united natio ns development fund aids, t mala ria in udan annual report gfatm_tm... · with...
TRANSCRIPT

Globa
UNITE
al Fund
AN
ED NATIO
to Fight
NNU
ONS DE
t AIDS, T
UA
EVELOPM
Sudan
Tubercu
AL R
2012
MENT P
ulosis an
REP
PROGRA
nd Mala
POR
AMME
aria in S
RT
Sudan
UNDP/ GFATM 2012 ANNUAL REPORT Page 2
Table of Contents
Acronyms .................................................................................................................................................. 4
EXECUTIVE SUMMARY............................................................................................................................ 6
Sudan Map ................................................................................................................................................ 8
BACKGROUND AND INTRODUCTION .................................................................................................... 9
Table 1: Overview of GFATM grants in Sudan since 2005. .............................................. 12
Table 2: Overview of the total approved, received funds and expenditures until December 31st 2012 ............................................................................................................................ 13
UNDP/GFATM PROJECTS............................................................................................... 13
1.1 OVERALL GOALS, OBJECTIVES AND ACHIEVEMENTS ......................................................... 13
1.1.1 Scaling up Malaria Interventions in Sudan .......................................................... 13
1.1.2 Scaling up the National Response for prevention and treatment of HIV/AIDS (Round 5) .......................................................................................................................... 15
1.1.3 Intensify the HIV/AIDS national response in Sudan (Round 10) ......................... 15
1.1.4 Single Stream Funding (SSF) – TB and Health Systems Strengthening Programme (SSF-TB/HSS) ............................................................................................... 16
1.1.5 Single Steam of Funding (SSF): Health System Strengthening .......................... 17
1.2 PROJECT MANAGEMENT ........................................................................................................... 19
1.3 PROCUREMENT........................................................................................................................... 20
1.3.1 Details of the construction activities under all grants ............................................................. 20
1.3.2 HIV/AIDS Grant- Construction and rehabilitation of health facilities ...................................... 20
1.3.3 Ensuring and improving drug storage conditions ................................................................... 20
1.3.4 SSF-TB/HSS ................................................................................................................................. 21
1.3.5 SSF-TB/HSS- rehabilitation / construction of the academies of health sciences ................. 22
Table 3: Summary of construction activities for all grants in 2012 .................................... 22
Table 4: Key pharmaceutical and non-pharmaceutical products procured- 2012 ............. 23
1.4 SUPPLY CHAIN MANAGEMENT ................................................................................................. 25
1.4.1 Logistics Management Information System (LMIS) ................................................................. 25
1.4.2 PSM Technical Assistance ......................................................................................................... 25
1.4.3 Central Medical Store .................................................................................................................. 25
1.5 MONITORING AND EVALUATION .............................................................................................. 26
1.6 CHALLENGES, LESSONS LEARNED AND RECOMMENDATIONS ......................................... 28
1.7 FOCUS AREAS FOR 2013 ........................................................................................................... 29
Annex I: Indicators ................................................................................................................................ 32
Annex I.1: Malaria Round 7 Indicators Update- 2012 ........................................................ 32
Annex I.2: Malaria Round 10 Indicators Update- 2012 ...................................................... 33
Annex I.3: HIV/AIDS Round 5 Indicators Update- 2012 .................................................... 34
Annex I.4 HIV Round10 Indicators Update- 2012 ............................................................. 35
Annex I.5 SSF TB/HSS Indicators Update- 2012 .............................................................. 36
UNDP/ GFATM 2012 ANNUAL REPORT Page 3
Annex II: Implementing Partners: ......................................................................................................... 38
Annex II.1: Organizations involved in the Malaria Round 7 grant implementation ............ 38
Annex II.2: Organizations involved in the Malaria Round 7 grant implementation ............ 39
Annex II.3: Organizations involved in the HIV/AIDS Round 5 grant implementation ......... 40
Annex II.4: Organizations involved in the TB/HSS SSF grant implementation .................. 41
Annex II.5: Organizations involved in the TB/HSS SSF grant implementation .................. 42

UNDP/ GFATM 2012 ANNUAL REPORT Page 4
Acronyms
AIDS
ACSM
Acquired Immunodeficiency Syndrome
Advocacy Communication & Social Mobilization
ART Anti Retroviral Therapy
BCC Behavioural Change Communication
CBO Community‐Based Organization
CBS Central Bureau of Statistics
CMS Central Medical Store
CCM Country Coordination Mechanism
CSM Condom Social Marketing
CSOs
DOTs
Civil Society Organizations
Direct Observatory Treatment
FSWs Female Sex Workers
GFATM/GF The Global Fund to fight AIDS, Tuberculosis and Malaria/Global Fund
HBV Hepatitis B Virus
HCP Health Care Provider
HCV Hepatitis C Virus
HIV
HSS
Human Immunodeficiency Virus HSS Health Systems Strengthening
Health System Strengthening
IDPs Internally Displaced Persons
IMAI Integrated Management of Adolescent and Adult Illness
LFA Local Fund Agency
LLIN Long Lasting Insecticidal Nets
MARPs Most At Risk Populations
M&E
MDR
Monitoring and Evaluation
Multiple Drug Resistance
NMCP National Malaria Control Programme
NGO Non Governmental Organization
NTP National Tuberculosis Control Programme
OI Opportunistic Infections
PITC Provider‐Initiated HIV Testing and Counselling
PLHIV People Living with HIV
PMTCT Prevention of Mother To Child Transmission
PR Principal Recipient

UNDP/ GFATM 2012 ANNUAL REPORT Page 5
PSM Procurement and Supply System
RH Reproductive Health
SFPA Sudan Family Planning Association
SGP Safe Guard Policy
SGS Second Generation Surveillance
SNAP Sudan National AIDS Control Programme
SOP Standard Operations procedures
SR Sub‐Recipient
SRCS Sudanese Red Crescent Society
SSF Single Stream Fund
STIs Sexually Transmitted Infections
TBMUs Tuberculosis Management Units
UNDP United Nations Development Programme
UNFPA United Nations Population Fund
UNICEF United Nations Children’s Fund
VCCT Voluntary Confidential Counselling and Testing
VNRBDs Voluntary Non‐Remunerated Blood Donors
WHO World Health Organization
UNDP/ GFATM 2012 ANNUAL REPORT Page 6
EXECUTIVE SUMMARY
This Report provides an overview of Global Fund financed activities implemented in 2012 in Sudan in
collaboration with partners and The Principal Recipient, UNDP. The Report will highlight the general
objectives of all active Grants throughout 2012, the main achievements; as well as the main
challenges faced. The report will also outline both short and longer term interventions that will be
implemented in 2013 and beyond.
Some of the major achievements in 2012 that are highlighted in this report are the following:
During the year, malaria project activities have enabled 2,894,862 cases of uncomplicated and severe
malaria cases to receive anti‐malarial treatment according to National standards and guidelines.
Through the malaria grant, a total of 3,106,115 bed nets were distributed protecting an
approximately 6.2 million people from getting malaria. 2,229 dispensaries in rural and hard‐to‐reach
parts of the country were fully supported to continue providing free Rapid Diagnostic Test for
malaria; while the project has continued supporting the provision of free anti malarial drugs for 4,330
health facilities throughout Sudan.
Through Behaviour Change Communication (BCC) interventions; HIV/AIDs grants reached over
168,000 people, almost 137,335 members of Most‐At‐Risk & vulnerable population (youth in IDPs) as
well as 4,000 young people from out‐of‐school settings. The HIV/AIDS grant reached 4,487 MARPs
(MSM&FSW) through a peer education approach. Counselling and testing services were also provided
to 60,036 people including pregnant women and MARPs.
More than 85,000 people have received HIV testing and counseling services; reaching 5,500 people
with advanced HIV infection to receive ARV combination therapy. During the year, 2,574 people were
retained on ARV treatment. A total of 2,032 TB patients have begun ARV treatment during or at the
end of their TB treatment. 79 pregnant women have also received ARV treatment as part of the
overall intervention to reduce the risk of mother to child transmission of HIV. In 2012, sseveral
capacity development interventions were held to PLHIV associations, other CSOs and SNAP. About
151 health care providers were trained on syndromic management of STIs according to the national
guideline, while 59 health care providers received training on Infection prevention in health care
settings.
With regard to Tuberculosis project, the grant has enabled the detection of 6,518 new smear positive
TB cases; with 70.6% of new smear positive cases being successfully treated. In 2012, a concerted
effort was made that enabled the detection and treatment of 254 MDR TB cases. As part of TB/HIV
collaborative activity a total of 190,589 condoms were distributed to TB patients. A total of 2, 827
people were trained on TB management, contact tracing and management, PPM, DOTS links and

UNDP/ GFATM 2012 ANNUAL REPORT Page 7
health communication skills in 2012. In an effort to expand TB services in Darfur states, 27 TBMUs &
54 DOTs were newly established during the year.
As part of the cross‐cutting health system strengthening effort, site assessment and design work for
rehabilitation of the Academies of health Sciences was finalized and rehabilitation and construction
initiated. 14 Academies of Health Sciences in 14 states were provided with minibuses to facilitate
their daily work and commute students to and from their practice health facilities and the Academies.
Equipment to upgrade 5 rural hospitals, 25 health centers, 15 laboratories & 5 Academies were
procured & handed over to MOH. A total of 293 health management personnel from 114 localities
were trained in decision‐making, teamwork, effective meetings, and health planning and district
health management. The capacity of Locality Health Management Teams is enhanced by the
provision of vehicles, office equipments and computers. 25 personnel from States and Federal level
were trained on M&E of the health system. 42 health managers from states and localities were also
trained in health economics/financing. 5 fellowships in health economics & health care management
were awarded in collaboration with the National Health Insurance Fund & the University of
Chulalongkorn, Bangkok, Thailand. 20 health managers from states & localities were enrolled in
health economics/financing in‐country for a medium term course.
At the end of the report, main challenges and future plans are listed. Several annexes are also
provided showing details of performances for specific indicators related to the respective projects. AS
can be seen from this report, it is clear that within the various challenges faced, the UNDP/ GFATM
projects did manage to reach and achieve the majority of the targets it had set from the beginning
and will continue to deliver more with a aim of saving lives, enhancing better health and
strengthening the health system to sustainably mitigate the impacts of the three diseases.

