willcoxgyrolab15
TRANSCRIPT
IntroductionDuring the clinical drug development stage, moving from Phase I first-in-human, healthy volunteer studies into Phase II/III disease-state population studies is a critical stage for a molecule. The focus has moved from a safety-first perspective to an efficacy, effectiveness and safety perspective. Biological matrices such as human serum/plasma contain a large mix of complex circulating proteins, including components such as hormones, antibodies, electrolytes and more (Figure 1). The composition of human serum can vary wildly between each individual in the healthy population (sex, race, age) and even more so in disease-state populations. This can have a large impact on clinical pharmacokinetic (PK) assays, as it is important that clinical PK assays are developed and validated using matrix appropriate for the destined dosed population, be it normal healthy volunteers (NHV) in Phase I studies or disease-state individuals in Phase II/III studies.
Figure 1. Plasma protein composition, A) high-abundance proteins; B) moderate- and low-abundance proteins.
Case Study InformationThis case study follows the development and validation of a PK assay for a monoclonal antibody (mAb) therapeutic in support of the Phase I and Phase II/III clinical trials for this molecule. The initial development activities were performed in-house by Novimmune and used the Gyrolab platform.
Gyrolab™ PlatformThe standard microtitre plate sandwich format (Figure 2) is followed by the Gyrolab platform with each step, capture-analyte-detection (Figure 3) added consecutively but separated by wash cycles. The platform uses fluorescence for analyte detection using a laser to excite detection reagents tagged with Alexa Fluor® 647. Due to the Gyrolab’s nanolitre scale format results can often be achieved within 1 hour.
Development StrategyThe development strategy adopted by Novimmune was to develop and validate an assay to support the Phase I clinical trial and therefore get a fully functional assay in NHV matrix before assessing the disease population. This is a common step-wise strategy adopted by the industry; however, it requires most, if not all assay parameters to be re-assessed within a new development/validation study before Phase II/III studies take place. It is important to consider the later stage work at this point to make sure the assay format used is transferable into the relevant disease-state. An alternative strategy is to begin the assay development including matrix from the Phase II/III disease-state population. This often makes the initial costs higher and is a riskier approach as there are no guarantees a compound will progress beyond Phase I.
Phase I Assay ParametersNovimmune was successful in developing an assay in NHV serum in-house. This assay was then successfully transferred into and validated at Covance with the following parameters achieved: Assay Range: 4.00-6900.00 ng/mL
Intra/Inter-Assay Accuracy and Precision: Pass: All QC levels within ±20% of nominal concentrations and within ±20% precision
Room Temperature Stability: 24 hours
Freeze/Thaw Stability: 5 additional cycles
Dilutional Linearity: 1 in 2,560 dilution (in addition to 1 in 4 MRD)
Selectivity: Pass: 95.00% of individuals within ±20 %RE of nominal concentration at LoQC and HiQC
Long-Term Freezer Stability: 12 months
Considerations for Clinical Pharmacokinetic Assays When Moving from Healthy Volunteers to Disease-State PopulationsSam Willcox1, Justine Collet2, Florence Guilhot2, Graeme Evans1, Ian Skitt1 and Robert Nelson21Covance Laboratories Ltd, Harrogate, UK; 2Novimmune SA, Geneva, Switzerland
Presented at the Gyrolab User Seminar, London, June 8-9th, 2015
Disease-State MatrixMoving the method into supporting the Phase II/III studies required the introduction of the disease-state population matrix, which can cause problems due to the additional variable factors that occur. These can include, but are not limited to:
▶ Increase/decrease soluble drug target▶ Increase/decrease in endogenous target ligands▶ High frequency of co-medications ▶ Increase/decrease or abnormal protein components▶ Autoimmunity ▶ Higher hormone/cytokine interference
Increasingly, a decision is made to cross-validate all parameters using both NHV and disease-state serum when moving into Phase II/III. This provides a robust set of data for comparison and means NHV matrix may be used for the preparation of calibrators and QC samples within the sample analysis, reducing costs and matrix sourcing difficulties associated with disease-state matrix.
Moving into Disease-State MatrixAs we moved into the Phase II/III development, a decision was taken to increase the lower limit of quantification (LLoQ) of the assay from 4.00 to 8.00 ng/mL. This decision was taken because matrix effects are typically more pronounced in the lower concentrations of an assay and often more so in the disease-state. During the validation of the Phase I study, the precision and accuracy of the LLoQ was acceptable but a little higher than desired (Figure 4). Due to the introduction of the disease-state matrix and because such a level of sensitivity was not required, the LLoQ was raised and the range of the assay modified.
Figure 4. LLoQ (4 ng/mL) mean concentrations in relation to %bias during the Phase I first-in-human study.
During the in-house development at Novimmune, poorer precision and accuracy was noted at the upper end of the calibration curve for the upper limit of quantification (ULoQ) standard and the top anchor point (6900 and 20000 ng/mL, respectively). Truncating the upper range slightly did not improve the robustness. A comparison of the signal amplification (PMT) settings was performed; the setting used in the Phase I assay (5%) was compared against a setting with lower sensitivity in fluorescence detection (1%). Figure 5 shows an overall reduction in relative error (RE) with the reduction in signal amplification settings.
