zeroing in on the patient to reduce alert fatigue
TRANSCRIPT

1
Zeroing in on the Patient to Reduce Alert FatigueSession 298, March 9, 2018
Charlie Hart, Pharm.D., Pharmacy Informatics, Mercyhealth

2
Charlie Hart, Pharm.D.
Salary: Mercyhealth
Consulting Fees: Wolters Kluwer - Pharmacy Informatics Advisory Board
Conflict of Interest

3
Agenda• The limitations of traditional drug drug interactions (DDI)
• Clinical prescribing scenario demonstrating traditional DDI limitations
• Leveraging patient data to enhance DDI alerts
• Hyperkalemia enhanced DDI alert demonstrated
• QTc prolongation enhanced DDI alert demonstrated
• Future possibilities explored

4
Learning Objectives• Demonstrate why it’s important to integrate patient specific
information into medication alerting systems
• Illustrate how to leverage information contained in the electronic medical record into alerts and trigger them at the most appropriate point in the workflow
• Assess how more specific alerting and care guidance can help to reduce the number of alerts – and subsequent alert fatigue
• Differentiate between medication alerts and more comprehensive care guidance that can have a more positive effect on patient care processes and potentially outcomes

5
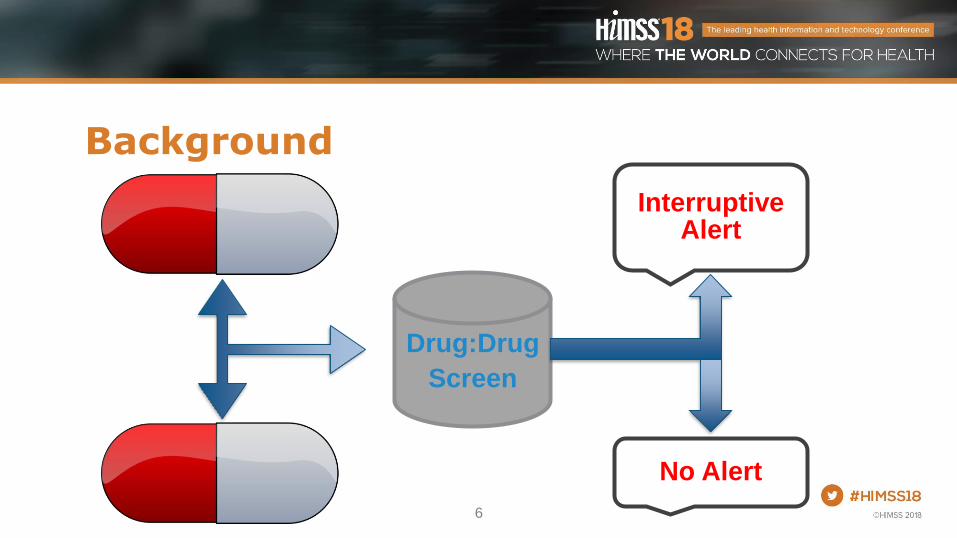
Background
Interruptive drug interaction alerts may reduce adverse drug events. Despite intensive efforts to improve commercial drug interaction alert system and to reduce alerting, override rates remain as high as reported over a decade ago. The results suggest the need to fundamentally question the premises of drug interaction alert systems.
1. Bryant AD, Fletcher GS, Payne TH. Drug interaction alert override rates in the meaningful use era. No evidence of progress. Appl Clin Inform. 2014;5(3):802–813. doi: 10.4338/ACI-2013-12-RA-0103.
6
Background
Drug:Drug
Screen
Interruptive Alert
No Alert

