world health organization meeting on the guidelines … health organization meeting on the...
TRANSCRIPT

World Health Organization
Meeting on the Guidelines for Drinking-water Quality
Microbial Aspects Working Group Meeting
Chemical Mixtures Meeting
5–7 June 2014
Singapore
Geneva, 2014

World Health Organization Meeting on the Guidelines for Drinking-water Quality
World Health Organization 2014 All rights reserved. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. This publication contains the collective views of an international group of experts and does not necessarily represent the decisions or the policies of the World Health Organization.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
iii
CONTENTS ABBREVIATIONS .............................................................................................................. iii
1. BACKGROUND .............................................................................................................. 4
2. OBJECTIVES OF THE MEETING ....................................................................................... 4
3. PARTICIPANTS .............................................................................................................. 4
4. ORGANIZATION OF THE MEETING ................................................................................. 4
5. OPENING SESSION ........................................................................................................ 5
5.1 Welcome by PUB, WHO Collaborating Centre ................................................................ 5
5.2 Update on key achievements on water quality and health............................................. 5
5.3 Future dissemination and format of the GDWQ ............................................................. 6
6. DECLARATIONS OF INTERESTS ....................................................................................... 8
7. PLAN OF WORK............................................................................................................. 9
7.1 Direct and indirect potable reuse .................................................................................... 9
#33. Potable reuse ............................................................................................................. 9
7.2 Chemical mixtures .......................................................................................................... 18
#52. Chemical mixtures .................................................................................................... 18
7.3 Chemical aspects ............................................................................................................ 23
#32a. Alternative disinfectants: Iodine ............................................................................ 23
#32b. Alternative disinfectants: Bromine ........................................................................ 26
#30. Alternative disinfectants: Silver ............................................................................... 28
7.4 Cross-cutting issues ........................................................................................................ 30
#36. Translating the Guidelines into national standards ................................................. 30
#34. Quality of the evidence ............................................................................................ 32
#37. PICO questions ......................................................................................................... 33
7.5 Microbial aspects ........................................................................................................... 34
#58. Revised structure of Chapter 7 ................................................................................. 34
#44. Multiple-barrier approach ....................................................................................... 35
#50. Reference pathogens ............................................................................................... 36
#41. Microbial fact sheets and pathogenic and non-pathogenic strains: Tables 7.1 and 7.2 ............................................................................................................................. 38
#46. Turbidity ................................................................................................................... 41
#43. Aggregating multiple steps for overall water treatment performance ................... 45
#51. QMRA ....................................................................................................................... 46

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
iv
#42. Background versus incidents (including short-term fluctuations) ........................... 48
#48. Microbial detection methods ................................................................................... 51
#39. Treatment tables ...................................................................................................... 52
#40. Water treatment and pathogens ............................................................................. 54
#45. Legionella ................................................................................................................. 54
#59. Rainwater harvesting ............................................................................................... 55
#49. Antimicrobial resistance ........................................................................................... 56
#47. Vulnerable populations ............................................................................................ 57
8. CLOSING SESSION ....................................................................................................... 57
ANNEX 1: List of participants for the WHO Meeting on the Guidelines for Drinking-water Quality ........................................................................................................................... 58
ANNEX 2: Agenda for the WHO Meeting on the Guidelines for Drinking-water Quality .... 64

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
iii
ABBREVIATIONS
ADI acceptable daily intake BDCM bromodichloromethane CT disinfectant concentration × contact time DALY disability-adjusted life year DBP disinfection by-product EFSA European Food Safety Authority FAO Food and Agriculture Organization of the United Nations GDWQ Guidelines for Drinking-water Quality GEMS Global Enteric Multicenter Study GRADE Grading of Recommendation Assessment, Development and Evaluation GRC Guidelines Review Committee (WHO) HAA halogenated acetic acid HACCP hazard analysis and critical control point IPCS International Programme on Chemical Safety (WHO) ISO International Organization for Standardization JECFA Joint FAO/WHO Expert Committee on Food Additives JMP Joint Monitoring Programme for Water Supply and Sanitation JMPR Joint FAO/WHO Meeting on Pesticide Residues KWR Kiwa Water Research LT2 Long Term 2 Enhanced Surface Water Treatment Rule (USEPA) mgd million gallons per day NDMA N-nitrosodimethylamine NSAID non-steroidal anti-inflammatory drug NTU nephelometric turbidity unit NUS National University of Singapore OECD Organisation for Economic Co-operation and Development PCB polychlorinated biphenyl PICO population, intervention, comparator, outcome PUB Public Utilities Board (Singapore) Q&A question and answer QMRA quantitative microbial risk assessment RegNet Regulators Network TCDD 2,3,7,8-tetrachlorodibenzo-p-dioxin TDI tolerable daily intake THM trihalomethane TTC threshold of toxicological concern USA United States of America USEPA United States Environmental Protection Agency VOC volatile organic compound WASH water, sanitation and hygiene WG working group WHO World Health Organization WSH Water, Sanitation, Health & Hygiene Programme (WHO) WSP water safety plan

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
4
1. BACKGROUND
A World Health Organization (WHO) Joint Expert Meeting on Water Quality and Health was held in Dübendorf, Switzerland, from 18 to 22 March 2013. Participants included WHO staff, representatives of the WHO regional offices and representatives of the expert groups responsible for preparing the WHO guidelines related to drinking-water, recreational water environments and the safe use of wastewater, excreta and greywater in agriculture and aquaculture. The key purpose of the Dübendorf meeting was to promote the harmonization of the drinking-water guidelines, the recreational water guidelines and the wastewater guidelines and to develop a workplan leading to the publication of the three revised guidelines by 2020. The experts recognized the importance of harmonized water quality regulations based on health (i.e. health-based targets), the concept of preventive health risk assessment and risk management (i.e. water safety plans [WSPs]) and water quality management. The key outputs of the Dübendorf meeting are being used as a guide to the future work on each of the WHO water quality guidelines. Following the Dübendorf meeting, WHO convened a technical meeting on 2–5 December 2013 bringing together experts to progress the workplan for the Guidelines for Drinking-water Quality (GDWQ). Although the meeting covered all aspects of the Guidelines, the focus was primarily on chemicals. The aim of the present meeting in Singapore is to progress the post–fourth edition workplan, especially on microbial aspects.
2. OBJECTIVES OF THE MEETING The objectives of the meeting were to:
Review progress to date on post–fourth edition activities of the GDWQ, with a particular focus on updates needed for the first addendum of the fourth edition related to microbial aspects;
Determine next steps in developing the first addendum of the fourth edition of the GDWQ related to microbial aspects; and
Further the work on chemical mixtures in drinking-water and source water.
3. PARTICIPANTS Twenty-six participants attended the meeting, including staff from WHO headquarters, experts on microbial aspects related to drinking-water quality (hereafter referred to as the Microbial WG), experts on chemical aspects related to drinking-water quality and chemical mixtures (hereafter referred to as the Chemical WG) and observers. A list of participants is given in Annex 1. 4. ORGANIZATION OF THE MEETING The meeting was organized by major themes (i.e. potable water reuse and chemical mixtures) as well as by working group issues (i.e. Microbial aspects, Chemical aspects and Cross-cutting

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
5
issues). Various participants chaired the individual sessions, and Marla Sheffer acted as rapporteur. The order of items presented in this meeting report reflects the order presented in the agenda, attached as Annex 2. It should be noted that some of the agenda items were discussed out of order during the meeting itself. It should also be noted that the agenda item on “Update on chemicals (selenium, uranium, manganese, aluminium, nickel, boron)” was not discussed, and the agenda items on “Quality of evidence”, “PICO questions” and “Vulnerable populations” were mentioned only briefly.
5. OPENING SESSION 5.1 Welcome by PUB, WHO Collaborating Centre Mong Hoo Lim, who is Chief Specialist (Water Quality), Water Quality Office, Public Utilities Board of Singapore (PUB), explained that PUB manages water quality, with an emphasis on the safety of drinking-water. The three key strategic thrusts of WaterHub, where the meeting was being held, are connect (a global water knowledge and connecting hub), academy (an institute of advanced learning for water professionals) and research and development (a vibrant water research and development incubator centre). PUB is a WHO collaborating centre and is very happy to be hosting and participating in this technical meeting, which is expected to be very informative and to provide PUB staff with access to resources from outside of PUB. 5.2 Update on key achievements on water quality and health
Bruce Gordon reminded participants that the close relationship between WHO and PUB Singapore began in Berlin in 2007. The highlight of this relationship to date was the launch of the fourth edition of the GDWQ in 2011 in Singapore, which concluded 10 years of work that accomplished many of the tasks detailed in the 2003 strategy. However, a lot of work on emerging issues, such as pharmaceuticals in water, and longstanding issues, such as arsenic, still remains, some of which was captured at the Tokyo meeting in 2010. At the same time, some marching orders from Member States, in the form of a World Health Assembly resolution, will take forward work on the GDWQ. The GDWQ are being taken up all over the world and are still among the most downloaded documents at WHO. One of the major accomplishments of the GDWQ is the introduction of WSPs, one of the main components of the framework for safe drinking-water. More than 50 countries in the world have scaled up plans to implement WSPs as part of their policies and strategies. A key performance indicator of WHO work in this area is the number of countries that have implemented WSPs, particularly in larger systems. Risk communication is a very important component of the GDWQ, and the Regulators Network (RegNet) helps communicate some of the guidance. The people attending this meeting include both new participants, to provide fresh ideas, as well as more experienced participants, to provide continuity. Bruce Gordon asked that chairs be clear about their objectives at the beginning of each discussion and clearly articulate the timelines for planned tasks.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
6
5.3 Future dissemination and format of the GDWQ
Sophie Boisson explained that publication of the first addendum of the GDWQ was planned for the last quarter of 2015, the second addendum for 2017 or 2018 and the fifth edition for 2020. Bruce Gordon noted that, in the past, WHO has published a print version of the addenda, correcting mistakes and updating the Guidelines under a rolling revision process. He suggested that a discussion on the process to be followed in the future might be useful, including whether print publication of addenda is necessary or whether only electronic publication would be sufficient. That wide-ranging discussion occurred at various times during the meeting, and the main comments are synthesized below: Policies and Procedures Manual
There needs to be more clarity in the Policies and Procedures Manual on the way in which supporting documents that are used as the basis for changes in the GDWQ are handled. Some are in production for long periods of time, others are expedited and still others are never released.
The different types of values derived for various chemicals (e.g. guideline values, health-based values, aesthetic values) should be clarified in the Policies and Procedures Manual.
The Policies and Procedures Manual is in a state of revision. There needs to be a discussion with this group on how to finalize this document.
Chemical aspects
Concerns have been raised that data have been misinterpreted or that some evidence has not been taken into account in establishing guideline values for certain chemicals. The group needs to be responsive to these concerns.
It needs to be clearly stated that even though some of the guideline values for chemicals are very old, they should not be revised unless there is a real demand for a revision or a substantial change in the science base. The implications for those implementing the Guidelines also need to be taken into consideration when deciding whether or not to revise a guideline value.
Although there needs to be stability in the guideline values, there is also a need to record new information. Perhaps there needs to be a public log in which it is recorded that new information is available and that the group is looking at it. If there is a major issue, the background document should be updated and disseminated quickly.
There is a need for more resources to bring older chemical background documents up to date (without necessarily changing the guideline values). For example, a recent Joint FAO/WHO Expert Committee on Food Additives (JECFA) assessment of arsenic is more up to date than the one in the GDWQ, and the background document should be updated to take it into account.
The differences between the different types of values derived for various chemicals (e.g. guideline values, health-based values, aesthetic values) are difficult to understand and should be clarified, both in the GDWQ and in the Policies and Procedures Manual. There is confusion between health-based values and aesthetic values with respect to manganese, for example, and the difference between a guideline value and a health-based value is not well understood. The differences between the different types of values need to be addressed to help Member States understand what they need to do in order to implement the Guidelines.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
7
Guideline values are not derived if a chemical is not likely to be found in drinking-water or if its concentration in drinking-water is well below the health-based value. However, there are still some areas where that chemical may occur. Although it was suggested that the policy determining when a guideline value is to be developed should be re-examined, it was pointed out that there are insufficient resources to include every chemical that could possibly occur in drinking-water somewhere in the world.
Health Canada creates a summary table to provide advice about the sources and the health implications of various drinking-water contaminants, which is easy to update when a new guideline value is derived or a guideline value is changed. This group may want to consider such a summary table for the future.
Microbial aspects
WHO appears to be tracking access to safe drinking-water using a different microbial value from that found in the GDWQ. The GDWQ use zero E. coli, but the Joint Monitoring Programme for Water Supply and Sanitation (JMP) appears to be using 10 E. coli per 100 mL. It was explained that some countries were unhappy with the way JMP was tracking access to safe drinking-water sources, and there was a lot of pressure on JMP to get a better understanding of water safety by adding a microbiological element to the metric used. A value of 10 E. coli per 100 mL was proposed by one of the JMP working groups to accommodate certain countries, but, in the face of overwhelming pushback, the task force finally accepted a value of zero E. coli to reconcile with the GDWQ.
In addition, some countries are using zero faecal coliforms instead of zero E. coli. Supporting Member States in using and implementing the GDWQ
The GDWQ are not readily accessible to and usable by all who need them. There may need to be a reconsideration of the usability of the Guidelines between now and 2020 to resolve this issue. Perhaps a small group should convene to discuss how to make the GDWQ more user friendly and to suggest the best way of delivering information.
There is a need for guidance to help Member States adapt the GDWQ to their own local situations. Although presenting more than one risk option in the Guidelines would provide more flexibility to Member States, which might want to choose a less conservative value, there is clarity in having a single value only. The document on translating guidelines into national standards should be a priority and should discuss the rational adaptation of risk assessment into standards. Perhaps there should be questions and answers (Qs&As) about the philosophy of the Guidelines, to help avoid misinterpretations. It is not possible to provide every option for Member States, but it should be made clear that the Guidelines can be adapted for national circumstances.
The GDWQ are taken as mandatory universal standards in some countries, rather than as recommendations. The flexibility in their application needs to be emphasized and should be addressed in the Qs&As on translating the guidelines into national standards.
In applying the GDWQ, Member States should first adopt the WSP approach to determine what is important to their individual systems.
The fourth edition articulated a new direction, necessitating the inclusion of a lot of rich scientific information on WSPs, health-based targets, quantitative microbial risk assessment (QMRA), etc. Although these amendments have been necessary, it is clear that the new concepts have caused some difficulties for some users. Perhaps it is not necessary to order and structure the GDWQ as they are now. Some of the detailed

