vitreomacular traction
TRANSCRIPT

VITREOMACULAR TRACTION

DEFINITION Disorder of the vitreo-retinal interface
characterized by: 1) an incomplete posterior vitreous detachment
(PVD)2) an abnormally strong adherence of the posterior
hyaloid face to the macula and3) anteroposterior traction exerted by the syneretic
vitreous pulling at adherent sites on the macula causing morphologic and often functional effects.

HISTORY• In 1953, Irvine described a vitreous tug syndrome caused
by vitreous incarceration at the corneal wound site following intra- and extra- capsular cataract extraction leading to cystoid macular edema (CME) from vitreomacular traction1
• In 1967, Jaffe described ‘vitreoretinal traction syndrome’ in 14 patients as a distinct entity. The condition he described mostly affected phakic patients, lacked multicystic macular lesions and fluorescein leakage, and demonstrated vitreoretinal adherence - features differentiating it from Irvine’s syndrome.2

• Reese et al. studied macular changes in VMT and reported Irvine’s and Jaffe’s descriptions as parts of a spectrum of disease, with aphakia predisposing to more severe changes via additional traction.3
• Histopathologic studies by Reese et al. confirmed ‘vitreomacular traction syndrome’ and showed partially detached posterior hyaloid with persistent attachment to the internal limiting membrane in the foveal region.4
1) Irvine SR. A newly defined vitreous syndrome following cataract surgery. Am. J. Ophthalmol. 1953;36(5):599–619. 2) Jaffe NS. Vitreous traction at the posterior pole of the fundus due to alterations in the vitreous posterior. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1967;71(4):642–52. 3) Reese AB, Jones IS, Cooper WC. Macular changes secondary to vitreous traction. Am. J. Ophthalmol. 1967;64(3):Suppl:544–9. 4) Reese AB, Jones IS, Cooper WC. Vitreomacular traction syndrome confirmed histologically. Am. J. Ophthalmol. 1970;69(6):975–7.

ANATOMY• The vitreous gel is a transparent extracellular matrix
that fills the cavity behind the lens of the eye.• It occupies an average volume of 4.4 ml in adulthood• The outer cortex of vitreous which is made up of
dense collagen (Type II) is firmly attached to internal limiting membrane (Type IV collagen).

Vitreous Attachments Vitreous Base Peripheral margin of the Optic Nerve Head Posterior pole– margin of the fovea– retinal veins in the mid-periphery ( may account for avulsed retinal vessels and HSTs with bridging vessels after acute PVD) Abnormal areas– Lattice degeneration– Cystic retinal tufts– Chorioretinal scars

• The VITREORETINAL INTERFACE is an adhesive sheet that facilitates the connection of the posterior vitreous cortex of the vitreous body to the internal limiting membrane of the retina.
• The vitreoretinal interface consists of matrix proteins including laminin, fibronectin and collagen IV, and it is thought that these may act as an extracellular matrix 'glue'
CLASSIFICATION

VMA

• VMA in symptomatic patients has been graded based on SD-OCT:
• Grade 1: incomplete cortical vitreous separation with attachment at the fovea
• Grade 2: Grade 1 findings plus intraretinal cysts or clefts
• Grade 3: Grade 2 findings plus subretinal fluid.

VMT

• VMT has also been classified on the basis of the morphology of the traction and it divides VMT into V type and J type.
• In the V type there is incomplete vitreous detachment nasally and temporally causing a V-shaped pattern due to persistent attachment at the fovea
• In the J type, there is an incomplete posterior vitreous detachment with persistent nasal attachment but detachment temporal to the fovea
• V-shaped and focal VMT were found to lead to tractional CME and macular hole while J-shaped and broad VMT were related to ERM and diffuse retinal thickening