UNDP/ GFATM 2012 ANNUAL REPORT Page 8
Sudan Map
Health Service Provision points supported by UNDP/ GFATM for the three diseases throughout the
country: (Needed here)

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 9
BACKGROUND AND INTRODUCTION
With an annual growth rate of 2.8%, the total population of Sudan as projected from 2008 census is equal to
34.1 million for 2012, 88% are settled, including 32.7% in urban areas, while 8% are nomads. Almost 6.9% of
the population is internally displaced. There has been increasing urbanization, with natural disasters, civil
conflicts and poor conditions in rural areas, contributing to this.
Sudan comprises 17 States each divided into localities, which in total are 1841 but varies with time due to
redrawing of the boundaries of the existing ones.
The epidemiological profile of Sudan is typical of other Sub‐Saharan African Countries, dominated by
malnutrition and communicable diseases, frequently aggravated by natural disasters (floods, heavy rains and
droughts) as well as sustained internal conflicts. The main causes of morbidity and mortality are infectious
and parasitic diseases, particularly malaria, tuberculosis, schistosomiasis, diarrheal diseases, acute respiratory
infections and protein‐energy malnutrition.
With changes in socio‐economic and lifestyle conditions, non communicable diseases (NCDs) are now
emerging as a public health problem in Sudan. Hypertension, diabetes, heart disease, cancer, asthma,
cataract and mental disorders are the major ones prioritized in the 2011‐2016 National Health Sector
Strategy.
Sudan made progresses towards the Millennium Development Goals (MDGs) with a reduction in child
mortality by a third between 1990 and 2010, and reduction in the maternal mortality rate by 60%. However
recent trends suggest that Sudan is unlikely to reach the MDG targets for child and maternal health by 2015.
Another feature is the marked disparity between states in health status, for example, the infant mortality rate
is 60 overall but ranges from 39 per 1,000 in Gezira state to 85 per 1,000 in Red Sea state2. The range is even
wider for maternal mortality rates, ranging from 106 per 100,000 in Northern to 335 per 100,000 in South
Darfur. These indicators demonstrate considerable inequity in health status across the country.
The health service delivery system in Sudan includes a range of public providers and both not for profit and
for profit private sector providers. The National (Federal) Ministry of Health (FMOH) has a leading role in
policy and stewardship while responsibility for delivery of public services is largely led by states and their
localities and by other agencies including police and army health services and the National Health Insurance
Fund (NHIF). In areas affected by conflict, Non‐Governmental Organization (NGOs) have been playing a
substantial role in service delivery. This has resulted in an uncoordinated patchwork of services, with gaps in
1 FMOH. Mapping of PHC services in Sudan 2010 2 Data from Sudan Household Health Survey 2010 (SHHS).

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 10
some states and duplication in others. The high proportion of public funding and qualified health workers
allocated to public hospitals and substantial costs of administration leaves less than 20% of public funds
allocated to primary health care (PHC) services and public health programmes.
PHC services include community level, small family health units, larger family health centres and rural/locality
hospitals, which report to the locality administration. Public health services (environmental, food safety,
campaigns) are managed from the locality level as well. The distribution of PHC facilities is uneven across the
country. The ratio of PHC facilities to population varies from 1:3,000 people in the Northern State to 1:21,000
people in South Darfur, compared to the planned 1:5,000 population. In six states over 20% of the population
lives more than 5 km from a health facility (HF) (five Darfur states and Red Sea). PHC services are variable,
with only 24% of facilities offering services in all the main components of the PHC package (reproductive
health, immunization, nutrition, prevention and treatment of common diseases and essential drugs).
Analysis of health system financing indicates that 65% of funding is from private sources, almost all out of
pocket expenditure. Reliance on out of pocket spending for health care exposes individuals to financial risk
and is likely to reduce access for the poor. Public funding has risen considerably in recent years and reached
9.8% of public expenditure in 2011. The allocation of public funding is very uneven across states once
population is taken into account, ranging from below 10 SDG per person in South Darfur to almost 40 SDG per
person in Red Sea state in 2008. The NHIF and other health insurance schemes (mainly for public sector staff)
fund some 7% of all health spending while coverage of health insurance is around 37% of the population; this
indicates that NHIF is only providing limited cover for the costs of health care. In addition payments are on a
fee for service basis which does not encourage efficiency and cost control.
Health information in Sudan is primarily based on health facility reporting supplemented by surveys. The
MOH hospitals generally report regularly but there are gaps in reporting from PHC facilities in many states
and low coverage of other sectors including private providers. There are multiple systems and forms for data
collection for different programmes. Data quality assurance is limited and systems for data management and
analysis are largely manual. Annual statistical reports are produced at national and state levels but there is
limited use of data at sub‐national levels.
Human Resources for Health (HRH) are a critical component of service delivery. Issues facing Sudan include
the relatively high number of medical doctors relative to nurses, midwives and paramedics, and the tendency
of doctors to emigrate for better conditions or to work in urban areas and referral hospitals, leaving PHC and
rural hospitals understaffed. States have established Academies of Health Sciences to redress this imbalance
in the skill mix and further efforts are required to improve the distribution of health workers and to maintain
their professional development. Community midwives have played an important role in Sudan in reaching

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 11
remote populations and more recently programmes have established specialized community workers such as
for malaria.
Basic equipment and services are not available in a significant proportion of health facilities especially in
poorer rural states. Medicines are a major share of the health expenditure by individuals (some 40%) and use
of antibiotics is very high, at over 70% of prescribed medicines, which suggests serious over‐use of these
medicines. There is a single supply agency for the public sector but in practice there are multiple procurement
and supply arrangements, including more than 15 different systems in the Federal MOH linked to different
programmes.
To help the country join the global fight against HIV/AIDS, TB and malaria, UNDP’s role is two‐fold: it manages
all funds allocated by the Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria (GFATM) in Sudan; as well
as implementing interventions that address these diseases as they affect development, governance, the
protection of human rights and gender equality.
Since 2005, the Country Coordinating Mechanism (CCM) in Sudan3 nominated UNDP as the Principal Recipient
(PR) for the implementation of the GFATM supported grants4. As the Principal Recipient for 8 grants (2005‐
2016) amounting to more than USD 400 million, UNDP is managing the largest fund portfolio in the Middle
East and North Africa Region. UNDP‘s management role consists of implementing grants, ensuring financial
accountability, and training of a variety of national and international counterparts on programme
management and financial accountability. The established GFATM Programme Management Unit, which falls
within UNDP’s MDG and Poverty Reduction Unit, is responsible for the programmatic and financial
management of the grants, the procurement of HIV/AIDS, malaria and TB‐related commodities and capacity
development of the national partners: Sudan National AIDS Programme (SNAP), National Malaria Control
Programme (NMCP), National TB Programme (NTP), Directorate General of International Health and Planning
(DGIHP) and national NGOs. To ensure the proper management and execution of grants, the Global Fund
Programme Management Unit is organized into eight sections‐ four managing the specific grants, a
Monitoring and Evaluation, Finance, Procurement and Supply Chain Management sections.
3 There were two CCMs overseeing GF grants implementation in North and South Sudan before the cessation of the South.
4 SUD-305-GO4-H, SUD-506-G08-H, SUD-506-G07-T, SUD-202-G03-M, SUD-708-G10-M, SUD-T-UNDP

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 12
Table 1: Overview of GFATM grants in Sudan since 2005
Grant Name Project Title Grant Period Budget in USD
Round 2 Malaria Malaria Prevention and Control Apr 1St 2005‐ Sep 30th 2009
33,240,453
Round 3 HIV/AIDS Sudan Proposal for fighting HIV/AIDS Apr 1st 2005‐ Sep 30th 2010
20,682,531
Round 5 Tuberculosis Comprehensiveness and Quality of DOTs in Sudan Jan 1st 2007‐ Dec 31st 2011
11,684,917
Round 5 HIV/AIDS Scaling up the National Response for prevention and treatment of HIV/AIDS in Sudan
Jan 1st 2007‐ Dec 31st 2011
84,976,035
Round 7 Malaria Scaling‐up Malaria Interventions in Northern Sudan Apr 1st 2009‐ Mar 31st 2014
77,156,461
Round 8 Tuberculosis Addressing TB control in war‐affected, post conflict areas and other challenges
Jan 1st 2010‐ Jun 30th 2010
3,171,523
Round 8 HSS Addressing TB control in war‐affected, post conflict areas and other challenges
Jan 1st 2010‐ Jun 30th 2010
714,791
SSF TB/HSS Comprehensiveness and quality of DOTs in Sudan Addressing TB control in war‐affected, post conflict areas and other challenges
Jul 1st 2010‐ Feb 28th 2015 45,267,705
HIV R10 To intensify the HIV/AIDS national response in Sudan Mar 1st 2011‐ Feb 28th 2013
19,180,279
Malaria R10 Scaling up for Universal Coverage with Community Participation
Mar 1st 2011‐ Feb 28th 2013
53,673,711
Total 349,748,406

