2016 anatomy of asana - the yoga space...adho mukha svanasana abdomen • gentle drawing of uddiyana...
TRANSCRIPT
8/12/16
1
Anatomy of Asana Presented by Stephen Byrne
Learning objectives
Relate basics of Anatomy to Asana Understand the systems of movement
Observe movement in relation to Yoga Asana
Actively apply the theoretical learning to teaching Yoga
Learning activities
Lectures Discussion
Role play
Practicums
Activities
In class observation Successful completion in class activity
Ability to work in a group
Teaching skills
8/12/16
2
Anatomy Review
Anatomical Terms • Planes of movement • Directions of movement: Relate to the joint NOT the bones!
• AB/ADDduction, Extension, Flexion, In/Ex-Rotation, at the joint!
Beginning to observe what specific muscles and bones make up important joint / body complexes. • Body disassociation: how we move
Keep studying anatomy (wikipedia!)
THEIME: Atlas of Anatomy Manual of Structural
Kinesiology
Anatomy of Asana
Looking at the body systems that allow performance of Asana • Balance
• Systems of balance
• Structure • Associate the structures of the body relevant to an Asana
• Movement • How we get there and what may restrict us
Balance and Proprioception
Balance: “An even distribution of weight enabling someone or something to remain upright and steady.”
1. Vision: External visual reference point 2. Proprioception: Joint position, muscle forces 3. Vestibular System: Inner ear balance Contributing - Affective Factors: • Pain • Muscular strength and control • Fatigue • Surface / BoS
8/12/16
3
Balance and Proprioception Injury and Pain: • Reduces proprioception
• Mind is busy with pain signals • Fatigue causes similar effect
• Muscular System • Reduced or over activation • Forms adaptive protective patterns
• May become maladaptive • Ligaments
• Host a great array of receptors • Strains and associated inflammation
block these receptors. • Full tears ruin reception completely.
Balance and Proprioception: Training Practice, Practice, Practice: • Practice integrating all body systems. • Bias particular systems:
• Vision: mirrors? drishti? • Proprioception: handling? • Vestibular: medication, handling? • Musculoskeletal: Exercise!
Retraining specific strategies: • Where is deficit?
• Ankle/Knee/Hip/Other • Compensatory locking (knee, ankle, etc)? • Muscle weakness?
Base of Support (BoS) Base of Support • The area of the body in contact with a
stability assisting surface
• Typically the area, on the floor, from one foot to the other.
• BoS may be increased by a walking aid. • Consider the BoS for some varying Asana
Base of Support (BoS)
8/12/16
4
Center of Mass (CoM) Center of Mass (CoM) • The central balance point of all mass in a
body.
• Interchangeably: Center of Gravity
• At this point: the sum of all mass causing torque in the body is zero.
• i.e. the body is balanced around this point.
• CoM Changes: • Where does CoM go when pregnant? • When wearing a backpack? • Holding a briefcase?
BoSCoM Center of Mass and Base of Support relate to stop us falling over!
If our CoM falls outside of the BoS we fall.
BoSCoM So how does this work?
BoSCoM: Activity Small groups (Four?) Each choose an Asana (or just any interesting / complex posture) Partners will explore your Base of Support Partners will explore your Center of Mass Partners will effect your Center of Mass with weight (Touching, holding a bolster, etc) How would this affect your teaching / adjusting methods? Everyone gets a go as the model
8/12/16
5
Flexibility “The property of being flexible; easily bent or shaped.” What effects flexibility: • Muscles • Fascial structures • Joint capsules • Neural structures • Nervous control • Activity • All the above effected by injury
Flexibility Muscles: • Increasing length between Origin and Attachment. • Trained through stretching exercises
• What is the process of increased flexibility? • Increased muscle cell count? • Reduced nervous re-activation?
• Heating effects muscle length • Internal is greater than external heating
• Greater blood flow or just comfort?
