update on systemic therapy for metastatic pancreas adenocarcinoma
TRANSCRIPT

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Update on Systemic Therapy for Metastatic Pancreas Adenocarcinoma
Anne M Noonan MBBChBAO, MSc Assistant Professor

AIMS
To outline the treatment options for first and second line therapies for metastatic pancreas cancer
Review approach to targeted therapies through molecular profiling

Pancreas adenocarcinoma is an aggressive disease 85% are adenocarcinomas arising from ductal epithelium Surgical resection offers the only chance of cure Only 15-20% of patients have resectable disease at
diagnosis Median survival: locally advanced unresectable disease is 8-12 months Metastatic disease – 3 to 6 months
Chemoresistance is a major problem
3
Background

First Line Regimens
4

Single agents – gemcitabine, 5FU, capecitabine and S1 objective response rates of ≈10% median overall survival of 6 to 7 months
Gemcitabine monotherapy (800mg/m2 IV weekly on days 1,8 and 15 of 28 day cycle) is generally now only considered for patients with performance status of ≥2 Response rate of 11% Clinical benefit rate (improvement in pain, PS and weight)
was 27% 5FU – response rate of 0-9% Capecitabine – first line response rate of 7% but CBR of
24%
5
In the past….
Multicenter randomized phase 2-3 trial of 342 patients FOLFIRINOX (oxaliplatin 85mg/m2, irinotecan 180mg/m2,
leucovorin 400mg and 5FU 400mg/m2 given as a bolus followed by 2400mg/m2 given as continuous 46hr intravenous infusion, every 2 weeks)
Versus
Gemcitabine 1000mg/m2 weekly for 7 of 8 weeks and then weekly for 3 of 4 weeks
Objective response rate was 31.6% with FOLFIRINOX and 9.4% with gemcitabine
6
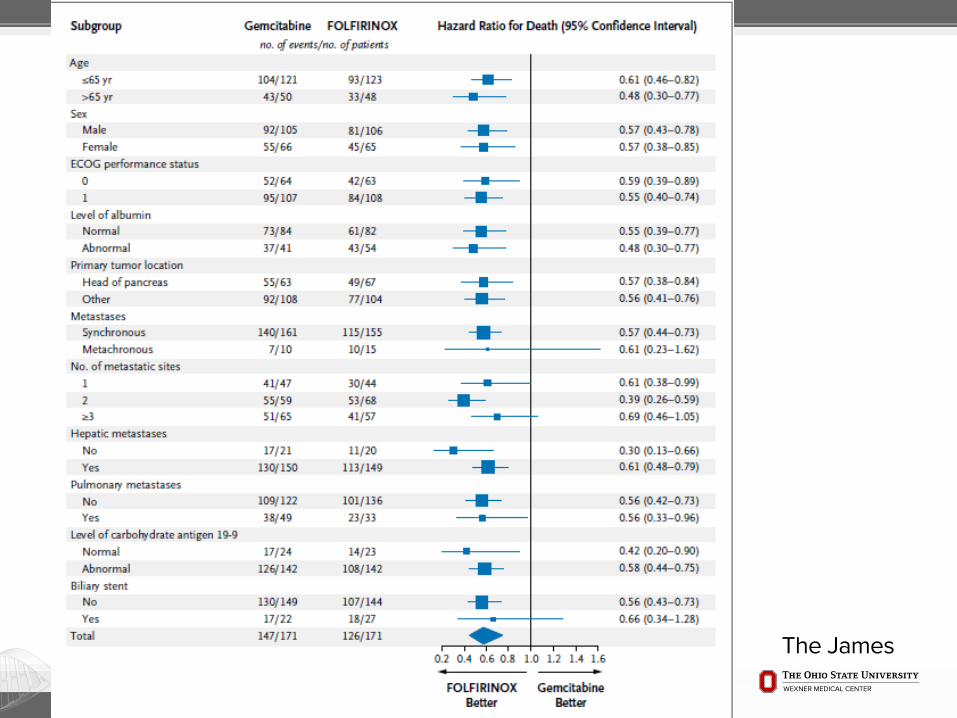
FOLFIRINOX