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 13
Table 2: Overview of the total approved, received funds and expenditures until December 31st 2012
Grant Name Approved Received Expenditures Balance
Round 2 Malaria Phase 1 14,237,853 14,237,853 13,156,250
Phase 2 19,002,600 18,840,189 19,206,292 715,500
Round 3 HIV/AIDS Phase 1 7,842,140 7,842,140 7,181,565
Phase 2 12,840,391 12,185,910 11,749,546 1,096,939
Round 5 Tuberculosis
Phase 1&2 11,684,917 11,684,917 11,684,917 0
Round 5 HIV/AIDS Phase 1 29,421,145 29,421,145 18,372,150
Phase 2 55,554,890 44,017,230 49,184,423 5,881,801
Round 7 Malaria Phase 1 28,503,242 35,373,169 25,027,861 10,345,308
Round 7 Malaria Phase 2 48,653,219 26,012,413 21,080,039 15,277,682
Round 8 Tuberculosis Phase 1 7,207,041 3,171,523 3,171,523 0
Round 8 HSS Phase 1 8,292,492 714,791 714,791 0
SSF TB/HSS Phase 1 19,851,519 20,129,456 15,587,385 4,542,071
SSF TB/HSS Phase 2 25,416,186 0 0 0
HIV R10 Phase 1 19,180,279 4,338,391 2,524,573 1,813,818
Malaria R10 Phase 1 53,673,711 27,353,645 19,813,874 9,568,860
Totals 361,361,625 255,322,772 216,426,101 38,896,670
UNDP/GFATM PROJECTS
1.1 OVERALL GOALS, OBJECTIVES AND ACHIEVEMENTS
Malaria
1.1.1 Scaling up Malaria Interventions in
Sudan
The overall goal of the Scaling‐up Malaria Interventions
(SMI) in Northern Sudan Project (Round 7 grant) which
started in April 2009, is to continue and expand disease
management activities implemented under the
previously closed project on Malaria Prevention and
Control (Round 2); which included home based
management of malaria, improvement of clinical and
Figure 1: The Launch of the 8th campaign for Bed Netdistribution. This picture is from Blue Nile State, Damazin locality. The State Governor, State Minister of Health , Undersecretary Federal Ministry of Health, Locality Governor and UNDP Project Officer handing over bed nets to mothers. Project supported by the GF, UNDP and UNICEF
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 14
laboratory diagnosis, ensuring availability and rational use of anti‐malarial drugs, establishing a Malaria Early
Warning System (MEWS) to ensure a rapid response to malaria outbreaks.
The other aspects of malaria case management in this project are a gradual shift from clinical, symptomatic ,
treatment to test‐based treatment by introducing the
use of rapid diagnosis test kits, preventing malaria
during pregnancy through the distribution of bed nets
and capacity building of national institutions. Another
objective of this project is to unify and standardize
interventions by all NGOs working in the field of
malaria control in Sudan in line with the national
framework. The Round 10 Malaria, as new grant that
started in March 2012, intends to scale‐up and reach
universal coverage with community participation by
bridging the gaps observed in Round 7 as well as the
introduction of IRS (in‐door Residual Spraying) for
vector control for locations with an in intensive irrigation schemes; mainly Gezira and Sennar states. In
addition, the grant is aimed at strengthening the organizational capacity of national counterpart and provides
support for Malaria Program Review.
Main Achievements in 2012
2, 894, 862 cases of uncomplicated and severe malaria cases received anti‐malarial treatment according
to National guidelines.
3, 106, 115 bed nets were distributed to protect approximately 6,212,890 people from malaria.
4, 330 health facilities were supported to continue the provision of free anti‐malarial drugs throughout
2012.
2, 229 dispensaries in rural and hard‐to‐reach parts of the country were fully supported to continue
providing free Rapid Diagnostic Test for malaria.
Figure 2: Blue Nile State: Children demonstrating bed net use to members of their community – Project supported by GF, UNDP and UNICEF
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 15
HIV/AIDS
1.1.2 Scaling up the National Response for prevention and treatment of HIV/AIDS (Round 5)
The overall goal of the Scaling up of the National Response for prevention and treatment of HIV/ AIDs project
(Round 5 grant) is to contribute to reduce HIV transmission and HIV mortality in Sudan. The project aims to
increase awareness of HIV/AIDS and other STDs further enhancing and reducing risk behaviours; and to
ensure availability and utilization of quality VCCT services in all states; increase access to condoms through
free distribution, social marketing and other outlets in target communities. In addition, the project targets
that more than eighty percent of blood transfused in government hospitals is from non‐remunerated
voluntary donors. The project has also a major component for care and support services to PLWHAs.
Main Achievements in 2012
HIV R5 Main Achievements
The project reached over 168,000 people from the general population through community outreach
Behavior change communication (BCC) interventions.
BCC interventions provided to 137,335 for members of Most at Risk Populations (MARPs) and
vulnerable population (youth in IDPs).
BCC interventions reached more than 4, 000 young people from out‐of‐school settings.
More than 85,000 people have completed HIV testing and counseling process.
About 5,500 people with advanced HIV infection are receiving ARV combination therapy.
2,032 TB patients have begun ART during or at the end of their TB treatment.
1.1.3 Intensify the HIV/AIDS national response in Sudan (Round 10)
The characteristics of the HIV epidemic in Sudan mirror that prevailing in the Middle East and North Africa
(MENA) region. HIV infection is concentrated among high‐risk populations with vulnerable populations being
the bridge of HIV transmission into the general population.
It is with in this context that the Round 10 HIV project, which is launched in 2012, aims to to reduce HIV
transmission and to reduce HIV morbidity and mortality in Sudan.
Objectives
1. To reduce HIV transmission through the provision of services for MARPs.
2. To improve access and utilization of PMTCT services in Northern Sudan.
3. To improve quality and uptake of existing care and treatment services in Northern Sudan.
4. To strengthen HIV prevention in health care settings in Northern Sudan.
5. To improve planning, management and monitoring of the HIV/AIDS response

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 16
Cross‐cutting Issues:
‐ TB/HIV is another cross‐cutting issue that is targeted in this project with training voluntary
counselling and testing for TB patients as well as condom distribution.
‐ The project is targeting the 17 states with focus on war affected areas and conflict zones with
activities and capacity building in the form of refurbishment of localities warehouses as well as
upgrading of locality staff capacity in planning and communication.
‐ Income generation activities target Most‐at‐risk populations (MARPs) to empower sex workers with
life skills, information and support needed to make informed decisions on their current and future life
and to abandon sex work or to reduce their risky behaviour. Study conducted in 2008 in Khartoum
state among FSWs showed that, 80.2% were selling sex due to economical reason, and more than
21% do not use condom because their partners refuse.
Round 10 HIV: Main Achievements in 2012
Reached 4,487 MARPs (MSM&FSW) through peer education.
Provided counselling and testing services to 60,036 people including pregnant women and
MARPS.
79 pregnant women received ARVs to reduce the risk of mother to child transmission of HIV.
Trained 151 health care providers on syndromic management of STI according to the national
guideline and 59 health care providers trained on Infection prevention in health care settings.
Retained 2,574 people on ARV treatment.
Tuberculosis and Health System Strengthening
1.1.4 Single Stream Funding (SSF) – TB and Health Systems Strengthening Programme (SSF‐
TB/HSS)
The overall goal of the TB component of this project is to drastically reduce the TB burden in Sudan,
particularly among poor and vulnerable populations in line with the 2015 MDGs and the Stop TB Partnership
targets. The project aims to decrease the burden of TB through reducing mortality, morbidity and
transmission of the disease until the disease no longer poses a threat to public health in Sudan. It also aims to
reduce human suffering and the social and economic burden which families and communities have to bear as
a consequence. The project aims to scale up and strengthen quality DOTs including creating access to war‐
affected and post conflict regions; strengthen partnership including PPM and engagement of health care
providers; prevent and control MDR‐TB, and address TB contact management; as well as raise awareness and
participation of communities and politicians, including the creation of positive perceptions toward TB

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 17
prevention, treatment efficacy and adherence, in addition to reducing stigmatizing attitudes the burden of
TB/HIV in Patients and PLWHA.
1.1.5 Single Steam of Funding (SSF): Health System Strengthening
The goal of the Health System Strengthening component of the SSF grant is to contribute to improving the
performance of National health system for a better response to the
three diseases to achieve MDGs, including MDG‐6 for AIDS TB and
Malaria. This cross cutting project aims to improve health services
delivery including laboratory services, assuring quality and equity of
access at all levels of health care; strengthen health management
information system, including surveillance and setting up a M&E
system for measuring the health system’s performance; strengthen the
procurement and management system for drugs, supplies and
equipment, including quality assurance; as well as quantitatively and
qualitatively scale up the availability of Human Resources for Health at
different levels of
health care; and
finally strengthen
health financing
function of health
system for assuring
equity and access to
health service.
Main Achievements in 2012
Tuberculosis
• TB treatment was provided to 19,831 TB cases.
• The project detected 6, 518 new smear positive TB cases.
• 70.6% of reported new smear positive TB cases were successfully treated.
• 254 TB cases were diagnosed as MDR‐TB cases and placed on treatment.
• 190,589 condoms were distributed to TB patients.
• 2, 827 people were trained on TB management, contact tracing and management, PPM, DOTS links and
health communication skills.
Figure 5: Mini‐buses delivered to Academy of Health Sciences to commute Students to and from hospitals/ Field appernteship to their Academies
Figure 4: Upgrading Rural Hospitals, Primary Health Care centers & Laboratories by equipping & furnishing
Figure 3: Vehicles: to enhance the capacity of Locality Health Management Teams, as part of the overall HSS programme.

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 18
• 27 TBMUs were newly established in Darfur states.
• 54 DOTs were newly established in Darfur states.
Health System Strengthening (HSS)
• A health system strengthening project implementation mechanism was created within the Ministry of
Health and the CCM, including establishing a HSS sub‐CCM committee
• Site assessment and design work for rehabilitation of the Academies of health Sciences finalized; and
civil work is on‐going to be realized by June 2013.
• 14 Academies of Health Sciences in 14 states were provided with minibuses to facilitate their daily work
and commute students between health facilities, the academies and communities.
• Equipments to upgrade five rural hospitals, 25 health centers, 15 laboratories & five health academies
were procured & handed over to MOH.
• 293 health management personnel from 114 localities trained in decision‐making, teamwork, effective
meetings, and health planning and district health management
• The capacity of Locality Health Management teams enhanced by the provision of vehicles, office
equipments and computers.
• 25 participants from states and federal level trained on M&E of the health system; out of which 5 staff
was nominated to participate in external advance training on M&E will be conducted in Liverpool
University.
• 42 health managers from states and localities trained in health economics/financing.
• A framework for community based health insurance (CNHI) has been designed.
• Five fellowships in health economics & health care management were awarded in collaboration with the
National Health Insurance Fund & University of Chulalongkorn, Bangkok, Thailand.
• 20 health managers from states & localities were enrolled in health economics/financing 4 week in
country short course in collaboration with the National Health Insurance Fund & University of
Chulalongkorn, Bangkok, Thailand.
• A new implementation strategy was developed in light of the changes in the implementation
arrangement for phase II.

