vasoconstrictor peptides and intolerance in patients ... heart j_dodds_1995.pdf · pathophysiology...
TRANSCRIPT
BrHeart3J 1995;73:25-31
Vasoconstrictor peptides and cold intolerance inpatients with stable angina pectoris
Paul A Dodds, Christopher M Bellamy, Ronald A Muirhead, Raphael A Perry
AbstractBackground-The exact mechanism thatexplains the phenomenon of cold intoler-ance in patients with angina remainscontroversial. Although the response tothe effects ofa cold environment has beenexamined in these patients, theirresponse to cold air inhalation has pro-duced conflicting results. In addition, thepossible role ofvasoactive peptides in thepathophysiology has not been explored.Objectives-The aims of this study wereto examine the response of patients withstable angina to the effects of cold airinhalation during exercise testing, and toinvestigate the possible role played by thevasoconstrictor peptides endothelin-l(ET-1) and angiotensin-II (AT-lI) in thepathophysiology.Methods-In a randomised order, 12 menwith stable angina, whose medication hadbeen stopped, underwent two separatesymptom limited treadmill exercise tests.At one visit the patients exercised whilebreathing room air and at the other visitthey exercised while breathing cold airfrom a specially adapted freezer. Serialperipheral venous blood samples weretaken for ET-1 and AT-II estimationsduring each visit.Results-Cold air inhalation resulted in asignificant reduction in the mean time toangina (232.7 (20.4) s v 274'1 (26.9) s,P = 0.04) and the mean total exercisetime (299.5 (27.0) s v 350'3 (23.9) s, P =0.008), but no significant change in thetime to 1 mm ST depression (223.3 (29.0) sv 241X3 (29.2) s, P = 0.25). There was nosignificant difference between the rate-pressure products at the onset of angina(P = 0X13) and the time to 1 mm STdepression (P = 0.85), but at peak exer-cise the rate-pressure product was signif-icantly lower in patients breathing coldair as opposed to room air (P = 0.049).There was an equivalent significantdecrease in ET-1 concentrations at peakexercise compared with that at rest atboth visits (room air 5*0 (0.7) pmolIl v 4-3(0.7) pmol/l, P = 003; cold air 4-4 (0.6)pmoMl v 3-8 (0-5) pmol/l, P = 0.02). Therewas a significant increase in AT-II con-centrations 10 min after peak exercise inpatients breathing room air (39.2 (6.1)pmol/l v 32'1 (4.8) pmol/l, P = 0 01) whichwas not repeated during cold air inhala-tion (36-6 (3.4) pmolIl v 28-3 (3.4) pmol/l,P = 0.07).
Conclusions-Cold air inhalation inpatients with stable angina results in anearlier onset of angina and a reduction inexercise capacity. Both peripheral andcentral reflex mechanisms appear to con-tribute to the phenomenon of cold intol-erance. Peripheral ET-1 and AT-II donot appear to play a significant role in thepathophysiology.
(Br Heart3J 1995;73:25-31)
Keywords: angina pectoris; vasoconstrictor peptides;cold intolerance
Many patients with coronary artery diseasecomplain of a deterioration in their angina incold weather.' The exact explanation for thiscold intolerance remains controversial, as it isunclear whether cold air inhalation or theeffects of a cold environment exhibit themajor influence on the pathophysiology. Twophysiological reflex responses have been pro-posed to account for the phenomenon,namely (a) an increase in peripheral vascularresistance resulting in an increase in cardiacwork at any given level of exercise,2 3 and (b)(coronary vasoconstriction (or the lack ofnormal coronary vasodilatation) duringexercise.45Most previous reports on the response of
patients with angina to cold temperatureshave examined the effects of a cold environ-ment,67 and very few studies have investigatedthe response to cold air inhalation. Further-more, such studies have either produced con-flicting results89 or demonstrated coldintolerance only during the inhalation of verycold air.'0
It is possible that naturally occurring vaso-constrictor peptides could play a role in thepathophysiology of cold intolerance inpatients with angina pectoris. Endothelin- 1(ET-1) belongs to a family of potent vasocon-strictor peptides, and has been shown toinduce vasoconstriction in both human resis-tance vasculature"I and human coronary arter-ies.'2 Raised plasma levels of ET-l have beenfound in healthy subjects following the coldpressor test,"3 and ET-1 has been implicatedin the pathophysiology of Raynaud's phenom-enon.'4
Similarly the principal active component ofthe renin-angiotensin system, angiotensin II(AT-II), is known to produce vasoconstric-tion. The renin-angiotensin system has beenimplicated in the elevation of blood pressurein rats during exposure to cold,'5 and raised
The CardiothoracicCentre, LiverpoolP A DoddsC M BellamyR A MuirheadR A PerryCorrespondence to:Dr P A Dodds, TheCardiothoracic Centre,NHS Trust, Thomas Drive,Liverpool L14 3PE.Accepted for publication13 September 1994
25

Dodds, BeUlamy, Muirhead, Peny
AT-II levels have been detected in response topacing induced ischaemia in patients with sta-ble angina.'6 It is possible therefore that eitherET-1 or AT-II may have a role in the mecha-nism of cold induced angina.The aims of this study were to examine the
effects of cold air inhalation during exercisetesting at room temperature in patients withchronic stable angina and to investigate thepossible part played by ET-1 and AT-II in thepathophysiology of cold intolerance.
