use of the optimal dose of arbs in hypertension and cv diseases ass. prof. roland kassab head of...
TRANSCRIPT
Use of the optimal dose of ARBs in hypertension and CV diseases
Ass. Prof. Roland KASSABHead of Division of Cardiology
HDF, Beirut
12/02/2005


“The objective of antihypertensive therapy should be to not only lower the blood pressure but to prevent the lethal and disabling cardiovascular sequelae.”
Kannel WB. Eur Heart J. 1992;13(suppl G):34–42.
How to get it ?
• Achieve BP goals
• Select appropriate agents and dosages
• Take into account comorbidities
How to get it ?
• Achieve BP goals
• Select appropriate agents and dosages
• Take into account comorbidities

Blood Pressure Classification: JNC VII
Normal <120 and <80
Prehypertension 120–139 or 80–89
Stage 1 HT 140–159 or 90–99
Stage 2 HT >160 or >100
BP Classification SBPmmHg DBPmmHg
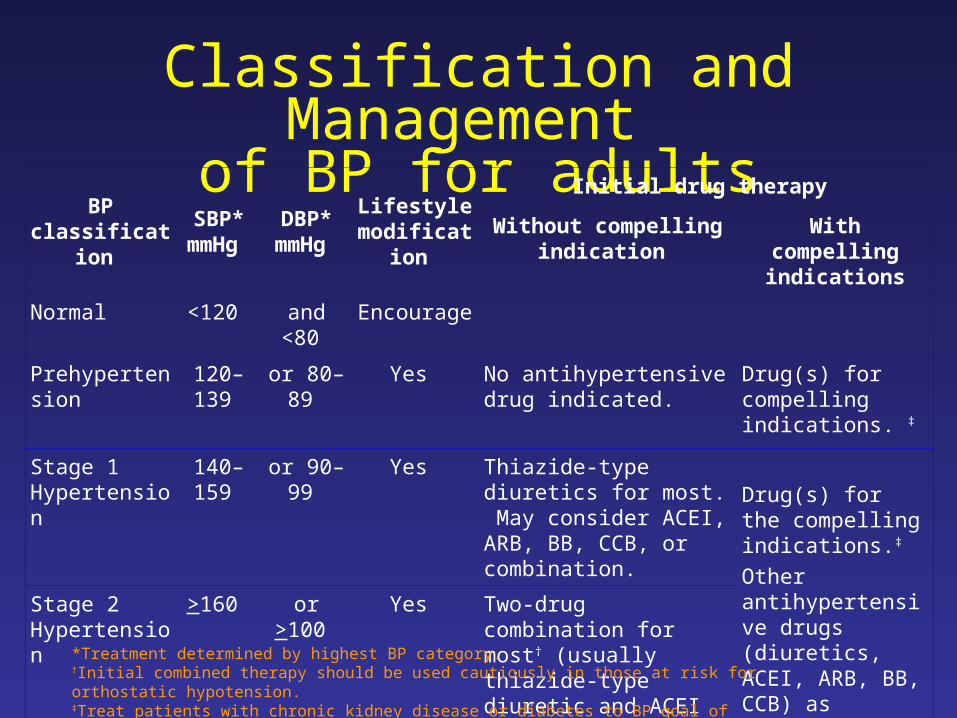
Classification and Management of BP for adults
BP classification
SBP* mmHg
DBP* mmHg
Lifestyle modification
Initial drug therapy
Without compelling indication
With compelling indications
Normal <120 and <80 Encourage
Prehypertension 120–139 or 80–89 Yes No antihypertensive drug indicated.
Drug(s) for compelling indications. ‡
Stage 1 Hypertension
140–159 or 90–99 Yes Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination.
Drug(s) for the compelling indications.‡
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed.
Stage 2 Hypertension
>160 or >100 Yes Two-drug combination for most† (usually thiazide-type diuretic and ACEI or ARB or BB or CCB). *Treatment determined by highest BP category.
†Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension.‡Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mmHg.

US Guidelines 2003 (JNC VII)

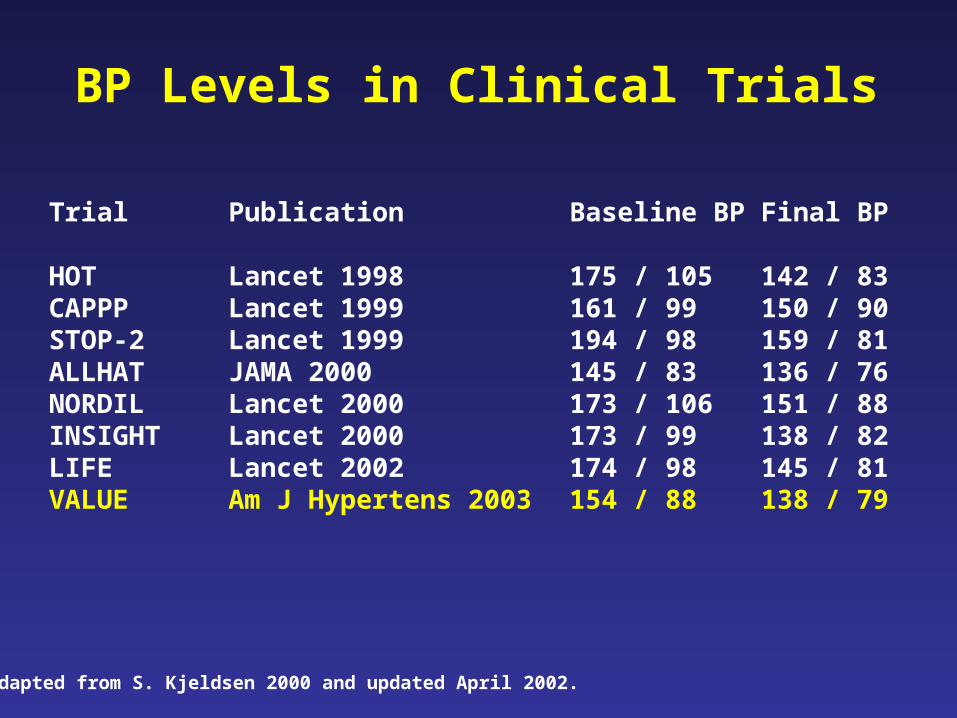
Trial Publication Baseline BP Final BP
HOT Lancet 1998 175 / 105 142 / 83CAPPP Lancet 1999 161 / 99 150 / 90STOP-2 Lancet 1999 194 / 98 159 / 81ALLHAT JAMA 2000 145 / 83 136 / 76NORDIL Lancet 2000 173 / 106 151 / 88INSIGHT Lancet 2000 173 / 99 138 / 82LIFE Lancet 2002 174 / 98 145 / 81VALUE Am J Hypertens 2003 154 / 88 138 / 79
BP Levels in Clinical Trials
Adapted from S. Kjeldsen 2000 and updated April 2002.

