update on glp 1ra and dpp 4i - university of colorado denver · update on glp ‐1ra and dpp‐ ......
TRANSCRIPT

Update on GLP‐1RA and DPP‐4i
Robert E. Ratner, MDChief Scientific and Medical OfficerAmerican Diabetes Association
Alexandria, VA

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
Patient‐Centered Approach“providing care that is respectful of and responsive to
individual patient preferences, needs, and values ‐ ensuring that patient values guide all clinical decisions.”
• Gauge patient’s preferred level of involvement.
• Explore, where possible, therapeutic choices.
• Utilize decision aids.
•Shared
decision making – final decisions re: lifestyle choices ultimately lies with the patient.
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print](Adapted with permission from: Ismail-Beigi F, et al. Ann Intern Med 2011;154:554)

ClassClass MechanismMechanism AdvantagesAdvantages DisadvantagesDisadvantages CostCost
DPP‐4inhibitors
• Inhibits DPP‐4• Increases GLP‐1, GIP
• No hypoglycemia• Well tolerated
• Modest
A1c • ? Pancreatitis• Urticaria
High
GLP‐1
receptor
agonists
• Activates GLP‐1 R•
Insulin,
glucagon•
gastric emptying•
satiety
• Weight loss• No hypoglycemia• ? Beta cell mass• ? CV protection
• GI• ? Pancreatitis• Medullary ca• Injectable
High
Amylin
mimetics
• Activates amylin
receptor•
glucagon•
gastric emptying•
satiety
• Weight loss•
PPG• GI• Modest
A1c • Injectable• Hypo w/ insulin• Dosing
frequency
High
Bile acid
sequestrant
s
• Bind bile acids•
Hepatic glucose
production
• No hypoglycemia• Nonsystemic•
Post‐prandial
glucose
• GI• Modest
A1c• Dosing
frequency
High
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Adapted Recommendations: When Goal is to Avoid Weight Gain
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Adapted Recommendations: When Goal is to Avoid Hypoglycemia
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

How do GLP-1 Receptor Antagonists and DPP4 Inhibitors Mediate Their Non-Glycemic Effects?
Weight loss
Glucose
FFAs
Insulin
Lipids
Other mechanisms?
Indirect
Direct Actions on Tissues/Organs

GLP-1 Receptor Agonists and DPP4 Inhibitors Have Anti-Inflammatory Effects in Patients With Diabetes:

Clinical Trials of GLPClinical Trials of GLP--1 RAs in 1 RAs in Neurodegenerative DiseasesNeurodegenerative Diseases
US National Institutes of Health. http://www.clinicaltrials.gov.
Agent NCT Number Phase Disease Anticipated Completion
Exendin-4 NCT01255163 2 Alzheimer disease 2015
Exendin-4 NCT01174810 2 Parkinson disease 2013
Liraglutide NCT01469351 Not provided Alzheimer disease 2013

Incretin-Based Therapy: CV Outcomes Studies
Study Name Agent Evaluated Estimated
Enrollment
Estimated Duration
SAVOR‐TIMI 53 Saxagliptin 16,500 May 2010 ‐
July 2013
EXAMINE Alogliptin 5,400 Oct 2009 ‐
Dec 2013
ELIXA Lixisenatide 6,000 June 2010 ‐
Sept 2014
TECOS Sitagliptin 14,000 Dec 2008 ‐
Dec 2014
LEADER Liraglutide 9,340 Aug 2010 ‐
Jan 2016
SUSTAIN 6 Semaglutide 3,260 Feb 2013 – Jan 2016
EXSCEL Exenatide once weekly 9,500 June 2010 ‐
Mar 2017
CAROLINA Linagliptin 6,000 Oct 2010 – Sept 2018
REWIND Dulaglutide 9,622 July 2011 – April 2019
Clinical Trials.gov –
Accessed 8 June, 2013

GLP-1 Agonists: Increase Stimulated Calcitonin Release and Tumor
Formation in Rodents
Bjerre Knudsen L et al Endocrinology 2010
Hypothesis: In rodents, GLP‐1 receptor activation may cause cAMPand calcitonin release from the rodent C cells. Over time, this continued stimulation may
cause C cell hyperplasia.

