where would you like to have your heart attack?
TRANSCRIPT
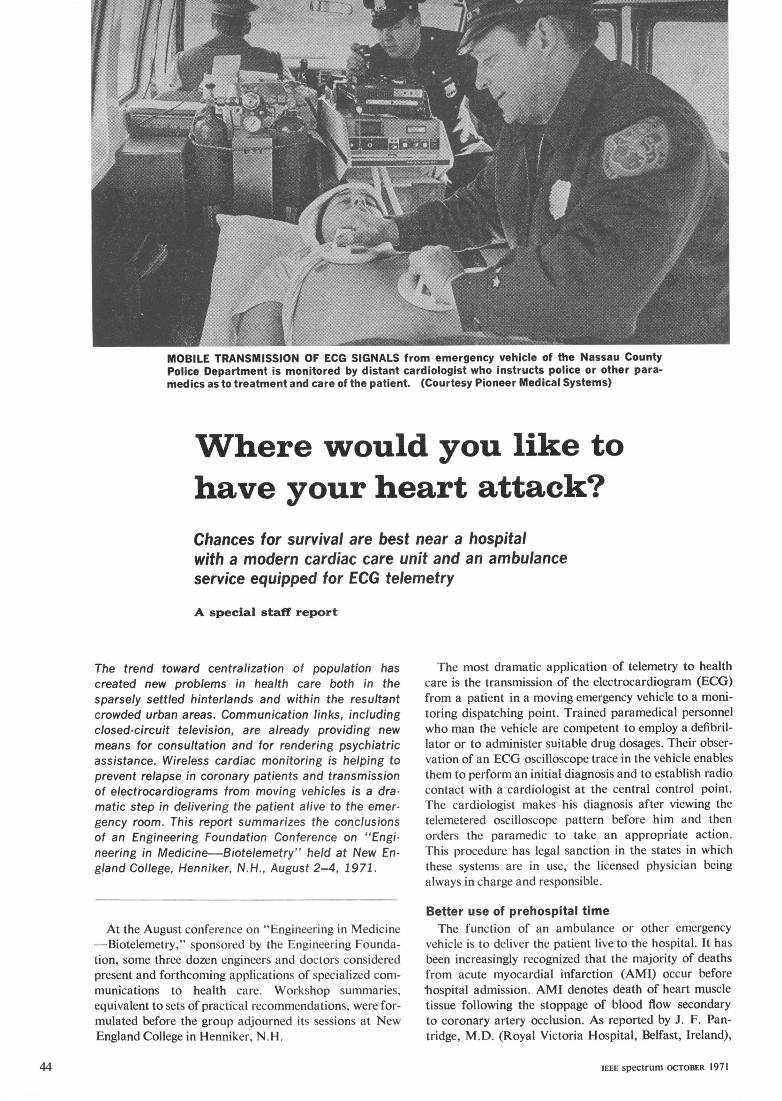
MOBILE TRANSMISSION OF ECG SIGNALS from emergency vehicle of the Nassau CountyPolice Department is monitored by distant cardiologist who instructs police or other para-medics as to treatment and care of the patient. (Courtesy Pioneer Medical Systems)
Where would you like tohave your heart attack?Chances for survival are best near a hospitalwith a modern cardiac care unit and an ambulanceservice equipped for ECG telemetry
A special staff report
The trend toward centralization of population has The most dramatic application of telemetry to healthcreated new problems in health care both in the care is the transmission of the electrocardiogram (ECG)sparsely settled hinterlands and within the resultant from a patient in a moving emergency vehicle to a moni-crowded urban areas. Communication links, including toring dispatching point. Trained paramedical personnelclosed-circuit television, are already providing new who man the vehicle are competent to employ a defibril-means for consultation and for rendering psychiatric lator or to administer suitable drug dosages. Their obser-assistance. Wireless cardiac monitoring is helping to vation of an ECG oscilloscope trace in the vehicle enablesprevent relapse in coronary patients and transmission them to perform an initial diagnosis and to establish radioof electrocardiograms from moving vehicles is a dra- contact with a cardiologist at the central control point.matic step in delivering the patient alive to the emer- The cardiologist makes his diagnosis after viewing thegency room. This report summarizes the conclusions telemetered oscilloscope pattern before him and thenof an Engineering Foundation Conference on "Engi- orders the paramedic to take an appropriate action.neering in Medicine Biotelemetry" held at New En- This procedure has legal sanction in the states in whichgland College, Henniker, N.H., August 2-4, 1971. these systems are in use, the licensed physician being
always in charge and responsible.
