urinary system - imperial college union · urinary system the kidneys and ... the renal corpuscle...
TRANSCRIPT
Sybghat Rahim
1
Urinary System The Kidneys and Urinary System by Dr Vik Khullar
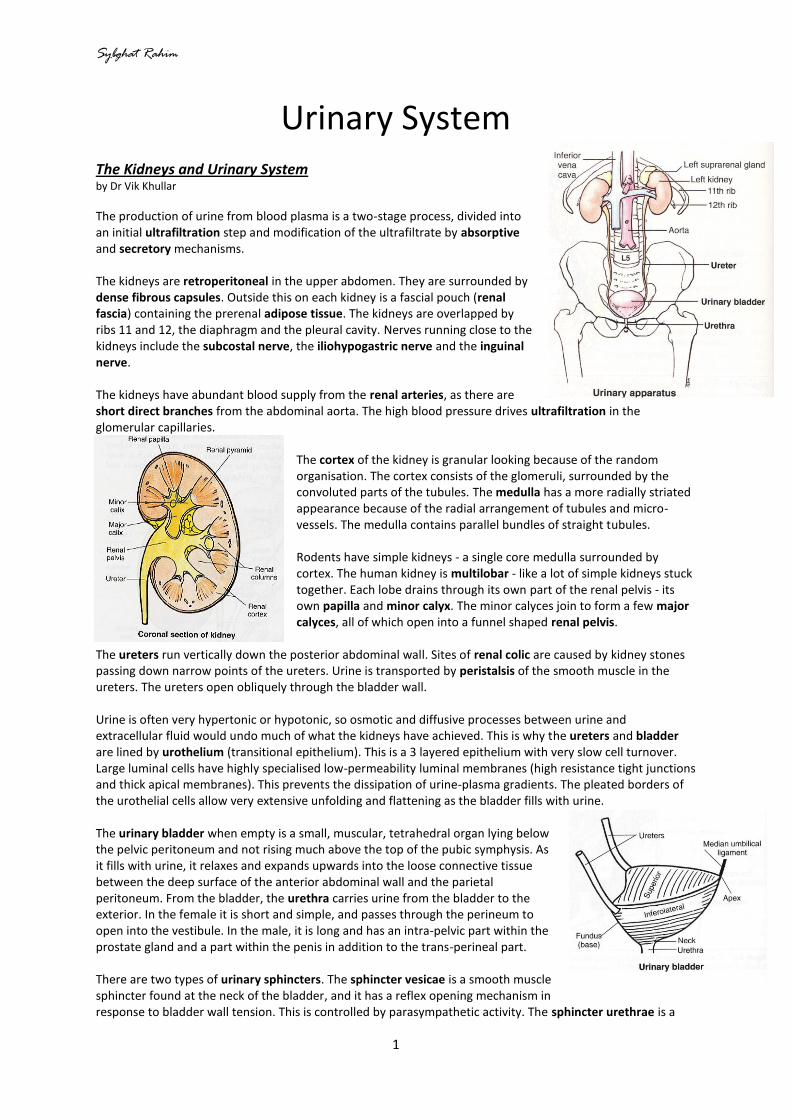
The production of urine from blood plasma is a two-stage process, divided into an initial ultrafiltration step and modification of the ultrafiltrate by absorptive and secretory mechanisms. The kidneys are retroperitoneal in the upper abdomen. They are surrounded by dense fibrous capsules. Outside this on each kidney is a fascial pouch (renal fascia) containing the prerenal adipose tissue. The kidneys are overlapped by ribs 11 and 12, the diaphragm and the pleural cavity. Nerves running close to the kidneys include the subcostal nerve, the iliohypogastric nerve and the inguinal nerve. The kidneys have abundant blood supply from the renal arteries, as there are short direct branches from the abdominal aorta. The high blood pressure drives ultrafiltration in the glomerular capillaries.
The cortex of the kidney is granular looking because of the random organisation. The cortex consists of the glomeruli, surrounded by the convoluted parts of the tubules. The medulla has a more radially striated appearance because of the radial arrangement of tubules and micro-vessels. The medulla contains parallel bundles of straight tubules. Rodents have simple kidneys - a single core medulla surrounded by cortex. The human kidney is multilobar - like a lot of simple kidneys stuck together. Each lobe drains through its own part of the renal pelvis - its own papilla and minor calyx. The minor calyces join to form a few major calyces, all of which open into a funnel shaped renal pelvis.
The ureters run vertically down the posterior abdominal wall. Sites of renal colic are caused by kidney stones passing down narrow points of the ureters. Urine is transported by peristalsis of the smooth muscle in the ureters. The ureters open obliquely through the bladder wall. Urine is often very hypertonic or hypotonic, so osmotic and diffusive processes between urine and extracellular fluid would undo much of what the kidneys have achieved. This is why the ureters and bladder are lined by urothelium (transitional epithelium). This is a 3 layered epithelium with very slow cell turnover. Large luminal cells have highly specialised low-permeability luminal membranes (high resistance tight junctions and thick apical membranes). This prevents the dissipation of urine-plasma gradients. The pleated borders of the urothelial cells allow very extensive unfolding and flattening as the bladder fills with urine. The urinary bladder when empty is a small, muscular, tetrahedral organ lying below the pelvic peritoneum and not rising much above the top of the pubic symphysis. As it fills with urine, it relaxes and expands upwards into the loose connective tissue between the deep surface of the anterior abdominal wall and the parietal peritoneum. From the bladder, the urethra carries urine from the bladder to the exterior. In the female it is short and simple, and passes through the perineum to open into the vestibule. In the male, it is long and has an intra-pelvic part within the prostate gland and a part within the penis in addition to the trans-perineal part. There are two types of urinary sphincters. The sphincter vesicae is a smooth muscle sphincter found at the neck of the bladder, and it has a reflex opening mechanism in response to bladder wall tension. This is controlled by parasympathetic activity. The sphincter urethrae is a

Sybghat Rahim
2
skeletal muscle sphincter found in the perineum. Its tone is maintained by somatic nerves in the pudendal nerve (from S2, 3 and 4). This sphincter is opened by voluntary inhibition of nerves. Sustained closure keeps the sphincter vesicae closed and reduces bladder tone. As the bladder fills it becomes very thin walled. Beyond a certain level of fullness the tension in the bladder wall increases, stimulating receptors that trigger a sacral parasympathetic reflex leading to contraction of the bladder smooth muscle and relaxation of the sphincter vesicae at the junction of bladder and urethra. Ascending pathways make the individual aware of bladder fullness. A decision to empty the bladder (micturate) leads to voluntary relaxation via descending inhibitory pathways that reduce the pudendal nerve’s stimulation of the sphincter urethrae that surrounds the urethra in the perineum. In the absence of a decision to empty the bladder (e.g. if socially inappropriate or during sleep), the urethral sphincter stays closed and this leads to a return to closure of the vesical sphincter and reduction of bladder tone.

Sybghat Rahim
3
The Structural Basis of Kidney Function by Dr Vik Khullar
The function of the kidneys is the production of urine. This is done by filtration of blood plasma. There is selective reabsorption of the contents to be retained, and also tubular secretion of some components, and all this leads to the concentration of urine as necessary. The kidneys are sensitive to body needs via hormones and nerves. The kidneys also have an endocrine function, as they can send signals to the rest of the body via hormones including rennin, erythropoietin, and 1,25-OH Vitamin D. The real job of the kidneys is homeostasis: maintaining the constancy of the internal environment. The kidneys are particularly important in regulating the ions in the bloodstream, and thereby in fact the whole intracellular environment in the body. Looking at the body as a whole, there is always fluid and food going in and faeces and undigested residue coming out. It is important to balance sodium, potassium, pH, bicarbonate, etc and also fluid volume in the body (regulation of osmolarity). Urine has the capability to be produced as large amounts of fluid or small amounts of fluid. The kidney has an interesting structure with clear zones: the cortex (granular appearance, not homogenous structure), and the central medulla (striated areas due to tubules and loops of Henlé). The proximal convolution is in the cortex of the kidney. The loop of Henlé runs down into the medulla. The distal convolution is again in the cortex. The convoluted tubules are doing work, which requires a blood supply for energy. It is efficient having the blood supply in the cortex, which is clearly where the work is done. Ultrafiltration occurs under a high pressure. Blood passing through the glomerulus is filtered, and the filtrate consists of all components that are under 50,000 in molecular weight. The afferent arteriole of the glomerulus is much larger than the efferent vessel. This causes a great build-up of pressure within the glomerulus itself, and it is a high pressure system in the first place because the vessels come straight off the aorta. The filtrate collects in the Bowman’s capsule. The endothelium of the Bowman’s capsule is fenestrated to allow things to pass through. Juxtaglomerular cells sit around the afferent arteriole, where they can sense pressure and secrete renin as necessary to increase blood pressure.