7
Background
Drug:Drug
Screen
Interruptive Alert
HyperkalemiaSpironolactone
Potassium
8
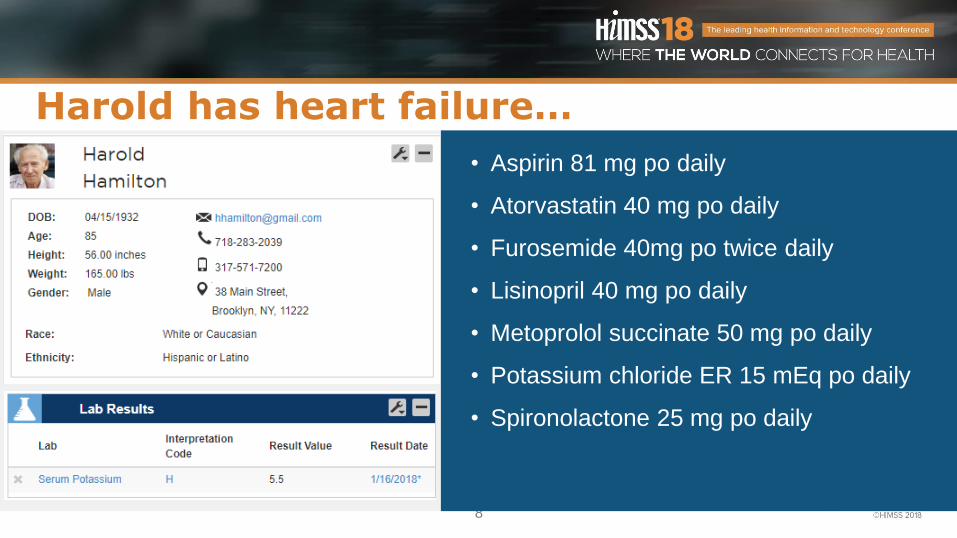
Harold has heart failure…
• Aspirin 81 mg po daily
• Atorvastatin 40 mg po daily
• Furosemide 40mg po twice daily
• Lisinopril 40 mg po daily
• Metoprolol succinate 50 mg po daily
• Potassium chloride ER 15 mEq po daily
• Spironolactone 25 mg po daily

9

10
Drug:Drug
Screen
Interruptive Alert
Hyperkalemiaspironolactone
Potassium

11
Drug:Drug
Screen
Interruptive Alert
HyperkalemiaLisinopril
Potassium

12
Harold has heart failure…
• Aspirin 81 mg po daily
• Atorvastatin 40 mg po daily
• Furosemide 40mg po twice daily
• Lisinopril 40 mg po daily
• Metoprolol succinate 50 mg po daily
• Potassium chloride ER 15 mEq po daily
• Spironolactone 25 mg po daily

13
Drug:Drug
Screen
Interruptive Alert
Hyperkalemiaspironolactone
Potassium

14
Drug:Drug
Screen
Interruptive Alert
HyperkalemiaLisinopril
Potassium

15
Background• Traditional (DDI) are Siloed
– When a drug is ordered it is checked serially against current ordered medications
• Additive Effects
• Dose Depended Effects
• Patient Factors not Evaluated
– Lab Values
– Patient Age
– Comorbidities

16
We Can Do Better
• Leverage EHR
– Demographics
– Lab
– Comorbidities
• Multi-Domain Drug Interactions
– Drug Drug Lab
– Drug Drug Disease
– Drug Drug Dose
– Drug Drug Drug
• Utilize Existing Drug Interaction Literature
– Established Risk Factors
– Validated Scoring Systems
CanWe Do Better?

17
System 1: Basic CDS vs. System 2: Advanced CDS
Source: Eppenga et.al. “Comparison of a basic and an advanced pharmacotherapy-related clinical decision support system in a hospital care setting in the Netherlands.” Journal of American Medical Informatics Association. 2012; 19: 66-71.