VALUE: Number of Antihypertensive Medications Taken Before
Randomisation
NoneNone(7.2%)(7.2%)
1 1 MedicationMedication
(36.8%)(36.8%)
2 2 MedicationsMedications
(31.1%)(31.1%)
3 or More 3 or More MedicationsMedications
(24.9%)(24.9%)
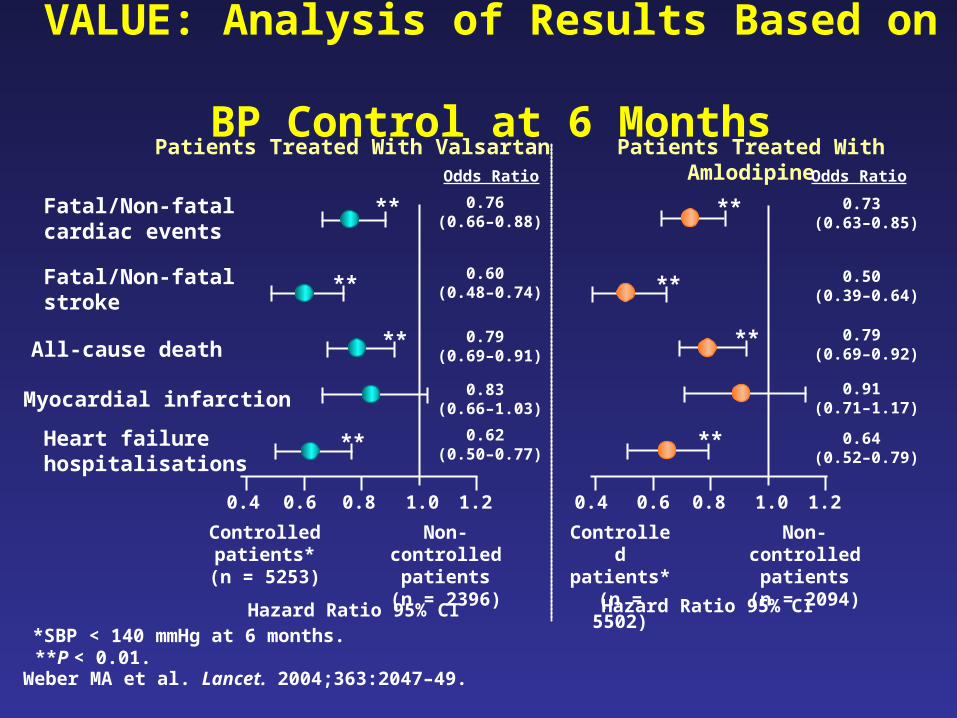
VALUE: Analysis of Results Based on BP Control at 6 Months
Fatal/Non-fatal cardiac events
Fatal/Non-fatal stroke
All-cause death
Myocardial infarction
Heart failure hospitalisations
*SBP < 140 mmHg at 6 months.**P < 0.01.
Patients Treated With Valsartan Patients Treated With Amlodipine
Hazard Ratio 95% CI
0.4 0.6 0.8 1.0 1.2
Controlled patients*(n = 5253)
Non-controlled patients
(n = 2396)
**
**
**
**
0.4 0.6 0.8 1.0 1.2
Controlled patients*(n = 5502)
Non-controlled patients
(n = 2094)
Hazard Ratio 95% CI
**
**
**
**
0.76 (0.66–0.88)
0.60 (0.48–0.74)
0.79 (0.69–0.91)
0.83 (0.66–1.03)
0.62 (0.50–0.77)
Odds Ratio
0.73 (0.63–0.85)
0.50 (0.39–0.64)
0.79 (0.69–0.92)
0.91 (0.71–1.17)
0.64 (0.52–0.79)
Odds Ratio
Weber MA et al. Lancet. 2004;363:2047–49.
How to get it ?
• Achieve BP goals– difficult but feasible– multiple drugs needed
• Select appropriate agents and dosages
• Take into account comorbidities
How to get it ?
• Achieve BP goals– difficult but feasible– multiple drugs needed
• Select appropriate agents and dosages
• Take into account comorbidities

Natural History of CVD Natural History of CVD ProgressionProgressionElevated BP Target
Organ DamageMore Recent Paradigm
A Proposed Future Paradigm
Elevated BP Target Organ
Damage
Vascular Dysfunction
Elevated BP
Target Organ
Damage
Vascular Dysfunction
EndothelialDysfunction
Early Paradigm
Angina Pectoris
Stroke
MIRenal
Damage
LVH?
Hypertension: The Disease Continuum

The Cardiovascular Continuum:Targeting Mechanisms and
Mediators
Adapted from Dzau V et al. Am Heart J. 1991.
EndothelialDysfunction
Maladaptive Cardiovascular RemodelingMaladaptive Cardiovascular Remodeling
Target OrganDamage
Risk FactorsRisk FactorsRisk FactorsRisk Factors
Vascular Vascular DysfunctionDysfunction
Vascular Vascular DysfunctionDysfunction
Vascular Vascular DiseaseDiseaseVascular Vascular DiseaseDisease
Tissue Tissue InjuryInjury
(MI, Stroke) (MI, Stroke)
Tissue Tissue InjuryInjury
(MI, Stroke) (MI, Stroke)
PathologicaPathologicall
RemodelingRemodeling
PathologicaPathologicall
RemodelingRemodelingTarget Organ Target Organ DysfunctionDysfunction(CHF, Renal)(CHF, Renal)
Target Organ Target Organ DysfunctionDysfunction(CHF, Renal)(CHF, Renal)
End-stageEnd-stageOrgan FailureOrgan Failure
End-stageEnd-stageOrgan FailureOrgan Failure
DeathDeathDeathDeath
AngiotensinAngiotensinIIII
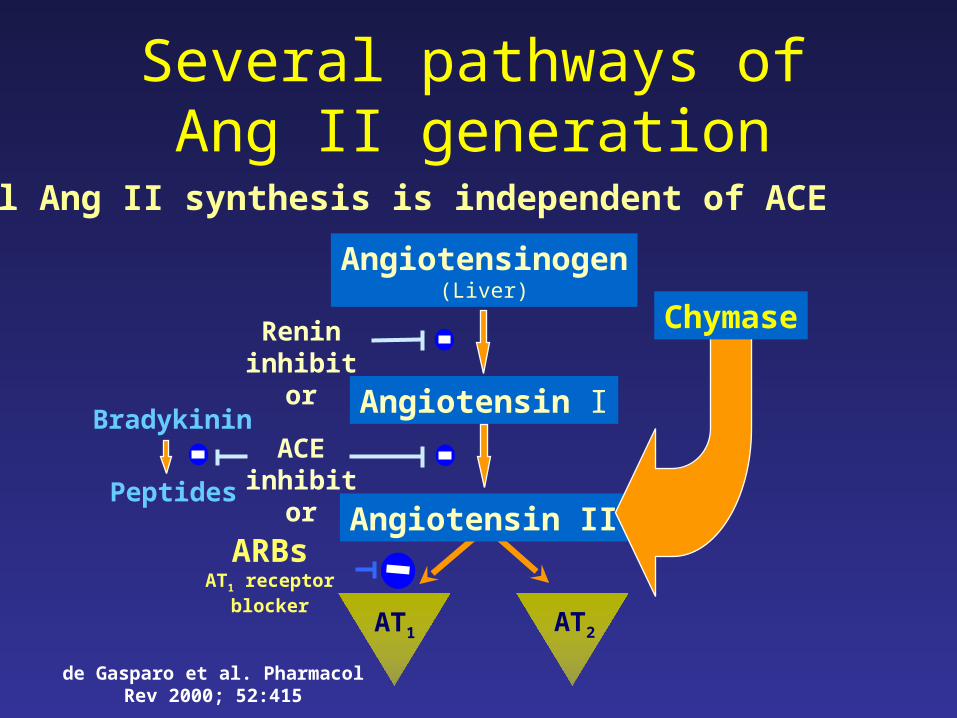
Angiotensin I
Angiotensinogen(Liver)
AT1 AT2
Angiotensin II
ACE inhibitor
ARBsAT1 receptor blocker
Renin inhibitor
Bradykinin
Peptides
Chymase
Local Ang II synthesis is independent of ACE
Several pathways of Ang II generation
de Gasparo et al. Pharmacol Rev 2000; 52:415
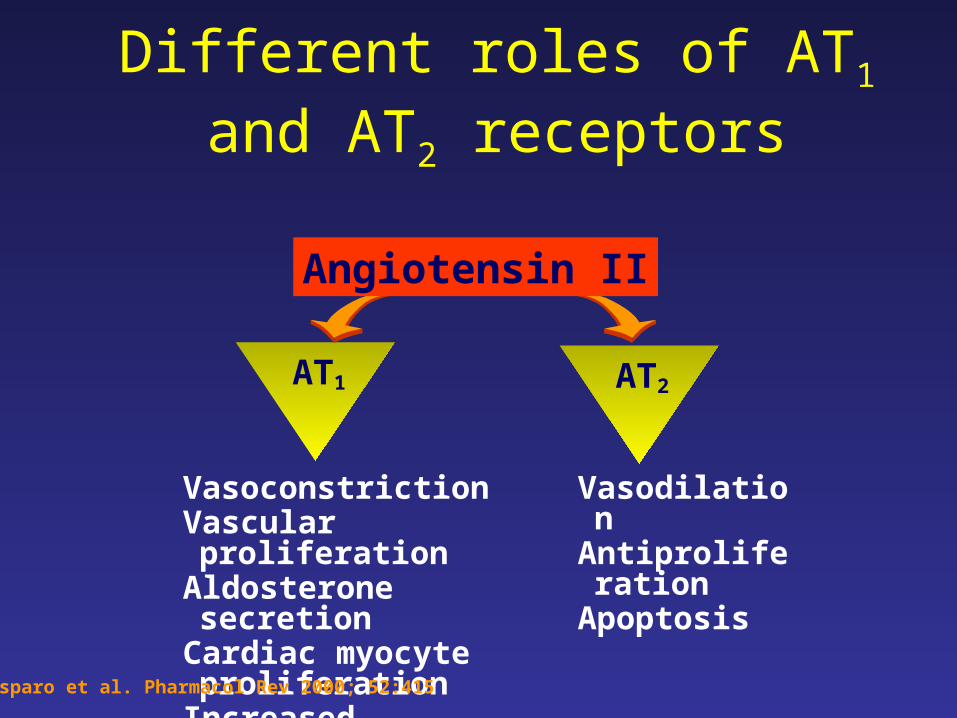
VasoconstrictionVascular proliferation Aldosterone secretionCardiac myocyte
proliferationIncreased sympathetic tone
VasodilationAntiproliferationApoptosis
AT1 AT2
Angiotensin II
Different roles of AT1 and AT2 receptors
de Gasparo et al. Pharmacol Rev 2000; 52:415
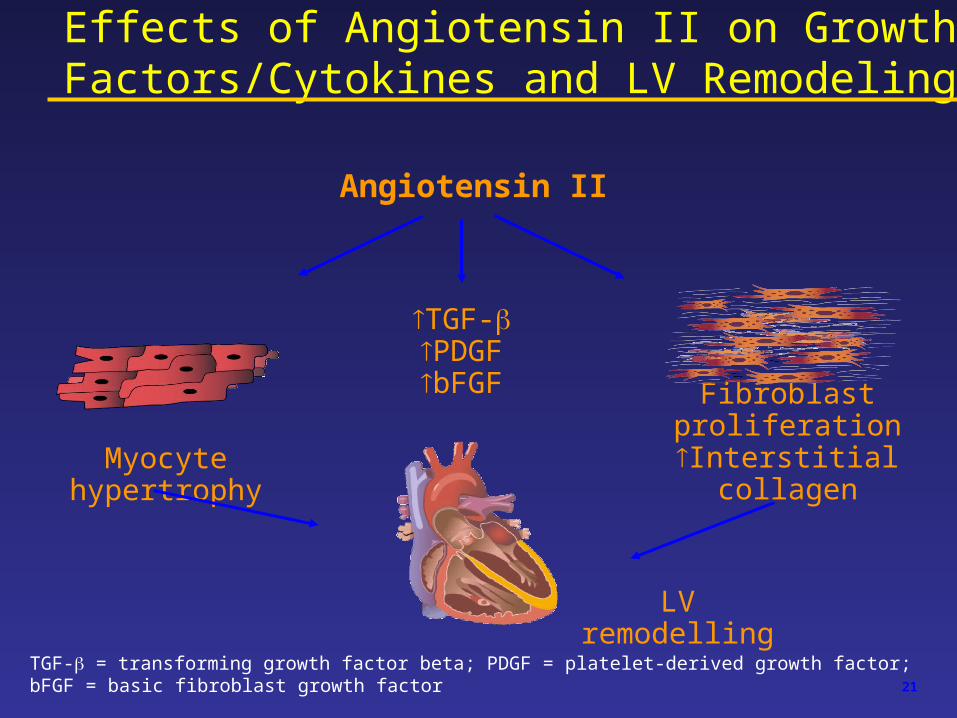
LV remodelling
TGF-PDGFbFGF
Fibroblast proliferation
Interstitial collagenMyocyte hypertrophy
TGF- = transforming growth factor beta; PDGF = platelet-derived growth factor; bFGF = basic fibroblast growth factor
Angiotensin II
Effects of Angiotensin II on Growth Factors/Cytokines and LV Remodeling
21
Vascular Health Benefits of RAAS blockers
• Positively impacts hypertension, oxidative stress, and endothelial functioning, thereby acting at the source of vascular damage
• Blocks the negative effects of Ang II at the AT1 receptor− improves vasodilation and arterial compliance
−reduces oxidative stress
− improves LVEF and LVIDD
−protects against end-organ damage
• Positively influences cardiovascular structure and function

