update on perinatal and pediatric vitamin d michael k. georgieff m.d., faap professor of pediatrics...
TRANSCRIPT

Update on Perinatal and Pediatric Vitamin D
Michael K. Georgieff M.D., FAAPProfessor of Pediatrics
University of Minnesota School of Medicine

Vitamin D
Vitamin D is a steroid hormone (not a vitamin)
Initial form is Vitamin D3 (cholecalciferol)
Created in dermal cells by UV light exposure (converts cholesterol to D3)
Active form is 1,25 di-hydroxy vitamin D (calcitriol)

Vitamin D
De Novo synthesis of Vitamin D requires
– Sun exposure +
– Intact liver +
– Intact kidney or…
– Dietary source of calcitriol

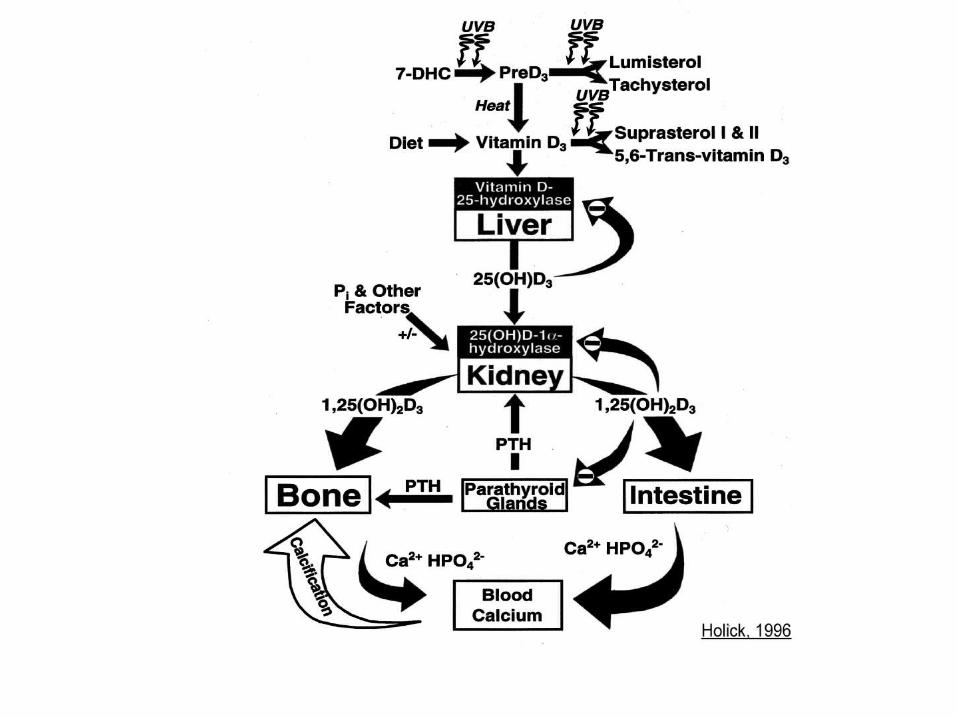
How Vitamin D Works Enhances intestinal absorption of
calcium and phosphorus
Increases tubular reabsorption of phosphorus
Does not work on bone (PTH does)
Important mediator of efficient recycling of calcium and phosphorus so they are available for bone growth and remodeling

Rickets General term refers to abnormal
bone growth and development due to pervasive lack of calcium and phosphorus substrate
Vitamin D deficient rickets results in disorganized cartilage in long bone growth plates
What about subclinical vitamin D deficiency?

Vitamin D Deficient Rickets
Presents between 6 and 18 months
Failure to attain or regression of motor milestones (notably walking or other weight- bearing activities)
Bowed legs, flared wrists, pain on major motor activity, growth failure
History of lack of sun exposure and dietary risk factors

Laboratory Findings Low serum calcium and phosphorus
Elevated PTH level (parathyroid hormone)
Very low 25-OH vitamin D level (hallmark finding)
– <27.5 nmol/L (11 ng/mL) is low in children
– <37.5 nmol/L (15 ng/mL) causes increase in PTH level in adults
– Unknown at what level PTH rises in children

Radiological Findings In Childhood Rickets
Flared epiphyses Bowing of long bones Rib changes Fractures

What are the Concerns?
• Healthy bone growth– In childhood– Bone banking for adulthood
• CNS effects• Genes regulated by vitamin D

Who is at Risk for Early Vitamin D Deficiency?
• Infants with low intrauterine accretion– Born to vitamin D deficient mothers– IUGR infants– Premature infants
• Infants with low vitamin D status– Lack of sun exposure +– Low dietary sources
Pediatric Vitamin D
Incidence of D deficiencyPopulations at Risk
Sources of vitamin DBreastfeeding
Supplementation (Baby or Mom?)

