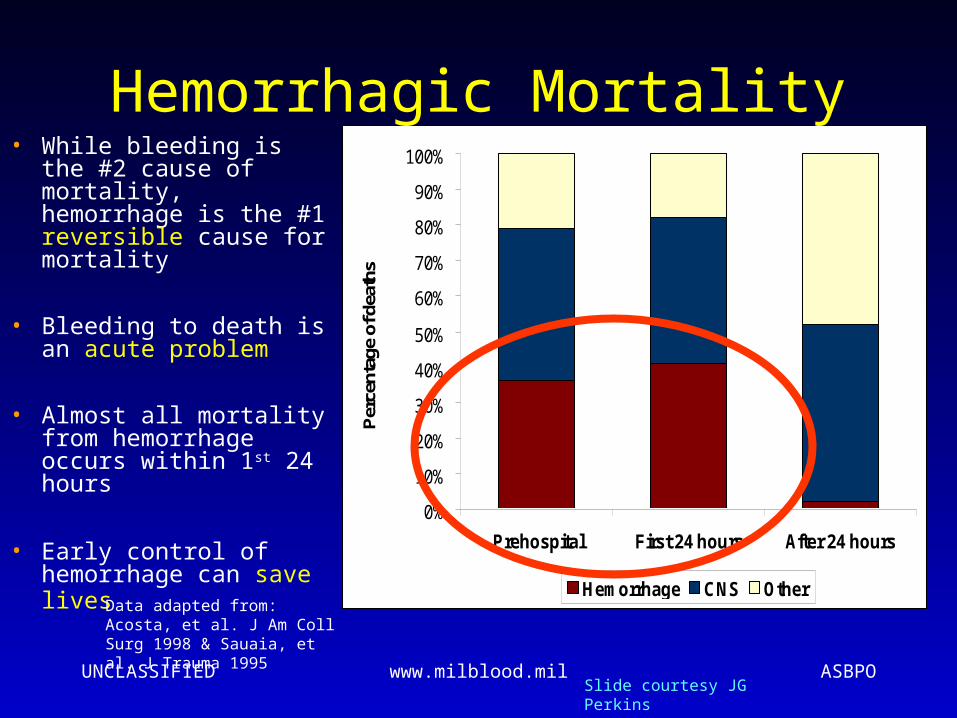
Hemorrhagic Mortality• While bleeding is the
#2 cause of mortality, hemorrhage is the #1 reversible cause for mortality
• Bleeding to death is an acute problem
• Almost all mortality from hemorrhage occurs within 1st 24 hours
• Early control of hemorrhage can save lives Data adapted from: Acosta, et al.
J Am Coll Surg 1998 & Sauaia, et al. J Trauma 1995
Slide courtesy JG Perkins

UNCLASSIFIED www.milblood.mil ASBPO
Massive transfusion
• One body volume in 24 hours
• “Dilutional” coagulopathy– depleted coagulation factors– thrombocytopenia– hypoperfusion– confounding conditions: DIC, sepsis
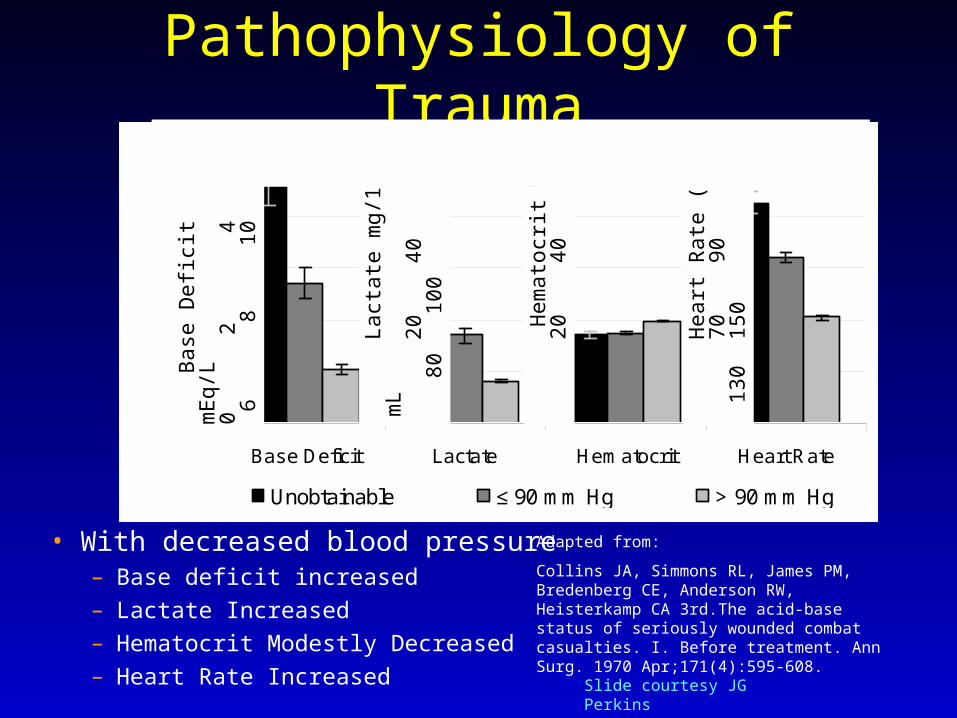
Pathophysiology of Trauma
• With decreased blood pressure– Base deficit increased– Lactate Increased– Hematocrit Modestly Decreased– Heart Rate Increased
Adapted from:
Collins JA, Simmons RL, James PM, Bredenberg CE, Anderson RW, Heisterkamp CA 3rd.The acid-base status of seriously wounded combat casualties. I. Before treatment. Ann Surg. 1970 Apr;171(4):595-608.
Base Deficit Lactate Hematocrit Heart Rate
Unobtainable ≤ 90 mm Hg > 90 mm Hg
B
ase
Def
icit
mE
q/L
0
2
4
6
8
1
0
Lact
ate
mg/
100
mL
20
40
6
0
80
100
Hem
atoc
rit %
20
40
Hea
rt R
ate
(BP
M)
70
90
11
0 1
30 1
50 N=450 combat casualties in the Vietnam War on Admission
Slide courtesy JG Perkins
Pathophysiology of Trauma
Coagulopathy
Acidosis
Hypothermia
UNCLASSIFIED www.milblood.mil ASBPO
Traditional resucitation• Replace lost volume first with crystalloid• May be able to restore normal BP• Blood transfusion comes later• Potential complications of aggressive fluid
resuscitation– “Pop the clot”– Hemodilution– Coagulopathy– Hypothermia– Acidosis
UNCLASSIFIED www.milblood.mil ASBPO