Patients and methodsSTUDY POPULATIONThe study group consisted of 12 men (agerange 52-69 years, mean age 61-0 years) withchronic stable exertional angina. Eight of thepatients gave a positive history of cold intoler-ance. Each patient had angiographically con-firmed coronary artery disease, with twopatients having single vessel disease, sevendouble vessel disease ahd three triple vesseldisease. Four patients had had a previousmyocardial infarction. None of the studygroup gave a history of hypertension, renaldisease, congestive cardiac failure or chronicrespiratory disease (for example, asthma orchronic obstructive airway disease). Patientstaking diuretic agents or angiotensin convert-ing-enzyme inhibitors were excluded from thestudy. Informed consent was obtained fromeach patient and the study was approved bythe hospital ethical committee.
EXERCISE TESTINGThe study involved each patient undergoingtwo symptom limited treadmill exercise testsusing the Bruce protocol 1 week apart. At onevisit the patient underwent exercise testingwhilst breathing room air and at another visitthe patient performed the exercise test whilstbreathing cold air obtained from a speciallyadapted freezer. This freezer contained a heatexchanger immersed in a glycol solution capa-ble of cooling air to a minimum temperatureof -1 5°C. The heat exchanger was connectedto a small fan unit capable of providing coldair at a maximum rate of 150 I/min. The fanunit was fitted with a short piece of insulated38'1 mm diameter bore hose, and the patientsbreathed the cold air obtained from thefreezer through a mask attached to this hose.An accompanying head strap was used toensure that the mask fitted snugly to thepatient's face. Exercise testing was performedin the early afternoon with each patient havingfasted for at least 4 h. All antianginal medica-tion was stopped for at least 2 days beforeexercise testing. Each patient wore a shirt andtrousers and the order of their visits was ran-domised.At each visit patients were asked to rest for
15 min after which peripheral venous bloodsamples were taken for measurement of ET-1and AT-II concentrations. In addition, restingheart rate and blood pressure were measured.For the visit during which room air wasbreathed, each patient performed a treadmillexercise test during which the time to angina,the time to 1 mm ST depression, and the total
exercise time were recorded. Heart rate andblood pressure were measured at these timepoints at peak exercise and after 10 minrecovery. Further peripheral venous bloodsamples were taken for determination of ET- 1and AT-II concentrations. For the visit duringwhich cold air was breathed, each patient wasasked to breathe cold air obtained from themodified freezer after the resting heart rate,blood pressure, and blood samples had beentaken. Repeat ET-1 and AT-II samples weretaken after 10 min of cold air inhalation atrest. The patient was then asked to performan exercise test whilst continuing to breathecold air and the time to angina, time to 1 mmST depression, and the total exercise timewere recorded. Heart rate and blood pressurewere measured at these time points. FurtherET-1 and AT-Il samples were taken at peakexercise and after 10 min recovery whilst thepatient continued to breathe cold air. Roomtemperature at each visit and the temperatureof the inspired cold air entering the mask weremeasured.
ET-1 AND AT-II ASSAYSAll peripheral venous blood samples taken fordetermination of ET-1 and AT-II concentra-tions were collected into prechilled tubes onice containing EDTA as anticoagulant. Thesamples were centrifuged within 1 h of collec-tion at 3000 rpm for 10 min at 4°C, and theplasma was stored at -20°C until assayed.Endothelin concentrations were measuredusing a radioimmunoassay technique (NicholsInstitute Diagnostics Endothelin 1251I Assay(Saffron Walden, Essex)). Antiserum cross-reactivity was ET-1 100%, endothelin-2 52%,endothelin-3 96%, and big-endothelin 7%.The inter-assay and intra-assay coefficients ofvariation based on pooled samples of plasmawere 9-2% (n = 5) and 4% (n = 12) respec-tively. The recovery of ET-1 from plasmasamples was 83% (range 77-89) (n = 4). Thelowest measurable concentration of the assaywas 0-8 pmol/l. AT-II concentrations werealso measured using a radioimmunoassaytechnique (Nichols Institute DiagnosticsAngiotensin-II 1251I Assay). Antiserum cross-reactivity was Asp'-Ileu5-angiotensin-II 100%,Val5-angiotensin-II 100%, Asp'-Ileu5-angio-tensin-I 0-1%, Asn'-Val5-angiotensin-II 30%,and Sar'-Ileu8-angiotensin-II 0-02%. Theinter-assay and intra-assay coefficients of vari-ation were 5-7% (n = 9) and 3-5% (n = 12)respectively. The recovery of AT-II fromplasma samples was 68% (range 62-74) (n =4). The lowest measurable concentration ofthe assay was 3-6 pmol/l.