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
8
information could be moved into separate background or supporting documents or into an annex. A slimmer version of the GDWQ containing only essential information, including guideline values, would be more user friendly.
It was pointed out that this discussion on reducing the size of the GDWQ already took place in Dübendorf. If detailed information is taken out of the Guidelines, there will inevitably be requests for this information. The GDWQ are a point of departure and need to contain a body of science; otherwise, they are devalued. If the GDWQ become a summary list of guideline values, this would be a serious mistake, moving away from the philosophy of this group. The GDWQ could perhaps be thinned down a little, but the book is not much bigger than other similar guideline documents around the world. In any case, no drastic change to the document can be made until 2020.
The GDWQ apply across the board, from rainwater tanks to municipal supplies, so a lot of detail is necessary.
If the GDWQ do not articulate this group’s philosophy well enough, then they should be revised in the next edition.
WHO collaborating centres could possibly facilitate this process by hosting virtual communications. Perhaps a small working group should be convened to explore the possibilities of electronic publishing.
There is a need to keep working on communication aspects. “Regional days” (which started with the Expert Consultation for the Fourth Edition of the GDWQ held in Berlin in 2007, where the host WHO region communicated its regional concerns to the meeting participants), the new text on application of the Guidelines, small community water supply meetings, RegNet meetings and the rolling revision process all help in communicating information and keeping things up to date.
Translation of the GDWQ is needed, as English is not the first language for many regions. For the third edition, an effort was made to translate the GDWQ into the six official WHO languages, but funds ran out when Chapter 12 was reached. The fourth edition was not translated. Shorter documents get translated into at least two, and up to six, languages. Fundraising is needed for the translations.
Future work on the GDWQ
The call for experts is still in process. In future, a certain quorum of experts will gather to discuss a small number of agenda items rather than having a large meeting with 100 agenda items.
At the Dübendorf meeting, agenda items were assigned to high, medium or low priority, and at the Geneva meeting, tasks were assigned to the first or second addendum or the fifth edition. It might be useful to compile a list of items assigned to the first addendum, the second addendum and the fifth edition to facilitate the work of this group.
6. DECLARATIONS OF INTERESTS All experts participating in the meeting completed the WHO standard form for declaration of interests prior to the meeting. At the start of the meeting, all participants were asked to confirm their interests and to provide any additional information relevant to the subject matter of the meeting.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
9
The following participants declared current or recent (within the past year) financial interests related to commercial organizations:
Joe Cotruvo Personal consulting services to CocaCola, American Chemistry Council and Liquitech, to the combined value of > US$ 10 000 per annum.
John Fawell Personal consulting services to Thames Water, to the value of < US$ 5000 per annum. Personal consulting services to CocaCola, to the value of > US$ 10 000 per annum.
Shane Snyder Research unit is recipient of equipment and cash donations (Xylem Inc., Agilent Technologies and Trojan UV), to the combined value of > US$ 10 000 per annum.
Mark Sobsey Co-founder of Aquagenx, on the Science Advisory Board of Amway, to the combined value of > US$ 10 000 per annum.
On the basis of these declared interests, no significant conflict was registered in relation to the objectives of the meeting, considering the types of issues that were addressed. 7. PLAN OF WORK Each agenda item was discussed in detail, and a summary of the discussions as well as next steps were recorded for each. The numbering of the individual agenda items reflects the numbering system used in the previous meeting report (Geneva, 2013); the numbering was initiated in that meeting report and does not bear any relation to the numbers of agenda items in other meeting reports on the GDWQ. Agenda items that were not discussed at the previous meeting have been assigned new agenda numbers (starting at #52). The order of the agenda items below reflects the order given in the agenda in Annex 2. 7.1 Direct and indirect potable reuse
#33. Potable reuse Background: At the Dübendorf meeting, it was concluded that WHO should produce guidance on planned indirect potable reuse of treated wastewater, and this was considered a high-priority item. Pressure on water resources due to climate change, increases in population and the increasing size of cities has led to the proposal for and, in some cases, the implementation of planned indirect (and sometimes direct) reuse of wastewater in many countries. Treated wastewater is often used to augment drinking-water sources or replace drinking-water for non-potable uses in urban areas. There is a need for internationally recognized guidance for potable reuse to assist regulators, suppliers and health professionals. It would help improve the population’s perception about the safety and acceptability of, and need for, potable reuse of treated wastewater. The guidelines would take the form of a stand-alone document that sets the WHO Guidelines in the particular context of potable reuse, which fits with a number of ongoing initiatives, such as the desalination guidance.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
10
Progress since previous meeting:
A proposed plan of work for the preparation of the Guidelines for the Safe Potable Reuse of Treated Wastewater was prepared for discussion at the Singapore meeting.
Presentations: Overview of objectives and expected outcomes (Kah Cheong Lai) This issue, first discussed in Dübendorf, is important because of the impacts of factors such as population growth, drought and climate change on drinking-water sources. Singapore has been practising potable reuse for some time. At the December 2013 meeting in Geneva, many issues related to potable reuse were discussed, and these have been compiled in a background document provided to participants. The background document also gives a brief introduction to potable reuse, explains the different types of potable reuse and emphasizes the importance of potable reuse from a resource management and environmental perspective. What form the guidance on potable reuse should take – whether a stand-alone document or a section in Chapter 6 of the GDWQ, or both – is to be discussed at this meeting. Contributors to the text of the guidance need to be identified, and a timeline should be determined. Potable reuse practices and principles (Joe Cotruvo) Water reuse discussions and debates have been going on for some time now. There are several different types of potable reuse, including unplanned indirect potable reuse, where treated or untreated upstream surface water discharge is subjected to conventional drinking-water treatment; planned indirect potable reuse, involving either groundwater recharge or treated wastewater discharge to surface waters; blended direct potable reuse, where treated wastewater is added at the head of the drinking-water treatment plant or blended post-treatment; and pipe to pipe direct potable reuse. At the 1980 United States Environmental Protection Agency (USEPA) Airlie Conference, criteria and standards for potable reuse and possible alternatives were discussed. Prior to 1980, there was less wastewater treatment, there were few regulatory controls on industrial discharges, the Safe Drinking Water Act had just been passed and water technology was very primitive in terms of analytical chemistry, microbiology and treatment. Recommendations from the conference included the need for standards to define potable water regardless of its source, detailed characterization of source waters, more non-potable reuse options, and a recognition of the challenge of social perception and public acceptability. Many countries have now made progress with respect to secondary wastewater treatment requirements, reduced industrial discharges, pretreatment regulations, and sophisticated analytical and treatment technologies. There are several examples of advanced direct and indirect potable reuse dating from the 1960s, including, in the United States of America (USA), Los Angeles, California (involving groundwater recharge, secondary and tertiary treatment, surface spreading, soil aquifer treatment, at least 1 year of groundwater passage and conventional drinking-water treatment), Occuquan, Virginia (involving reservoir augmentation and tertiary treatment), Orange County, California (groundwater replenishment and seawater intrusion barrier), Cloudcroft, New Mexico (a proposed recycling system for the summer tourist season), and Big

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
11
Springs, Texas (where the natural source water is high in salinity); as well as Windhoek, Namibia (a final blend with about 30% recycled water), Singapore (NEWater) and even the International Space Station (urine distillate and air condensate recovery). Much has been resolved since 1980. Many source waters are much improved with respect to contamination. Source water discharge controls, pretreatment requirements, monitoring and process management, and technological options are all much improved. The microbial risk issues for highly treated water have been resolved, but the organics risk issue remains a philosophical one. Constant reliability is essential, as are multiple barriers. Consumer acceptability is still an issue – the goal is not to expect that everyone is going to want to drink the water, but to make the water safe for consumption. Unified drinking-water standards or guidelines are possible and needed, not separate reuse standards. What are the worst-case scenarios, how likely are they, and what is the risk to consumers? Is an environmental barrier or diversion or temporary storage required to deal with upsets? Available guidelines include the Australian potable reuse guidelines (2009) and the International Life Sciences Institute food and beverage guidelines (2013). The USA has initiated consensus guidelines, and the International Organization for Standardization (ISO) has a process in progress, but not for potable reuse. This is a timely initiative for WHO, as a lot of efforts are under way, and it would be useful to merge the thinking. Summary of discussion:
There is agreement that there is no need for separate standards for the quality of potable reuse water. Drinking-water is drinking-water, and there should be the same standards for all drinking-water.
Examples of where things have gone wrong with respect to potable reuse are needed. Although this could put people off, it is important to explain lessons learnt from things going wrong.
It is important to define an emergency situation. If there is deviation from an operational parameter in potable reuse, an emergency is declared. However, this is not always done for the normal drinking-water supply, although identifying the range of predictable events and responses is part of the WSP approach.
One of the principles is multiple barriers – not relying on a single technology to protect against exposure to a particular contaminant. If one part of the system is not operating fully, others will compensate.
The most crucial issue is public acceptance. Although people can be convinced that potable water reuse is a good strategy, this does not necessarily translate into total acceptance. Given the choice, these same people may use water filters or drink bottled water at home. In Australia, only one of two schemes has succeeded in dealing with public acceptance. Political acceptance can be far more important than public acceptance and is fraught with challenges.
The final guidance document needs to place this issue in the context of water scarcity and should address comments about public perception. It should provide guidance up front in the document on where and when to use potable reuse.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
12
Evidence gaps (John Fawell) Unplanned potable reuse is widely practised in Europe and elsewhere. WHO is in the process of developing new quality guidelines for planned potable reuse. The USA is currently developing guidelines for planned indirect and direct potable reuse, and Australia’s potable reuse guidelines are well advanced. Wastewater reuse is already important in small communities in many countries, particularly to support agriculture. The existing WHO guidelines for wastewater reuse for agriculture and aquaculture are highly technical, not well understood and underutilized. These guidelines will be revised in the future (by 2019) to provide practical guidance on reuse. Interim practical publications, to be published in 2015–2017, include those on urban reuse, updates on agriculture and aquaculture, biosolids use, indirect potable reuse and greywater use in buildings. Issues of concern may involve primarily perception and reassurance. In addition, there are emerging chemical (e.g. pharmaceuticals, personal care products, endocrine disruptors, perfluorinated compounds) and microbial issues. The form the guidance will take has not yet been decided. It will probably be similar to the desalination guidance, and it should be linked to the GDWQ. It will need to be based on WSPs, which provide a flexible way forward. Should it include process-based guidance, such as appropriate operational monitoring of processes, the capabilities of different technologies and treatment trains, etc.? Summary of discussion:
The USA has three different versions of potable reuse guidelines in process. California, in particular, has been regulating potable reuse for a long time.
The National Water Research Institute in the USA is convening a group to develop a white paper to describe the concepts and principles of potable reuse, then an industry consensus guideline. The USEPA may participate in this process.
The USEPA has potable reuse guidance that is primarily a compilation of information, but without any numerical guidelines.
The Australian framework for safe drinking-water (based on the principles of WSP) was adapted to recycled water.
Overconservatism in terms of chemical quality is a significant barrier to potable reuse. In the Australian guidelines, there are a lot more chemical guidelines for recycled water than for drinking-water. Massive lists of chemicals, some with real public health risks and others without, are not useful. If there are particular concerns, the GDWQ has a mechanism to deal with those. These potable reuse guidelines need to have broader application.
With respect to the approach for microbial quality, two sets of log reductions for potable reuse are available: Australia (8–9.5 log) and California (up to 12 log).
WHO needs to develop guidance that is applicable to less wealthy countries.
For potable reuse, WSPs and the GDWQ should apply, starting from the source, which could be raw sewage, all the way to the final product.
WHO needs to take a holistic approach to address non-potable reuse scenarios, some of which involve direct human exposure (e.g. produce irrigation). The need for water of an

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
13
appropriate quality that is fit for purpose should be articulated. However, potable reuse is a big enough task for this group, and another group is looking at non-potable reuse.
Guideline values must be derived from the best available scientific evidence and should not be based on public acceptance. Public communication is a separate issue from public safety, and safety should not be influenced by public acceptance.
Should this document be a guideline document that includes numbers? The GDWQ already contain guideline values for chemical quality of drinking-water. Is the remaining issue log reductions for microbial quality?
The document would be primarily on guidance, best practices, etc. It should include principles, approaches, multiple barriers, source protection, real-time monitoring and recommendations on overall log removal.
There is already a lot of information in one form or another in WHO documents. There is a need to make sure that the numbers of pathogens in raw sewage are appropriate, then to decide on log reductions on a QMRA basis to get down to acceptable levels of risk (e.g. 10−6 disability-adjusted life years, or DALYs). This is not so different from what we already have.
An existing approach (log reductions) and best practices (Chapters 7 and 8 of the GDWQ) are already available. There is a need to address chemicals that have been raised (e.g. personal care products, endocrine disruptors) and perhaps give stronger advice on how to deal with these (e.g. source control). There is a need to recognize that the source water in potable reuse is the worst possible source water.
Drinking-water should not be the sole focus. Domestic water is also used for showering, toilet flushing, etc. There is a need to clearly define what the guidelines are intended for.
The guidelines will differ depending on the applications and uses of the water (e.g. use for cooling towers, use of greywater in buildings). However, the focus should be on potable reuse as a priority.
Quantity and sustainability in the face of water scarcity are important issues. The sole focus should not be on water quality, such as log reductions, although it is recognized that safety is paramount and must never be compromised.
Emergency/disaster situations should be included.
Definitions of terms, such as direct potable reuse, need to be stated clearly, as there may be different international interpretations of the terminology used.
Regulatory aspects (David Cunliffe) The quality of source water for potable reuse is the poorest possible; the source water potentially contains microbial pathogens, pharmaceuticals, natural hormones, and industrial and agricultural chemicals. Regulators need to be satisfied that schemes will reliably produce safe drinking-water subject to good management. To accomplish this, regulators need to be engaged in the development of potable reuse schemes. The WHO framework for safe drinking-water is the basis for responding to the above challenges. In terms of health-based targets, 10−6 DALY per person per year should be used for microbial contaminants, with application of QMRA. This will require 8–10 log reductions for viruses, protozoa and bacteria from sewage. For chemicals, the guideline values from the GDWQ will apply, although trace organics, pharmaceuticals and personal care products, natural hormones, etc. will also need to be addressed (using, for example, tolerable daily intakes [TDIs] for food additives, threshold doses with safety factors, the threshold for

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
14
toxicological concern [TTC] approach, etc.). A mechanism for developing screening values is preferred to a long list of guideline values.
With respect to the first component of the WSP, hazard identification and risk assessment, data are available on concentrations of viruses, bacteria and protozoa in sewage, although percentages that are viable or infective are often not known. Chemical hazards will depend on discharges and activities in the catchment. As public perception can lead to increased attention being paid to pharmaceuticals, natural hormones and trace industrial chemicals, there is a need to strike a balance between responding to concerns and monitoring requirements. Control measures need to deal with microbial and chemical hazards. There is some variation in existing schemes, with conservative schemes including secondary treatment, ultrafiltration, advanced oxidation processes and reverse osmosis. The combinations of treatment processes do not matter, providing the end result meets the health-based targets. This needs to be validated before construction and installation. Validation incorporates removal/inactivation capabilities with the sensitivity of operational monitoring; in its purest form, sensitivity is equal to demonstrated hazard reduction (e.g. disinfection), but often it is less than demonstrated log reductions for many physical processes (and the lower figure is usually applied). It is crucial to identify operational monitoring programmes, including what needs to be monitored (e.g. turbidity), the monitoring frequency (usually continuous online), target criteria (early warning signal), critical limits (separate acceptable and unacceptable performance) and corrective actions. Examples of operational monitoring include, for reverse osmosis flow meters, measurement of conductivity and total organic carbon (as surrogates) and boron, N-nitrosodimethylamine (NDMA) and chloroform (as indicators). For verification monitoring, microbial parameters could include E. coli, coliphage and sulfate-reducing clostridia. Pathogen testing is not very meaningful, as safe water contains less than one virus or protozoan per several thousand litres. Chemical parameters could include those identified in the GDWQ, key organic chemicals (e.g. NDMA) as well as indicators or index parameters. Biological monitoring is also possible, but is not widely used at present. The selection of index chemicals is based on occurrence and physicochemical properties (size, polarity, functional groups, volatility), representatives of key groups (hormones, pharmaceuticals, etc.) and analytical capability. In Western Australia, 16 index chemicals (including indicators of disinfection by-products [DBPs] – chloroform and bromo-dichloromethane [BDCM]; indicators of pharmaceuticals – diclofenac and carbamazepine; an indicator of hormones – estrone; and indicators of volatile organic compounds [VOCs], metals, anions, organics and pesticides) are monitored to give confidence that the treatment processes are removing a broad range of organic chemicals. If an incident occurs and is not managed properly, the potential for harm can be very high. Incident protocols need to specify both the issue and time period (e.g. turbidity exceeding critical limit for 15 minutes), include all critical limits, include emergency contact personnel, specify reporting time frames, and specify who is briefed within organizations and the government and the time period for briefings.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
15
The following summarizes the required regulatory activities according to the component of the framework for safe drinking-water:
Health-based targets – identify/endorse
WSP – approve/audit
WSP (control measures and validation) – approve/endorse, confirm that health-based targets will be met
WSP (operational monitoring, including parameters, frequencies, critical limits) – approve/endorse
WSP (verification monitoring) – approve/endorse
WSP (incident protocol) – approve/endorse and participate
Surveillance – direct/perform. Summary of discussion:
There is a need to spend a lot of time with the utility identifying the issues, and it is very beneficial for the regulator to be involved in this process.
The use of indicators for monitoring is conceptually a very nice approach.
The index organisms reflect public perceptions and concerns and the public need for reassurance.
The set of indicators can be varied. All have some level of industrial input. Each utility should perform its own risk assessment, as per the GDWQ, then develop its own list of index chemicals.
The list of indicators utilized in Australia is similar to the list developed by California.
Drinking-water plans are audited every year, and changes to the list of indicators could result from the auditing.
Water utility perspective (Mong Hoo Lim) NEWater is used primarily for direct non-potable uses in Singapore. The entire water cycle must be managed from source to tap to produce drinking-water for potable use and from the collection of used water in sewers and treatment of the used water to produce NEWater for direct non-potable use. NEWater production processes include conventional treatment of used water followed by microfiltration/ultrafiltration, reverse osmosis and ultraviolet disinfection treatment. The water undergoes comprehensive water quality monitoring at all stages of the treatment and disinfection process. The NEWater is distributed to industrial consumers or sent to the reservoir, where it can then be used as a source of potable water following further treatment. A comprehensive sampling and monitoring programme (more than 133 000 tests) has been carried out on reclaimed water. Over 300 water quality parameters were tested, including those for which guideline values have been specified by WHO and the USEPA. These covered all categories of parameters, such as physical, inorganic and organic parameters, pesticides, radionuclides, wastewater signature compounds, synthetic and natural hormones, and microbiological parameters. In a comparison of the quality of PUB tap water with NEWater, the quality of NEWater consistently met the latest USEPA and WHO guidelines.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
16
Planned indirect potable use as a source of water supply is not new, but has been practised in several parts of the USA for more than 20 years. The organizational structure of the NEWater Study Project includes an expert panel (including Choon Nam Ong), a demonstration plant (a 10 000 m3/day advanced water reclamation plant that was designed following research and pilot plant studies and incorporating learning from overseas experiences, operational since 2000) and a sampling and monitoring programme (which includes 190 water quality parameters, including 100 specified by the USEPA and WHO). NEWater factories are located in Kranji (17 million gallons per day [mgd]), Bedok (18 mgd), Changi (50 mgd) and Ulu Pandan (32 mgd). The total NEWater supply network includes about 360 km of pipelines. It is important to link all of the NEWater factories and to manage NEWater demand as a whole. The primary purpose of NEWater is for direct non-potable reuse (non-domestic, commercial and industries), which frees up potable water for other purposes (domestic/residential). NEWater is used primarily for industrial processes (e.g. water fabrication, petrochemical, power plants, manufacturing), as well as for cooling towers, hospitals and institutions, and commercial buildings and, to a lesser extent, for general washing and toilet flushing. The secondary purpose of NEWater is for indirect potable reuse. NEWater meets about 30% of Singapore’s needs at present, which should increase to 40% by 2020. Public communication strategies include describing the processes in layman’s terms using non-technical language and illustrations, good branding and good choice of terminology (NEWater, not recycled or reclaimed water; used water, not wastewater; water reclamation, not sewage treatment). PUB and its parent ministry have carried out many activities to educate the public and gain public acceptance. Summary of discussion:
Reverse osmosis is very effective, and the 300 chemicals monitored in Singapore generally give negative results.
In Western Australia, there were a lot of negative results. The small detects before reverse osmosis were used to inform what might be included in the group of 16 index chemicals. Most schemes would start with a broad range of chemicals, as in the Singapore scheme, and then keep decreasing the number of chemicals monitored.
PUB has been using NEWater for some years. In that time, data on the lifespan of reverse osmosis (e.g. wear and tear, ageing of membrane) have been collected. PUB is willing to share some of the data collected over the years with its colleagues.
The nitrate concentration is a good indicator that the reverse osmosis membrane has aged.
It is very important to have a limited set of parameters in global guidance. It is difficult to communicate to the public why, after 5 years of non-detects, it is no longer necessary to evaluate those parameters. There should be an indication of those parameters that are very important for health and should always be monitored. For others, if they are not detected for 1 or 2 years, there should be no need to monitor them again.
It was agreed that a certain number of parameters, the ones identified as significant from the hazard identification, would not be dropped. However, even though heavy metals are