Prevalence
Rickets thought to be disease of the past
–“Disappeared” in early 1960s due to:• Recognition of role of sunlight in vitamin D
homeostasis; fortification of milk• Use of multivitamin preps• Higher prevalence of formula use• AAP CON recommended 400 IU/d starting at
2 weeks of age

PrevalenceIncreased case reports and series of
nutritional rickets since late 1970’sExact prevalence remains unknown
but prevalence of risk factors increasing–Less sun exposure–Higher prevalence of nursing –Decreased prescription of vitamins for nursing infants

Estimated Incidence from Hospitalized Children
No national data on incidence in US Georgia (1997-99)
9 per million hospitalized children 5/9 due to nutritional rickets (all darkly
pigmented children) All breastfed
National Hospital Discharge Survey (NHDS) 9 per million hospitalized children in US 75% darkly pigmented children; 50%<12
months

Estimated Incidence from Office-Seen Children
Pediatric Research in Office Setting (PROS) network of AAP– 23-32 cases per million child office
visits between 1/99 and 6/00.– Survey (low response rate=26%)– All darkly pigmented – All breastfed– Maternal Vitamin D status unknown

Estimated Incidence from Literature
13 articles published between 1996 and 2001
122 cases reported 12 US states 87% darkly pigmented Age range from 4 to 58 months at
diagnosis

What are the concerns?• Is the scientific evidence solid?
• Adverse effect on breastfeeding• Expense of supplementation• Risks of supplementation• Addressing the multiplicity of
issues• Increasing the risk of unhealthy
sun exposure behaviors

What are the questions? • What level of Vitamin D is adequate? • What do we really know about sunshine,
prevention of rickets, and risks of skin cancer• How much does skin pigmentation alter the dose?• If one were to recommend supplementation:
– Should the mother, the infant, or both receive supplementation
– Should this be universal or targeted?– What would be the correct dose?– What is the right age to start supplements
• Are the benefits worth the expense?

Low Sun Exposure: Major Risk Factor for
Rickets Northern climate (but not exclusively)
Seasonal
Dark pigmentation (but not exclusively)
Covered skin
Sunscreen use Proper sunscreen use decreases vitamin D
synthesis by 97%

Effects of Latitude and Season on D Status
• Iowa (41 degrees N) (EH Ziegler et al, 2006)
– During winter, 78% of breastfed infants were D deficient (25-OH level < 11 ng/ml)
• In South Carolina (32 degrees N) (LA Basile et al, 2007)
– African-American newborns had mean cord serum 25-OH level of 10.5 ±0.6 ng/ml
– Winter decreased cord serum 25-OH levels in A-A by 25% and in Caucasians by 35%

Appropriate Sunlight Exposure Prevents
Rickets• Infants born to mother’s with low Vit D
– Diaper only: 10-30 minutes/week– Fully clothed, no hat: 2 hours/week
• Infants born to mother’s with adequate Vit D– Diaper only: < 10 minutes/week– Fully clothed, no hat: 30 minutes/week
• Outside in the shade doesn’t work• 6-fold increased need in darkly pigmented
infants

In the Absence of Adequate Sunlight
ExposureLow dietary intake of Vitamin D becomes a major issue
Vitamin D deficient situations in infancy – Exclusive human milk feeding
– Infants consuming < 500 ml/d of fortified infant formula
– Not receiving vitamin prep containing vitamin D
– Vitamin D deficient pregnant or nursing mother

Dietary Content of Vitamin D
Human milk (22 to 100 IU/L)– Varies with maternal diet,
pigmentation/sun exposure– Light pigmentation 68 IU/L– Dark pigmentation 35 IU/L– Both fall far short of RDA/DRI (infant
does not consume 1L until 14 lbs=5-6 months of age)
– Maternal 3000 IU/d supplement-> 100 IU/L

Relative Importance of Fetal Stores, Milk and
Sun Sources Maternal and Infant 25-OH D serum
concentrations highly correlated until 8 weeks of age– Combined effects of maternal serum
levels on fetal stores (transplacental) and breastmilk content
After 8 weeks, sunlight exposure outweighs effects of mother’s vitamin D status