Figure 5. Relative error of calibration curve concentrations across multiple runs when analysed with two different photo multiplier tube (PMT) settings.
Phase II/III Assay Parameters Moving the assay into Phase II/III required the following parameters to be re-assessed:
▶ Intra/inter-assay accuracy and precision of QC samples performed in disease-state/NHV serum
▶ Matrix effects performed in disease-state serum
▶ Room temperature and freeze-thaw stability performed in disease-state serum
▶ Long-term freezer stability performed in disease-state serum
▶ Dilutional linearity performed in disease-state serum
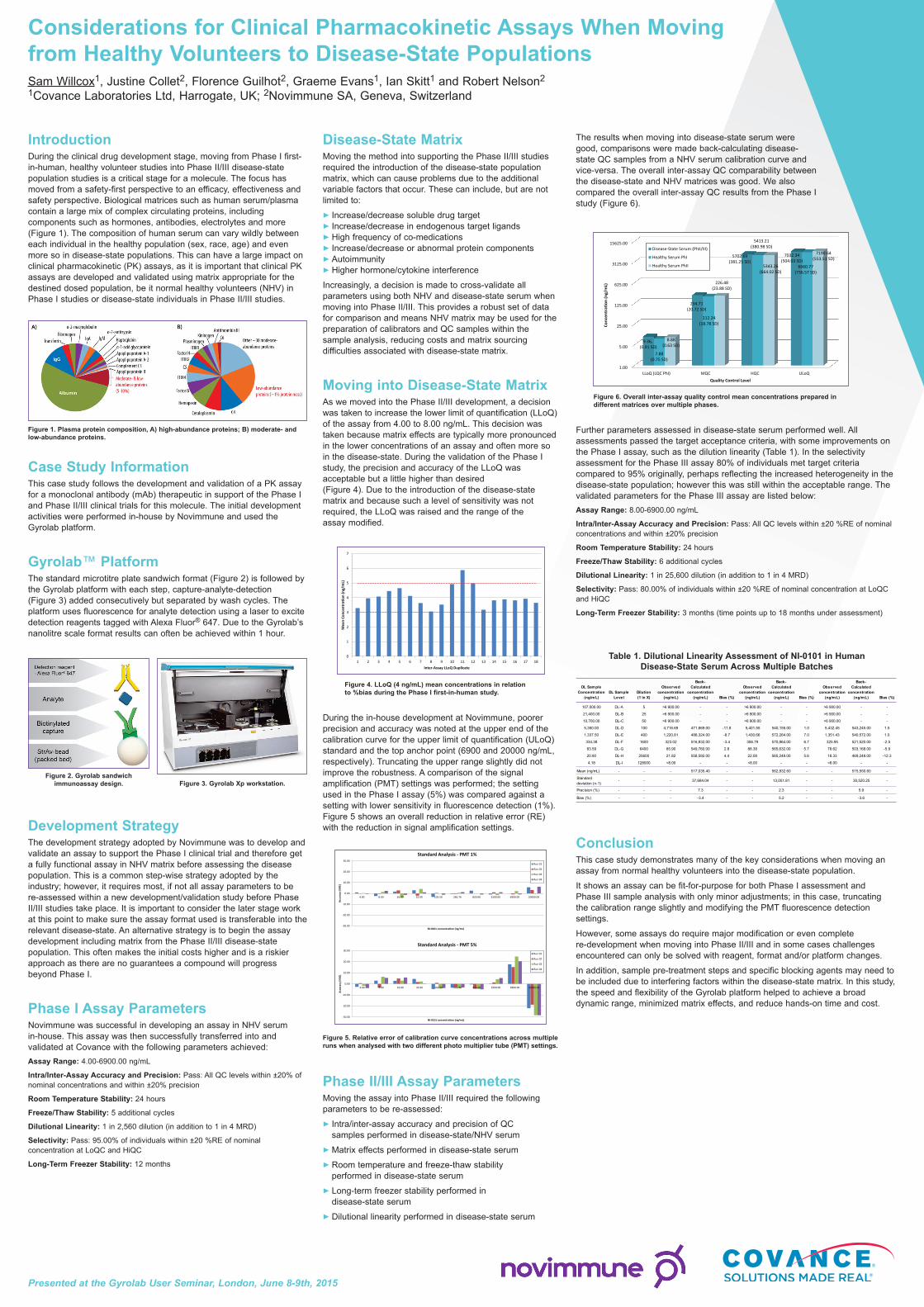
The results when moving into disease-state serum were good, comparisons were made back-calculating disease-state QC samples from a NHV serum calibration curve and vice-versa. The overall inter-assay QC comparability between the disease-state and NHV matrices was good. We also compared the overall inter-assay QC results from the Phase I study (Figure 6).
Figure 6. Overall inter-assay quality control mean concentrations prepared in different matrices over multiple phases.
