vitamin d reynald altema, md. consequences of low vit d 1-↑ cardiovascular risk factors. 2-↑...
TRANSCRIPT
VITAMIN D
REYNALD ALTEMA, MD
CONSEQUENCES OF LOW VIT D
1-↑ Cardiovascular risk factors.
2-↑ All-cause mortality.
3-↑ Risk of cancer of breast, colon.
A-Martins et al. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the United States: data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2007, 167, 1159-1165.
B-Melamed et al. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch Intern Med. 2008 Aug 11;168(15):1629-37.
C-Giovannuci, E. Vitamin D and Cancer in the Harvard Cohorts. Ann of Epidemiology. 2009;19-84-88.
BASIC PHYSIOLOGY 2 Sources of Vit D:
A- Diet- small amount.
B-Skin upon exposure to sunlight. Major source.
Vit D synthesis 7-DehydroCholesterol uv light
Cholecalciferol (D3) for maximum of 20,000 IU/ day
Cholecalciferol liver
Calcidiol
Calcidiol aka 25-OH Vit D

Vit D synthesis
Calcidiol
Calcitriol (kidney)Pathway 1
Cacitriol(tissue)
Pathway 2
Calcitriol in blood

Vitamin D
Unit of Vitamin D concentration:
1-ng/ml
2-nmole/L (#1 x 2.5)
Normal values:
At least 30 ng/ml.
Dose of Vitamin D:
International Units (IU).

Testing for Vit DCalcidiol, i.e. 25-OH Vit D and not 1,25-OH
Vit D.
Calcidiol represents the storage status of Vit
D. No good relation exists between level of