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 19
1.2 PROJECT MANAGEMENT
UNDP as Principal Recipient of the GFATM grants has the primary role in ensuring that the implemented
activities, undertaken by sub recipients (SRs), contribute to the national response against HIV, TB and malaria.
At the state and locality level the implementation is carried out by SNAP, NTP and NMCP states’ coordinators.
WHO, UNFPA, UNICEF, UNAIDS and UNHCR are the major Sub‐Recipients responsible for the management
and provision of technical support in areas of treatment, prevention and awareness raising activities for the
various projects, while the UNDP as the Principal Recipient oversees the management and implementation,
including the release of funds and tracking of their use. To ensure the proper management and execution of
grants, the Global Fund Programme Management Unit is divided into eight sections‐ four sections managing
the specific grants (HIV, Malaria, TB and HSS), a Monitoring and Evaluation, Finance, Procurement and Supply
Chain Management sections. The PMU adopted a standard operating procedure for efficient and proper
implementation of all GFATM grants. UNDP’s standard project management framework and internal controls
govern the project execution. The project is also staffed with the relevant programme, Finance, procurement
and other support personnel. In addition, all grants undergo the regular and periodic review and assessment
by the Local Funding Agent (LFA) which is contracted by the Global Fund. UNDP has also annual audits
undertaken by the Office of Audit and Investigations.
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 20
1.3 PROCUREMENT
1.3.1 Details of the construction activities under all grants
Delivering adequate health services in Sudan was severely affected by prolonged conflicts and instability in
the country. UNDP, through the Global Fund support and in‐collaboration with local partners, has taken the
lead in health system strengthening initiatives which include rehabilitation and renovation of health
infrastructure; as well as capacity building and
improving the skills of health personnel.
As part of advance procurement planning, a
Request for Proposal for the Provision of Services
for Rehabilitation/Construction Works in Sudan was
launched at the end of 2011 for pre‐qualified
national and International Engineering and
Consulting Firms to engage them under Long Term
Agreement (LTA) for one year to participate in the
civil works as per the 2012 PSM Plans. Accordingly,
a Long Term Agreement was signed with consulting firms in April 2012.
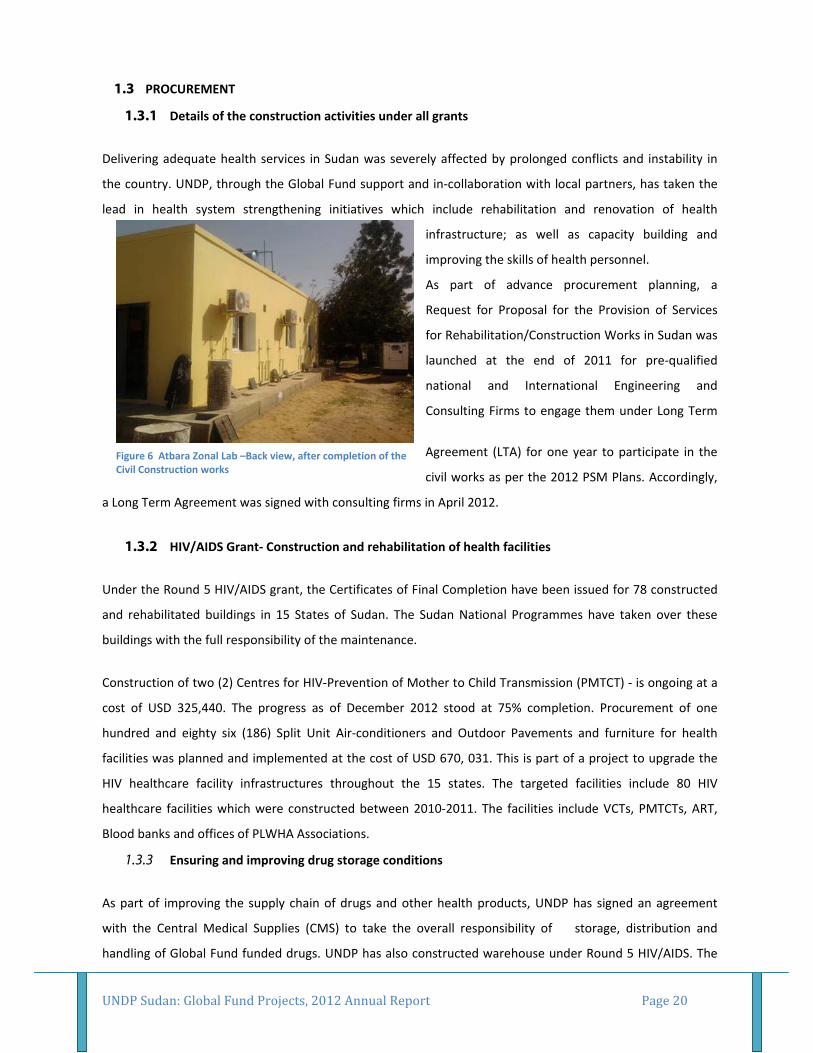
1.3.2 HIV/AIDS Grant‐ Construction and rehabilitation of health facilities
Under the Round 5 HIV/AIDS grant, the Certificates of Final Completion have been issued for 78 constructed
and rehabilitated buildings in 15 States of Sudan. The Sudan National Programmes have taken over these
buildings with the full responsibility of the maintenance.
Construction of two (2) Centres for HIV‐Prevention of Mother to Child Transmission (PMTCT) ‐ is ongoing at a
cost of USD 325,440. The progress as of December 2012 stood at 75% completion. Procurement of one
hundred and eighty six (186) Split Unit Air‐conditioners and Outdoor Pavements and furniture for health
facilities was planned and implemented at the cost of USD 670, 031. This is part of a project to upgrade the
HIV healthcare facility infrastructures throughout the 15 states. The targeted facilities include 80 HIV
healthcare facilities which were constructed between 2010‐2011. The facilities include VCTs, PMTCTs, ART,
Blood banks and offices of PLWHA Associations.
1.3.3 Ensuring and improving drug storage conditions
As part of improving the supply chain of drugs and other health products, UNDP has signed an agreement
with the Central Medical Supplies (CMS) to take the overall responsibility of storage, distribution and
handling of Global Fund funded drugs. UNDP has also constructed warehouse under Round 5 HIV/AIDS. The
Figure 6 Atbara Zonal Lab –Back view, after completion of the Civil Construction works

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 21
procurement of Storage Racks, application of Epoxy flooring, installation of Central Air‐Conditioning System,
Construction of internal partitioning, reconstruction of fences, and building of security rooms planned and
initiated at a cost of USD 448,850. Epoxy flooring work for this central warehouse was completed in
December 2012; with the remaining activities to be completed by March of 2013.
In addition, seven (7) Diesel Generators of 80 KVA capacity were procured for States and Regional
Warehouses at a cost of USD 167,996.
Under the Round 7 Malaria grant, three Diesel Generators were procured for Malaria Institutes in Sinar,
Khartoum and Gazeera States at a cost of USD 179,666
As part of refurbishing medical stores in different States, the remaining 4 locality medical stores –out of 107‐
in South Darfur States are supplied with shelving/racking systems. Diesel generators for 4 locality medical
stores in South Kordofan are stored in Central Medical Supplies (CMS) Warehouse in Khartoum due to the
current volatile security situation in the area.
1.3.4 SSF‐TB/HSS
Following a gap analysis done in 2011, refurbishment was planned under the SSF‐TB/HSS grant to
strengthening of Tuberculosis Management Units (TBMUs) in post conflict areas including the rehabilitation
of 18 TBMUs, 45 TBMU Laboratories and 54 DOTs centres, with an estimated budget of USD 519,000.
The improvement of infrastructure of the 18 TBMUs and 54 DOTS centres was achieved as per the approved
plan for phase 1, by supplying and installing basic office furniture with a total cost of USD 32,130. All targeted
facilities were successfully reached apart from 10 locations in Darfur where the supply and installation is
expected to be completed by March 2013
Rehabilitation works for the National Reference Laboratory in Khartoum are completed at the cost of USD
154,522. The certificate of substantial completion was issued on August 2012 and the site was handed over to
the National Programme. In addition, the National Reference Laboratory in Khartoum is supplied with
150KVA Diesel Generator at the cost of USD 33,860.69.
Three (3) Zonal Laboratories are being rehabilitated at the cost of USD 126,627 and will be handed over to
National Programme by mid of March 2013.
To improve quality of TB services and to reduce MDR TB cases, construction of two TB MDR patient wards in
Khartoum is held at the cost of USD 123,907. The construction work commenced in December 2012.

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 22
The rehabilitation of another seven (7) Tuberculosis Quality Control laboratories and two (2) Zonal
Laboratories is planned at the cost of USD 311,533; the rehabilitation is expected to commence by March
2013.
As part of upgrading the health facility infrastructures, five (5) Diesel Generators of 20 KVA capacity were
procured for the TB Zonal Laboratories at the cost of USD 92,772.
1.3.5 SSF‐TB/HSS‐ rehabilitation / construction of the academies of health sciences
Following an assessment to verify the rehabilitation requirements for selected academies of health sciences,
the plan for rehabilitation and construction of five (5) Academies of Health Sciences (AHSs) has been
approved by the global fund with an estimated cost of USD720, 000.
Construction/ Rehabilitation of the AHSs is intended to improve the availability of Human Resources for
Health at different levels of health care both quantitatively and qualitatively. Construction/ Rehabilitation of
the five AHSs are being held at the cost of USD 650,000. The construction work has started since December
2012, with a planned completion by June 2013.
Table 3: Summary of construction activities for all grants in 2012
Description of Procurement
Grant/
source of
funding
Value (USD)
Rehabilitation of the National TB Reference
Laboratory TB 154,522
Construction of Two PMTCT Centres and
Rehabilitation of Three (3) Zonal Labs HIV & TB 452,067
Procurement of (186) Split Units for HIV
healthcare facilities in Different States in Sudan HIV 146,125
Procurement of Outdoor Pavements for HIV
healthcare facilities in Different States in Sudan HIV 148,206
Procurement of Diesel Generators for (7) States
Regional Warehouses, National TB Reference lab,
(5) TB States Zonal Laboratories and (3) Malaria
Institutes
TB & Malaria 474,295
Procurement of Storage Racks, application of
Epoxy flooring, installation of Central Air‐
Conditioning System, Construction of internal
Malaria 448,850

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 23
partitioning, re constructing the fence, and build
security room
Procurement of 3 stand by Diesel Generators for
Public Health Institute , Blue Nile National
Institute for Communicable Diseases and Algadal
Malaria Training Institute in Sennar
Malaria 160,000
Construction of two TB MDR patient wards in
Khartoum TB 123,907
Construction/ Rehabilitation of (5) Academies Of
Health Sciences HSS 650,000
Rehabilitation Works for 7 Tuberculosis Quality
Control laboratories and 2 Zonal Laboratories in
Different States in Sudan
TB 311,533
Table 4: Key pharmaceutical and non‐pharmaceutical products procured‐ 2012
Grant Name Description of Procurement Value (USD)
SSF‐TB/HSS IT Equipment 41,223
Round 7 Malaria Malaria Health Equipment (Lab) 215,233
Round 10 Malaria Anti Malarial Drugs ( ACTs) ‐Malaria 518,880
Round 7 Malaria Anti Malarial Drugs ( ACTs) ‐Malaria 4,365,492
Round 5 HIV/AIDS HIV/AIDS ARVs 757,638
Round 5 HIV/AIDS HIV/ AIDS drugs 128,673
Round 5 HIV/AIDS HIV/ AIDS Test Kits 121,814.40
Round 5 HIV/AIDS HIV/ AIDS Lab. Equipment 437,551.22
SSF‐TB/HSS Laboratory Equipment 896,792
SSF‐TB/HSS Hospital Equipment 935,714.42
SSF‐TB Second line Drugs 516,412
SSF‐TB First line Drugs 1,343,685
Round 10 Malaria RDT’s 632,520
Round 10 Malaria IRS+ Accessories 3,398,564
Round 10 Malaria Sprayers 395,370
Round 5 HIV/AIDS Furniture 218,661.15
SSF‐HSS Furniture 258,256