Evidences from RCTs on the efficacy of RAAS blockers in preventing clinical events
along the CV continuum
• CV prevention in high risk patients– HOPE ACE-i ramipril
– EUROPA ACE-i perindopril
– PEACE ACE-i trandolapril
• High risk hypertensive patients– LIFE ARB losartan
– SCOPE ARB candesartan
– VALUE ARB=CCB valsartan/amlodipine

Evidences from RCTs on the efficacy of RAAS blockers in preventing clinical events
along the CV continuum
• Post-MI LVSD/HF– SAVE ACE-i captopril– AIRE ACE-i ramipril– TRACE ACE-i trandolapril– VALIANT ACE-i=ARB Valsartan/captopril
• Heart Failure– CONSENSUS ACE-i enalapril– SOLVD ACE-i enalapril– Val-HeFT ARB valsartan– CHARM ARB candesartan

Inhibiting Ang II Production and/or Its AT1 Receptor: Expanding Therapeutic Opportunities
• Hypertension
• Heart failure
• LV dysfunction/post-MI
• Prevention of ischemic cardiovascular events in high-risk patients
But what about dosages ?

0
100
0
100
0
100
Relationship Between Neurohormone Levels and Survival (CONSENSUS)
Ang II Norepinephrine Aldosterone
SurvivorsDeaths
Swedberg K et al. Circulation. 1990;82:1730-1736.
pg/mL pg/mL pg/mL
P<0.05P<0.05P<0.05P<0.05
P<0.05P<0.05P<0.05P<0.05
P<0.05P<0.05P<0.05P<0.05

0.50.5 1.01.0Odds Ratio
1.251.25
Favors captopril Favors losartan
All-cause mortality(15.9% vs 17.7%: P = 0.16)
Sudden death/resuscitated arrest(7.3% vs 9.0%: P = 0.08)
All-cause mortality/hospitalizations(44.9% vs 47.7%: P = 0.21)
Withdrawal rate 14.5% vs 9.4%: P <0.001
ELITE II: Summary of Major Findings
3,152 elderly CHF patients randomized to losartan (50 mg od) or captopril (50 mg tid)
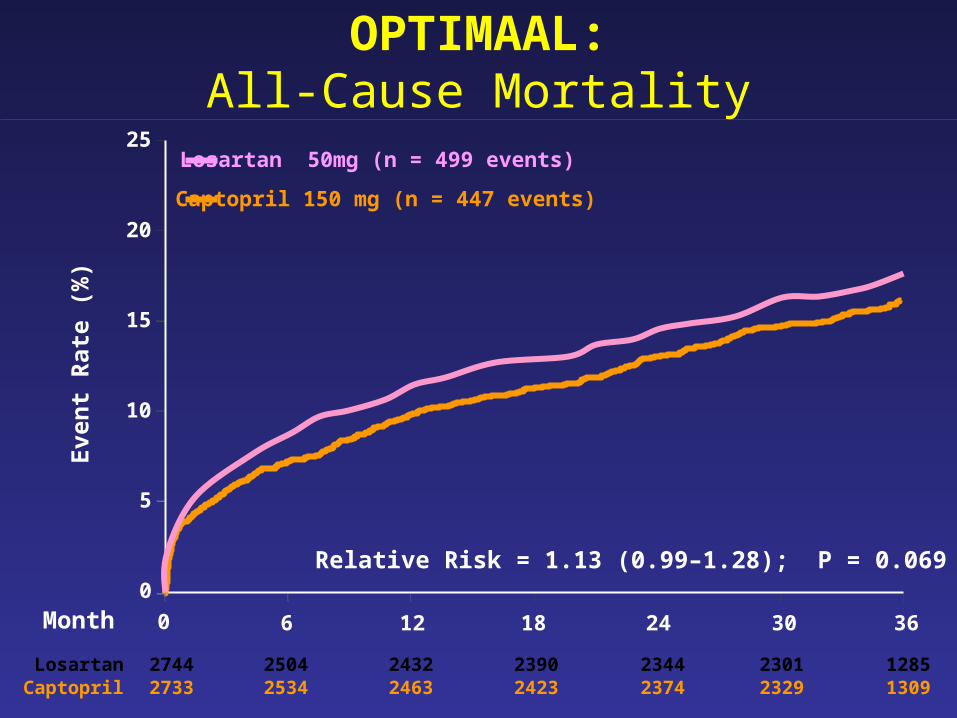
Month 6 12 18 24 30 36
0
5
10
15
20
25
Eve
nt
Rat
e (%
)
Captopril 150 mg (n = 447 events)
Relative Risk = 1.13 (0.99–1.28); P = 0.069
0
OPTIMAAL:All-Cause Mortality
Losartan 50mg (n = 499 events)
Losartan 2744 2504 2432 2390 2344 2301 1285Captopril 2733 2534 2463 2423 2374 2329 1309
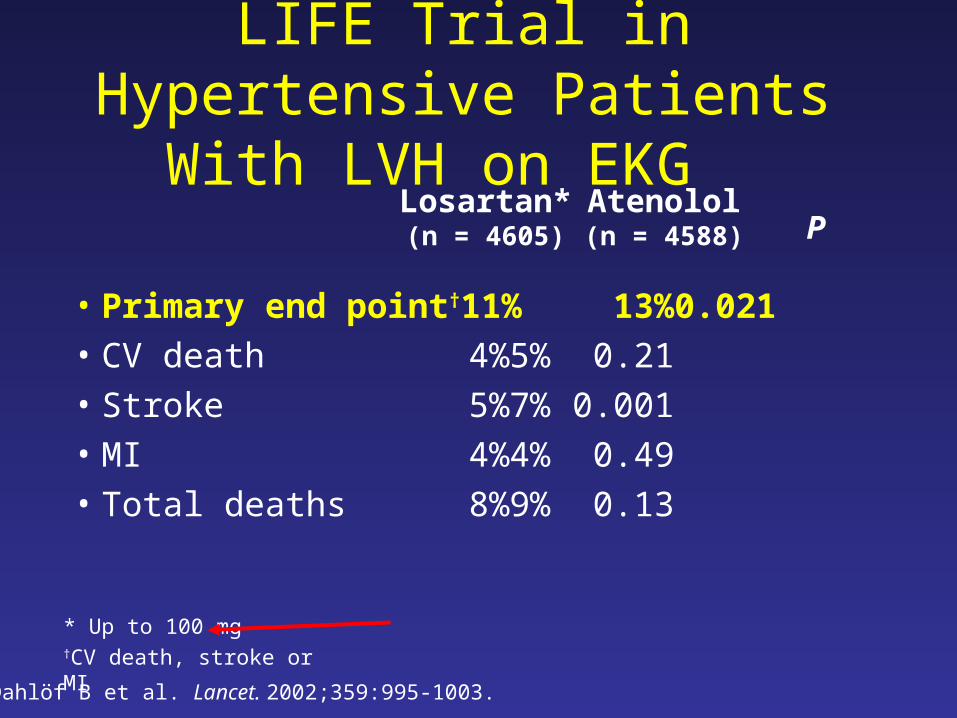
LIFE Trial in Hypertensive Patients With LVH on EKG
• Primary end point† 11% 13% 0.021• CV death 4% 5% 0.21• Stroke 5% 7% 0.001• MI 4% 4% 0.49• Total deaths 8% 9% 0.13
Losartan*(n = 4605)
Atenolol(n = 4588)
Dahlöf B et al. Lancet. 2002;359:995-1003.
P
* Up to 100 mg†CV death, stroke or MI