STATISTICAL ANALYSISResults are expressed as means (SEM). Thedata were normally distributed, and differ-ences between variables were analysed usingthe Student's paired t test. Statistical signifi-cance was taken as P < 0 05.
ResultsThere was no significant difference in roomtemperature when the patients were breathing
26

Vasoconstrictor peptides and cold intolerance in patients with stable angina pectoris
500
400
cn
*,, 300
2000
E
1001
o
A
-ES
0
0
E0)
._a)
.0
xC)
0F-
P = 0.04
Room air Cold air
500
400 k
300
200H
100l LP = 0-008
vRoom air Cold aiir
-
c0 400
0 0a. 400
0
300
E
E 200
0"I" 100
10
-c
P=NSRoom air Cold air
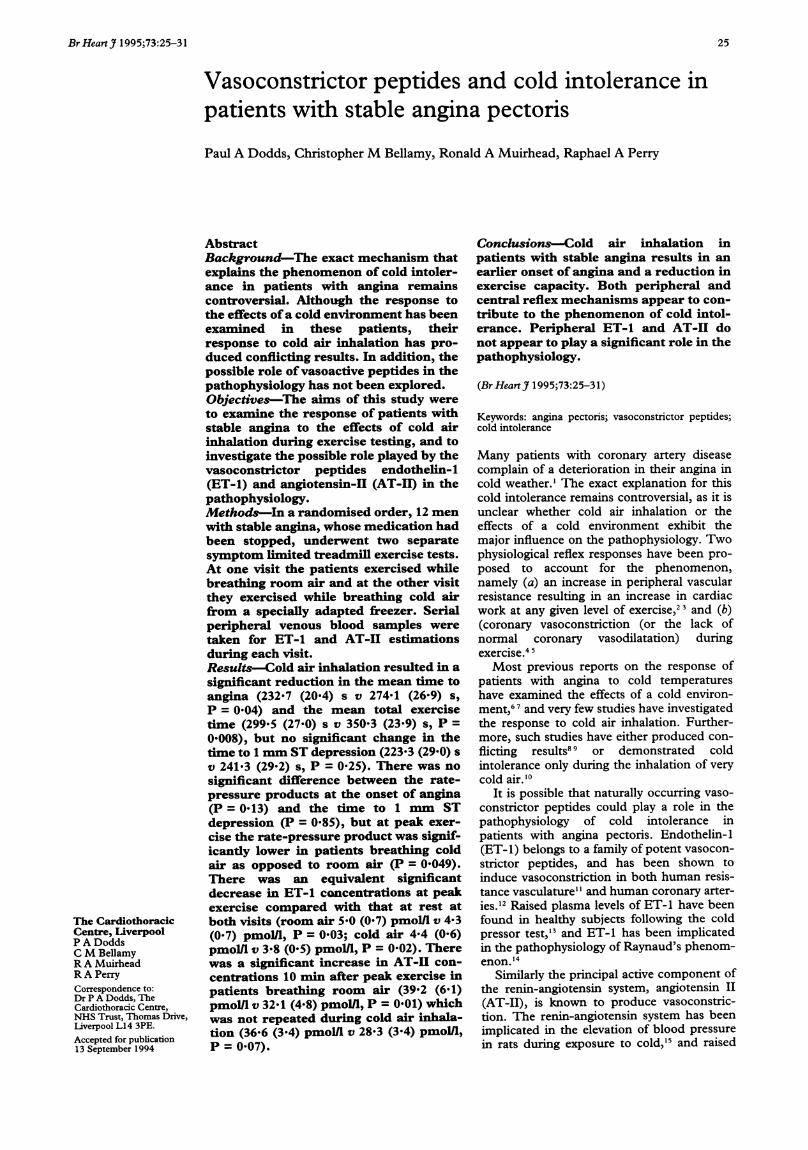
(A) Time to angina, (B) total exercise time, and (C) time to 1 mm ST depression in 12 patients undergoing exercise testing during inhalation ofcold orroom air. Bars represent means (SEM).
warm air (22-3 (0a 1)°C) compared with thatof cold air inhalation (22-5 (0-3)°C). Thetemperature of the inspired,cold air was -&8(0 2)°C.There was a significant decrease in the time
to angina (fig (A)) and in the total exercisetime (fig (B)) in patients breathing cold air as
opposed to room air, but there was no changein the time to 1 mm ST depression (fig (C)).
There was no significant difference in therate-pressure products at the onset of eitherangina or the 1 mm ST.depression, but.atpeak exercise the rate-pressure product was
significantly lower when patients were breath-ing cold air as opposed to room air (table 1).There were no significant differences in heartrate, systolic blood pressure, or diastolicblood pressure at each of these time points(table 2).