Damage Control Resucitation• Do not replace volume quickly• Hypovolemia / hypotension is tolerated• Stop bleeding• Correct abnormal physiology later• “... inaccessible or uncontrolled sources of blood
loss should not be treated with intravenous fluids until the time of surgical control.” --Cannon WB, FaserJ, CollewEM: The preventive treatment of wound shock. JAMA, 47:618, 1918
1918! Not a totally new idea

UNCLASSIFIED www.milblood.mil ASBPO
Coagulopathy of Trauma
• Hemodilution due to resucitation… and
• Coagulopathy that is due to the trauma itself
• Evidence that coagulopathy starts before fluid resuscitation; not a dilutional coagulopathy
• Molecular mechanism: thrombomodulin, protein C (Brohi, K)
UNCLASSIFIED www.milblood.mil ASBPO
Massive Transfusion,Transfusion considerations
• assessment: clinical and lab together– microvascular bleeding– PT/PTT > 1.5 nl, plt < 50 – 100– Warm patient
• one 6-pk platelets roughly same coag. factors as U FFP
• Plt, CRYO, FFP short/difficult supply
• Fresh whole blood
UNCLASSIFIED www.milblood.mil ASBPO
Massive Transfusion,Problematic transfusion management
– Transfused plasma is foreign to recipient; has anti-A, -B; A substance, B substance
– ABO incompatible plasma (e.g. type O rbc/WB/Plt to type A patient) may be associated with adverse outcome (Blumberg, N)
UNCLASSIFIED www.milblood.mil ASBPO
Massive Transfusion,complications
• Citrate toxicity– Hypocalcemia, prolonged QT– With normal liver, not generally a problem– Rapid infusion centrally can be a problem– Alkalosis with metabolism
• Hyperkalemia?– Usually the opposite: with metabolic
derangement, K+ goes low– Theoretic problem in renal failure
UNCLASSIFIED www.milblood.mil ASBPO
Massive Transfusion,complications
• Hypothermia (use of blood warmer)– PT/PTT elevation– Platelet dysfunction
• Dilutional coagulopathy
• Old blood is bad blood?
