who-paho guidelines for the use of foreign field hospitals in the
TRANSCRIPT

Natural and complex disasters can cause a dramatic increase in the demand for emergencymedical care. Local health services can be overwhelmed, and damage to clinics and hospi-tals can render them useless.
Many countries maintain mobile field hospi-tals for defense or humanitarian purposes.Dispatching these facilities to disaster-affect-ed countries would seem to be the idealresponse to emergency medical needs.Unfortunately, experience has shown that inthe case of natural disasters field hospitalsoften have not met the expectations of recip-ients and donor institutions. In July 2003, the World Health Organizationand Pan American Health Organizationsponsored a workshop in El Salvador to dis-cuss the pros and cons of using foreign fieldhospitals in the aftermath of natural disas-ters. These guidelines are the result of thatworkshop.
The workshop participants identified different phases when foreign field hospitals and special-ized medical personnel are most useful. They can provide advanced trauma care and life sup-port if at the disaster site within 48 hours of the impact of an event; they would provide fol-low-up care for trauma victims and resumption of routine medical care in the two weeks fol-lowing the event; during rehabilitation and reconstruction phases (from two months to twoor more years), a field hospital might serve as a temporary replacement for damaged healthfacilities. These guidelines propose conditions that field hospitals and their staff shouldmeet for each of these phases. The guidelines also outline issues that authorities in donorcountries and disaster-affected countries should discuss before mobilizing a field hospital.

Forei
gn Fi
eld H
ospit
alsWHO-PAHO
Guidelines for the Use of
Foreign Field Hospitals in the Aftermath
of Sudden-ImpactDisasters
Area on Emergency Preparednessand Disaster Relief
Pan American Health Organization
Department of Emergency andHumanitarian Action
World Health Organization
International meetingHospitals in Disasters—Handle with Care
San Salvador, El Salvador, 8–10 July 2003
Washington D.C. • 2003

2 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
© Pan American Health Organization (PAHO), 2003
A publication of the Area on Emergency Preparedness and DisasterRelief of PAHO in collaboration with the Department of Emergencyand Humanitarian Action of the World Health Organization (WHO).
The views expressed, the recommendations made, and the termsemployed in this publication do not necessarily reflect the currentcriteria or policies of PAHO/WHO or of its Member States.
PAHO and WHO welcome requests for permission to reproduce ortranslate, in part or in full, this publication. Applications andinquiries from the Americas should be addressed to the Area onEmergency Preparedness and Disaster Relief , Pan American HealthOrganization, 525 Twenty-third Street, N.W., Washington, D.C.20037, USA; fax: (202) 775-4578; email: [email protected]; the ones from the rest of the world shouldbe made to the Department of Emergency and HumanitarianAction, World Health Organization, 20 avenue Appia, Geneva,Switzerland; fax: (4122) 791-4844; e-mail: [email protected].
This publication has been made possible through the financial sup-port of the International Humanitarian Assistance Division of theCanadian International Development Agency (IHA/CIDA), theOffice for Foreign Disaster Assistance of the United States Agencyfor International Development (OFDA/USAID), and the UnitedKingdom’s Department for International Development (DFID).
3
Introduction
Early Emergency Medical Care
Follow-up Trauma and Medical Care
Donation of FFH (Without Personnel) to Serve
as a Temporary Hospital
57
1016
ContentsC o n t e n t s

5INTRODUCTION
Both natural and complex disasters may produce a massivenumber of casualties that outstrip the ability of the local health caresystem to provide the required care. Damage to the health care infra-structure will further compromise the delivery of health services.
As a consequence, affected and collaborating countries areanxious to find ways to provide immediate medical care to victims.An obvious solution would seem to be the dispatch of mobile fieldhospitals to the stricken area.
In complex disasters (civil conflicts and wars), field hospi-tals—civilian or military—have been used with notable success.However, the experience in the aftermath of natural disasters indeveloping countries has proven to be less satisfactory in terms ofeffectiveness and cost.
These perceived shortcomings prompted the World HealthOrganization (WHO) and the Pan American Health Organization(PAHO) to convene a meeting of experts to review guidelinesregarding the dispatch or donation of foreign field hospitals (FFH)to areas in which a disaster has compromised the delivery of healthservices, particularly in developing countries.
Systematic and independent evaluation of FFH used in disas-ters will be required to further refine the following recommenda-tions.
Introduction