Subdividing the patients dependent on
whether they gave a history of cold intolerancerevealed that, for the eight with such a
history, there was a trend towards a reductionin the time to angina, time to 1 mm STdepression, and total exercise time duringcold air inhalation compared with that of
Table 1 Rate-pressure product values during each exercise test
Time to angina Time to I mm ST depression Peak exercise
Patient no Room air Cold air Room air Cold air Room air Cold air
1 20 900 17 510 16 200 16 830 24 510 21 6002 21 420 19 890 18 870 19 210 21 960 21 7803 20 700 18 700 22 860 18 020 24 890 22 3204 23 220 21 780 21 080 22 500 23 580 23 9405 16 800 18 530 16 320 17 120 16480 18 7006 13 950 14 560 13 950 17 340 16 320 17 3407 18 700 21 250 19 550 20 740 22 140 21 0808 18 540 16 490 19 080 19 260 19 440 19 2609 25 620 20 710 26 040 22 040 27 300 21 66010 21 960 24 200 25 400 24 400 27 720 24 60011 25 650 22 800 19 620 22 800 26 220 24 51012 24 990 22 420 18 360 18 700 26 460 23 560Mean (SEM) 21 037 (1043) 19 903 (819) 19 778 (1045) 19 913 (730) 23 085 (1138) 21 696 (672)*
*P = 0 049.
Table 2 Heart rate and blood pressure data during exercise tests
Time to I mm Total exerciseTime to angina ST depression time
Heart rate (beats/min)Warm air 115-2 (3-4) 112-3 (3.2) 122-9 (3-5)Cold air 1118 (3-1) 112-5 (2 5) 119-3 (2 7)
Systolic blood pressure (mm Hg)Warm air 181-7 (5.1) 175 8 (5 3) 186-7 (5-0)Cold air 177-5 (3 5) 176 7 (3 3) 181-7 (2 7)
Diastolic blood pressure (mm Hg)Warmair 84-2 (1-5) 83-3 (1-4) 85-0 (1-5)Cold air 86-7 (1-4) 86-7 (1-4) 87-5 (1-3)
Values are means (SEM).
Table 3 Exercise test data for patients intolerant and tolerant to cold
Intolerant to cold Tolerant to cold
Room air Cold air p Value Room air Cold air p Value
Time to angina (s) 247-5 (28 9) 212-1 (18-6) 0-22 327-2 (51-4) 273-8 (45-9) 0 03Time to 1 mm ST 209-0 (20 6) 196-0 (32 8) 0 47 305-8 (72 7) 277-8 (52.5) 0-42
depression (s)Total exercise time (s) 331-5 (26 6) 285-9 (34-0) 0-07 388-0 (47 7) 326-7 (47 4) 0-07
Values are means (SEM).
-f
27
600 rB,
k

Dodds, Bellamy, Muirhead, Perry
Table 4 Concentrations ofET-1 (pmolll)
Room air Cold air
10 min Rest and 10 Peak exercise 10 min after exercisePatient no Rest Peak exercise after exercise Rest min of cold air and cold air and cold air
1 8-0 8-2 8-2 5-6 4 9 3-1 4-42 2-3 1-7 1-8 1-7 1-6 1-6 1-63 1-5 1-4 1-5 1-2 1-7 1-3 1-54 2-3 2-1 2-2 2-5 1-9 1.9 2-15 5-3 3-6 3-7 3-1 3-2 3-6 3-16 3-6 3-4 3-5 4-2 3-3 2-8 3-77 4-5 4-9 5-7 5 9 6-5 5-3 4-48 6-2 5-1 4-4 4-3 4-5 4-4 4-79 4-6 4 0 4-3 5 0 6-1 5-2 5-5
10 6-0 2-8 39 4-3 4-6 3-5 3-811 7-3 7-3 7-4 7 0 6-0 6-2 5-612 8-9 7-1 7-5 8-6 8-6 6-9 7-2Mean (SEM) 5 0 (0-7) 4-3 (0-7)* 4-5 (0-7) 4-6 (0-6) 4 4 (0 6) 3-8 (0.5)** 4 0 (0.5)****P = 0-03 v rest; **P = 0-02 v rest and 10 min of cold air; ***P = 0 04 v rest and 10 min of cold air.
Table S Concentrations ofA-II (pmolll)
Room air Cold air
10 min Rest and Peak exercise 10 min after exercisePatient no Rest Peak exercise after exercise Rest cold air and cold air and cold air
1 35-2 43-2 44-2 30-2 37-7 34-4 43-52 21-6 27-1 28-1 18-1 20-1 22-8 22-43 40 4 42-4 44-8 57 0 55 0 42-9 35-64 11-5 9 4 13-2 13-5 11-8 18-2 37-15 29-0 503 56-0 26-9 22-7 32-6 62-06 31-2 22-0 31-2 28-4 20-8 35-4 29-67 72-9 73-9 84-8 25-1 34-6 43.9 39-28 20-7 26-6 28-5 43-6 24-8 330 37-79 16-9 18-9 16-7 24-8 42-2 55-1 47-4
10 44-6 42-8 61-1 28-3 28-7 29-2 39 711 19-7 15-7 18-2 18-2 16-2 17-1 17-512 41-9 43-4 43-5 26-0 26-3 26-9 27-0Mean (SEM) 32-1 (4 8) 34-6 (5 2) 39-2 (6-1)* 28-3 (3 4) 28-4 (3 5) 32-6 (3 2) 36-6 (3 4)
*P = 0-01 v rest and P = 0-02 v peak exercise.
room air inhalation, but these findings failedto reach statistical significance (table 3). Forthe four patients who stated that they werecold tolerant, however, there was a significantreduction in the time to angina when breath-ing cold air (table 3).