Dietary Sources of Vitamin D
Unfortified cow milk (24 IU/L)– High variability in measured vitamin
D in fortified cow milk (NEJM) Infant formula (400 IU/L)
– Infant must consume 1/2 L per day to receive DRI of 200 IU/day
– Term infant consumes that amount; preterm does not
Tri-vitamin (ADC) prep: 400 IU/dose

Daily Dietary Vitamin D Requirement to Prevent Rickets (0-36 months)
Dietary source-USA (IOM, 2001)
–200 IU/day (5 mcg) is the AI
Dietary source-Canada
–400 IU/day in summer–800 IU/day in winter

Nutritional Strategies to Improve Vitamin D StatusEffective strategies in infants (current
recs)– 200 IU vitamin D/day
• 1/2 dose tri-vitamin (ADC) prep• 500 ml of fortified infant formula• 5 mcg calcitriol
Recent strategies (experimental)– Supplementing the pregnant mother– Supplementing the nursing mother– Single high dose therapy

Maternal Vitamin D Supplementation During
Pregnancy• IOM (2001) determines
– AI as 200 IU/day– UL as 2,000 IU/day
• NHANES data: 50% of African-American women of reproductive age have low vitamin D level
• Infants born to Vitamin D deficient mothers have lower vitamin D stores– Dark skin ± skin coverage during pregnancy: 63%
rate of D deficiency in NBs compared to 16% in light skin/no skin coverage (Dijkstra et al, 2007)

Does Supplementation During Pregnancy Work?
• Supplementation of pregnant women– Improves neonatal calcium handling– Improves 9 year bone status– Improves maternal vit D levels if she was
deficient– Does not alter already sufficient maternal D
status
• Doses up to 2000 U/day are tolerated, but no trials to determine efficacy on fetal/neonatal stores

Does Maternal Vitamin D Supplementation During
Lactation Work?• Human milk vitamin D content is low and
reflects maternal vitamin D status• Supplementation of deficient mothers
increases milk D levels• The AI during lactation is 200 IU/day
(IOM, 2001)• The UL is 2,000 IU/day (IOM, 2001)• 3000 IU/day increases milk levels to 100
IU/L; still too low

High Dose Supplementation of Lactating Mothers (CL Wagner et al,
2006) • Mothers randomized at 1 month to 400 vs 6400
IU/d X 6 months• Control infants received 300 IU; infants of
supplemented mothers received 0 IU• Results: anti-rachitic activity of maternal
supplemented infants equaled that of infants receiving only postnatal dietary supplementation
• No toxicity noted in high dose mothers• Shows feasibility of maternal supplementation
only

Cost to prevent Is universal supplementation of infants
cost effective?– Cost of Tri-Vi-Sol ($6.00/month)– Incidence estimate
• 5 hospitalized per million children• 25 ambulatory cases per million
– Cost per hospitalization averted: $4,800,000
– Cost per case averted: $958,000 Cost to prevent far outweighs cost to treat

Summary of Pediatric Vitamin D
• Vitamin D deficiency is increasingly recognized– Seasonal and Geographical– Mostly in breastfed infants of color
• Contributors are lack of sunlight exposure and low levels of D in unsupplemented milk
• Effective therapies include supplementation of breastfed infants with 200 IU and supplementation of lactating mothers with >4000 IU/day– Only the former is currently recommended by AAP

Perinatal Vitamin D
Populations at RiskOsteopenia of Prematurity
Does Postnatal D work?Can Prenatal D prevent?

Osteopenia (Rickets) of Prematurity
Staging:1. Hypodensity of bones2. Abnormalities of metaphyses
Fraying and cuppingDense line (healing)
3. Above findings and fractures
1.
2.
3.
Courtesy of Steve Abrams MD

Osteopenia of prematurity: Usually a disease of inadequate calcium and phosphorus intake
Calcium intake (mg/kg/d)
Calcium retention (%)
Calcium retention (mg/kg/d)
In Utero N/A N/A 100-120Human milk 40 60-70 25-30Routine cow milk-based formula
80-90 40-50 35-45
Total parenteral nutrition
Up to 80 >95% 70-80

Vitamin D in preterm infants• Adequate Intake (AI) for vitamin D for full-term infants is 200
IU/day. Upper limit (UL) is 1000 IU/d (US 1997).
• There is substantial evidence that little Ca absorption is
transcellular “active” (Vitamin D-dependent) in first months of
life in premature or even in full-term infants.
• Multiple studies demonstrate that intake of 160-400 IU/day
leads to adequate vitamin D levels (Cooke 1990, Pittard 1991,
Backstrom 1999, Koo JPGN, 1995).
• Preterm formula provides, when fed at 120 cal/kg/d to a 1.5 kg infant: SSC:150 IU/100 kcal = 270 IU/day and EPF: 270 IU/100 kcal = 486 IU/day
• Human milk fortifiers marketed in US provide 150 IU/4 packets.