• Transfusion reactions– More error prone– Less likely to recognize
UNCLASSIFIED www.milblood.mil ASBPO
Packed Red Blood Cellspurpose of the transfusion
• To increase oxygen carrying capacity in an anemic patient when it is needed
• Need is based on clinical assessment of risk of complications of low oxygen delivery (e.g.. when cardiac oxygen demand increases to increase cardiac output)
UNCLASSIFIED www.milblood.mil ASBPO
Traditional Guidelines
UNCLASSIFIED www.milblood.mil ASBPO
Existing Guidelines
• Red cell transfusion– Purpose: oxygen carrying– loss of 30%+ of blood volume– normovolemic, P>100, SBP<100, ssx
• Diluent: normal saline only
• Assessment: clinical; H/H may not be valid
• Golden Hour
UNCLASSIFIED www.milblood.mil ASBPO
Red Cell Indicationsclinical studies
• Hébert, et al. 1999– randomized, controlled clinical trial, 838 critically ill
patients• liberal group: Hb tx. trigger 10g/dl• restrictive group: trigger 7 g/dl
– findings:• overall 30-day mortality similar (p=0.11)• lower rates for restrictive group for less acutely ill and
age<55 (p=0.02, 0.03)• in-hospital mortality rate lower in restrictive group
(p=0.05)
UNCLASSIFIED www.milblood.mil ASBPO
Red Cell Indicationsclinical studies
• Hébert, et al. 1999– findings:
• liberal group had significantly higher rates for:– MI (p=0.02)– pulmonary edema (p<0.01)
• no significant difference in other complications• trend toward lower 30-day mortality in
restrictive group• decreased blood exposure in restrictive group

UNCLASSIFIED www.milblood.mil ASBPO
Red Cell Indicationsclinical studies
• Carson, 1998– almost 9000 patients 60 years and older getting hip
fracture repair– at pre-transfusion Hb (“trigger”) of 8 to 10 g/dl, no
difference in 30- and 90-day mortality between transfused and not transfused
• Weiskopf, 1998– experiment in isovolemic hemodilution in 23 healthy
adults– Hb as low as 5g/dl tolerated at rest
UNCLASSIFIED www.milblood.mil ASBPO
Treating Bleeding Related to Coagulation Abnormalities
Platelets, FFP, and CRYO
• General rule: If bleeding greater than expected and is of a microvascular nature and lab values meet threshold (or not available in time or dysfunction of hemostasis is known or suspected)
UNCLASSIFIED www.milblood.mil ASBPO
Microvascular Bleeding
• surgical: wetness/oozing from all or most exposed tissue, no visible vessel to mechanically stop
• non-surgical:– ecchymosis at sites other than surgical wound– oozing around catheters; from mucosal
surfaces
UNCLASSIFIED www.milblood.mil ASBPO
PlateletsIndications, Guidelines and Practice Parameters• American Society of Anesthesiology
– Prophylactic transfusion is rarely indicated if thrombocytopenia is due to increased destruction
– With surgery, • usually not indicated >100,000• usually indicated <50,000• between 50 and 100,000: base on risk of bleeding
– With microvascular bleeding, • same guidelines as for surgery• known platelet dysfunction
– Procedures associated with insignificant blood loss may be done <50,000
UNCLASSIFIED www.milblood.mil ASBPO
Fresh Frozen PlasmaIndications, Guidelines and Practice Parameters
• American Society of Anesthesiology, 1996– urgent reversal of warfarin effect– correction of known factor deficiency– for correction of microvascular bleeding in the
presence of elevated (>1.5 x nl.) PT or PTT– for correction of microvascular bleeding in a
patient who has received >1 blood volume
UNCLASSIFIED www.milblood.mil ASBPO
Fresh Frozen PlasmaIndications, Guidelines and Practice
Parameters
• College of American Pathologists, 1994– with active bleeding or procedure and
• PT* 1.5 x midpoint of normal (18s) or• PTT* 1.5 x top of normal (51s)
– in massive transfusion with microvascular bleeding and coagulation abnormality
*fibrinogen must be normal, >100mg/dl; patient not on heparin
UNCLASSIFIED www.milblood.mil ASBPO
Fresh Frozen PlasmaInappropriate Use
• Volume expander, Source of albumin, When heparin is cause of lab abnormality, When a specific therapy is available (VIII, IX, ATIII, Vitamin K, DDAVP)
• On a routine schedule with red cell transfusion (prophylactically in massive transfusion) British JH 2004
UNCLASSIFIED www.milblood.mil ASBPO
Evidence against Routine Schedule of Plamsa in Massive Transfusion
Mannucci et al. Vox Sang 42(3):113-23 (1982)
“Standard schemas involving the administration of platelet concentrates and/or fresh-frozen plasma without evaluation of hemostasis … failed to decrease the requirements for … packed red cells. Therefore, indiscriminate administration in the massively transfused postoperative patient of blood components based on preestablished schemes appears to be unjustified.”