There was a significant decrease in ET-1concentrations at peak exercise comparedwith that at rest at both visits (table 4), but themagnitude of this decrease at each visit wassimilar, and no significant difference could beestablished between the responses to room air(percent decrease 14-3 (4.9)) and cold airinhalation (percent decrease 1 1 6 (4 1)) (P =0 70).
There was a significant increase in AT-IIconcentrations 10 min after peak exercisecompared with that at both rest and peak
Table 6 Maximal ST depression achieved during exercisetests
Maximal ST depression (mm)
Patient no Warm air Cold air
1 3-0 3-32 1-4 1-73 1-1 1-24 2-0 2-05 2-3 3-06 1-9 1-67 2-4 1-78 2-2 1.09 1-6 1-110 1-4 1-01 1 2-8 2-312 2-2 1 9Mean (SEM) 2-0 (0-2) 1-8 (0-2)
exercise during room air inhalation, but therewere no significant changes in AT-II through-out the exercise test during cold air inhalation(table 5).
DiscussionIn the investigation of cold intolerance inpatients with angina, consideration has to begiven to the potential differences between theeffects of a cold environment and those ofcold air inhalation. The results of this studyindicate that in patients with chronic stableangina, cold air inhalation results in an earlieronset of angina and a fall in overall exercisecapacity. It is the first study to demonstratecold intolerance whilst breathing moderatelycold air and indicates that cold air inhalationper se is an important factor in the phenome-non of cold intolerance. Peripheral ET-1 or
AT-II do not appear to play a significant role inthe mechanism of cold induced angina, butthis is the first study to demonstrate a fall inET-1 levels during exercise in patients withchronic stable angina.
For many patients with ischaemic heart dis-ease, cold weather produces a deterioration intheir symptoms and a reduction in exercisecapacity. Furthermore, there is an overallincrease in cardiac mortality during coldspells,17 and a Canadian study has associatedrapid drops in temperature with increasingdeaths from coronary artery disease.18 Ofthe two reflexk responses that have been pro-posed to explain the phenomenon of cold
28

Vasoconsttictor peptides and cold intolerance in patients with stable angina pectoris
intolerance, published data in the setting of acold environment have suggested that anincrease in peripheral vascular resistanceresulting in an increase in cardiac work forany given level of exercise is the more impor-tant mechanism.67 This theory, however, hasnot met with universal support. Juneau et al19found that a subgroup of eight cold sensitivepatients developed 1 mm ST depression 30%sooner during treadmill exercise testing in acold chamber at - 8°C compared with that at20°C. The rate-pressure product (heart ratex systolic blood pressure) at the onset of1 mm ST depression was significantly lowerin the cold, suggesting that ischaemia wasoccurring at a lower myocardial oxygen con-sumption. Juneau et al concluded that areduction in coronary flow could explain theearlier onset of ischaemia in the cold.The results of the present study suggest
that a combination of both peripheral andcentral mechanisms could explain the phe-nomenon of cold induced angina during coldair inhalation. Cold air inhalation resulted in asignificant reduction in the time to angina (fig1(A)), with no significant difference in therate-pressure product at this time point ateach visit (table 1). Rate-pressure product hasbeen shown to correlate well with myocardialoxygen consumption,20 and therefore the ear-lier onset of angina during cold inhalation canbe attributed to an increase in cardiac work.At each visit there was no significant differ-ence in systolic blood pressure or heart rate atthe onset of angina, suggesting that theincreased myocardial oxygen consumptionduring cold air inhalation is likely to havebeen caused by a combination of the increasein both these variables. Cold exposure inpatients with angina has been shown to pro-duce peripheral vasoconstriction and a rise inblood pressure,2 mediated via cold receptorsin the skin which stimulate an increase insympathetic outflow to the peripheral vessels.As cold receptors are also located in the upperairways, cold air inhalation is likely to stimu-late these receptors and trigger a reflexincrease in peripheral vascular resistance, arise in blood pressure and an increase in car-diac work. Similarly, a sympathetically medi-ated reflex increase in heart rate during coldair inhalation would result in increased heartwork.
In contrast, cold air inhalation resulted in asignificant reduction in total exercise time,and this time point was reached at a signifi-cantly lower rate-pressure product comparedwith that of room air. This suggests thatmyocardial oxygen consumption was lower atpeak exercise during cold air inhalation thanat the same time point during room air inhala-tion. The implication of this result is that acentral mechanism such as a reduction incoronary flow is the major determinant ofmaximal exercise capacity during cold airinhalation. Overall, the results of the studysuggest that peripheral reflex responsesaccount for the earlier onset of angina duringcold air inhalation, but as exercise continuesthen central mechanisms play an increasing
role in the pathophysiology and determine apatient's overall exercise capacity.
