when and how to cleanse surgical wounds
TRANSCRIPT

Page 1 of 4
Wound CareAdults
When and how to cleanse surgical woundsEdited by June Jones, Independent Nurse Consultant, Southport, Merseyside
©2021 Clinical Skills Limited. All rights reserved
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Ensure privacy. Position the patient comfortably and in such a way that you can freely carry out the procedure, for example the supine position may be appropriate if the patient has a wound on the abdomen (above left), while the left lateral position (above right) is good for working on the back, the backs of the legs or the buttocks. Limit exposure of the patient’s body to the part you need to access for the procedure.
Examples of patient position: supine (left) and left lateral (right)
Healing of a surgical wound proceeds through the same phases whether the wound is healing by primary or secondary intention. In a surgical wound healing by primary intention, sutures, clips or butterfly tapes have apposed the dermal layers and the underlying tissues. Consequently, the initial phase of haemostasis and coagulation rapidly seals the tissue, protecting it from any potential bacterial infiltration. Such wounds can be cleansed, if necessary, with sterile saline up to 48 hours after surgery, and thereafter using a clean technique (Rowley et al., 2010) (see below). Lloyd Jones (2012) reminds us that, if the wound is clean and free from debris, cleansing has the potential to be detrimental: cleansing can damage the fragile granulation tissue and cool the wound bed to below the core body temperature if the cleansing solution is not warmed, delaying wound healing (Main, 2008).
Surgical wounds healing by secondary intention (e.g. following excision of an abscess) have such a loss of tissue that the apposing edges cannot be brought together. These wounds may be deep and can be colonised or infected, with damage to the surrounding skin. In some cases (e.g. excision of pilonidal sinus) the method of wound cleansing will be a bath or shower (after 48 hours), as these wounds will also be colonised. A clean technique is acceptable for cleansing surgical wounds healing by secondary intention (Kingsley, 2008) (see below). In contrast, surgical drain sites should be managed using an aseptic technique (see also clinicalskills.net procedure on “Aseptic technique: key principles”), as the integrity of the skin has been broken, and bacteria could enter the wound site. Wound management of all surgical wounds should, however, employ the principles of asepsis to prevent and/or minimise the risk of cross infection and delayed wound healing (Preston, 2005). The aim is to minimise the risk of
introducing pathogenic bacteria into a surgical wound, and to prevent the transfer of bacteria from one patient to another (Rowley et al., 2010).
Healthcare professionals should use an aseptic technique to manage wounds in the following cases:• Surgical wounds with debris, such as devitalised tissue or excessive exudate;• Any deep wound which leads to a cavity or sinus;• Wound dressings in patients who are immunosuppressed, have diabetes or who are at high risk of infection;• Open orthopaedic wounds (with, for example, exposed bone/tendon).
Lister et al., (2020) define a clean technique as “a modified aseptic technique [which] aims to avoid introducing microorganisms to a susceptible site and also to prevent cross infection to patients and staff”. A clean technique is performed in a similar way to an aseptic technique, but allows use of clean single-use gloves instead of sterile gloves, and potable tap water instead of sterile saline. When clean, single-use gloves are worn, a non-touch technique is required to avoid contaminating a susceptible site. It is therefore important to avoid touching the patient (or parts of equipment that will touch the patient) during the procedure. Wilson (2019) advocates a clean technique suitable for suture and drain removal and the care of dry surgical wounds after 48 hours.
Whatever method you adopt, always follow local policies. This guideline describes the use of an aseptic technique for dressing a surgical wound. Before beginning, explain the procedure to the patient, and obtain their explicit consent to proceed. Document the consent in the patient’s notes. If the wound is painful, the patient should have regular analgesia and may require a bolus dose before dressing the wound.

SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
Steripod
LOT
20ml
!
Sodium chloride 0.9%
w/v Ph. Eur
Discard su
rplus
Steripod
LOT
20ml
!
Sodium chloride 0.9%
w/v Ph. Eur
Discard surplus Hand disinfectant
Alcohol GelSteripod
LOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
SteripodLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard su
rplus
Assemble non-sterile equipment Warm the wound-cleansing fluid
Purell
Decontaminate your hands
WOUNDCARE PACK BLUELATEX FREE POWDERED04/2022
STERILE
Select and check equipmentClean the working area
Wound Care
Adults
When and how to cleanse surgical wounds Page 2
Place equipment on lower shelf of trolley. You will need access to alcohol-based hand sanitiser. You may also need non-sterile gloves for patient preparation before starting the aseptic procedure.