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
17
usually negative, they should not be dropped. If one is monitored, it would usually cover the whole group of heavy metals.
Summary of discussion (Kah Cheong) Suitable authors to contribute to developing these guidelines need to be identified. The key focus of the guidance will include the points below:
It is important to understand the need for potable reuse in the context of water quantity (scarcity) and water quality.
The focus should be on potable reuse, not all the other forms of reuse (there is already a lot of guidance on non-potable reuse). Boundaries need to be set, and terms need to be defined.
The point at which water is injected into the distribution system needs to be defined.
The GDWQ and the framework for safe drinking-water form a good basis for the guidance. Chemical indicators, in addition to what the GDWQ specify, can be included.
The WSP approach is the process to be used to monitor, approve and endorse schemes.
Summary of discussion:
This project is a high priority, as there is a lot of demand for guidance on potable reuse.
This should follow a similar process as was followed for the water safety in distribution systems text or the pharmaceuticals document. A physical meeting should be avoided until there is a robust document to review.
As using several authors with varying styles makes it difficult to ensure consistency, a consultant with technical knowledge in the area to take the lead role as author/writer may be beneficial. A sample of a section for determining the level of language and detail to use would be useful.
This could be a technical document that could be transformable to a chapter or a section of the Guidelines document, or it could be published as an addendum to the Guidelines. Either way, it will need to be included in the GDWQ Guidelines Review Committee (GRC) submission.
Input from Member States throughout the process is essential. Expected product(s): Potable reuse guidelines (by mid-2016) Next steps (Chemical and Microbial WGs):
A core group of volunteers was identified, and other authors will be pulled in as the project progresses. The core group includes David Cunliffe, Joe Cotruvo, USEPA (Lesley D’Anglada to suggest a participant), Michèle Giddings, Ana Maria de Rosa Husman, Choon Nam Ong, Shane Snyder, John Fawell (in a limited role) and Jiangyong Hu.
PUB will identify someone to coordinate the development of the document, as Kah Cheong Lai is ending his term in his present position at PUB and will not be available to coordinate this guidance document. WHO coordination (Jennifer De France, Sophie Boisson, Phil Callan) is also needed.
David Cunliffe was identified as lead author, responsible for continuity, incorporation of revisions and much of the writing in between contributions from selected specialists.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
18
The next task, after identification of a PUB coordinator, is to identify the contents (taking into consideration comments made at this meeting and the draft provided to participants), the authors of each section, potential authors of case-studies and reviewers (noting that a period of about 6 months needs to be allowed for review by the working group, then by outside reviewers).
David Cunliffe and the PUB coordinator will draft a table of contents, circulate it to the core group, then hold a teleconference to finalize the table of contents and identify authors.
7.2 Chemical mixtures
#52. Chemical mixtures1 Background: This is a WHO/USEPA collaboration on the management of chemical mixtures in drinking-water and source water. The tasks were to review available tools for human health risk assessment and management approaches, building on the already established WHO/International Programme on Chemical Safety (IPCS) framework methodology for such assessments; to explore innovative chemical grouping, screening and prioritization approaches; to provide practical recommendations to support risk assessment and risk management; and to identify key challenges and associated research needs. At the Dübendorf scoping meeting, convened in March 2013, discussions were initiated on these topics. The key outcome of the meeting was that there is sufficient information to develop a toolbox to help regulators address some chemicals in source water and drinking-water as groups. The toolbox should include information on available tools for the risk assessment of combined exposures to multiple chemicals, including temporal co-exposures (i.e. chemical mixtures). Potential for co-exposure, similar toxicity profiles or modes of action, common origins, and analytical and treatment aspects should be considered in grouping chemicals. The above factors for grouping of chemicals can be considered in the problem formulation stage of the WHO/IPCS framework. WHO commissioned Cranfield University to prepare a draft document entitled “Risk assessment and management of combined exposure to multiple chemicals in drinking-water and source water”, for discussion at the December meeting. Progress since previous meeting: Ruth Bevan updated the draft document based on feedback from the group at the December meeting. The revised document includes an example of a case-study and a map of other possible case-studies. Presentation (Ruth Bevan):
Managing all contaminants individually does not optimize the use of resources.
New approaches are needed to manage risk from contaminants sharing common features.
1 This agenda item was discussed at a separate meeting in Geneva 2013 and was not assigned an agenda number in the previous meeting report.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
19
The WHO/IPCS framework for combined exposure to multiple chemicals is the basis for this guidance document.
Sufficient information is available on combined exposures to develop a toolbox to help regulators address some chemicals in surface water and drinking-water as groups.
The purpose of the current document is to collate international efforts to address contaminants as groups rather than as single contaminants.
The second draft, provided to participants, contains amendments suggested following the meeting in Geneva in December 2013.
The main issues identified at that meeting were as follows: - ensuring consistency in terminology - making the document accessible to water regulators and suppliers in both developed
and developing countries - the addition of text regarding risk assessment practices for source water (initial step
to defining what will need to be assessed in drinking-water) - the best way to illustrate the use of the framework (de novo versus established
examples).
Points for discussion of the second draft include the following: - consistency of terminology - comments on new text - section 3 structure and worked example - tiers 0–3 worked examples for Appendix 4 - inclusion of the Cefic (combination effects of chemicals) decision-tree2 - the tone of the document.
Summary of discussion: Need for guidance
The USEPA initiated this project because it was faced with requests for dealing with mixtures (e.g. grouping all VOCs together) and wanted to look at ways this could be done. The final product is not guidelines, but provides tools to Member States to help them develop guidelines, if considered a priority.
Regulators are faced with demands to regulate many chemicals. The guidance provides a stepwise process to identify priorities and gain efficiencies in dealing with potential for combined exposures. The document can be thought of as a user’s guide: if regulators are faced with this issue, this is how they can approach it.
Most jurisdictions are faced with a need to consider combined exposure to multiple chemicals. This document provides some tools that can help them decide whether to invest more resources in going down the path of addressing risks from particular mixtures or deprioritize specific groupings based on preliminary consideration of available information.
When characterizing relative importance in terms of health, care needs to be taken not to suggest that chemical risk is more important than microbiological risk. The rationale behind this report is public perception, more than burden of disease.
2 Cefic decision-tree: http://www.cefic.org/Documents/PolicyCentre/ Identifying_and_assessing_chemical_combinations_of_concern_decision_tree_tool_explained.pdf

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
20
Terminology
Terminology in this document is a critical issue and needs to be made consistent with WHO/IPCS terminology. For example, combined exposures to multiple chemicals is preferred to chemical mixtures, as the latter implies temporal co-exposure.
The term “non-regulated contaminants” is a better term than “emerging contaminants” or “contaminants of concern”, as many are not new (although some of them are regulated, such as microcystins).
General content
The title is quite academic and maybe needs a subtitle.
An introductory section on the basics, including why regulators might want to use this, should be added.
It is important to frame this document for the intended audience. The audiences (both regulators and the regulated) should be defined at the outset. Early-tier assessment would be relevant to most evaluators.
The problem formulation examples need to be more drinking-water specific.
Text needs to be added on how this approach could be used in certain circumstances. This approach will allow developed countries to further improve their approach to risk assessment and aid risk assessment in developing countries.
Even if limited to the early tiers, the output can still be used in a communication context. This needs to be made clear.
An explicit description of how chemical mixtures have already been dealt with in the GDWQ needs to be included in this document.
It is important for scientific underpinnings and weaknesses to be clearly stated.
There needs to be more emphasis in the document on the communication aspects as one walks through a tiered analysis. For example, it is important that information on groups of chemicals that have been considered for combined exposure assessments, but set aside at early tiers, be communicated to a range of audiences internationally.
The document will not be cast in stone and is likely to need to evolve, as things change rapidly in this field.
What is or is not possible, what research is ongoing and what the knowledge gaps are need to be clarified.
A sentence should be added to indicate that some multiple exposures lead to less toxicity, rather than more toxicity (e.g. iodide and perchlorate).
Bette Meek has several suggestions for Ruth Bevan on how to change the problem formulation questions and on how to make sure the concepts fit together consistently, which she will pass on to her after the meeting.
Chemical groupings
Is the intent to group chemicals for regulatory purposes? Are scientific or practical aspects of grouping to be covered? VOCs, for example, share similar methods of analysis, but have very different toxicology.
Chemicals can be grouped based on different things, such as similar uses or applications, chemicals managed together and common target organs. Mode of action information is not available for the majority of chemicals. Even if there is not extensive mode of action information, it may be determined using this approach that the chemical grouping does not pose a risk.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
21
From a hazard perspective, there is no restriction to grouping by mode of action (e.g. chemicals with similar structures and target organs could be grouped). Restricting to grouping on the basis of mode of action biases to a very narrow group of compounds, as this information is lacking for the vast majority of chemicals. The WHO/IPCS framework is based on exposure and hazard, so analysis and treatment are not specifically illustrated in case examples for the framework currently.
Regulators can demonstrate that specified groups may not be a priority for consideration based on tiered analysis as outlined in the framework (e.g. pharmaceutical example in section 3).
E. coli (indicator) could be considered the simplest grouping for regulatory purposes.
The document will not make recommendations to group chemicals. Rather, it will provide the tools with which to group and assess chemicals if regulators are faced with this issue.
Should we be more systematic about what groups of chemicals lend themselves to grouping? Is there value in exploring what groupings are possible?
The principles related to how chemicals may be grouped are incorporated. It is important to note that groups important to one regulator will not necessarily be important to another one.
Combined exposure needs to be explicitly addressed, as it has been and continues to be an issue of interest to the public. Where information is lacking at present, it is important to identify gaps to the extent possible and perhaps chart some meaningful path forward from a drinking-water perspective, based on experience with the framework. Reasonable next steps for specific cases for which groups are considered priorities would be recommendations concerning acquisition of additional data.
Case-studies: General
Case examples are needed to illustrate various aspects of the framework. Should this document break new ground, with de novo case-studies? Or should it be conservative, drawing on existing case-studies? Examples that already exist are preferred, in the interest of time (and as agreed at the previous meeting). It was also pointed out that resources are not available to develop de novo case-studies.
The GDWQ already deal with some “mixtures” (e.g. nitrate/nitrite, trihalomethanes [THMs], atrazine/simazine, radionuclides).
Previously discussed suggestions included DBPs, nitrate/nitrite, VOCs, THMs and N-nitrosamines (e.g. NDMA), with a focus on exposure and hazard.
Case-studies: Pesticides
There is considerable Japanese experience in pesticide control. Some pesticides (e.g. carbamates, anticholinesterases) have similar modes of action, functional groups and methods of analysis. A pesticide case-study from Japan can be provided in a similar format to the case-study already included in this document.
The carbamates case-study included in the WHO/IPCS framework was based on a USEPA assessment and was very labour intensive. It went through all the tiers, although it might have been possible to set the compounds aside at an earlier tier in framework analysis.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
22
Case-studies: Disinfection by-products
Perhaps THMs and other DBPs can be briefly addressed in the report as an exploratory example to identify further work. Bette Meek would be happy to contribute to it. Perhaps some thought can be devoted to it as the document is revised.
It is not a simple task to identify existing studies and put them into the document in the correct format, which takes a lot of thought.
Considering how new DBPs can be grouped is a research project of significant size for which resources are unavailable. Even looking at existing chemicals would take resources away from other projects. This may be something for the future, but it is going beyond the scope of what this group was asked to do.
It would be an interesting case-study to look at the main DBPs that are regulated, THMs and halogenated acetic acids (HAAs), to see if there is a way to group them more scientifically. The conclusion may be that the selection of a guideline value of 100 µg/L for THMs is acceptable.
DBPs are an important group for drinking-water. It would be quite interesting to walk THMs (or HAAs), for which there are considerable toxicity and exposure data, through the process, as an exploratory case-study. It is not clear what the end result would be using this approach.
There are practical reasons to regulate HAAs as group, but they are different toxicologically.
THMs are grouped by common origin and analysis, not by mode of action. Depending on relevant legislation and guidance, a regulatory agency may have a hard time justifying regulating based on something other than mode of action.
THMs would probably require a higher-tier approach, involving mode of action. Other chemical groups can be set aside at an early stage. Early-tier assessment is usually used for setting things aside, not for regulation (otherwise, one would need to use higher tiers).
Case-studies: Pharmaceuticals
The case-study on pharmaceuticals (non-steroidal anti-inflammatory drugs [NSAIDs] and statins) in drinking-water in section 3 is a nice example, and the TTC approach for contaminants in drinking-water in Appendix 4 is an older example of an early-tier assessment. Suggestions for additional case-studies, volunteers to prepare them and timelines for their development in parallel with the document itself are needed.
The current case-study on pharmaceuticals is a good one (the outcome was not known until the pharmaceuticals were walked through the tiers), and pharmaceuticals are really relevant to drinking-water, so perhaps another case-study on the pharmaceutical group (maybe estrogens) should be added.
Other case-studies
Case-studies on 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and congeners and polychlorinated biphenyls (PCBs) have been done, but these chemicals are not that relevant to drinking-water.
One suggestion is total microcystins, as they are broadly distributed and a lot of data are available on them. The current WHO guideline is for microcystin-LR, which is the most toxic of the group. However, different microcystin congeners require different treatment. Andrew Humpage of Australia might agree to contribute to or write this case-study. Ingrid Chorus was also suggested as a potential author.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
23
Other suggestions include perchlorate and nitrate (thyroid effects) and perchlorate, chlorate and chlorite. There is insufficient information on these at present to develop a case-study.
Expected product(s): Report with case-studies (by end of 2014) Next steps:
Mari Asami will prepare a 3- to 5-page case-study on pesticides, following the example already included in the document, in the next month or so. Ruth Bevan, John Fawell or Bette Meek can provide guidance on how the case-study should be structured.
Ruth Bevan will address comments provided by the meeting, noting that the report cannot be completed without the case-studies, which will have implications for the conclusions of the document.
David Cunliffe will inquire about Andrew Humpage’s interest in contributing to a case-study on microcystins within 2 weeks and inform the group of the results. John Fawell is also familiar with microcystins and could collaborate with Andrew.
John Fawell and Ruth Bevan will select another pharmaceutical example for a case-study.
The time frame for delivery of the case-studies is within the next 6 weeks, so that the document can be finalized by the end of the year.
Any comments on the document should be compiled and sent to Sophie Boisson within the next 2 weeks.
7.3 Chemical aspects
The objective of this session was to get an update on some of the documents that are in progress, discuss outstanding issues and get a brief update on those documents that are in the early stages. #32a. Alternative disinfectants: Iodine Background: Iodine was added to the rolling revision as part of the agenda item on alternative disinfectants, as it is increasingly being used as a disinfectant. It was identified as a high-priority item at the Dübendorf meeting. WHO commissioned Cranfield University to review the toxicity and efficacy data on iodine. Ruth Bevan prepared a briefing note on the use of iodine as a drinking-water disinfectant, focusing on the efficacy and toxicity data.
Progress since previous meeting:
A background document was drafted, incorporating comments on the briefing note presented at the Geneva meeting, based on the same model as the silver document prepared by Lorna Fewtrell.
Presentation (Ruth Bevan):
The document has progressed considerably since the briefing note presented at the last meeting. Its aim is to evaluate the evidence to provide guidance concerning the use of iodine as a disinfectant for drinking-water, taking into account efficacy, toxicology and environmental considerations.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
24
Different iodine species affect microbial groups to different extents.
Iodine can be used to disinfect swimming pools; it is also used in the International Space Station.
The advantages of iodine over chlorine are that it works better for water of poor quality (i.e. more contaminated), it has a more acceptable odour or taste, there is less disinfectant demand and it has greater chemical stability.
The disadvantages of iodine compared with chlorine are that some people are sensitive to iodine, iodine is not safe for pregnant women or people with thyroid disease, the safety of the long-term consumption of iodine has not yet been established, and a higher concentration is required for disinfection.
Iodine is a vital micronutrient, being an essential component of the thyroid hormones thyroxine and triiodothyronine.
Diet is the sole source of iodine for humans (from water and soil). Coastal regions are richer in iodine content compared with inland areas.
Iodine deficiency disorder is the most common endocrinopathy in the world.
Iodine deficiency has multiple adverse effects on growth and development, including goitre, neurodevelopmental deficits in infants and increased risk of thyroid cancer (follicular form).
Iodine excess also results in goitre and is a risk factor for thyroid papillary cancer; there are also acute poisoning symptoms associated with excess iodine intake.
The acceptable intake of iodine in an emergency needs to be discussed.
There is no WHO guideline value for iodine, as available date for iodine are insufficient, and it is considered inappropriate to use data for iodide as the basis for a guideline value for iodine. The European Food Safety Authority (EFSA) published adequate intake levels in 2014, and a tolerable upper intake limit was established by the European Commission’s Scientific Committee on Food (the forerunner of EFSA).
Summary of discussion: Safety versus essentiality
There needs to be a balance point between the two parts of WHO concerned with iodine: one wants to increase iodine consumption in deficient parts of the world, and the other wants to use it only for emergency applications to avoid thyroid problems. Perhaps this group was too conservative in discounting iodine use for long-term exposures.
Other organizations have established tolerable intakes for iodine (including the Institute of Medicine in the USA).
The United States army has used iodine for decades in the field. This group needs to be clear about whether such chronic use is toxicologically appropriate.
Some point-of-use devices have iodine in them and are being sold around the world for household water treatment. Some families are therefore using iodine in this form on a regular basis. There is also pressure to use iodine routinely in municipal supplies. This group needs to be careful in outlining the circumstances under which use of iodine may or may not be suitable.
Discussions are ongoing with the nutrition department of WHO on essential elements. This group is trying to explore this area more in its guidelines.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
25
If iodine is used in an area with high iodine intake, it would be very easy to exceed the upper tolerable intake. This is quite different from the chlorine situation.
There is anecdotal evidence about thyroid problems in developing countries where iodine was used.
A definitive conclusion on the use of iodine for disinfection is needed. A recommendation for the long-term use of iodine, such as “the upper water concentration should not be higher than X mg/L”, would be a major step forward.
The group’s recommendations for the use of iodine need to be contextualized. There are still many questions, and the group should be cautious about recommending it for long-term use. The draft report needs to expand on this.
Iodine is the only alternative disinfectant where there are potential benefits under certain circumstances; can this group go beyond the current recommendation? The GDWQ state that the use of iodine is acceptable in case of emergency, but iodine is not recommended for long-term use; this needs to be reconciled with the need for iodine in deficient regions.
Can this group take a step forward regarding the appropriate conditions of use of iodine and the circumstances where it may be beneficial beyond disinfection? Or are these higher-level decisions and beyond what this group can accomplish at this table?
Efficacy
A lot more information than is currently included in the document is available on the use of iodine as a disinfectant against viruses and Cryptosporidium. This information needs to be added to the document. Although the GDWQ state that iodine is ineffective against Cryptosporidium, recent information suggests that this has changed.
The effective dose levels given in the report should be checked, as some of them seem to be too high.
Disinfection by-products
The reaction of iodine with organic substrates can result in the formation of highly toxic DBPs. This should be discussed in the report.
There is currently not much information on iodine DBPs. However, if iodine were to be approved widely for use as a disinfectant in municipal supplies, a lot of research on its by-products and their toxicity would likely be initiated.
Some DBPs are being detected and found to be biologically active. Iodoform has been tested and is not carcinogenic. Maybe the DBPs just become part of the iodine pool.
Content
Monitoring methodology, storage and other practical issues need to be considered in the report.
The Grading of Recommendation Assessment, Development and Evaluation (GRADE) approach needs to be included in the iodine document (as Lorna Fewtrell did in the silver document).
Prior compilations of information (e.g. an older USEPA document) can be referred to for background information.
Expected product(s): New background document and fact sheet on iodine as a disinfectant (first or second addendum)