Although there was a trend towards adecrease in the time to 1 mm ST depressionin patients breathing cold air as opposed toroom air, this failed to reach statistical signifi-cance. This could be explained by the size ofthe study group, and the change in this exer-cise test parameter may well have become sig-nificant if a larger number of patients hadbeen studied. Furthermore, it is difficult toestablish the effect of patient expectation dur-ing the cold air exercise test. Some patientsmay have assumed that they would experienceangina sooner during the cold air exercise test,and this may have resulted in the early onsetof chest pain and termination of exercisebefore the appearance of significant STchanges on the electrocardiogram.
Division of the study group into patientstolerant and intolerant to cold showed a sig-nificant reduction in the time to angina inpatients tolerant to cold breathing cold aircompared with that of breathing room air.Although there was a trend towards a reduc-tion in the time to angina in patients intoler-ant to cold breathing cold air, this failed toreach statistical significance. One potentialexplanation for this finding is that patientsintolerant to cold have developed an adaptivemechanism and are partially conditioned tothe cold. This conditioning may modify theirresponse to formal exercise testing duringcold air inhalation, thus delaying the onset ofsymptoms and improving their overall exer-cise capacity. This adaptive response may notoccur in patients tolerant to cold. In addition,it is uncertain as to the effect of patient expec-tation (that is-reluctance to go outdoors dur-ing cold weather, mode of dress) on theresults. Patients who do not complain of coldintolerance may not have been exposed to, ormay have taken steps to avoid, the phenome-non. Furthermore, clearly outdoor conditionsare not exactly mimicked in the laboratorysetting, and this could also contribute to theseobserved differences. In general, however, wewould expect that the face is the only area sig-nificantly exposed to the cold, and that inhala-tion of cold air to be the major effect of coldweather.
Although increased endothelin and renin-angiotensin levels have been demonstrated inpatients following acute myocardial infarc-tion,2' 22 whether these vasoactive peptides areactivated during episodes of acute myocardialischaemia is less well defined. Raised AT-IIlevels have been detected in response to pac-ing induced ischaemia in patients with stableangina,'6 but no data are available on thepossible part played by either ET-1 or AT-IIin the pathophysiology of cold inducedangina.
In the present study, there was a similarsignificant decrease in ET-1 concentrationsat peak exercise compared with that at restirrespective of whether the patients werebreathing room or cold air. Concentrations ofET-1 returned to resting levels 10 min afterpeak exercise during the warm air exercise
29

Dodds, Bellamy, Muirhead, Perry
test, but remained significantly reduced com-pared with resting levels 10 min after peakexercise during the cold air exercise test. Theeffect of exercise on ET- 1 has not been studiedin man, although a decrease in the meanplasma concentration of ET-1 after exerciseperformed until semi-exhaustion or exhaus-tion has been demonstrated in rats.23 Thedecrease in ET-1 concentrations seen in ourstudy group at peak exercise could be theresult of its rapid removal by different tissues,especially the lungs, during exercise. Overall,the findings of our study suggest that periph-eral ET-1 does not play a significant role inthe phenomenon of cold intolerance inpatients with stable angina.
There was a significant increase in AT-IIconcentrations 10 min after peak exercisecompared with that at both rest and peakexercise in patients breathing room air.During cold air inhalation, however, therewere no significant changes in AT-II concen-trations. A rise in AT-II levels in response toexercise has been demonstrated in normalmen,24 with exercise stimulating the secretionof renin via sympathetic stimulation of thejuxtaglomerular apparatus and by othermechanisms such as a loss of sodium and areduction in the extracellular volume throughsweating. Consequently, plasma renin activityand the plasma concentration of AT-II riseduring exercise. In addition, exercise inducedmyocardial ischaemia in patients withischaemic heart disease may produce left ven-tricular dysfunction, and subsequent renalhypoperfusion could also result in reninrelease from the kidney.When the study group were breathing room
air, their exercise capacity and maximal work-load would have been less than that of normalsubjects undergoing maximal exercise testing.Consequently, although activation of themechanisms stimulating a rise in the level ofAT-II would have started during exercise test-ing, they would not have produced a signifi-cant increase in AT-II by the time that theexercise was completed. It seems likely thatthese mechanisms will remain active at leastduring the early stages of recovery and resultin a significant rise in AT-II 10 min after peakexercise. There was a significant reduction intotal exercise time in patients breathing coldair as opposed to room air, and therefore it islikely that there was little stimulation of therenin-angiotensin response to exercise beforepeak exercise was reached. This may explainthe fact that there were no significant changesin AT-II concentrations with exercise duringcold air inhalation. This possibility seemsmore likely than any effect of ischaemiainduced left ventricular dysfunction on AT-II,as there was no significant difference in maxi-mal ST depression during exercise with eitherroom air or cold air inhalation (table 6).Similar to the ET-1 findings, it appearsunlikely that peripheral AT-II plays a signifi-cant role in the pathophysiology of cold intol-erance in patients with stable angina.The results of the present study differ from