Valsartan + ACE-I in HF: Valsartan Heart Failure Trial (Val-HeFT)
5010 patients 18 years; EF <40%; NYHA II–IV; LVIDd >2.9 cm/m2
ACE inhibitors (93%), diuretics (86%),digoxin (67%), β-blockers (36%)
Valsartan 40 mg bid titrated to 160 mg bid
906 deaths (events recorded)
Randomized to
Receiving standard therapy
Placebo
EJ = ejection fraction; LVIDd = left ventricular internal diastolic diameter.Cohn JN et al. Eur J Heart Fail. 2000;2:439-446.

Effect of Valsartan on Combined Mortality and Morbidity End Point* in Overall
Population
Months
3 6 9 12 15 18 21 24 270
65
70
75
80
85
90
95
100
Probability of Event-Free
Survival
0
*All-cause mortality, sudden death with resuscitation, hospitalization for worsening heart failure, or therapy with IV inotropes or vasodilators.
Cohn JN et al. N Engl J Med. 2001;345:1667-1675.
30
Valsartan
Placebo
P = 0.00913.2% risk reduction
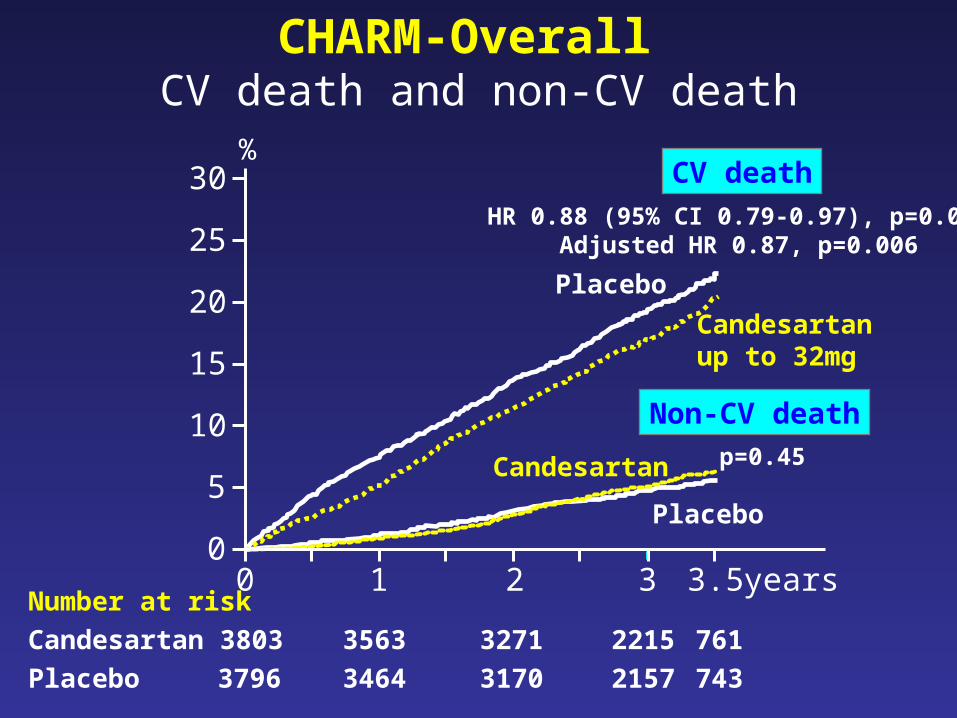
CHARM-Overall CV death and non-CV death
0 1 2 3 years
5
10
15
20
25
30%
0
CV death
Non-CV death
Placebo
Candesartanup to 32mg
Placebo
Candesartan
HR 0.88 (95% CI 0.79-0.97), p=0.012Adjusted HR 0.87, p=0.006
p=0.45
3.5Number at risk
Candesartan 3803 3563 3271 2215 761
Placebo 3796 3464 3170 2157 743
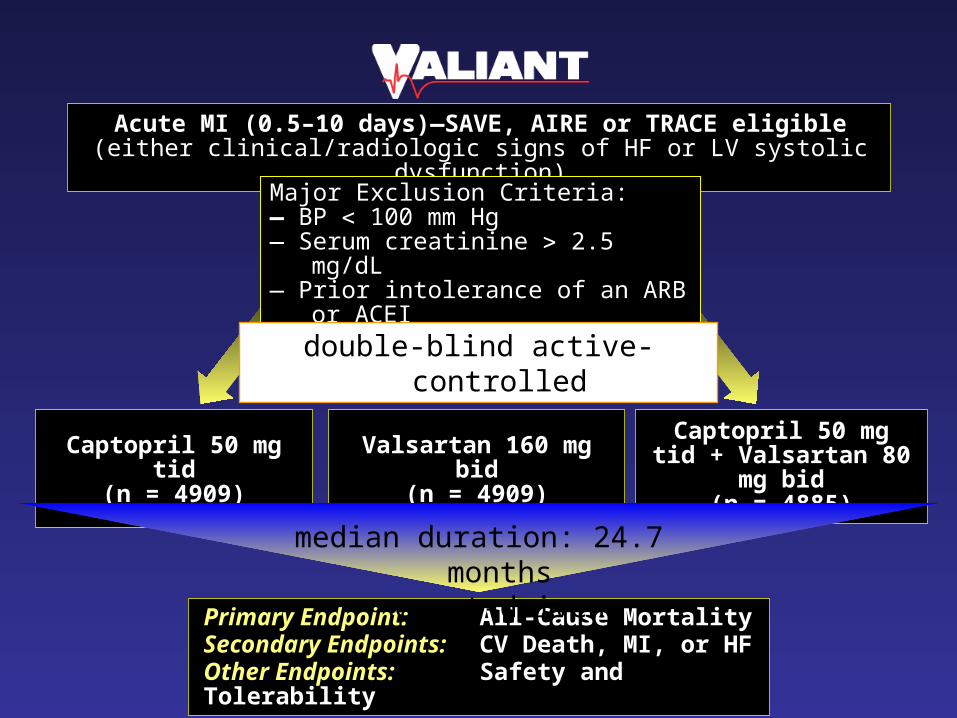
Primary Endpoint: All-Cause MortalitySecondary Endpoints: CV Death, MI, or HFOther Endpoints: Safety and Tolerability
Captopril 50 mg tid(n = 4909)
Valsartan 160 mg bid(n = 4909)
Captopril 50 mg tid + Valsartan 80 mg bid
(n = 4885)
Acute MI (0.5–10 days)—SAVE, AIRE or TRACE eligible(either clinical/radiologic signs of HF or LV systolic dysfunction)
Major Exclusion Criteria:— BP 100 mm Hg— Serum creatinine 2.5 mg/dL— Prior intolerance of an ARB or ACEI— Nonconsent
double-blind active-controlled
median duration: 24.7 monthsevent-driven
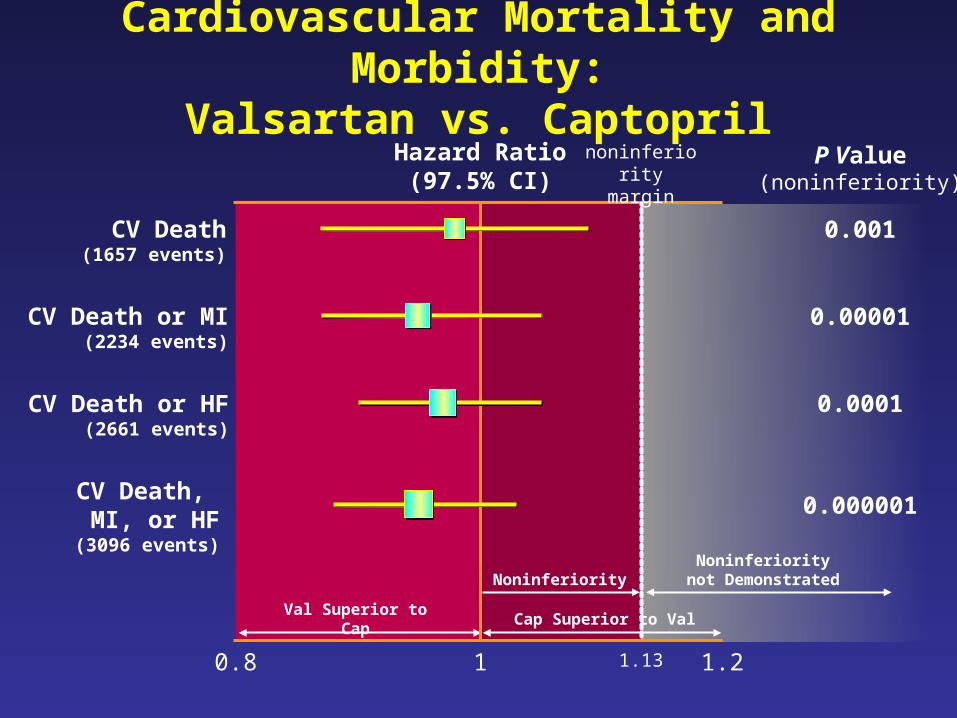
Noninferiority
Val Superior to Cap Cap Superior to Val
Noninferiority not Demonstrated
Cardiovascular Mortality and Morbidity:Valsartan vs. Captopril
0.8 1 1.2
Hazard Ratio(97.5% CI)
1.13
P Value(noninferiority)
noninferiority margin
CV Death(1657 events)
0.001
CV Death or HF(2661 events)
0.0001
CV Death or MI(2234 events)
0.00001
CV Death, MI, or HF(3096 events)
0.000001
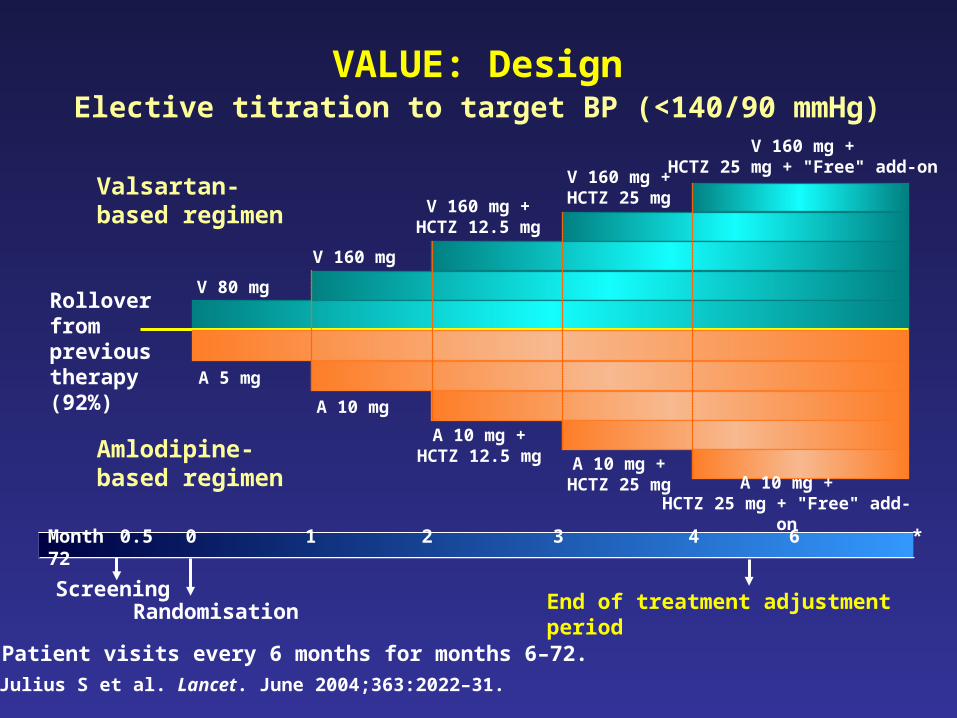
VALUE: DesignElective titration to target BP (<140/90 mmHg)
Month 0.5 0 1 2 3 4 6 * 72
A 10 mg +HCTZ 25 mg
A 5 mg
A 10 mg +HCTZ 12.5 mg
A 10 mg
V 80 mg
V 160 mg
V 160 mg +HCTZ 12.5 mg
V 160 mg +HCTZ 25 mg
Amlodipine-based regimen
V 160 mg +HCTZ 25 mg + "Free" add-on
A 10 mg +HCTZ 25 mg + "Free" add-on
Valsartan-based regimen
ScreeningRandomisation End of treatment adjustment period
Rolloverfromprevious therapy(92%)
*Patient visits every 6 months for months 6–72.
Julius S et al. Lancet. June 2004;363:2022–31.