Sybghat Rahim
4
Mechanisms of Urine Production in the Kidney: The renal corpuscle is composed of the Bowman’s capsule, the glomerulus (consists of capillaries) and podocytes associated with the glomerulus. This is where ultrafiltration occurs. In summary, the blood supply is at the vascular pole of the corpuscle from the afferent arteriole, and runs at high pressure in the glomerular capillaries. The filtration barrier consists of fenestrae in the capillary endothelium, as well as a specialised basal lamina, and there are filtration slits between foot processes of podocytes. Filtration allows the passage of ions and molecules less than 50,000 in molecular weight. Reabsorption occurs in the proximal convoluted tubule for material to be retained. This includes ions, glucose, amino acids, small proteins, water, etc. The proximal convoluted tubule is where 70% of glomerular filtrate is reabsorbed. Because lots of energy is requires, mitochondria are present in the cells. There is Na
+
uptake by a basolateral sodium pump. Water and anions follow the sodium ions. The glucose uptake is by a sodium-glucose co-transporter, and amino acid uptake is by a sodium-amino acid co-transporter. Protein uptake is by endocytosis. The structural features of the cells give specialisation for absorption. The cells are in the form of a cuboidal epithelium, sealed with fairly water-permeable tight junctions which stop leakage, and the membrane surface area is increased (by a brush border and interdigitations of the lateral membrane) to maximise the rate of reabsorption. There are also aquaporins (proteins mediating transcellular water diffusion) present on the membranes. An important mechanism is the creation of a hyper-osmotic extracellular fluid. This is the main function of the loop of Henlé, and is a countercurrent mechanism. In the descending thin tubule there is a passive osmotic equilibrium (aquaporins are present) across the simple squamous epithelium. In the ascending thick limb, sodium and chloride are actively pumped out of the tubular fluid, and there are very water-impermeable tight junctions. These membranes lack aquaporins and so there is low permeability to water, which results in a hypo-osmotic tubular fluid and a hyper-osmotic extracellular fluid. The blood vessels are also arranged in a loop, as the blood is in rapid equilibrium with the extracellular fluid. The loop structure stabilises the hyper-osmotic sodium concentration. Another important mechanism is the adjustment of ion content of urine. This is principally a function of the distal convoluted tubule, which controls the levels of Na
+, K
+, H
+ and NH4
+. The distal convoluted tubule
(cortical collecting duct) is the site of osmotic re-equilibration, and is controlled by vasopressin. The adjustment of the ions is controlled by aldosterone. In the collecting duct there are cuboidal epithelia with few microvilli, but complex lateral membrane interdigitations with sodium pumps and numerous large mitochondria. Finally, the concentration of urine occurs at the collecting tubule. This is the movement of water down an osmotic gradient into the extracellular fluid, and is controlled by vasopressin (ADH). The medullary collecting duct passes through the medulla, with its hyper-osmotic extracellular fluid. Water moves down the osmotic gradient to concentrate urine. The rate of water movement depends on aquaporins-2 in the apical membrane, and the content is varied by the exo/endocytosis mechanism and under control from the pituitary hormone vasopressin. The basolateral membrane has aquaporins-3, and is not under control. The duct has simple cuboidal epithelium, but the cell boundaries do not interdigitate. There is little active pumping, so there are fewer mitochondria. Urine drains into the minor calyx at the papilla of the medullary pyramid. The minor and major calyces and pelvis have urinary epithelium. A quick note on the juxtaglomerular apparatus, they have endocrine specialisation and secrete renin to control blood pressure via angiotensin. The juxtaglomerular apparatus senses stretch in the arteriole wall and also senses the concentration of chloride in the tubule. The cellular components are the macula densa of the distal convoluted tubule, and juxtaglomerular cells of the afferent tubule.

Sybghat Rahim
5
Renal Blood Flow and Glomerular Filtration by Dr Michael Emerson
Glomerular filtration is important because kidney failure is defined as a fall in glomerular filtration. To understand kidney failure therefore, the process of glomerular filtration must be understood, and to diagnose kidney failure, the measurement of glomerular filtration must be understood. The basic functions of the kidney include the excretion of metabolic products (urea, uric acid, creatinine, etc) and excretion of foreign substances such as drugs - pharmacokinetics is an integrated function of the kidney. The kidneys are also integral to the homeostasis of body fluids, electrolytes and acid-base balance, as well has having important functions in regulating blood pressure by secreting hormones such as renin. Glomerular filtration is the formation of an ultrafiltrate of plasma in the glomerulus. An abrupt fall in glomerular filtration is renal failure. Abnormalities in renal circulation and urine production lead to reduced glomerular filtration, i.e. renal failure. Glomerular filtration is a passive process, as fluid is driven through the semi-permeable (fenestrated) walls of the glomerular capillaries into the Bowman’s capsule space by the hydrostatic pressure of the heart. The filtration barrier (fenestrated endothelium of capillaries and semi-permeable Bowman’s capsule) is highly permeable to:
- Fluids - Small solutes (these are “freely filtered”, so there is actually the same concentration of solutes in the
filtrate as in the plasma, the only difference is the amounts of solute in each case
The filtration barrier is impermeable to:
- Cells - Proteins - Anything protein-bound
o e.g. Drugs A clear fluid (ultrafiltrate), completely free from blood and proteins, is produced containing electrolytes and small solutes - primary urine.
An important thing to note is that there is one input, being the renal artery, but there are two outputs - either out through the tubule or out through the efferent tubule. Once fluid is in the tubule, different substances are reabsorbed or secreted depending on whether or not they should be retained in the body or excreted. The amount of urine that is excreted depends upon the amount that is filtered, the amount secreted and the amount absorbed:
Amount excreted = amount filtered + amount secreted - amount absorbed
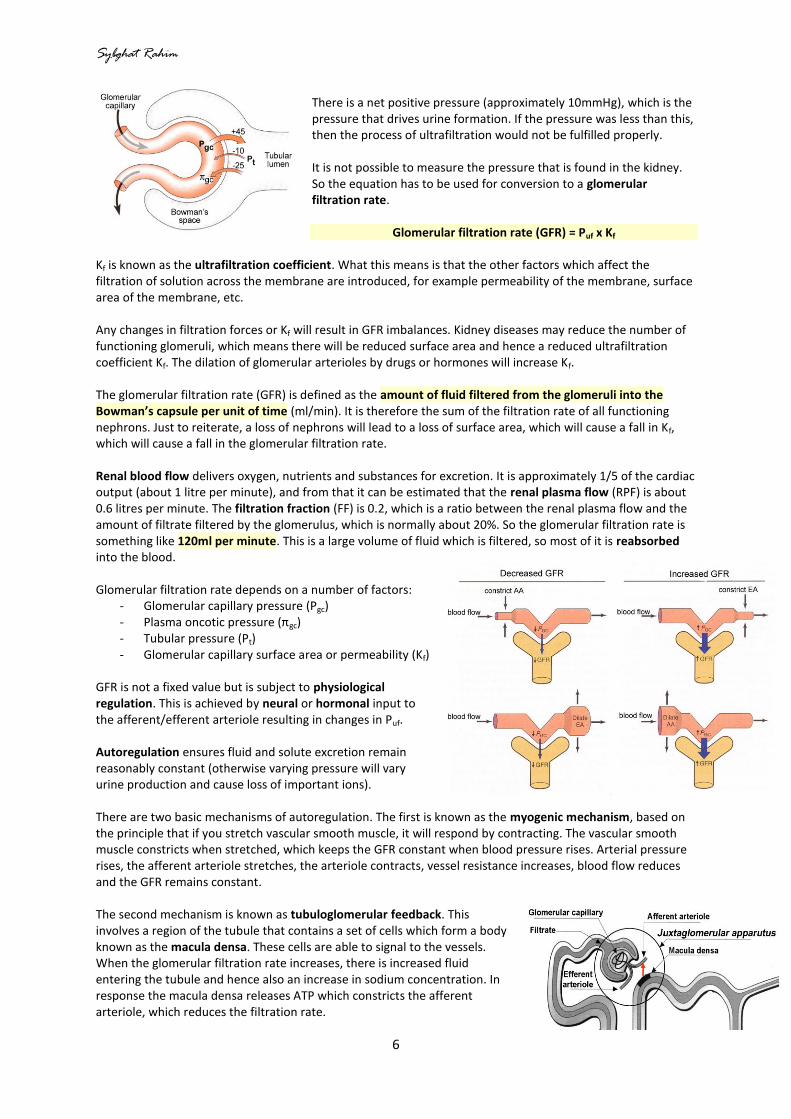
The driving force of glomerular filtration is the hydrostatic pressure in the glomerular capillaries due to blood pressure. The opposing pressures are the hydrostatic pressure of the tubule (Pt) and the osmotic pressure of plasma proteins in the glomerular capillaries (πgc). Together, these determine the net ultrafiltration pressure (Puf). Puf = Pgc - Pt - πgc
Sybghat Rahim
6
There is a net positive pressure (approximately 10mmHg), which is the pressure that drives urine formation. If the pressure was less than this, then the process of ultrafiltration would not be fulfilled properly. It is not possible to measure the pressure that is found in the kidney. So the equation has to be used for conversion to a glomerular filtration rate.
Glomerular filtration rate (GFR) = Puf x Kf Kf is known as the ultrafiltration coefficient. What this means is that the other factors which affect the filtration of solution across the membrane are introduced, for example permeability of the membrane, surface area of the membrane, etc. Any changes in filtration forces or Kf will result in GFR imbalances. Kidney diseases may reduce the number of functioning glomeruli, which means there will be reduced surface area and hence a reduced ultrafiltration coefficient Kf. The dilation of glomerular arterioles by drugs or hormones will increase Kf. The glomerular filtration rate (GFR) is defined as the amount of fluid filtered from the glomeruli into the Bowman’s capsule per unit of time (ml/min). It is therefore the sum of the filtration rate of all functioning nephrons. Just to reiterate, a loss of nephrons will lead to a loss of surface area, which will cause a fall in Kf, which will cause a fall in the glomerular filtration rate. Renal blood flow delivers oxygen, nutrients and substances for excretion. It is approximately 1/5 of the cardiac output (about 1 litre per minute), and from that it can be estimated that the renal plasma flow (RPF) is about 0.6 litres per minute. The filtration fraction (FF) is 0.2, which is a ratio between the renal plasma flow and the amount of filtrate filtered by the glomerulus, which is normally about 20%. So the glomerular filtration rate is something like 120ml per minute. This is a large volume of fluid which is filtered, so most of it is reabsorbed into the blood. Glomerular filtration rate depends on a number of factors:
- Glomerular capillary pressure (Pgc) - Plasma oncotic pressure (πgc) - Tubular pressure (Pt) - Glomerular capillary surface area or permeability (Kf)
GFR is not a fixed value but is subject to physiological regulation. This is achieved by neural or hormonal input to the afferent/efferent arteriole resulting in changes in Puf. Autoregulation ensures fluid and solute excretion remain reasonably constant (otherwise varying pressure will vary urine production and cause loss of important ions). There are two basic mechanisms of autoregulation. The first is known as the myogenic mechanism, based on the principle that if you stretch vascular smooth muscle, it will respond by contracting. The vascular smooth muscle constricts when stretched, which keeps the GFR constant when blood pressure rises. Arterial pressure rises, the afferent arteriole stretches, the arteriole contracts, vessel resistance increases, blood flow reduces and the GFR remains constant. The second mechanism is known as tubuloglomerular feedback. This involves a region of the tubule that contains a set of cells which form a body known as the macula densa. These cells are able to signal to the vessels. When the glomerular filtration rate increases, there is increased fluid entering the tubule and hence also an increase in sodium concentration. In response the macula densa releases ATP which constricts the afferent arteriole, which reduces the filtration rate.