Befter use of prehospital timeAt the August conference on "Engineering in Medicine The function of an ambulance or other emergency
-Biotelemetry," sponsored by the Engineering Founda- vehicle is to deliver the patient live to the hospital. It hastion, some three dozen engineers and doctors considered been increasingly recognized that the majority of deathspresent and forthcoming applications of specialized com- from acute myocardial infarction (AMI) occur beforemunications to health care. Workshop summaries, hospital admission. AMI denotes death of heart muscleequivalent to sets of practical recommendations, were for- tissue following the stoppage of blood flow secondarymulated before the group adjourned its sessions at New to coronary artery occlusion. As reported by J. F. Pan-England College in Henniker, N.H. tridge, M.D. (Royal Victoria Hospital, Belfast, Ireland),
IEEE spectrum OCTOBER 1971
among men of middle age and younger, 63 percent of such availability is limited to weekdays from 8 o'clock in thedeaths occur within an hour of the onset of symptoms. morning until midnight. The cost of the equipped vehicle
Because most deaths occur before hospital admission, was about S60 000 and salaries at present amount to abouta mobile coronary care unit was started in Belfast in S45 000. Such costs are too high for the average com-January 1966. The system provides a junior physician munity and those in charge of the program believe thatand nurse as well as monitoring apparatus, drugs, intra- futLre trends will be in the direction of rescue squadsvenous solutions, and a portable defibrillator. Tele- supplied with portable equipment for handling coronarymetering equipment and radiotelephone keep the team attack victims. Although extensive special training isin contact with the hospital coronary care unit. It is of necessary for personnel, it is estimated that equipmentinterest that hospital mortality of patients managed by would cost about $5400 for each squad.the mobile unit is lower than that recorded among pa-tients admitted to coronary care units in the usual way, Nassau County experiencereducing the mean from 22.6 percent to 12.3 percent. Dr. Costas T. Lambrew, cardiologist at the NassauIn 1969, for example, among 447 patients with acute County Medical Center in East Meadow, N.Y., describedmyocardial infarction managed by the mobile unit, an emergency mobile system that has been in operationventricular fibrillation (chaotic, uncoordinated muscular since March 1971. The program serves an area containingcontractions of the heart leading to no blood flow) was some 1.5 million people that has heavy tralfic problemscorrected outside the hospital and before transport in and many automobile-induced injuries. The community14 patients, or 3 percent. has tended to meet this challenge by providing a county-
wide police service with which is associated an ambulanceMobile cardiac unit service operated by uniformed civilian personnel. Emier-An ambitious progranm in Montgomery County in gency vehicles are available in the eight precincts into
Maryland makes use of a Heartmobile, a special motor which the county is divided, and there are seven rovingvehicle, high enough for standing, equipped with a de- vehicles. An average of ten hospitals receive patients.mand pacemaker, cardioverter, resuscitator, and ECG The relatively flat terrain that is characteristic of alland pulse recorder connected to the transmitter of the two- Long Island makes for relatively reliable radio commu-way radio communications equipment. The vehicle is nication. A remote transmitter and receiver are nowstalled by paramedical personnel, including a nurse with mounted on a water tower on the North Shore; the mainexperience in treating cardiac patients, a cardiology antenna for the hospital base station is atop a new 19-technician, and a driver who is an experienced emergency- story Center building, providing excellent communication.room technician. The Heartmobile is credited with saving Concern for the large number of cardiac patients dyingat least one life each month since being put into service outside the hospital (35 percent) and Dr. Lambrew'sin March 1970. Manned by two three-menmber teams, its desire to develop a means for avoiding arrythmia have
What we know and what we need to doReport of the Emergency- Vehicle Worksihop
1. Whyhavetelemetryatall? abilities of the cardiovascular system, one of theirHealth care delivery systems of the future trend most important functions will have been accom-toward centralized physician/decision makers. Re- plished.mote personnel will be paramedical people who will 4. Given these needs, one sees that a large partneed to supply some classes of information so that of the emergency procedure will involve simple,treatment can be decided upon and ordered by the direct observation such as signs of shock andphysician. Therefore, remote parts of the system-- easily read and interpreted signals such as bloodfor example, emergency vehicles-will require two- pressure. Such information is most readily trans-way communications of two kinds: voice com- mitted, if required, by voice communication. Inmunication, and telemetered biosignals; also, given many cases-if not most--transmission of medicaladequate technological control, video communica- data from direct observation is more importanttion. than transduction and telemetering of physiologi-
2. What are the most important roles of EVs? cal signals. Patients in emergency situations are(a) Cardiac disabilities. usually classified by potential physiologic threat,(b) Vehicular accidents. which can be observed and verbally described to a(c) Drug overdoses. remote physician.
3. The prime objective of emergency-vehicle 5. The biological signals that appear to be im-service is simply to get the patient into the hospital, portant for emergency transduction would appearalive. There are three major emergency physiologi- to be limited to (a) electrical activity of the heart,cal problems: (a) respiratory block, (b) distur- (b) mechanical activity of the heart, and (c) thebances in electrical activity of the heart (bearing concentration of blood oxygen and carbonprincipally on maintenance of cardiac-pulmonary dioxide. There seems to be little need for otherfunction), and (c) hemorrhage. If the emergency- telemetry signals, especially given the less than tenvehicle services can deal adequately with problems minutes typical transit time from pickup to hos-of ventilation and electrical and mechanical dis- pital in an urban area. And in such a brief time, a
Where would you like to have your heart attack? 45

NORMAL ECG shows recurring healthy rhythm of the heart.