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 24
SSF‐HSS Skill lab 34,058
HIV/AIDS R5 Vehicles 103,996
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 25
1.4 SUPPLY CHAIN MANAGEMENT
During 2011, UNDP/ GFATM, in close collaboration with partners, developed a strategic roadmap to
strengthen the supply chain management system and identified key interventions for establishing a viable
and agile supply chain system in the country. This project supports the national programmes in establishing a
responsive and sustainable supply system capable of delivering appropriate, sufficient quality health
commodities to the right places at the appropriate time and free of charge. Below are the key interventions in
2012.
1.4.1 Logistics Management Information System (LMIS)
UNDP/GFATM is supporting mechanisms aimed at providing reliable logistics data captured through a
functioning LMIS in health facilities and transferred effectively and efficiently along the nationwide supply
chain up to the CMS, national programs and UNDP. The reports to be delivered through the LMIS include
National Physical Inventory reports, Stock Status reports, HIV/AIDS TB and Malaria commodities consumption
reports, Patients per regimen reports and Expiry Risk Analysis reports.
1.4.2 PSM Technical Assistance
UNDP/GFATM contracted Axios Foundation as the PSM technical assistance provider to strengthen the
national supply chains for HIV/AIDS, TB and Malaria programmes in Sudan; as well as assess the current
logistic system. The foundation is to document the system’s strengths and weaknesses, as well as support the
availability of an agile supply chain system.
Axios Foundation had completed the first year work plan as per the agreement. Major deliverables include
the PSM system assessment, PSM system redesign & the support to the national forecasting & quantification
technical working group, manual SCM system development, defined requirements for an electronic LMIS, and
Training of PSM and CMSC staff.
1.4.3 Central Medical Store
UNDP/ GFATM signed a Sub Recipient agreement with the CMS in 2011, with a mandate for the management
of procurement and supply of pharmaceuticals in Sudan. The main objective is the delivery of a wide range of
supply chain interventions to ensure consistent availability of products at all levels and to prevent treatment
disruptions by establishing a sound and reliable logistics system.

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 26
1.5 MONITORING AND EVALUATION
Monitoring and evaluation are indispensable learning and management tools for improving current and
future program planning, implementation and decision making. Regular verification of data, and data quality
assurance were among the priority areas for the UNDP/ GFATM M&E section throughout 2012. In order to
avoid creation of an M&E system parallel to the national one, UNDP/ GFATM has exerted efforts into
strengthening the latter. To guarantee collection of data for all indicators using data tools from national
programs which feed the quarterly reports, UNDP/ GFATM, continued working in collaboration with all
partners to review these tools to ensure all important information is captured, and data quality is maintained.
Towards the second half of the year, UNDP‐ GFATM PMU conducted HIV/AIDS Round 5 Outcome Evaluation
Studies focusing on (i) Prevention; and (ii) Care and Treatment components of the program, as an effort to
improve the quality and effectiveness of the national, multi‐sectoral response to HIV/AIDS in Sudan.
The evaluation revealed that program targets were achieved or exceeded except for those related to ART
programme coverage and patient retention, and TB and HIV collaborative activities. Accordingly, the study
recommended investigating the factors contributing to the low patient retention rates at ART centres. This
evidence should then guide a national strategy to improve patient retention and ART adherence monitoring.
The evaluation findings also emphasized the need to strengthen the ability to collect and interpret
information regarding the progression of the HIV epidemic and the influence of the country’s unique socio‐
cultural dynamics on the uptake and utilization of care and treatment services. Such effort would allow
continually monitoring the relevance of the HIV care and treatment programme and adapting it accordingly.
The evaluation studies have underscored that the Round 5 HIV grant made a significant contribution to the
HIV Integrated Bio‐Behavioural Surveillance Survey (IBBS survey project); the findings of which have
established a baseline for the states and served as a means for generating strategic information to design
appropriate interventions for the key populations.
During the fourth quarter of the year UNDP‐GFATM PMU and the LFA conducted On‐Site Data‐Verification
(OSDV) for the TB & HIV grants and Rapid Service Quality Assessment (RSQA) for the HIV grant. The exercise
was intended to verify reported results mainly focusing on treatment and training indicators. The OSDV &
RSQA exercises covered selected health facilities in Khartoum, El Gezira and El Gadarif states.
The OSDV exercise made a number of recommendations including the need to develop standard operating
procedures (SOPs) in order to guide the recording and documentation process at all levels. The need for an
integrated and comprehensive database has also been highlighted through observations of the Global Fund,
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 27
the Local Fund Agent (LFA) and various national partners. Observations and recommendations made during
these visits were shared with the UNDP‐ GFATM PMU, CCM and partners.
In order to closely monitor the grant implementation, based on the findings of the shared quarterly reports,
UNDP‐GFATM PMU, SRs and national programmes jointly conducted over 20 field visits to facilities supported
with GF grants (10 field visits to the HIV/AIDS facilities, four visits to TB facilities, five visits to Malaria
facilities, and two visits covering training related activities). Ten out of the seventeen states in Sudan were
covered during those visits. The visits covered the data quality assurance, staff training status; facilities’
supply stock status which includes drugs and test kits; inspection of the warehouses for storage conditions of
the drugs and test kits as well as expired supplies. Reports of the visits with findings and recommendations
were shared timely with the implementing partners.
M&E Related Achievements and Challenges in 2012:
Major achievements:
Contribution to development of National M&E Plans for HIV/AIDS & TB Programs
Initiation of the first National TB Prevalence Survey
Contribution to the implementation of the National Malaria Indicator Survey (MIS)
Successful completion of two evaluation studies on HIV/AIDS prevention, care and treatment
Major challenges:
Limited access in some states for M&E and supervision due to security related restrictions
Lack of National Strategic Framework on M&E
Poorly developed M&E systems & infrastructure especially at the state level
Lack of national policy or strategy on Health Management Information System (HMIS)
Poor progress in finalizing results of HIV/AIDS sero‐behavioural survey
High turnover of trained staff at all levels of the health system, especially at state level
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 28
1.6 CHALLENGES, LESSONS LEARNED AND RECOMMENDATIONS
Challenges Related to Security
In 2012, the volatile security situation in certain parts of the country posed constraints on the implementation
and monitoring of project activities. This has been prominent in certain regions of the country, mainly in the
Blue Nile, South Kordofan and several areas of Darfur States. The Darfur states were less accessible for
supervision visits by national health cadres. Consequently, there is also a high turnover of trained state
ministries’ of health staff which negatively impacted the timely reporting from the health facilities to the
state and federal levels. Uneven distribution of health workers in the country, especially the shortage in
security volatile and hard to reach areas has continued to negatively affect access to and quality of services.
Challenges related to programme implementation
Although the unpredictable security situation in many parts of the country posed a continued challenge to the
activities; security challenges are not the only problem facing GFATM projects. At the national level, although
information/ statistics of the prevalence rates of the three diseases is available, there is a lack of information
on the quality and access to health services available throughout the country.
Additionally, the monitoring role of the local administration at the state levels is limited. The sustainability
and ownership of all the programmatic activities at the state levels is crucial to the sustained control of the
three diseases and strengthening the health system in Sudan. However, the changing and limited leadership
role of the local administration continues to be a challenge.
At the national level, there is a substantially high rate of medical staff turnover due to the economic
challenges facing medical staff throughout the country; as well as brain drain. Finally, the limited capacity of
national CSOs when trying to access GFATM funds is problematic. Since the UN and GFATM requirements for
funding are quite strict, this has deterred access of local and national organisations working with the three
diseases. However, by September 2012, the GFATM Board has modified the additional safeguard policy
imposed on Sudan and partially approved the direct access to resources by government entities and CSOs.
This is a major and positive development in terms of creating capacity and reaching most hard to reach
communities in the country. Although in 2012, there were several activities focusing on capacity building of
national NGOs, this remained to be a challenge throughout the year.
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 29
1.7 FOCUS AREAS FOR 2013
In line with UNDP’s major intervention and the modified Additional Safeguard Policy, UNDP as a PR will be
engaging several government implementing entities and NGOs to directly implement Global Fund grants as
key Sub‐recipients. This new implementation arrangement will start with TB and HSS grants while other
grants will adopt this arrangement gradually in the years to come. In this context, UNDP will be implementing
several Capacity development activities to national entities and NGO implementing partners, mainly focusing
on Program management and institutional capacity. In this regard, preparations are underway since late 2012
to hold several trainings on grant management, financial management and compliance and Monitoring and
evaluation.
Another major area of engagement for UNDP in 2013 is the alignment of GFATM programs with the recent
reform introduced within the Ministry of Health. Reform created and merged several programs into
respective directorates with significant changes in role and responsibilities. This transition requires a close
follow up and coordination, while ensuring the continuity of service delivery and achievement of the different
targets set for GFATM grants.
With regard to specific grants, UNDP along with the relevant partners will be focusing on the following major
areas of work in 2013:
Round 7 Malaria Grant
To continue delivering the first line drugs for malaria treatment free of charge to more than 4, 630
health facilities with special focus on IDPs, refugees and peripheral communities.
To enhance malaria vector control interventions through the distribution of approximately 1.3 million
long lasting insecticide bed net to targeted communities.
To strengthen the procurement and supply system by refurbishing 4 malaria warehouses in South
Kordofan state.
To continue upgrading the capacity of malaria control staff at the sub national level by conducting
various training courses in the field of malaria.
Completion of Malaria Indicator Survey (MIS) by March, 2013 and dissemination of the report
Round 10 Malaria Grant
Completion of Malaria Programme Review (MPR) to assess where the programme stands and to
update the national strategic plan for malaria control in the country with special focus on the national
M&E plan.
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 30
Continue supporting the implementation of M&E e‐database to strengthen the malaria surveillance
for timely reporting as well as timely feedback. This will be done in conjunction with the ongoing
national effort to unify the health management information system (HMIS)
To equip malaria sentinel sites with computers and internet services to monitor the malaria trends to
contain malaria outbreaks.
To distribute more than 2.3 million lasting insecticide treated bed nets to protect approximately 1.5
million people including pregnant women and children under the age of 5.
To continue supporting IRS intervention in Gezira and Sennar states
Round 5 HIV Grant
Ensure the proper and complete closure of the round 5 HIV grant and finalize the implementation of
activities which were part of the grant close plan.
Round 10 HIV Grant
To provide HIV testing and counseling services for at least 400,000 people from the general
population and 2,700 MARPs.
To provide ART for a minimum of 217 HIV positive pregnant women as part of MTCT of HIV
To provide ART services to 5,000 adults and children with advanced HIV infection.
To distribute 2.5 million condoms for free through health facilities and community based out‐ lets.
Tuberculosis (SSF TB)
All procurement for 2013 for Laboratories (equipment & consumables), 1st line and 2nd line drugs
have already been procured with staggered deliveries as per the needs and forecasted delivery dates.
Pharmaceuticals/Health Products, non‐pharmaceuticals and services worth of $2,530,401, $1,725 &
$196,214, respectively will also be provided in 2013 to support the program and improve access and
quality of services.
In 2012 equipment and furniture for TBMUs, DOTS centres & TBMU Labs have been requested. The
furniture for the 18 TBMUs and 54 DOTS is already delivered and installed in the respective facilities
while additional 5 Zonal Labs & 10 QC Labs will be equipped in 2013 once the on‐going physical
renovations of these facilities is completed.
Renovation of all 10 QC labs & 35 TBMU labs, 5 Zonal Labs 2 wards of Abu Anja MDR Hospital will
continue and is planned to be completed in 2013.
Preparation for all three TB surveys is completed during 2012 including the Drug Resistance Survey
(DRS), KAP survey and TB prevalence survey. These surveys will be conducted in 2013 and2014.