Clinical Data: Calcitonin Levels & Incidence of C-Cell Pathology
• T2DM or nondiabetic obese patients in
clinical trials > 5000 subjects treated
with liraglutide
• 6 cases of C‐cell pathology– 4 in liraglutide group (0.11%) – all
C‐Cell hyperplasia
– 2 in active comparator group
(0.14%)
• 1 MTC in situ (GLIM + MET),• 1 MTC (GLAR + MET + GLIM, pre‐
randomization)
• Interpreted as “no evidence of
calcitonin release from human C cells”,
with limitations of:
– Duration of exposure (< 2 years)– Number of subjects
Hegedüs L, et al. J Clin Endocrinol Metab. 2011;96:853-860.Bjerre Knudsen L, et al. Endocrinology. 2010;1151:1473-1486.
Basal CT Levels (LEAD‐6, N = 464)
Time (weeks)
LIRA 1.8 mg (n = 233)EXN BID 10 mcg (n = 231)
Upper normal range males (8.4 ng/L)
Upper normal range females (5.0 ng/L)
0
2
4
6
8
10
LS M
ean Ca
lcito
nin (ng/L)
0 12 2620

Recommendations for GLP-1 RAs: Potential for C-cell Hyperplasia/
Medullary Thyroid Tumors in Animals • Liraglutide and Exenatide once weekly are contraindicated in patients with MEN2 or a
personal or family history of MTC1
– Counsel patients regarding MTC risk and symptoms of thyroid tumors1
• The value of routine calcitonin and/or ultrasound monitoring is uncertain; such
monitoring may lead to unnecessary procedures1
– Patients with thyroid nodules or elevated serum calcitonin levels identified for other
reasons should be sent to an endocrinologist1
• To monitor potential associations, report MTC to state cancer registry, regardless of
treatment: http://www.naaccr.org/Membership/MembershipDirectory.aspx2,3
MEN2, multiple endocrine neoplasia syndrome type 2; MTC, medullary thyroid carcinoma.
1. US FDA. Drugs@FDA. GLP-1 RA prescribing information. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA.
2. Bristol-Myers Squibb, AstraZeneca. Bydureon MTC registry information. http://www.bydureonhcp.com/Content/pdf/MTC_Registry_Information.pdf.
3. Novo Nordisk. Victoza MTC registry information. http://www.victozapro.com/pdf/Dear_Healthcare_Professional_Letter.pdf.

NIDDK-NCI Workshop on Pancreatitis-Diabetes-Pancreatic Cancer. http://www2.niddk.nih.gov/News/Calendar/PDPC2013.htm
• 2‐day workshop sponsored by NIDDK, NCI, and Pancreatic Cancer Action
Network
• Coming‐together of exocrine and endocrine fields
• Invited speakers from academia, NIH, FDA, industry
• 6 core sessions
• 1 session (7 presentations and panel discussion) dedicated to “Effects of DM
Treatment on Pancreatic Ductal Adenocarcinoma”

Increased Risk of Pancreatitis and Pancreatic Cancer with Type 2 Diabetes
Huxley et al, British Journal of Cancer 2005
Pooled estimate RR 1.82 (1.66, 1.99)

Reverse causality: Is diabetes an early symptom of pancreatic cancer?
Huxley et al, British Journal of Cancer 2005
Individuals in whom diabetes had only recently been diagnosed (<4 years) had a
50% greater risk of the malignancy compared with individuals who
had diabetes for
5 years (OR 2.1 vs 1.5; P=0.005).