VALUE: Systolic Blood Pressure in Study
Julius S et al. Lancet. June 2004;363:2022–31.
Valsartan (N= 7649)
Amlodipine (N = 7596)
135
140
145
150
155
mm
Hg
Months (or final visit)
Sitting SBP by Time and Treatment Group
Baseline 1 24 482 3 4 6 12 18 30 36 42 54 60 66
01.02.03.04.0
1 24 48
mm
Hg
2 3 4 6 12 18 30 36 42 54 60 66
Months (or final visit)
5.0Difference in SBP Between Valsartan and Amlodipine
–1.0

VALUE: Outcome and SBP Differences at Specific Time Periods: Primary Endpoint
Time Interval(months)
Overall study
36–4824–3612–246–12
0–3
48−end
Favours amlodipine
1.0 2.00.5
PRIMARY ENDPOINT Odds Ratios and 95% CIs
SBPmmHg
1.41.61.82.0
3.8
1.7
2.2
3–6 2.3
Favours valsartan
4.0
Julius S et al. Lancet. June 2004;363:2022–31.

For dose-responsive efficacy and excellent blood-pressure control1
1. Pool et al. Clin Ther 1998;20:1106-1114
Net
mea
n c
han
ge
in S
SB
P (
mm
Hg
)
Net
mea
n c
han
ge
in S
DB
P (
mm
Hg
)
0
-1
-2
-4
-3
-5
-6
-7
40 80 160 320
-3.9
-6.4
-5.1
-2.6-2.6
0
-1
-2
-4
-3
-5
-6
-7
40 80 160 320
-6.8
-9.0-8.6
-5.3
-8
-9
DIASTOLIC SYSTOLIC
Valsartan®Dose (mg) q.d.
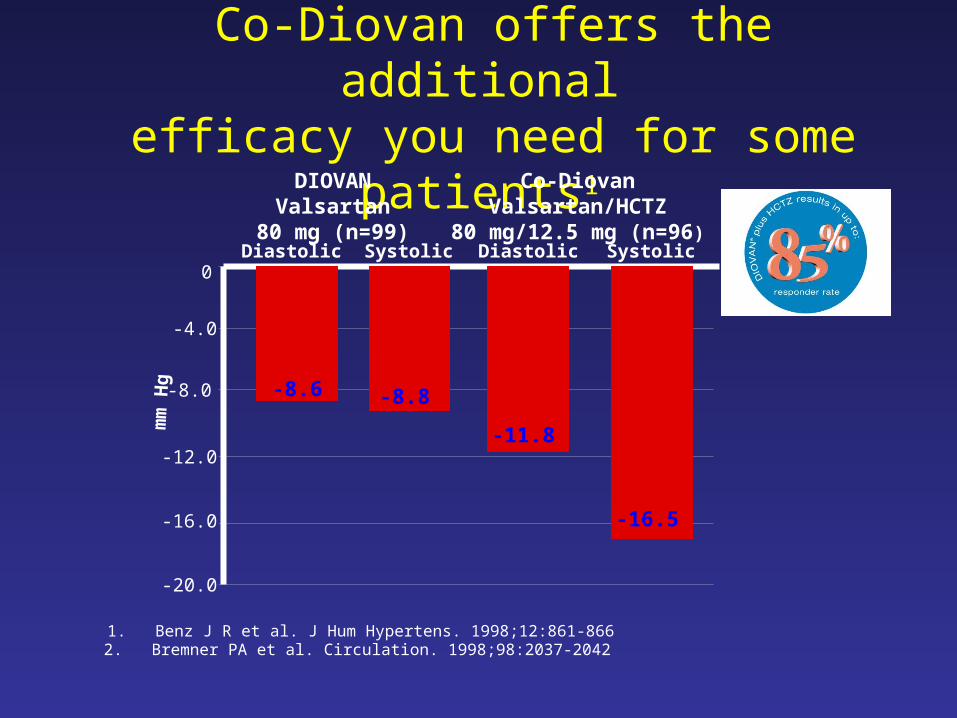
Co-Diovan offers the additional efficacy you need for some patients1
1. Benz J R et al. J Hum Hypertens. 1998;12:861-866
2
2. Bremner PA et al. Circulation. 1998;98:2037-2042
-11.8
-8.8-8.6
0
-4.0
-8.0
-12.0
-16.0
-20.0
Diastolic DiastolicSystolic Systolic
-16.5
DIOVANValsartan
80 mg (n=99)
Co-DiovanValsartan/HCTZ
80 mg/12.5 mg (n=96)
mm
Hg