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 31
The PR through its TB, finance & M&E team will continue to enhance and improve the capacity of the
National counterparts especially the new SRs such as NTP, Epi‐Lab & STPA through on the job
trainings, supportive Supervision, training on Monitoring and Evaluation, reporting, and financial,
accounting and book keeping.
Detailed targets set to be reached in 2013 interims of service delivery; case detection, treatment and
other programmatic indicators are provided in the annex of this report.
Health System Strengthening
The health system strengthening project is a cross cutting project, addressing the mainstream health
care delivery in areas of governance, health care delivery, health information systems, and human
resources for health, pharmaceutical supply management and service delivery. These components of
the project are wrapped around and cross cut the different functions of the health system ensuring
project deliveries. In 2013, the main focus is to enable government counterparts and the Ministry of
Health manage GFATM projects directly by themselves. This entails, In light of the additional safe
guard policy applied by the Global Fund, engaging new SRs, especially the government, requires a lot
of capacity development and risk management interventions. In 2013, organizational leadership,
management, transparent decision‐making and ensuring accountability systems are in place
In addition, the regular HSS interventions in areas of service delivery, HMIS HRH, PSM and Health care
financing will continue. In this regard, additional rural hospitals will be upgraded, referral laboratories
will be equipped and furnished, Primary health care centres will be provided with the necessary
medical equipments and furniture, more focus will be given in training newly recruited CHVs; a total
of 570 in 2013. Additional two AHSs will be renovated and equipped. The IT infrastructure will be
supported to galvanize the government’s effort to streamline and consolidate the HMIS system.
Locality and State Health management teams will be provided both technical and material support.
CONCLUSION
This Annual report is intended to capture the main achievements of the year. However, it is worth underlining
the importance of the huge efforts exerted by all stakeholders involved. The GFATM has gone a long way
since the beginning of activities in 2005. Although there is a lot to be praised; we hope that the coming years
will sustain previous achievements as well as accomplish further successes. All those involved understand
that the road was a difficult one and there is also a lot to look forward to in the coming years head; with the
hope that finally all the people of Sudan will enjoy the benefit of a healthy life.
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 32
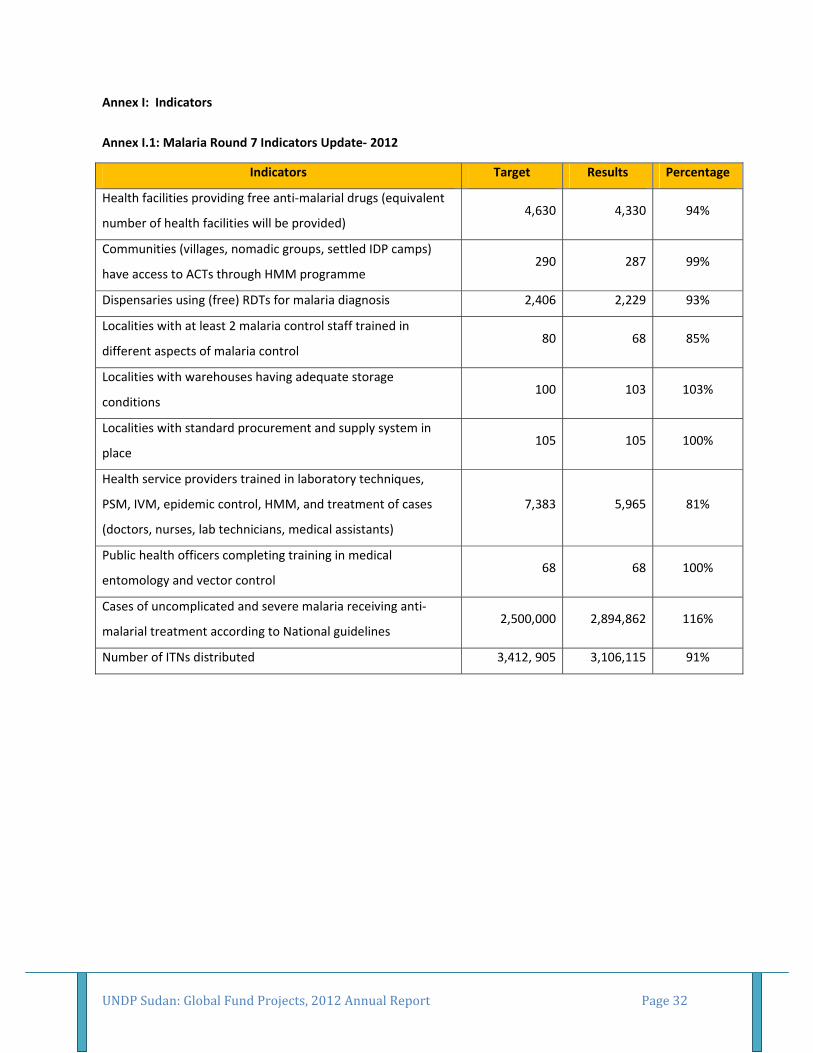
Annex I: Indicators
Annex I.1: Malaria Round 7 Indicators Update‐ 2012
Indicators Target Results Percentage
Health facilities providing free anti‐malarial drugs (equivalent
number of health facilities will be provided) 4,630 4,330 94%
Communities (villages, nomadic groups, settled IDP camps)
have access to ACTs through HMM programme 290 287 99%
Dispensaries using (free) RDTs for malaria diagnosis 2,406 2,229 93%
Localities with at least 2 malaria control staff trained in
different aspects of malaria control 80 68 85%
Localities with warehouses having adequate storage
conditions 100 103 103%
Localities with standard procurement and supply system in
place 105 105 100%
Health service providers trained in laboratory techniques,
PSM, IVM, epidemic control, HMM, and treatment of cases
(doctors, nurses, lab technicians, medical assistants)
7,383 5,965 81%
Public health officers completing training in medical
entomology and vector control 68 68 100%
Cases of uncomplicated and severe malaria receiving anti‐
malarial treatment according to National guidelines 2,500,000 2,894,862 116%
Number of ITNs distributed 3,412, 905 3,106,115 91%
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 33
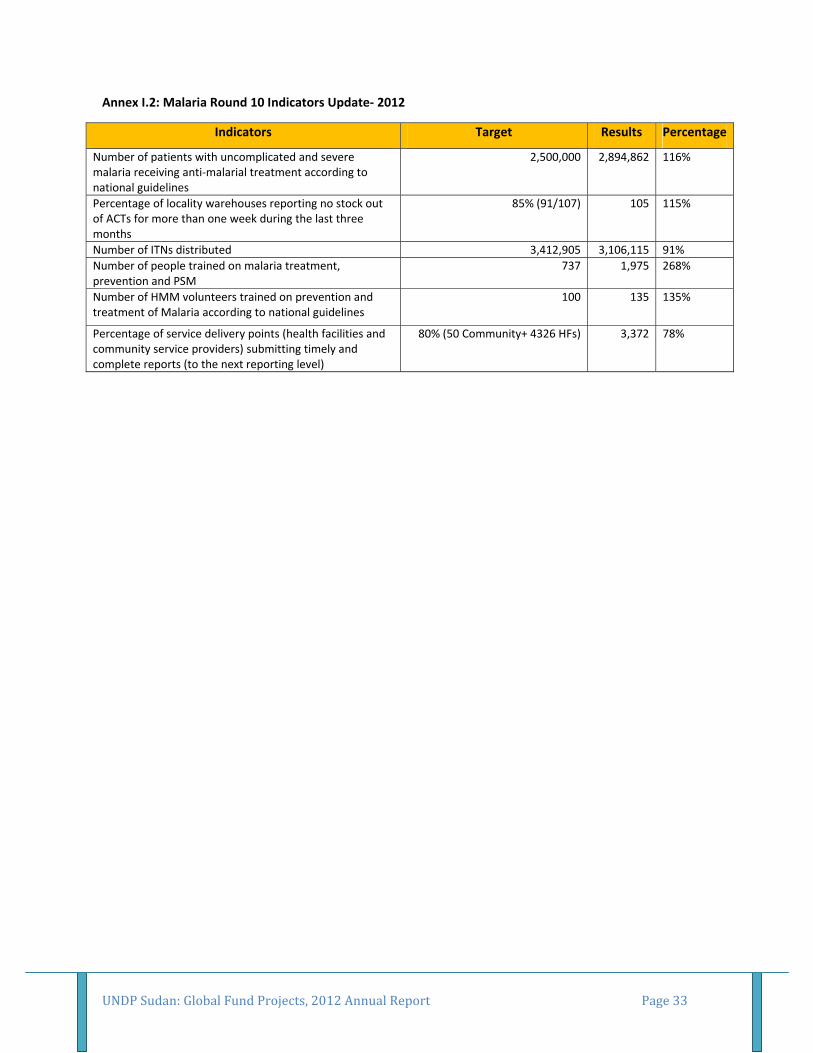
Annex I.2: Malaria Round 10 Indicators Update‐ 2012
Indicators Target Results Percentage
Number of patients with uncomplicated and severe malaria receiving anti‐malarial treatment according to national guidelines
2,500,000 2,894,862 116%
Percentage of locality warehouses reporting no stock out of ACTs for more than one week during the last three months
85% (91/107) 105 115%
Number of ITNs distributed 3,412,905 3,106,115 91%
Number of people trained on malaria treatment, prevention and PSM
737 1,975 268%
Number of HMM volunteers trained on prevention and treatment of Malaria according to national guidelines
100 135 135%
Percentage of service delivery points (health facilities and community service providers) submitting timely and complete reports (to the next reporting level)
80% (50 Community+ 4326 HFs) 3,372 78%
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 34
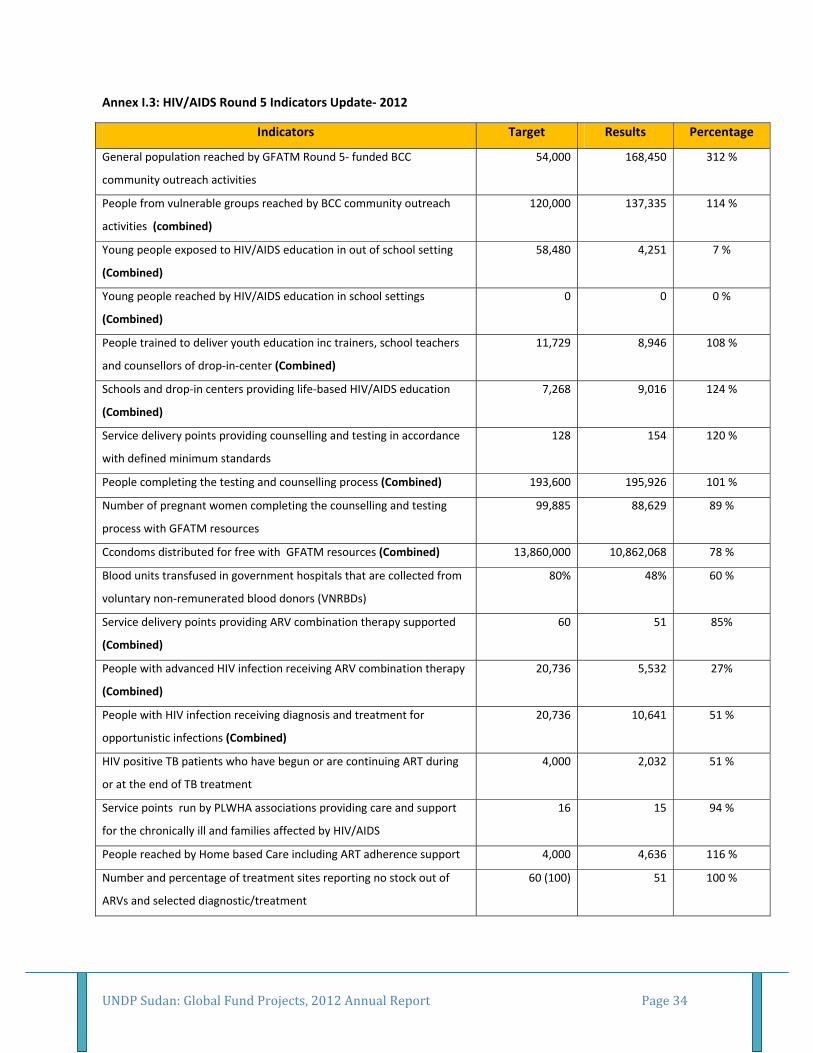
Annex I.3: HIV/AIDS Round 5 Indicators Update‐ 2012
Indicators Target Results Percentage
General population reached by GFATM Round 5‐ funded BCC
community outreach activities
54,000 168,450 312 %
People from vulnerable groups reached by BCC community outreach
activities (combined)
120,000 137,335 114 %
Young people exposed to HIV/AIDS education in out of school setting
(Combined)
58,480 4,251 7 %
Young people reached by HIV/AIDS education in school settings
(Combined)
0 0 0 %
People trained to deliver youth education inc trainers, school teachers
and counsellors of drop‐in‐center (Combined)
11,729 8,946 108 %
Schools and drop‐in centers providing life‐based HIV/AIDS education
(Combined)
7,268 9,016 124 %
Service delivery points providing counselling and testing in accordance
with defined minimum standards
128 154 120 %
People completing the testing and counselling process (Combined) 193,600 195,926 101 %
Number of pregnant women completing the counselling and testing
process with GFATM resources
99,885 88,629 89 %
Ccondoms distributed for free with GFATM resources (Combined) 13,860,000 10,862,068 78 %
Blood units transfused in government hospitals that are collected from
voluntary non‐remunerated blood donors (VNRBDs)
80% 48% 60 %
Service delivery points providing ARV combination therapy supported
(Combined)
60 51 85%
People with advanced HIV infection receiving ARV combination therapy
(Combined)
20,736 5,532 27%
People with HIV infection receiving diagnosis and treatment for
opportunistic infections (Combined)
20,736 10,641 51 %
HIV positive TB patients who have begun or are continuing ART during
or at the end of TB treatment
4,000 2,032 51 %
Service points run by PLWHA associations providing care and support
for the chronically ill and families affected by HIV/AIDS
16 15 94 %
People reached by Home based Care including ART adherence support 4,000 4,636 116 %
Number and percentage of treatment sites reporting no stock out of
ARVs and selected diagnostic/treatment
60 (100) 51 100 %
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 35
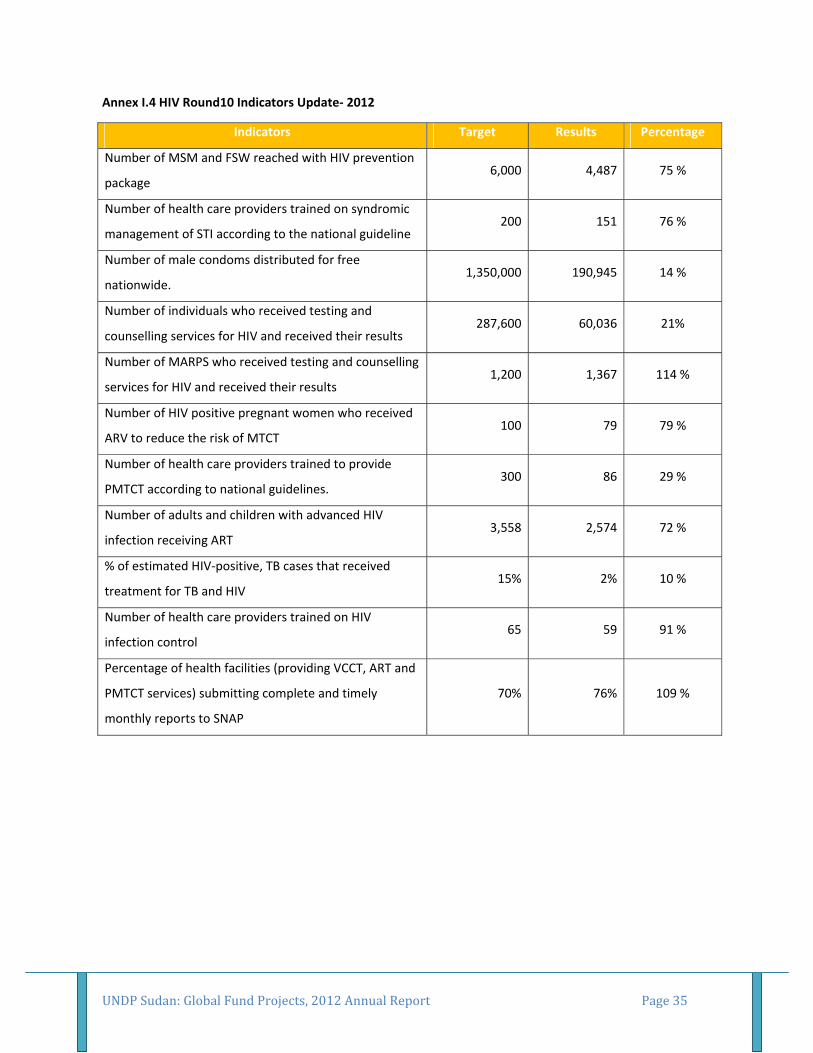
Annex I.4 HIV Round10 Indicators Update‐ 2012
Indicators Target Results Percentage
Number of MSM and FSW reached with HIV prevention
package 6,000 4,487 75 %
Number of health care providers trained on syndromic
management of STI according to the national guideline 200 151 76 %
Number of male condoms distributed for free
nationwide. 1,350,000 190,945 14 %
Number of individuals who received testing and
counselling services for HIV and received their results 287,600 60,036 21%
Number of MARPS who received testing and counselling
services for HIV and received their results 1,200 1,367 114 %
Number of HIV positive pregnant women who received
ARV to reduce the risk of MTCT 100 79 79 %
Number of health care providers trained to provide
PMTCT according to national guidelines. 300 86 29 %
Number of adults and children with advanced HIV
infection receiving ART 3,558 2,574 72 %
% of estimated HIV‐positive, TB cases that received
treatment for TB and HIV 15% 2% 10 %
Number of health care providers trained on HIV
infection control 65 59 91 %
Percentage of health facilities (providing VCCT, ART and
PMTCT services) submitting complete and timely
monthly reports to SNAP
70% 76% 109 %