6 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
Definition
For the purpose of these guidelines, a field hospital is definedas a mobile, self-contained, self-sufficient health care facility capableof rapid deployment and expansion or contraction to meet immedi-ate emergency requirements for a specified period of time.
The field hospital may be temporarily dispatched with person-nel or donated without personnel.
It is understood that: field hospitals are deployed only: (a) fol-lowing an appropriate declaration of emergency and a request fromthe health authorities of the affected country; (b) when they are inte-grated into the local health services system; and (c) when the respec-tive roles and responsibilities for their installation and operationalsustainment have been clearly defined.
Uses for Foreign Field Hospitals
Field hospitals may be used to substitute or complementmedical systems in the aftermath of sudden-impact events that pro-duce disasters for three distinct purposes:
1. Provide early emergency medical care (including AdvancedTrauma Life Support—ATLS). This period lasts only up to 48hours following the onset of an event.
2. Provide follow-up care for trauma cases, emergencies, rou-tine health care and routine emergencies (from day 3 to day15).
3. Act as a temporary facility to substitute damaged installationspending final repair or reconstruction (usually from the sec-ond month to two years or more).
The FFH should meet some essential requirements to ensurethat it benefits the affected population. Ideally, it should also meetsome additional (optional) criteria.
The World Health Organization (WHO) and the PanAmerican Health Organization (PAHO) suggest the following“essential requirements” and “additional (or optional) criteria” foreach intended purpose.
7EARLY EMERGENCY MEDICAL CARE
Essential requirements:
• Be operational on site within 24 hours after the impact ofdisaster
The interval must begin from the time of occurrence of themass casualties and not, as usually advertised by donors, from thetime the request is acted upon by the assisting country or organiza-tion. This is an essential medical requirement for life-savingresponse and is not an administrative condition that can be waived.
• Be entirely self-sufficient
In the early phase, FFH should be able to operate with a min-imum of support/utilities from the affected community. At the least,they should have sufficient power generating capacity and medicalsupplies and equipment to operate independently for the first 48hours. The staff should require minimal or no support (food, accom-modation, etc.) from the host community.
• Offer comparable or higher standards of medical care thanwere available in the affected country prior to the precipita-ting event
The medical personnel should be qualified and have priorexperience in managing mass casualties (including the concept oftriage) and in treating victims with acute, multiple injuries.
Early Emergency Medical Care
(First 48 Hours)

8 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
Optional criteria:
• Be familiar with the health situation and culture of theaffected country
Sharing the same language and culture or being familiar withthe health systems and level of technology of the affected country arehighly desirable even in the immediate aftermath of a natural disas-ter (first two days).
In practice, those medical facilities that are available withinthe first 24 hours most likely will come from the closest neighborswho share the same language and culture.

9EARLY EMERGENCY MEDICAL CARE
Issues that must be clarified before accepting/requestinga field hospital for early emergency trauma/medical care
(first 48 hours).
Questions both parties (recipient and donor) should ask:
Questions Comments
When can the FFH actuallyand effectively start assessingand treating victims?
If not within 24 hours of the impact, consideraccepting this facility using the criteria for sec-ondary care and routine emergencies (3–15days).Beware of vague answers or misleading state-ments that indicate that the hospital can be“activated” or mobilized within, for example, 6hours. What you need to know is when it can beoperational on site.
Is the hospital fully self-suffi-cient (including power andwater)? For how long?
Only self-sufficient hospitals should be accept-ed.
Type of equipment and servic-es available?Number of beds?Stabilization and transfer ofpatients only?Full operating room capacity?General anesthesia?Blood bank and laboratory?
The reply will tell you what you can reasonablyexpect in terms of performance and services.
Type of medical staff avail-able?Number, qualifications andseniority?Prior experience in masscasualty management?
Medical staff inexperienced in disasters, toojunior or from a specialty unrelated to trau-ma/medical emergencies are not as useful asemergency physicians and trauma surgeonsfrom a busy trauma department.
How long can the FFH stay? Longer is not necessarily better. FFH staff unfa-miliar with local culture and health servicesquickly outlive their usefulness (and welcome).Needs change after a few days, as should theprofile of the assisting medical staff.
What is the most appropriatelocation for installation of thisFFH?
This depends on medical needs (identified byrecipient country), logistical imperatives (roads,infrastructure) and access by victims. Generally,FFH are better placed in the proximity of a localhealth facility (even if it is out of service).