Flexibility Fascia: • Responsible for holding many times it’s weight
in force • Excessive short-range use causes tightening
and toughening • Adhesions may develop. Securing Fascia to
local structures (i.e. not sliding) • How to Lengthen:
• Heat: Deep • Naturally over an active day • Body Work • Long hold stretches accompanied by relaxed
muscle
Flexibility Joint capsules: • A form of fascia • Previous slide on fascia relates to joint capsules.
• Specific to Joint Capsules: • More Related to movement (which occurs at the joint!) • Distraction techniques reduce joint immobilisation • Full range of movement exercises required to exercise whole of
joint capsule. • Ageing process naturally reduces joint mobility
• Joint capsule range may be inhibited by boney structure of the joint capsule
8/12/16
6
Flexibility Nervous Structures: • Nerves stemming from the spinal cord innervate the whole body. • These nerves are required to follow the length of any available
Range of Movement.
• A common source of strong pain (i.e. Sciatica) • Due to immobility or irritation • Pins / burning / numbness
• Typically not considered able to “stretch” • How do they stretch as we grow from child > adult?
Activity: Slump Test
Flexibility Nervous Control: • Muscles (perhaps fascia??) are controlled by nerves. • If the nervous system innervates the muscle to contract then
flexibility will be decreased. • Consider breathing into source of inflexibility. • Mindful release of physical tension.
• Serious injury or anxiety may block our conscious release of Nervous Control
• The shaking muscle observation
Flexibility Activity • All the above factors are effected by activity or exercise. • Day tasks:
• Sitting • Surfing • Mechanics • Teaching Yoga
• Whole body systems are trained to adapt to regular activities. • Thus Daily yoga practice!
Flexibility Injury • Injury restructures the previously listed structures.
• Healing occurs in the same direction of movement. • No rehab causes healing to be bundled
• Structures form a messy web with disorganised innervation.
• Rehabilitation causes restructuring to occur in the direction of the performed exercises. • Results in coherent and innervated structures • Better able to accept force in trained direction.
8/12/16
7
Body Levers Basics of Movement • Movement is a product of:
• Force generation (muscle contraction) • Force transference (lever systems)
Simple Levers • Fulcrum, Load, Effort
Body Levers Example levers
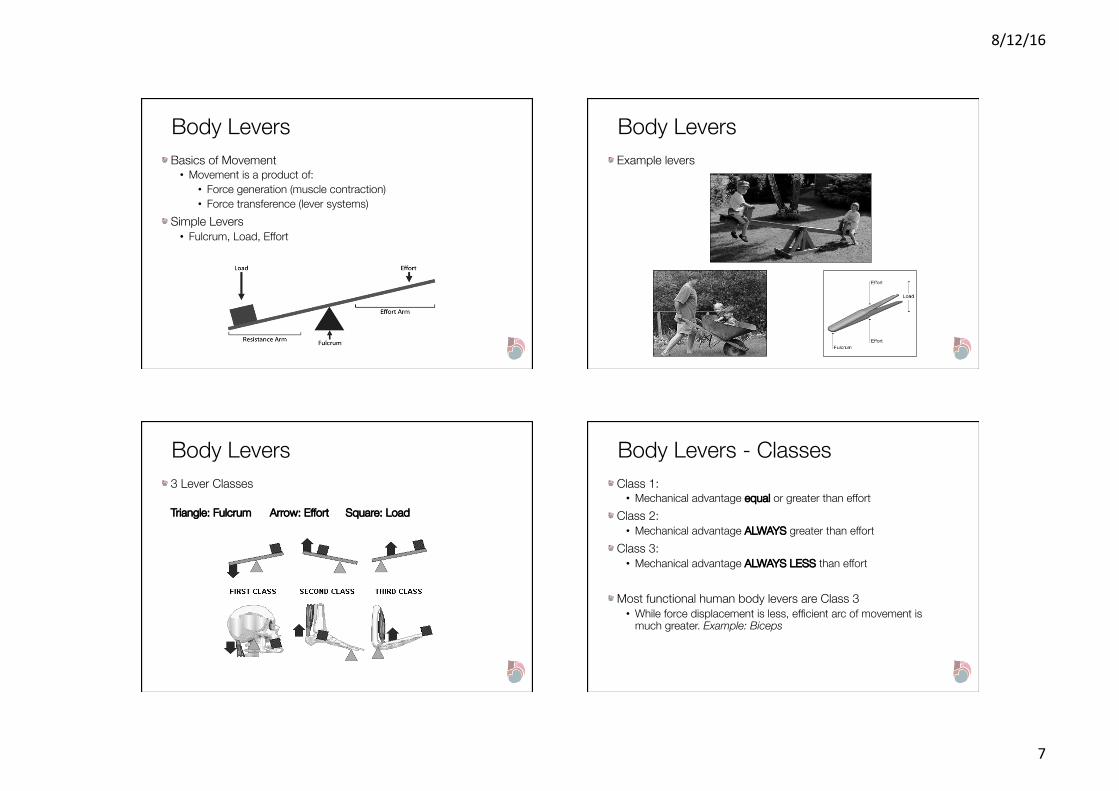
Body Levers 3 Lever Classes
Triangle: Fulcrum Arrow: Effort Square: Load
Body Levers - Classes Class 1: • Mechanical advantage equal or greater than effort
Class 2: • Mechanical advantage ALWAYS greater than effort
Class 3: • Mechanical advantage ALWAYS LESS than effort
Most functional human body levers are Class 3 • While force displacement is less, efficient arc of movement is
much greater. Example: Biceps
8/12/16
8
Body Levers – Short & Long When applying external force the increasing length of a lever increases it’s efficiency. • Re-examine the arc RoM of the biceps
Adjusting • Adjustments exert external force on a students lever • Short levers exert less force • Long levers exert greater force
• Example: Adjust Baddhakonasana
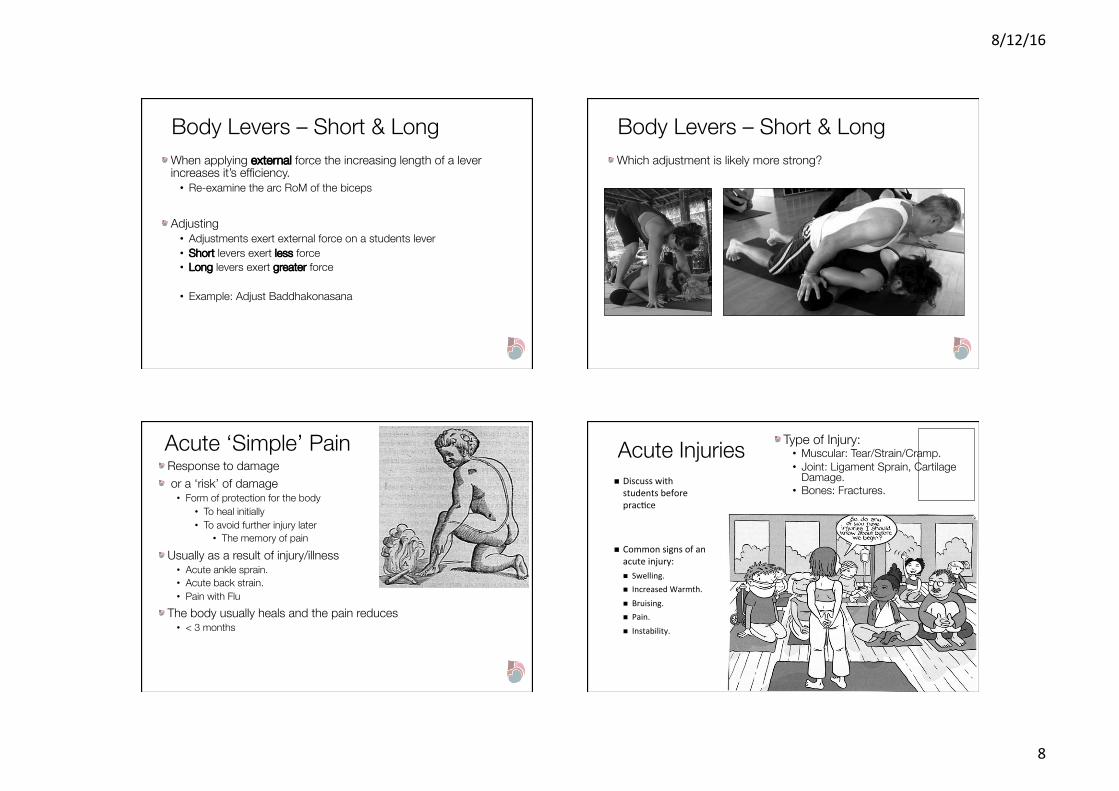
Body Levers – Short & Long Which adjustment is likely more strong?