HIGH vs LOW Dose◙ ACEIs :
► NETWORK: No difference between 5, 10
and 20 mg Enalapril
► ATLAS: High dose Lisinopril:
signif. ↓ mortality + hospit. for CHF
◙ ARBs : Highest tolerated dose in Val-HeFT
and CHARM trials. Low dose in ELITE II
→ HEAAL trial: 50 mg vs 150 mg Losartan

ATLASMajor outcome findings
Primary endpoint 8% in all-cause mortality (non-significant trend: p=0.128)
Secondary endpoints 12% in combined all-cause mortality and all-cause hospitalisation
(p=0.002) 10% in cardiovascular mortality (non-significant trend: p=0.073) 8% in combined all-cause mortality and cardiovascular hospitalisation
(p=0.036) 9% in combined cardiovascular mortality and hospitalisation (p=0.027) 8% in fatal and non-fatal MI and hospitalisation for unstable angina
(p=0.374)
Post-hoc analysis 15% in combined all-cause mortality and hospitalisation for heart failure
(p<0.001)
‘High dose’ lisinopril versus ‘low dose’ lisinopril resulted in risk reductions of:

ATLAS compared with SOLVD
Treatments Reduction in risk Reduction in risk compared of death of death or
hospitalisation for HF
High dose vs.placebo (SOLVD) 16% 26%
Low dose vs. placebo(not studied) not known not known
High dose vs. low dose (ATLAS) 8% 15%
Use of low dose ACEi provides only about half of the benefit that can be achieved with high dose.

How to get it ?
• Achieve BP goals– difficult but feasible– multiple drugs needed
• Select appropriate agents and dosages– evidences on CV prevention with RAAS inhibitors are
overwhelming– only up-titration to high dosages seems to be effective
• Take into account comorbidities
How to get it ?
• Achieve BP goals– difficult but feasible– multiple drugs needed
• Select appropriate agents and dosages– evidences on CV prevention with RAAS inhibitors are
overwhelming– only up-titration to high dosages seems to be effective
• Take into account comorbidities

ADA Treatment Recommendations for Diabetic Patients with Hypertension
• Recommended target blood pressure
– Systolic <130 mm Hg
– Diastolic <80 mm Hg
• Drug therapy mandatory above 140 mm Hg systolic and 90 mm Hg diastolic
• Recommended first-line agents for patients with microalbuminuria or clinical albuminuria
– ARBs and ACE-IsARBs and ACE-Is
American Diabetes Association. Diabetes Care. 2002;25(Suppl 1):S71-S73.

Meta-analysis of Patients With Renal Dysfunction and Type 2 Diabetes (RENAAL, IDNT, IRMA 2 trials)
05
1015202530
Deaths % CV events %
ARBs (n = 1719)
Placebo (n = 1532)
Rouleau JL et al. Can J Cardiol. 2002
P = 0.22P = 0.22 P = 0.034P = 0.034

3535
4545
4040
3030
2525
2020
1515
1010
55
00
Subjects (%)
Subjects (%)
Control(n = 201)Control(n = 201)
150 mg(n = 195)150 mg
(n = 195)300 mg
(n = 194)300 mg
(n = 194)
IrbesartanIrbesartan
24%24%
34%34%
21%21%
IRMA 2Normalization of urinary albumin excretion rate
Parving H-H et al. N Engl J Med 2001;345:870–8.Parving H-H et al. N Engl J Med 2001;345:870–8.
p = 0.006

HOPE and PEACE: new onset diabetes
0
2
4
6
8
10
12
HOPE PEACE
ACE-i Placebo
3.6%5.4%
9.8%
11.5%
HR 0.66 95% CI 0.51-0.85p <0.001
HR 0.83 95% CI 0.72-0.96p =0.014

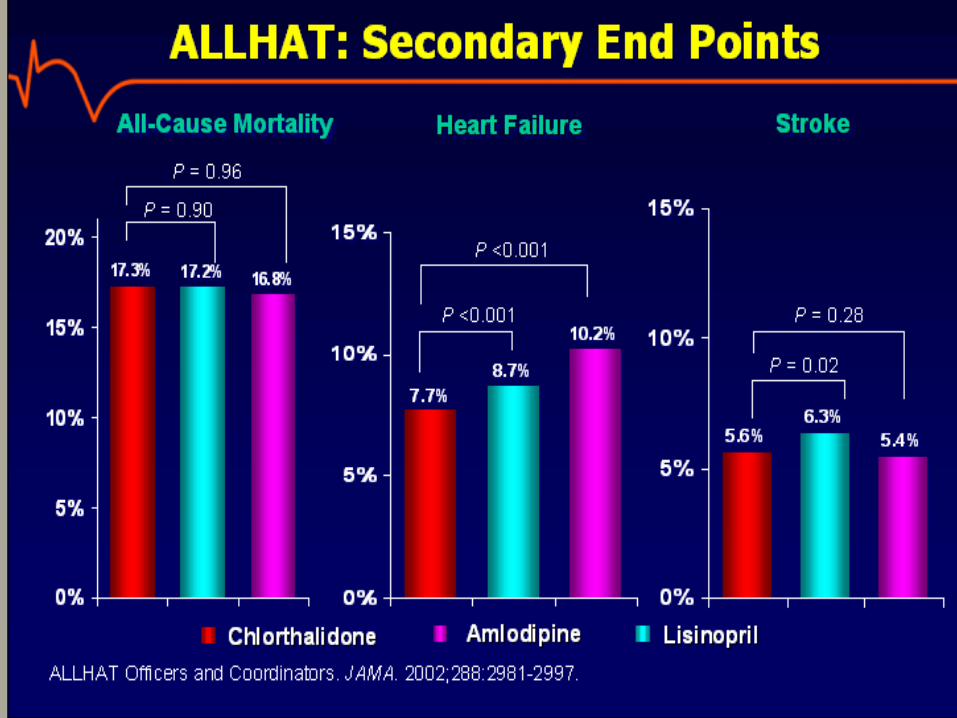
100.5 (19.5)*103.1 (27.7)104.4 (28.5)4 Years
Diabetes incidence (follow-up fasting glucose 126 mg/dL)
Among baseline non-diabetics with baseline <126 mg/dL
Total
4 Years
Baseline
4 Years
Baseline
8.1%*9.8%*11.6%
93.3 (11.8)93.0 (11.4)93.1 (11.7)
121.5 (51.3)*123.7 (52.0)126.3 (55.6)
122.9 (56.1)123.1 (57.0)123.5 (58.3)
LisinoprilAmlodipineChlorthalidone
ALLHATBiochemical Results–
Fasting Glucose (mg/dL)
*P < 0.05 compared to chlorthalidone.
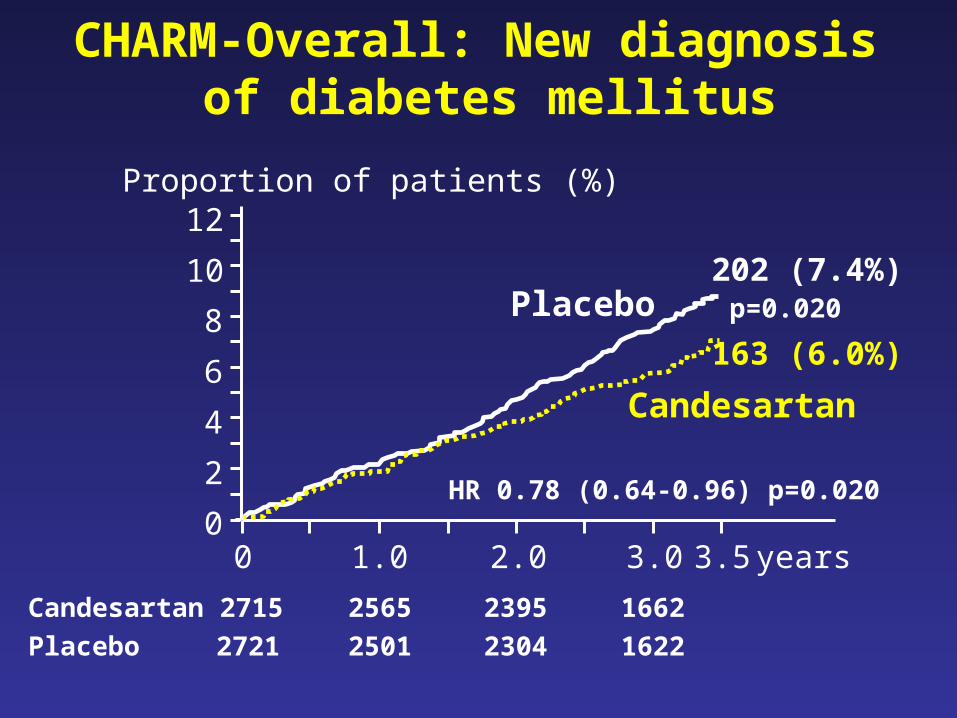
CHARM-Overall: New diagnosis of diabetes mellitus
years0
2
4
6
8
Proportion of patients (%)
p=0.020
HR 0.78 (0.64-0.96) p=0.020
0 1.0 2.0 3.0 3.5
Placebo
Candesartan
12
10 202 (7.4%)
163 (6.0%)
Candesartan 2715 2565 2395 1662
Placebo 2721 2501 2304 1622