10 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
Following the first 48 hours when provision of acute caredoes save lives, the health services are progressively overwhelmedby the need for secondary or maintenance care for the trauma vic-tims as well as the demand resulting from the rapid emergence ofnormal emergencies or routine medical care. The health facilitiesmay not be fully operational and staff will urgently need some restand time to care for possible personal losses.
When the local health installations remain functional, thisneed of external assistance is better met by medical brigades orteams from within the country or from culturally compatible neigh-bors rather than by expensive or bulky FFH.
The primary role of the FFH is to temporarily fill the gaps inemergency medical assistance resulting either from the large num-ber of casualties or the inability of the local health services torespond to normal emergencies. The duration of the FFH operationsshould usually not exceed 15 days but can be extended at the speci-fic request of the affected country.
Essential requirements:
• Be fully operational within 3–5 days
Early arrival at the site is no longer a matter of life or death asalmost all victims will have received acute care from the local healthworkers and the few FH or medical teams from outside the disaster-affected area who were able to arrive in time to provide effectivemedical care.
A few hours may not make a significant difference after thefirst 24 hours, so hasty decision-making by the recipient governmentis counterproductive. Nevertheless, in order to assist with the provi-sion of health care that meets immediate needs of the affected com-munity, such field hospitals must be operational within three to fivedays following the impact.
Day 3 to Day 15
Follow-upTrauma and
Medical Care

11FOLLOW-UP TRAUMA AND MEDICAL CARE
• Minimal need for support from the local communities
The FFH must be self-sufficient (staff, medicines, equipmentand supplies, orthopedic surgery and minor interventions, anesthe-sia, external consultation and accommodation of the FFHstaff). Water and power may be restored at least for criticalfacilities in the community affected. The FFH may reason-ably expect to receive some support from the local author-ities. However, due to the expected unreliability of theseservices, the FFH should be able to provide its ownsource of energy and water when necessary.
• Basic knowledge of the health situation and lan-guage, and respect for the culture
The FFH personnel is expected to initiate orcontinue to provide services after the initial acute care phase (first48 hours) and must be able to communicate with the patients, thelocal authorities and colleagues in the health services. The staffshould have some familiarity with endemic local pathology. Some ofthe staff should speak the local language or interpreters must beprovided.
Medical personnel utterly unfamiliar with the environmenthave proven to be not only of limited utility but often have turned outto be a burden and a source of contention for the host community.
• Availability of selected specialties
The FFH must include health professionals in areas otherthan orthopedics, such as general surgery, anesthesiology, internalmedicine, gynecology and obstetrics, and pediatrics with the para-medical and support staff to meet the type and variety of servicesthey will be called on to provide. The equipment and facilities shouldallow assessment and treatment of all patients regardless of age orgender.
• Sustainability (appropriate technology)
The bulk of the assistance from the FFH may consist of exter-nal consultations and routine (non-disaster related) hospital care.FFH do not stay for extended periods of time and the local healthworkers are expected to assume full function within a few weeks afterthe precipitating event.