Acute ‘Simple’ Pain Response to damage or a ‘risk’ of damage • Form of protection for the body
• To heal initially • To avoid further injury later
• The memory of pain Usually as a result of injury/illness • Acute ankle sprain. • Acute back strain. • Pain with Flu
The body usually heals and the pain reduces • < 3 months
Acute Injuries n Discusswithstudentsbeforeprac<ce
n Commonsignsofanacuteinjury:n Swelling.n IncreasedWarmth.n Bruising.n Pain.n Instability.
Type of Injury: • Muscular: Tear/Strain/Cramp. • Joint: Ligament Sprain, Cartilage
Damage. • Bones: Fractures.
8/12/16
9
Acute Injury Prevention Can be more difficult than preventing ‘Chronic/Recurring’ injuries • Sometimes difficult to see
coming! • Know your students
before pushing • E.g. Fundamental postures
before advanced postures
Verbal Cues • ‘Slowly’, ‘Controlled’,
‘Being Mindful’
n Observa<onalskillsn E.g.Keyareasnottomiss
n Hyperextensionofjointsn Hinginglowerbackn Lackofobviousstrengthn Pulling/YankingintoPosturesn Pushingexcessively–i.e.Jumpingwithoutcontrol
Flexibility Articular/Joint Structure • Hypomobility: restricted joint range of motion.
• Disuse: • Not taking joints through their full range. • = adhesions and restrictions.
• Joint degeneration in association with aging – continued movement allows for ongoing nutrition to cartilage from synovial fluid movement. • Keep moving!
• Scar tissue formation post surgery/injury. • Yin – Long Holds.
n Hypermobility:excessivejointrangeof
mo<on.n Reduc<oninrestric<onbybothpassive
andac<vestructures.n Gene<cPredisposi<on–collagentypes.n Injurytoligaments–overstretchingof
ligaments.n Pregnancy–influenceofrelaxin.
Flexibility • Practical Implications: • Experience DOMS as a
result – can last 24-36 hours post activity.
• Notable when first starting yoga or picking up after a long break.
n MuscularRestric<onn Lackofextensibilityduetoreducedtensionloading:n i.e.reducedstretching.
n Changeof<ssuecomposi<onwithageing.
n Stretchingbeyondnormalrange=microtears=adapta<on.n Asexperiencedwithstrengtheningbeyondnormalrange.
Flexibility Neural Shortening • There is a continual loosening and tightening
of nerves – particularly when immobile. • Symptoms:
• Burning/pins and needles/altered sensations. • Pain referral.
n Prac<calImplica<ons:n AdhoMukhaSvanasana:par<cularlyfirstthinginthemorning.n Addi<on/reduc<onofcervicalflexion?Influenceonsensa<on.
n Extendedarmwithcontra-laterallateralflexion.
n Cau<on–canbeprovoca<ve.
8/12/16
10
Observation and Verbal Cues Using the previous system • From the ground up • Joints as points of focus
• Movement occurring about the joints Verbal Cues • Use knowledge of anatomy to deepen students
understanding of the posture • Try not to overwhelm
• Demonstrate and bring awareness to a certain muscle/joint/movement prior to integrating terminology into class • E.g. Demonstrate to them the location of the upper trapezius
• Contracting – “Shoulders to ears” • Relaxing – “Shoulders away from ears”
• Refer to multiple times during the class • E.g. Increased thoracic extension vs. lumbar hinging
Surya Namaskar B Sun Salutation B
Tadasana Teach Tadasana with appreciation for the anatomical but not anatomically!