UNCLASSIFIED www.milblood.mil ASBPO
Current Practice with Plasma
• More aggressive? earlier
• Agrees with traditional guidelines:– Apply aggressive strategy for patients that
present with coagulopathy– Is treating bleeding assoc with abnl lab
• Apparent conflict with guidelines (ratio, routine schedule), but not if there is evidence of coagulopathy
UNCLASSIFIED www.milblood.mil ASBPO
Evidence Supporting use of1:1 Ratio RBC:plasma
• Borgman, MA. J Trauma 2007
• Retrospective study
• Stratified patients by ratio of plasma:rbc
• Improved outcome with higher plasma proportion
UNCLASSIFIED www.milblood.mil ASBPO
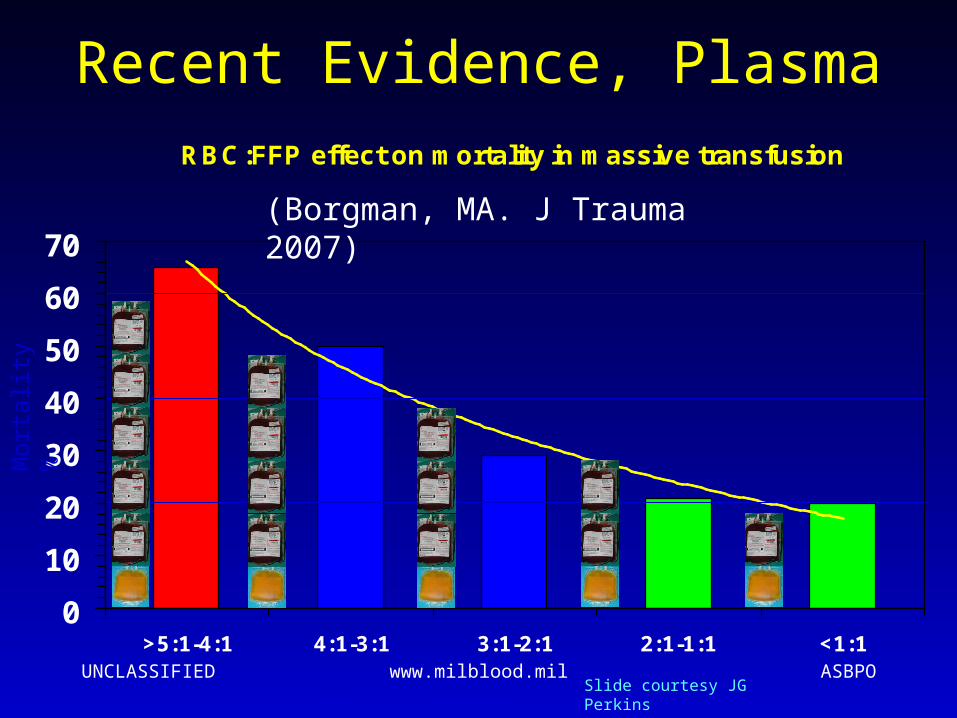
Recent Evidence, PlasmaRBC:FFP effect on mortality in massive transfusion
0
10
20
30
40
50
60
70
>5:1-4:1 4:1-3:1 3:1-2:1 2:1-1:1 <1:1
Mor
talit
y %
RBC:FFP ratio
(Borgman, MA. J Trauma 2007)
Slide courtesy JG Perkins
UNCLASSIFIED www.milblood.mil ASBPO
Evidence Supporting use of Apheresis Platelets
• Retrospective study pts at Ibn Sina
• Received 10 or more rbcs/FWB
• Compare groups:– Did not get platelets or FWB– Received platelets and not FWB– Received FWB
• Findings:
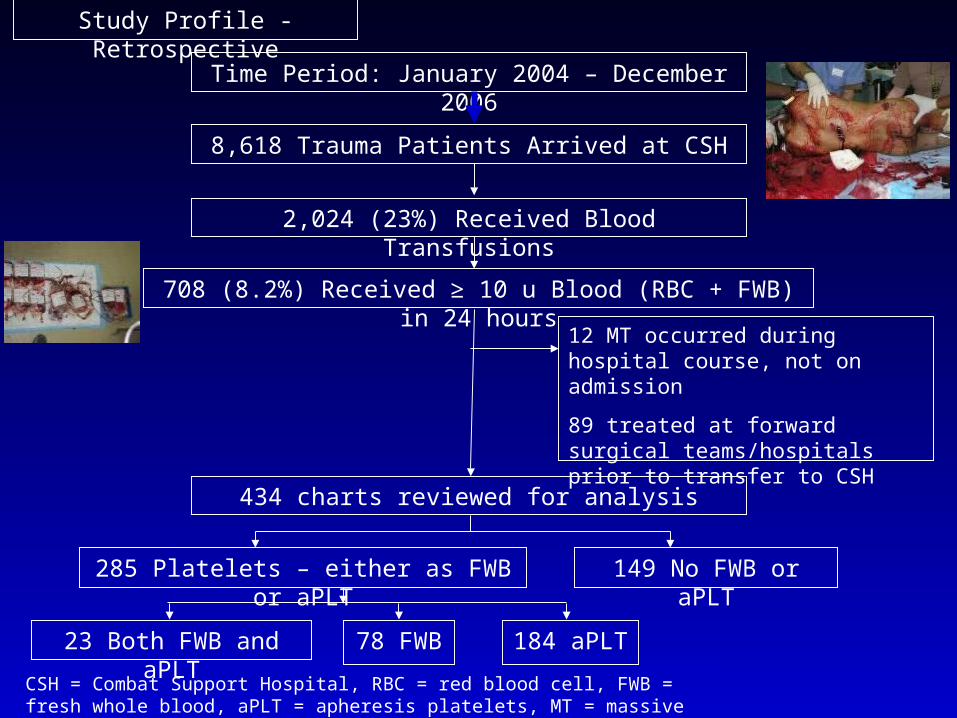
Time Period: January 2004 – December 2006