Sybghat Rahim
7
There are certain events that can affect the glomerular filtration rate. For example, severe haemorrhage will reduce the glomerular filtration rate because there would be a reduction in the driving force (hydrostatic pressure of the heart). If there is an obstruction in the nephrons tubule, the glomerular filtration rate will be reduced as there will be an increase in pressure in the tubule itself. If there was a reduced plasma protein concentration, the glomerular filtration rate would increase. And if there was a small increase in blood pressure, the glomerular filtration rate would actually stay the same because of the autoregulation mechanisms such as the myogenic mechanism - only severe conditions of blood pressure would have a significant effect. In a normal carrying out a daily routine, the glomerular filtration rate and renal blood flow will be maintained at 120ml/minute. Quantifying renal function: Renal Clearance As substances in the blood pass through the kidney, they are filtered to different degrees. The extent to which they are removed from the blood is called clearance. Clearance is the number of litres of plasma that are completely cleared of the substance per unit time (measured in ml / min). Defined by the equation:
C = U x V P
Where U = concentration of substance in urine P = concentration of substance in plasma V = rate of urine production
e.g. for Na, suppose P = 145mM, U = 290mM, V = 1ml/min
Of the 120ml per minute in the glomerular filtration rate, only 2ml are cleared of sodium, which means that most of the sodium is reabsorbed into the blood. If a molecule is freely filtered and is neither reabsorbed nor secreted in the nephron, then the amount filtered equals the amount excreted. Thus the glomerular filtration rate can be measured by measuring clearance of this molecule.
One example is inulin. This is a plant polysaccharide that is freely filtered and neither reabsorbed nor secreted. It is not toxic, and is measureable in urine and plasma. Inulin gives a clearance value of 120ml/min which is the glomerular filtration rate for an average adult. It is not, however, found in mammals so to measure clearance it is a complicated process by which it is infused into the patient beforehand, or an endogenous molecule with a similar clearance can be used. Glomerular filtration rate is normally estimated from creatinine clearance in humans. Creatinine is a waste product from creatine in muscle metabolism. The amount of creatinine released is fairly constant, and if renal function is stable, then the amount of creatinine in the urine is stable. Low values of creatinine clearance may indicate renal failure. High values of creatinine may indicate renal failure.
Renal plasma flow is measured by PAH (para-aminohippurate) clearance, which is about 625ml/min. PAH is filtered and is actively secreted in one pass of the kidney, and thus can be used to measure renal plasma flow. In other words, all of the PAH is removed from the plasma passing through the kidney so its clearance equals the renal plasma flow.
The amount of substance appearing in the urine reflects the combined effects of filtration, reabsorption from the nephron tubule to the blood and secretion from the blood into the tubular fluid. A fall in GFR is the cardinal feature of renal disease. If GFR falls, excretory products will build up in the plasma. A raised concentration of creatinine is diagnostic of renal disease. Excretion of many other substances (e.g. drugs) will also be impaired in renal failure. This needs to be taken into account when calculating drug doses: pharmacokinetics.

Sybghat Rahim
8
Basic Tubular Function by Dr Paul Kemp
The kidney is a central regulator of homeostasis. On an average day we consume 20 to 25% more water and salt than we need to replace that which is lost. This is a buffer which allows us to survive in hot weather (sweat) and overcome illnesses like diarrhoea. We do need to lose the excess water and salt, and other waste products (e.g. urea). In an ideal situation, excess sodium, potassium, other ions, excess water and waste products would all pass straight through in glomerular filtration and be excreted. But this is not the case. We produce urine by passive filtration, through a molecular sieve (glomerular filtration). But we can’t afford to lose all of the water and small molecules that pass through the filter. Controlled reabsorption and secretion ensure that we get rid of the waste and keep the good stuff. We need to reabsorb 99% of ultrafiltrate, and need to maintain a solute balance, plasma concentration and pH. Osmolarity is a measure of the osmotic pressure exerted by a solution across a perfect semi-permeable membrane. It is dependent on the number of particles in a solution and not the nature of the particles. Osmolarity is all the concentration of the different solutes (measured in mmol/l) added together. Each ion is “counted” separately. Normal plasma osmolarity is between 285 and 295mosmol/l (fairly constant). Normal urine osmolarity can range between 50 to 1200mosmol/l (very varied). It is important to bear in mind that any solute present at equal concentrations either side of a semi-permeable membrane can have no net effect on water movement. The renal tubular wall is a single layer of epithelial cells, with basolateral and luminal membranes. The junctions are not completely tight, as there are proteins present which allow e.g. water and other substances to pass through. Solutes can pass through the cells (transcellular) or between the cells (paracellular). This depends on whether or not there are proteins present to allow this movement, and also for the transcellular path whether the solute can dissolve in the membrane. The types of transport are osmosis through semi-permeable membrane, active transport dependent on energy, facilitated diffusion by co-transporters and diffusion and movement down electrochemical gradients. Passive movement includes protein independent transport (lipophilic molecules) as well as protein dependent transport (hydrophilic molecules, saturation kinetics shown). Active movement is dependent on cellular energy. This can be either by being directly coupled to ATP hydrolysis, or indirectly coupled to ATP hydrolysis by a sodium-potassium pump. Water moves by osmosis, moving through proteins (aquaporins in the membrane). Regulation of a passive uptake system is by storing the proteins that allow components through the cell somewhere, and then fusing them with the membrane when they are needed. Proteins are reabsorbed in the kidneys. Lots of low molecular weight proteins pass through the glomerular filtration system, and need to be reabsorbed (e.g. insulin). They bind to low affinity but high capacity receptors that sit in the membrane. Those are then taken into the cell via the endocytic pathway. Ions are then pumped into this endosome to produce a lysosome which contains the protein to be broken down. There is then a recycling endosome that takes the receptor back to the membrane so the system can go through again. Transport maxima are the points at which the rate of uptake levels out graphically. They don’t just apply to individual cells, but actually apply to the whole system. Transport maxima are rarely exceeded, as this can lead to diabetes mellitus and ingestion of large quantities of vitamins B and C.
Sybghat Rahim
9
Once inside the lumen of the nephron, small molecules, such as ions, glucose and amino-acids, are reabsorbed from the filtrate. Specialised proteins called transporters are located on the membranes of the various cells of the nephron. These transporters trap the molecules as they flow by them. Each transporter traps only one or two types of molecule. For example, glucose is reabsorbed by a transporter that also traps sodium. Water gets reabsorbed passively by osmosis in response to build up of sodium in intercellular spaces. Some transporters require energy, usually in the form of ATP (active transport), while others do not (passive transport). Transporters are located in different parts of the nephron. Most of the sodium transporters are located in the proximal tubule, while fewer are spread out through other segments. Secretion moves substances from peritubular capillaries into the tubular lumen. Like filtration, this constitutes a pathway into the tubule. Secretion can occur by diffusion or by transcellular mediated transport. The most important substances secreted are H
+ and K
+. Choline, creatinine, penicillin and other drugs are also secreted.
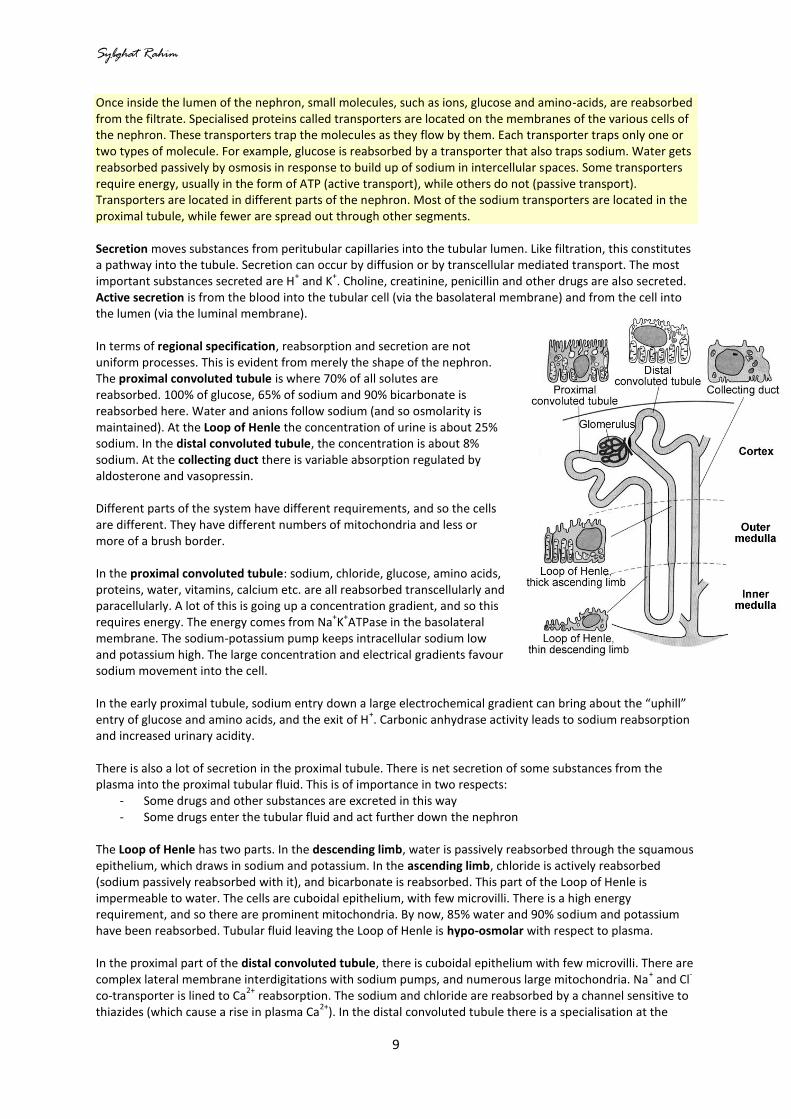
Active secretion is from the blood into the tubular cell (via the basolateral membrane) and from the cell into the lumen (via the luminal membrane). In terms of regional specification, reabsorption and secretion are not uniform processes. This is evident from merely the shape of the nephron. The proximal convoluted tubule is where 70% of all solutes are reabsorbed. 100% of glucose, 65% of sodium and 90% bicarbonate is reabsorbed here. Water and anions follow sodium (and so osmolarity is maintained). At the Loop of Henle the concentration of urine is about 25% sodium. In the distal convoluted tubule, the concentration is about 8% sodium. At the collecting duct there is variable absorption regulated by aldosterone and vasopressin. Different parts of the system have different requirements, and so the cells are different. They have different numbers of mitochondria and less or more of a brush border. In the proximal convoluted tubule: sodium, chloride, glucose, amino acids, proteins, water, vitamins, calcium etc. are all reabsorbed transcellularly and paracellularly. A lot of this is going up a concentration gradient, and so this requires energy. The energy comes from Na
+K
+ATPase in the basolateral
membrane. The sodium-potassium pump keeps intracellular sodium low and potassium high. The large concentration and electrical gradients favour sodium movement into the cell. In the early proximal tubule, sodium entry down a large electrochemical gradient can bring about the “uphill” entry of glucose and amino acids, and the exit of H
+. Carbonic anhydrase activity leads to sodium reabsorption
and increased urinary acidity. There is also a lot of secretion in the proximal tubule. There is net secretion of some substances from the plasma into the proximal tubular fluid. This is of importance in two respects:
- Some drugs and other substances are excreted in this way - Some drugs enter the tubular fluid and act further down the nephron
The Loop of Henle has two parts. In the descending limb, water is passively reabsorbed through the squamous epithelium, which draws in sodium and potassium. In the ascending limb, chloride is actively reabsorbed (sodium passively reabsorbed with it), and bicarbonate is reabsorbed. This part of the Loop of Henle is impermeable to water. The cells are cuboidal epithelium, with few microvilli. There is a high energy requirement, and so there are prominent mitochondria. By now, 85% water and 90% sodium and potassium have been reabsorbed. Tubular fluid leaving the Loop of Henle is hypo-osmolar with respect to plasma. In the proximal part of the distal convoluted tubule, there is cuboidal epithelium with few microvilli. There are complex lateral membrane interdigitations with sodium pumps, and numerous large mitochondria. Na
+ and Cl
-
co-transporter is lined to Ca2+
reabsorption. The sodium and chloride are reabsorbed by a channel sensitive to thiazides (which cause a rise in plasma Ca
2+). In the distal convoluted tubule there is a specialisation at the