Further parameters assessed in disease-state serum performed well. All assessments passed the target acceptance criteria, with some improvements on the Phase I assay, such as the dilution linearity (Table 1). In the selectivity assessment for the Phase III assay 80% of individuals met target criteria compared to 95% originally, perhaps reflecting the increased heterogeneity in the disease-state population; however this was still within the acceptable range. The validated parameters for the Phase III assay are listed below:Assay Range: 8.00-6900.00 ng/mL
Intra/Inter-Assay Accuracy and Precision: Pass: All QC levels within ±20 %RE of nominal concentrations and within ±20% precision
Room Temperature Stability: 24 hours
Freeze/Thaw Stability: 6 additional cycles
Dilutional Linearity: 1 in 25,600 dilution (in addition to 1 in 4 MRD)
Selectivity: Pass: 80.00% of individuals within ±20 %RE of nominal concentration at LoQC and HiQC
Long-Term Freezer Stability: 3 months (time points up to 18 months under assessment)
Conclusion This case study demonstrates many of the key considerations when moving an assay from normal healthy volunteers into the disease-state population.
It shows an assay can be fit-for-purpose for both Phase I assessment and Phase III sample analysis with only minor adjustments; in this case, truncating the calibration range slightly and modifying the PMT fluorescence detection settings.
However, some assays do require major modification or even complete re-development when moving into Phase II/III and in some cases challenges encountered can only be solved with reagent, format and/or platform changes.
In addition, sample pre-treatment steps and specific blocking agents may need to be included due to interfering factors within the disease-state matrix. In this study, the speed and flexibility of the Gyrolab platform helped to achieve a broad dynamic range, minimized matrix effects, and reduce hands-on time and cost.
0
1
2
3
4
5
6
7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Mea
n Co
ncen
trati
on (n
g/m
L)
Inter-Assay LLoQ Duplicate
1.00
5.00
25.00
125.00
625.00
3125.00
15625.00
LLoQ (LQC PhI) MQC HQC ULoQ
9.36,(0.91 SD)
234.71(20.72 SD)
5702.69(381.25 SD)
7032.34(504.03 SD)
7.88(0.75 SD)
212.24 (18.78 SD)
5413.21(380.98 SD)
6660.77(736.57 SD)
8.88(0.63 SD)
226.48(23.88 SD)
5343.26(664.02 SD)
7190.64(553.51 SD)
Conc
entr
ation
(ng/
mL)
Quality Control Level
Disease-State Serum (PhII/III)
Healthy Serum PhI
Healthy Serum PhII
-30.00
-20.00
-10.00
0.00
10.00
20.00
30.00
4.00 8.00 16.00 32.00 102.50 282.76 820.00 2500.00 6900.00 20000.00
Accu
racy
(%RE
)
NI-0101 concentration (ng/mL)
-30.00
-20.00
-10.00
0.00
10.00
20.00
30.00
4.00 8.00 16.00 32.00 102.50 282.76 820.00 2500.00 6900.00 20000.00
Accu
racy
(%RE
)
NI-0101 concentration (ng/mL)
Standard Analysis - PMT 1%
Standard Analysis - PMT 5%
Run 01
Run 02
Run 03
Run 04
Run 01
Run 02
Run 03
Run 04
Figure 2. Gyrolab sandwich immunoassay design. Figure 3. Gyrolab Xp workstation.
DL Sample Concentration
(ng/mL)DL Sample
LevelDilution (1 in X)
Observed concentration
(ng/mL)
Back-Calculated
concentration (ng/mL) Bias (%)
Observed concentration
(ng/mL)
Back-Calculated
concentration (ng/mL) Bias (%)
Observed concentration
(ng/mL)
Back-Calculated
concentration (ng/mL) Bias (%)
107,000.00 DL-A 5 >6 900.00 - - >6 900.00 - - >6 900.00 - -
21,400.00 DL-B 25 >6 900.00 - - >6 900.00 - - >6 900.00 - -
10,700.00 DL-C 50 >6 900.00 - - >6 900.00 - - >6 900.00 - -
5,350.00 DL-D 100 4,716.69 471,669.00 -11.8 5,401.55 540,155.00 1.0 5,432.45 543,245.00 1.5
1,337.50 DL-E 400 1,220.81 488,324.00 -8.7 1,430.66 572,264.00 7.0 1,351.43 540,572.00 1.0
334.38 DL-F 1600 323.02 516,832.00 -3.4 356.79 570,864.00 6.7 325.95 521,520.00 -2.5
83.59 DL-G 6400 85.90 549,760.00 2.8 88.38 565,632.00 5.7 78.62 503,168.00 -5.9
20.90 DL-H 25600 21.82 558,592.00 4.4 22.08 565,248.00 5.6 18.33 469,248.00 -12.3
4.18 DL-I 128000 <8.00 - - <8.00 - - <8.00 - -
Mean (ng/mL) - - - 517,035.40 - - 562,832.60 - - 515,550.60 -
Standard deviation (n-1)
- - - 37,684.04 - - 13,051.81 - - 30,520.25 -
Precision (%) - - - 7.3 - - 2.3 - - 5.9 -
Bias (%) - - - -3.4 - - 5.2 - - -3.6 -
Table 1. Dilutional Linearity Assessment of NI-0101 in Human Disease-State Serum Across Multiple Batches