Study Profile - Retrospective
CSH = Combat Support Hospital, RBC = red blood cell, FWB = fresh whole blood, aPLT = apheresis platelets, MT = massive transfusion
8,618 Trauma Patients Arrived at CSH
2,024 (23%) Received Blood Transfusions
12 MT occurred during hospital course, not on admission
89 treated at forward surgical teams/hospitals prior to transfer to CSH
434 charts reviewed for analysis
708 (8.2%) Received ≥ 10 u Blood (RBC + FWB) in 24 hours
285 Platelets – either as FWB or aPLT 149 No FWB or aPLT
23 Both FWB and aPLT 78 FWB 184 aPLT

UNCLASSIFIED www.milblood.mil ASBPO
48 Hour and 30 Day Survival by Platelet versus No Platelet Groups
0%
20%
40%
60%
80%
100%
48hr 30day
Platelets
No Platelets
Log Rank p=0.003
P<0.001
p=0.04
1 Compared using Chi-square and Mantel-Cox Log Rank
2 Forty-Eight Hour Survival: Platelet Group (218/266, 82 ± 2%), No platelet Group (90/137, 66 ± 3%) p <0.001
3 Thirty Day Survival: Platelet Group 121/196 (62 ± 4%), No Platelet Group (53/107) (50 ± 5%) p-=0.04
UNCLASSIFIED www.milblood.mil ASBPO
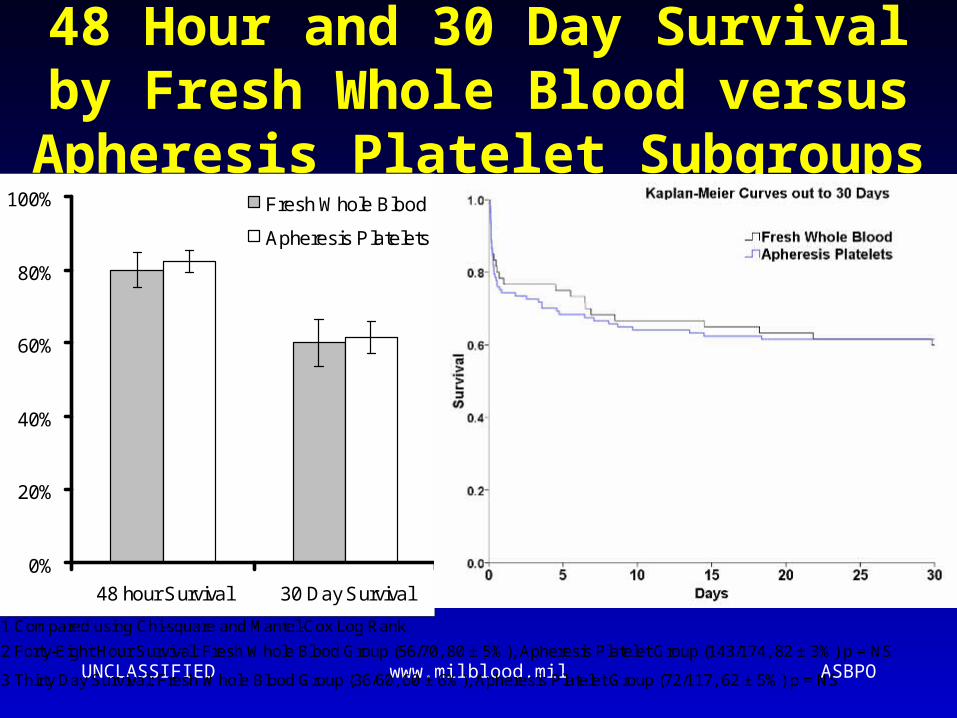
48 Hour and 30 Day Survival by Fresh Whole Blood versus
Apheresis Platelet Subgroups
0%
20%
40%
60%
80%
100%