Calcitriol (1,25-OH Vit D) and reserve of Vit
D.
Cheapest cost $47.25 for Life Extension
Member (lef.org).
Vitamin DCholecalciferol aka D3.
available over the counter.
Dose 1,000-10,000 International Units.
Usual dose 4 to 5,000 IU a day.
Calcitriol
Available as prescription only. Rocaltrol, Hectorol, Zemplar (IV route). Latter two are used when kidneys are unable to make Calcitriol.
Vitamin D
Ergocalciferol- aka D2- derived from plants.
Commercially available as either Drisdol or
Calciferol. Less potent than Cholecalciferol.
Dose is usually 30,000-50,000 International
Units weekly or monthly.

Vitamin D
Holick, M. Molecular Aspects of Medicine. Dec 2008. 29(6). 361-368.
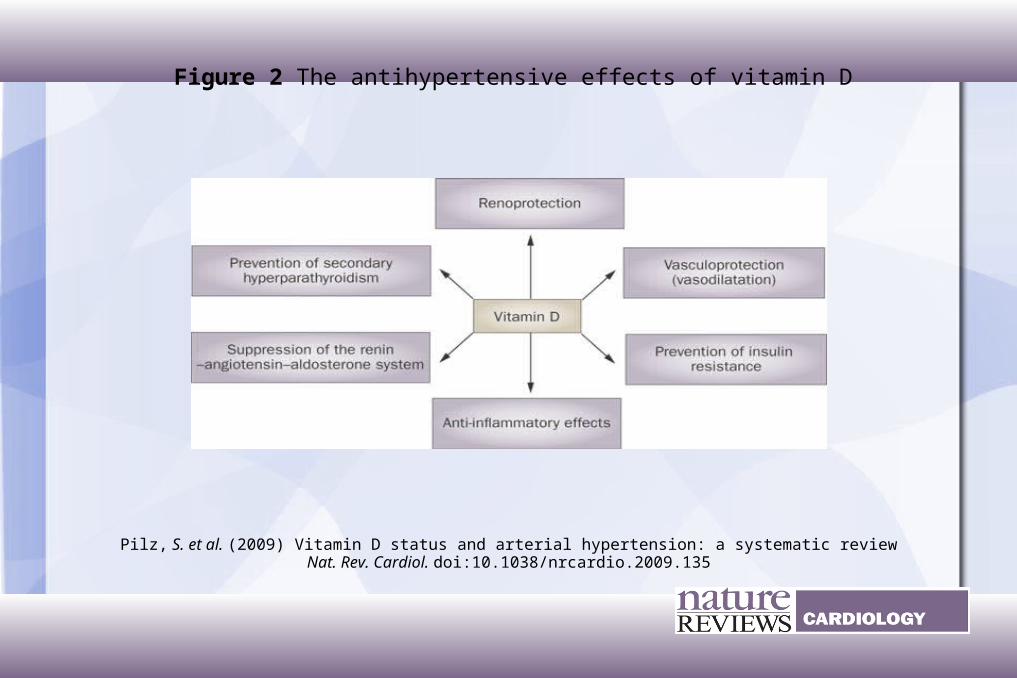
Figure 2 The antihypertensive effects of vitamin D
Pilz, S. et al. (2009) Vitamin D status and arterial hypertension: a systematic reviewNat. Rev. Cardiol. doi:10.1038/nrcardio.2009.135
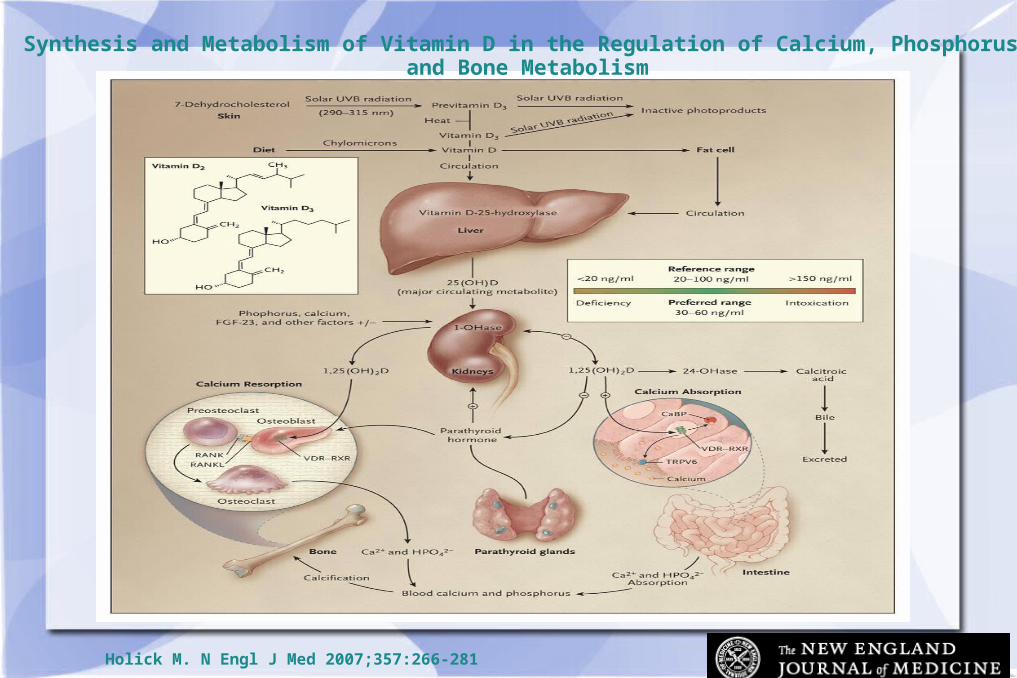
Synthesis and Metabolism of Vitamin D in the Regulation of Calcium, Phosphorus, and Bone Metabolism
Holick M. N Engl J Med 2007;357:266-281
Holick M. N Engl J Med 2007;357:266-281
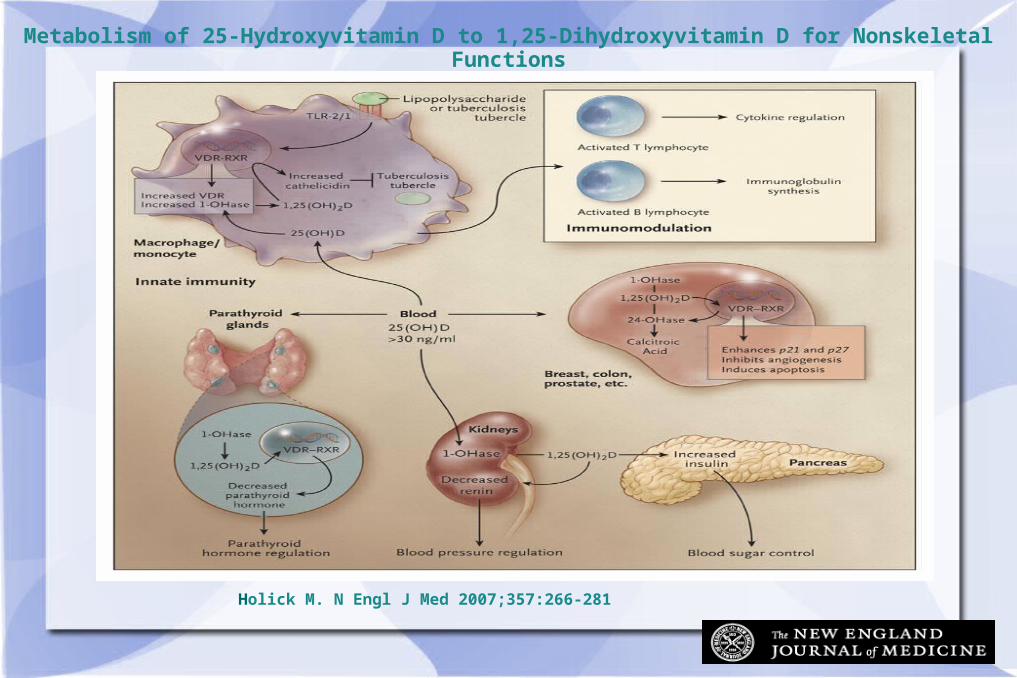
Metabolism of 25-Hydroxyvitamin D to 1,25-Dihydroxyvitamin D for Nonskeletal Functions

Holick, M. Molecular Aspects of Medicine.Dec 2008. 29(6). 361-368.
