zika outbreak preparedness: lessons from ebola
TRANSCRIPT
Outbreak preparedness: lessons from Ebola
Angela MC Rose
CDRC, TMRI, UWI
Barbados
Bridgetown, Barbados
05 February 2016
2
• Outbreak preparedness
• Lessons learned from Ebola
– global, WHO level (4 key lessons)
– field level
• Features of a Zika outbreak/what to expect
• PAHO’s 3 pillars of control
– Barbados example
• Summary
Outline
Ebola
• Direct transmission – case-finding, contact-
tracing key elements
• Urgent response – high mortality rate
• Community engagement
– changes in cultural practice
– stigma for survivors
• Need for research
3
Ebola vs Zika disease
Zika
• Vector-borne disease
– vector control key
• Urgent response
– ? MR, ? associated birth defects
– rapid spread thru naïve pop’n
• Community engagement – understanding of disease, risk
– stigma for families
• Urgent need for research
• State of being prepared, ready
• Having all necessary tools for control
“Give me six hours to chop down a tree and I will spend the first four sharpening the axe”
Abraham Lincoln
• Learning from previous outbreaks
4
Outbreak preparedness
An early lesson from the Ebola outbreak
in the three most affected countries
“The outbreak was particularly
challenging because health system
and public health infrastructure in
all three affected countries were
extremely fragile…
Business as usual is not an option”
(Report of the Ebola Interim Assessment Panel,
WHA 68: 2015)
Source: WHO Ebola Preparedness Team (EPT) & GOARN Operational Support Team (OST)
5

Lessons learned from Ebola: WHO level
• WHO global Ebola preparedness activities
– weak health system components
– lack of core capacities to effectively respond
– insufficient numbers/training for decentralised response
– no standard mechanisms to test response capability
– gaps in strategic health plans
• not just technical capacity
• planning, co-ordination, logistics, financing
– emergency preparedness activities
• applied vertically and time-fragmented
• no translation into overall emergency planning
Source: WHO OPT & GOARN OST
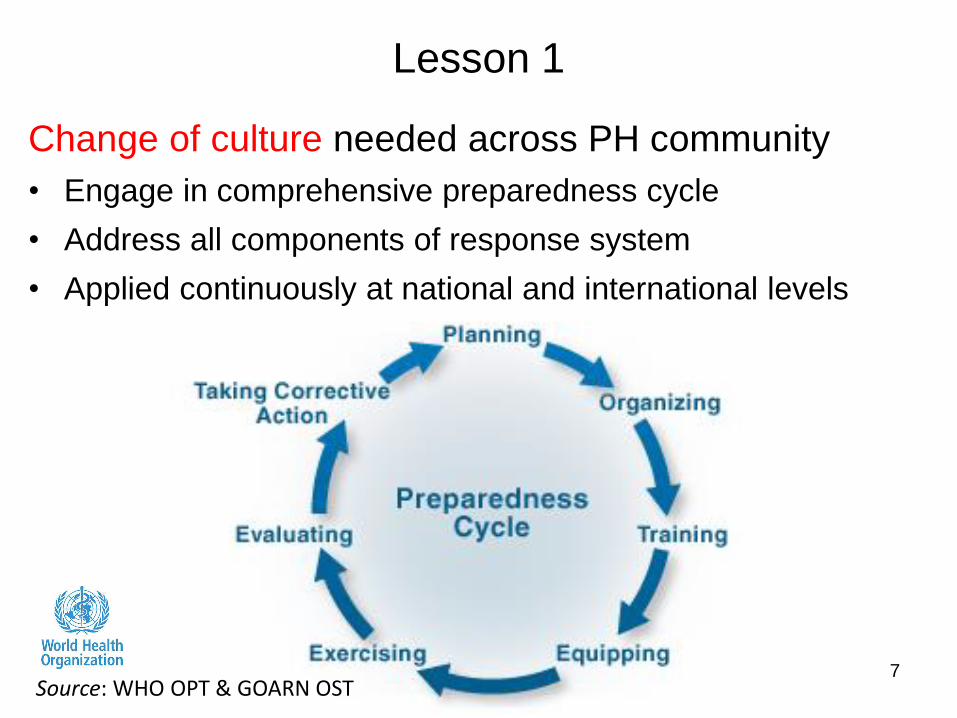
Lesson 1
Change of culture needed across PH community
• Engage in comprehensive preparedness cycle
• Address all components of response system
• Applied continuously at national and international levels
7 Source: WHO OPT & GOARN OST
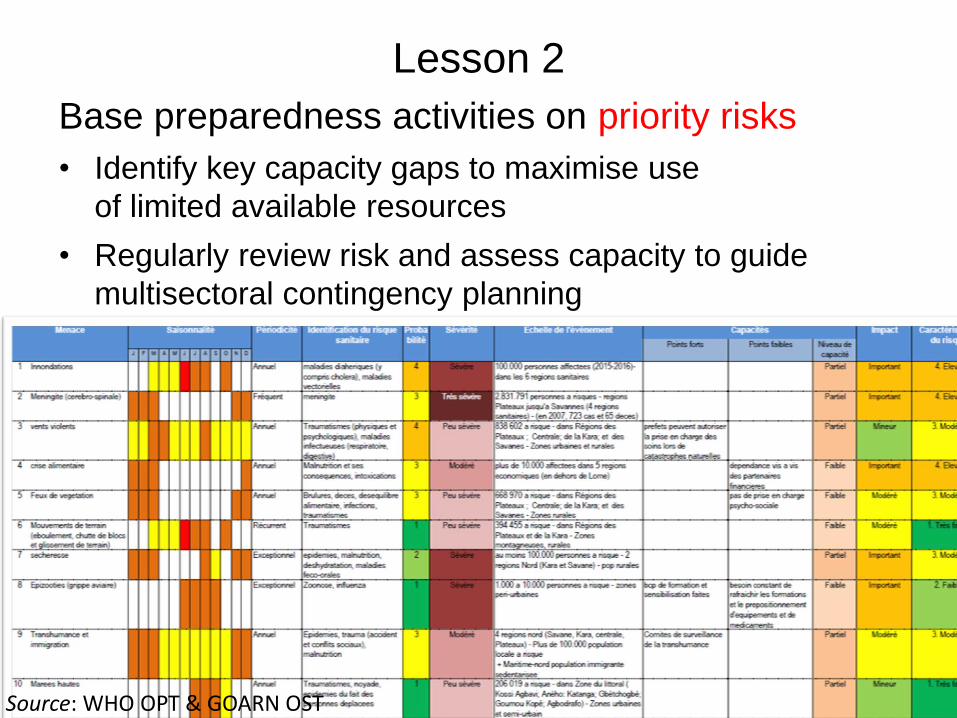
Lesson 2
Base preparedness activities on priority risks
• Identify key capacity gaps to maximise use
of limited available resources
• Regularly review risk and assess capacity to guide