Higher glucose, insulin concentrations and resistance associated with
increased pancreatic cancer risk, especially >10 years of follow up
Stolzenberg‐Solomon JAMA 2005


Mechanistic Evaluation of Exendin‐4 on Pancreatic Changes in Mice1
• Pdx‐1 Kras mice– Model primed to develop chronic pancreatitis and pancreatic cancer
• “These models can characterize the cellular and molecular pathology of pancreatic neoplasia and
cancer and constitute the best tool to investigate new therapeutic approaches, chemopreventive
and/or anticancer treatments”2
– Treated with exendin‐4 for 12 weeks– Results: expansion of pancreatic duct glands, mucinous metaplasia, columnar atypia
• Also identified GLP‐1 receptors in rodent and human– Pancreatic duct glands– Premalignant pancreatic intraepithelial lesions (PanIN)
• The investigators concluded that GLP‐1 RAs may– Induce focal proliferation in exocrine pancreas– Accelerate neoplastic PanIN lesion formation and exacerbate chronic pancreatitis in
the context of exocrine pancreas dysplasia
1Gier B, et al. Diabetes. 20122Herrerros-Villanueva M, World J Gastroenterol 2012

FDA Nonclinical Surveillance of Adverse Drug Effects
• Re‐examined data from chronic toxicology and carcinogenicity studies: – Minimal alteration of background findings at highest dose
• Issued post‐marketing requirement to conduct a pancreatic toxicology study in
rodent model of T2 DM, at least 3 months’
duration in a model marked by high
blood glucose and triglycerides, including extensive histological assessment
and proliferative staining– 3 studies meeting criteria submitted for review– Sporadic and minimal exacerbation of background histological changes– None definitively demonstrated treatment‐related adverse effect on
exocrine histology or proliferation• Initiated research into identifying appropriate experimental model with
ongoing non‐clinical investigation
Hummer BT. Abstracts from the NIH Workshop on Pancreatitis- Diabetes-Pancreatic Cancer

Observational Studies on Pancreatitis Risk With Exenatide &
Sitagliptin
Nauck M. Diabetes Care. 2013 May 6. [Epub ahead of print].

Methodological Limitations of Observational Studies in Assessing
Pancreatic Risk• Inadequate outcome validation• Incomplete covariate adjustment• Inadequate confounding control• Limited power for rare events• Biases
– Reporting bias– Stimulation bias, notoriety bias– Channeling bias (preferential prescribing to specific patient populations)– Selection bias– Protopathic bias (inadvertent prescription for early disease manifestation)
NIDDK-NCI Workshop on Pancreatitis-Diabetes-Pancreatic Cancer. http://www2.niddk.nih.gov/News/Calendar/PDPC2013.htmTES statement.
https://www.endocrine.org/sitecore%20modules/web/~/media/endosociety/Files/Advocacy%20and%20Outreach/Position%20Statements/All/TheEndocrineSo cietyStatementontheRiskofPancreatitisinPatientsTreatedwithGLP1basedTherapies.pdf#search=%22Singh%2
AACE, ADA press release. http://www.diabetes.org/for-media/2013/2013-aace-ada-jama-article.html;

Randomized Controlled Trial Evidence: GLP-1 Agonists
• Liraglutide1
– N > 6500; > 5000 patient‐years of exposure– Pancreatitis
• 1.8 cases per 1000 PYE ‐
none externally adjudicated• Background rate in DM: 0.5 – 4.2 cases per 1000 PYE
– Pancreatic cancer [3 cases (0.4 per 1000 PYE)]• 1: treated with liraglutide for 152 days• 1: treated with liraglutide for 7 days; Stage 4; weight loss prior• 1: diagnosed prior to randomization
• Exenatide twice daily2
– 19 clinical trials –
Exenatide (n = 3261), pooled comparators (n = 2333)– Pancreatitis ‐
no significant difference between groups• Exenatide: 0.27 per 100 PY• Control: 0.18 per 100 PY
PYE, patient-year of exposure
1. Moses, A. NIDDK-NCI Workshop on Pancreatitis-Diabetes-Pancreatic Cancer. http://www2.niddk.nih.gov/News/Calendar/PDPC2013.htm
2. MacConell L, et al. Diabetes Metabolic Syndr Obes. 2012 Jun 6. [Epub ahead of print].