48 hour Survival 30 Day Survival
Fresh Whole Blood
Apheresis Plateletsp=0.72
p=0.87
Log Rank p=0.96
1 Compared using Chi-square and Mantel-Cox Log Rank
2 Forty-Eight Hour Survival: Fresh Whole Blood Group (56/70, 80 ± 5%), Apheresis Platelet Group (143/174, 82 ± 3%) p = NS
3 Thirty Day Survival: Fresh Whole Blood Group (36/60, 60 ± 6%), Apheresis Platelet Group (72/117, 62 ± 5%) p = NS
UNCLASSIFIED www.milblood.mil ASBPO
1
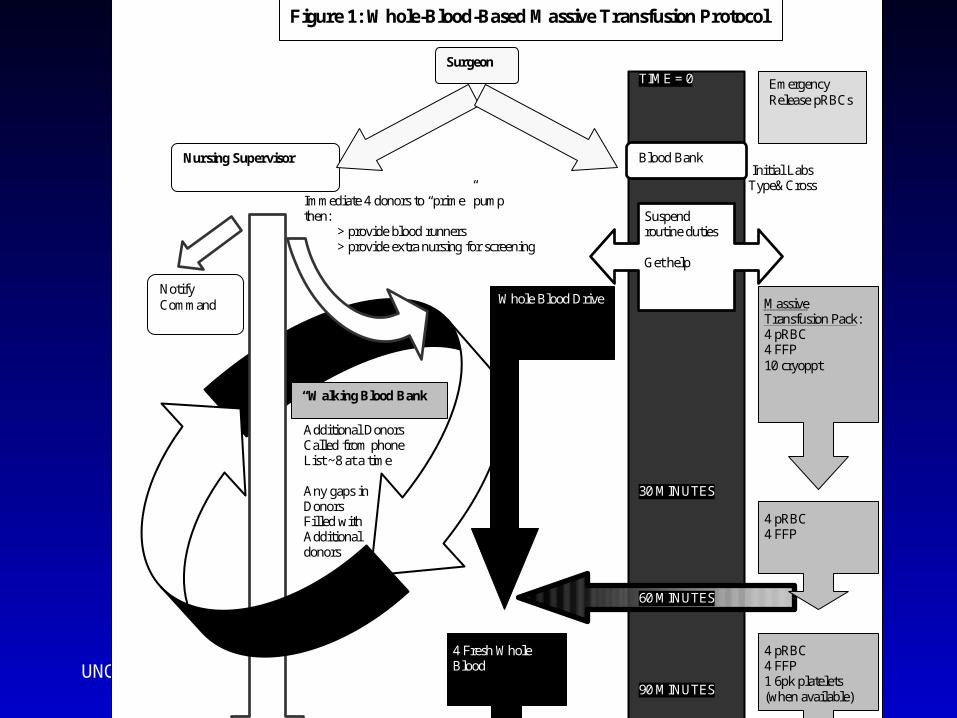
TIME = 0 Initial Labs Type&Cross Immediate 4 donors to “prime” pump
then: > provide blood runners > provide extra nursing for screening
Additional Donors
Called from phone List ~8 at a time Any gaps in 30 MINUTES Donors Filled with Additional donors 60 MINUTES 90 MINUTES 120 MINUTES
4 pRBC 4 FFP
Blood Bank Nursing Supervisor
Surgeon
Notify Command
Suspend routine duties Get help
Whole Blood Drive
Massive Transfusion Pack: 4 pRBC 4 FFP 10 cryoppt
4 pRBC 4 FFP 1 6pk platelets (when available)
4 Fresh Whole Blood
4 pRBC 4 FFP
4 Fresh Whole Blood
“Walking Blood Bank”
Emergency Release pRBCs
PROTOCOL TERMINATED WHEN NO LONGER NEEDED
Figure 1: Whole-Blood-Based Massive Transfusion Protocol
UNCLASSIFIED www.milblood.mil ASBPO
Factor VII Use