Sybghat Rahim
10
macula densa, part of the juxtaglomerular apparatus, which detects changes in sodium concentration of filtrate. The distal part of the distal convoluted tubule and cortical collecting duct are involved in the “fine tuning” of the filtrate to maintain homeostasis. In the distal convoluted tubule, sodium is reabsorbed (dependent on aldosterone). In the collecting duct, sodium is also reabsorbed (dependent on aldosterone). There is also the adjustment of sodium, potassium, proton and ammonium concentrations. Water is reabsorbed under the control of ADH. The distal part of the nephron is impermeable to water without ADH. The cortical collecting duct involves:
- an apical sodium channel sensitive to aldosterone - a linked potassium channel - pH control
Principal cells are important in sodium, potassium and water balance (mediated via Na/K pump). Intercalated cells are important in acid-base balance (mediated via H
+-ATP pump). Principal cells have very tight epithelium,
and so there is very little paracellular transport, unless there is influence by vasopressin. Single gene defects that affect tubular function Renal tubule acidosis: hyperchoremic metabolic acidosis, impaired growth and hypokalaemia. The mechanisms underlying the main types of defects in distal renal tubular acidosis are secretory defects where there is a failure of H
+ ion secretion even when conditions are favourable for its secretion.
Bartter syndrome: excessive electrolyte secretion. Antenatal Bartter syndrome leads to premature birth and polyhydramnios. There is severe salt loss, moderate metabolic acidosis, hypokalaemia and renin and aldosterone hypersecretion. Fanconi syndrome: increased excretion of low molecular weight proteins and increased excretion of uric acid and glucose phosphate.
Sybghat Rahim
11
Water Balance by Dr Paul Kemp
Osmolarity is a measure of the solute concentration in a solution (osmoles/litre). 1 osmole is 1 mole of dissolved solutes per litre. It depends on the number of dissolved solutes present. The greater the number of dissolved particles, the greater the osmolarity. Water flows across a semi-permeable membrane from a region of low osmolarity to a region of high osmolarity. Considering an impermeable membrane, the regulation of water and salt balance are inter-related as osmolarity is variable. Increased salt and/or decreased water will lead to increased osmolarity. Decreased salt and/or increased water will lead to a decreased osmolarity. In a semi-permeable membrane, however, increasing salt and water increases volume, and decreasing salt and water decreases volume, but in both of these cases the osmolarity is unchanged. On an average day we consume 20 to 25% more water and salt than we need to replace that lost.
- It is important to get rid of the excess volume, or this will result in oedema and blood pressure will increase.
- It is important to get rid of any excess water, or salt in the body will become diluted and cells will swell up and be at risk of lysis.
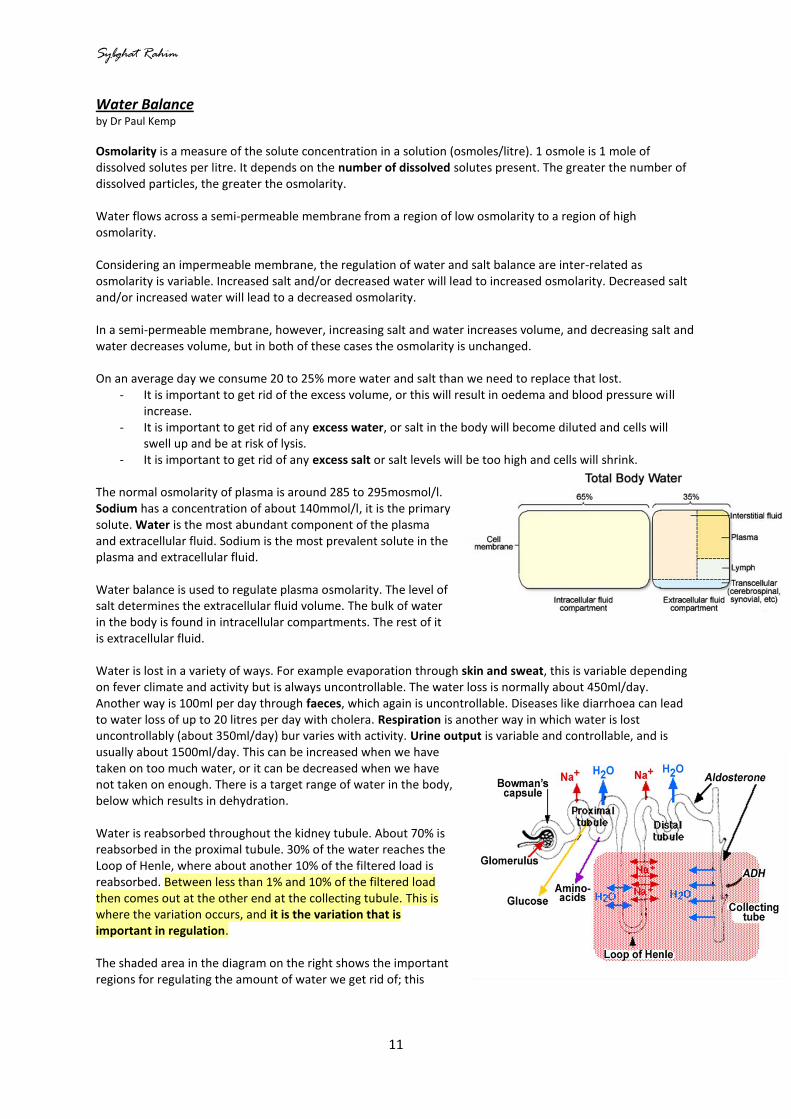
- It is important to get rid of any excess salt or salt levels will be too high and cells will shrink. The normal osmolarity of plasma is around 285 to 295mosmol/l. Sodium has a concentration of about 140mmol/l, it is the primary solute. Water is the most abundant component of the plasma and extracellular fluid. Sodium is the most prevalent solute in the plasma and extracellular fluid. Water balance is used to regulate plasma osmolarity. The level of salt determines the extracellular fluid volume. The bulk of water in the body is found in intracellular compartments. The rest of it is extracellular fluid. Water is lost in a variety of ways. For example evaporation through skin and sweat, this is variable depending on fever climate and activity but is always uncontrollable. The water loss is normally about 450ml/day. Another way is 100ml per day through faeces, which again is uncontrollable. Diseases like diarrhoea can lead to water loss of up to 20 litres per day with cholera. Respiration is another way in which water is lost uncontrollably (about 350ml/day) bur varies with activity. Urine output is variable and controllable, and is usually about 1500ml/day. This can be increased when we have taken on too much water, or it can be decreased when we have not taken on enough. There is a target range of water in the body, below which results in dehydration. Water is reabsorbed throughout the kidney tubule. About 70% is reabsorbed in the proximal tubule. 30% of the water reaches the Loop of Henle, where about another 10% of the filtered load is reabsorbed. Between less than 1% and 10% of the filtered load then comes out at the other end at the collecting tubule. This is where the variation occurs, and it is the variation that is important in regulation. The shaded area in the diagram on the right shows the important regions for regulating the amount of water we get rid of; this
Sybghat Rahim
12
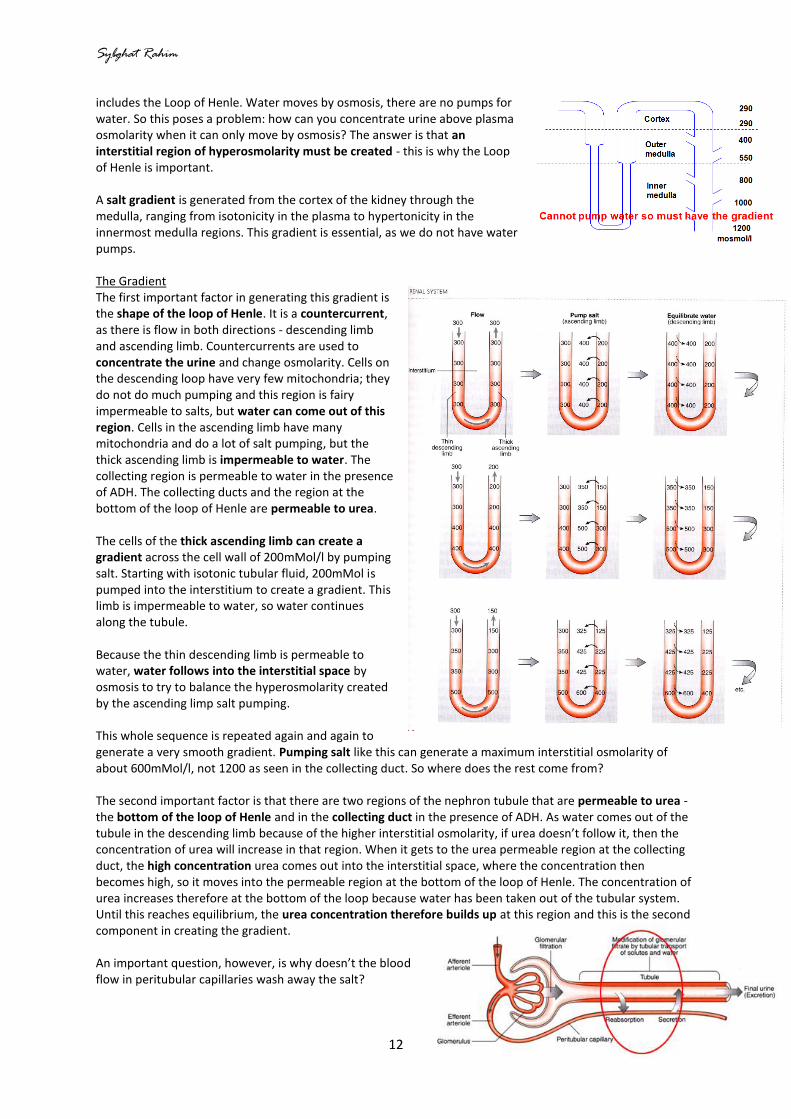
includes the Loop of Henle. Water moves by osmosis, there are no pumps for water. So this poses a problem: how can you concentrate urine above plasma osmolarity when it can only move by osmosis? The answer is that an interstitial region of hyperosmolarity must be created - this is why the Loop of Henle is important. A salt gradient is generated from the cortex of the kidney through the medulla, ranging from isotonicity in the plasma to hypertonicity in the innermost medulla regions. This gradient is essential, as we do not have water pumps. The Gradient The first important factor in generating this gradient is the shape of the loop of Henle. It is a countercurrent, as there is flow in both directions - descending limb and ascending limb. Countercurrents are used to concentrate the urine and change osmolarity. Cells on the descending loop have very few mitochondria; they do not do much pumping and this region is fairy impermeable to salts, but water can come out of this region. Cells in the ascending limb have many mitochondria and do a lot of salt pumping, but the thick ascending limb is impermeable to water. The collecting region is permeable to water in the presence of ADH. The collecting ducts and the region at the bottom of the loop of Henle are permeable to urea. The cells of the thick ascending limb can create a gradient across the cell wall of 200mMol/l by pumping salt. Starting with isotonic tubular fluid, 200mMol is pumped into the interstitium to create a gradient. This limb is impermeable to water, so water continues along the tubule. Because the thin descending limb is permeable to water, water follows into the interstitial space by osmosis to try to balance the hyperosmolarity created by the ascending limp salt pumping. This whole sequence is repeated again and again to generate a very smooth gradient. Pumping salt like this can generate a maximum interstitial osmolarity of about 600mMol/l, not 1200 as seen in the collecting duct. So where does the rest come from? The second important factor is that there are two regions of the nephron tubule that are permeable to urea - the bottom of the loop of Henle and in the collecting duct in the presence of ADH. As water comes out of the tubule in the descending limb because of the higher interstitial osmolarity, if urea doesn’t follow it, then the concentration of urea will increase in that region. When it gets to the urea permeable region at the collecting duct, the high concentration urea comes out into the interstitial space, where the concentration then becomes high, so it moves into the permeable region at the bottom of the loop of Henle. The concentration of urea increases therefore at the bottom of the loop because water has been taken out of the tubular system. Until this reaches equilibrium, the urea concentration therefore builds up at this region and this is the second component in creating the gradient. An important question, however, is why doesn’t the blood flow in peritubular capillaries wash away the salt?
Sybghat Rahim
13
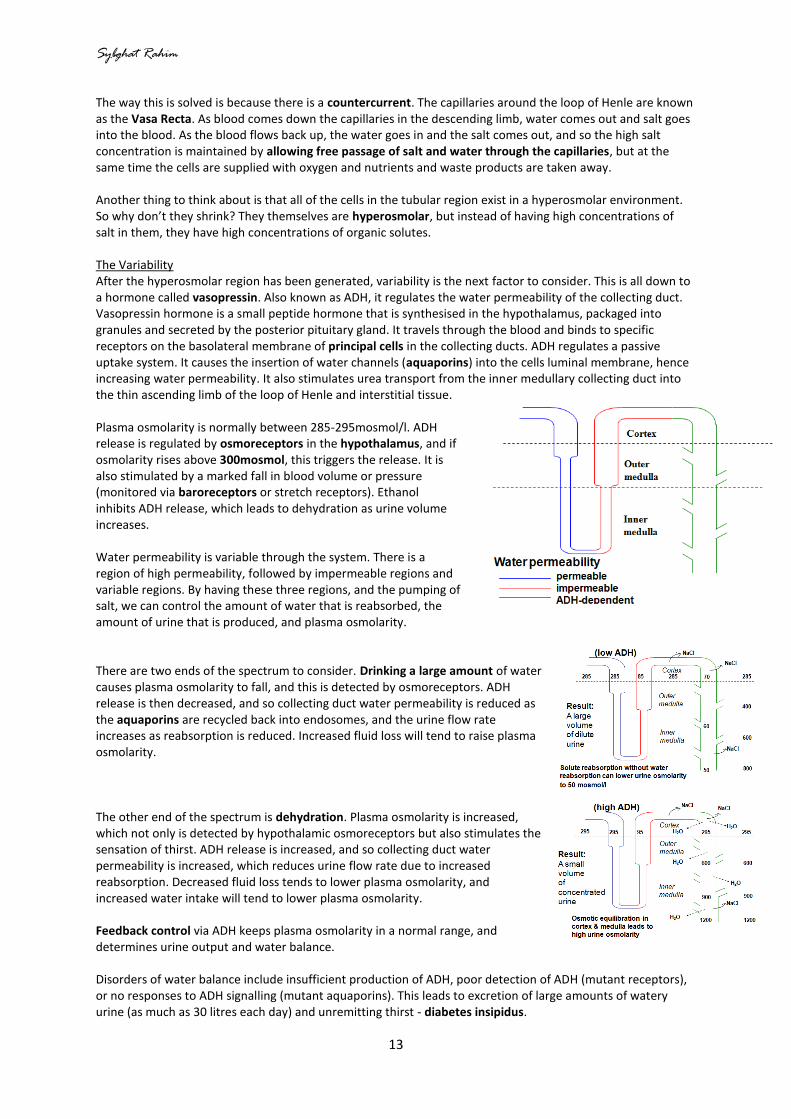
The way this is solved is because there is a countercurrent. The capillaries around the loop of Henle are known as the Vasa Recta. As blood comes down the capillaries in the descending limb, water comes out and salt goes into the blood. As the blood flows back up, the water goes in and the salt comes out, and so the high salt concentration is maintained by allowing free passage of salt and water through the capillaries, but at the same time the cells are supplied with oxygen and nutrients and waste products are taken away. Another thing to think about is that all of the cells in the tubular region exist in a hyperosmolar environment. So why don’t they shrink? They themselves are hyperosmolar, but instead of having high concentrations of salt in them, they have high concentrations of organic solutes. The Variability After the hyperosmolar region has been generated, variability is the next factor to consider. This is all down to a hormone called vasopressin. Also known as ADH, it regulates the water permeability of the collecting duct. Vasopressin hormone is a small peptide hormone that is synthesised in the hypothalamus, packaged into granules and secreted by the posterior pituitary gland. It travels through the blood and binds to specific receptors on the basolateral membrane of principal cells in the collecting ducts. ADH regulates a passive uptake system. It causes the insertion of water channels (aquaporins) into the cells luminal membrane, hence increasing water permeability. It also stimulates urea transport from the inner medullary collecting duct into the thin ascending limb of the loop of Henle and interstitial tissue. Plasma osmolarity is normally between 285-295mosmol/l. ADH release is regulated by osmoreceptors in the hypothalamus, and if osmolarity rises above 300mosmol, this triggers the release. It is also stimulated by a marked fall in blood volume or pressure (monitored via baroreceptors or stretch receptors). Ethanol inhibits ADH release, which leads to dehydration as urine volume increases. Water permeability is variable through the system. There is a region of high permeability, followed by impermeable regions and variable regions. By having these three regions, and the pumping of salt, we can control the amount of water that is reabsorbed, the amount of urine that is produced, and plasma osmolarity. There are two ends of the spectrum to consider. Drinking a large amount of water causes plasma osmolarity to fall, and this is detected by osmoreceptors. ADH release is then decreased, and so collecting duct water permeability is reduced as the aquaporins are recycled back into endosomes, and the urine flow rate increases as reabsorption is reduced. Increased fluid loss will tend to raise plasma osmolarity. The other end of the spectrum is dehydration. Plasma osmolarity is increased, which not only is detected by hypothalamic osmoreceptors but also stimulates the sensation of thirst. ADH release is increased, and so collecting duct water permeability is increased, which reduces urine flow rate due to increased reabsorption. Decreased fluid loss tends to lower plasma osmolarity, and increased water intake will tend to lower plasma osmolarity. Feedback control via ADH keeps plasma osmolarity in a normal range, and determines urine output and water balance. Disorders of water balance include insufficient production of ADH, poor detection of ADH (mutant receptors), or no responses to ADH signalling (mutant aquaporins). This leads to excretion of large amounts of watery urine (as much as 30 litres each day) and unremitting thirst - diabetes insipidus.