Tadasana Foot • Pronation/Supination
Knee • Positioning • Quadriceps activation
Hips • Excessive external rotation?
• Toes out?
8/12/16
11
Tadasana Pelvis
• Anterior vs. Posterior Tilt Abdomen
• Bracing through the Upper Abdominals • Subtle drawing of Uddiyana Bandha/Mula
Bandha
Spine • Increased Lumbar Lordosis/
Hinging • Chin Protraction
• Increased cervical lordosis
Shoulder • Elevation - > Upper
Trapezius Activation
Uttanasana"Forward Bending Spinal movement • Observe side on and from behind
• Fluidity of movement between each vertebrae
• Groups moving together – points of hinging – left or right shift (unloading/loading)
Knees raised • Knees extended or flexed • Quadriceps active
• Reciprocal Inhibition of hamstrings.
Uttanasana"Forward Bending
Hamstring vs Lumbar Length • Lumbar length (Quadratus
Lumborum/Erector Spinae) • Minimal pelvic shift
• Hamstring length • Anterior tilt of pelvis – raising of
ischial tuberosities
Compare with Paschimottanasna
Uttanasana"Forward Bending
n VerbalCuesn “Controlledloweringofthespine”n “Vertebraebyvertebrae”
n Cau<on–explainfurthern “Li9ingthesitbones”n “Breathingintothelowerleg,backofthigh,lowerback”n V.s.“Calves,hamstringsandthoracolumbarfascia”
n Explaintostudents++
8/12/16
12
Chaturanga Downward Facing Dog"Adho Mukha Svanasana Wrist/Hands
• Weight in the heel of the hands? • Spreading of the fingers
Elbows • Slight bend/avoiding hyperextension
• Cocontraction
Shoulders • Shoulder blades moving along the back • External rotation/Away from the ears
• Winging? • Opening through the chest • Shoulder blades coming together
Downward Facing Dog"Adho Mukha Svanasana
Abdomen • Gentle drawing of Uddiyana Bandha/Lower Abdominals
• Avoid “Clench”/ “Brace” • Lengthening through the obliques/space between the ribs
Pelvis • Tuck – lumbar fascia • Lift – hamstrings
Knees • Lift the knee caps • Note hyperextension