LIFE: new onset diabetes
0
5
10
15
20
LIFE
Losartan Atenolol
13.0%
17.4%
HR 0.75 95% CI 0.63-0.88p =0.001
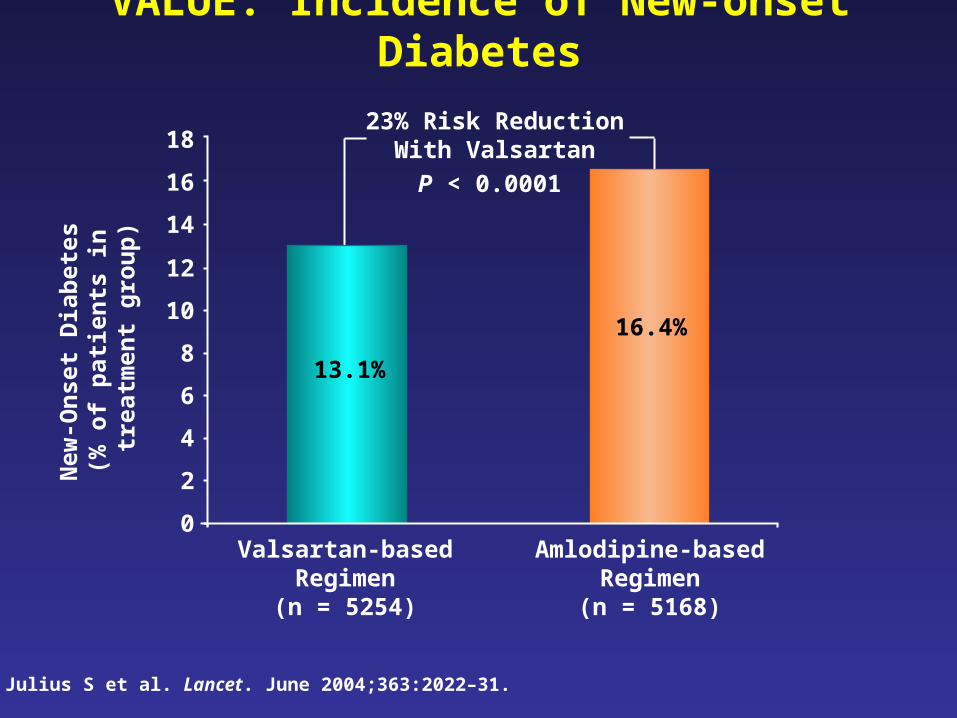
VALUE: Incidence of New-onset DiabetesN
ew-O
nset
Dia
bete
s (%
of
pati
ents
in
tre
atm
ent
grou
p)
Julius S et al. Lancet. June 2004;363:2022–31.
0
2
4
6
8
10
12
14
Valsartan-based Regimen(n = 5254)
Amlodipine-based Regimen(n = 5168)
13.1%
16.4%
23% Risk Reduction With Valsartan
16
18
P < 0.0001

NAVIGATORNateglinide and Valsartan in Impaired Glucose
Tolerance Outcomes Research
• Multinational trial in 9524 IGT patients randomized to either placebo or:– Nateglinide 60 mg tid ac– Valsartan 160 mg/d– Combination of nateglinide (60 mg tid ac) and valsartan (160
mg/d)
• Study duration of 5-6 years• Represents the largest diabetes prevention study
to date and the only one powered to assess CVD

NAVIGATOR: Primary Objectives
• Evaluate the effect of nateglinide, valsartan or the combination on progression to diabetes in patients with IGT
• Evaluate the effect of nateglinide, valsartan or the combination on the composite CV end point (CV mortality, non-fatal MI, stroke, unstable angina, revascularization)

Utility of Antihypertensives by Co-morbidity
nephroprotectionnephroprotection+ ACE-I, ARB+ ACE-I, ARB+ loop diuretics+ loop diuretics
Renal insufficiencyRenal insufficiency
resistance to urinary flowresistance to urinary flow+ + 11-blocker-blockerBenign prostatic hyperplasiaBenign prostatic hyperplasia
nephroprotectivenephroprotectivemetabolically neutral, metabolically neutral, prognosis prognosis
ACE-I, ARBACE-I, ARBcardioselective beta-blocker cardioselective beta-blocker thiazide diureticsthiazide diuretics
Metabolic syndrome, diabetes Metabolic syndrome, diabetes mellitusmellitus
prognosisprognosisACE-I, ARBACE-I, ARBbeta-blockerbeta-blocker
Post myocardial infarctionPost myocardial infarction
antianginal, antianginal, prognosisprognosisbeta-blockerbeta-blockerACE-IACE-I
Coronary artery diseaseCoronary artery disease
re- and afterload re- and afterload prognosisprognosis preload preload reduction in mortality post-MIreduction in mortality post-MI
ACE-I, ARBACE-I, ARBdiuretics diuretics beta-blockersbeta-blockers
Heart failure Heart failure
ReasoningReasoningDrug ClassesDrug ClassesCo-MorbidityCo-Morbidity
Braun J, Dorman A. eds. Clinical Guide to Internal Medicine. 8th ed. München: Urban & Fischer; 2001. Braunwald E, Zipes DP, Libby P. eds. Heart Disease. 6th ed. WB Saunders; 2001:972.The HOPE Study Investigators. N Engl J Med. 2000;342:145-153. American Diabetes Association. Diabetes Care. 2002;25(Suppl 1):S71-S73. WHO
Guidelines subcommittee. J Hypertens. 1999;17:151-183. JNC VI. Arch Intern Med. 1997;152:2413-2446.

“The objective of antihypertensive therapy should be to not only lower the blood pressure but to prevent the lethal and disabling cardiovascular sequelae.”
Kannel WB. Eur Heart J. 1992;13(suppl G):34–42.