Sybghat Rahim
14
Sodium and Potassium Balance by Dr Paul Kemp
Osmolarity is a measure of the solute concentration in a solution, and depends on the number of dissolved solutes present in a solution. The greater the number of dissolved particles, the greater the osmolarity. Across a semi-permeable membrane, the regulation of water and salt balance are inter-related to keep a constant osmolarity. Increased salt means water has to be increased, which leads to just an increased volume, and similarly decreased salt and decreased water lead to only decreased volume - the osmolarity is kept constant. Sodium is the most prevalent and important solute in extracellular fluid. A high sodium diet will lead to an increase in weight, as the body takes on more water to balance out the osmolarity. Increased dietary sodium should lead to increased osmolarity, but the body won’t let this happen. Therefore the body takes on more water to increase the extracellular volume, and so this increases blood volume and pressure and also weight. Decreased dietary sodium leads to a decreased osmolarity, but again the body can’t let this happen. There is therefore a decrease in extracellular volume and a decrease in blood volume and pressure. The important issues to address therefore are:
- How sodium excretion is balanced with dietary intake - How sodium excretion is increased in times of excess - How sodium excretion is reduced in times of low sodium levels
The first thing to consider is where sodium is reabsorbed in the nephron. Like most other solutes, it is mainly in the proximal convoluted tubule. 65% of sodium is reabsorbed in the proximal tubule, about 25% is reabsorbed in the loop of Henle, about 8% in the distal tubule and up to 2% in the collecting ducts. Because the filtered load may change, there is some regulation in the proximal convoluted tubule. This needs to be so because if our glomerular filtration rate changes, this can lead to a large change in sodium excretion, which would cause the associated changes in blood volume and pressure. As the glomerular filtration rate increases, the amount of sodium reabsorption in the proximal convoluted tubule is also increased. The reason for this is that a lot of sodium is reabsorbed with other things, such as glucose and amino acids in co-transport mechanisms. As GFR drops, the reverse happens. Another feature is that as GFR increases, the amount of protein that gets through the oncotic pressure in the proximal convoluted tubule increases, and this forces more sodium through the paracellular walls. Regulation of Sodium Excretion and Reabsorption When things are not so constant, there are a range of mechanisms to regulate sodium excretion and reabsorption. Firstly, the amount of sodium being reabsorbed responds to sympathetic nervous activity. An increase in sympathetic drive causes vasoconstriction in the afferent arteriole, which reduces the glomerular filtration rate. Also, sympathetic activity directly regulates sodium uptake in the proximal convoluted tubule and stimulates the cells in the juxtaglomerular apparatus to secrete renin, which regulates angiotensin, which regulates sodium uptake in the proximal tubule and regulates the production of aldosterone. Aldosterone regulates sodium uptake in the distal convoluted tubule. These mechanisms increase sodium reabsorption.