Randomized Controlled Trial Evidence: DPP‐4 Inhibitors
Sitaglipitin Comparator
N 7726 6885
Mean Duration Exposure 284 days 264 days
Exposure‐adjusted
incidence rate
pancreatitis, including
“pancreatitis acute”
0.08 events/100 patient‐
years
0.09 events/100 patient‐
years
Exposure‐adjusted
incidence rate Pancreatic
cancer
0.05 events/100 patient‐
years
0.06 events/100 patient‐
years
Engel, S. NIDDK‐NCI Workshop on Pancreatitis‐Diabetes‐Pancreatic Cancer.
http://www2.niddk.nih.gov/News/Calendar/PDPC2013.htm

Incretin Therapy Effect on Human Pancreas?
• Pancreata from JDRF Network for Pancreatic Organ Donors with Diabetes (nPOD)
– Brain‐dead donors (N = 34)– Classified as Nondiabetic, DM – No Incretin, and DM‐Incretin
• Results for DM – Incretin– Enlarged pancreata vs DM – No Incretin– Increased exocrine pancreas cell proliferation– Increased PanIN lesion frequency– β‐
and ɑ‐cell hyperplasia, glucagon‐expressing microadenomas (3/8),
1 glucagon‐expressing neuroendocrine tumor
Butler A, et al. Diabetes. 2013 Mar 22. [Epub ahead of print].
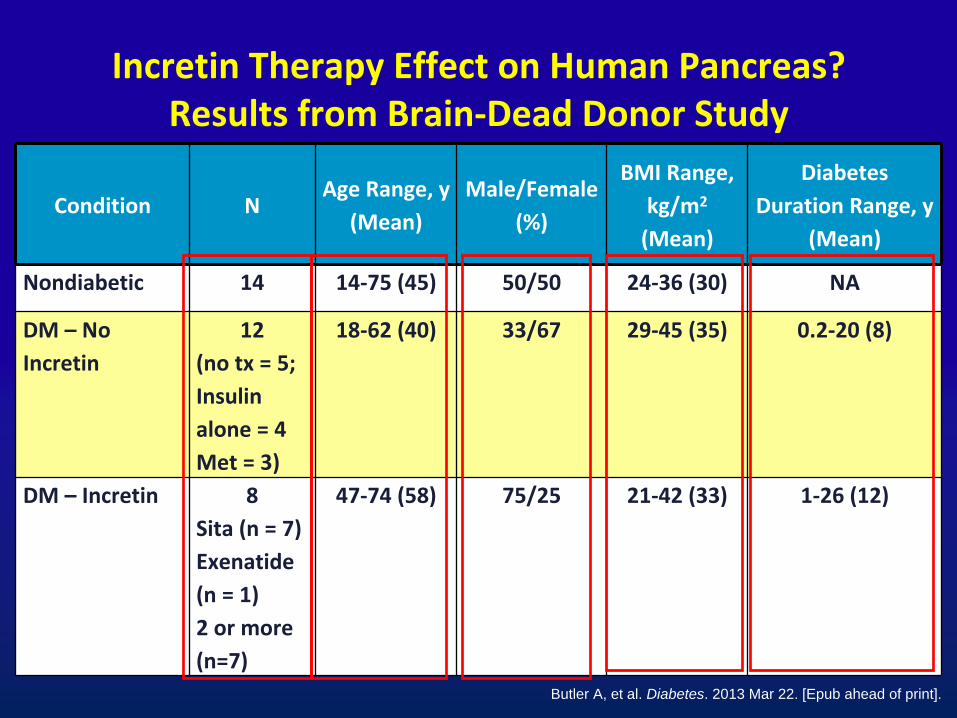
Incretin Therapy Effect on Human Pancreas? Results from Brain‐Dead Donor Study
Butler A, et al. Diabetes. 2013 Mar 22. [Epub ahead of print].
Condition NAge Range, y
(Mean)Male/Female
(%)
BMI Range,
kg/m2
(Mean)
Diabetes
Duration Range, y(Mean)
Nondiabetic 14 14‐75 (45) 50/50 24‐36 (30) NA
DM – No
Incretin12
(no tx = 5;Insulin
alone = 4Met = 3)
18‐62 (40) 33/67 29‐45 (35) 0.2‐20 (8)
DM –
Incretin 8Sita (n = 7)Exenatide
(n = 1)2 or more
(n=7)
47‐74 (58) 75/25 21‐42 (33) 1‐26 (12)