F.C. Campbell et al. The Yin and Yang of vitamin D receptor (VDR) signaling in neoplastic progression: . Biochem Pharmacol. 2010 January 1 79(1): 1–9.

Notwithstanding the wide distribution of VDR and CYP27B1, 1α,25-(OH)2 D3 shows highly tissue-specific functional effects on hormone secretion, immune function, cell differentiation and growth. For example, 1α,25-(OH)2 D3 inhibits PTH secretion in the parathyroid glands [30] but stimulates pancreatic β-cell insulin secretion [50], inhibits adaptive immunity [51] but enhances some innate immune responses [52], inhibits differentiation of B lymphocytes [53] but enhances keratinocyte differentiation [54].
F.C. Campbell et al. The Yin and Yang of vitamin D receptor (VDR) signaling in neoplastic progression: Operational networks and tissue-specific growth control. Biochem Pharmacol. 2010 January 1; 79(1): 1–9.
.
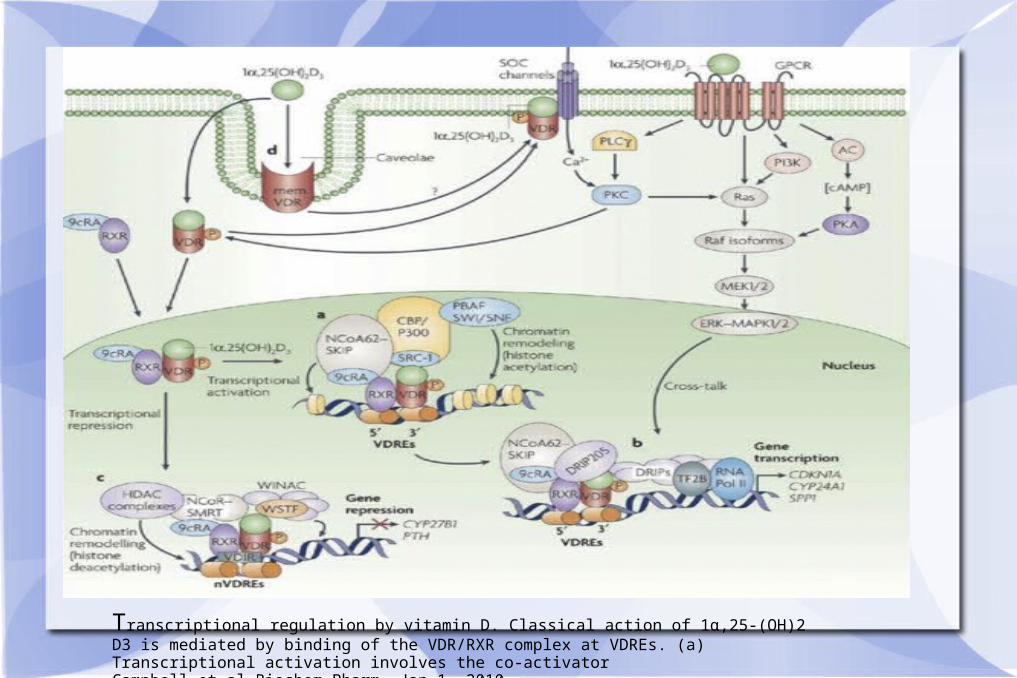
Transcriptional regulation by vitamin D. Classical action of 1α,25-(OH)2 D3 is mediated by binding of the VDR/RXR complex at VDREs. (a) Transcriptional activation involves the co-activator Campbell et al.Biochem Pharm. Jan 1, 2010.