• rFVIIa (NovoSeven)– Hemophiliac with anti-VIII (approved for)– Coumadin reversal– Stroke– Massive transfusion

UNCLASSIFIED www.milblood.mil ASBPO
Factor VII Use and Outcome in OIF1 of 2
• Jan04 – Oct05, records for 61 of 117 patients who rec’d FVIIa
• Groups:– Early (FVIIa before 8 units blood)– Late (after 8 units)
• Groups similar for severity of injuries
- Perkins, JG. J Trauma, 2007 May;62(5):1095-9
UNCLASSIFIED www.milblood.mil ASBPO
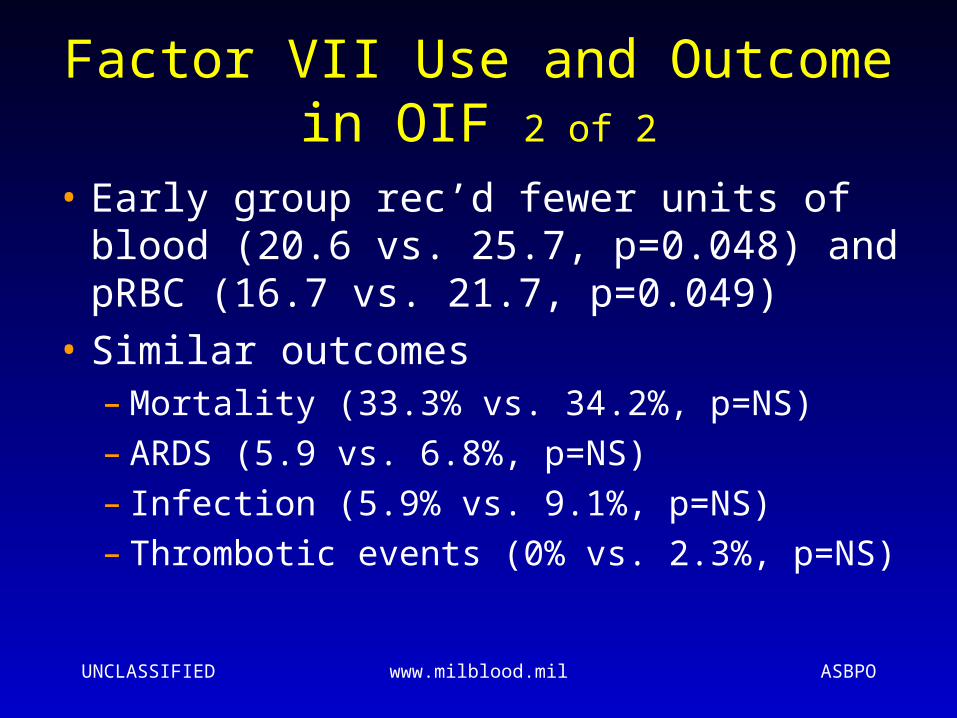
Factor VII Use and Outcome in OIF 2 of 2
• Early group rec’d fewer units of blood (20.6 vs. 25.7, p=0.048) and pRBC (16.7 vs. 21.7, p=0.049)
• Similar outcomes– Mortality (33.3% vs. 34.2%, p=NS)– ARDS (5.9 vs. 6.8%, p=NS)– Infection (5.9% vs. 9.1%, p=NS)– Thrombotic events (0% vs. 2.3%, p=NS)
UNCLASSIFIED www.milblood.mil ASBPO
Conclusions Regarding Blood Therapy in Massive Transfusion
For select patients with coagulopathy (7-8%)• Use of either FWB or aPLT is associated with
improved survival at 48 hrs and 30 days• FWB and aPLT appear equivalent with
regards to survival• FFP:RBC ratios 1:2 to 1:1 are associated
with improved survival at 48 hours, though this survival benefit is not apparent at 30 days.