multisectoral contingency planning
Source: WHO OPT & GOARN OST
Lesson 3
Operational readiness
• Relies on strong and clear organisational systems
– able to access and co-ordinate financial, material and
human resources, as well as technical capacities
• mount emergency responses at the field level
– functionality of response systems reinforced and tested
regularly through simulation exercises
9 Source: WHO OPT & GOARN OST
Lesson 4
A “whole-of-government” and “whole-of-society”
approach to emergency readiness is required
• Large-scale health emergencies will overwhelm capability
of any one entity to mount effective and timely response
• Preparedness activities should bring together all key actors
10 Source: WHO OPT & GOARN OST
• Social mobilisation/community engagement key
– do not underestimate the power of the internet, rumour, etc.
• Gain trust of population – without trust, we cannot hope to engage public
– messages to public need care
– public’s risk perception different from that of “experts”
– perception rooted in sub-conscious, often not logical
– e.g. US Ebola survey (N>1000) o 64%: 21 days quarantine even without symptoms
o 56%: US should ban travel from affected countries
o 22%: avoid public transport in the US during holiday season
11
Lessons learned from Ebola: field level
• Co-ordination – need for transparency, communication, data/info. sharing
• Risk assessment – early phase: identify gaps and strengths
– adapt over time
• Inter-sectoral co-operation – civil society, public and private sectors
– tourism, environment, health, education
– identify challenges to co-operation
12
Lessons learned from Ebola: field level
• Travel issues – cost impact of tourism loss to economy
– impact of mass gatherings o carnival
o cricket
o 50th independence celebrations
• Stigmatisation – region, country, individual
– we fear what we don’t know
– key is openness, information sharing, communication
– start generating discussion
– dispel myths, rumours
13
Lessons learned from Ebola: field level
• Generally mild, short-lived – high number of cases
• Potential link with neurological conditions – microcephaly (babies) – GBS (adults)
• Similar to other circulating flavivirus infections – dengue, chikungunya – fever, rash, conjunctivitis, joint pain – ? co-infections
14
Key features of Zika
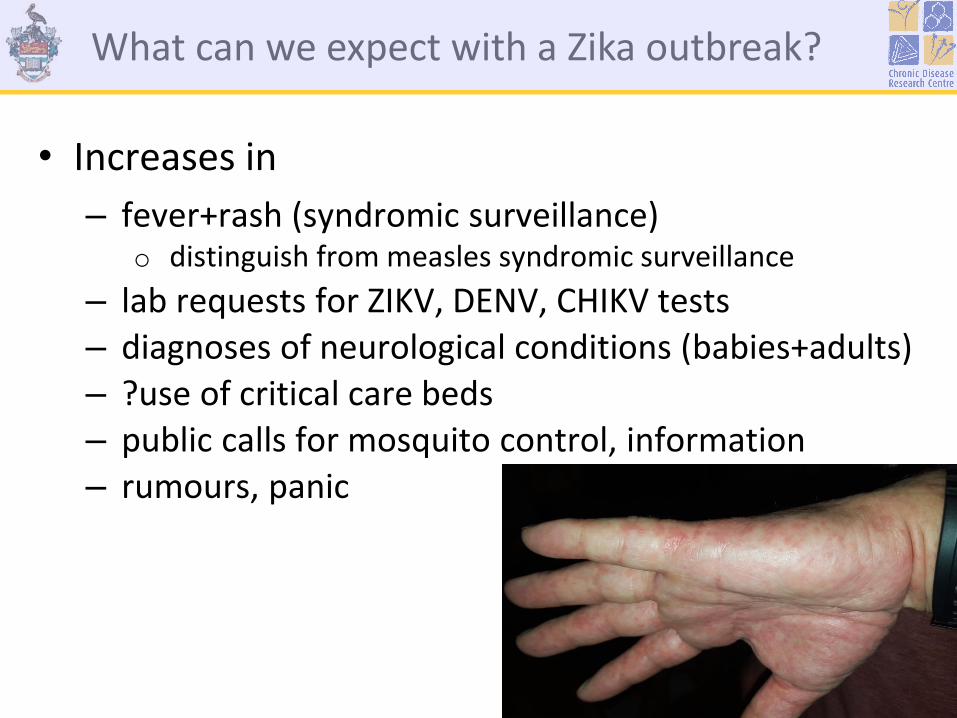
• Increases in
– fever+rash (syndromic surveillance) o distinguish from measles syndromic surveillance