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
26
Next steps (Chemical and Microbial WGs):
The deadline to submit comments and supporting references is 1 July 2014. These should be sent to Ruth Bevan and Sophie Boisson. The supporting references include the efficacy papers referred to in the above discussion and references to support all requests for the addition of information to this report (e.g. iodine use in the United States military).
Ruth Bevan will revise the background document on iodine and submit it to Jennifer De France, who will send it out to the Chemical and Microbial WGs for review.
A shorter fact sheet will be prepared from the final background document (based on the sodium diisocyanurate model presented at the Geneva meeting).
#32b. Alternative disinfectants: Bromine Background: Bromine was added to the rolling revision as part of the agenda item on alternative disinfectants, as it is increasingly being used as a disinfectant. It was identified as a high-priority item at the Dübendorf meeting. WHO commissioned Cranfield University to review the toxicity and efficacy data on bromine. Ruth Bevan prepared a briefing note on the use of bromine as a drinking-water disinfectant, focusing on the efficacy and toxicity data.
Progress since previous meeting:
A background document was drafted, incorporating comments on the briefing note presented at the Geneva meeting, based on the same model as the silver document prepared by Lorna Fewtrell.
Presentation (Ruth Bevan):
The document is not as extensive as the one for iodine, as information on bromine is not as readily available. Its aim is to evaluate the evidence to provide guidance concerning the use of bromine as a disinfectant for drinking-water, taking into account efficacy, toxicology and environmental considerations.
Bromine is primarily used as an alternative disinfectant for swimming pools, spas and cooling towers; it is also used as a potable water disinfectant in non-residential settings (e.g. cruise ships).
Bromine is a weaker disinfectant than chlorine in high-quality water, but is more efficient for inactivating coliphages in highly contaminated water.
Bromine has potential use for disaster relief scenarios.
Bromine is greatly understudied, and there are large knowledge gaps.
Bromine is not consistently shown to be essential in humans.
Exposure to bromine occurs occupationally or through the consumption of contaminated seafood or crops, where it is used as a soil disinfectant or fumigant.
There is no formal WHO guideline value for bromine, as available data are insufficient.
There are occupational limits for the inhalation of bromine. In addition, the USEPA has a food additive tolerance maximum of 1 part per million, and the United Kingdom has a TDI of 1 mg/kg body weight per day, based on the Joint FAO/WHO Meeting on Pesticide Residues (JMPR) acceptable daily intake (ADI).
Acute exposure to bromine via inhalation produces irritation symptoms.
Ingestion of bromine can lead to haemorrhagic nephritis.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
27
There are no human data on repeated exposure by any route. Oral toxicity studies are limited, showing some blood effects, salivation, increased urinary volume with urinary protein and decreased activity in rats.
There is no evidence of carcinogenicity. Liquid bromine is mutagenic in the Ames test.
There are no data on reproductive/developmental effects in animals. Summary of discussion: Uses
Bromine is used widely in swimming pools. It is marketed as a replacement for chlorine, as there are no asthma problems for lifeguards (which result from exposure to nitrogen trichloride when chlorine is used).
Bromine is used for water fountains, indoor swimming pools and cooling towers. After the bromine is added, the water is chlorinated to convert the bromine back to hypobromous acid, which is a very effective disinfectant.
It is important to think about existing applications of bromine. Bromodichlorodimethyl-hydantoin, which can be used as a source of bromine in water, is now incorporated into household water treatment products on the market in India, for example.
Chemistry and efficacy
Bromine reacts extremely quickly with ammonium to form bromamine, so there is concern about the persistence of bromine residual in water containing ammonium.
The efficacy of bromine in poor quality waters, including those containing ammonium, at both high and low pH levels has been observed. Bromine is quite efficacious as a disinfectant, even though the chemistry might predict otherwise. Whatever species are present appear to be microbiocidal.
In ocean desalination plants using combined chlorine, bromamine degrades to bromide in hours, so bromamine is not the disinfectant.
The fact that chlorine is not efficacious in the presence of ammonium, but bromine is, can be easily explained chemically.
Disinfection by-products
The hypobromite formed reacts with organics, so the main issue is with brominated DBPs.
In some specially designed systems, bromine does not produce DBPs.
In a point-of-use device that suppresses DBP formation, bromine could be used as a drinking-water disinfectant.
If bromine were to be introduced more widely, there would be an increase in research on its DBPs and their toxicity.
It might be useful to produce a summary of the strengths and weaknesses (and unknowns, e.g. DBPs) of the various disinfectants.
Other issues
On the basis of the available data, bromine would not be recommended for use in drinking-water supplies. In some areas, its use in point-of-use devices might be appropriate.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
28
Practical handling of bromine is a problem. It is usually combined with an organic carrier. Isocyanurate can be used in combination with bromine. Such a system would probably be better for use when organic matter or ammonium is present, as it provides a longer-term release of bromine. How useful it is in widespread use remains to be determined.
The GRADE approach needs to be included in the bromine document (as Lorna Fewtrell did for the silver document).
Expected product(s): New background document and fact sheet on bromine as a disinfectant (first or second addendum) Next steps (Chemical and Microbial WGs):
The literature review done by Mark Sobsey’s graduate student will soon be publicly available (in his thesis), and Mark Sobsey will send the relevant parts or the whole thesis to Ruth Bevan and Sophie Boisson. The thesis contains information on the effect of bromine on Cryptosporidium.
Any specific comments and supporting references are to be sent to Ruth Bevan and Sophie Boisson within the next 2 weeks.
Ruth Bevan will revise the background document on bromine and submit it to Jennifer De France, who will send it out to the Chemical and Microbial WGs for review.
A shorter fact sheet will be prepared from the final background document (based on the sodium diisocyanurate model presented at the Geneva meeting).
#30. Alternative disinfectants: Silver Background: Silver was added to the rolling revision as part of the agenda item on alternative disinfectants, as it is increasingly being used as a disinfectant. Lorna Fewtrell prepared a background document on the efficacy and toxicity of silver-containing compounds for review at the Dübendorf meeting. The database on silver is limited, and it was suggested that Lorna Fewtrell may need to speak to researchers involved in this area to obtain unpublished information. Additions to the background document suggested at that meeting included other types/treatments involving silver (colloidal silver, nanosilver, silver coatings) and toxicity outside of water. Progress since previous meeting:
The draft background document was revised based on feedback from the Chemical and Microbial WGs at the December meeting. A fact sheet was also prepared (modelled on the fact sheet on sodium dichloroisocyanurate) and circulated for feedback among the group.
Presentation (John Fawell):
The efficacy of ionic silver and nanosilver is somewhat uncertain, but they do not appear to be particularly efficacious, particularly against viruses and Cryptosporidium. They may be more bacteriostatic than bacteriocidal.
Ionic silver is widely used in point-of-use devices and in jug filters, and nanosilver is increasingly being used in consumer products.
Toxicity data on silver are quite limited. Silver combines with sulfhydryl groups. Argyria is considered to be a cosmetic effect. Silver can cross the placental and blood–brain barriers

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
29
and can accumulate in the body, but it is not known if this results in long-term adverse health effects.
In conclusion, silver may be useful in some circumstances, particularly in combination with copper, but its efficacy is limited; it probably has acceptable toxicity, but there are some data gaps.
Summary of discussion: Efficacy and use
Silver/copper combinations are efficacious, but not as drinking-water disinfectants, because they are very slow, taking several hours to work. However, they are very good for use in plumbing systems against bacteria. They are more than a bacteriostat, but they kill organisms slowly.
The USEPA has registered copper/silver as a disinfectant system. Its efficacy in solution is clear in laboratory studies, but there is debate as to what happens in biofilms, which is where the organisms are growing. Nevertheless, hospitals use this combination worldwide, and it seems to work.
If water is being stored, perhaps rapid inactivation is not necessary. The disinfectant can be applied one day, and the water can be used the next day. This is similar to the situation with monochloramine; slowness is accepted in municipal systems.
Silver use on ceramic filters is being widely promoted as a low-cost technology. However, it is unknown whether the silver is contributing to efficacy or just the filtration itself. Studies are ongoing, and new evidence may continue to emerge.
There have been some successes and some failures with copper/silver in hospital systems. This probably has to do with its water chemistry. Advice was issued in Australia against the use of copper/silver in spas and swimming pools because of efficacy concerns and a tragic outcome.
Silver takes a long time to act if used alone and is not so effective. Chlorine and silver in combination are very effective and are useful in hospitals, especially in high-risk wards.
There is no discussion on protozoa in the document, and it should be included.
There is a whole series of new studies by Jim Smith on Cryptosporidium. An attempt should be made to introduce these recent Cryptosporidium studies to the document.
In studies in Singapore, a toxicological assessment was carried out on low levels of nanosilver in water. There was some sort of toxicological effect under high, unrealistic concentrations. The differences compared with normal silver were not very significant, but the efficacies were different.
Silver is used as a bacteriostat to protect against the growth of bacteria within filters. This is a different use from disinfection of drinking-water, and the report needs to be clear about the difference.
The overall feeling is that silver is efficacious for some uses, but not drinking-water; there are questions about its use, even in swimming pools. There are insufficient data to support its use in municipal supplies, but there is some support for its use in point-of-use devices for household water treatment.
Silver is being considered in Europe for approval as a biocide, so maybe some manufacturers will be generating necessary data, but the new information should not have an impact on the bottom line.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
30
Commercial interests are at stake, so any recommendations need to be supported by the best available scientific evidence and carefully worded.
General comments
The current draft is much improved from the previous version. From a regulatory point of view, this report is a step in the right direction.
The document seems to be promoting the use of silver-coated ceramic filters without a complete toxicological and efficacy database.
WHO has a scheme to evaluate household water treatment, which is testing filters on pathogens. There is also a parallel evaluation scheme looking at the efficacy of disinfection. The recommendation from this group on silver has to feed across to the WHO household water treatment evaluation scheme.
The background document and fact sheet have been circulated for comments, and comments have been received and incorporated, so the background document and fact sheet are nearly ready for editing and publication. Lorna Fewtrell is not expecting any major changes; only some minor wordsmithing on the conclusions is necessary.
Expected product(s): New background document and fact sheet on silver as an alternative disinfectant (first addendum) Next steps (Chemical and Microbial WGs):
Any editorial comments should be submitted to Sophie Boisson within 2 weeks.
Minor revisions to the fact sheet and background document will be made (by Lorna Fewtrell/Sophie Boisson/John Fawell), after which Sophie Boisson will circulate the final versions to members.
The documents will be edited, for publication in the first addendum. 7.4 Cross-cutting issues
#36. Translating the Guidelines into national standards Background: At the Dübendorf meeting, WHO regional offices emphasized their need for guidance on using the Guidelines to establish national standards, in particular advice on selecting priority parameters. John Fawell and David Cunliffe were to continue to work on the document on translating the Guidelines into national standards. As this document is developed, there will be a training exercise on how to develop national standards in a couple of countries or regions; feedback from this exercise can feed into finalization of the document. Progress since previous meeting:
The Chemical and Microbial WGs sent feedback (including answers to questions that had not yet been answered as well as suggested revisions to already existing responses). Phil Callan, David Cunliffe and John Fawell revised the document in light of comments received.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
31
Presentation (David Cunliffe):
The basic principles of this project, which was initiated at the Berlin meeting, are to explain the GDWQ and provide guidance so people do not just blindly accept all of the numbers without considering local circumstances.
A major change in the content is that it was converted into a series of 49 Qs&As, divided into sections. The content covers quite a broad range of topics.
The document has been circulated to participants for comments. Summary of discussion: Format
Should this document be formatted as part of the Guidelines? It is an important document that needs a high profile; it should not be just a brochure.
Although it was questioned whether the Q&A approach should be retained and suggested that the report needs a more professional format, it was noted that a complete change of format may delay publication of this important document and that there is some precedent for a less formal approach, which is what is needed here.
The document should be formatted so that it looks like the GDWQ. Perhaps a photo of the GDWQ book can be added on the cover.
The document is not yet written in the correct language for the target audience. The language can be kept less formal than in the GDWQ.
This should not be too long a document. It should be kept basic, with a couple of examples (like the arsenic box on p. 2). It should not try to cover everything.
The document needs to be translated into the six WHO languages. Content
Establishing national standards and regulatory requirements are two different things. The title of this document is on establishing regulations; guidance on standards is missing. This would provide useful information to regulators.
The title should be changed to establishing national standards, as regulations have other components (e.g. penalties and enforcement) that are not dealt with.
One of the objectives of this document is to encourage focus on a more reasonable number of locally relevant parameters. The WHO document on prioritizing chemical risks, published in 2008, was not the document to accomplish the task of minimizing the number of parameters to monitor, as it was not very accessible.
The most important thing is to provide guidance on how to minimize the number of chemicals to be monitored. The training pack from the second edition refers to priority chemicals (nitrate, fluoride, arsenic), which is very useful for developing countries. That type of information should be delivered in the document.
Guidance on regulations is also needed, as countries are asking for legal advice.
The document needs to clearly describe under what circumstances a guideline value can be exceeded.
Perhaps case-studies on experiences of countries with adaptation of the GDWQ for local circumstances would be useful.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
32
Enrique Calderon has written a paper on the limitations of the Guidelines; this will be incorporated into the revision of these Qs&As.
A couple of one-page elaborations are also needed on how to interpret the guidelines for arsenic and E. coli, for example, in terms of relative risk.
Can a water quality index be created based on the most important parameters, similar to the air quality index established by the WHO group that publishes the guidelines for air quality? Technically, a water quality index would be very difficult to create, as there is a lot of variation in exposure and types of contaminants, and could not be established in a short time frame. As this document needs to be published soon, this concept should not be dealt with now, but could be considered in the future.
Feedback
Input is needed from those using the Guidelines as well as those producing the Guidelines, so the document should be disseminated to users in several countries for feedback. Feedback from countries using the Guidelines could be received in 2 months. Users may come up with aspects that are not covered here.
The document can be distributed in draft form to RegNet members and to select water suppliers for comment.
It is important to get stakeholders’/practitioners’ views. The document should fulfil its purpose, as the need for the document came from the regional offices in the first place.
Expected product(s): Guidance on translating the GDWQ into national standards (time frame unknown) Next steps (Chemical and Microbial WGs):
Comments from this group should be sent to Phil Callan and Sophie Boisson by the end of June.
Phil Callan, David Cunliffe and John Fawell will revise the document in light of comments received during the meeting and within the month following the meeting.
The Secretariat will identify key stakeholders to whom to distribute the text and from whom to get feedback. They will be requested to look at the format and content of the document and determine whether the document suits their purposes or whether revised or additional questions are needed.
Phil Callan, David Cunliffe and John Fawell will revise the document following feedback from the regions and other key stakeholders. The document will then be sent to the Chemical and Microbial WGs for comment.
#34. Quality of the evidence Background: WHO guidelines must meet the highest-quality standards for evidence-based guidelines, be based on high-quality systematic reviews of all relevant evidence, use GRADE (Grading of Recommendation Assessment, Development and Evaluation) to assess the quality of the evidence and strength of the recommendations, incorporate multiple processes to minimize bias and optimize usability, and incorporate transparency in all judgements and decision-making. The GRADE approach examines five domains of quality to permit judgement of the overall quality of the body of evidence for each outcome. Recommendations are judgements based on the quality of the evidence as well as on trade-offs between benefits