12 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
The quality and sophistication of the care provided by theFFH must be sustainable by the local health services once the FFHhas departed. Short-lived availability of higher technological care(diagnosis, medicines, etc.) often raises unrealistic expectationsfrom the population and leaves the local health services in a weak-ened position.
• Evaluation of the cost-effectiveness and cost-benefit associ-ated witht he use of the FFH
Setting up a field hospital is an expensive undertaking. Adetailed agreement between the recipient and donor must be madespecifying who will be responsible for costs associated with ship-ment, site preparation, maintenance, operational costs, staffing, etc.Donors sometimes expect the host country to cover local expensesinvolved in operating a field hospital(e.g., utilities, fuel, and othersupport), but local health services are not usually able to meet thesecosts.
Optional criteria:
• Cultural similarity
Familiarity with and a respect of the local culture and lan-guage are essential requirements. Ideally, the staff should share thesame language and culture. Dissimilarity of culture and languagehas resulted in misunderstandings between the external helpers andthe local staff.1
• Broad range of medical disciplines
The FFH should include a broad range of clinicians and pub-lic health professionals. Epidemiologists, hygiene/sanitation expertsand mental health experts have proven to be valuable assets.
1 In most instances, the time of the medical staff of a FFH is dedicated increasingly to providingexternal (ambulatory) consultations to outpatients. The total number of consultations will farexceed the normal rate for reasons not necessarily associated with the disaster but rather withpoverty or poor coverage of the health services. Increase in demand for services can be attrib-uted to:
• Prestige of foreign doctors;• Availability of new diagnosis, treatment or medicines;• Unformulated wish for second opinions on minor ailments; and/or• Economic incentives (absence of a token fee for consultations or medicines).
The short duration of this otherwise valuable assistance leaves the local staff in a debilitatedand uncomfortable position. Statistics on numbers of consultations during this period alsotend to exaggerate the impact of the disaster and the relevance of the FFH.
13FOLLOW-UP TRAUMA AND MEDICAL CARE
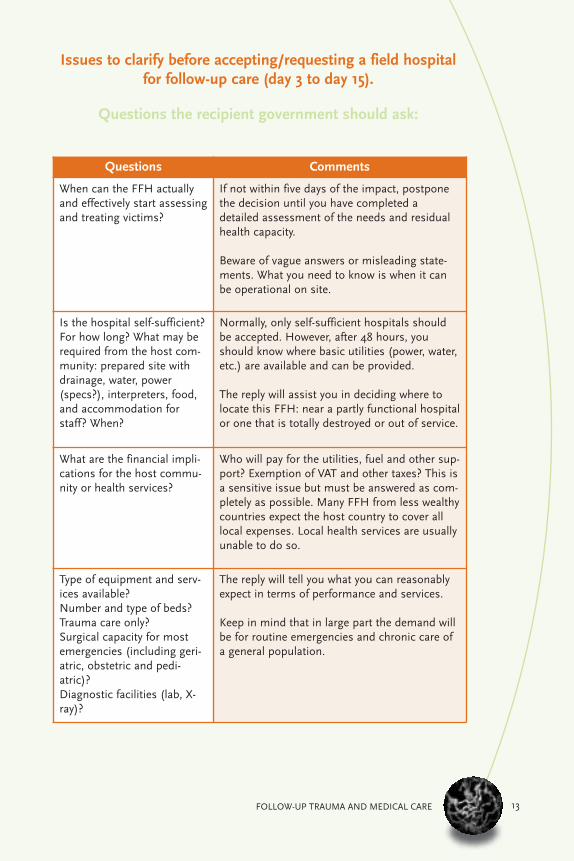
Issues to clarify before accepting/requesting a field hospitalfor follow-up care (day 3 to day 15).
Questions the recipient government should ask:
Questions Comments
When can the FFH actuallyand effectively start assessingand treating victims?
If not within five days of the impact, postponethe decision until you have completed adetailed assessment of the needs and residualhealth capacity.
Beware of vague answers or misleading state-ments. What you need to know is when it canbe operational on site.
Is the hospital self-sufficient?For how long? What may berequired from the host com-munity: prepared site withdrainage, water, power(specs?), interpreters, food,and accommodation forstaff? When?