Sybghat Rahim
15
The other side of the coin which decreases sodium reabsorption is the production of atrial naturietic peptide, which reduces sodium uptake in the proximal tubule and in the medullary region of the collecting duct. It is also a potent vasodilator, affecting mainly the efferent arteriole which decreases perfusion pressure which decreases GFR. These combined factors reduce sodium reabsorption. In the distal nephron, there are cells (the macula densa) which sense when there is very little sodium. When there is sodium present, the cells suppress the production of renin. Renin is an enzyme that cleaves angiotensinogen into angiotensin I, which is then converted to angiotensin II by ACE, and this stimulates the release of aldosterone. This is another multi organ system that is involved in regulating blood pressure and Na
+ excretion, as renin is produced in the
juxtaglomerular apparatus but acts in the blood stream on angiotensinogen produced in the liver. The angiotensin I produced is then activated by ACE predominantly from the lungs to generate angiotensin II which acts on the blood vessels and adrenal gland causing vasoconstriction and release of aldosterone respectively. Low blood pressure, low fluid volume and sympathetic activity all stimulate renin release, as well as a low salt concentration. The effect of angiotensin II in the vascular system is vasoconstriction which increases blood pressure. In the proximal tubule angiotensin II increases sodium uptake, which increases water reabsorption which increases extracellular fluid which increases blood pressure. In the adrenal gland it stimulates aldosterone synthesis. Aldosterone Aldosterone is a steroid hormone synthesised and released from the adrenal cortex. It is released in response to angiotensin II, a decrease in blood pressure or a decreased osmolarity of ultrafiltrate. Aldosterone stimulates sodium reabsorption by activating sodium channels in the distal tubule and collecting duct. As well as increased sodium reabsorption, it stimulates increased potassium secretion and hydrogen ion secretion. Aldosterone excess leads to hypokalaemic alkalosis. Aldosterone stimulates the production of Na
+K
+ATPase and it stimulates the expression of apical sodium
channels of the collecting duct as well as the proteins that regulate the channels. It does all this with transcription factors for the corresponding mRNA. There are diseases of aldosterone secretion, for example hypoaldosteronism. Reabsorption of sodium in the distal nephron is reduced, urinary loss of sodium is increased, extracellular volume falls and there is increased renin, angiotensin II and ADH. This leads to symptoms of dizziness, low BP, salt craving and palpitations. Hyperaldosteronism increases sodium reabsorption in the distal nephron, reduces urinary loss of sodium, increases extracellular fluid volume (hypertension), reduces renin, angiotensin II and ADH. This results in high blood pressure, muscle weakness, polyuria and thirst. Liddle’s syndrome is an inherited disease of high blood pressure. It is a mutation in the aldosterone activated sodium channel - the channel is always on, which results in sodium retention leading to hypertension. Effects of Blood Volume and Pressure Baroreceptors on the low pressure and high pressure sides measure stretch of vessels. On the low pressure side, there are baroreceptors that measure pressure in the atria, the right ventricle, and the pulmonary vasculature. On the high pressure side, there are baroreceptors in the carotid sinus, aortic arch and juxtaglomerular apparatus.