Vitamin D and cofactorsVit D works best when cofactors are available: Mg,
Boron,Vit K2, Zinc. Mg is most important. Sources of Mg: seeds, nuts, green veggies, dried fruits.
Vit D and Retinol (active form of Vit A):
competitively fight for same cellular receptor.
Vit D receptor and Retinoid X Receptor form a complex inside the nucleus.
Dose of B-carotene/day is 1-2,000 IU.
Cod liver oil may contain too much Vit A.

Holick, M. Molecular Aspects of Medicine.Dec 2008. 29(6). 361-368.
Colon, prostate, skin, monocytes among other tissues and cells can convert 25-hydroxyvitamin D [25(OH)D] to 1, 25-dihydroxyvitamin D [1,25(OH)2D]. Once formed within the cell, it can induce a wide variety of genes by interacting with its vitamin D receptor to regulate differentiation, proliferation, and apoptosis.
Holick, M. (ibidem).

Vitamin D mechanisms• Vitamin D and its metabolites reduce the incidence of many
types of cancer by inhibiting tumor angiogenesis
• stimulating mutual adherence of cells.
• and enhancing intercellular communication through gap junctions, thereby strengthening the inhibition of proliferation that results from tight physical contact with adjacent cells within a tissue (contact inhibition).
• Vitamin D metabolites help maintain a normal calcium gradient in the colon epithelial crypts.
• 1,25(OH)2D inhibits mitosis of breast epithelial cells. Pulsatile release of ion-ized calcium from intracellular stores, including the endoplasmic reticulum, induces terminal differentiation and apoptosis, and 1,25(OH)2D enhances this release. Garland F. et al. Am J Public Health. 2006 February; 96(2): 252–261.