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
33
and harms, values and preferences, and resource uses. The strength of a recommendation reflects the extent to which there is confidence that the desirable effects of a management strategy outweigh the undesirable effects. It is necessary for the drinking-water group to systematically review and update the evidence and recommendations in the existing Guidelines in accordance with GRC processes. Progress since previous meeting: An updated paper on quality of the evidence was prepared by Phil Callan and distributed to participants. Also, Lorna Fewtrell modified her proposed approaches for grading the evidence in the silver background document (see agenda item #30) based on input provided at the Geneva meeting. Discussion:
Phil Callan reminded people who are developing documents to evaluate the strength and quality of the evidence using the GRADE approach. This includes the iodine and bromine documents being prepared by Ruth Bevan (see agenda items #32a and #32b). They can follow the approach used by Lorna Fewtrell for the silver document (see agenda item #30).
There was insufficient time for further discussion on this agenda item. Expected product(s): Assessment of quality of the evidence incrementally added to key recommendations and background documents (time frame unknown) Next steps (Chemical and Microbial WGs):
Ruth Bevan is to grade the evidence in the iodine and bromine background documents.
The Secretariat will continue to consult with the GRC and will keep the group apprised of any developments in this area.
#37. PICO questions Background: To ensure that all of the intervention recommendations in the GDWQ are developed in accordance with the requirements of the WHO GRC, they must be justified following the PICO (population, intervention, comparator, outcomes) format. PICO questions are not being derived for policy recommendations, threshold levels or surveillance recommendations. The PICO questions will be used to guide the evidence synthesis. Progress since previous meeting: Phil Callan prepared an updated paper on PICO questions, which was distributed to participants. Summary of discussion:
There was insufficient time for discussion of this agenda item. Expected product(s): Key recommendations together with PICO questions for submission to the GRC by mid-2014 Next steps (Microbial WG):
This agenda item will be added to the agenda of the next meeting of the Microbial and Chemical WGs, for an update by Phil Callan.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
34
7.5 Microbial aspects
#58. Revised structure of Chapter 7 Background: One of the issues raised at the Dübendorf meeting was the disjointed flow of Chapter 7. The flow was retained from the third edition, dealing first with hazards, then performance targets, treatment to achieve the performance targets, and concentrations in water. It was agreed at the Geneva 2013 meeting (during a discussion on agenda item #43, below) that the structure of Chapter 7 should be discussed with the whole Microbial WG at the June 2014 meeting and, if there is a more logical order (e.g. introducing WSPs first, then source water protection, distribution integrity, etc.), it should be changed for the fifth edition. It was also suggested that it would be useful to get feedback on the chapter’s structure and content from people who actually use it.
Progress since previous meeting: A revised structure of Chapter 7 (based on comments at the Berlin meeting) was prepared for discussion. Presentation (Anna Maria de Roda Husman):
A transition to a source to tap paradigm is suggested (restructuring Chapter 7 along the lines of the hydrological cycle).
WSPs will be introduced first, then source water protection, treatment efficiency, distribution integrity, etc.
The aim is not to delete or add text, but simply to restructure it to make it more accessible and user friendly.
QMRA (see agenda item #51) should be introduced later in the chapter. As the QMRA document is currently being finalized, discussion is needed on what needs to be retained in Chapter 7 and what needs to be removed from the chapter.
A revised table of contents was distributed to participants and compared with the current table of contents.
Summary of discussion:
It was suggested that the revised structure should follow the risk analysis approach, with the chapter being divided into microbial risk assessment and microbial risk management and with health-based targets and hazard identification as subheadings under risk assessment. It was agreed that risk assessment and risk management should be more clearly articulated. Sections 7.3–7.6 may become subheadings under risk management. Section 7.4 on possible interventions could be changed to risk management options.
QMRA is included under the heading “Characterization of risk”. Perhaps the headings need to be amended to more clearly reflect the contents. The GDWQ should be linked to the QMRA document.
Under treatment, small systems should be included as well as central treatment and household treatment.
There needs to be harmony between the revised Chapter 7 and Chapter 8 on chemicals.
Turbidity, aggregating multiple steps and other developments will need to be incorporated within the new structure. The basic structure has been outlined, but the actual content will change in response to other issues.
Occurrence is no longer a separate section, but will be included in other sections.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
35
Regarding guidance on methodology, pathogen detection methodology was left out on purpose, but microbial risk assessment is being introduced. New methodologies for rapid detection are coming out all the time, and it would be good to give some guidance as to what the different types of methods are. This is not included yet, but it should be.
In the new structure, indicator organisms are introduced much earlier in the chapter, as the basis for the rest of the chapter.
Requests for guidance on water testing products have been received from the regions.
A decision-tree on microbial methods is being completed in the Netherlands, which focuses mostly on E. coli and thermotolerant coliforms, but addresses turbidity as well. It will be piloted in several countries.
Guidance on developing a good sampling programme is needed. The number of samples, the importance of choosing the correct sampling points (fit for purpose) as well as sampling frequency are all issues of concern. The new section 7.6, on verification monitoring, will need to deal with location and frequency of sampling. There is some text on this in Chapters 5 and 7, but it is not strong enough. Some basic information – key principles and issues – will be included here, with cross-reference to other documents, such as the WSP manual. Volume 3 also addresses sampling in terms of number of people served.
The Guidelines can be improved to help small water suppliers. For example, as water is not continuously being monitored for pathogens, chlorine dosing is critical. It has to be emphasized that if the chlorine pump is not working, the operator must get an alarm or notification on the telephone. Section 7.5 on operational monitoring would be a good place to include that sort of information (on turbidity, chlorine dosing), perhaps drawing some text from Chapter 4.
Monitoring of microbial-related indicators, including turbidity, pH, chlorine and redox potential, needs to be included. This is included in Chapter 4, but is not cross-referenced. It needs to be added to Chapter 7. Besides operational and verification monitoring, there may be other objectives for monitoring.
The way in which health-based target setting is addressed in Chapter 7 may need to be clarified.
Cross-referencing to other documents needs to be improved.
The revised structure is planned for the fifth edition, but additional work items (e.g. turbidity, microbial methods) are planned for the first and second addenda and can be published before the fifth edition.
Expected product(s): Revised Chapter 7 (fifth edition) Next steps (Microbial WG):
Ana Maria de Roda Husman and David Cunliffe will prepare a more detailed version of this structure for discussion by the Microbial WG at the next meeting. The revised structure will take into consideration feedback from participants at this meeting.
#44. Multiple-barrier approach Background: The importance of the multiple-barrier approach, in particular the problem of intermittent distribution in developing countries, was discussed at the Dübendorf meeting. It was decided to ensure that the “catchment to tap” paradigm is captured in Chapter 7. Text

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
36
needs to be added to Chapter 7 on catchment protection of surface water, catchment protection of groundwater, safe piped water distribution and storage, safe water in buildings and safe storage in household water systems, based on the supporting documents. Guidance on distribution systems was identified as a high priority. If text for Chapter 7 is needed, a workplan needs to be developed. Progress since previous meeting: The water safety in distribution systems text has been completed and is currently at the layout stage. Presentation (Ana Maria de Roda Husman):
Text needs to be added to Chapter 7 on the catchment to tap paradigm, including text based on the new guidance document on water safety in distribution systems.
A volunteer is needed to condense the water safety in distribution systems document into one or two paragraphs for Chapter 7.
Summary of discussion:
There is a contradiction between WSPs based on the hazard analysis and critical control point (HACCP) approach and the multiple-barrier approach. A critical control point implies that this is the last barrier. This contradiction needs to be explained.
This issue was raised at the Expert Consultation on Effective Approaches to Regulating Microbial Drinking-water Quality in Adelaide in 2001. A barrier can be a critical control point only if there is no barrier after it. Therefore, there can be only one critical control point. An expert on HACCP in food was brought in to address hazards in foods. He informed the group that there was more than one barrier and more than one critical control point in drinking-water control and that it was acceptable to vary this guidance.
Critical control point in HACCP terminology was not included in the GDWQ because of a slightly different conceptual application. At various points in the system, there are measures to inform whether each part of the system is in control. There is no intention to place one barrier above another one. If all parts are in control, all is well; if one part fails, this does not necessarily mean that there will be a problem.
This agenda item is more on intermittent distribution systems than on the multiple-barrier approach.
Expected product(s): Revised text for Chapter 7 (first addendum) Next steps (Microbial WG):
David Cunliffe, Ana Maria de Roda Husman and Lesley D’Anglada will produce some short text for Chapter 7 for publication in the first addendum.
#50. Reference pathogens Background: It was identified at the Dübendorf meeting that reference pathogens (index pathogens and indicators) used for performance targets differ from place to place. Issues included the need to add norovirus and helminths as reference pathogens in wastewater, the use of protozoa as the reference pathogen for helminths, norovirus and dose–response, and reference pathogens and risk for all groups. The way forward (as a medium priority for the second addendum) was identified as reviewing the data, including seasonality and potential

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
37
reference data such as DALYs and dose–response data, finding data on helminths, increasing the text on viruses and bacteria and providing examples. The QMRA guidebook was to be used as a reference for the discussion on the text review. Progress since previous meeting: The QMRA text is close to completion. Presentation (David Cunliffe):
At the Dübendorf meeting, reference pathogens were addressed in the context of wastewater. Issues included the need to add norovirus and helminths as reference pathogens in wastewater and the use of protozoa as the reference pathogen for helminths.
Norovirus is an issue for drinking-water. Rotavirus is the current reference pathogen used in the GDWQ, but questions have been raised about its suitability because of the rotavirus vaccine. Should this group consider other reference pathogens?
It was decided at the Geneva meeting to wait until completion of the QMRA text before progressing on this agenda item. The QMRA text does not make recommendations on what the reference pathogens should be, but it does suggest the characteristics of a reference pathogen, one of which is the availability of dose–response information for that pathogen.
The Australian group has looked at norovirus as a reference pathogen. It has calculated DALYs per case for norovirus and there are dose–response data, so norovirus has the necessary components to be used as a reference pathogen.
This group could wait to see if there will be any change in the QMRA document, but that document will probably not change significantly at this late stage. Alternatively, the data from Australia could be used.
Numerical examples have not been given in the current text. These could be added, for use in developing log reductions.
The group should consider whether the reference pathogens currently included in the GDWQ are the best examples. Is Campylobacter the best reference pathogen for bacteria? Should Cryptosporidium or Giardia be used for protozoa?
Summary of discussion:
The GDWQ state how to select reference pathogens and give examples. Do we have information suggesting that norovirus is more important than rotavirus? This is related to the QMRA document and the decisions made there.
Perhaps the text should be modified to mention the rotavirus vaccine as an issue and that dose–responses are available for a variety of these pathogens, with a cross-reference to the QMRA text.
It is important to make some modifications to the text. There has been pushback on rotavirus as a reference pathogen by physicians, given its low disease burden, the availability of a rotavirus vaccine and the widespread contribution of norovirus to diarrhoeal disease burden, suggesting that it may be a more appropriate choice. So norovirus should be identified as a candidate based on the criteria for reference pathogens. Alternatively, a graph with dose–response curves for 8–10 pathogens could be added. People could consider pathogen contributions in their part of the world and make their choices of reference pathogens accordingly. It is not clear whether that

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
38
provides a better service or a disservice, as it moves the decision-making burden to the user.
Another flaw with rotavirus is that two curves, one for low-income countries and the other for high-income countries, have been given, and it was a fairly arbitrary decision to use the curve for high-income countries. With norovirus, that factor is not applicable.
DALYs per case need another look. For rotavirus, it is based on all disease being in 0- to 6-year-olds. For norovirus, DALYs per case for norovirus is quite low, as when mortality occurs, it is mostly in the elderly, so the years of life lost are fewer.
This has moved a long way from providing standards. The default position has to be clear. The group should err on the side of clarity and prescription. Dose–response curves could also be provided.
The group is trying to bring this information to the least informed user, which is why the graphs were put in the document in the first place. Defaults should be provided, but also simple information so people can find the risk associated with a particular dose. Providing information in a simplified form makes it more accessible to users. Graphs should be used as examples as part of the presentation of the material.
Perhaps a table should be used instead of a graph (e.g. a modification of Table 4.7 from the QMRA text). Then four reference pathogens could be chosen from the table and detailed calculations done only for those four chosen ones.
The current text refers to dose–response curves for several organisms. The relationship between this text and the QMRA text is important. How to select reference pathogens needs to be explained, with examples of what can be done.
The Global Enteric Multicenter Study (GEMS) is a rich source of data on enteric pathogens collected in the same way.
Reference pathogens are needed for each of bacteria, viruses and protozoa.
This issue was identified at the Dübendorf meeting as being of medium priority, for the second addendum.
It was also agreed at the Dübendorf meeting to move a lot of technical material into appendices, yet this discussion seems to suggest that the main body of the GDWQ should become more and more technical.
It is important to keep the contribution of the QMRA document to this document in mind (see agenda item #51).
Expected product(s): Revised text in Chapter 7 (second addendum) Next steps (Microbial WG):
David Cunliffe will prepare an outline on reference pathogens for consideration at the next meeting, with contributions from Mark Sobsey, Ana Maria de Roda Husman and Stephanie McFadyen from Health Canada.
#41. Microbial fact sheets and pathogenic and non-pathogenic strains: Tables 7.1 and 7.2 Background: Tables 7.1 and 7.2 list a range of pathogens, only some of which include the type and subtype. These and other inconsistencies need to be corrected, the organisms included in the tables need to be reviewed to determine if they should be retained and suggestions for new organisms to be included need to be considered. The information in the tables needs to correspond to the information given in the fact sheets in Chapter 11. The existing fact sheets