Higher doses of vitamin D?•No evidence for benefits in preterm
infants. One study evaluating up to 1000 IU found no short or long-term benefit (up to 11 yrs!) of higher amounts (Backstrom, JPGN, 1999).
•Some, especially in Europe, recommend providing up to 1000 IU/d routinely for preterm infants- little evidence for or against this.

High dose effects
• Preterm formula, 2700 IU/L. (1200-1700 IU/L in US)
• Unanswered question is: What is the target 25-OHD?
Nako, Pediatrics International 2004;46:439-443.

When might more vitamin D be helpful?
•Vitamin D related absorption increases at 6-8 weeks of age – when osteopenia worsens. Provide 400-600 IU/d if alk phos > 800 IU/L.
•Cholestatic babies cannot form 25-hydroxyvitamin D in their liver. Consider increasing intake for direct bili > 4 to a maximum of 1000 IU/day total vitamin D.
–If no response or worsening alk phos, consider adding 1,25 dihydroxyvitamin D (calcitriol, Rocaltrol). Obtain 25-OHD level first and treat if < 20-25 ng/mL.

Assessment and Plans

Arctic Circle Equator
Geographic Location
SeasideElevation Mountains
Sun-seeking Behaviors Always outside Never outside
DeepSkin Pigmentation Light
Mostly uncovered
Cultural Dress Mostly covered
Never Owned Any Sunscreen Use Applies to any exposed skin
SUNLIGHT EXPOSURE FACTORS
Prenatal Assessment of Maternal Vitamin D Stores
Diet No milk, No fish Vit D fortified Milk, Salmon 3 X a week
Present Diseases assoc. with Vit D Deficiency
Not present
Supplements No supplements 400 IU Vit D per day
DIETARY FACTORS

Prenatal CounselingEither sun exposure or dietary
sources should meet requirements
Good sources & stores
Acknowledge good habits
Counsel regarding appropriate diet and
sun exposure
Few or no sources
Counsel regarding appropriate diet and sun exposure and
consider supplements
Counsel regarding appropriate diet and sun exposure and
prescribe supplements
Questionable sources & stores

Counseling Options for Mothers
• Drink Vitamin D fortified milk• Eat one serving salmon 3 times a week • Expose hands, face, and arms to sunlight
for 5-15 minutes 2-3 times a week• Increased time may be necessary for
persons with deeper pigmented skin• Take Vitamin D supplement of 200 IU
per day

Infant Vitamin D Status - Assessed at 2 months of age
Arctic Circle Equator
Geographic Location
Elevation Seaside Mountains
Sun-seeking Behaviors Always outside, frequently in the sun
Never outside
Skin Pigmentation Deep Light
Cultural Dress Diaper onlyMostly covered
Sunscreen Use Never Owned Any Applies to any exposed skin
SUNLIGHT EXPOSURE FACTORS
Weather Long winters Long summers
Diet Exclusively breastfeeding Exclusively formula feeding
Present Diseases assoc. with Vit D Deficiency
Not present
Supplements No supplements 200 IU Vit D per day
DIETARY FACTORS

Counseling Options for Infants
• Diaper only: 10-30 minutes/week• Fully clothed, no hat: 2 hours/week• Increased time may be necessary for babies
with deeper pigmented skin• Take Vitamin D supplement of 200 IU per day• When weaning, use only infant formula to
replace breastfeedings• Vitamin D supplement should be stopped if
infant is consuming 500 ml of formula

Summary“Upsurge” in rickets is real, but the
actual incidence is unknown (esp. subclinical)
Upsurge is due to inadequate sunlight exposure, not dietary deficiency
Safe sun exposure can address the problem
Adequate dietary intake will correct the effect of lack of sunlight exposure
Effective dose is 200 IU starting in first two months