Sybghat Rahim
16
ANP stands for Atrial Natriuretic Peptide, which is a small peptide made in the atria. It is released in response to atrial stretch (i.e. high blood pressure). It causes vasodilation of renal blood vessels, and inhibition of sodium reabsorption in the proximal tubule and in the collecting ducts. It also inhibits the release of renin and aldosterone, and reduces blood pressure.
Sodium levels determine the extracellular fluid volume. Reducing extracellular fluid volume reduces blood pressure. This is why regulation of salt and water balance are inter-related. Reducing sodium reabsorption reduces total sodium levels, extracellular fluid volume and blood pressure. Effect of Drugs ACE inhibitors lower blood pressure by stopping the conversion of angiotensin I to angiotensin II. The effects of the consequent reduction in angiotensin II and aldosterone levels are not just confined to the kidney though. Diuretic drugs can be confined to the kidney, and these include osmotic diuretics, which increase the osmolarity in the tubular system and so allow less water and sodium to exit via the paracellular routes. There are also carbonic anhydrase inhibitors, loop diuretics, thiazides and potassium sparing diuretics. Different diuretics regulate sodium and water reabsorption in different parts of the kidney. Carbonic anhydrase inhibitors prevent the production of protons and block pumps in the proximal convoluted tubule. Loop diuretics such as furosemide block sodium channels (e.g. the triple transporter) in the ascending loop of Henle. Thiazides work in the distal convoluted tubule cells. They are potassium sparing diuretics because they block the potassium/chloride co-transporters, which leads to a change in calcium uptake because less sodium is taken in. Potassium Regulation The other significant cation is potassium, which is our main intracellular ion. The extracellular levels are kept very low, and this allows membrane potentials to form, which allows muscles to contract and nerves to function. Both low and high potassium levels can lead to arrhythmias. Our diets are quite high in potassium, but the extracellular levels must be kept low. As K
+ is absorbed, plasma
concentration increases. The potassium is then taken up into cells to maintain the low extracellular concentration, and fortunately this is regulated by insulin, which is released after a meal. It is also influenced by aldosterone and adrenaline. The immediate response to dietary potassium is for it to be pumped into cells via Na
+K
+ATPase. Over time it then equilibrates out and it is excreted as appropriate via the kidneys. To start
with it is reabsorbed in the proximal tubule, and about 30% is present in the loop of Henle, and 10% reaches the distal tubule. However, the output at the collecting ducts ranges between 1 and 80% of what goes in to the tubular system. This variation is stimulated by plasma potassium levels, aldosterone levels, tubular flow rate, and plasma pH. There are three basic mechanisms by which potassium secretion by principal cells is regulated. The first is

Sybghat Rahim
17
Na+K
+ATPase activity, the second is the permeability of potassium channels (aldosterone), and the third is
tubular flow (flow sensors primary cilium are linked to potassium channel). Hypokalaemia is one of the most common electrolyte imbalances, it is seen in up to 20% of hospitalised imbalances. It is partly to do with diuretics (due to increased tubular flow rates), surreptitious vomiting, diarrhoea and genetics (e.g. Gitelman’s syndrome; mutation in the Na/Cl transporter in the distal nephron). Hyperkalaemia is a common electrolyte imbalance present in 1 to 10% of hospitalised patients. It is seen in response to potassium sparing diuretics, ACE inhibitors and in the elderly.

Sybghat Rahim
18
Mechanisms of Acid-Base Balance by Dr Daqing Ma
Acid: a substance that can release hydrogen ions in solution. Base: a substance that can accept hydrogen ions in solution. Buffer: addition or removal of hydrogen ions resulting in minimal changes to pH. pH: measures hydrogen ion concentration and indicates acidity of a solution. The more acid the solution,
the more hydrogen ions present: pH = - log [H+]. pH varies inversely with H
+ concentration. An
increase in H+ concentration reduces pH, and a decrease in H
+ elevates pH.
The Importance of a Controlled pH Value [H
+] is maintained in very narrow limits at a very low concentration. Normal extracellular level is
approximately 40nmol/l, which is equal to a pH of 7.4. The normal plasma pH range in man is between 7.35 and 7.45. Outside a pH range of 7.2 to 7.6 is regarded as a serious pathological condition. The range of plasma [H
+] compatible with life is 16 to 160nmol/l, which is equal to a pH of 6.8 to 7.8. The pH range of urine varies
from 4 to 8.5. Control of pH is important for a number of reasons. Metabolic reactions are highly sensitive to pH or H
+
concentration. H+ ions can also change the shapes of proteins such as enzymes by interfering with the ionic
bonding patterns within tertiary protein structures. H+ ions are created and destroyed all the time.
Acid-Base Balance and Cellular Buffering The basic steps of acid-base balance regulation involve extracellular and intracellular buffers, with the control of CO2 partial pressure in the blood (by alterations in the rate of alveolar ventilation) and control of plasma HCO3
-
concentration (by changes in renal H+ excretion).
In metabolic acidosis, only 15 to 20% of the acid load is buffered by the CO2/HCO3
-
system in extracellular fluid and most of the remainder is buffered in cells. In metabolic alkalosis, about 30 to 35% of the OH load is buffered in cells. In respiratory acidosis/alkalosis, almost all the buffering is intracellular. The CO2/HCO3
- system is the most important extracellular buffer:
H+ + HCO3
- ↔ H2CO3 ↔ H2O + CO2
HCO3
- and the partial pressure of CO2 are regulated independently. Bicarbonate by changes in renal H
+
excretion, and the partial pressure of carbon dioxide by changes in the rate of alveolar ventilation. At a local level, H2SO4 and HCl produced during metabolism do not circulate as free acids but are immediately buffered in extracellular fluid by HCO3
-.
H2SO4 + 2 NaHCO3 Na2SO4 + 2 H2CO3 2 H2O + CO2
HCl + NaHCO3 NaCl + H2O + CO2
These reactions minimise the increase in extracellular hydrogen ion concentration, but excess H+ must still be
excreted by the kidney to prevent progressive depletion of HCO3-.
Hydrogen Ion Excretion There are both physiological and pathological sources of body H
+ ions.
Physiological sources include carbohydrates and fats (H2O and CO2), sulphur containing amino acids (e.g. cysteine) and also from arginine, histidine, lysine and HCl. Pathological sources include hypoxia, carbohydrates and fat (e.g. lactic acid), and also diabetes (ketoacids). Volatile acids are produced from the metabolism of carbohydrates and fats that results in CO2 production. 15,000mmol of CO2 are generated each day, and this is lost through respiration. Non-volatile acids are derived from the metabolism of proteins, but only 50 to 100mmol of acid are produced in this way each day. These H
+
ions are excreted by the kidneys.
Sybghat Rahim
19
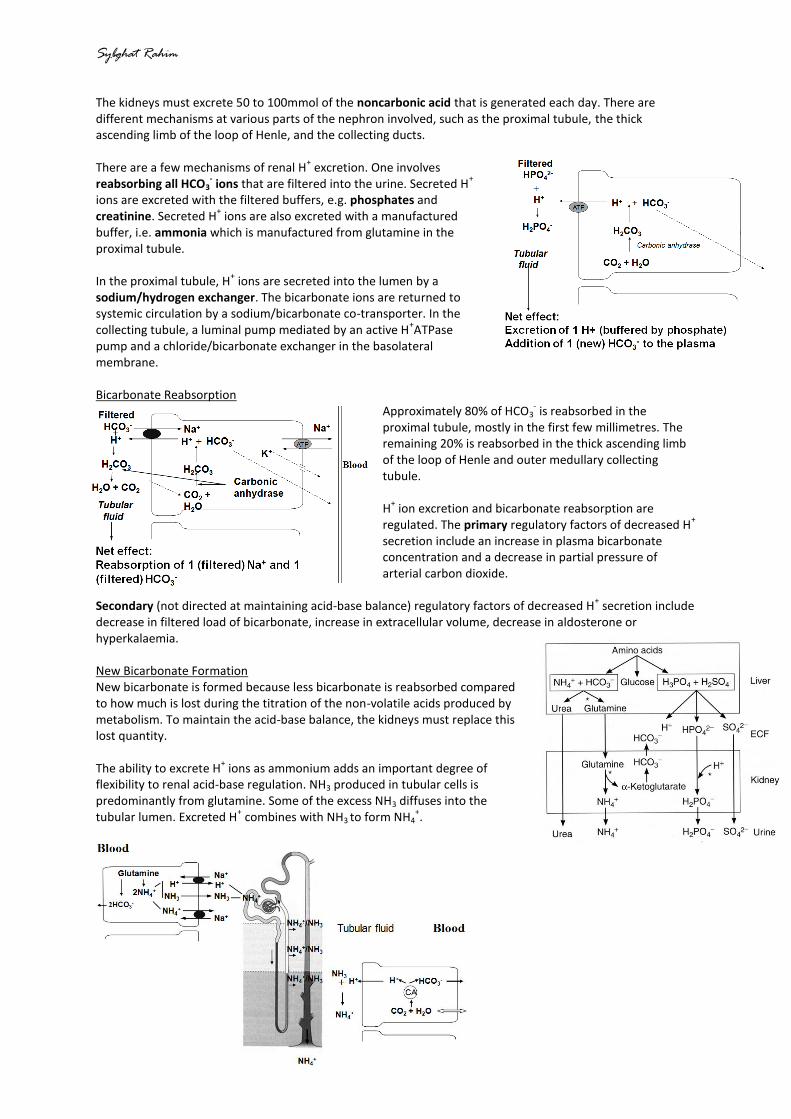
The kidneys must excrete 50 to 100mmol of the noncarbonic acid that is generated each day. There are different mechanisms at various parts of the nephron involved, such as the proximal tubule, the thick ascending limb of the loop of Henle, and the collecting ducts. There are a few mechanisms of renal H
+ excretion. One involves
reabsorbing all HCO3- ions that are filtered into the urine. Secreted H
+
ions are excreted with the filtered buffers, e.g. phosphates and creatinine. Secreted H
+ ions are also excreted with a manufactured
buffer, i.e. ammonia which is manufactured from glutamine in the proximal tubule. In the proximal tubule, H
+ ions are secreted into the lumen by a
sodium/hydrogen exchanger. The bicarbonate ions are returned to systemic circulation by a sodium/bicarbonate co-transporter. In the collecting tubule, a luminal pump mediated by an active H
+ATPase
pump and a chloride/bicarbonate exchanger in the basolateral membrane. Bicarbonate Reabsorption
Approximately 80% of HCO3- is reabsorbed in the
proximal tubule, mostly in the first few millimetres. The remaining 20% is reabsorbed in the thick ascending limb of the loop of Henle and outer medullary collecting tubule. H
+ ion excretion and bicarbonate reabsorption are
regulated. The primary regulatory factors of decreased H+
secretion include an increase in plasma bicarbonate concentration and a decrease in partial pressure of arterial carbon dioxide.
Secondary (not directed at maintaining acid-base balance) regulatory factors of decreased H+ secretion include
decrease in filtered load of bicarbonate, increase in extracellular volume, decrease in aldosterone or hyperkalaemia. New Bicarbonate Formation New bicarbonate is formed because less bicarbonate is reabsorbed compared to how much is lost during the titration of the non-volatile acids produced by metabolism. To maintain the acid-base balance, the kidneys must replace this lost quantity. The ability to excrete H
+ ions as ammonium adds an important degree of
flexibility to renal acid-base regulation. NH3 produced in tubular cells is predominantly from glutamine. Some of the excess NH3 diffuses into the tubular lumen. Excreted H
+ combines with NH3 to form NH4
+.