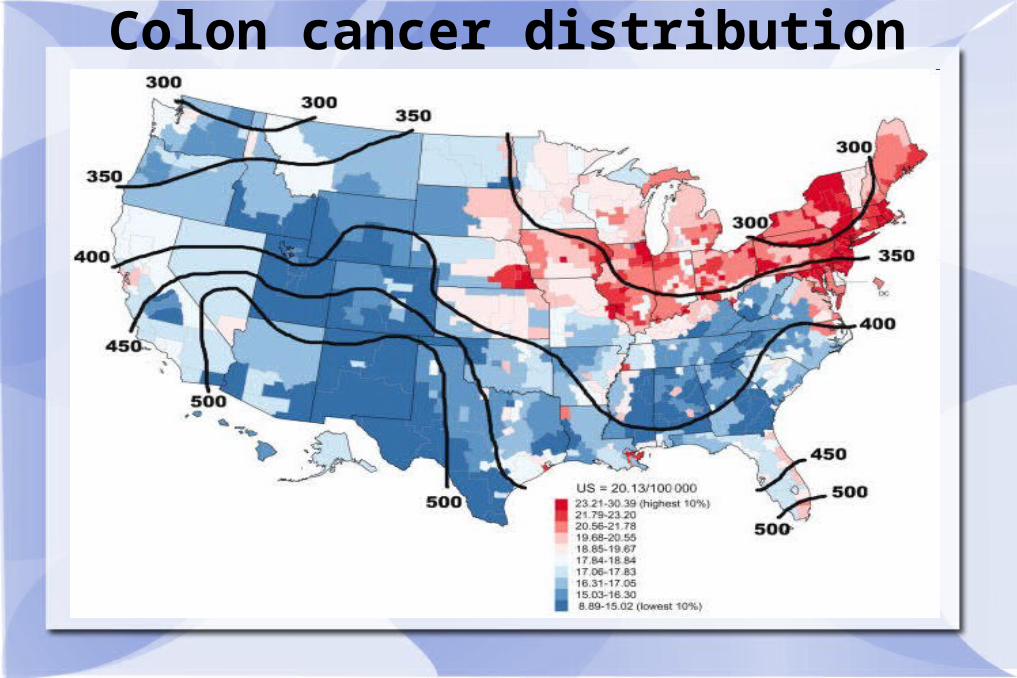
Colon cancer distribution

Breast cancer distribution
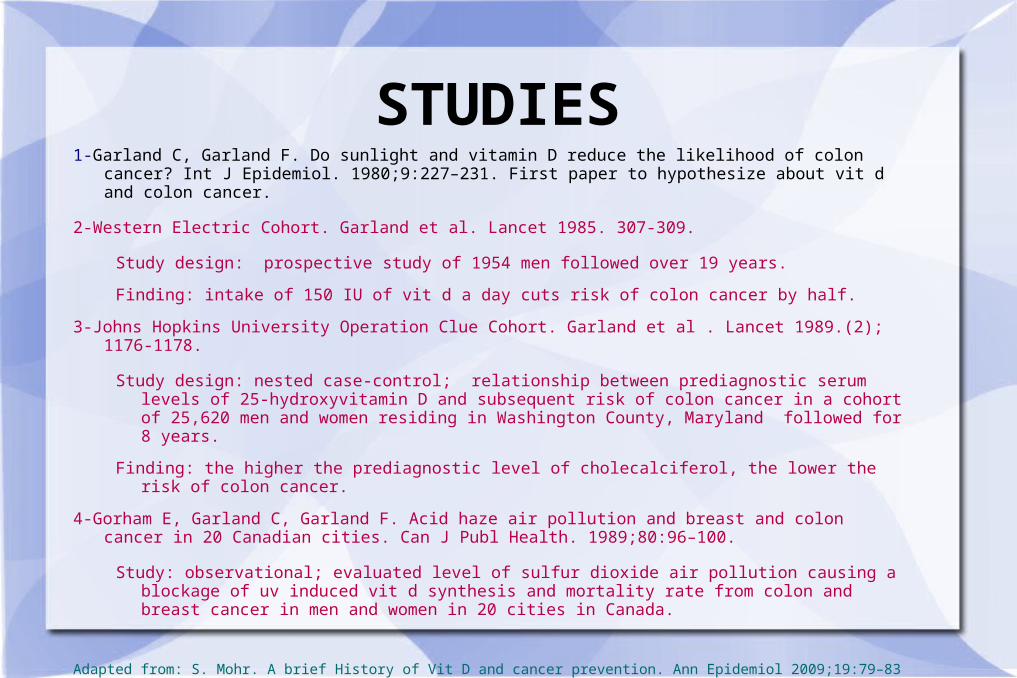
STUDIES1-Garland C, Garland F. Do sunlight and vitamin D reduce the likelihood of colon cancer? Int J
Epidemiol. 1980;9:227–231. First paper to hypothesize about vit d and colon cancer.
2-Western Electric Cohort. Garland et al. Lancet 1985. 307-309.
Study design: prospective study of 1954 men followed over 19 years.
Finding: intake of 150 IU of vit d a day cuts risk of colon cancer by half.
3-Johns Hopkins University Operation Clue Cohort. Garland et al . Lancet 1989.(2); 1176-1178.
Study design: nested case-control; relationship between prediagnostic serum levels of 25-hydroxyvitamin D and subsequent risk of colon cancer in a cohort of 25,620 men and women residing in Washington County, Maryland followed for 8 years.
Finding: the higher the prediagnostic level of cholecalciferol, the lower the risk of colon cancer.
4-Gorham E, Garland C, Garland F. Acid haze air pollution and breast and colon cancer in 20 Canadian cities. Can J Publ Health. 1989;80:96–100.
Study: observational; evaluated level of sulfur dioxide air pollution causing a blockage of uv induced vit d synthesis and mortality rate from colon and breast cancer in men and women in 20 cities in Canada.