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 36
Annex I.5 SSF TB/HSS Indicators Update‐ 2012
Indicators Target Results Percentage
Number of new smear positive cases detected. 10,120 6,518 64%
New smear‐positive TB patients successfully treated (cured plus
completed treatment) among the new smear positive TB patients
registered during a specified period (number and percentage).
7,742
(85%)
5,129
(71%) 83%
Number of new smear positive TB cases detected in the newly
established TBMUs/DOTS centres in Darfur and post‐conflict areas. 330 239 72%
New smear‐positive TB patients successfully treated (cured plus
completed treatment) among the new smear positive TB patients
registered during a specified period (number and percentage) ‐ in
the newly established TBMUs/DOTS centres in Darfur and post‐
conflict areas.
187 (85%)201
(69%) 81%
Number of private health facilities, TBMUs and DOTs links from
public health facilities that report to the NTP timely (as defined in
M&E Plan)
690 451 65%
Number of TB patients who receive HIV counselling and testing
(among registered TB patients) ( results from 12 TBMUs with VCT
capability).
2,400 2,791 116%
Number of condoms distributed for TB patients through TBMUs. 320,000 190,589 60%
Number of MDR‐TB cases diagnosed. 350 254 73%
Number of TB patients supported with an income generation
scheme. 150 117 78%
Number of new TBMUs established in Darfur and post‐conflict areas. 18 27 150%
Number of new DOTS centres established in Darfur and post‐conflict
areas. 54 54 100%
Number of TBMU laboratories renovated. 45 0 0.0%
Number of Health management personnel from 114 localities
trained in decision‐making, teamwork, effective meetings, health
planning and district health management
432 293 68%
Number of Rural hospitals, dispensaries and PHC centres equipped
and furnished according to national standards 53 30 57%
Number of Rural and State Hospital laboratories upgraded to provide
referral service, including for the three diseases. 35 19 54%
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 37
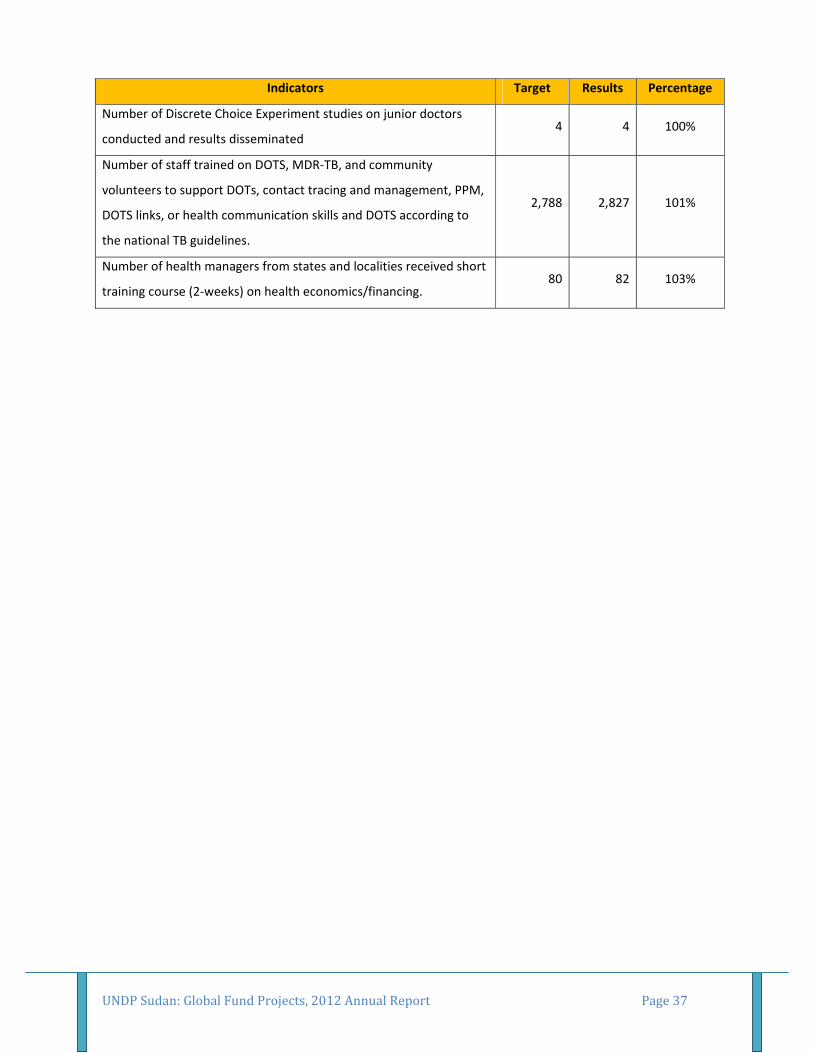
Indicators Target Results Percentage
Number of Discrete Choice Experiment studies on junior doctors
conducted and results disseminated 4 4 100%
Number of staff trained on DOTS, MDR‐TB, and community
volunteers to support DOTs, contact tracing and management, PPM,
DOTS links, or health communication skills and DOTS according to
the national TB guidelines.
2,788 2,827 101%
Number of health managers from states and localities received short
training course (2‐weeks) on health economics/financing. 80 82 103%
UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 38
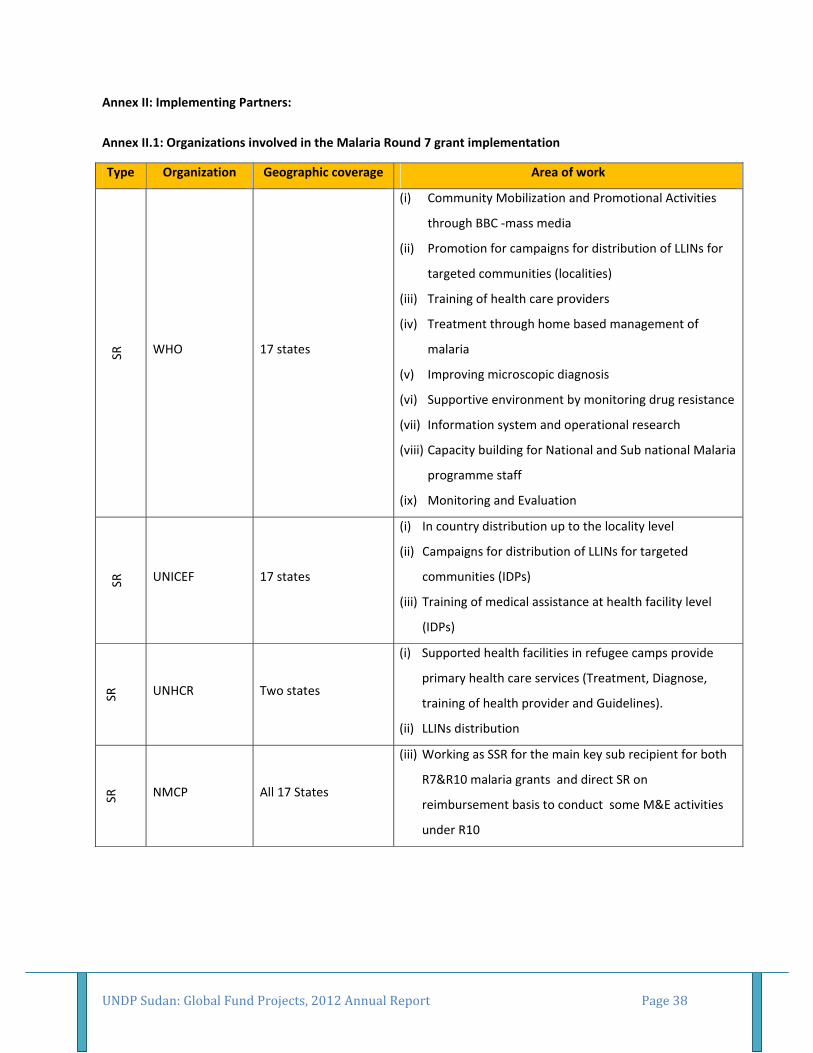
Annex II: Implementing Partners:
Annex II.1: Organizations involved in the Malaria Round 7 grant implementation
Type Organization Geographic coverage Area of work
SR
WHO 17 states
(i) Community Mobilization and Promotional Activities
through BBC ‐mass media
(ii) Promotion for campaigns for distribution of LLINs for
targeted communities (localities)
(iii) Training of health care providers
(iv) Treatment through home based management of
malaria
(v) Improving microscopic diagnosis
(vi) Supportive environment by monitoring drug resistance
(vii) Information system and operational research
(viii) Capacity building for National and Sub national Malaria
programme staff
(ix) Monitoring and Evaluation
SR
UNICEF 17 states
(i) In country distribution up to the locality level
(ii) Campaigns for distribution of LLINs for targeted
communities (IDPs)
(iii) Training of medical assistance at health facility level
(IDPs)
SR
UNHCR Two states
(i) Supported health facilities in refugee camps provide
primary health care services (Treatment, Diagnose,
training of health provider and Guidelines).
(ii) LLINs distribution
SR
NMCP All 17 States
(iii) Working as SSR for the main key sub recipient for both
R7&R10 malaria grants and direct SR on
reimbursement basis to conduct some M&E activities
under R10