the previously reported effects of cold air
inhalation in patients with angina.Hattenhauer and Neill9 studied a populationof 33 male patients with coronary artery dis-ease, 11 of whom gave a positive history ofcold intolerance. Seventeen of these patientsunderwent inhalation of cold air at - 20°C for4 min, and this resulted in typical angina atrest in four patients. Cold air inhalation alsoproduced angina in four of the seven patientswho were paced at a heart rate which was sub-anginal at room temperature. Cold air inhala-tion did not significantly increase myocardialoxygen consumption, or alter coronary bloodflow determined by the xenon clearancemethod. In a separate arm of the Hattenhauerand Neill study, cold air inhalation for 90 s in18 patients produced no detectable-constric-tion of coronary arteries visualized arterio-graphically. The authors concluded fromthese findings that cold induced angina couldnot be explained by an increase in cardiacwork and myocardial oxygen consumption. Inaddition, as neither large coronary artery norgeneralized coronary arteriole constrictionseemed to occur during cold air inhalation,the authors proposed that cold inducedangina could be the result of constriction ofminute coronary collaterals or other vesselsspecifically affecting blood flow to potentiallyischaemic regions of the myocardium. Thedifferences between the results ofHattenhauer and Neill and the present studyare likely to be a consequence of the use ofdifferent modalities of stress testing, particu-larly as atrial pacing is a relatively non-physio-logical form of exercise testing. Furthermore,a greater proportion of patients in the presentstudy gave a positive history of cold intoler-ance (75% v 33%).
Lassvik and Areskog10 studied 12 malepatients with exertional angina and a positivehistory of cold intolerance using exercise bicy-cle tests with separation of inspiratory androom air. They demonstrated that inhalationof moderately cold (-10°C) or very cold(- 35°C) air whilst resting in a room at 20°Cproduced no change in heart rate, systolicblood pressure or rate-pressure product com-pared with that of pontrol conditions (inhala-tion of air at 20°C in a room at 20°C).Inhalation of cold air at - 35°C in a room at20°C resulted in a significant decrease in workcapacity expressed as workload at the onset ofangina and maximal workload compared withthat of control conditions. There was no sig-nificant difference between the rate-pressureproducts at maximal workload in control con-ditions and during cold air (- 35°C) inhala-tion, and the authors concluded that thedecrease in work capacity during very cold airinhalation was because of an increase in car-diac work and myocardial oxygen demand.Lassvik and Aveskog,1' however, failed todemonstrate any decrease in workload ateither the onset of angina or maximal work-load during inhalation of moderately cold air(- 10°C) in a room at 20°C.One potential limitation in our study is that
during the control exercise tests the patientswere not wearing a mask or breathing through
30
Vasoconstrictor peptides and cold intolerance in patients with stable angina pectoris
the same equipment as they did during thecold air exercise tests. This raises the possibil-ity that during the cold air tests patients per-formed additional work in breathing throughthe face mask and accompanying equipment,contributing to the earlier onset of angina andreduction in overall exercise capacity. Thespecially adapted freezer, however, containeda small fan unit capable of providing cold airat a maximum rate of 150 I/min, connected tothe face mask by a short piece of 38 1 mmdiameter hose. This equipment ensured thatthe cold air was actively supplied to thepatient and that no extra work was required tobreathe through the face mask and accom-panying equipment.
Another potential limitation of our work isthat laboratory conditions do not exactlyreplicate the outdoor conditions experiencedby patients during cold weather. It is difficultto accurately reproduce outdoor conditions inan exercise room, but our study does showthat breathing cold air is an important factorin the pathophysiology of cold inducedangina. In response to strong winds, snow andfreezing temperatures patients normally wearwarm clothing such as coats, gloves and hats,but pay little attention to protecting them-selves from the effects of direct cold airinhalation. Our work suggests that such prac-tices as covering ones nose and mouth with ascarf or other such accessory may help to limitthe effect of direct cold air inhalation andimprove the patient's exercise capacity duringcold spells.
ConclusionWhen investigating the mechanisms involvedin cold induced angina, potential differencesexist between the response to cold air inhala-tion and the effects of a cold environment.Cold air inhalation in patients with chronicstable angina results in an earlier onset ofsymptoms and a significant reduction in exer-cise capacity. Haemodynamic data suggestthat a combination of peripheral and centralreflex mechanisms is the most likely explana-tion for these clinical findings.
There was a similar significant decrease inconcentrations of ET-1 during exercise test-ing irrespective of the temperature of theinhaled air, and a significant increase in AT-IIconcentrations in response to exercise whilebreathing room air which was not repeatedduring cold air inhalation. Peripheral ET-1and AT-II do not appear to play a part in thepathophysiology of cold intolerance inpatients with stable angina.