Adapted from: S. Mohr. A brief History of Vit D and cancer prevention. Ann Epidemiol 2009;19:79–83
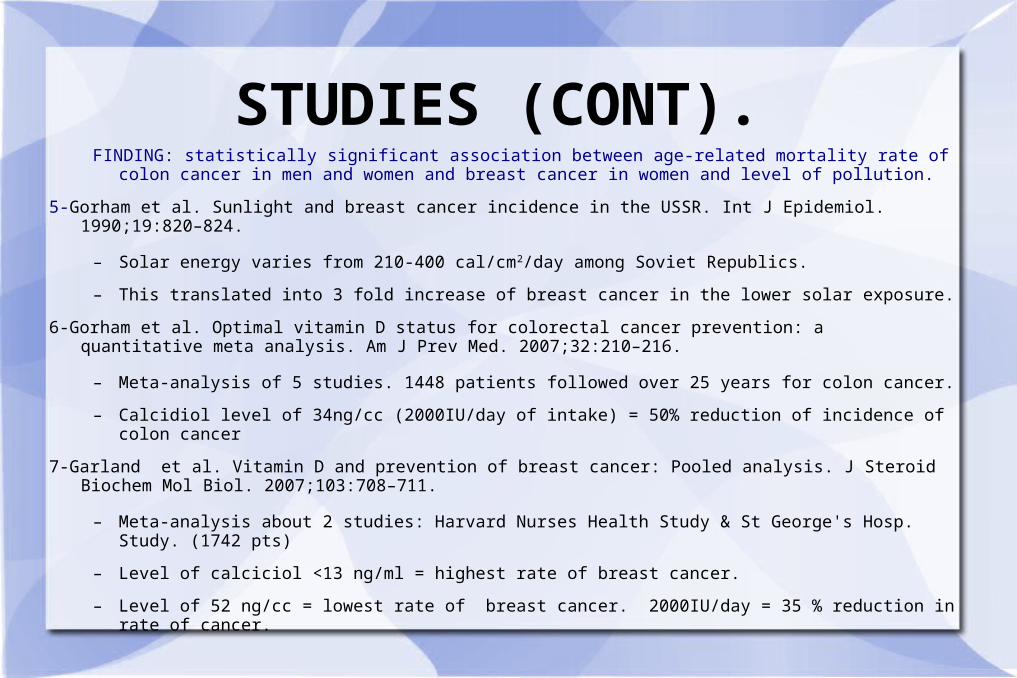
STUDIES (CONT).FINDING: statistically significant association between age-related mortality rate of colon cancer in men
and women and breast cancer in women and level of pollution.
5-Gorham et al. Sunlight and breast cancer incidence in the USSR. Int J Epidemiol. 1990;19:820–824.
– Solar energy varies from 210-400 cal/cm2/day among Soviet Republics.
– This translated into 3 fold increase of breast cancer in the lower solar exposure.
6-Gorham et al. Optimal vitamin D status for colorectal cancer prevention: a quantitative meta analysis. Am J Prev Med. 2007;32:210–216.
– Meta-analysis of 5 studies. 1448 patients followed over 25 years for colon cancer.
– Calcidiol level of 34ng/cc (2000IU/day of intake) = 50% reduction of incidence of colon cancer
7-Garland et al. Vitamin D and prevention of breast cancer: Pooled analysis. J Steroid Biochem Mol Biol. 2007;103:708–711.
– Meta-analysis about 2 studies: Harvard Nurses Health Study & St George's Hosp. Study. (1742 pts)
– Level of calciciol <13 ng/ml = highest rate of breast cancer.
– Level of 52 ng/cc = lowest rate of breast cancer. 2000IU/day = 35 % reduction in rate of cancer.
STUDIESHARVARD COHORTS
1-Nurses' Health Study (NHS).1980-2002; over 47,000 nurses; 2747 cases of adenoma. Low Vit A intake (<2646 IU/day) and elevated Vit D intake yields reduced rate of colon & rectal adenoma in postmenopausal women not on Estrogens.
Breast cancer. Reduced rate with elevated Vit D intake; conflicting result on menopause.
2-Health Professionals Follow-up Study (HPFS). 1986-2000. 691 cases of cancer; 47,000 cohorts. Independent variables such as exposure to sun, Vit D intake, geographical location, BMI. Increment of 25 nMole/L yields reduced rate of colon cancer.
African-American men have 32% higher risk of cancer (specially in GI tract) and 89% greater risk of mortality compared to white men.
3-Physicians' Health Study.
Giovannuci, E. Vitamin D and Cancer in the Harvard Cohorts. Ann of Epidemiology. 2009;19-84-88.
Vit D and MyocyteElevated parathyroid hormone (PTH) levels are commonly observed in patients with vitamin D deficiency to maintain
normal serum calcium levels despite insufficient vitamin D effects on calcium metabolism [50]. Secondary hyperparathyroidism has been associated with increased risk of cardiovascular diseases [50]. Deleterious PTH effects on the vessels and the myocardium suggest that increased PTH is a causal pathophysiologic link between vitamin D deficiency and myocardial diseases [50].
Apart from this, accumulating evidence exists that vitamin D deficiency indirectly contributes to the development of arterial hypertension, diabetes mellitus, dyslipidemia, and other cardiovascular risk factors [51-53]. It was also shown that vitamin D exerts direct anti-atherosclerotic effects on endothelial and vascular smooth muscle cells [3][4][51]. Hence, it is conceivable that vitamin D might prevent ischemic myocardial diseases by direct anti-atherosclerotic effects and by beneficial effects on cardiovascular risk factors. However, associations of vitamin D deficiency with vascular diseases have not been consistently observed and there exists some controversy about the causality of the link between the low 25(OH)D levels and the development of atherosclerosis [3][51][54].