resulted in a systei whereby patients are monitored by Keeping this time short is imEportant because of theparamiedics with portable EGG equipment during the roughly 500 000 who die in the United States each yearambulance trip. The ECG output is used to modulate the from AMI. 40 to 70 percent of the deaths occur within themobile transmitter and the resultant demodulated pattern first hour after the onset of symptoms.is observed by the cardiologist on duty at the monitoring It is planned to extend treatment to administration ofpoint. He gives instructions to the ambulance personnel. drugs after the paramedical personnel have been givenpossibly to apply voltage pulses from a defibrillator if further training. A patient with a developing arrythmiasevere arrythmia has already begun. A cassette magnetic- is better treated with either atropine or lidocaine---de-tape recorder provides a permanent record for analysis pending on the nature of the arrythmia, visible on theand as possible legal protection. Of some 1300 patients ECG trace to the monitoring cardiologist---than toso far managed during this program, 234 complained of proceed into fibrillation.chest pains, 550 were found to have suffered traumas. The Nassau County situation is ideal in many respectsand the balance had other problems. The paramedics and the solutions effective there cannot necessarily behave been taught to consider a patient with chest pains applied to all medical or engineering problems.a probable cardiac case. The experience to this pointshows that 28 patients worsened, 18 were resuscitated. Serving the Hartford areaand 25 were found dead on arrival of the ambulance at Less fortunate in his choice of terrain, Dr. Robert J.the pickup point. The average time of an ambulance Huszar of St. Francis Hospital, Hartford, Conn., becamebetween pickup and arrival at the hospital is 6.8 minutes. a cardiologist by way of an earlier hobby in electronics.
patient simply cannot be coupled into many mon- ments are modest, but adequate communicationitoring systems. frequency assignments have yet to be made. It
6. With respect to these three measurements, should be noted that a single voice channel maythe first-electrical activity of the heart-is tech- also be used on a time-shared basis for telemetrynically in hand and proven valuable. The second, signals. The principal difficulties appear to bemechanical action of the heart, is only partially economic.approached by blood-pressure measurement (and 8. There are several reasons for expanding theit should be noted that this need not be telemetered: technology of telemetering physiological signalsverbal reporting may suffice). Fundamental re- besides that of immediate meeting of threat to thesearch is required and should be encouraged for patient's life. One is to find out more about pre-other indexes of deteriorated cardiac function. hospital patient monitoring and care, a topic aboutMonitoring mechanical parameters, along with which little is known. Another is further to trainelectric signals, should be useful. With respect to paramedical personnel, for if such people are tothe third class of measurements, the techniques for play an important role in the medical care of themonitoring blood gases are still imperfect, and future, then they must have adequate remote con-further development of transduction (and perhaps sultative facilities with physicians who will providetelemetering) technology appears to be called for. final medical judgment. However, we should not
7. Planners of emergency-vehicle health services try to substitute biometric telemetry for the ade-have two distinct technological problems. The first, quate training of paramedical personnel. Sophis-to decide what measurements are required or are ticated measurement, quantification, and automa-useful, is not well explored; disagreement exists tion do not necessarily lead to improvement.among experts and more investigation clearly is Then, too, there are reasons of physical control forrequired. But for now, at least, the number is legal purposes; for example, since paramedicalsmall. The second problem area, that of technical personnel are not medically licensed, the physician,integration of spoken and telemetrically transduced to maintain ultimate control and responsibility,information into communication networks, is also must have available those data about which sophis-imperfect, but principally because elegant system ticated decisions must be made. ECG waveformsdesign has not yet matured on a widespread basis. provide one example.State-of-the-art communications techniques and 9. The several successful but isolated and in-components seem adequate. Bandwidth require- complete experiments in emergency-vehicle telem-
46 IEEE spectrum OCTOBER 1971

LETHAL ARRYTHMIA showing ventricular fibrillation.