MACULAR HOLE
• Vitreomacular Adhesion: focal adhesion of the vitreous face within macular region.
• Vitreomacular Traction: VMA causing focal tractional distortion of macula.
• Vitreo macular traction syndrome: VMT associated with loss of visual function
• Spaide et al popularised the concept of the area of attachment and its relation with ocular morbidity.
• He proposes that the diameter of the vitreomacular attachment is inversely related to macular morbidity and foveal deformation.
• The narrower the vitreomacular attachment, the greater the force exerted on the macula, whereas diffuse vitreomacular adhesion might distribute the tractional force beyond the foveal border

EPIDEMIOLOGY
• The prevalence of isolated VMT syndrome is reported to be 22.5 per 100,000 population.
• The annual incidence of isolated VMT syndrome is 0.6 per 100,000 population.
• The prevalence and incidence of VMT associated with diabetic retinopathy, diabetic macular edema, age-related macular degeneration, and other macular diseases (concurrent VMT) is much higher
• VMT syndrome can affect either gender, although women have a slightly higher incidence presumably from the postmenopausal low-estrogen state that causes premature vitreous liquefaction and earlier onset of PVD.
• It can occur at any age, and in individuals of any race

PATHOGENESIS
• Starting in the fourth decade of life, the vitreous body witnesses a significant decrease in gel volume with a concomitant increase in the liquid volume
• The vitreous gel forms pockets of fluid within the vitreous (synchysis) which leads to a contraction or condensation (syneresis) of the vitreous
• As the age advances vitreous detaches from retina, a process known as Posterior vitreous Detachment (PVD)

• With loss of vitreous volume, there is a tractional pull exerted at sites of vitreoretinal and vitreopapillary attachments by means of the condensing dense vitreous cortex.
• At the same time, there is weakening of these attachments between the vitreous and the internal limiting membrane (ILM)
• When anterior vitreous pull and weakening of attachments occur synchronously, a normal posterior vitreous detachment (PVD) occurs.
• However, when these occur asynchronously (tractional component preceding or proceeding faster than the vitreoretinal detachment), an anomalous PVD develops which can result in VMT and other vitreoretinal diseases

Anomalous PVD is defined as partial vitreous detachment with persistent attachment in the macular region featuring an anomalous strength of adhesion to one or more structures in the posterior pole, resulting in tractional deformation of retinal tissue
Sebag J. Anomalous posterior vitreous detachment: a unifying concept in vitreo-retinal disease. Graefes Arch Clin Exp Ophthalmolo 2004; 242: 690-8.

• The anomalous adherence of the posterior hyaloid to the retina can be either a primary abnormality or develop secondary to cellular proliferation from cortical vitreous remnants after a partial posterior vitreous detachment, also known as vitreoschisis, or from concurrent diseases (e.g. proliferative diabetic retinopathy) that provide a fibrovascular scaffold for cellular proliferation and contraction.
• An epiretinal membrane (ERM) is commonly associated with both the vitreofoveal and vitreomacular traction. It has been shown to proliferate from the retinal surface, coursing up the cone of attached vitreous, and then growing along the back surface of the detached perifoveal hyaloid

HISTOPATHOLOGY• Fibrocellular proliferation consisting of fibrous
astrocytes, myofibroblasts, fibrocytes and RPE cells.• It usually forms a ‘double membrane’ that bridges the
posterior hyaloidal and the retinal interfaces. • The anterior layer may simply represent a thickened
posterior hyaloid.• In addition, a double layer of posterior hyaloid may
sometimes be present, an anatomical abnormality known as hyaloidoschisis which is more frequently observed in high myopic and diabetic eyes.
• Deeper, on the surface of the retina, an ERM may be present

S/S
• SYMPTOMS• VMA: Asymptomatic• VMT: Symptomatic with blurred or reduced vision,
metamorphopsia, micropsia, scotoma, and difficulties with daily vision-related tasks such as reading.
• Onset and progression of symptoms are usually gradual, except in a few cases of sudden onset of vision loss/scotoma due to severe traction causing foveal detachment

• The diagnosis of VMT syndrome is often difficult to establish clinically.
• Even with thorough fundus contact lens examination, firm translucent adhesions of the vitreous at the macula may be imperceptible which explains why this condition was considered rare and may remain underdiagnosed

SIGNS 1. Cystic changes in the macula, including
tractional CME.2. Epiretinal membrane: 40-100% eyes with VMT have an ERM (depending on whether the ERM is detected by biomicroscopy, OCT or electron microscopy)3. Thickened and taut posterior hyaloid4. Subretinal/subfoveal fluid5. When it occurs concurrently with other diseases (e.g. exudative age-related macular degeneration, proliferative diabetic retinopathy, etc.), findings specific to those diseases may be noted.