Several infectious diseases can affect the myocardium and the cardiac valves and can thus contribute to myocardial diseases by causing arrhythmias, myocardial dysfunction, and valvular heart diseases. Given that vitamin D plays an important role for the immune system including resistance to infectious diseases, it could be hypothesized that a sufficient vitamin D status might prevent myocardial diseases by reducing the incidence of infections of the heart [55]. Moreover, the increased prevalence of autoimmune diseases in vitamin D-deficient individuals and the proposed involvement of autoimmunological processes in the development of heart diseases suggest that anti-autoimmunological properties of vitamin D might be another protective mechanism against myocardial diseases [4][56]. Finally, further evidence exists that vitamin D exerts anti-inflammatory and anti-oxidative effects on the myocardium [1-4].
Plitz et al. March 29 2010
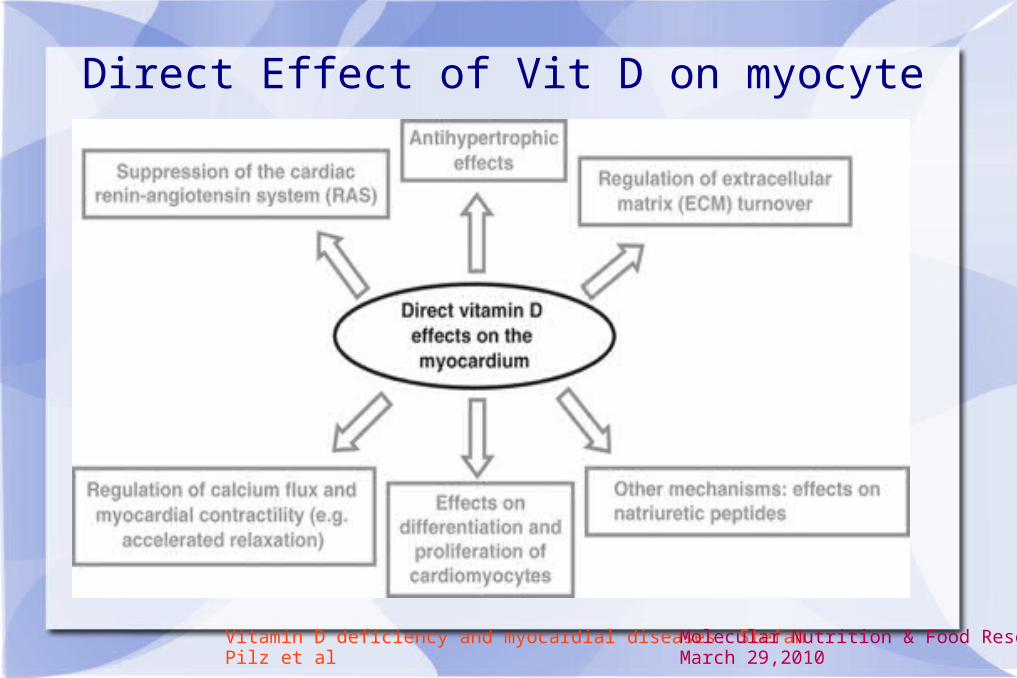
Direct Effect of Vit D on myocyte
Vitamin D deficiency and myocardial diseases. Stefan Pilz et alMolecular Nutrition & Food Research. March 29,2010
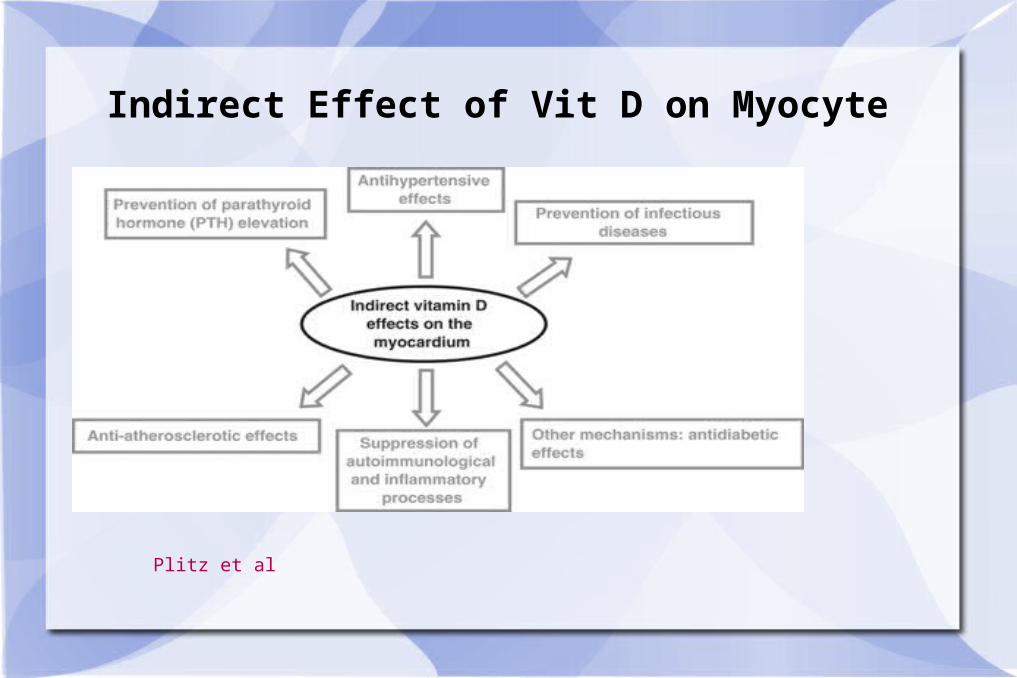
Indirect Effect of Vit D on Myocyte
Plitz et al
Vit D & Infectious Diseases1-Vitamin D3, gamma interferon, and control of proliferation of Mycobacterium
tuberculosis by human monocytes. G A Rooke et al, Immunology. 1986 January; 57(1): 159–163
Famous article that proves that in the presence of Vit D, infected monocyte develops Anti TB activity. Mechanism of action: Calcitriol induces antimicrobial peptide “cathelicidin.”
2-Yamshchikov et al. VITAMIN D FOR TREATMENT AND PREVENTION Of INFECTIOUS DISEASES: A SYSTEMATIC REVIEW OF RANDOMIZED CONTROLLED TRIALS. Endocr Pract. 2009 Jul–Aug; 15(5): 438–449
Exhaustive review of controlled trials from 1948 to 2009 of intervention and treatment of infectious diseases in humans using Vit D. 13 studies; 10 had placebo groups. 9/10 were controlled, double-blind studies. “On the basis of studies reviewed to date, the strongest evidence supports further research into adjunctive vitamin D therapy for tuberculosis, influenza, and viral upper respiratory tract illnesses.”