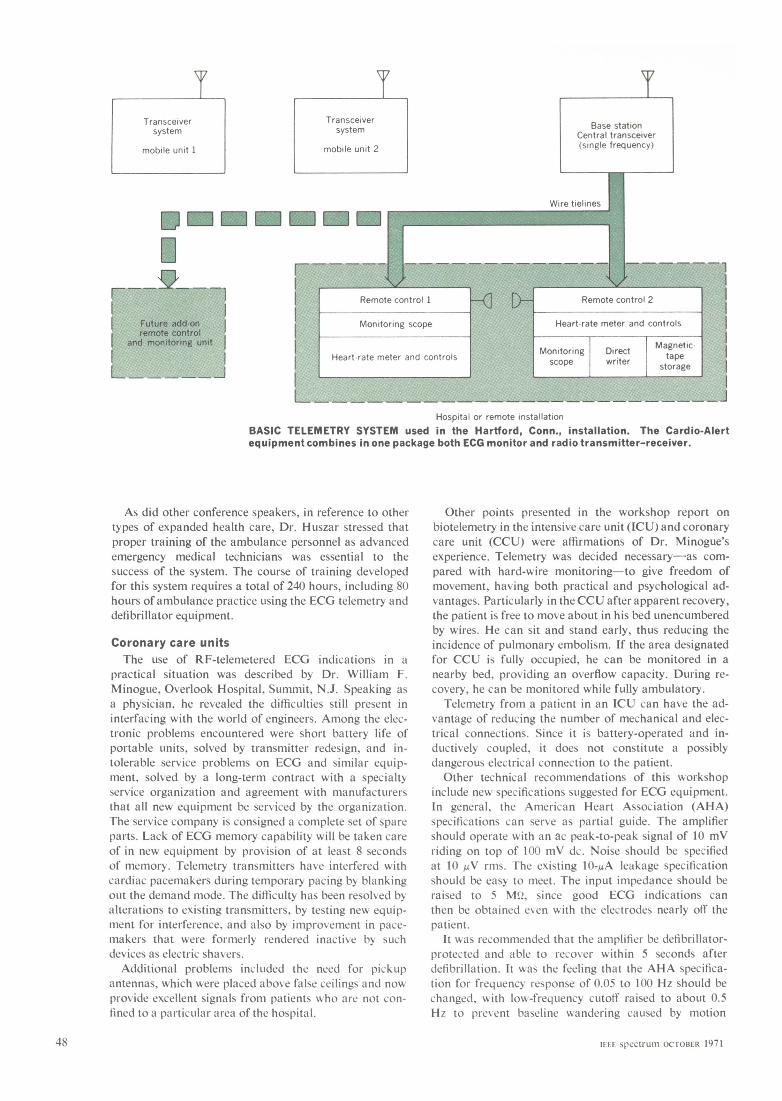
Besides contributing engineering knowledge unusual in telemetry system, a demodulator and amiplifier give aan M.D., he has found it necessary to develop means for suitable ouitput for the oscilloscope, direct writer, or tapefunding his $42 000 project without federal assistance. deck. The system has been designed to provide continLu-When fully operational, the system will serve a population ous monitoring at the patient's location and en route toof over a half million within Hartford (260 000) and sur- the hospital with periodic short transmissions of the ECGrounding communities. Costs include portable equipment to the hospital when necessary for evaluation. If thefor live coronary ambulances and extension of monitoring physician wants to interrupt the ECG transmission, heto two other hospitals. In addition to radiotelephone operates a tone recall at the hospital that is picked up intransceivers, remote receivers, and tower and telephone- the ambulance during an automatic 0.5-second silentline rental, the cost of ECG and defibrillation equipment period that alternates with the 15-second ECG transmitis included. cycle.The communications/telemetry equipment, which Dr. The present radiotelemetry system comprises a base
Huszar designed, combines a portable ECG signal modu- station with transmitter and receiver atop the highestlator and monitoring system with existing land mobile building in Hartford. It is connected by telephone line tovoice-communication equipment. The Cardio-Alert am- remote consoles located in the St. Francis Hospitalplifies the ECG signal, generates an FM subcarrier, pro- Research Laboratory and Emergency Room. The two-vides a visual and audible heart-rate readout, automati- way portable voice/telemetry equipment has been in usecally keys the transmitter by abnormal heart rates, and in a private ambulance serving the area for more thangenerates a calibration signal. At the receiving end of the two years.
etry systems clearly indicate that there is value in consultation availability on medical, engineer-the approach and that widespread evolution and ing, and legal details.incorporation of such systems should be en- (c) Studies of optimum systems design.couraged. But progress is observed to be rather (d) Extensive leadership at local levels andslow, particularly in light of present technological pressure on local governments to provide taxresouirces. What holds back more advanced de- funds. (Emergency-vehicle service is estimated tovelopment.' There are four basic reasons: cost as little as75l per year for each person in