FOLFIRINOX
Median overall survival was 11.1 months in FOLFIRINOX group and 6.8 months in gemcitabine group
Median progression-free survival was 6.4 months in FOLFIRINOX group and 3.3 months in gemcitabine group


Due to toxicity, FOLFIRINOX is reserved for good performance status patients aged <76
Most clinicians would recommend against giving it to patients >70
In practice, omitting the bolus of 5FU and the leucovorin can improve tolerability
10

Phase III trial of 861 patients Nab-paclitaxel 125mg/m2 followed by gemcitabine
1000mg/m2 on days 1, 8 and 15 every 4 weeks versus Gemcitabine 1000mg/m2 weekly for 7 of 8 weeks then on
days 1,8 and 15 every 4 weeks Response rate was 23% in nab-paclitaxel with
gemcitabine group compared to 7% with gemcitabine alone
Rate of disease control (confirmed response or stable disease for ≥16 weeks) was 48% in nab-paclitaxel plus gemcitabine versus 33% in the gemcitabine alone group
11
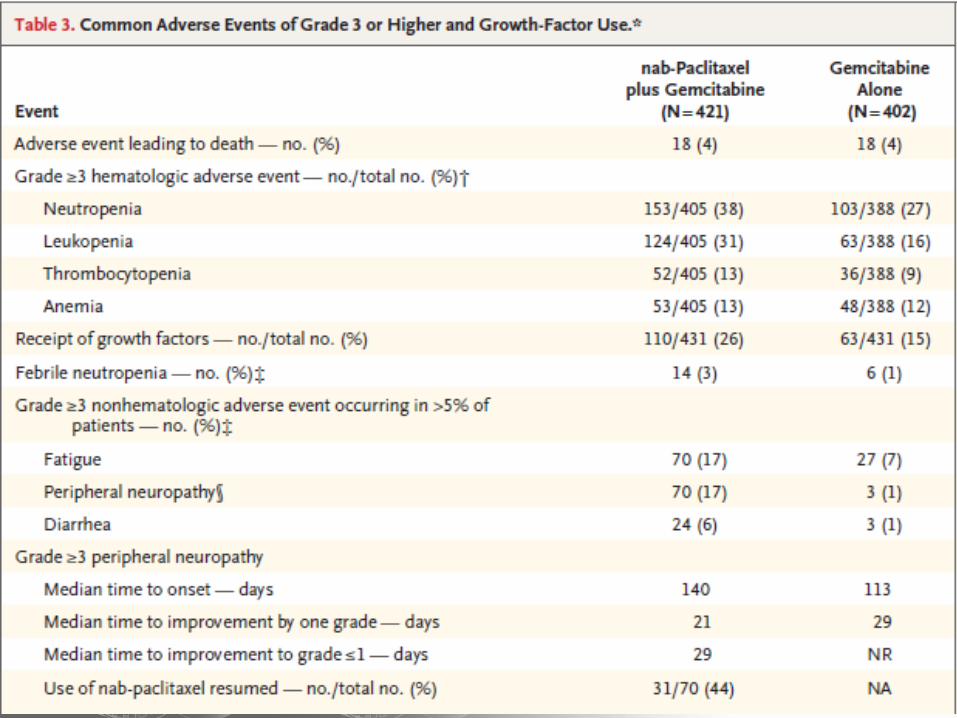
Gemcitabine and Nab-Paclitaxel
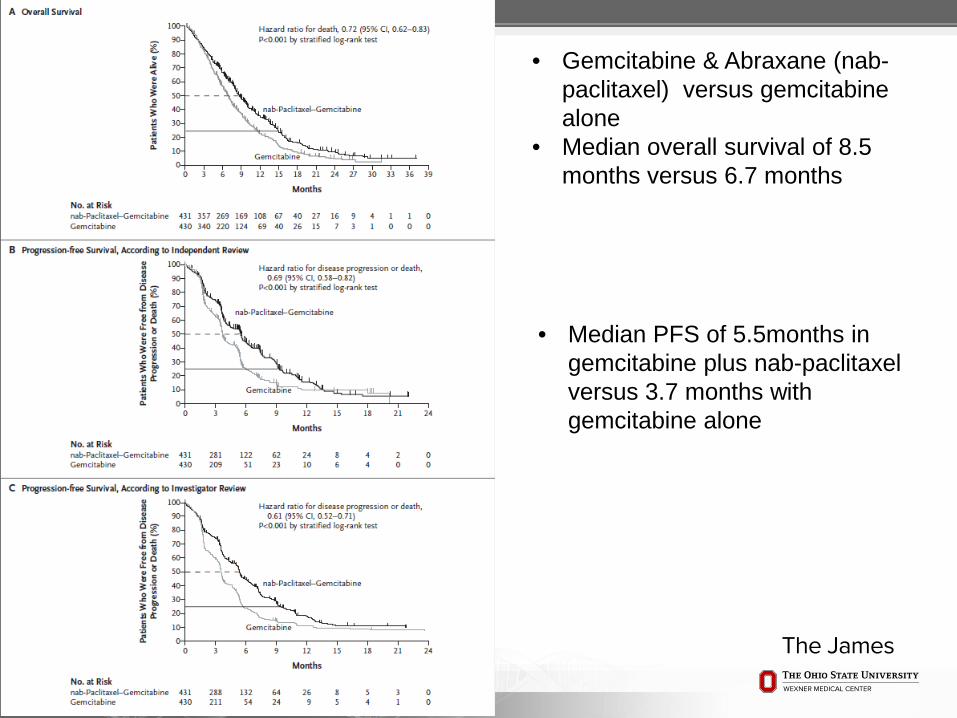
• Gemcitabine & Abraxane (nab-paclitaxel) versus gemcitabine alone
• Median overall survival of 8.5 months versus 6.7 months
• Median PFS of 5.5months in gemcitabine plus nab-paclitaxel versus 3.7 months with gemcitabine alone