Vit D and Infectious Diseases
Problems identified:
1-Dose of Vit D given not standardized. Some studies use higher doses than others.
2-Duration of observation varies.
Patterns observed: Higher dose of Vit D improvement.

SPECIAL CASES1-Vit D and Chronic kidney disease
In patients with any stage of chronic kidney disease, 25-hydroxyvitamin D should be measured annually, and the level should be maintained at 30 ng per milliliter or higher, as recommended in the Kidney Disease Outcomes Quality Initiative guidelines from the National Kidney Foundation.6,91,93,94 It is a misconception to assume that patients taking an active vitamin D analogue have sufficient vitamin D; many do not. Levels of 25-hydroxyvitamin D are inversely associated with parathyroid hormone levels, regardless of the degree of chronic renal failure.2,6,93,94,95,96 Parathyroid glands convert 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, which directly inhibits parathyroid hormone expression.6,93,94,95,96,120 Patients with stage 4 or 5 chronic kidney disease and an estimated
glomerular filtration rate of less than 30 ml per minute per 1.73 m2 of body-surface area, as well as those requiring dialysis, are unable to make enough 1,25-dihydroxyvitamin D and need to take 1,25-dihydroxyvitamin D3 or one of its less calcemic analogues to maintain calcium metabolism and to decrease parathyroid hormone levels and the risk of renal bone disease (Table 3).6,91,93,94
Holick, M. NEJM 2007; 357:266-281.M

SPECIAL CASESSARCOIDOSIS
1- Hypercalcemia is a common complication.
2- It is due to Calcitriol overproduction by macrophage.
3- Vitamin D should not be given to patients with Sarcoidosis.
4-Corticosteroids are the drug of choice.
Second tier drugs: Chloroquine, Hydroxychloroquine and
Ketoconazole.
Sharma O. P., Vitamin D, Calcium and Sarcoidosis. Chest 1996; 109: 535-539