(a) There is no leadership and little pressure a densely populated urban community, whereasto achieve widespread use of advanced methods. in rural areas unit costs will probably be slightly
(b) There is no central clearinghouse for med- greater.)ical, engineering, and funding information for (e) A public-relations campaign to createuse by would-be service innovators, a grass-roots demand for emergency-vehicle
(c) Efforts so far have been fragmented and ill- services that are at least as adequate as othersupported, and consequently the art is em- local services, such as police and fire, that may bebryonic. There is not yet a critical mass of know- even less important to the entire populace now.how or positive evidence of successfil design and (f) Development and extension of regionalpractice. programs sponsored by community hospitals
(d) Funding agencies, most particularly federal and clinics.ones, appear to be dollar-limited and more con- If. In summary, emergency-vehicle medicalcerned with other problems. service appears to have a minor component in10. Listed in the following are the fundamental technological problems (both medical and engi-
needs we see; the items are more or less equal in neering) that can be dealt with by modest researchimportance--no rank ordering is intended, and development effort, and it has a major com-
(a) Proposals and funding for pilot experi- ponent in the economic and widespread-deploy-mental projects on a regional (for example, ment aspects. Considerable effort is required here.statewide) basis, especially to find a full list of A national organization would appear to be calleduseful measurements that will permit establish- for. Shiny Cadillacs with chrome stretchers can bement of a data base on which emergency medi- replaced by usefui neat wagons if we see to it.cal services can be objectively evaluated. L. D.ifarinon
(b) A national information clearinghoulse and Worksnop Chairman
Where would you like to have vour hearrt attack? 47
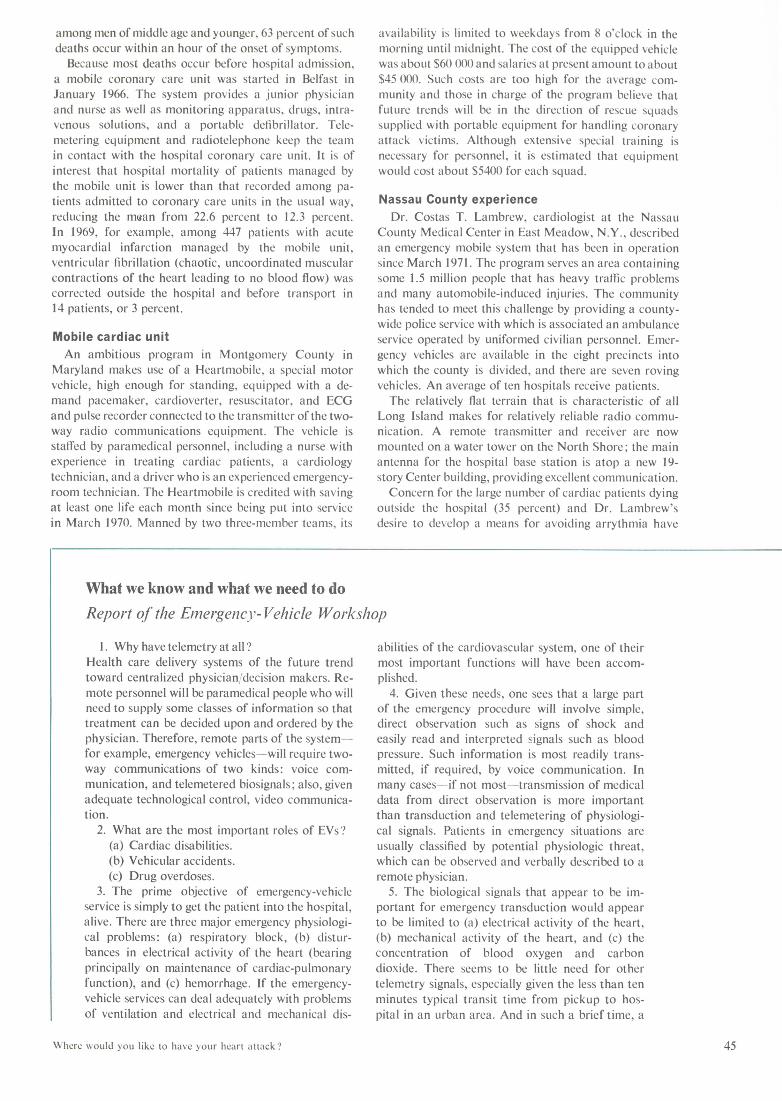
Transceiver Transceiver Base stationsystem system Central transceiver
mobile unit 1 mobile unit 2 (single frequency)
Wire tielines
|~~~~~~~~~~~~Rmt coto I Reot coto 2
Hospital or remote installationBASIC TELEMETRY SYSTEM used in the Hartford, Conn., installation. The Cardio-Alertequipment combines in one package both ECG monitor and radio transmitter-receiver.