Feet • Shifting weight to the back
• Lifting sit bones up and back
Urdhva Mukha Svanasna"Upward Facing Dog E.g. • Wrist/Hands
• Weight in the heel of the hands • Increased difficulty compared to Down
Dog • With increased weight bearing
8/12/16
13
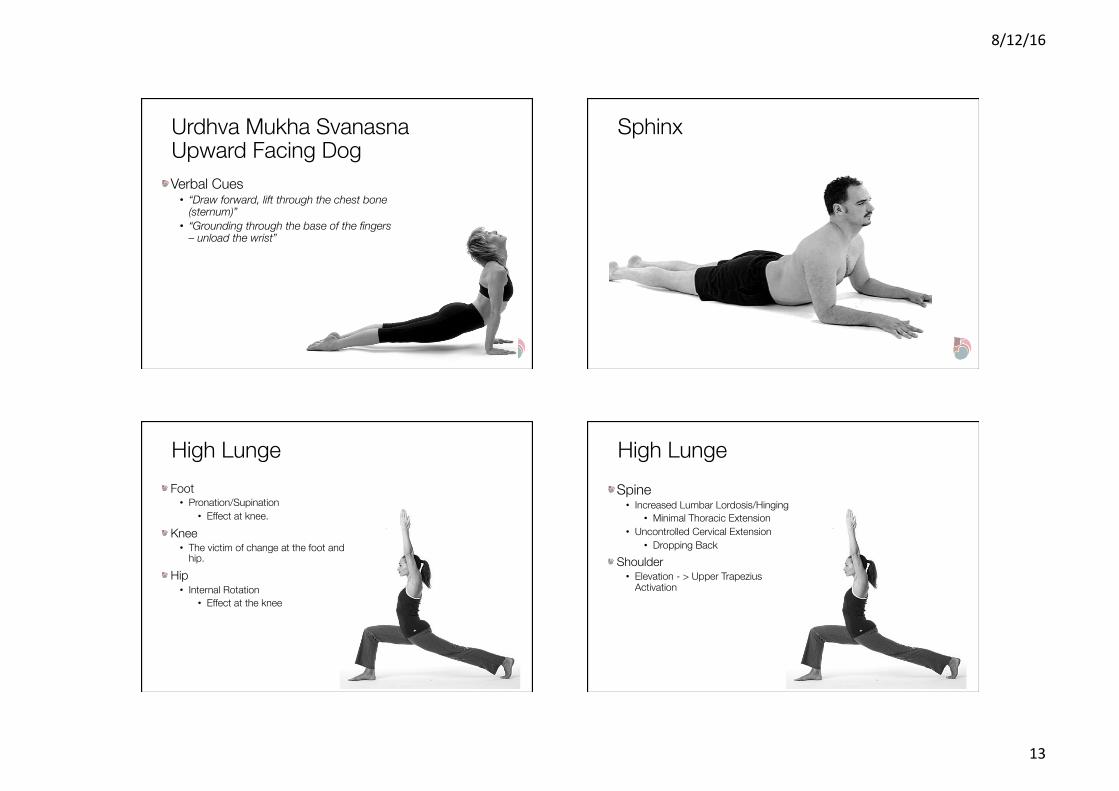
Urdhva Mukha Svanasna"Upward Facing Dog Verbal Cues • “Draw forward, lift through the chest bone
(sternum)” • “Grounding through the base of the fingers
– unload the wrist”
Sphinx
High Lunge Foot • Pronation/Supination
• Effect at knee. Knee • The victim of change at the foot and
hip. Hip • Internal Rotation
• Effect at the knee
High Lunge Spine • Increased Lumbar Lordosis/Hinging
• Minimal Thoracic Extension • Uncontrolled Cervical Extension
• Dropping Back Shoulder • Elevation - > Upper Trapezius
Activation
8/12/16
14
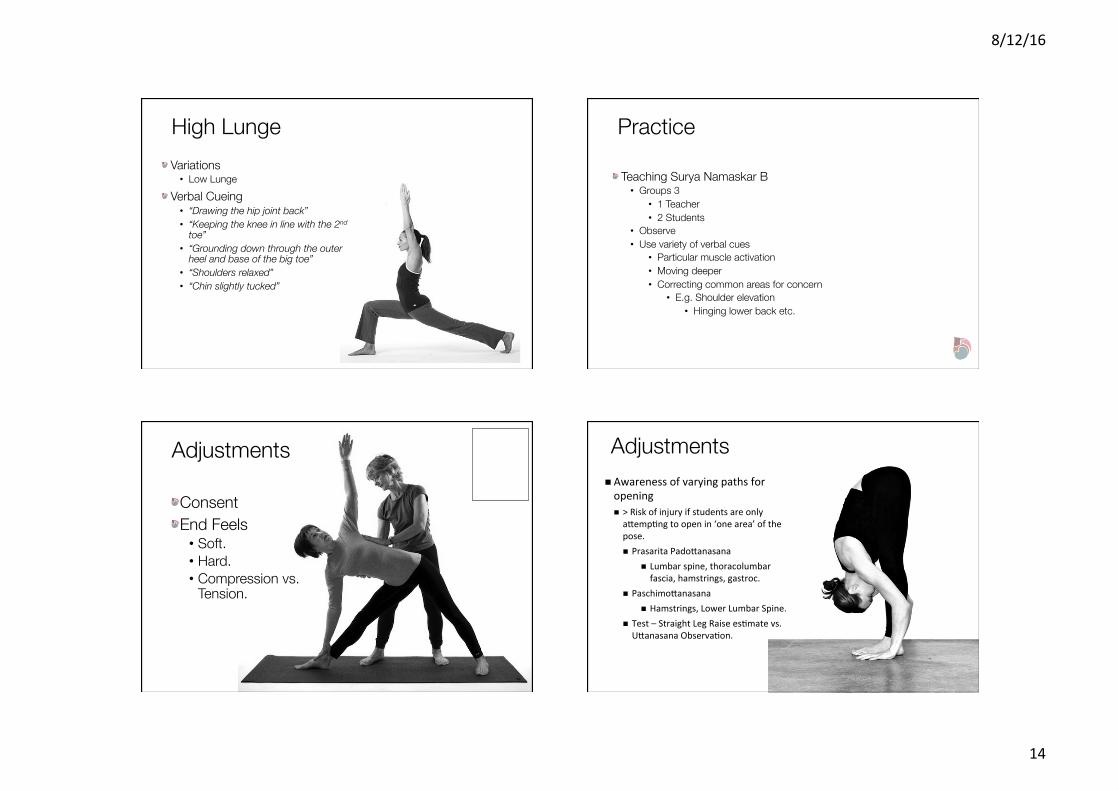
High Lunge Variations • Low Lunge
Verbal Cueing • “Drawing the hip joint back” • “Keeping the knee in line with the 2nd
toe” • “Grounding down through the outer
heel and base of the big toe” • “Shoulders relaxed” • “Chin slightly tucked”
Practice
Teaching Surya Namaskar B • Groups 3
• 1 Teacher • 2 Students
• Observe • Use variety of verbal cues
• Particular muscle activation • Moving deeper • Correcting common areas for concern
• E.g. Shoulder elevation • Hinging lower back etc.
Adjustments
Consent End Feels • Soft. • Hard. • Compression vs.
Tension.
Adjustments n Awarenessofvaryingpathsforopeningn >Riskofinjuryifstudentsareonlyacemp<ngtoopenin‘onearea’ofthepose.n PrasaritaPadocanasana
n Lumbarspine,thoracolumbarfascia,hamstrings,gastroc.
n Paschimocanasanan Hamstrings,LowerLumbarSpine.
n Test–StraightLegRaisees<matevs.UcanasanaObserva<on.
8/12/16
15
Basic Acute Injury Management E.g. Post a tear/strain of connective tissue/muscle fibers e.g. Hamstring strain • Connective tissue- adhesion formation/restriction to movement.