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
39
need to be reviewed and referenced. A prioritized workplan for revising the fact sheets needs to be established, and focal points need to be assigned. Progress since previous meeting: A short document on proposed revisions to Tables 7.1 and 7.2 and suggestions for inclusions and revisions of fact sheets was prepared, for discussion. Presentation (David Cunliffe):
The background document was provided to participants. Included was a comparison of the organisms in the tables with the organisms for which fact sheets have been prepared.
Decisions need to be made regarding which organisms should be included in the tables, which organisms require fact sheets and whether additional organisms are needed.
All fact sheets require reviewing. The priorities for updating fact sheets (most of which were originally prepared in 2001) need to be determined.
There is inconsistent uses of species names. Options for resolving this are offered, including the addition of a “Type species” column.
Summary of discussion: Inclusion/exclusion of pathogens
There should be a focus on organisms for which there is strong evidence of their transmission through drinking-water. Leptospira, for example, is not found in drinking-water.
There is a fact sheet on Bacillus, and it is not clear why, as it is not included in either Table 7.1 or Table 7.2.
Organisms should not be left out just because they are rarely found in drinking-water; it is context specific. Rather, the presentation should be organized so that it is understood that such differences in the prevalence of organisms in drinking-water exist.
Having fact sheets for all pathogenic organisms with potential for transmission through drinking-water is useful. This is one of the few compilations of such data in the world from an authoritative source.
Should Pseudomonas be included as an indicator organism in section 11.6?
It might be useful to identify core organisms and not confuse people with a long list of organisms.
The title of the tables could be changed, or the tables could be divided into more important and less important organisms, or the decision could be made not to include any fact sheets for those organisms in Table 7.2.
There should be fact sheets for organisms in each of the tables, but they could be separated, and the significance for drinking-water could be highlighted up front instead of being buried within the fact sheet.
The tables include water-associated pathogens, not strictly waterborne pathogens. There are opportunities for contact and exposure via routes other than the ingestion route. Even though these routes may be minor, there is not zero risk.
Content and format
References for each organism are included in the fact sheets. Newer references are needed, as the older ones will not be up to date on taxonomy and nomenclature.
WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
40
One participant noted a preference for a non-alphabetical approach, in which organisms are ordered according to their importance. However, it was pointed out that the organisms are listed alphabetically because they are easier to find when users look up the organisms that are most important in their own systems.
The titles of the tables refer to transmission of pathogens through drinking-water. Does this refer to drinking-water that is in compliance with all drinking-water standards or just source water that is to be used for consumption?
The type species column is a good addition to the tables.
It is clear that some organisms should always be considered pathogenic (e.g. Cryptosporidium hominis, norovirus, etc.); others may be opportunistic pathogens. Perhaps those distinctions should be addressed so that they are understood by the user community.
Miscellaneous
A plant in Argentina was closed when Pseudomonas aeruginosa was detected in one sample. This was a political decision, made without a good understanding of the significance of this detection.
This is part of the health risk–based approach to managing drinking-water. Operators can push back when approached by a misinformed person under the new paradigm, because there is a rational basis to do so. That is how this problem should be solved, not by deleting organisms from these two tables.
Perhaps the geographical distribution of pathogens should be considered post–fifth edition. The distribution of pathogens is changing, especially as a result of climate change, and it is no longer possible to predict where pathogens will be found.
Fact sheets were prepared on about 20 pathogens, including most or all of the pathogens in these tables, by the USEPA for the Contaminant Candidate List. These can be provided to this group to be used as a basis for revising the fact sheets.
Organisms included in the tables need a fact sheet. The priority for revising the fact sheets should be on pathogens first, indicators second and any others last.
Volunteers are needed to revise the fact sheets. The pathogens could be divided up by type (bacteria, viruses, etc.).
Expected product(s): Revised Tables 7.1 and 7.2 (including possibly a revised heading for the level of evidence) (first addendum); revised microbial fact sheets for Chapter 11 (second addendum or fifth edition) Next steps (Microbial WG):
Ana Maria de Roda Husman and David Cunliffe will add type species columns to Tables 7.1 and 7.2 and correct an error in one of the headings of Table 7.2.
With respect to revising the fact sheets, the Secretariat will investigate the possibility of drawing from the pool of people who have volunteered to contribute to GDWQ-related activities and ask if they would be interested in contributing to the revisions of the fact sheets.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
41
#46. Turbidity Background: The text in the GDWQ on turbidity needs to be revised, as the guidelines are being misused or misinterpreted, with different nephelometric turbidity unit (NTU) values being given for public acceptability, disinfection and measurement of filtration effectiveness. There is a need to expand advice on turbidity, breaking it down into its various components (use as a surrogate for performance measurement in operational monitoring, acceptability, disinfection) in both Chapter 7 and Chapter 10 of the GDWQ. The usefulness of turbidity as an indicator of water quality needs to be emphasized. The development of a fact sheet on turbidity should be considered. This was identified as a high priority at the Dübendorf meeting. A workplan for the development of this text needs to be decided upon. Progress since previous meeting: A background document summarizing guidance on turbidity from Canada, Australia and the USA and proposing content of material to be included in Chapter 7 and a supporting fact sheet on turbidity was prepared, for discussion at the current meeting. Presentation (David Cunliffe):
Turbidity documents from the Australian National Health and Medical Research Council and Health Canada were provided to participants, as well as a summary of the guidance from Canada, Australia and the USEPA Long Term 2 Enhanced Surface Water Treatment Rule (LT2). The LT2 includes detailed guidance on the relationship between turbidity and removal of Cryptosporidium by filtration processes.
Text on turbidity was increased in the fourth edition, but it was recognized even at that time that it was insufficient. Most of the guidance on turbidity is located in Chapter 10 on acceptability, with a little bit of guidance also in Chapter 7. There has been a lot of feedback on the need for additional guidance, particularly to clear up the confusion regarding the interpretation of the NTU values provided.
Turbidity is important for three reasons: 1) as a measure of acceptability; 2) for its influence on processes such as disinfection (<1 NTU for disinfection, ideally); and 3) as a measure of the effectiveness of filtration (different NTU values depending on the type of filtration used) to ensure that removal of both Cryptosporidium and viruses is achieved.
Text is needed for section 7.3, text needs to be moved from Chapter 10, and more clarity is required.
The relatively new Australian and Canadian guidelines both deal with impacts on disinfection, filtration and acceptability. The Canadian guidelines are more detailed and raise several additional issues, including the increase in turbidity as a result of water main breaks; turbidity and chemical quality; impacts of turbidity on microbial testing; and the relationship between turbidity and illness. The USEPA also has guidance on turbidity and filtration. Information is available from these guideline documents on sources of turbidity, measurement, turbidity as an indicator of water quality (corrosion, intrusion, biofilm release), filtration performance (by type of filtration), impacts on disinfection (chlorine, ultraviolet, ozone, etc.) and impacts of turbidity on aesthetic quality. The amount of text in the guidance and the form that guidance should take (i.e. a fact sheet or background document in addition to revisions to the GDWQ) need to be decided.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
42
Summary of discussion:
This task was identified as a first addendum priority at the Geneva meeting, as the topic has not been given the level of attention it deserves in the past.
There is a lot of confusion around the world with respect to the importance of turbidity and interpretation of the NTU values. If a turbidity fact sheet is produced, it would be beneficial to have it published in the first addendum.
There is a need to talk about small supplies, which will struggle to measure turbidity. This is a similar situation to aluminium, where there are different guidelines for small and large supplies. The message should be that turbidity should not be ignored just because it cannot be measured. There is a statement to this effect already included in Chapter 10.
In Japan, it is very important to pay attention to source water turbidity in small water supplies. There should be more emphasis on monitoring turbidity in raw water.
The document should not address only organized supplies. It needs to be made clear how turbidity is going to be addressed for point-of-use household water treatment and very small supplies. Settling or informal coagulation (e.g. stirring chunks of alum in water) is standard practice for many people around the world, so it needs to be addressed in some form or other. Very small systems do not have resources for expensive turbidimeters. The Jackson candle turbidimeter, an old technology, measures down to 4 NTU and could be used in these circumstances. These techniques need to be mentioned, as well as any others that could be used in low-resource settings. This would encourage manufacturers to think about ways to measure turbidity other than with a tube (e.g. use of very sophisticated optical capacity of smartphones).
Volume 3 of the GDWQ is being updated in parallel to address challenges faced by small systems.
There should be different guidelines for large and small supplies. Large supplies should not consider 5 NTU as being perfectly adequate, as they can achieve lower turbidities than this. Elevations in turbidity can have a huge impact in large systems (e.g. incident in New York City).
Another issue is the statement that, ideally, for effective disinfection, turbidity should be kept below 1 NTU. In Australian work on the disinfection of viruses, data have shown that disinfection still occurs at 20 NTU, but the disinfectant concentration × contact time (CT) value goes up. It is therefore too negative to state that, ideally, turbidity should be <1 NTU. Rather, it should be indicated that disinfection will work at higher turbidities, but longer contact times and possibly higher doses of disinfectant may be needed. The GDWQ should not discourage people from disinfecting at higher turbidities. Rather, people should try to keep turbidity down and consider adding more chlorine to satisfy demand if turbidity increases. This concept needs to be addressed in the GDWQ.
It was suggested that Moringa seeds, which are used in point-of-use household water treatment, should be noted in the GDWQ. Enquiries about the safety of the use of these seeds are expected, as the academic community is concerned about the potential toxicity of Moringa seeds. Other plant polysaccharides (e.g. cacti) are also being used in point-of-use household water treatment.
There is a big international push to promote point-of-use household water chlorination. However, there are big debates about the wisdom of chlorinating highly turbid water when it is not known how to choose and control the dose to achieve disinfection. This needs to be captured in the GDWQ.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
43
Turbidity is an essential indicator for evaluating disinfection processes (not just in terms of its impact on disinfection efficiency), as well as filtration and aesthetic quality. The GDWQ guidance should place more emphasis on this concept.
Why is the focus just on filtration? Why is turbidity not considered an indicator of the effectiveness of all treatment processes (coagulation, sedimentation, flocculation, etc.)? It was noted that the GDWQ is not a technical manual giving detailed instructions on how to treat drinking-water.
Table 1 in the Health Canada turbidity document addresses some of the concerns being raised above, and perhaps a similar table should be included in the turbidity fact sheet (under sources of turbidity).
Table 1 in the Health Canada document suggests that the types of particles that are making up turbidity are known. Most people will not know the source of the turbidity. Most large utilities just look at total turbidity, not at the source. However, there is value in making sure that people are aware of the different types of turbidity, which have impacts on understanding the source. This might help to manage water and to understand the impacts of turbidity on treatment and other aspects of the WSP.
Two other agenda items are related to turbidity: the update of the treatment tables (see agenda item #39) and aggregating multiple steps (see agenda item #43), which has some text on turbidity.
A decision-tree is being developed for microbial methods, with a minimum set of parameters that are important, including E. coli or thermotolerant coliforms, but also pH, turbidity and chlorine residuals. When Chapter 7 is restructured, a place will be found for this decision-tree.
The text in the GDWQ should be as short and concise as possible, with a link to supplementary information. This group should focus on three to five main points for the GDWQ. There are some very important points that need to be addressed, especially clearing up misinterpretations in the GDWQ. The discussion on turbidity needs to be included in different places in the GDWQ.
This group needs to make generally available a short fact sheet (2–5 pages) that is easy to translate. WHO is asking for simple, accessible, two-page fact sheets in the style used for diseases. This format was already used for water for travellers, so if turbidity lends itself to this format, it should be done. The two-page fact sheet could be based on the Health Canada and Australian documents. From that document, text could be extracted to go into the GDWQ.
There could also be a longer background document that includes all the detailed information, or existing documents could be referred to. As the water treatment book by Mark LeChevallier is going to be updated, this group should request that the subject of turbidity be addressed in that document. This would avoid the need for a separate document.
Volunteers are needed to write the text. One source of volunteers that could be utilized is the Water, Sanitation, Health & Hygiene Programme’s (WSH) large roster of experts, characterized by their technical expertise.
Summary of off-topic discussion on household water treatment evaluation:
WHO has published new burden of disease update brochures in the journal Tropical Medicine & International Health and will publish a concise consolidation of these brochures (which this group should be given the opportunity to review). With respect to

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
44
household chlorination, strong evidence from the new burden of disease study suggests that the epidemiological benefits of household chlorination are low, perhaps due to chlorine’s slow efficacy against Cryptosporidium.
As part of WHO’s household water treatment evaluation scheme, laboratories are testing the microbiological performance of household water treatment devices across three pathogen classes. So far, all testing has been done by collaborating centres of WHO: one laboratory in the USA and one in the Netherlands. PUB, which is also a collaborating centre, may want to do some of this testing in the future.
In implementation of the new approach to evaluating household water treatment technologies, the evaluation protocol (essentially NSF International/USEPA performance requirements, with slightly different numbers) requires that evaluations be carried out in laboratories that have the capability to measure viruses, bacteria and Cryptosporidium. As a result, only a handful of laboratories are able to implement this protocol. More consideration should be given to evaluating point-of-use devices in a more inclusive fashion. The ultimate aim is to develop the capacities of laboratories around the world and transition away from a centralized process. In future, it is hoped to have at least one testing laboratory in Africa and in Asia.
This group should keep aligned with the advisory committee on the evaluation of household water treatment options. This topic should be added to the agenda of the next meeting, once people have had a chance to become familiar with the background information.
The 2011 document “Evaluating household water treatment options: health-based targets and microbiological performance specifications” (Mark Sobsey and Joe Brown) is based on the log reduction tables in the GDWQ and outlines three performance levels: highly protective, protective and interim. This is similar to the USEPA approach.
The “Evaluating household water treatment options” document contains an excellent flow chart on establishing health-based household water treatment performance targets. When this group later discusses QMRA (see agenda item #51), this flow chart should be shown to illustrate how simple QMRA can be.
Expected product(s): Revised text in Chapters 7 and 10 (first addendum); fact sheet on turbidity (first addendum) Next steps (Microbial WG):
David Cunliffe will coordinate the work on the fact sheet. Mark Sobsey will approach someone in Jamie Bartram’s Water Institute programme at the University of North Carolina, John Fawell will look for someone from Cranfield University and Lesley D’Anglada will look for someone from the USEPA to help on this project. Enrique Calderon is interested in contributing. John Fawell and Michèle Giddings will act as reviewers. If more volunteers are needed, the Secretariat will investigate the pool of people with relevant expertise who have volunteered as participants in GDWQ-related activities.
Volunteers will report back to Sophie Boisson on prospective candidates within 30 days.
Phil Callan and the rest of the Secretariat will be involved in translating the fact sheet to the GDWQ.
The draft text needs to be completed within 1 year so there is time for review before including the revised text in the first addendum.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
45
The Secretariat will request that the subject of turbidity be addressed in the updated water treatment book by Mark LeChevallier.
The Secretariat will add the evaluation of household water treatment options to the agenda of the next meeting. In the meantime, the Secretariat will organize a teleconference for interested people, in which it will give a presentation and get strategic input from participants. Interested participants include Mark Sobsey, David Cunliffe, Enrique Calderon, Shane Snyder and Michèle Giddings.
#43. Aggregating multiple steps for overall water treatment performance Background: At the Dübendorf meeting, there was a detailed discussion on the issue of the validity of aggregating the effects of multiple steps on overall water treatment performance with respect to microbial reduction. Han Heijnen’s studies from Kiwa Water Research (KWR) showed that the efficacy from multiple steps was lower than the efficacy from each of the processes individually. On the other hand, studies in Australia have found multiple steps to be more effective than each individual step. It was agreed to review examples and papers from KWR to evaluate the advantages and disadvantages (high priority) and to add text to or edit Chapter 7, section 7.3.2, on the integration between unit processes and the need to incorporate moments of poor performance when aggregating the efficacy of unit processes to overall treatment efficacy (medium priority). The need for a literature review should be confirmed and a workplan developed. Progress since previous meeting: None Presentation (Ana Maria de Roda Husman):
The issue is the validity of aggregating the effects of multiple steps on overall water treatment performance with respect to microbial reduction.
No review was found on aggregating multiple steps, although a couple of papers (Haas and Trussell 1998 and Teunis et al. 2009) were found that assessed the treatment efficiency of multiple barriers independently.
Three (very brief) examples of how multiple steps are currently addressed in the GDWQ were found: pretreatment before membrane filtration; coagulation/flocculation/ sedimentation; and a subsection on combination (multiple-barrier) treatment approaches in the household water treatment section.
This work is related to other agenda items: updated treatment Tables 7.7 and 7.8 (see agenda item #39) and update of the QMRA text (see agenda item #51).
The need for a literature review for examples of the impact of aggregating multiple treatment steps should be confirmed.
Text could be added to, or current text could be edited in, Chapter 7, sections 7.3.2 and 7.3.3, on aggregating multiple steps and the need to incorporate text on moments of poor performance.
Summary of discussion:
Australia is looking at this, as well as Gertjan Medema in the Netherlands. It might be worth putting the aggregating multiple steps project on hold until the results of these studies are available, probably in 1 or 2 years.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
46
Rhodes Trussell is the author of a soon-to-be released book on this subject. KWR has produced a series of books, one titled “Log10 reductions”.
There may be a need to address this for large and small supplies, as well as household water treatment. In the current Guidelines, treatment is discussed under the headings Central treatment and Household treatment only. This might be resolved in the restructuring of Chapter 7.
There may not yet be enough information to do this, as only two references were found in the literature. However, there are other sources of information that have not been adequately mined, some peer reviewed, others in the grey literature. For example, the USEPA must have consulted the literature or generated new studies for the LT2 in the USA, and the results of the search and/or any new studies could be a good source of information.
Given the apparent lack of information and the expected availability of data in 1 or 2 years, perhaps this group should focus on preparing text for the second addendum or the fifth edition. Alternatively, the Mark LeChevallier text could address this.
As the GDWQ support the use of multiple steps, it is essential to have an evidence base to back up this support. As Gertjan Medema raised this issue, the group could ask him to look for data and also ask other people for data on the positive or negative influences of aggregating multiple steps.
Perhaps a few sentences should be written to address this for inclusion in the GDWQ. Volunteers are needed to write this text.
If one has the ability to evaluate the capability of multiple-barrier treatment processes to meet performance requirements, how necessary is it to evaluate the individual treatment steps? It was noted that if only total performance is evaluated, problems in the intermediate steps could be missed. It is important to evaluate each individual process; without this information, results cannot be interpreted correctly. One would end up with minimum removal, but would not be aware of the range possible with a treatment train.
Perhaps this group should look for examples, rather than doing a literature review; this would make it more feasible to complete the task before the first or second addendum.
Expected product(s): Text for treatment paragraph (first or second addendum); revised Chapter 7 (fifth edition); literature review (medium priority) Next steps (Microbial WG):
Lesley D’Anglada, David Cunliffe and Mari Asami volunteered to write some text for sections 7.3.2 and 7.3.3 on aggregating multiple steps.
Lesley D’Anglada will share information developed for the LT2 with this group.
The Secretariat will also ask Mark LeChevallier to address this issue in his treatment book.
The group will look for examples of positive or negative influences of aggregating multiple steps (including requesting data from Gertjan Medema). The literature review will be postponed for now.
#51. QMRA Background: Following the Dübendorf meeting, the Microbial WG requested a response as to how the following issues were being dealt with in the QMRA document: performance targets, multiple-barrier approach/aggregating multiple steps for water treatment performance,

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
47
short-term fluctuations and microbial methods. A response was received from Susan Petterson, one of the key authors of the QMRA document. The Microbial WG expressed its desire to confirm that issues related to the GDWQ are sufficiently addressed in the draft QMRA document. Progress since previous meeting: The QMRA document is nearing completion. A clean draft for final review should be ready by the end of July. Presentation (David Cunliffe):
Following the Dübendorf meeting, the Microbial WG asked whether certain issues (performance targets, aggregating multiple-barrier steps, short-term fluctuations, microbial methods) were covered adequately in the QMRA document and, if not, requested that text be added to cover those items.
Short-term fluctuations and performance targets are now dealt with, and microbial methods are included in Appendix B of the QMRA document. There is some discussion on barriers, but not necessarily on aggregating multiple barriers.
The QMRA document is being finalized. Comments from peer reviewers were received, and most, but not all, have been incorporated (by Susan Petterson and co-authors). A clean version should be ready by the end of July, to be sent back for another review.
Summary of discussion:
There seemed to be some confusion on this issue. There was considerable discussion about whether the authors of the QMRA document were aware of these issues and, if so, whether they had been addressed. However, David Cunliffe reported that three of the four issues had already been addressed, and the only issue remaining was aggregating multiple steps.
The QMRA text should acknowledge that aggregating multiple steps is an issue – that when steps are added together, performance may not be improved, but may actually be lowered. This issue falls into the category of uncertainty and could get framed in this context. The QMRA tools are all based on separate steps and do not take aggregation into account. There is a need to be transparent about this in the QMRA document.
In a review of the QMRA document, some concerns were expressed about certain aspects of the document, particularly regarding its accessibility. Some of the issues raised were on how to use QMRA when there are not enough data and on the complexity of presenting the data.
Gertjen Medema’s presentation at the Singapore International Water Week on going from low data to high data should be taken into consideration in the revisions of the QMRA document.
The 1999 book on QMRA by C.N. Haas, J.B. Rose and C.P. Gerba has been revised and should be released by the end of the calendar year. It should be informative, with new and more contemporary information to use as a resource.
Expected product(s): Revised text in Chapter 7 (fifth edition) Next steps (Microbial WG):
The Secretariat will contact the authors of the QMRA document and ask them to address the issue of aggregating multiple steps (see also agenda item #43).