As did other conference speakers, in reference to other Other points presented in the workshop report ontypes of expanded health care, Dr. Huszar stressed that biotelemetry in the intensive care unit (ICU) and coronaryproper training of the ambulance personnel as advanced care unit (CCU) were affirmations of Dr. Minogue'semergency medical technicians was essential to the experience. Telemetry was decided necessary-as com-success of the system. The course of training developed pared with hard-wire monitoring-to give freedom offor this system requires a total of 240 hours, including 80 movement, having both practical and psychological ad-hours of ambulance practice using the ECG telemetry and vantages. Particularly in theCCU after apparent recovery,defibrillator equipment. the patient is free to move about in his bed unencumbered
by wires. He can sit and stand early, thus reducing theCoronary care units incidence of pulmonary embolism. If the area designatedThe use of RF-telemetered ECG indications in a for CCU is fully occupied, he can be monitored in a
practical situation was described by Dr. William F. nearby bed, providing an overflow capacity. During re-Minogue, Overlook Hospital. Summit, N.J. Speaking as covery, he can be monitored while fully ambulatory.a physician, he revealed the difficulties still present in Telemetry from a patient in an ICU can have the ad-interfacing with the world of engineers. Among the elec- vantage of reducing the number of mechanical and elec-tronic problems encountered were short battery life of trical connections. Since it is battery-operated and in-portable units, solved by transmitter redesign, and in- ductively coupled, it does not constitute a possiblytolerable service problems on ECG and similar equip- dangerous electrical connection to the patient.ment, solved by a long-term contract with a specialty Other technical recommendations of this workshopservice organization and agreement with manufacturers include new specifications suggested for ECG equipment.that all new equipment be serviced by the organization. In general, the American Heart Association (AHA)The service company is consigned a complete set of spare specifications can serve as partial guide. The amplifierparts. Lack of ECG memory capability will be taken care should operate with an ac peak-to-peak signal of 10 mVof in new equipment by provision of at least 8 seconds riding on top of 100 mV dc. Noise should be specifiedof memory. Telemetry transmitters have interfered with at 10 ,uV rms. The existing 10-yA leakage specificationcardiac pacemakers during temporary pacing by blanking should be easy to meet. The input impedance should beout the demand mode. The difficulty has been resolved by raised to 5 MQ, since good ECG indications canalterations to existing transmitters, by testing new equip- then be obtained even with the electrodes nearly off thement for interference. and also by improvement in pace- patient.makers that were formerly rendered inactive by such It was recommended that the amplifier be defibrillator-devices as electric shavers. protected and able to recover within 5 seconds after
Additional problems included the need for pickup defibrillation. It was the feeling that the AHA specifica-antennas, which were placed above false ceilings and now tion for frequency response of 0.05 to 100 Hz should beprovide excellent signals from patients who are not con- changed, with low-frequency cutoff raised to about 0.5fined to a particular area of the hospital. Hz to prevent baseline wvandering caused by motion
48 IFEF spectrum OCTOBER 1971
artifacts. The high-frequency cutoff should be lowered to Cruces. Funds are not available to carry the project be-about 50 Hz to reduce muscle-to-tremor noise. yond initial study, but the plans envision a physician-The need to monitor ambulatory cardiac patients for monitored control center with remote-site clinics and
much longer periods than are now feasible is stressed as mobile dispensaries. Equipment might eventually com-a particular value for RF telemetry. prise a television system, two-way voice transmission,
high-fidelity FM system for monitoring heart and breathRemote health care sounds, and a computer terminal, displays, and recordThe delivery of preventive-medicine services and storage at the control center.
medical treatment to populations who have no present Lister Hill Center for Biomedical Communications, ofaccess to these services is generally described as remote the National Library of Medicine, Bethesda, Md., hashealth care. It was agreed in a workshop meeting covering been funding what they term a "social experiment" usingthis broad area that, although it is implicit that lack of simple ground communications equipment in conjunctionaccess to such care is the result of geographical separa- with a fixed communications satellite to provide remotetion, urban groups can be comparably remote and suffer health care consultation in Alaska.similar deprivation. Earlier attempts at daily communication between
Mrs. Charlotte J. Sanborn, Dartmouth Medical School, hospital health service centers and village health aidesHanover, N.H., described a research project funded by a had been unsatisfactory because of the unreliability offour-year grant from the National Institutes of Mental HF radio propagation in an auroral environment. TheHealth. Its purpose is to provide 24-hour psychiatric ATS-1 satellite will permit commercial mobile radioconsultation service for nonpsychiatric physicians serving equipment installed at the homes of village aides toa semirural population relatively remote from a teaching communicate with the seven native health service hos-center by using two-way closed-circuit television. pitals. Simple helical antennas with 13-dB gain areThe school was linked with a studio in Claremont, a directed at the satellite. Time is scheduled through NASA
county seat with a population of about 15 000 and 48 km for a total of four hours a day, five days a week. The up-away. The county is without a psychiatrist, psychologist, frequency is 149.22 MHz and the ground receivers areor psychiatric social worker. Both Hanover and Clare- tuned to 135.60 MHz.mont are within line of sight of Mt. Ascutney, Vt., the site The University of Alaska is the overall project man-of the microwave relay station necessary to link the two ager. The prime consideration is the establishment ofterminals. This service is rented from the telephone com- voice consultation service, and it is hoped that un-pany and the audio circuit uses leased lines. attended reception of messages for scheduling and healthThe Hanover psychiatrist is located in a studio with a education can be accomplished. A quality check of the
television screen that shows the Claremont patient. He technical facilities is under contract to the University ofalso has a split-screen monitor that shows himself and Wisconsin, Stanford University, and the University ofthe Claremont end. A videotape machine is available to Washington. It is hoped that ECG traces can be trans-record sessions for teaching purposes. In Claremont, mitted. Experiments will determine the requirements forthere are two adjoining rooms. The patient sits in a com- sending X-ray information, facsimile, and telemetering offortable chair amid pleasant surroundings and talks physiological signals.to the psychiatrist, whose image he sees on the televisionmonitor before him. In the adjoining room, the referring Intensity-modulated laserphsyician has two monitors, one showing the psychiatrist An unusual laser television circuit was described byand the other the patient. He can see and hear but not Dr. Yoh Han Pao of Case-Western Reserve University,talk.