Incretin Therapy Effect on Human Pancreas?1: Study Limitations2, 3
• Limitations of this study, which should inform future study design in this field
– Inadequate controls; non‐matched populations• Could age difference (18 years) explain findings?• Type of diabetes? • Duration of diabetes• Medications
– Effect of prolonged life support– Small numbers– Requirement for more rigorous sampling, multivariate
modeling, and validation – Specificity of antibodies and techniques used in tissue
studies1. Butler A, et al. Diabetes. 2013 Mar 22. [Epub ahead of print].
2. NIDDK-NCI Workshop on Pancreatitis-Diabetes-Pancreatic Cancer: . Panel Discussion,
3Kahn SE, Diabetes 2013 April 17

Staining Specificity of GLP-1R Antibodies
Monoclonal ab3F52
Polyclonal abAB39072
Polyclonal abLS-A1205
Polyclonal abAP23801
Non‐transfectedBHK cells
GLP‐1RtransfectedBHK cells
Pyke C, Knudsen L. Endocrinology. 2013.

Safety Evaluation of Adverse Reactions
in Diabetes (SAFEGUARD): Funding, Aim and Participants
• European Medicines Agency endorsed funding by the European Union
• Aim: To assess the cardio-, cerebrovascular, renal and pancreatic safety of currently marketed non-insulin glucose-lowering agents
• Fifteen international (EU and US) partners - mainly academic
• Eight work packages to assess safety of glucose lowering agents
Smits MM et al: Abstracts of the Pancreatitis Diabetes Pancreatic Cancer Workshop, NIH 6/12-13/13

1.
CV outcome studies (n=9) afford a unique opportunity to identify and adjudicate pancreatic events (pancreatitis and
pancreatic cancer)2.
Creation of independent expert committee that has access to
all patient‐level data ‐> ADA Press Release June 10, 20133.
Collaborative efforts to design and implement long‐term,
prospective epidemiological studies specifically designed to address these issues
4.
Re‐evaluate current pharmacovigilance system based on spontaneous reporting, with goal of improving quality of data
collected and means of adjudicating and processing the information
Cefalu
W et al Diabetes Care online May 21, 2013

Endocrine Society Statement: 6/18/13
• The Endocrine Society believes that more research is needed in all areas of incretin‐based therapy before
any conclusion can be reached about its safety with regard to pancreatitis and pancreatic cancer risk.
• Support ADA’s effort to independently evaluate pooled patient‐level data.
• In interim, patients should be made aware of potential risk and symptoms of pancreatitis and providers should balance risk and benefit of treatment paradigms.

ADA/EASD/IDF Recommendations for Clinicians and People with Diabetes Concerning the Use of Incretin
Therapy
and Pancreatic Disease – June 28, 2013
The three organizations firmly believe that people taking these medications, or those who may consider taking them, should be informed of all that is currently known about their potential risks and advantages in order to make the best possible decisions
about their treatment and care, in consultation with their health care providers.
At this time, there is insufficient information to modify current treatment recommendations. No patient should discontinue
medication without first consulting with their health care provider. Their health care provider should take into account the
patient’s therapeutic responses and adverse events when considering whether to maintain or alter established therapy.

In Sum…• Are there potential mechanisms to explain the safety issues
discussed? Yes
• Is there concrete clinical evidence to suggest an alteration of current risk/benefit profiles of these agents? No
• Are there any substantial changes in clinical recommendations based on the recent studies? No
• Is there a need to pool together appropriate expertise, databases, and methodologies to address these questions
with scientific rigor? Yes!