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
48
#42. Background versus incidents (including short-term fluctuations) Background: The short-term fluctuations document by Peter Teunis et al. was never published. However, a short summary of the document was included in section 7.2.3 in the GDWQ. Health-based targets should be based on normal variation in the system and not on 100-year events or extreme events. Short-term fluctuations or system breakdowns should be defined to differentiate from natural noise or variability. Outbreaks are the final events of short-term fluctuations in drinking-water. At the Dübendorf meeting, determining whether the text included in section 7.2.3 is sufficient or whether it should be expanded and reviewing the consequences of outbreaks were identified as high priorities (for the first addendum). A workplan needs to be developed. The question about whether health-based targets should be set for general conditions or for the 95th percentile remains a high-priority (first addendum) issue with implications for Chapters 3, 7, 8 and 9. Progress since previous meeting: A briefing document on issues that need to be included in section 7.2.3 was prepared by David Cunliffe, for discussion at the current meeting. Presentation (David Cunliffe):
The Teunis et al. paper on “Short-term fluctuations in drinking water quality and their significance for public health” was provided to participants.
There is a brief mention of short-term fluctuations in pathogen concentration increasing disease risks and potentially triggering outbreaks of waterborne disease in section 7.1.3. At the end of section 7.2.3, it is recommended that arithmetic means of variables such as concentrations of pathogens in raw water be used.
One question is whether treatment plants should be operated to always be able to respond to incidents. The 95th percentile could be applied to source water concentrations, and treatment plants could be designed to respond to this. Another argument is to use the 50th percentile and look at extreme events separately. As discussed at the Dübendorf meeting, Australia is debating the use of 50th versus 95th percentiles for microbial data.
Issues to consider include variability in source water quality (pathogen concentrations and parameters such as turbidity, which affect treatment performance) and performance of control measures; the averaging of source water concentrations and treatment performance over a 12-month period to accommodate health outcome targets; the need for operating systems to continually deal with infrequent events; and the need to identify potential causes of catastrophic events and include responses in WSPs.
An example table of factors that influence variability and potential responses was provided, broken down into three components: source water, treatment and distribution (adapted from the draft QMRA text).
Next steps are to consider expanding the text in Chapter 7 (in the section on treatment or in the existing location), using either the Teunis et al. text or text from the QMRA document.
Summary of discussion:
The obvious application is to take these short-term fluctuations into account in risk assessment. A short text in the GDWQ (in Chapter 7, and perhaps also in Chapter 4 on

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
49
WSPs, with a cross-reference to the scoring matrix table in that chapter) and expanded text in the WSP manual are needed.
The frequency with which monitoring is performed affects the way in which peaks appear; this should be taken into account and flagged.
The recreational water quality guidelines clearly articulate that water quality changes after storms, for example.
This is a normal part of WSP training – the raw water quality may vary, and this needs to be taken into account. If the well known phenomenon that pathogen levels vary has not been conveyed in the GDWQ, this needs to be fixed.
There is some text in section 7.2.3 on QMRA about how to deal with variability. As the QMRA document deals with this, there is no need to add a lot of text.
Health-based targets (e.g. 10−6 DALY per person per year) are annual targets (based on average risks over a 12-month period). The GDWQ does not give guidance on how to treat data. There is a lot of normal variation in source water throughout the year (aside from catastrophic events). There is a straightforward way of dealing with this, but the GDWQ does not provide guidance on it. In the LT2, for example, Cryptosporidium numbers are averages from a certain number of samples. Brief guidance on this is important. Should the GDWQ go with average figures? What about short-term fluctuations?
Is this guidance aimed at water suppliers or regulators? The approach would differ depending on the audience.
Recent publications show that short-term decreases in efficacy result in profound health risks; this means that the goal is to always have a system in good control and responsive to incidents and fluctuations. How does that get operationalized for operators and managers? What is the direction to be provided for users of the GDWQ?
Variations in source water quality should be discussed in Chapter 7, whereas variations in treatment would go into Chapter 4.
How is normal variation to be interpreted? How much variation is the responsibility of the supplier? It is difficult to interpret the causes of variation (e.g. decreases in chlorine, increases in coliforms). What is the normal variation that has to be accepted?
The focus should be on large suppliers. This does not belong in Chapter 4. There is a need to make decisions on fluctuations in source water and to have a system that can deal with these. This belongs with specifications for system upgrades and QMRA.
There are three separate but related issues: 1) A short discussion of the issues covered by the Teunis et al. paper and the QMRA
document, on short-term fluctuations around normal performance (short-term variations in performance, short-term fluctuations in water quality), belongs in Chapter 7 as a general discussion or in terms of treatment.
2) Extreme events are a Chapter 4 issue, as the WSP responds to incidents; this is already covered in Chapter 4. Perhaps there should be a cross-reference from Chapter 7 to Chapter 4 for extreme events.
3) 10−6 DALY as an annual target – what does it mean in terms of monitoring data? The USEPA LT2 requires 24 monitoring points, working out the average and setting performance targets based on the average. How one arrives at the 1 Cryptosporidium per x litres number is not dealt with sufficiently in Chapter 7. It can be a simple piece of text.
The terminology used in Chapters 4 and 7 to refer to incidents and peaks or fluctuations is different. This should be looked at and harmonized. Should the GDWQ be using the

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
50
terminology used in the WSP manual? The WSP manual refers to incidents and risky circumstances.
Major incidents are a Chapter 4 and WSP manual issue; a cross-reference from Chapter 7 to Chapter 4 would be sufficient. A short text on short-term variation could go into Chapter 7, and the table of log reductions in Chapter 7 should be retained. Arithmetic means are already mentioned in section 7.2.3 and should be reinforced in other parts of the text. This might be sufficient.
Fluctuations apply primarily to source water; no background fluctuation in E. coli in drinking-water is acceptable.
The minor refinements required can be done when revising Chapter 7. The cross-referencing to Chapter 4 is not an urgent issue and can also be done when revising Chapter 7. The one part that is missing is the short-term fluctuations. Is it an urgent issue or one that can be addressed when Chapter 7 is restructured, given that the QMRA text deals with it in some detail?
If short-term fluctuations (not just incidents) are not included in the WSP manual, they should be, and in a way that can be readily put into practice.
Brief text needs to be added on short-term fluctuations, because the QMRA text already deals with it and can be cross-referenced. The WSP manual does not seem to deal with short-term fluctuations, but refers to the Teunis et al. text as “in press”. The Teunis et al. text has probably been overtaken by the QMRA text by now. This is not identified as an urgent issue and can be dealt with when Chapter 7 is revised.
Many countries are experiencing extreme events, which have increased in number and severity. This is going to be addressed in the climate change and WSP document being prepared by PUB. That document has been circulated to the regional offices. There has been some feedback on improving the document in terms of addressing water quantity issues and incorporating information on diversifying water sources and integrated water resource management into the document. Case-studies from developing countries (e.g. Nepal) are also needed. These are the next steps for this document.
The WSP manual in its current format emphasizes qualitative risk assessment, hazards and hazardous events. What is not embedded in the document is being more effective in the development of health-based targets in relation to fluctuations in source water quality and QMRA. This links more to QMRA than it does to WSPs.
Does the WSP manual address what to do in the event of fluctuations in turbidity, etc.?
In Argentina, normal fluctuation in one parameter, such as turbidity, is not usually considered a hazard. If the value is outside of the range of the average + two standard deviations, then it is considered abnormal.
Some incidents are not related to critical parameters (and risk), whereas others are. WSP users will know the distinction between critical and non-critical parameters.
When Chapter 7 is revised, there may be a need to revise the QMRA section.
The Mark LeChevallier text will deal with treatment variability and short-term fluctuations.
Expected product(s): Revised Chapter 7 to address background versus incidents, including short-term fluctuations (fifth edition)

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
51
Next steps (Microbial WG):
David Cunliffe and Ana Maria de Roda Husman will take the above discussion points into consideration when revising Chapter 7 for the fifth edition.
#48. Microbial detection methods Background: There is a need to include in the GDWQ general information on microbial methods, on the value of the different methods (e.g. culture, microscopy, nucleic acid amplification/detection, including quantitative polymerase chain reaction, immunoassay), and on when particular methods should be used to detect pathogens. Examples, limitations for each of the methods and data interpretation for methods that are most useful for characterizing the data should be included. Information should also be included in the QMRA document. A WHO project is in development on rapid testing to help in decision-making in low-resource settings, and a pilot study will be done. The Dübendorf meeting concluded that text should be included in section 7.4, in the QMRA document and in the rapid testing project. Progress since previous meeting: None Presentation (Ana Maria de Roda Husman):
There is a need to include general information on microbial methods in the GDWQ – on the value of the different methods available for different targets, on when particular methods should be used to detect pathogens and on the limitations of each of the methods.
There are only two brief mentions of microbial methods in two parts of the current GDWQ: at the top of p. 137 and in section 7.5 on methods of detection of faecal indicator bacteria, including Table 7.11 on ISO methods.
This agenda item is related to other agenda items: the restructuring of Chapter 7 (see agenda item #58), QMRA (see agenda item #51) and the new document in progress on the development of rapid testing to help in decision-making in low-resource settings.
Is a background document needed? Several books are available on methods that could be referenced. There is a WHO/Organisation for Economic Co-operation and Development (OECD) book titled Assessing microbial safety of drinking water: Improving approaches and methods (Chapter 8: Analytical methods for microbiological water quality testing).
Discussion is needed on text to be added to section 7.4 on microbial monitoring and alignment with the QMRA document and the rapid testing project.
Summary of discussion:
The QMRA document contains a brief text on analytical methods, which could be adapted to the GDWQ when Chapter 7 is revised (see agenda item #58).
It is agreed that a simple brief text is all that is required.
It should be noted that methods of detection of pathogens should be of sufficient quality.
It is necessary to emphasize that although different methods detect pathogens, they quantify pathogens in different ways. A general statement could be made, with cross-references to other documents.
Perhaps it would be useful to explain when methods can be used, for operational monitoring, for compliance, etc.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
52
Existing text in Chapter 4 suggests a certain set of parameters that are important to measure, which does not include monitoring for pathogens.
There is no need to capture detailed protocols; that should be left to ISO and similar organizations. However, it would be useful to provide some guidance on what test to use under certain situations and on how to interpret the reliability of tests in countries without centralized laboratories.
Should WHO be making statements about the suitability of certain tests – for instance, new rapid tests for E. coli monitoring?
The text could mention some pathogens that are measured in quite different ways (e.g. Legionella).
The text in the GDWQ should try to capture these concerns very briefly, with reference to other documents for more detail (preferably to a WHO document, but if not, then to one other paper as an example).
Expected product(s): New text for section 7.4 (first addendum); updated text for the QMRA document Next steps (Microbial WG):
Ana Maria de Roda Husman will draft some new text for section 7.4 for the first addendum.
#39. Treatment tables Background: Chapter 7 includes a treatment section with two tables (Tables 7.7 and 7.8) summarizing treatment processes that are commonly used to reduce microbes; it also refers to Annex 5 on treatment methods and performance. The treatment tables need to be updated. Recommendations at the Dübendorf meeting included updating Tables 7.7 and 7.8 with log reductions and with some information on CT values and turbidity; cross-linking both tables to documents with more information (e.g. CT values for chlorine); and including a note on Table 7.10 on the limitations of the use of E. coli as an indicator for other pathogens. A way forward needs to be proposed, including the identification of additional resources that should be reviewed in revising these treatment tables. Progress since previous meeting: The literature search reported on at the Geneva meeting has been updated to March 2014. Presentation (Kah Cheong Lai)
This is a joint effort by PUB and the National University of Singapore (NUS).
For the removal of microbial contaminants, the focus is on the performance of treatment technologies used in large community supplies (i.e. Table 7.7, not Table 7.8 on household water treatment).
For Table 7.7, on reductions of bacteria, viruses and protozoa, the literature search was conducted for papers published from 2006 to March 2014. Only English abstracts were reviewed.
The methodology was as described during the December 2013 Geneva meeting.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
53
The papers were grouped into three categories: 1) abstract clearly mentions a reduction in pathogens by the treatment process; 2) the reduction in pathogens is implied; and 3) does not fulfil criteria. Of 303 hits (PubMed database), 57 were category 1 papers and 52 were category 2 papers.
In the Table 7.7 review, for storage reservoirs (protozoa), conventional clarification (viruses) and slow sand filtration (viruses and bacteria) – treatment technologies with a sufficient number of category 1 hits – the literature search did not show minimum or maximum log reduction removals that were much different from those provided in the GDWQ.
A similar search was carried out for the chemical treatment tables in Annex 5 (Tables A5.1–A5.5). Only a few chemicals in each annex table had sufficient hits for analysis. Of these, changes to the removal of only arsenic (coagulation and activated carbon) and cadmium (activated carbon) were suggested by the literature search results; the rest remained unchanged.
Summary of discussion:
For arsenic, are the results from large-scale or small-scale facilities? This is important, as the arsenic guideline value is treatment based. Choon Nam Ong will share the arsenic information with Michèle Giddings, as this is important for the Health Canada arsenic guideline.
The suggestion to change the arsenic removal from >50% to >80% needs to be looked at carefully. It is not clear whether the data are from a municipal supply or a small supply. Small suppliers may not be able to achieve such a high removal.
The oxidation state of arsenic is useful information for treatment. If the speciation is available, it should be added to the table.
There needs to be consistency in the presentation of the numbers in the tables. At the moment, the number of significant digits used is inconsistent (e.g. 80% versus 97.21%). It was noted that the tables currently provide the actual values obtained from the literature. A subsequent panel could review the methodology and process followed.
PUB is considering creating a depository of these references so that they can be easily accessed.
Two of the three proposed revisions for arsenic and cadmium involved activated carbon. Skepticism was expressed about changing values on the basis of studies employing tailored, highly specific activated carbon.
As the Mark LeChevallier treatment text is being revised, there will need to be cross-checking against the results of this literature search. However, there is no need to wait for the publication of the LeChevallier text before proceeding with the updating of the treatment tables.
Integrating the results into the new Chapter 7 as it is restructured would be a good approach.
There should be an attempt to be systematic about presenting the sources of information.
It is emphasized that these are preliminary data only. These data now provide an evidence base for microbial removals from drinking-water.
Expected product(s): Updated Table 7.7 (with correction of heading error), Table 7.8 and Tables A5.1–A5.5 (fifth edition)