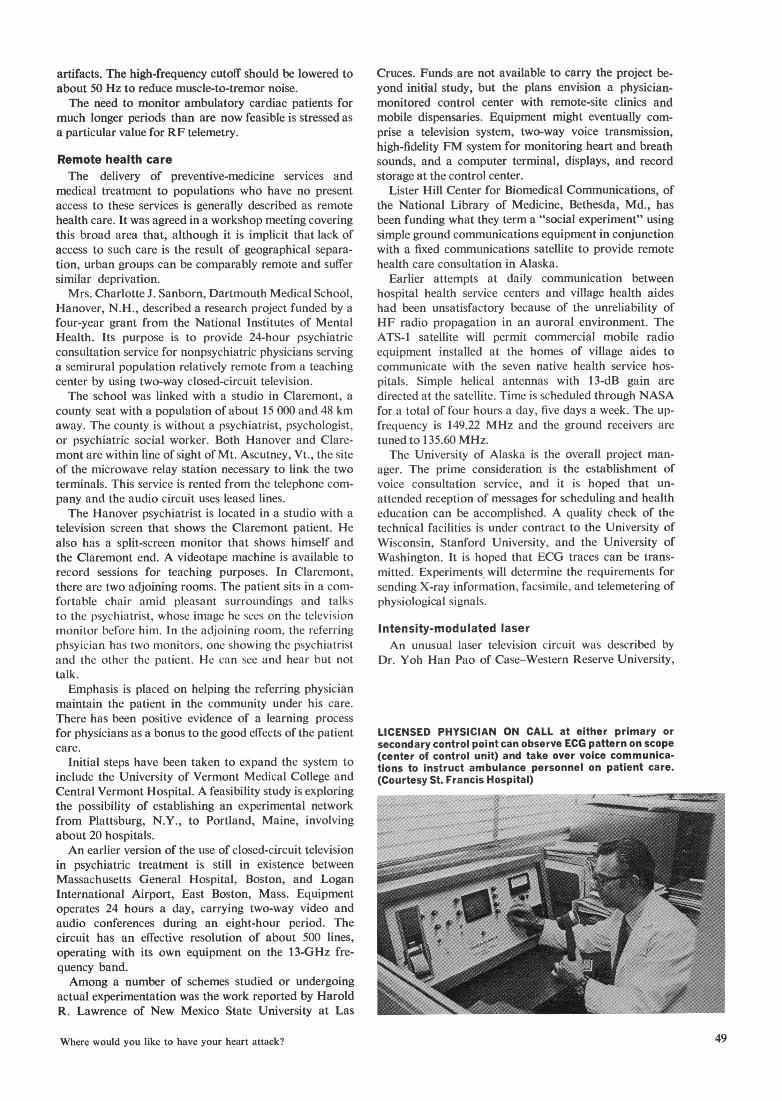
Emphasis is placed on helping the referring physicianmaintain the patient in the community under his care.There has been positive evidence of a learning processfor physicians as a bonus to the good effects of the patient LICENSED PHYSICIAN ON CALL at either primary orcare. secondary control point can observe ECG pattern on scope
Initial steps have been taken to expand the system to (center of control unit) and take over voice communica-Inital tep haeben akento xpad te sste to tions to instruct ambulance personnel on patient care.include the University of Vermont Medical College and (Courtesy St. Francis Hospital)Central Vermont Hospital. A feasibility study is exploringthe possibility of establishing an experimental network ifrom Plattsburg, N.Y., to Portland, Maine, involving ~"about 20 hospitals.An earlier version of the use of closed-circuit television .
in psychiatric treatment is still in existence betweenMassachusetts General Hospital, Boston, and LoganInternational Airport, East Boston, Mass. Equipmentoperates 24 hours a day, carrying two-way video andaudio conferences during an eight-hour period. Thecircuit has an effective resolution of about 500 lines,operating with its own equipment on the 1 3-GHz fre-quency band.Among a number of schemes studied or undergoing
actual experimentation was the work reported by HaroldR. Lawrence of New Mexico State University at Las
Where would you like to have your heart attack? 49
Cleveland, Ohio. It is used for educational purposes communication is provided, because the military vehiclesbetween University Hospital and the Veterans Admin- are so equipped.istration Hospital several kilometers away. A problem Three of the sites are Army bases: Fort Sam Houston,with visual (laser) communications is scintillation of the San Antonio, Tex.; Fort Lewis, Wash.; and Fort Carson,signal as a result of atmospheric turbulence. In the in- Colo. Two sites are Air Force bases: Mountain Hometensity-modulation system described, the laser beam is AFB, Boise, Idaho, and Luke AFB in Arizona. Themade to blink sinusoidally at 30 MHz and the intelligence medical study is being made by Ohio State University andis carried on a frequency-modulated subcarrier. Capable Stanford Research Institute is handling the vehicularof handling a color television channel, the circuit is study for the Department of Defense.claimed to be 99.9 percent reliable over a few kilometers, Modulating the signal with physiological data has notwith a signal-noise ratio of 50 dB. It has functioned with- yet been tried. In one case reported, however, it wasout loss of quality in very bad weather, including heavy requested that the Coast Guard transport a heart patientsnow. from one of the British islands into Miami, Fla. The
Coast Guard asked for a heart specialist to accompanyGovernment support limited the flight and a Fire Department representative tookThe federal government's representation at the con- portable ECG equipment with him. Readings were suc-
ference was headed by Dr. Edward J. Burger, Jr., Office cessfully transmitted back to Miami without an ex-of Science and Technology, Executive Office of the ternal antenna through an open door of the helicopterPresident, whose keynote address cautioned that people that was oriented in the direction of the receiving station.outside engineering are questioning technology, andto beware the concept of a gadget looking for a job. FCC rule-makingHe urged that the types of information required by a Practical considerations of obtaining licenses for thephysician be listed in order to decide how technology operation of specific radio systems from the Federalcan improve its acquisition. His exhortation to consider Communications Commission were discussed by Dr.the interplay between devices and people was frequently Fred B. Vogt, University of Texas. By the time of pub-reechoed throughout the meetings. lication of this report, comments must have been re-From a medical viewpoint, Dr. David D. Rutstein, ceived by FCC on their proposal to provide frequencies