18
Interruptive Alert
Hyperkalemiaspironolactone
Potassium
Patient Hyperkalemia Risk Factors
Drug:Drug
Screen
No / Passive Alert

19
Established Scoring System
Risk Score
>2 = Interruptive Alert <2 = Passive Alert
Hyperkalemia Risk Factors
Age > 70 CrCl < 50 DiabetesHeart
FailureACE-I /
ARB K Sparking Diuretics

20
Interruptive Alert
Hyperkalemiaspironolactone
Potassium
Patient Hyperkalemia Risk Factors
Drug:Drug
Screen
No / Passive Alert

21
Phone Home• EHR sends CDA to Drug Data Vendor
• Drug Data Vendor Send Back a Response
• Vendor Maintains and Updates Clinical Content of Alert
• Response Will Vary Based on Patient
– Related Alerts Consolidated
– Recommend Actions
– Recommend Follow ups

22
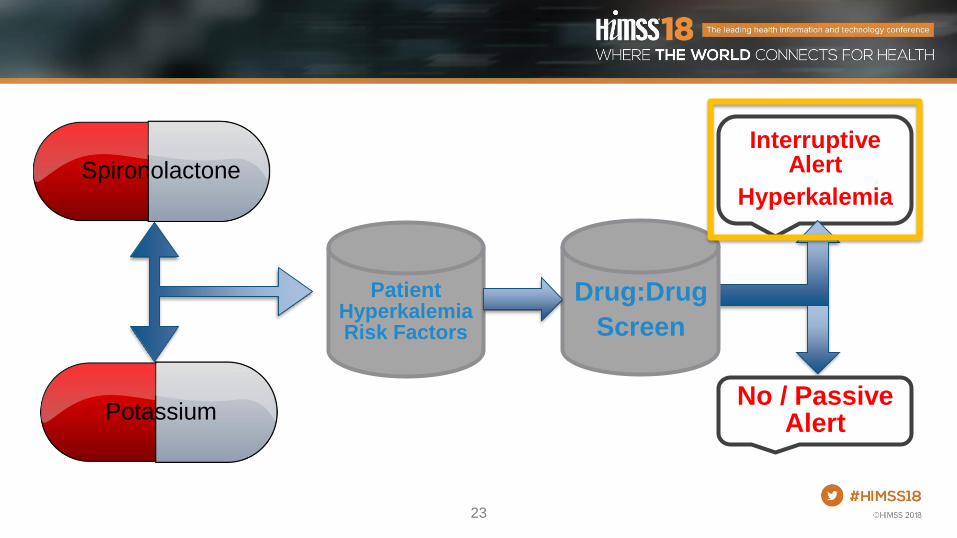
23
Interruptive Alert
HyperkalemiaSpironolactone
Potassium
Patient Hyperkalemia Risk Factors
Drug:Drug
Screen
No / Passive Alert
24
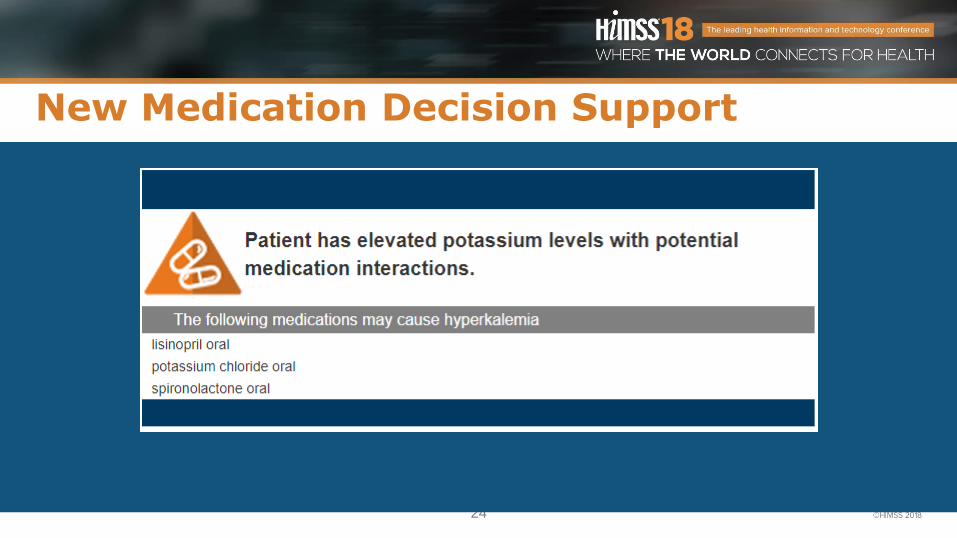
New Medication Decision Support