Saline for wound cleansing should be warmed, to avoid discomfort for the patient and to prevent unnecessary cooling of the wound bed, which can delay healing (Brown, 2018; Main, 2008). Place the container(s) of saline in warm water in a jug or a sink for a few minutes. (Always discard any unused warmed saline.)
Loosen the dressing Dispose of gloves and wash your hands
Using an aseptic technique (see “Aseptic technique: key principles”), prepare a sterile field using a sterile dressing pack. Ensure all necessary equipment and new dressings are to hand. Put on clean gloves.
Decontaminate your hands by either washing with soap and water and drying well or by using alcohol-based hand sanitiser, or according to local policy (see also “Routine hand hygiene”). Put on a disposable apron.
Select the equipment you will need. For example, the appropriate sterile pack, sterile cleaning fluid (if required), new dressing or sterile scissors. Check that the packaging is intact and that expiry dates have not passed.
The trolley or other surface (such as a tray) should be clean and dry. Use detergent or alcohol-based wipes to clean all areas effectively, or clean them according to local policy. (See also “Aseptic technique: key principles”.)
Page 2 of 4
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Jug
Aseptic technique should be carried out in a clean, dust-free environment. Ward-cleaning activities should be minimised in the immediate vicinity while wound dressings are performed (Ayliffe, 2000). Put on non-sterile gloves and loosen the dressing. If the dressing has adhered, you will need to soak it away later (see next page).
After loosening the dressing, discard the gloves into an infectious waste bag. Decontaminate your hands by washing with soap and water or by using alcohol-based hand sanitiser. It is preferable to wash hands following glove removal (Loveday et al., 2014).
Cleansing fluid (e.g. 0.9% saline)
Non-sterile gloves
Alcohol-based hand sanitiser
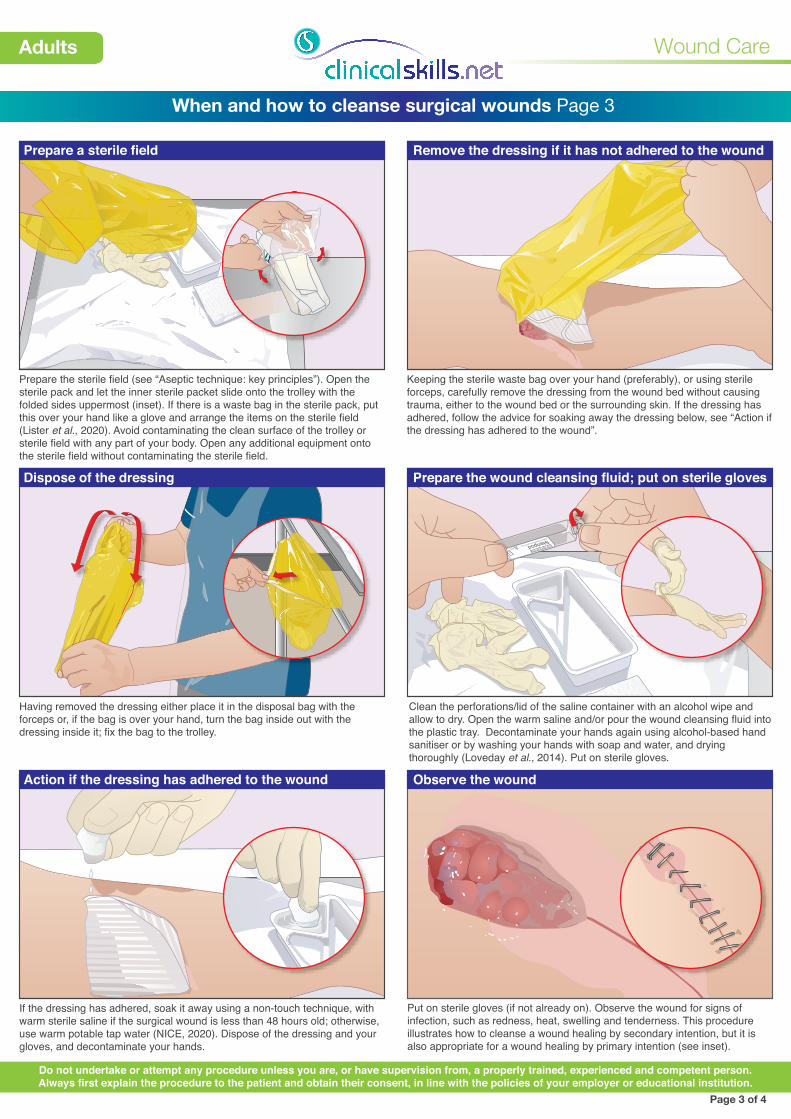
Prepare a sterile field Remove the dressing if it has not adhered to the wound
Steripod NOT FOR INJECTIONLOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard surplus
Dispose of the dressing Prepare the wound cleansing fluid; put on sterile gloves
Wound Care
Adults
When and how to cleanse surgical wounds Page 3
Prepare the sterile field (see “Aseptic technique: key principles”). Open the sterile pack and let the inner sterile packet slide onto the trolley with the folded sides uppermost (inset). If there is a waste bag in the sterile pack, put this over your hand like a glove and arrange the items on the sterile field (Lister et al., 2020). Avoid contaminating the clean surface of the trolley or sterile field with any part of your body. Open any additional equipment onto the sterile field without contaminating the sterile field.