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 39
Annex II.2: Organizations involved in the Malaria Round 7 grant implementation
Type Organization Geographic coverage Area of work SR
WHO 17 states
(x) Community Mobilization and Promotional Activities
through BBC ‐mass media
(xi) Promotion for campaigns for distribution of LLINs for
targeted communities (localities)
(xii) Training of health care providers
(xiii) Treatment through home based management of
malaria
(xiv) Improving microscopic diagnosis
(xv) Supportive environment by monitoring drug resistance
(xvi) Information system and operational research
(xvii) Capacity building for National and Sub national Malaria
programme staff
(xviii) Monitoring and Evaluation
SR
UNICEF 17 states
(iv) In country distribution up to the locality level
(v) Campaigns for distribution of LLINs for targeted
communities (IDPs)
(vi) Training of medical assistance at health facility level
(IDPs)
SR
NMCP All 17 States
(iv) Working as SSR for the main key sub recipient for both
R7&R10 malaria grants and direct SR on
reimbursement basis to conduct some M&E activities
under R10

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 40
Annex II.3: Organizations involved in the HIV/AIDS Round 5 grant implementation
Type Organization Geographic coverage Area of work SR
UNFPA
River Nile, El Gazeera,
Kassala, Khartoum
State
(i) Awareness outreach activities an mainstreaming of
HIV/RH services
(ii) Condom promotion and distribution
(iii) Providing health care services
(iv) Capacity building activities of local NGOs
UNICEF All 15 states
(i) Behaviour Change Communication‐Communication
Outreach
(ii) Youth Education
(iii) Provision of VCCT services
(iv) PMTCT and community mobilization
WHO All 15 states
(i) Blood safety
(ii) Provide VCCT services for clients
(iii) Care and support for PLHIV
(iv) Training of health care providers on ART
(v) Provision of OIs diagnosis and treatment
UNAIDS All 15 states (i) Coordination, monitoring and evaluation
(ii) Partnership development

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 41
Annex II.4: Organizations involved in the TB/HSS SSF grant implementation
Type Organization Geographic coverage Area of work
SR WHO
All 15 States
(i) Health workers trainings
(ii) Improvement of cased detection and treatment
(iii) Improvement of reporting
SR NTP Darfur States &
Khartoum State
(i) Identify/develop partnership with NGOs in war‐affected
Darfur States through conducting 2 workshops in each
Darfur state and one central workshop in Khartoum
state
SR EpiLab
All 15 States but
centrally at Khartoum
state level
(i) Build capacity with TB staff on health communication
skills.
(ii) Conduct message pre‐testing for ACSM communication
program
SR STPA All 15 States
(i) Expand existing ACSM networks by engaging health
educators, NGOs and civil society
(ii) Build capacity for TB advocacy with the media
(iii) Empower TB patients and their families through
supportive environments
(iv) Support TB female patient empowerment

UNDP Sudan: Global Fund Projects, 2012 Annual Report Page 42
Annex II.5: Organizations involved in the TB/HSS SSF grant implementation
Type Organization Geographic coverage Area of work
SR
WHO National
(v) Improve health services delivery including laboratory
services, assuring quality and equity of access at all
levels of health care;
(vi) Strengthen health management information system,
including surveillance and setting up a M&E system for
measuring the health system’s performance;
(vii) Build capacity of the system for drugs, supplies and
equipment procurement and management, including
quality assurance;
(viii) Scale up, quantitatively and qualitatively, the
availability of HRH at different levels of health care that
matches the basic standards;
(ix) Strengthen health financing function of health system
for assuring equity and access to health service