• Complications can include:1. Full thickness macular hole2. Tractional macular schisis3. Tractional foveal/macular detachment

INVESTIGATIONS
• OCT• In VMT syndrome, the posterior hyaloid space
usually appears hyperreflective and thickened on OCT, firmly adherent to the foveal region, causing morphological alterations

• V shaped(better surgical outcomes) or J shaped• Focal(<1500– microns) or broad(>1500
microns)• Johnson*-VMT syndrome would encompass
macular adhesions around 1500μm, while vitreofoveolar traction would be considered a distinct entity with macular adhesions smaller than 500μm.
*Johnson MW. Posterior vitreous detachment:evolution and complications of its early stages. Am J Ophthalmol 2010;149:371-382.

• Dynamic B-scan ultrasonic examination of VMT syndrome may demonstrate the peripherally detached hyaloid with attached hyaloid over the posterior pole, differentiating this syndrome from idiopathic macular pucker in which a complete PVD and Weiss ring is usually present.
• Ultrasonic B-scan has higher sensitivity and specificity for evaluating the vitreoretinal relationship as compared to stereoscopic slit lamp biomicroscopy, and can be useful in eyes with opaque media, where OCT is not possible, or when OCT devices are not available

D/D
• Differential diagnosis The differential diagnosis can include:• Early full thickness macular hole • Pseudophakic CME • Other causes of CME (uveitis, diabetic macular
edema, exudative age related macular degeneration, macular telangiectasia)
• ERM

MANAGEMENT
• OBSERVATION• In patients of VMT with good visual acuity and mild to
moderate symptoms the first approach is to observe for 3 months and re-examine the patients using OCT
• Patient should be advised to perform periodic self examinations with the Amsler grid or monocular reading tests.
• In case intensity of symptoms or disability increases they can be reassessed earlier
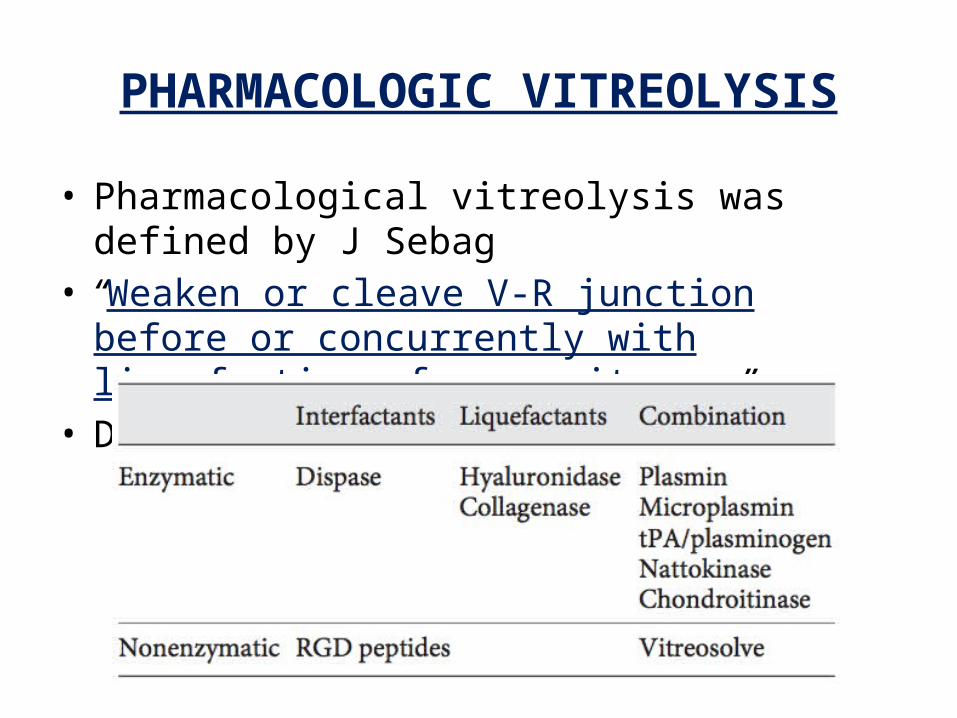
PHARMACOLOGIC VITREOLYSIS
• Pharmacological vitreolysis was defined by J Sebag• “Weaken or cleave V-R junction before or
concurrently with liquefaction of core vitreous”• Different agents:

• These agents break down the peptide bonds in laminin and fibronectin molecules which keeps the adhesion between ILM and vitreous.
• Plasmin is manufactured from patients own blood and it is very unstable.
• Ocriplasmin, is a recombinant truncated form of human plasmin with molecular weight 27.8kDa
• It is a DNA molecule which is more stable than plasmin and has emerged as new vitreolytic agent. It is recombinant protease with activity against fibronectin and laminin



• Safety and efficacy of ocriplasmin for the treatment of VMA was evaluated in two phase 3 trials (MIVI-006 and MIVI-007).
• Both multicenter, randomized, placebocontrolled, double-masked, 6 month studies.
• Identical in design (except for allocation ratio of 2:1 in TG-MV-006 and 3:1 in TGMV- 007) and conduct (except for geography: -006 conducted in the US and - 007 conducted in the EU and the US.






Ocular adverse effects of Ocriplasmin injection are • Vitreous floaters, • photopsia, • blurred vision, • conjunctival hemorrhage, • potential for lens subluxation, • retinal breaks and dyschromatopsia (as yellow
vision).

• ERG changes in the form of reduced ‘a’ and ‘b’ wave amplitude is reported in patients experiencing dyschromatopsia.
• Patients can experience transient loss of vision, which is attributed to the disruption in the ellipsoid layer( previously known as photoreceptor IS/OS junction).
• Wide spread retinal dysfunction can develop in patients due to its effect on laminin which is present in other layers of retina, including Bruch membrane, interphotoreceptor matrix, External limiting membrane, Outer plexiform layer, inner plexiform layer and ILM.
• Pharmacologic vitreolysis though carrying a lower success rate than vitrectomy, provides an alternative for patients who have overriding travel needs that preclude a gas injection; difficulties with surgery and postoperative management, such as positioning; or would have a significant benefit from avoiding cataract surgery.
• Its relatively lower invasiveness (compared with PPV) might prompt expanded treatment indications for patients with lesser degrees of symptoms or VMA once doubts about its safety have been cleared.
• At present its high cost per dose and low success rate are also limiting factors for its worldwide acceptance as a treatment modality for VMT

SURGERY
• Patients of VMT with decreased visual acuity good visual acuity with severe metamorphopsia and moderately symptomatic VMT that fail to improve with
observation, or demonstrate progression of the traction effects are indications for PPV.
• There is no consensus on level of visual acuity that should be considered significant but usually a visual acuity of 6/12 or worse is taken as an indication for PPV.

• Vitrectomy may be combined with one or more additional interventions including stripping of the posterior hyaloid, ERM peeling, ILM peeling, air-fluid exchange, and gas or air endotamponade
• Complications of surgery include cataract, new or residual ERM, full thickness macular hole, lamellar macular hole, persistent CME, persistent subretinal fluid, macular atrophy, retinal breaks, retinal pigment epithelial damage, visual field defects, glaucoma, endophthalmitis, and hypotony

POOR PROGNOSTIC FACTORS
• Macular schisis• prominent CME• chronic retinal detachment, and • premacular fibrosis• Duration > 6 months• Thicker central macular thickness preop• Pre op visual acuity worse than 20/100


Thank you