– lab requests for ZIKV, DENV, CHIKV tests – diagnoses of neurological conditions (babies+adults) – ?use of critical care beds – public calls for mosquito control, information – rumours, panic
15
What can we expect with a Zika outbreak?

• Detect
– surveillance strengthening o GBS surveillance, birth defect surveillance if none o arbovirus surveillance in mosquitoes o strengthening lab platform
• Prevent – step up vector-control activities
o insecticide monitoring tool
• Respond – risk communication, public awareness
– prepare health services o children born with neurological compliactions; adults with GBS
– clinical, radiology and lab work
– universal coverage for health services
PAHO: 3 pillars of control
P
rom
ote
re
se
arc
h a
nd g
enera
tion o
f evid
ence
17
Example from Barbados
• Strategic Management Team – intensive integrated management strategy
o ZIKV, DENV, CHIKV vector reduction/elimination
o Aedes aegypti
– addresses all six pillars (WHO) and three pillars (PAHO)
• Strengthened laboratory capacity
• Epidemiological surveillance – collect and analyse data weekly from various sources
– private and public sector facilities
– information for planning and response
18
Example from Barbados
(“detect”)
• Mosquito surveillance, prevention and control activities
– house to house inspections
– surveillance at ports of entry
– use of GIS/GPS in decision-making
– fogging of high risk areas o permethrin for sensitive locales (schools, health facilities)
• Integrated vector management – collaboration with tourism and other partners – mosquito breeding places
o identify and eliminate in communities 19
Example from Barbados
(“prevent”)
(“ prevent… respond”)
• Clinical case management – treatment guidelines for Zika management
– interim guidelines for pregnant women at risk o prevention, treatment, testing
• Community engagement – press releases
– advice to pregnant women
– intensification of public education o mosquito control and behaviour modification (household)
20
Example from Barbados
(“respond”)

• Detect, prevent, respond
• Lessons learned from Ebola
– community engagement is key (prev’n, info’n, rumour, stigma)
– strengthen surveillance (human and vector), lab capacity
– maintain routine healthcare services
– all-of-government, all-of-society approach
• Barbados: preparation
has started
21
Summary
“It’s not the strongest species that survive,
nor the most intelligent – but the ones
most responsive to change”
Charles Darwin
Acknowledgements
• Barbados Ministry of Health colleagues
• WHO GOARN Operational Support Team •
• PAHO colleagues