Sybghat Rahim
20
Basic Acid-Base Disorders Metabolic acidosis is low plasma pH and bicarbonate. This is caused by the addition of non-volatile acids (e.g. ketoacidosis in diabetes), loss of non-volatile alkalis (e.g. diarrhoea), or failure to reabsorb sufficient bicarbonate (renal failure). Respiratory compensation occurs by raised ventilation due to peripheral chemoreceptor stimulation. The partial pressure of carbon dioxide falls by 1.2mmHg for every 1mmol/l fall in bicarbonate. Renal excretion of net acid increases if possible. Metabolic alkalosis is raised plasma pH and bicarbonate. It is caused most commonly by loss of non-volatile acid (e.g. vomiting), and is also caused by raised aldosterone. Compensation occurs by reduced ventilation, as the partial pressure of carbon dioxide rises by 0.7mmHg for every 1mmol/l rise of plasma bicarbonate. Compensation is also in the form of renal excretion of excess bicarbonate, but this can be limited if there is a low blood volume with sodium and chloride depletion. Respiratory acidosis is low plasma pH and high partial pressures of CO2. This is caused by reduced alveolar ventilation or impaired gas diffusion. Renal compensation occurs by increasing the bicarbonate and ammonium secretion, which takes several days. In the intervening acute phase, cellular buffering minimises changes to plasma pH. For a change of CO2 partial pressure by 10mmHg, the plasma bicarbonate increases by 1mmol/l in the acute phase, and by about 3.5mmol/l in the chronic phase. pH rises back towards, but not above normal. Respiratory alkalosis is elevated plasma pH and reduced pCO2. This is caused by increased alveolar ventilation. Renal compensation occurs by decreasing bicarbonate reabsorption and ammonium secretion, but this takes several days. In the acute intracellular buffering phase, the plasma bicarbonate decreases by 2mmol/l for a drop of pCO2 of 10mmHg. In the chronic phase, plasma bicarbonate decreases by 5mmol/l. The pH falls back towards normal, but not below normal. Clinical Implications Analysis of an acid-base disorder is directed at identifying the underlying cause so that treatment can be initiated. A medical history and associated physical findings often provide valuable clues about the nature and origin of an acid-base disorder. Often, arterial blood is required for analysis.

Sybghat Rahim
21
What happens when the kidneys stop working? by Dr Andrew Frankel
Loss of excretory function: this leads to the accumulation of waste products. Loss of homeostatic function: this leads to disturbance of electrolyte balance, loss of acid-base control, and inability to control volume homeostasis. Loss of endocrine function: this leads to impairment of the renin-angiotensin system. The clinical features are determined by the rate of deterioration.
A Case Study Mrs EH, a 75 year old woman is admitted as an emergency. She has a 3 week history of feeling she had the “flu”, becoming increasingly weak, losing appetite and drinking only 2 cups of tea a day. She has a 24 hour history of being too weak to move. She has a past medical history of “kidney problems” after the birth of her 2
nd child - found to have reflux
nephropathy. She had a myocardial infarct 2 years previously, and her plasma creatinine was 163μmol/L at the time of her myocardial infarction (normal range 50 to 110). On examination she is “very unwell”. She is pale, has cold hands, poor skin turgor, a pulse rate of 50 beats per minute and a blood pressure of 67/35mmHg. A jugular venous pulse is not visible and she is tachypnoeic, although she has clear lungs on auscultation. Initial blood results: low sodium, high potassium, very high urea, very high creatinine, low haemoglobin. Arterial blood gases: mild acidosis, low carbon dioxide, high oxygen, low bicarbonate, -ve base excess. Summary of clinical findings:
- symptoms of extreme lethargy and anorexia - clinically volume depleted resulting in severe hypotension - elevated plasma urea and creatinine make diagnosis of renal failure - complicated by
o hyperkalaemia o hyponatraemia o metabolic acidosis
- ultrasound = two small shrunken kidneys The symptoms of lethargy and anorexia are caused by several factors. Firstly, the accumulation of nitrogenous waste products, hormones, peptides and other ‘middle-sized’ molecules (molecular weight 2 to 5000). Secondly, acidosis and hyponatraemia, as well as volume depletion (low blood pressure) and anaemia. Salt and water imbalance is caused by the inability to decrease sodium excretion (i.e. increase sodium reabsorption) when sodium is depleted. Osmotic dieresis is caused by the high concentration of small molecular weight waste substances, e.g. urea. This inappropriately high loss of salt and water results in volume depletion which causes the low blood pressure. Salt and water loss is usually found in patients with tubulointerstitial disorders in which the concentrating mechanisms have been damaged. It is more usual for patients with renal dysfunction to have difficulty in excreting salt and water. This leads to a tendency to retain sodium, which in turn can cause hypertension, oedema, and pulmonary oedema. Acidosis is caused by decreased excretion of H
+ ions and by retention of acid bases. It is buffered by H
+ ions
passing into cells in exchange for K+ ions, which in turn actually aggravates the tendency to hyperkalaemia.
Another complication mechanism is increasing CO2 loss through the lungs (Kussmahl respiration or “air hunger”). Acidosis exacerbates anorexia and increases muscle catabolism. Hyperkalaemia is caused by failure of the distal tubule to secrete potassium. It is exacerbated by acidosis, which causes the shift of potassium from intracellular to extracellular space. It can cause cardiac arrhythmias and even arrest. Clinical features of hyperkalaemia are dependent on the chronicity of the hyperkalaemia.

Sybghat Rahim
22
The kidney also has to be seen as a metabolic organ. Erythropoietin is produced by the kidneys. Decreased erythropoietin production in renal failure results in anaemia. Low 1-25 vitamin D levels result in poor intestinal calcium absorption, hypocalcaemia (short term) and hyperparathyroidism (longer term). There is also increased cardiovascular risk. Loss of kidney function will cause patients to present with anaemia, acidosis, tendency to hyperkalaemia, hypocalcaemia or renal osteodystrophy, metabolic complications, tendency to hyponatraemia, oedema and hypertension. Acute kidney failure will mean the renal size is unchanged and there is previously normal creatinine. Chronic kidney failure will mean the renal size is often reduced, and there was previously abnormal creatinine. Initial Management of Patient
- Intravenous normal saline to correct fluid depletion - Intravenous sodium bicarbonate to correct acidosis - Intravenous insulin and dextrose to lower plasma potassium (by driving K
+ ions back into cells)
- Transfer to Charing Cross for dialysis Outcome of Treatment
- Mrs EH felt better - Urine output initially 100ml/day (no longer has osmotic diuresis) - After 2 weeks, urine output increases to 300 to 400ml/day and pre-dialysis creatinine stabilises at 400
to 450μmol/L. - Discontinuing regular dialysis determined by glomerular filtration rate.
Assessing Glomerular Filtration Rate
• UREA – Poor indicator – Confounded by diet, catabolic state, GI bleeding, drugs, liver function etc
• CREATININE – Affected by muscle mass, age, race, sex etc. Need to look at the patient when interpreting
the result • CREATININE CLEARANCE
– Difficult for elderly patients to collect an accurate sample • ESTIMATED GFR
– Equation which automatically calculates GFR from serum creatinine – Easiest equation uses age and ethnicity (MDRD equation) – Alternatives can include weight, albumin etc – Generally unreliable for well preserved GFR (>60ml/min)
• INULIN CLEARANCE – Laborious - used for research purposes only
• RADIONUCLIDE STUDIES – EDTA clearance etc – Reliable but expensive
Long Term Management Glomerular filtration rate as measured by
52Cr EDTA clearance was 4.5ml/min, so the patient remains on
regular haemodialysis for 4 hours 3 times a week. The patient is advised a low potassium diet and fluid restriction, and is given erythropoietin injections to correct anaemia. 1-25 Vitamin D supplements are given to prevent hyperparathyroid bone disease.