Normally, only self-sufficient hospitals shouldbe accepted. However, after 48 hours, youshould know where basic utilities (power, water,etc.) are available and can be provided.
The reply will assist you in deciding where tolocate this FFH: near a partly functional hospitalor one that is totally destroyed or out of service.
What are the financial impli-cations for the host commu-nity or health services?
Who will pay for the utilities, fuel and other sup-port? Exemption of VAT and other taxes? This isa sensitive issue but must be answered as com-pletely as possible. Many FFH from less wealthycountries expect the host country to cover alllocal expenses. Local health services are usuallyunable to do so.
Type of equipment and serv-ices available?Number and type of beds?Trauma care only?Surgical capacity for mostemergencies (including geri-atric, obstetric and pedi-atric)?Diagnostic facilities (lab, X-ray)?
The reply will tell you what you can reasonablyexpect in terms of performance and services.
Keep in mind that in large part the demand willbe for routine emergencies and chronic care ofa general population.
14 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
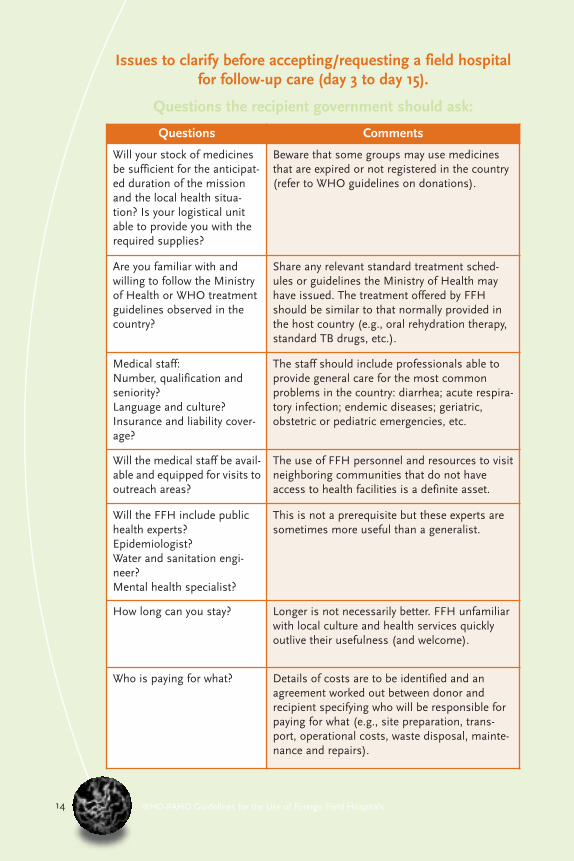
Questions Comments
Will your stock of medicinesbe sufficient for the anticipat-ed duration of the missionand the local health situa-tion? Is your logistical unitable to provide you with therequired supplies?
Beware that some groups may use medicinesthat are expired or not registered in the country(refer to WHO guidelines on donations).
Are you familiar with andwilling to follow the Ministryof Health or WHO treatmentguidelines observed in thecountry?
Share any relevant standard treatment sched-ules or guidelines the Ministry of Health mayhave issued. The treatment offered by FFHshould be similar to that normally provided inthe host country (e.g., oral rehydration therapy,standard TB drugs, etc.).
Medical staff:Number, qualification andseniority?Language and culture?Insurance and liability cover-age?
The staff should include professionals able toprovide general care for the most commonproblems in the country: diarrhea; acute respira-tory infection; endemic diseases; geriatric,obstetric or pediatric emergencies, etc.
Will the medical staff be avail-able and equipped for visits tooutreach areas?
The use of FFH personnel and resources to visitneighboring communities that do not haveaccess to health facilities is a definite asset.
Will the FFH include publichealth experts?Epidemiologist?Water and sanitation engi-neer?Mental health specialist?
This is not a prerequisite but these experts aresometimes more useful than a generalist.
How long can you stay? Longer is not necessarily better. FFH unfamiliarwith local culture and health services quicklyoutlive their usefulness (and welcome).
Who is paying for what? Details of costs are to be identified and anagreement worked out between donor andrecipient specifying who will be responsible forpaying for what (e.g., site preparation, trans-port, operational costs, waste disposal, mainte-nance and repairs).
Issues to clarify before accepting/requesting a field hospitalfor follow-up care (day 3 to day 15).
Questions the recipient government should ask:

15FOLLOW-UP TRAUMA AND MEDICAL CARE
Issues to clarify before accepting/requesting a field hospitalfor follow-up care (day 3 to day 15).
Questions the donor should ask:
Questions Comments
Where (city, village, or community)should we install the FFH? Availableutilities: water, power, etc? Nearest health facility or hospital?Is the site prepared to install theFFH?
Details on the site requirements (area,drainage, etc.) and the need for utilitiesshould be provided to facilitate decision-making by the authorities. Field hospi-tals are expected to be self-sufficient.
What will be provided as a counter-part contribution (no cost to thedonor) by the host country? Sitepreparation, utilities, security, addi-tional staff, transportation, accom-modation?
Ideally, the FFH should be donated witha budget to cover all local expenses,from utilities to hiring local staff. If thisis not the case, specify in advance whatyou expect as a counterpart contributionfrom the host country.
Whom should we report to in thecapital and locally?
The FFH must report to theregional/local health authority. Clarifythe channel: The director of the hospi-tal? Someone else?
Will the Ministry of Health assign apermanent liaison officer to theFFH?
A liaison officer assigned from the hostMinistry of Health to the FFH will facili-tate smooth coordination.
Size of the population? Number andseverity of injuries? Any particularhealth problem in this community?
This information is important but oftenis unavailable at the time of deployment.
Status of the (nearest) local hospitalor health center? What type of servic-es is it able to offer? If damaged andout of service, what will be the roleof the local health staff? Should theybe absorbed and utilized?
It is essential to determine whether theFFH will supplement or replace the localfacility. Local health workers must beintegrated into the FFH if the local facili-ty is destroyed.
What information and reports willthe host country require?Should the local reporting format beused or adapted?
Reporting on activities and diseases in aformat required by the host health serv-ices is an obligation of the FFH, includ-ing military ones.