Gemcitabine and nab-paclitaxel is a reasonable first line treatment option for patients with metastatic pancreas cancer
Better tolerated than FOLFIRINOX so gemcitabine and nab-paclitaxel is preferred for older patients >70 and patients with ECOG of 2/KPS of 70
14

Second Line Regimens
15

Global randomized phase III trial of 417 patients Previously treated with gemcitabine-based therapy Nanoliposomal irinotecan (Onyvide) (80mg/m2 equivalent
to 70mg/m2 of irinotecan base) with 5FU and leucovorin Compared to 5FU and LV monotherapy or nanoliposomal
irinotecan (120mg/m2 [100mg/m2 irinotecan base]) monotherapy every 3 weeks
Primary endpoint was overall survival 16% of patients assigned nanoliposomal irinotecan with
5FU/LV had an objective response vs 1% in 5FU/LV group and 6% in the nanoliposomal irinotecan monotherapy group
16
Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1)

Kaplan-Meier survival analysesHR=hazard ratio. (A) Overall survival with nanoliposomal irinotecan plus fluorouracil and folinic acid versus fluorouracil and folinic acid. (B) Overall survival with nanoliposomal irinotecan monotherapy versus fluorourauracil and folinic acid. (.
Andrea Wang-Gillam, et al. THE LANCET Volume 387, Issue 10018, 6–12 February 2016, Pages 545–557
Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial
Median OS 6.1 months vs 4.2 months
Median OS 4.9 months vs 4.2 months

(C) Progression-free survival with nanoliposomal irinotecan plus fluorouracil and folinic acid versus fluorouracil and folinic acid. (D) Progression-free survival with nanoliposomal irinotecan monotherapy versus fluorouracil and folinic acid.
Andrea Wang-Gillam, et al. THE LANCET Volume 387, Issue 10018, 6–12 February 2016, Pages 545–557
Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial
Median PFS 3.1 months vs 1.5 months
Median PFS 2.7 months vs 1.6 months