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
54
Next steps (Microbial WG):
PUB will work together with the authors of the rewrite of Chapter 7 (see agenda item #58) to incorporate this information for the fifth edition.
#40. Water treatment and pathogens Background: At the Dübendorf meeting, the updating of the Water treatment and pathogen control book (by Mark LeChevallier) to include WSPs, validation methods, information on surrogates, issues included in aggregating multiple steps and the multiple-barrier approach was identified as a medium priority. Progress since previous meeting: A co-author has committed to the project. Summary of discussion:
There have already been several suggestions from this meeting for additions to the content of the updated water treatment document: turbidity (see agenda item #46), aggregating multiple steps (see agenda item #43), intermittent distribution systems (see agenda item #44), reference pathogens (see agenda item #50) and short-term fluctuations (see agenda item #42).
Mark LeChevallier has obtained a commitment from Dr Kwok Kung Au to act as co-author.
Other volunteers have been identified who are willing to participate as contributors.
The literature search for an update of the treatment tables has been completed, and the full papers are now being checked (see agenda item #39).
Expected product(s): Revised Tables 7.7 and 7.8 (fifth edition) (see also agenda item #39); updated Water treatment and pathogen control book (time frame unknown) Next steps (Microbial WG):
The Secretariat will follow up with Mark Chevallier and his co-author to negotiate the timeline and suggest specific content for the revised text.
#45. Legionella Background: Prior to the Dübendorf meeting, it was noted that the risks posed by Legionella spp. in institutional hot water systems and the recommended management solutions probably need further consideration. Aspects that may be inadequately addressed in the GDWQ and supporting documents are recommendations for surveillance and analytical methods for detection and molecular typing. At the Dübendorf meeting, it was noted that the range of sources of Legionella is expanding, with more detection from cold water and from new devices with hot/cold water and compressors. It was suggested that the text in Chapter 6 (Special circumstances) should be edited to include alternative sources of exposure and to expand on risk analysis and WSPs. A lower priority was to review the Legionella document. The Geneva meeting agreed to update the text in Chapter 6 for the second addendum. Progress since previous meeting: The systematic review on alternative sources of Legionella in the Netherlands is almost completed.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
55
Summary of discussion:
The Geneva meeting agreed to add additional sources of Legionella that have been identified, such as ice machines, to Chapter 6 of the GDWQ.
The systematic review on alternative sources of Legionella in Australia has been initiated.
Ana Maria de Roda Husman’s PhD student has almost finished the systematic review of alternative sources of Legionella. Besides tap water and cooling towers, environmental sources (e.g. natural soils and bioaerosols) have been identified, and the effects of climate change are being explored. This information is worth adding to the GDWQ.
This is a global issue. Hotels are worried about legionellosis because of tourism.
The United States Centers for Disease Control and Prevention and the USEPA have conducted a literature search on the treatment of legionellosis. A document should be ready for external peer review by the end of 2014.
Are there any plans to set guideline values for Legionella in drinking-water? The USEPA has a maximum contaminant level goal of 0 as a target.
Numbers in warm water systems are much lower than those in cool water systems. There is increased discussion on Legionella coming from cold water systems. This is quite a complicated area. In buildings, systems may be poorly designed, with poor insulation, proximity to hot water pipes and storages in roofs.
Inhalation is more important than drinking-water ingestion for Legionella exposure.
Legionella contamination of showerheads is an issue of concern.
The Legionella issue is premise plumbing related, and the guidance needs to deal with this. There are already a lot of books published on this, including a WHO book.
One of the major issues is that Legionella may not be found in drinking-water, but it may be found if swab testing is done on water from water fountains, hot water heaters, storage tanks or spas.
Expected product(s): Revised text of Chapter 6 (second addendum) Next steps (Microbial WG):
The Microbial WG will wait for the outcomes of the two systematic reviews on alternative sources of Legionella and then revise the text of Chapter 6 for the second addendum.
#59. Rainwater harvesting Background: Rainwater harvesting is in use in many countries throughout the world. Rainwater collected and used on-site can supplement or replace other sources of household water. Rainwater can also be used as drinking-water if it is properly treated before use. The GDWQ Final Task Force meeting in 2003 identified safe rainwater harvesting as an important omission from the GDWQ and requested that a text to address it be developed as soon as possible. Text on rainwater harvesting for Chapter 6 of the GDWQ was published in the second addendum to the third edition (section 6.11) and in the fourth edition (section 6.2), but a stand-alone document (with a main focus on the development of WSPs for rainwater harvesting systems) has still not been finalized. Summary of discussion:
The rainwater text in the GDWQ has preceded the stand-alone text, which is long overdue. The focal point lead is Han Heijnen.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
56
The rainwater harvesting topic potentially can be linked to addressing stored water (which was not included as a separate agenda item). Mark Sobsey wrote a briefing note on hygienic storage of water for the Dübendorf meeting. Joe Brown has agreed to work on a document on water storage, but the scope of the document needs to be negotiated with him.
Rainwater could be mentioned as a source water in Chapter 7. Expected product(s): Stand-alone text on rainwater harvesting (time frame unknown) Next steps (Microbial WG):
Sophie Boisson will follow up with Han Heijnen. #49. Antimicrobial resistance Background: Since the 1940s, antimicrobial drugs have significantly decreased mortality from infectious diseases and supported advancements in modern medicine, such as surgery. However, the world is now facing a crisis, because antimicrobial resistance is progressively eroding the effectiveness of antimicrobial drugs. At the Dübendorf meeting, it was noted that recent publications on antimicrobial resistance in wastewater suggested that recycling or reusing water may be a source of contamination. It is important to learn the relevance of antimicrobially resistant bacteria and to understand the different mechanisms in the transference of antimicrobial resistance genes. The Geneva meeting was asked to review the initial work on a literature search related to antimicrobial resistance and water, sanitation and hygiene (WASH) and review the workplan. These activities can be incorporated with the antimicrobial resistance activities on wastewater. Summary of discussion:
Mark Sobsey gave a presentation on antimicrobial resistance at Singapore International Water Week.
The relationship between antimicrobial resistance and WASH has been elevated to a higher priority at WHO. The issue was brought before the World Health Assembly in May 2014, and it was agreed that there was a high-level need to address this issue. An action plan is to be developed. The six-page briefing note to the World Health Assembly can be shared with meeting participants. The work group included Ana Maria de Roda Husman, Nick Ashbolt and Paul Hunter, among others.
The GDWQ should address antimicrobial resistance in some way. This group will need to consider where this should be included and what should be included. A plan of work needs to be developed on the issue of antimicrobial resistance in the context of drinking-water, sanitation and hygiene.
PUB has information to share with this group on antimicrobial resistance.
Expected product(s): Additional text for GDWQ (fifth edition) Next steps (Microbial WG):
Sophie Boisson will share the World Health Assembly briefing note with meeting participants.
PUB will share its information on antimicrobial resistance with this group.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
57
A plan of work needs to be developed at the next meeting of the Microbial WG. #47. Vulnerable populations Background: The Final Task Force meeting in 2003 recommended that guidance be developed to address the specific concerns of vulnerable populations in the fourth edition of the GDWQ, in particular to propose effective action for the reduction of waterborne disease in these populations. Text was developed for Chapters 6 and 7 to address this issue. The Dübendorf meeting concluded that future iterations of the Guidelines should consider how vulnerable subpopulations exposed to different waters under different local circumstances should be identified, how risk should be assessed for vulnerable subpopulations and whether health-based targets should be set for vulnerable subpopulations. It was also concluded that future iterations of the water quality guidelines should present vulnerable groups more consistently and that the standpoint on vulnerable groups should be harmonized in the overarching document on the three water guidelines. The Geneva meeting identified next steps for work on vulnerable groups. Summary of discussion:
As a result of time constraints, this issue was not discussed in detail. Ana Maria de Roda Husman reminded participants that in the future, all new documents, revised documents or new editions of the Guidelines should consider how to identify and assess risk for vulnerable populations.
Expected product(s): Various publications (fifth edition) Next steps (Microbial WG):
This agenda item should be discussed at the next meeting of the Microbial WG. 8. CLOSING SESSION The next meeting of the Chemical WG is tentatively scheduled for the first quarter of 2015, and a meeting of the Microbial WG is tentatively scheduled for the second quarter of 2015. Both meetings will aim to progress items for inclusion in the first addendum to the fourth edition, to be published at the end of 2015. Bruce Gordon thanked the experts for their contributions, Sophie Boisson for her preparations for the meeting, the chairs of the individual sessions and Marla Sheffer for rapporteuring the meeting. He also acknowledged Japan, the USA, Singapore and the Netherlands for their support of the meeting and Singapore for their warm hospitality. Mong Hoo Lim expressed his pleasure in participating for the first time in this expert meeting and reiterated that PUB was happy to be part of this WHO initiative. Mark Sobsey thanked Bruce Gordon, Sophie Boisson and the WHO leadership for bringing this group together. The meeting was closed.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
58
ANNEX 1: List of participants for the WHO Meeting on the Guidelines for Drinking-water Quality
LIST OF PARTICIPANTS3
WHO Meeting on the Guidelines for Drinking-water Quality
Singapore, 5–7 June 2014
Mari Asami Department of Water Supply Engineering National Institute of Public Health 2-3-6 Minami Wako Saitama 351-0197 Japan Ruth Bevan Lecturer in Human Health and Risk Assessment, and Project/Resource Manager Cranfield Health Vincent Building Cranfield University Bedfordshire MK43 0AL United Kingdom Enrique Calderon AYSA Tucuman 752 Buenos Aires Argentina Philip Callan Consultant 28 Helen Mayo Crescent Bonython ACT 2905 Australia Joseph Cotruvo Joseph Cotruvo & Associates and NSF International WHO Collaborating Centre 5015 46th Street NW Washington, DC 20016 USA David Cunliffe Department of Health Public Health PO Box 6
3 An asterisk (*) indicates that the individual was invited but unable to attend.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
59
Rundle Mall Adelaide SA 5001 Australia Lesley V. D’Anglada Office of Water Office of Science and Technology United States Environmental Protection Agency 1200 Pennsylvania Avenue, NW (MC 4304T) Washington, DC 20460 USA Ana Maria de Roda Husman National Institute of Public Health and the Environment (RIVM) Center for Infectious Disease Control Laboratory for Zoonoses and Environmental Microbiology (LZO; Bag 63) Department of Environment PO Box 1 / Antonie van Leeuwenhoeklaan 9 3720 BA Bilthoven The Netherlands John Fawell Visiting Professor Cranfield University 9 Dandridge Drive Bourne End Bucks, SL8 5UW United Kingdom Lorna Fewtrell* Institute of Geography & Earth Sciences Aberystwyth University Llandinam Building Penglais Campus Aberystwyth, SY23 3DB United Kingdom Michèle Giddings Health Canada Water Quality & Science Division Water and Air Quality Bureau 3rd Floor (Rm 3-005A) 269 Laurier Avenue West, A.L. 4903A Ottawa, Ontario Canada K1A 0K9 Yoshihiko Matsui* Division of Environmental Engineering Faculty of Engineering Hokkaido University

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
60
N13W8 Sapporo 060-8628 Japan Gertjan Medema* Chair on Water & Health Delft University of Technology / KWR Watercycle Research Institute NL-3430 BB - Nieuwegein The Netherlands Bette Meek Associate Director, Chemical Risk Assessment McLaughlin Centre for Population Health Risk Assessment University of Ottawa One Stewart Street, Suite 309 Ottawa, Ontario Canada K1N 6N5 Edward Ohanian* Associate Director for Science Office of Water (Mail Code 4301T) United States Environmental Protection Agency Ariel Rios Building 1200 Pennsylvania Avenue, NW Washington, DC 20460-0001 USA Choon Nam Ong Environmental Research Institute National University of Singapore Lower Kent Ridges Road Singapore 119077
Marla Sheffer 1553 Marcoux Drive Orleans, Ontario Canada K1E 2K5 Shane Snyder Large University and Research Centers 1133 E. James E. Rogers Way Harshbarger 118 Tuscon Arizona 85721 USA Mark Sobsey University of North Carolina at Chapel Hill CB No. 7431 Rosenau Hall, Room 149C Chapel Hill

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
61
North Carolina 27599-7431 USA WHO Secretariat Sophie Boisson Water, Sanitation, Health & Hygiene (WSH) World Health Organization 20 Avenue Appia 1211 Geneva 27 Switzerland Bruce Gordon Water, Sanitation, Health & Hygiene (WSH) World Health Organization 20 Avenue Appia 1211 Geneva 27 Switzerland Kah Cheong Lai (outposted secondee to WHO) Public Utilities Board 40 Scotts Road #22-01 Environment Building Singapore 228231 WHO Regional Offices Mohd Nasir Hassan* Environment Health World Health Organization Western Pacific Regional Office PO Box 2932 1099 Manila Philippines Alexander von Hildebrand Environment Health World Health Organization Western Pacific Regional Office PO Box 2932 1099 Manila Philippines PUB participants
Suok Kai Chew Deputy Director of Medical Services (Health Regulation Group) Ministry of Health Singapore

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
62
Jiangyong Hu Associate Professor Department of Civil and Environmental Engineering National University of Singapore (NUS) 1 Engineering Drive 2, E1A 07-03 Singapore 117576 Mong Hoo Lim Chief Specialist (Water Quality) Water Quality Office Public Utilities Board 40 Scotts Road #22-01 Environment Building Singapore 228231 Aik Num Puah Chief Specialist (Water Treatment) Technology Department Public Utilities Board 40 Scotts Road #22-01 Environment Building Singapore 228231 Kee Wei Wong Chief Specialist (Water Supply Network) Water Supply (Network) Department Public Utilities Board 40 Scotts Road #22-01 Environment Building Singapore 228231 Observers Toyozumi Kojima Deputy Director Water Supply Division Health Service Bureau Ministry of Health, Labor and Welfare 1-2-2 Kasumigaseki Chiyoda-ku Tokyo 100-8916 Japan Tsze Han Tan4 Senior Planning Officer Policy & Planning Department Public Utilities Board 40 Scotts Road
4 For reuse session only.

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
63
#22-01 Environment Building Singapore 228231
Chee Hoe Woo Principal Specialist (Water Quality) Water Quality Office Public Utilities Board 40 Scotts Road #22-01 Environment Building Singapore 228231

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
64
ANNEX 2: Agenda for the WHO Meeting on the Guidelines for Drinking-water Quality Day 1: Thursday 5 June 2014
Time Agenda item Notes
0830–0900 Daily preparatory meeting of chair, rapporteur and WHO secretariat
0900–1030 Session 1 - Introductions, objectives and updates Chair: Bruce Gordon
Welcome by PUB, WHO Collaborating Centre (Mong Hoo Lim)
Update on key achievements on water quality and health (Bruce Gordon)
Meeting overview, objectives and methods of work
Declaration of interests and Election of officers (Sophie Boisson)
1030–1100 Coffee
1100–1230 Session 2 – Direct and indirect potable reuse Chair: Michèle Giddings
#33
Overview of objectives and expected outcomes (Michèle Giddings/Kah Cheong Lai)
Potable reuse practices and principles (Joe Cotruvo)
Evidence gaps (John Fawell)
See annotated agenda for reference documents and session objectives
1230–1330 Lunch
1330–1500 Session 3 – Direct and indirect potable reuse (cont.) Chair: Michèle Giddings
Regulatory aspects (David Cunliffe)
Water utility perspective (Mong Hoo Lim)
Wrap-up, follow-up and next steps
See annotated agenda for reference documents and session objectives
1500–1530 Coffee
1530–1730 Session 4 – Chemical mixtures Chair: Bette Meek
#52 Introduction and objectives of the session (Bette Meek)
Review of background document structure and content (Ruth Bevan)
Review of case study examples (Ruth Bevan)
Wrap-up, follow-up and next steps
See annotated agenda for reference documents and session objectives
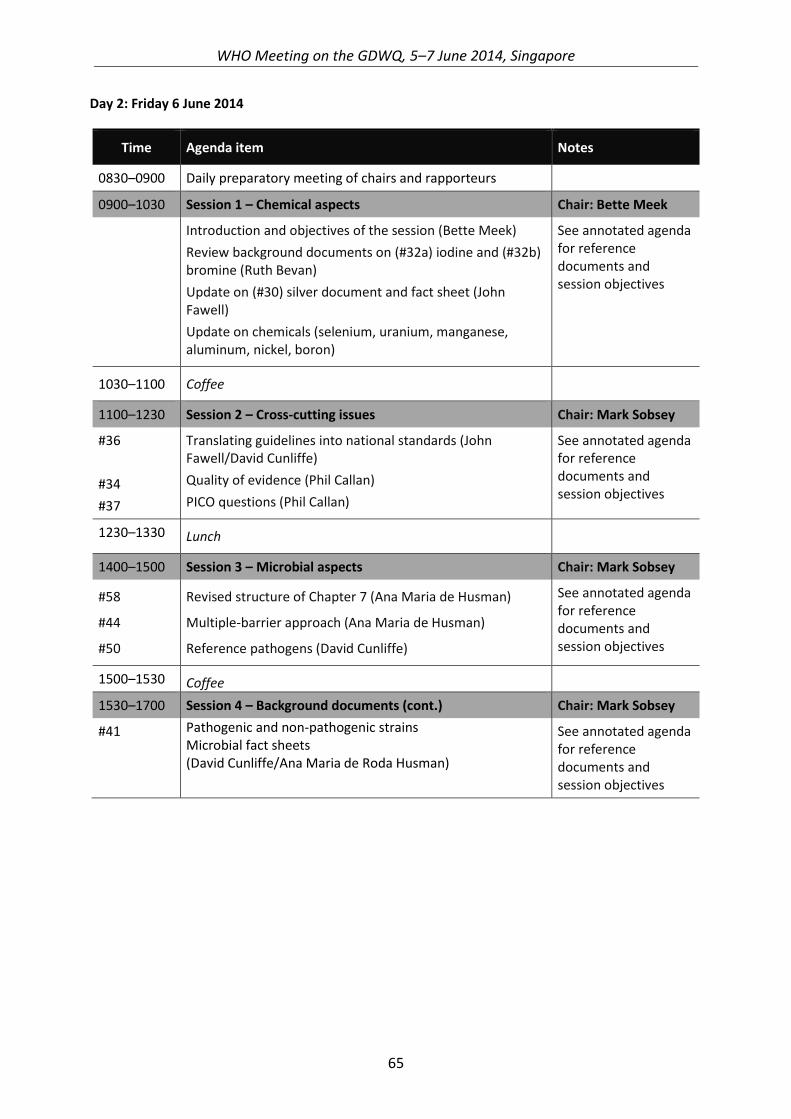
WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
65
Day 2: Friday 6 June 2014
Time Agenda item Notes
0830–0900 Daily preparatory meeting of chairs and rapporteurs
0900–1030 Session 1 – Chemical aspects Chair: Bette Meek
Introduction and objectives of the session (Bette Meek)
Review background documents on (#32a) iodine and (#32b) bromine (Ruth Bevan)
Update on (#30) silver document and fact sheet (John Fawell)
Update on chemicals (selenium, uranium, manganese, aluminum, nickel, boron)
See annotated agenda for reference documents and session objectives
1030–1100 Coffee
1100–1230 Session 2 – Cross-cutting issues Chair: Mark Sobsey
#36
#34
#37
Translating guidelines into national standards (John Fawell/David Cunliffe)
Quality of evidence (Phil Callan)
PICO questions (Phil Callan)
See annotated agenda for reference documents and session objectives
1230–1330 Lunch
1400–1500 Session 3 – Microbial aspects Chair: Mark Sobsey
#58
#44
#50
Revised structure of Chapter 7 (Ana Maria de Husman)
Multiple-barrier approach (Ana Maria de Husman)
Reference pathogens (David Cunliffe)
See annotated agenda for reference documents and session objectives
1500–1530 Coffee
1530–1700 Session 4 – Background documents (cont.) Chair: Mark Sobsey
#41 Pathogenic and non-pathogenic strains Microbial fact sheets (David Cunliffe/Ana Maria de Roda Husman)
See annotated agenda for reference documents and session objectives

WHO Meeting on the GDWQ, 5–7 June 2014, Singapore
66
Day 3: Saturday 7 June 2014
Time Agenda item Notes
0830–0900 Daily preparatory meeting of chairs and rapporteurs
0900–1030 Session 1 – Microbial aspects (cont.) Chair: Mark Sobsey
#46
#43
Turbidity (David Cunliffe/Michèle Giddings)
Aggregating multiple steps
See annotated agenda for reference documents and session objectives
1030–1100 Coffee
1100–1230 Session 2 – Microbial aspects (cont.) Chair: Mark Sobsey
#51
#42
#48
QMRA (David Cunliffe)
Background versus incidents (David Cunliffe)
Microbial detection methods (Ana Maria de Roda Husman)
See annotated agenda for reference documents and session objectives
1230–1330 Lunch
1330–1500 Session 3 – Microbial aspects (cont.) Chair: Mark Sobsey
#39
#40
#45
#59
#49
#47
Treatment tables (Kah Cheong Lai/Choon Nam Ong)
Water treatment and pathogens (Ana Maria de Roda Husman)
Review of priorities
- Legionella (David Cunliffe)
- Rainwater harvesting (David Cunliffe)
- Antimicrobial resistance (Mark Sobsey)
- Vulnerable populations (Ana Maria de Roda Husman)
Confirmation of way forward and closing microbial meeting
See annotated agenda for reference documents and session objectives