• FVIIa use might reduce red cell with no appreciable excess adverse outcome
UNCLASSIFIED www.milblood.mil ASBPO
Is Old Blood Bad Blood?
• “Age:” duration of storage
• Storage lesion– Decreased pH– Increased K+– Decreased 2,3-DPG– Decreased deformability
• Clinical outcomes worse? (or not)
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the Evidence
• Retrospective• Inconsistent definition of age• Different preservatives, modifications• Inconsistent findings• Uniform or near uniform
findings/conclusions:– Number of units is associated with worse
outcome– Findings are insufficient to recommend
routine use of “young” units
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the Evidence
Basran Anesth Analg 2006;103:15–20
• Retrospective, 321 re-do CABG pts
• Measures of age: mean; oldest unit
• Findings: correlates with longer LOS, mortality
• Conclusions: should be studied with RCT before informing practice
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the Evidence
Vamvakas Transfusion 1999;39:701-710
• Retrospective, 269 cardiac surgery pts
• Measures of age: mean;
• Findings: age correlates with pneumonia, not with wound infection
• Conclusions: should be studied with RCT before guiding transfusion policy
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the Evidence
Vamvakas Transfusion 2000;40:101-109
• Retrospective, 268 cardiac surgery pts
• Measures of age: mean; oldest; 2 oldest
• Findings: age does not correlate with LOS, time on ventilator
• Conclusions: future studies of transfusion should consider age
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the Evidence
Keller J Trauma 2002;53:1023–1025• Retrospective registry 18 hospitals, 86
trauma pts who rec’d 1-4 units• Measures of age: mean; oldest; 2
oldest; number >7d; >14d; >21d; >28d• Findings: only number of units >14d
correlated with total LOS, not with ICU stay or vent
• Conclusions: further study needed
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the EvidenceLeal-Noval Anesthesiology 2003;98:815-22
• Prospective cohort, 585 cardiac surgery pts• Measures of age: mean; oldest; youngest• Findings:
– age does not correlate with LOS, time on ventilator, MI
– Oldest unit and youngest unit correlates with pneumonia
• Conclusions: age does not increase morbity except maybe pneumonia (number of units)
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the Evidence
Van de Watering Transfusion 2006;46:1712-1718• Retrospective, 2732 cardiac surgery pts• Measures of age: mean; oldest; youngest;
comparisons for patients with all units < 18d vs all units > 18d
• Findings: age correlates with number; no correlation with outcome
• Conclusions: there is no justification for limitation of storage time
UNCLASSIFIED www.milblood.mil ASBPO
Age of Blood: the EvidenceWalsh Crit Care Med 2004; 32(2):364 –371
• Randomized ControlledTrial, 22 critical pts
• Comparison: ≤5d vs ≥20d
• Findings: age has no adverse effect on gastric function or measures of global oxygenation
• Conclusions: no support for the use of fresh red cells in critically ill patients
UNCLASSIFIED www.milblood.mil ASBPO
Summary• Current resucitation emphasizes early control
of bleeding, later correction of injury• Aggressive plasma transfusion is probably
best practice for coagulopathic bleeding patient
• Component therapy better than FWB• FWB as good when component therapy not
available• rFVII may be helpful in reducing red cell use• We will do our patients more good (or at least
less harm) by reducing number of units compared with reducing age of units