Further work into cold intolerance inpatients with angina should aim at clarifying
potential central reflex mechanisms andexplore a possible central action for vasoactivepeptides.
1 Hall RJC, Bullock RE, Albers C. The effect of cold onpatients with angina pectoris-a review. Postgrad MedJ1983;59 (suppl 2):55-7.
2 Epstein SE, Stampfer M, Beiser GD, Goldstein RE,Braunwald E. Effects of a reduction in environmentaltemperature on the circulatory response to exercise inman. Implications concerning angina pectoris. N Engl JfMed 1969;280:7-1 1.
3 Hayward JM, Holmes WF, Gooden BA. Cardiovascularresponses in man to a stream of cold air. Cardiovasc Res1976;10:691-6.
4 Raizner AE, Chahine RA, Ishimori T, Verani MS, ZaccaN, Jamal N, et al. Provocation of coronary artery spasmby the cold pressor test. Hemodynamic, arteriographicand quantitative angiographic observations. Circulation1980;62:925-32.
5 Nabel EG, Ganz P, Gordon JB, Alexander RW, SelwynAP. Dilation of normal and constriction of athero-sclerotic coronary arteries caused by the cold pressortest. Circulation 1988;77:43-52.
6 Lassvik CA, Areskog NH. Angina in cold environmentReactions to exercise. BrHeartJ 1979;42:396-401.
7 Peart I, Bullock RE, Albers C, Hall RJC. Cold intolerancein patients with angina pectoris: effect of nifedipine andpropranolol. BrHeartJ 1989;61:521-8.
8 Leon DF, Amidi M, Leonard JJ. Left heart work and tem-perature responses to cold exposure in man. Am JCardiol 1970;26:38-45.
9 Hattenhauer M, Neil WA. The effect of cold air inhala-tion on angina pectoris and myocardial oxygen supply.Circulation 1975;51:1053-8.
10 Lassvik CA, Areskog NH. Angina pectoris during inhala-tion of cold air Reactions to exercise. Br Heart J 1980;43:661-7.
11 Miyauchi T, Tomobe Y, Shiba R, Ishikawa T, YanagisawaM, Kimura S, et al. Involvement of endothelin in theregulation of human vascular tonus. Potent vasocon-strictor effect and existence in endothelial cells.Circulation 1990;81:1874-80.
12 Chester AH, Dashwood MR, Clarke JG, Larkin SW,Davies GJ, Tadjkarimi S, et al. Influence of endothelinon human coronary arteries and localization of its bindingsites. AmY Cardiol 1989;63:1395-8.
13 Fyhrquist F, Saijonmaa 0, Metsarinne K, Tikkanen I,Rosenlof K, Tikkanen T. Raised plasma endothelin-Iconcentration following cold pressor test. BiochemBiophys Res Commun 1990;169:217-21.
14 Zamora MR, O'Brien RF, Rutherford RB, Weil JV. Serumendothelin-I concentrations and cold provocation inprimary Raynaud's phenomenon. Lancet 1990;336:1144-7.
15 Shechtman 0, Fregly MJ, van-Bergen P, Papanek PE.Prevention of cold-induced increase in blood pressure ofrats by captopril. Hypertension 1991;17(6 pt 1):763-70.
16 Remme WJ, de Leeuw PW, Bootsma M, Look MP,Kruijssen DACM. Systemic neurohumoral activationand vasoconstriction during pacing-induced acutemyocardial ischaemia in patients with stable angina pec-toris. Am J Cardiol 1991;68:181-6.
17 Rose G. Cold weather and ischaemic heart disease. Br JPrev Soc Med 1966;20:97-100.
18 Anderson TW, Rochard C. Cold snaps, snowfall andsudden death from ischaemic heart disease. Can MedAssocJ 1979;121:1580-3.
19 Juneau M, Johnstone M, Dempsey E, Waters DD.Exercise-induced myocardial ischemia in a cold environ-ment. Effect of antianginal medication. Circulation 1989;79:1015-20.
20 Gobel FL, Nordstrom LA, Nelson RR, Jorgensen CR,Wang Y. The rate-pressure product as an index ofmyocardial oxygen consumption during exercise inpatients with angina pectoris. Circulation 1978;57:549-56.
21 Ray SG, McMurray Jj, Morton JJ, Dargie HJ. Circulatingendothelin in acute ischaemic syndromes. Br Heart J1992;67:383-6.
22 Dargie HJ, McAlpine HM, Morton Jj. Neuroendocrineactivation in acute myocardial infarction. J CardiovascPharmacol 1987;9 (suppl 2):S21-4.
23 Allevard AM, Gauquelin G, Gharib C. Endothelin andatrial natriuretic peptide after exercise performed untilexhaustion in the rat. Life Sci 1991;49:1803-8.
24 Staessen J, Fagard R, Hespel P, Lijnen P, Vanhees L,Amery A. Plasma renin system during exercise in normalmen. YAppl Physiol 1987;63:188-94.
31