Keeping the sterile waste bag over your hand (preferably), or using sterile forceps, carefully remove the dressing from the wound bed without causing trauma, either to the wound bed or the surrounding skin. If the dressing has adhered, follow the advice for soaking away the dressing below, see “Action if the dressing has adhered to the wound”.
Page 3 of 4
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Having removed the dressing either place it in the disposal bag with the forceps or, if the bag is over your hand, turn the bag inside out with the dressing inside it; fix the bag to the trolley.
Action if the dressing has adhered to the wound Observe the wound
Put on sterile gloves (if not already on). Observe the wound for signs of infection, such as redness, heat, swelling and tenderness. This procedure illustrates how to cleanse a wound healing by secondary intention, but it is also appropriate for a wound healing by primary intention (see inset).
If the dressing has adhered, soak it away using a non-touch technique, with warm sterile saline if the surgical wound is less than 48 hours old; otherwise, use warm potable tap water (NICE, 2020). Dispose of the dressing and your gloves, and decontaminate your hands.
Clean the perforations/lid of the saline container with an alcohol wipe and allow to dry. Open the warm saline and/or pour the wound cleansing fluid into the plastic tray. Decontaminate your hands again using alcohol-based hand sanitiser or by washing your hands with soap and water, and drying thoroughly (Loveday et al., 2014). Put on sterile gloves.

Mrs Smith’s wound has been cleansed with sterile saline and dressed with
DATE/TIME ACTIVITY PROBLEM/NEED
PROGRESS REPORT
2·03·2108·00
SteripodNOT FOR INJECTION
LOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard
surpl
us
SteripodNOT FOR INJECTION
LOT
20ml!
Sodium chloride 0.9% w/v Ph. Eur
Discard
surpl
us
Wound cleansing: (a) (b)
(c) Apply a new dressing
Dispose of equipment Wash your hands
Wound Care
Adults
When and how to cleanse surgical wounds Page 4
It is also possible to cleanse the wound by either gently dripping saline from the swab or from the container, to avoid damaging new tissue. Squeezing the container firmly will also produce a jet of saline for wound irrigation, if needed.
Page 4 of 4
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Select an appropriate dressing and dress the wound. Make the patient comfortable. As appropriate, arrange a review appointment and provide the patient with advice on bathing with the dressing in place.
Wash and dry your hands thoroughly. In the patient’s care plan, document the cleansing method used, the condition of the wound and the surrounding skin, and the type of new dressing applied.
Routine cleansing of a wound can traumatise fragile new tissue in and around the wound bed, so only clean the wound if necessary. Only remove wound exudate if it is present in copious amounts or there are signs of infection, as wound exudate can have bactericidal properties and may contain growth factors that help to promote wound healing (Main, 2008). Use a non-touch technique to clean the wound, using a fresh swab moistened with saline for each wipe. Discard each swab after use.
If the wound does not require cleansing, but exudate is present around the wound, it may be necessary to clean the surrounding area, using either warm sterile saline with sterile gauze (if the surgical wound is less than 48 hours old) or warm potable tap water (NICE, 2020).
On completion of the dressing, discard all remaining dressing waste into an infectious waste bag, including your apron and gloves, or follow local policy. Place any sharp items into a yellow sharps container.