How to get it ?• Achieve BP goals
– difficult but feasible– multiple drugs needed
• Select appropriate agents and dosages– evidences on CV prevention with RAAS inhibitors are overwhelming– only up-titration to high dosages seems to be effective
• Take into account comorbidities– RAAS inhibitors seem to prevent diabetes and related CV complications
• ARB (specifically Valsartan) is the most studied class of drugs along the CV continuum



PEACE trial: Other Outcomes
0.0480.77 (0.60-1.00)3.22.5CHF hospitalization
0.130.89 (0.76-1.04)8.17.2Death (any cause)
0.0140.83 (0.72-0.96)11.59.8New diabetes
1.7
2.8
Trandolapril n=4158
%
2.2
3.7
Placebo n=4132
%
0.0180.75 (0.59-0.95)CHF hospitalization or CHF death
0.090.76 (0.56-1.04)Stroke
P-value
Hazard Ratio (95% CI)
Outcome
NEJM 2004;351:2058-68

VALUE: Primary Composite Cardiac Endpoint
14
12
10
8
6
4
2
0
Time (months)
0 6 12 18 24 30 36 42 48 54 60 66
Pro
port
ion
of P
atie
nts
W
ith
Fir
st E
ven
t (%
)Valsartan-based regimen
Amlodipine-based regimen
HR = 1.03; 95% CI = 0.94–1.14; P = 0.49
Julius S et al. Lancet. June 2004;363:2022–31.
Number at risk
Valsartan
Amlodipine 7596
7649
7469
7459
7424
7407
7267
7250
7117
7085
6772
6732
6955
6906
6576
6536
5959
5911
3725
3765
1474
1474
6391
6349

High-risk hypertensive patientsHigh-risk hypertensive patients SBP >140 mm Hg DBP >90 mm Hg
OR Took medication for hypertension and
at least 1 additional CAD risk factor Age >55 years
RandomizationRandomization
Eligible for lipid-lowering Not eligible for lipid-lowering
Randomize
Pravastatin Usual care
Follow for occurrence of CAD until death or end of study (mean 4.9 years)• Primary end point – Fatal coronary heart disease and nonfatal MI• Secondary end points – All-cause mortality, stroke, and major cardiovascular disease events (CHF, coronary revascularization, angina, and peripheral vascular disease)
ALLHAT: Study Design
Davis BR et al. Am J Hypertens. 1996;9:342-360.
Chlorthalidone 12.5-25 mg/dChlorthalidone 12.5-25 mg/d
Amlodipine 2.5-10 mg/dAmlodipine 2.5-10 mg/d
Lisinopril 10-40 mg/dLisinopril 10-40 mg/d
Doxazosin 2-8 mg/dDoxazosin 2-8 mg/d(N(N = 42,418)= 42,418)
Add-on medicationsStep 2Step 2: reserpine, clonidine, atenololStep 3Step 3: hydralazine

PLASMA RENIN LEVELS AFTER 2 AND 4 WEEKS OF TREATMENT WITH
DIFFERENT AT-1R BLOCKERS
0
35
70
105
140
2 Weeks 4 Weeks
Placebo Telmisartan 40 mg Losartan 50 mg Valsartan 80 mg
pg/ml
* * ***
**
* p < 0,05 ** p < 0,01 vs placeboFogari et al. Current Ther Res 2002; 63 : 1-14
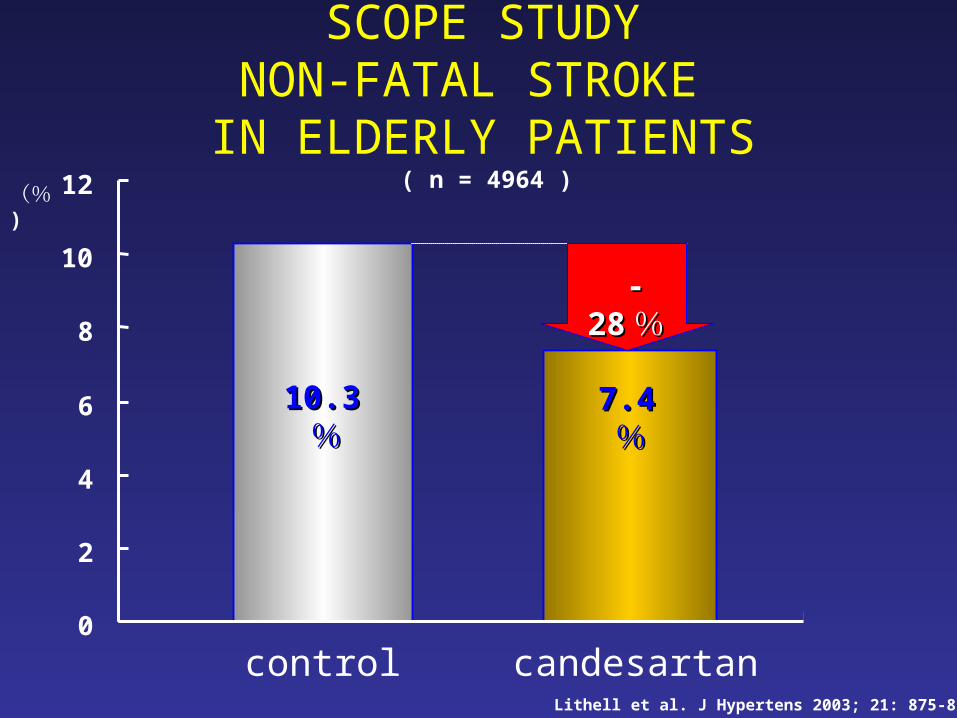
0
2
4
6
8
10
12
control candesartan
10.310.3%%
7.47.4%%
(%)
--2828 %%
SCOPE STUDYNON-FATAL STROKE
IN ELDERLY PATIENTS
Lithell et al. J Hypertens 2003; 21: 875-836
( n = 4964 )
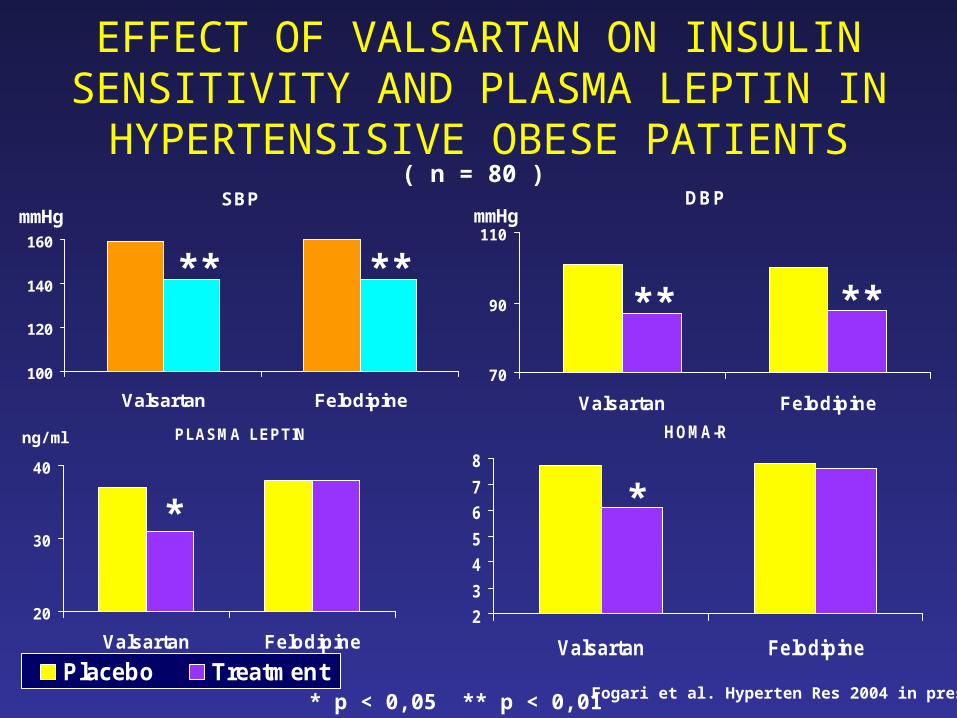
EFFECT OF VALSARTAN ON INSULIN SENSITIVITY AND PLASMA LEPTIN IN
HYPERTENSISIVE OBESE PATIENTSSBP
100
120
140
160
Valsartan Felodipine
HOMA-R
2
3
4
5
6
7
8
Valsartan Felodipine
PLASMA LEPTIN
20
30
40
Valsartan Felodipine
Placebo Treatment
DBP
70
90
110
Valsartan Felodipine
ng/ml
* *
****
****
( n = 80 )
mmHg mmHg
* p < 0,05 ** p < 0,01 Fogari et al. Hyperten Res 2004 in press

CHARM Val-HeFTAll Added Alternative All With
ACEI
(93%)
Non-ACEI
(7%)
N= 7601 2548 2028 5010 4644 366
Dose 32mg 320mg
All cause mortality RR
NS NS 33% p=0.017
-Combined all cause M&M
-CV death and/or hospitalization RR
16% p<0.0001
15%p<0.011
23%P=0.0004
13.2%p=0.009
13.2%p=0.009
44.0%P<0.001
Hospitalization for CHF
21%p<0.0001
17%p<0.014
23%p<0.0001
27.5%p<0.001
27.5%p<0.001
53%p<0.001
CV death 12%p=0.012
16%p=0.029
15%p=0.072
NDA NDA 24%p<0.074