Harvard University Medical School, Boston, Mass., for biotelemetry (SPECTRUM, Sept. 1971, p. 106).urged that the important end result of applying tech- The conference was led by Charles W. Garrett,nology be to diminish disease, disability, and untimely National Academy of Engineering, and James T. Rich-death. ards, National Aeronautics and Space Administration,
Federal representatives from the areas of financing was cochairman. The workshops were headed by Leonindicated clearly that funds are in very short supply, if D. Harmon, John G. Webster, and James N. Brown.not completely unavailable, and Dr. Arthur Barsky, from Alexander A. McKenziethe National Center for Health Services Research andDevelopment, stated that their present time frame is Considerable information has been furnished since the Confer-not five years but two. ence through the kindness of several individuals: Al Feiner, Dr.
Pierre M. Hahn, Dr. Robert J. Huszar, Dr. Costas T. Lambrew,Representatives from other branches stated that sup- Charles E. Lathey, Norman Lemieux, Capt. Frank Parker, Missport for suitable health projects is already being provided Elizabeth A. Penick, Mrs. Charlotte J. Sanborn, Dr. Fred B.and more is available, especially in cooperative ventures Vogt.that do not require dollar funding. Among these wereDr. John D. Chase of the Veterans Administration; Col. SECTDBLIG PHDihr.John. ChaloeofcthoolVetera Administratio;M ic *'Biomedical electronics," special issue, Proc. IRE, Nov. 1959.Richard S. Malone, School of Aerospace Medicine,
Caceres, C. A., (ed.), Biomedical Telemetry. New York; Academic,Brooks Air Force Base, Tex.; James T. Richards, NASA; 1965.and Bernard Shacter, National Institutes of Health. Miller, A., et al., "Recent developments in biomedical engineer-
In reporting the evaluation of some 1400 grant-in-aid ing," NEREM Record, pp. 112-123, Nov. 1966.programs, Charles E. Lathey, Office of Telecommunica- "Recommendations for standardization of instruments in electro-
cardiography and vectorcardiography, report of Subcommittee ontions, Department of Commerce, mentioned both Project Instrumentation Committee on Electrocardiography, American2020 and MAST, essentially health-care studies that are Heart Association," IEEE Trans. Bio-Medical Engineering, vol.supported by the Department of Transport. BME-14, pp. 60-68, Jan. 1967.
Although bio r hStark, Lawrence, et al., "Status of research in biomedical engineer-Although biotelemetry has not yet become a factor in ing," IEEE Trans. Bio-Medical Engineering, vol. BME-15, pp.either program, the radio communications necessarily 210-231, July 1968.available make further exploitation using instrumentation Lown, Bernard, and Selzer, Arthur, "The coronary care unit,"a practical follow-on. Am. J. Cardiol., vol. 22, pp. 597-602, Oct. 1968.
Projec 2020 iastyGrace, W. J., "The mobile coronary care unit and the intermedi-Project 2020 is a study comparing the effectiveness ate coronary care unit in the total systems approach to coronaryof helicopters with land ambulances in Nebraska. Al- care," Chest, vol. 59, pp. 363-368, Oct. 1970.though it has beencompleted,nofinalreportisyetavail- Pantridge, J. F., "Mobile coronary care," Chest, vol. 58, pp.able. The work was performed in part by the University 229-234, Sept. 1970.
., Mackay, R. S., Bio-Medical Telemetry (2 ed.). New York: Wiley,of California at Los Angeles and the eventual report Will 1970.be available from the National Technical Information "4Communications technology for urban improvement," NationalService, Springfield, Va. Academy of Engineering, 1971; available from National TechnicalMAST (Military Assistance to Safety and Traffic), now Information Service, Springfield, Va. 22150, $3.00.
in the demonstration phase at five sites, provides heli- Reprints of this article (X71-103) are available to readers.copters and crews from existing military capability to Please use the order form on page 8, which gives infor-be utilized at the request of civil authorities. Voice mation and prices.
50 Where would you like to have your heart attack?