25
25
Internal to EHR External to EHR
• Local Knowledge & Data
• Local Computation & Rule Logic
• Technical & workflow integration matters
• Consistency with internal CDS avoids confusion
• May not require Vendor programming
• Enables new types of CDS that rely on computing power (eg. A.I.) or Registries/massive data (eg. PDMP, genomics)
EHR Proprietary Extensibility

26
System 1: Basic CDS vs. System 2: Advanced CDS
Source: Eppenga et.al. “Comparison of a basic and an advanced pharmacotherapy-related clinical decision support system in a hospital care setting in the Netherlands.” Journal of American Medical Informatics Association. 2012; 19: 66-71.

27
Results• Using Traditional Drug Drug Hyperkalemia Screening
– 10,896 interruptive alerts per year
• Patient Based Drug Screen
– 5,636 per year
• Incidence of Actual Hyperkalemia unchanged
– 13 patients / 27,998 doses of potassium administered (>5.5)

28
QT Wave Prolongation• Time Between the Start of the Q WaveEnd of the T Wave
– QT interval represents electrical depolarization and repolarization of the ventricles
– Prolonged QT interval is a marker for the potential of ventricular tachyarrhythmia
• Torsades de pointes
• Risk factor for sudden death
• QTc – Heart-rate Corrected QT Interval
29
QTc Prolongation• 37 drugs known to increase QTc and clearly associated with TdP
even when taken as recommended
– Abx – azithromycin, ciprofloxacin, levofloxacin
– Antidepressants – citalopram, escitalopram
– Surgical – ondansetron, propofol, sevoflurane
• 90 drugs known to increase QTc but lacking evidence for risk of TdPwhen taken as recommended
• 41 drugs associated with TdP buy only under certain conditions such as hypokalemia or excessive dose

30
Alert Fatigue• QTc Prolongation
– 4 of the Top 10 Drug Drug Alerts
– 11% of all Drug Drug Alerts

31
QTc Prolongation
Drug:Drug
Screen
Interruptive Alert Ondansetron
Levofloxacin

32
QTc Prolongation
Drug:Drug
Screen
Interruptive Alert Ondansetron

33
QTc Prolongation• Single Drugs in Patients with Risk Factors for Adverse Drug Events
Cannot be Screened
• Only Somewhat Addressed by Other Modules
– Drug Disease
– Geriatric
– Pediatric
• Risk Factors Other Than Age and Diagnosis Left Unaddressed

34
Established Scoring System
Risk Score
>7 = Interruptive Alert <7 = Passive Alert
Hyperkalemia Risk Factors
Age > 68
FemaleCHF MI Sepsis
QTc K <3.5Loop
DiureticsQTC
Drugs

35
Interruptive Alert
QTcOndansetron
Levofloxacin
Patient QTcRisk Factors
Drug:Drug
Screen
No / Passive Alert

36
Interruptive Alert
QTcOndansetron
Patient QTcRisk Factors
Drug:Drug
Screen
No / Passive Alert
37
Results• Using Traditional Drug Drug QTc Screening
– 93,916 interruptive alerts per year
• Patient Based Drug Screen (projected)
– High Risk 3,276 interruptive alerts per year
– Moderate Risk 18,004 interruptive alerts per year
– 78% reduction in interruptive alerts

38
Future• Opiate Morphine Milligram Equivalents (MME)
– Calculate MME for all Opiates the patient is on, not just the one being prescribed
• ACE-I + Loop diuretic (Hypotension)
– Normal sodium
• Drug Induced Myopathy
– Age, Sex, BMI, Common Co-Morbidities
• Antimicrobial Stewardship
• Therapeutic Substitutes

39
Questions
• Charlie Hart
• www.linkedin.com/in/charles-hart-PharmD
• Please remember to complete online session evaluation