19
Nanoliposomal irinotecan plus fluorouracil and folinic acid combination therapy (n=117)
Nanoliposomal irinotecan monotherapy (n=147)
Fluorouracil and folinic acid control (n=134)
Any grade Grades 3–4 Any grade Grades 3–4 Any grade Grades 3–4
Diarrhea 69 (59%) 15 (13%) 103 (70%) 31 (21%) 35 (26%) 6 (4%)
Vomiting 61 (52%) 13 (11%) 80 (54%) 20 (14%) 35 (26%) 4 (3%)
Nausea 60 (51%) 9 (8%) 89 (61%) 8 (5%) 46 (34%) 4 (3%)
Decreased appetite 52 (44%) 5 (4%) 72 (49%) 13 (19%) 43 (32%) 3 (2%)
Fatigue 47 (40%) 16 (14%) 54 (37%) 9 (6%) 37 (28%) 5 (4%)
Neutropenia* 46 (39%) 32 (27%) 37 (25%) 22 (15%) 7 (5%) 2 (1%)
Anemia 44 (38%) 11 (9%) 48 (33%) 16 (11%) 31 (23%) 9 (7%)
Hypokalemia 14 (12%) 4 (3%) 32 (22%) 17 (12%) 12 (9%) 3 (2%)
5FU and oxaliplatin or capecitabine and oxaliplatin both demonstrated median overall survival of 4.8 to 5.9 months compared to best supportive care 2.3 to 3.3 months)
Capecitabine and erlotinib was tested in a phase II trial of 32 patients 10% response rate median overall survival of 6.5 months but significant diarrhea
20
Other second line regimens after gemcitabine

No randomized data Gemcitabine and nab-paclitaxel Prospective multicenter cohort study of 57 patients Objective response rate of 18% Disease control rate of 58% Median overall survival of 8.8 months Median PFS of 5.1 months
Gemcitabine alone Single agent taxane
21
Second-line agents after FOLFIRINOX

Molecular Profiling and Targeted Therapies
22

Erlotinib is the only targeted agent approved for metastatic pancreas cancer
In a phase III trial of gemcitabine and erlotinib versus gemcitabine alone, overall survival was 6.2 months versus 5.9 months
Gain in survival was statistically significant but the two week improvement in survival is not clinically meaningful
FDA approved but not used in practice
Cetuximab and bevacizumab have also been tested in combination with gemcitabine but no benefit seen
23
Targeted Therapies

4 classes identified Squamous Aberrantly differentiated endocrine
exocrine (ADEX) Pancreatic progenitor Immunogenic
ADEX tumors display upregulation of genes that regulate networks involved in KRAS activation
Targeting of KRAS has not been successful to date
24
Molecular classes and transcriptional networks defining PDAC
P Bailey et al. Nature 1-6 (2016) doi:10.1038/nature16965

25
Immune pathways in PDAC
P Bailey et al. Nature 1-6 (2016) doi:10.1038/nature16965

Clinical Trials at The James
26
27
OSU-14249 A Phase I/II, Two-Part, Multicenter Study to Evaluate the Safety and Efficacy of M402 (necuparanib) in Combination with nab-Paclitaxel and Gemcitabine in Patients with Metastatic Pancreatic Cancer
OSU-14146 A Phase Ib Clinical Study of BBI608 in Combination with Gemcitabine and nab-Paclitaxel in Adult Patients with Metastatic Pancreatic Adenocarcinoma
First line metastatic pancreas trials

28
OSU-14250 A Phase 1, Open-label, Multicenter, Safety Study of Nivolumab (BMS-936558) in Combination with nab-Paclitaxel Plus or Minus Gemcitabine in Pancreatic Cancer
OSU-15169 A Phase 1 Multicenter, Open-label, Dose-escalation and Dose-expansion Study to Evaluate the Safety, Tolerability, Pharmacokinetics, Immunogenicity, and Antitumor Activity of MEDI9447 Alone and in Combination with MEDI4736 in Adult Subjects with Select Advanced Solid Tumors
Second line trials

29
Metastatic pancreas cancer is a challenging disease due to chemoresistance
FOLFIRINOX as first-line therapy is reserved for good performance status patients and <70 years of age
Gemcitabine and nab-paclitaxel is better tolerated and preferred if ECOG PS is 2
Nanoliposomal irinotecan with 5FU/LV is an option for second-line therapy after progression on gemcitabine-based regimens
Molecular profiling to define subtypes and immune-based approaches offer promise for more effective therapies
Conclusions

Thank You To learn more about Ohio State’s cancer program, please visit cancer.osu.edu or
follow us in social media:
30