• LIGHT stretching during the first 48 hours to allow for the fibers to heal in correct alignment – providing functional tissue formation.
• Reduce time holding the stretch – increased frequency. • Return to modified practice
SPRICERM • For sprains/strains acute injury. • Not always the case for chronic/recurring injury. Sometimes yes sometimes no.
Referral
Chronic ‘Complex’ Pain
“Pain that persists after an injury has healed or after and illness has passed.”
Timeframe • Usually > 3 months. • Without significant re-injury – recurrent ankle sprains
that keep getting better.
Chronic ‘Complex’ Pain II Involves a broader ‘systemic’ problem • Immune, hormonal and endocrine systems involved • Behavioural and emotional components • ‘Yellow Flags’ commonly present
• Fear avoidance behaviors • Pain is continuing to = damage. • Start to fear particular movements unnecessarily
• Catastrophising – High anxiety levels associated with pain.
• > Peripheral Sensitisation • Central Sensitisation
• Neural processing of pain is altered.
Chronic ‘Complex’ Pain III Implications for Management • Unlikely to respond completely to a solely
musculoskeletal based approach.
• Holistic Approach Needed • Education • Multidisciplinary approach • Revision of case and prognosis

8/12/16
16
Chronic Pain IV Beneficial Aspects of Yoga • Understanding of key postures enables observation of adaptive/maladaptive
changes. • Essential to keep moving.
• Controlled movement with a variety of props/supportive elements. • Mindfulness/Meditation:
• Walking Meditation/Bodyscan: Reveal interesting information about an injury/bodily change. • Blockages and limitations in sensory awareness often demonstrated.
• Yoga Nidra/Meditation: • Enable an increased sense of present awareness: shown to facilitate
a reduction in catastrophising behaviors.