16 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
The use of donated, transportable hospitals may appear touninformed decision-makers as the ideal no-cost, ready-to-use alter-native pending the repair or reconstruction of a major health facility.However, it is not the miracle solution anticipated by health author-ities of the host country.
The deployment of FFHs presents particular challenges andshould be considered cautiously. In the aftermath of recent disas-ters, hasty political decisions and unrealistic expectations havecaused problems ranging from inadequate facilities for patients andstaff, unexpected costs to the host and political misunderstandingsbetween both parties.
National authorities should approach the issue of a donationof a FFH in terms of providing a durable, temporary hospital (rehabil-itation phase) until a permanent solution (reconstruction phase) isavailable. A mobile FFH is one of the many alternatives for the pro-vision of routine health care and must be considered on the basis ofcost-effectiveness and cost-benefit.
(from Second Monthto Several Years)
Donation of FFH(Without Personnel)
to Serve as aTemporary Hospital

17
Essential requirements:
• Lack of other more cost-effective alternatives
Donating field hospitals involves serious expenditures forboth the donor and recipient (transportation, maintenance, utili-ties). Field hospitals are not cost-effective from either the recipient’sor donor’s point of view.
Given the expected duration of the need for temporary facili-ties (years and not months as generally expected by local healthadministrators) and the technical shortcomings of this solution,other and more suitable temporary facilities should be proposedusing the funds assigned to this highly visible measure. It is recom-mended that the donor consider building a more durable temporaryfacility using, by order of priority: pre-fabricated modules, metal con-tainers, wood and plywood, and adaptation of an existing building.
Should funds be earmarked exclusively for the donation of aFFH, some additional conditions should be met.
• Appropriate standards for both the patients and the staff
Considering the duration of the use of the temporary facilitiesand the admission of long-term patients, the FFH should provide alevel of comfort for patients, health workers and support personnelin terms of space, temperature control and resistance to water andother environmental elements appropriate to the local climatic con-ditions.
Similarly, the donated medical equipment should meet thestandards to which the health services are accustomed. These stan-
dards will vary from country tocountry and from urban to ruralareas.
• Design for use until finalreconstruction
A temporary accom-modation should be able towithstand abuse and poormaintenance, and remainwater-tight and functional
DONATION OF FFH (WITHOUT PERSONNEL)
18 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
for the anticipated duration of reconstruction of the damaged hospi-tal (generally two years or more). Tents and inflatable modules dete-riorate due to lack of maintenance and careless handling by the staffand public. Under the best care, tents must be replaced every sixmonths. Steel containers have a much longer useful life makingthem a more durable choice. Prefabricated modules also offer attrac-tive solutions and allow more flexibility in selecting or using medicalequipment.
The initial time frame for a field hospital given as a donationshould be for a period of one year with the possibility of extensiononly by agreement between the donor and recipient. (This time limitshould serve to stimulate national officials to completerepairs/rebuilding of the damaged/destroyed facility.)
• Installation and maintenance support provided at no cost tothe affected country
Deployment and maintenance of a field hospital is a complextask requiring significant support from the donor institution. A for-mal agreement between the donor and recipient for a mutuallyagreed period of time2 must be formulated, including:
• Operational and financial responsibility of the donor foron-site installation of the facility as well as its “sustain-ment” (this military term includes daily maintenance,preservation and preventive replacement);
• Provision of spare parts especially for equipment notavailable locally;
• Training of the medical/technical staff and the mainte-nance personnel in the use and care of the equipment;
• Clear definition of responsibilities of each party includingthe conditions for transfer of responsibilities;
• Mechanism for joint evaluation of the hospital use, itscost-effectiveness and cost-benefit.
2 The agreement should cover the replacement of all tents and similar material every six months.Costs for such sustainment over one year will exceed those required for building temporaryfacilities that could last for several years.
DONACION DE UN FHH (SIN PERSONAL) 19
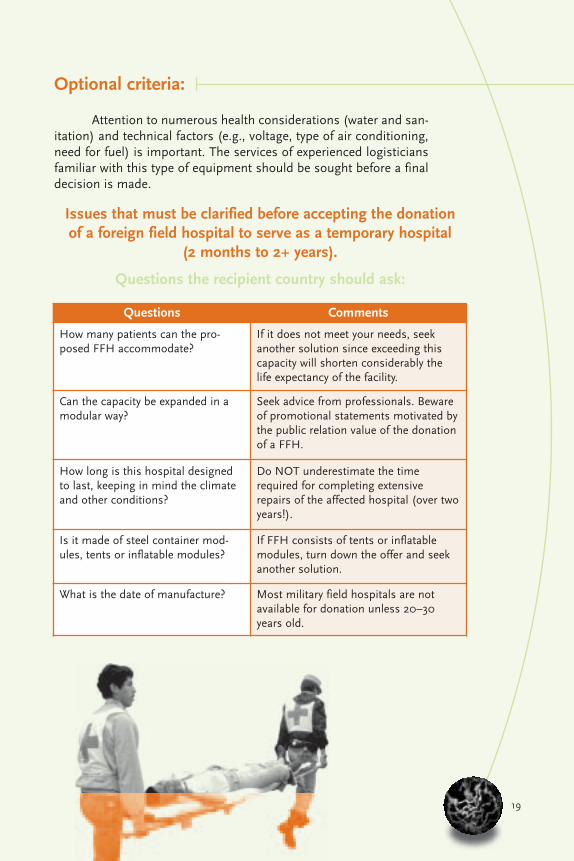
Optional criteria:
Attention to numerous health considerations (water and san-itation) and technical factors (e.g., voltage, type of air conditioning,need for fuel) is important. The services of experienced logisticiansfamiliar with this type of equipment should be sought before a finaldecision is made.
Issues that must be clarified before accepting the donationof a foreign field hospital to serve as a temporary hospital
(2 months to 2+ years).
Questions the recipient country should ask:
Questions Comments
How many patients can the pro-posed FFH accommodate?
If it does not meet your needs, seekanother solution since exceeding thiscapacity will shorten considerably thelife expectancy of the facility.
Can the capacity be expanded in amodular way?
Seek advice from professionals. Bewareof promotional statements motivated bythe public relation value of the donationof a FFH.
How long is this hospital designedto last, keeping in mind the climateand other conditions?
Do NOT underestimate the timerequired for completing extensiverepairs of the affected hospital (over twoyears!).
Is it made of steel container mod-ules, tents or inflatable modules?
If FFH consists of tents or inflatablemodules, turn down the offer and seekanother solution.
What is the date of manufacture? Most military field hospitals are notavailable for donation unless 20–30years old.

20 WHO-PAHO Guidelines for the Use of Foreign Field Hospitals
Issues that must be clarified before accepting the donationof a foreign field hospital to serve as a temporary hospital
(2 months to 2+ years).
Questions that the recipient country should ask:
Questions Comments
Is the donor willing to assumeoperational and financial responsi-bility for complete installation(including site preparation,drainage, etc.) as well as daily andperiodic maintenance (includingreplacement as needed) for theintended duration?
Maintenance of FFH is demanding, costly andtime-consuming. Hospital engineers are notequipped and are too busy for this task. If thedonor is not willing to assume full responsibility(assigning funds and staff), seek another alter-native in order to avoid disappointment andmisunderstandings from all parties.
Are those funds potentially avail-able for the building of moredurable temporary facilities?
Considerable funds are required, often fromboth the donor and the recipient, to make aFFH serve satisfactorily as a temporary civilianfacility. If the answer to the question is “yes”,suggest that the donors build a temporarywood/plywood or metal container facility.
If the funds are earmarked exclusively for the donation of this FFH, technical expertsshould discuss:
Site requirements Drainage of the site is critical. Access to utilitiesand sewage cannot be improvised.
Power and utility needs (and cost) Military equipment may have special require-ments for fuel (aviation) or power.
Specifications of the medico-surgi-cal equipment
In most instances, the hospital staff will find itmore convenient to salvage equipment from thedamaged hospital rather than use outdatedmaterial designed for military use.
Air-conditioning: Compatibilitywith isolation of patients withinfectious diseases
A closed circuit system is most common andincreases the risk of circulating pathogens.
Is the donor willing to support thecost of the travel of experts fromthe recipient country to discusstechnical specifications with med-ical logisticians who are familiarwith specific equipment?
Many additional questions will need to beanswered by experts before deciding whetherthe donation will benefit the patients ratherthan becoming a source of embarrassment.

Natural and complex disasters can cause a dramatic increase in the demand for emergencymedical care. Local health services can be overwhelmed, and damage to clinics and hospi-tals can render them useless.
Many countries maintain mobile field hospi-tals for defense or humanitarian purposes.Dispatching these facilities to disaster-affect-ed countries would seem to be the idealresponse to emergency medical needs.Unfortunately, experience has shown that inthe case of natural disasters field hospitalsoften have not met the expectations of recip-ients and donor institutions. In July 2003, the World Health Organizationand Pan American Health Organizationsponsored a workshop in El Salvador to dis-cuss the pros and cons of using foreign fieldhospitals in the aftermath of natural disas-ters. These guidelines are the result of thatworkshop.
The workshop participants identified different phases when foreign field hospitals and special-ized medical personnel are most useful. They can provide advanced trauma care and life sup-port if at the disaster site within 48 hours of the impact of an event; they would provide fol-low-up care for trauma victims and resumption of routine medical care in the two weeks fol-lowing the event; during rehabilitation and reconstruction phases (from two months to twoor more years), a field hospital might serve as a temporary replacement for damaged healthfacilities. These guidelines propose conditions that field hospitals and their staff shouldmeet for each of these phases. The guidelines also outline issues that authorities in donorcountries and disaster-affected countries should discuss before mobilizing a field hospital.